
Is mHealth a Useful Tool for Self-Assessment and Rehabilitation of People with Multiple Sclerosis? A Systematic Review


Abstract
:1. Introduction
2. Methods
2.1. Search Strategy and Selection Criteria
2.2. Eligibility Criteria
- Population: pwMS performing training (rehabilitation exercises) or self-assessment in home-environment, studies with inpatient treatment or assisted-rehabilitation were not included.
- Intervention: mHealth rehabilitation intervention (planned and supervised interventions), or self-assessment studies with repeated measurements over time, using any type of support (e.g., smartphones, phones, apps, web applications). Studies using non-specific games, virtual reality or active video games (e.g., Nintendo Wii, Microsoft Xbox Kinect), or computer-supported therapy were not included.
- Control: usual care or no intervention.
- Outcome measures: any type of outcome measure related to the International Classification of Functioning, Disability and Health (ICF).
- Study design: RCTs, explorative studies.
2.3. Quality Assessment
2.4. Data Extraction
2.5. Statistical Analysis
2.6. Ethical Approval
3. Results
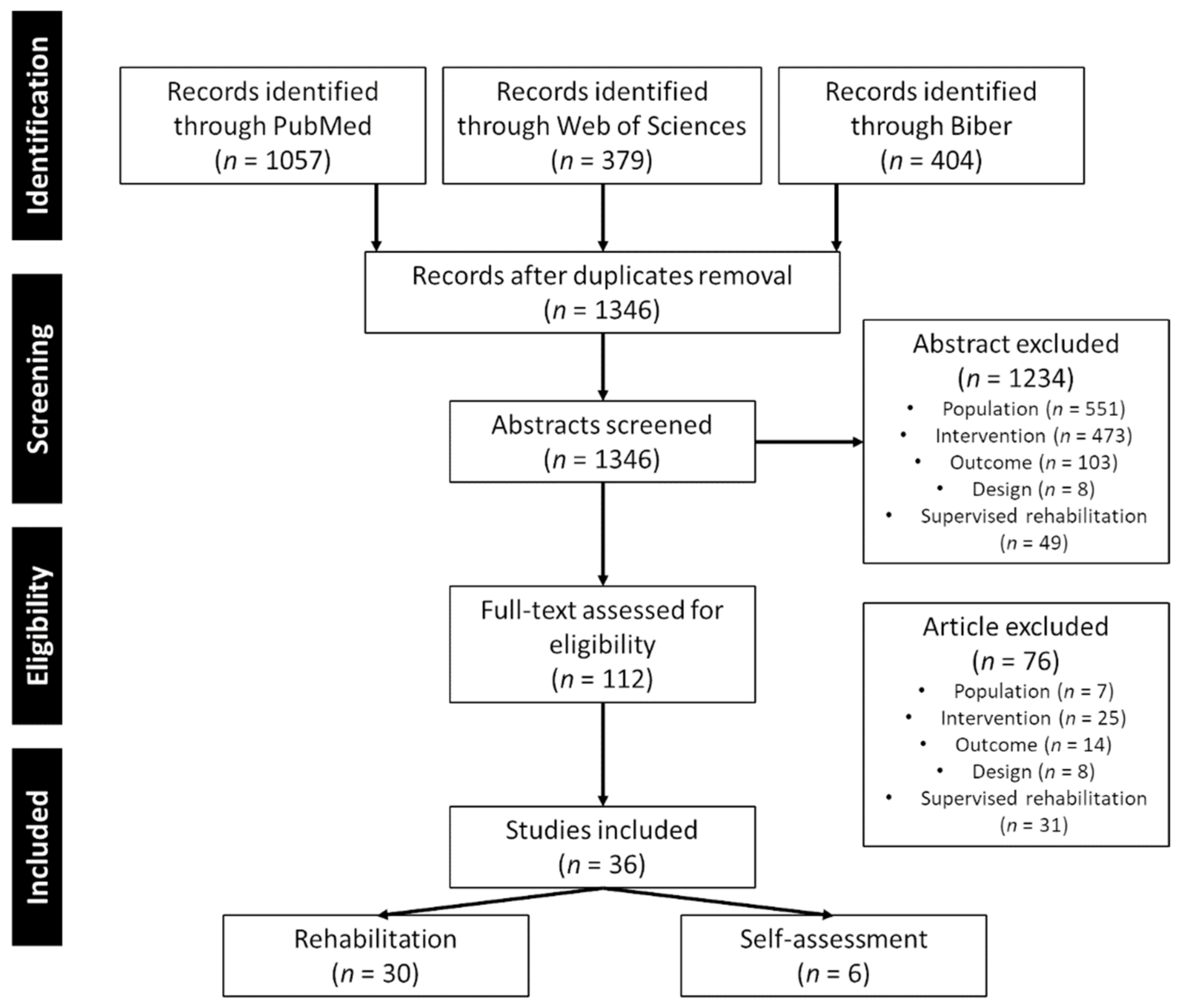
3.1. Search Results
3.2. Characteristics of the Included Studies
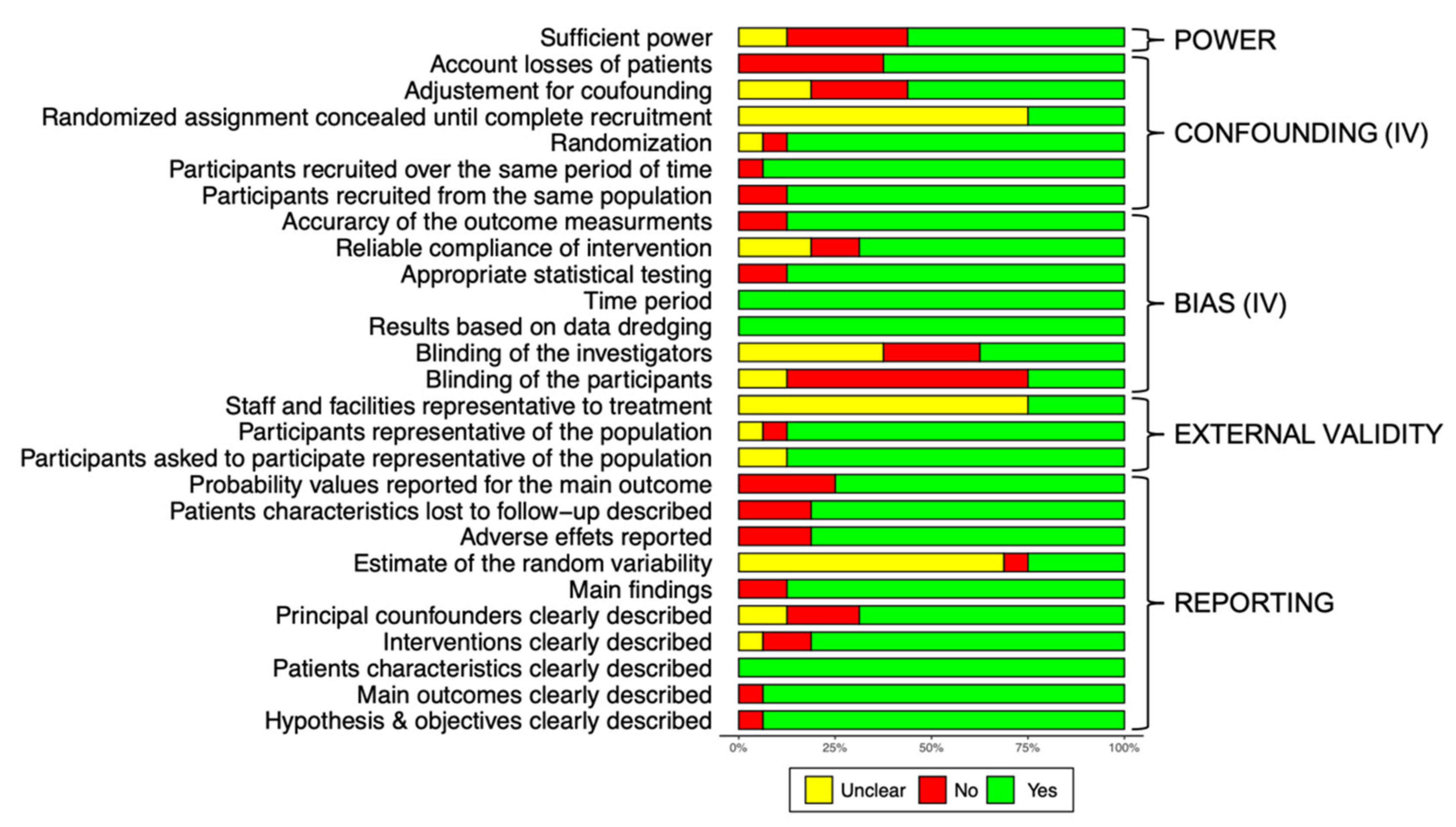
3.3. Quality Assessment
3.4. Description of the Available mHealth Solutions
3.5. Outcome Data Related to ICF
3.5.1. Rehabilitation
3.5.2. Self-Assessment
3.6. Summary
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Papanicolas, I.; Mossialos, E.; Gundersen, A.; Woskie, L.; Jha, A.K. Performance of UK National Health Service Compared with Other High Income Countries: Observational Study. BMJ 2019, 367, l6326. [Google Scholar] [CrossRef] [Green Version]
- Flachenecker, P.; Buckow, K.; Pugliatti, M.; Kes, V.B.; Battaglia, M.A.; Boyko, A.; Confavreux, C.; Ellenberger, D.; Eskic, D.; Ford, D.; et al. Multiple Sclerosis Registries in Europe—Results of a Systematic Survey. Mult. Scler. 2014, 20, 1523–1532. [Google Scholar] [CrossRef]
- WHO. Fact Sheets: Rehabilitation. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/rehabilitation (accessed on 1 July 2021).
- Statista. Number of Smartphone Users Worldwide from 2016 to 2026. Available online: https://www.statista.com/statistics/330695/number-of-smartphone-users-worldwide/ (accessed on 6 July 2021).
- Anderson, K.; Burford, O.; Emmerton, L. Mobile Health Apps to Facilitate Self-Care: A Qualitative Study of User Experiences. PLoS ONE 2016, 11, e0156164. [Google Scholar] [CrossRef] [Green Version]
- Birkhoff, S.D.; Smeltzer, S.C. Perceptions of Smartphone User-Centered Mobile Health Tracking Apps Across Various Chronic Illness Populations: An Integrative Review. J. Nurs. Sch. 2017, 49, 371–378. [Google Scholar] [CrossRef]
- Hernandez Silva, E.; Lawler, S.; Langbecker, D. The Effectiveness of MHealth for Self-Management in Improving Pain, Psychological Distress, Fatigue, and Sleep in Cancer Survivors: A Systematic Review. J. Cancer Surviv. 2019, 13, 97–107. [Google Scholar] [CrossRef] [PubMed]
- Zheng, C.; Chen, X.; Weng, L.; Guo, L.; Xu, H.; Lin, M.; Xue, Y.; Lin, X.; Yang, A.; Yu, L.; et al. Benefits of Mobile Apps for Cancer Pain Management: Systematic Review. JMIR Mhealth Uhealth 2020, 8, e17055. [Google Scholar] [CrossRef] [PubMed]
- Kapoor, A.; Nambisan, P.; Baker, E. Mobile Applications for Breast Cancer Survivorship and Self-Management: A Systematic Review. Health Inform. J. 2020, 26, 2892–2905. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Long, H. The Effect of Smartphone App-Based Interventions for Patients With Hypertension: Systematic Review and Meta-Analysis. JMIR Mhealth Uhealth 2020, 8, e21759. [Google Scholar] [CrossRef] [PubMed]
- Giebel, G.D.; Gissel, C. Accuracy of MHealth Devices for Atrial Fibrillation Screening: Systematic Review. JMIR Mhealth Uhealth 2019, 7, e13641. [Google Scholar] [CrossRef] [PubMed]
- Bateman, D.R.; Srinivas, B.; Emmett, T.W.; Schleyer, T.K.; Holden, R.J.; Hendrie, H.C.; Callahan, C.M. Categorizing Health Outcomes and Efficacy of MHealth Apps for Persons With Cognitive Impairment: A Systematic Review. J. Med. Internet Res. 2017, 19, e301. [Google Scholar] [CrossRef] [PubMed]
- Elavsky, S.; Knapova, L.; Klocek, A.; Smahel, D. Mobile Health Interventions for Physical Activity, Sedentary Behavior, and Sleep in Adults Aged 50 Years and Older: A Systematic Literature Review. J. Aging Phys. Act. 2019, 27, 565–593. [Google Scholar] [CrossRef] [PubMed]
- Rintala, A.; Hakala, S.; Paltamaa, J.; Heinonen, A.; Karvanen, J.; Sjögren, T. Effectiveness of Technology-Based Distance Physical Rehabilitation Interventions on Physical Activity and Walking in Multiple Sclerosis: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Disabil. Rehabil. 2018, 40, 373–387. [Google Scholar] [CrossRef]
- Marziniak, M.; Brichetto, G.; Feys, P.; Meyding-Lamadé, U.; Vernon, K.; Meuth, S.G. The Use of Digital and Remote Communication Technologies as a Tool for Multiple Sclerosis Management: Narrative Review. JMIR Rehabil. Assist. Technol. 2018, 5, e5. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- Downs, S.H.; Black, N. The Feasibility of Creating a Checklist for the Assessment of the Methodological Quality Both of Randomised and Non-Randomised Studies of Health Care Interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deeks, J.J.; Dinnes, J.; D’Amico, R.; Sowden, A.J.; Sakarovitch, C.; Song, F.; Petticrew, M.; Altman, D.G.; International Stroke Trial Collaborative Group; European Carotid Surgery Trial Collaborative Group. Evaluating Non-Randomised Intervention Studies. Health Technol. Assess. 2003, 7, 1–173. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.; Welch, V. Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; Wiley-Blackwell: Hoboken, NJ, USA, 2019; ISBN 978-1-119-53662-8. [Google Scholar]
- Carter, E.C.; Schönbrodt, F.D.; Gervais, W.M.; Hilgard, J. Correcting for Bias in Psychology: A Comparison of Meta-Analytic Methods. Adv. Methods Pract. Psychol. Sci. 2019, 2, 115–144. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Sutton, A.J.; Ioannidis, J.P.A.; Terrin, N.; Jones, D.R.; Lau, J.; Carpenter, J.; Rücker, G.; Harbord, R.M.; Schmid, C.H.; et al. Recommendations for Examining and Interpreting Funnel Plot Asymmetry in Meta-Analyses of Randomised Controlled Trials. BMJ 2011, 343, d4002. [Google Scholar] [CrossRef] [Green Version]
- Pustejovsky, J.E.; Rodgers, M.A. Testing for Funnel Plot Asymmetry of Standardized Mean Differences. Res. Synth. Methods 2019, 10, 57–71. [Google Scholar] [CrossRef] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLOS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Cerasa, A.; Gioia, M.C.; Valentino, P.; Nisticò, R.; Chiriaco, C.; Pirritano, D.; Tomaiuolo, F.; Mangone, G.; Trotta, M.; Talarico, T.; et al. Computer-Assisted Cognitive Rehabilitation of Attention Deficits for Multiple Sclerosis: A Randomized Trial with FMRI Correlates. Neurorehabil. Neural Repair 2013, 27, 284–295. [Google Scholar] [CrossRef]
- Amato, M.; Goretti, B.; Viterbo, R.; Portaccio, E.; Niccolai, C.; Hakiki, B.; Iaffaldano, P.; Trojano, M. Computer-Assisted Rehabilitation of Attention in Patients with Multiple Sclerosis: Results of a Randomized, Double-Blind Trial. Mult. Scler. 2014, 20, 91–98. [Google Scholar] [CrossRef]
- Charvet, L.; Shaw, M.; Haider, L.; Melville, P.; Krupp, L. Remotely-Delivered Cognitive Remediation in Multiple Sclerosis (MS): Protocol and Results from a Pilot Study. Mult. Scler. J.—Exp. Transl. Clin. 2015, 1, 205521731560962. [Google Scholar] [CrossRef] [Green Version]
- Hancock, L.M.; Bruce, J.M.; Bruce, A.S.; Lynch, S.G. Processing Speed and Working Memory Training in Multiple Sclerosis: A Double-Blind Randomized Controlled Pilot Study. J. Clin. Exp. Neuropsychol. 2015, 37, 113–127. [Google Scholar] [CrossRef]
- Hubacher, M.; Kappos, L.; Weier, K.; Stöcklin, M.; Opwis, K.; Penner, I.-K. Case-Based FMRI Analysis after Cognitive Rehabilitation in MS: A Novel Approach. Front. Neurol. 2015, 6, 78. [Google Scholar] [CrossRef] [Green Version]
- Fischer, A.; Schröder, J.; Vettorazzi, E.; Wolf, O.T.; Pöttgen, J.; Lau, S.; Heesen, C.; Moritz, S.; Gold, S.M. An Online Programme to Reduce Depression in Patients with Multiple Sclerosis: A Randomised Controlled Trial. Lancet Psychiatry 2015, 2, 217–223. [Google Scholar] [CrossRef]
- Campbell, J.; Langdon, D.; Cercignani, M.; Rashid, W. A Randomised Controlled Trial of Efficacy of Cognitive Rehabilitation in Multiple Sclerosis: A Cognitive, Behavioural, and MRI Study. Neural Plast. 2016, 2016, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Pedullà, L.; Brichetto, G.; Tacchino, A.; Vassallo, C.; Zaratin, P.; Battaglia, M.A.; Bonzano, L.; Bove, M. Adaptive vs. Non-Adaptive Cognitive Training by Means of a Personalized App: A Randomized Trial in People with Multiple Sclerosis. J. Neuroeng. Rehabil. 2016, 13, 88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charvet, L.E.; Yang, J.; Shaw, M.T.; Sherman, K.; Haider, L.; Xu, J.; Krupp, L.B. Cognitive Function in Multiple Sclerosis Improves with Telerehabilitation: Results from a Randomized Controlled Trial. PLoS ONE 2017, 12, e0177177. [Google Scholar] [CrossRef]
- Messinis, L.; Nasios, G.; Kosmidis, M.H.; Zampakis, P.; Malefaki, S.; Ntoskou, K.; Nousia, A.; Bakirtzis, C.; Grigoriadis, N.; Gourzis, P.; et al. Efficacy of a Computer-Assisted Cognitive Rehabilitation Intervention in Relapsing-Remitting Multiple Sclerosis Patients: A Multicenter Randomized Controlled Trial. Behav. Neurol. 2017, 2017, 1–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conroy, S.S.; Zhan, M.; Culpepper, W.J.; Royal, W.; Wallin, M.T. Self-Directed Exercise in Multiple Sclerosis: Evaluation of a Home Automated Tele-Management System. J. Telemed. Telecare 2018, 24, 410–419. [Google Scholar] [CrossRef]
- Stuifbergen, A.K.; Becker, H.; Perez, F.; Morrison, J.; Brown, A.; Kullberg, V.; Zhang, W. Computer-Assisted Cognitive Rehabilitation in Persons with Multiple Sclerosis: Results of a Multi-Site Randomized Controlled Trial with Six Month Follow-Up. Disabil. Health J. 2018, 11, 427–434. [Google Scholar] [CrossRef]
- Fjeldstad-Pardo, C.; Thiessen, A.; Pardo, G. Telerehabilitation in Multiple Sclerosis: Results of a Randomized Feasibility and Efficacy Pilot Study. Int. J. Telerehabil. 2018, 10, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Pöttgen, J.; Moss-Morris, R.; Wendebourg, J.-M.; Feddersen, L.; Lau, S.; Köpke, S.; Meyer, B.; Friede, T.; Penner, I.-K.; Heesen, C.; et al. Randomised Controlled Trial of a Self-Guided Online Fatigue Intervention in Multiple Sclerosis. J. Neurol. Neurosurg. Psychiatry 2018, 89, 970–976. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cavalera, C.; Rovaris, M.; Mendozzi, L.; Pugnetti, L.; Garegnani, M.; Castelnuovo, G.; Molinari, E.; Pagnini, F. Online Meditation Training for People with Multiple Sclerosis: A Randomized Controlled Trial. Mult. Scler. 2019, 25, 610–617. [Google Scholar] [CrossRef]
- Chiaravalloti, N.D.; Goverover, Y.; Costa, S.L.; DeLuca, J. A Pilot Study Examining Speed of Processing Training (SPT) to Improve Processing Speed in Persons With Multiple Sclerosis. Front. Neurol. 2018, 9, 685. [Google Scholar] [CrossRef]
- Plow, M.; Finlayson, M.; Liu, J.; Motl, R.W.; Bethoux, F.; Sattar, A. Randomized Controlled Trial of a Telephone-Delivered Physical Activity and Fatigue Self-Management Interventions in Adults With Multiple Sclerosis. Arch. Phys. Med. Rehabil. 2019, 100, 2006–2014. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, T.A.; Ziccardi, S.; Dwyer, M.G.; Charvet, L.E.; Bartnik, A.; Campbell, R.; Escobar, J.; Hojnacki, D.; Kolb, C.; Oship, D.; et al. Response Heterogeneity to Home-Based Restorative Cognitive Rehabilitation in Multiple Sclerosis: An Exploratory Study. Mult. Scler. Relat. Disord. 2019, 34, 103–111. [Google Scholar] [CrossRef]
- Vilou, I.; Bakirtzis, C.; Artemiadis, A.; Ioannidis, P.; Papadimitriou, M.; Konstantinopoulou, E.; Aretouli, E.; Messinis, L.; Nasios, G.; Dardiotis, E.; et al. Computerized Cognitive Rehabilitation for Treatment of Cognitive Impairment in Multiple Sclerosis: An Explorative Study. J. Integr. Neurosci. 2020, 19, 341–347. [Google Scholar] [CrossRef]
- Jeong, I.C.; Liu, J.; Finkelstein, J. Association Between System Usage Pattern and Impact of Web-Based Telerehabilitation in Patients with Multiple Sclerosis. Stud. Health Technol. Inform. 2020, 272, 346–349. [Google Scholar] [CrossRef]
- Kratz, A.L.; Atalla, M.; Whibley, D.; Myles, A.; Thurston, T.; Fritz, N.E. Calling Out MS Fatigue: Feasibility and Preliminary Effects of a Pilot Randomized Telephone-Delivered Exercise Intervention for Multiple Sclerosis Fatigue. J. Neurol. Phys. Ther. 2020, 44, 23–31. [Google Scholar] [CrossRef] [Green Version]
- Flachenecker, P.; Bures, A.K.; Gawlik, A.; Weiland, A.-C.; Kuld, S.; Gusowski, K.; Streber, R.; Pfeifer, K.; Tallner, A. Efficacy of an Internet-Based Program to Promote Physical Activity and Exercise after Inpatient Rehabilitation in Persons with Multiple Sclerosis: A Randomized, Single-Blind, Controlled Study. Int. J. Environ. Res. Public Health 2020, 17, 4544. [Google Scholar] [CrossRef]
- Manns, P.J.; Mehrabani, G.; Norton, S.; Aminian, S.; Motl, R.W. The SitLess With MS Program: Intervention Feasibility and Change in Sedentary Behavior. Arch. Rehabil. Res. Clin. Transl. 2020, 2, 100083. [Google Scholar] [CrossRef] [PubMed]
- Donkers, S.J.; Nickel, D.; Paul, L.; Wiegers, S.R.; Knox, K.B. Adherence to Physiotherapy-Guided Web-Based Exercise for Persons with Moderate-to-Severe Multiple Sclerosis: A Randomized Controlled Pilot Study. Int. J. MS Care 2020, 22, 208–214. [Google Scholar] [CrossRef] [Green Version]
- Messinis, L.; Kosmidis, M.H.; Nasios, G.; Konitsiotis, S.; Ntoskou, A.; Bakirtzis, C.; Grigoriadis, N.; Patrikelis, P.; Panagiotopoulos, E.; Gourzis, P.; et al. Do Secondary Progressive Multiple Sclerosis Patients Benefit from Computer- Based Cognitive Neurorehabilitation? A Randomized Sham Controlled Trial. Mult. Scler. Relat. Disord. 2020, 39, 101932. [Google Scholar] [CrossRef] [PubMed]
- Minen, M.T.; Schaubhut, K.B.; Morio, K. Smartphone Based Behavioral Therapy for Pain in Multiple Sclerosis (MS) Patients: A Feasibility Acceptability Randomized Controlled Study for the Treatment of Comorbid Migraine and Ms Pain. Mult. Scler. Relat. Disord. 2020, 46, 102489. [Google Scholar] [CrossRef] [PubMed]
- Van Geel, F.; Geurts, E.; Abasıyanık, Z.; Coninx, K.; Feys, P. Feasibility Study of a 10-Week Community-Based Program Using the WalkWithMe Application on Physical Activity, Walking, Fatigue and Cognition in Persons with Multiple Sclerosis. Mult. Scler. Relat. Disord. 2020, 42, 102067. [Google Scholar] [CrossRef] [PubMed]
- Bove, R.; Rowles, W.; Zhao, C.; Anderson, A.; Friedman, S.; Langdon, D.; Alexander, A.; Sacco, S.; Henry, R.; Gazzaley, A.; et al. A Novel In-Home Digital Treatment to Improve Processing Speed in People with Multiple Sclerosis: A Pilot Study. Mult. Scler. 2021, 27, 778–789. [Google Scholar] [CrossRef] [PubMed]
- Tarakci, E.; Tarakci, D.; Hajebrahimi, F.; Budak, M. Supervised Exercises versus Telerehabilitation. Benefits for Persons with Multiple Sclerosis. Acta. Neurol. Scand. 2021. [Google Scholar] [CrossRef] [PubMed]
- Williams, K.L.; Low Choy, N.L.; Brauer, S.G. Center-Based Group and Home-Based Individual Exercise Programs Have Similar Impacts on Gait and Balance in People With Multiple Sclerosis: A Randomized Trial. PM R 2021, 13, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Miller, D.M.; Moore, S.M.; Fox, R.J.; Atreja, A.; Fu, A.Z.; Lee, J.-C.; Saupe, W.; Stadtler, M.; Chakraborty, S.; Harris, C.M.; et al. Web-Based Self-Management for Patients with Multiple Sclerosis: A Practical, Randomized Trial. Telemed. e-Health 2011, 17, 5–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greiner, P.; Sawka, A.; Imison, E. Patient and Physician Perspectives on MSdialog, an Electronic PRO Diary in Multiple Sclerosis. Patient 2015, 8, 541–550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’hooghe, M.; Van Gassen, G.; Kos, D.; Bouquiaux, O.; Cambron, M.; Decoo, D.; Lysandropoulos, A.; Van Wijmeersch, B.; Willekens, B.; Penner, I.-K.; et al. Improving Fatigue in Multiple Sclerosis by Smartphone-Supported Energy Management: The MS TeleCoach Feasibility Study. Mult. Scler. Relat. Disord. 2018, 22, 90–96. [Google Scholar] [CrossRef] [Green Version]
- Midaglia, L.; Mulero, P.; Montalban, X.; Graves, J.; Hauser, S.L.; Julian, L.; Baker, M.; Schadrack, J.; Gossens, C.; Scotland, A.; et al. Adherence and Satisfaction of Smartphone- and Smartwatch-Based Remote Active Testing and Passive Monitoring in People With Multiple Sclerosis: Nonrandomized Interventional Feasibility Study. J. Med. Internet Res. 2019, 21, e14863. [Google Scholar] [CrossRef] [Green Version]
- Newland, P.; Oliver, B.; Newland, J.M.; Thomas, F.P. Testing Feasibility of a Mobile Application to Monitor Fatigue in People With Multiple Sclerosis. J. Neurosci. Nurs. 2019, 51, 331–334. [Google Scholar] [CrossRef]
- Pratap, A.; Grant, D.; Vegesna, A.; Tummalacherla, M.; Cohan, S.; Deshpande, C.; Mangravite, L.; Omberg, L. Evaluating the Utility of Smartphone-Based Sensor Assessments in Persons With Multiple Sclerosis in the Real-World Using an App (ElevateMS): Observational, Prospective Pilot Digital Health Study. JMIR Mhealth Uhealth 2020, 8, e22108. [Google Scholar] [CrossRef] [PubMed]
- Baddeley, A. Working Memory; Clarendon Press: Oxford, UK; Oxford University Press: Oxford, UK, 1986. [Google Scholar]
- Tacchino, A.; Pedullà, L.; Bonzano, L.; Vassallo, C.; Battaglia, M.A.; Mancardi, G.; Bove, M.; Brichetto, G. A New App for At-Home Cognitive Training: Description and Pilot Testing on Patients with Multiple Sclerosis. JMIR Mhealth Uhealth 2015, 3, e85. [Google Scholar] [CrossRef]
- Sohlberg, M.M.; Mateer, C.A. Effectiveness of an Attention-Training Program. J. Clin. Exp. Neuropsychol. 1987, 9, 117–130. [Google Scholar] [CrossRef]
- Finkelstein, J.; Wood, J.; Shan, Y. Implementing Physical Telerehabilitation System for Patients with Multiple Sclerosis. In Proceedings of the 2011 4th International Conference on Biomedical Engineering and Informatics (BMEI), Shanghai, China, 15–17 October 2011; pp. 1883–1886. [Google Scholar]
- Exell, S.; Thristan, M.; Dangond, F.; Marhardt, K.; St Charles-Krohe, M.; Turner-Bowker, D.M. A Novel Electronic Application of Patient-Reported Outcomes in Multiple Sclerosis—Meeting the Necessary Challenge of Assessing Quality of Life and Outcomes in Daily Clinical Practice. Eur. Neurol. Rev. 2014, 9, 49. [Google Scholar] [CrossRef] [Green Version]
- Williams, A.; Fossey, E.; Farhall, J.; Foley, F.; Thomas, N. Impact of Jointly Using an E-Mental Health Resource (Self-Management And Recovery Technology) on Interactions Between Service Users Experiencing Severe Mental Illness and Community Mental Health Workers: Grounded Theory Study. JMIR Ment. Health 2021, 8, e25998. [Google Scholar] [CrossRef]
- Lampit, A.; Heine, J.; Finke, C.; Barnett, M.H.; Valenzuela, M.; Wolf, A.; Leung, I.H.K.; Hill, N.T.M. Computerized Cognitive Training in Multiple Sclerosis: A Systematic Review and Meta-Analysis. Neurorehabil. Neural. Repair 2019, 33, 695–706. [Google Scholar] [CrossRef] [PubMed]
- Yang, T.-T.; Wang, L.; Deng, X.-Y.; Yu, G. Pharmacological Treatments for Fatigue in Patients with Multiple Sclerosis: A Systematic Review and Meta-Analysis. J. Neurol. Sci. 2017, 380, 256–261. [Google Scholar] [CrossRef]
- Heine, M.; van de Port, I.; Rietberg, M.B.; van Wegen, E.E.H.; Kwakkel, G. Exercise Therapy for Fatigue in Multiple Sclerosis. Cochrane Database Syst. Rev. 2015, CD009956. [Google Scholar] [CrossRef]
- Tramontano, M.; Morone, G.; De Angelis, S.; Casagrande Conti, L.; Galeoto, G.; Grasso, M.G. Sensor-Based Technology for Upper Limb Rehabilitation in Patients with Multiple Sclerosis: A Randomized Controlled Trial. Restor. Neurol. Neurosci. 2020, 38, 333–341. [Google Scholar] [CrossRef] [PubMed]
- Wendebourg, M.J.; Heesen, C.; Finlayson, M.; Meyer, B.; Pöttgen, J.; Köpke, S. Patient Education for People with Multiple Sclerosis-Associated Fatigue: A Systematic Review. PLoS ONE 2017, 12, e0173025. [Google Scholar] [CrossRef]
- Rieckmann, P.; Centonze, D.; Elovaara, I.; Giovannoni, G.; Havrdová, E.; Kesselring, J.; Kobelt, G.; Langdon, D.; Morrow, S.A.; Oreja-Guevara, C.; et al. Unmet Needs, Burden of Treatment, and Patient Engagement in Multiple Sclerosis: A Combined Perspective from the MS in the 21st Century Steering Group. Mult. Scler. Relat. Disord. 2018, 19, 153–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brydges, C.R. Effect Size Guidelines, Sample Size Calculations, and Statistical Power in Gerontology. Innov. Aging 2019, 3, igz036. [Google Scholar] [CrossRef]
- Bonnechère, B.; Langley, C.; Sahakian, B.J. The Use of Commercial Computerised Cognitive Games in Older Adults: A Meta-Analysis. Sci. Rep. 2020, 10, 15276. [Google Scholar] [CrossRef]
- US Food & Drug Administration. FDA Permits Marketing of First Game-Based Digital Therapeutic to Improve Attention Function in Children with ADHD. Available online: https://www.fda.gov/news-events/press-announcements/fda-permits-marketing-first-game-based-digital-therapeutic-improve-attention-function-children-adhd (accessed on 28 June 2021).
- Marra, C.; Gordon, W.J.; Stern, A.D. Use of Connected Digital Products in Clinical Research Following the COVID-19 Pandemic: A Comprehensive Analysis of Clinical Trials. BMJ Open 2021, 11, e047341. [Google Scholar] [CrossRef]
- Carl, J.R.; Jones, D.J.; Lindhiem, O.J.; Doss, B.D.; Weingardt, K.R.; Timmons, A.C.; Comer, J.S. Regulating Digital Therapeutics for Mental Health: Opportunities, Challenges, and the Essential Role of Psychologists. Br. J. Clin. Psychol. 2021. [Google Scholar] [CrossRef]
- Scott Kruse, C.; Karem, P.; Shifflett, K.; Vegi, L.; Ravi, K.; Brooks, M. Evaluating Barriers to Adopting Telemedicine Worldwide: A Systematic Review. J. Telemed. Telecare. 2018, 24, 4–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rangachari, P.; Mushiana, S.S.; Herbert, K. A Narrative Review of Factors Historically Influencing Telehealth Use across Six Medical Specialties in the United States. Int. J. Environ. Res. Public Health 2021, 18, 4995. [Google Scholar] [CrossRef] [PubMed]
- Almathami, H.K.Y.; Win, K.T.; Vlahu-Gjorgievska, E. Barriers and Facilitators That Influence Telemedicine-Based, Real-Time, Online Consultation at Patients’ Homes: Systematic Literature Review. J. Med. Internet Res. 2020, 22, e16407. [Google Scholar] [CrossRef]
- Engelsma, T.; Jaspers, M.W.M.; Peute, L.W. Considerate MHealth Design for Older Adults with Alzheimer’s Disease and Related Dementias (ADRD): A Scoping Review on Usability Barriers and Design Suggestions. Int. J. Med. Inform. 2021, 152, 104494. [Google Scholar] [CrossRef] [PubMed]
- Bevens, W.; Gray, K.; Neate, S.L.; Nag, N.; Weiland, T.J.; Jelinek, G.A.; Simpson-Yap, S. Characteristics of MHealth App Use in an International Sample of People with Multiple Sclerosis. Mult. Scler. Relat. Disord. 2021, 54, 103092. [Google Scholar] [CrossRef]
- Spina, E.; Trojsi, F.; Tozza, S.; Iovino, A.; Iodice, R.; Passaniti, C.; Abbadessa, G.; Bonavita, S.; Leocani, L.; Tedeschi, G.; et al. How to Manage with Telemedicine People with Neuromuscular Diseases? Neurol. Sci. 2021. [Google Scholar] [CrossRef]
- Bergier, H.; Duron, L.; Sordet, C.; Kawka, L.; Schlencker, A.; Chasset, F.; Arnaud, L. Digital Health, Big Data and Smart Technologies for the Care of Patients with Systemic Autoimmune Diseases: Where Do We Stand? Autoimmun. Rev. 2021, 20, 102864. [Google Scholar] [CrossRef]
- Bonnechère, B.; Omelina, L.; Kostkova, K.; Van Sint Jan, S.; Jansen, B. The End of Active Video Games and the Consequences for Rehabilitation. Physiother. Res. Int. 2018, 23, e1752. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study | D&B (/28) | Study Design | Intervention | Duration | Participants | Type of MS and Disability Level | ICF | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Motor Function | Activity Level | Cognition | Fatigue | Quality of Life | |||||||
| Cerasa et al., 2013 [24] | 23 | RCT | RehaCom | 6 weeks of training (2 × 60 min/week) | 17 MS patients 33 (4) years old 85% female | RRMS: 17 EDSS: 3 (0; 4.0) | X | X | |||
| Amato et al., 2014 [25] | 21 | RCT | Attention Processing Training Program (APT) | 12 weeks of training (2 × 60 min/week) | 88 MS patients 41 (11) years old 78% female | Type not available EDSS: 2.7 (1.5) | X | ||||
| Charvet et al., 2015 [26] | 24 | RCT | Luminosity | 12 weeks of training (5 × 30 min/week) | 20 MS patients 40 (8) years old 70% female | RRMS: 20 EDSS: 2 (0; 3.5) | X | ||||
| Hancock et al., 2015 [27] | 22 | RCT | Posit Science inSight (now BrainHQ) | 6 weeks of training (6 × 30 min/week) | 40 MS patients 50 (6) years old | Type and EDSS not available | X | ||||
| Hubacher et al., 2015 [28] | 24 | RCT | BrainStim | 4 weeks of training (4 × 45 min/week) | 10 MS patients 46 (7) years old 50% female | RRMS: 10 EDSS: 2 (1.0; 3.5) | X | ||||
| Fischer et al., 2015 [29] | 23 | RCT | Deprexis | 9 weeks of training | 90 MS patients 45 (12) years old 78% female | RRMS: 40, SPMS: 21, PPMS: 14, unclear: 18 | X | ||||
| Campbell et al., 2016 [30] | 22 | RCT | RehaCom | 6 weeks of training (3 × 45 min/week) | 35 MS patients 47 (8) years old 71% female | RRMS: 27, SPMS: 11 EDSS: 5.0 (3.5; 6.0) | X | ||||
| Pedullà et al., 2016 [31] | 24 | RCT | COGNI-TRAcK | 8 weeks of training (5 × 30 min/week) | 28 MS patients 47 (6) years old 71% female | RRMS: 17, SPMS: 11 EDSS: 3.8 (1.9) | X | ||||
| Charvet et al., 2017 [32] | 23 | RCT | BrainHQ | 12 weeks of training (5 × 60 min/week) | 135 MS patients 51 (13) years old 77% female | RRMS: 89, SPMS: 35, PPMS: 7, EDSS: 3.5 (2.5; 4.5) | X | ||||
| Messinis et al., 2017 [33] | 23 | RCT | RehaCom | 10 weeks of training (2 × 60 min/week) | 58 MS patients 46 (10) years old 69% female | RRMS: 58 EDSS: 3.2 (1.0; 5.5) | X | X | |||
| Conroy et al., 2018 [34] | 23 | RCT | MS HAT system | 6 months of intervention Self-paced rehabilitation | 54 MS patients 50 (12) years old 77% female | RRMS: 14, SPMS: 35, PPMS: 2 PDSS: 4.1 (1.5) | X | X | |||
| Stuifbergen et al., 2018 [35] | 22 | RCT | MAPSS-MS | 8 weeks of training 2 h/week group session + 3 × 45 min/week home-based training program | 183 MS patients 50 (8) years old 87% female | RRMS: 124 EDSS 5.2 (1.6) | X | X | |||
| Fjeldstad-Pardo et al., 2018 [36] | 21 | RCT | CG: exercise sheet tIG: telerehabilitation aIG: in-person rehabilitation + exercise sheet | 8 weeks -CG: 5 × week -tIG: 2 × week -aIG: 2 × week | 30 MS patients 55 (12) years old 68% female | RRMS: 18, SPMS: 8, PPMS: 4 EDSS: 4.3 (1.1) | X | X | X | X | X |
| Pöttgen et al., 2018 [37] | 23 | RCT | ELEVIDA | 12 weeks of intervention Self-paced rehabilitation | 275 MS patients 41 (11) years old 81% female | RRMS: 200, SPMS: 40, PPMS: 11, unclear: 24 | X | X | |||
| Cavalera et al., 2019 [38] | 24 | RCT | MBSR program (mindfulness)-MBI (intervention group) or online psychoeducation (active control group) | 8 weeks of training 1 weekly session | 121 MS patients 42 (8) years old 34% female | RRMS: 113; SPMS: 8 EDSS: median 3 | X | ||||
| Chiaravalloti et al., 2018 [39] | 23 | RCT | Processing speed apps (similar to BrainHQ) | 5 weeks of training 2/week | 21 MS patients 48 (8) years old 75% female | RRMS: 21 | X | ||||
| Plow et al., 2019 [40] | 22 | RCT | Contact-control social support intervention Fasting-mimicking diet physical activity plus fatigue self-management intervention PA-only physical activity only intervention | 12 week intervention 12 week follow-up Mix between group phone calls and individualized phone calls | 208 MS patients 52 (8) years old 85% female | RRMS: 176, SPMS: 11, PPMS: 6, PRMS: 1, unknown: 14 | X | X | |||
| Fuchs et al., 2019 [41] | 20 | Experimental study | BrainHQ | / | 51 MS patients 56 years old | RRMS: 35, SPMS: 12, PPMS: 4 EDSS: 4 [2.0; 6.0] | X | ||||
| Vilou et al., 2020 [42] | 22 | Explorative study | BrainHQ | 6 weeks of training (2 × 20 min/week) -weekly contact + 2 weeks scheduled visit (semi-assisted) | 47 MS patients 35 (16) years old 85% female | RRMS: 47 EDSS: 3.2 (2.0) | X | ||||
| Jeong et al., 2020 [43] | 23 | Retrospective analysis | MS-HAT | 6 months of follow-up 2.5 h/week | 17 MS patients 60 (11) years old | Type and EDSS not available | X | X | X | ||
| Kratz et al., 2020 [44] | 24 | RCT (pilot) | Web-based and telephone delivered exercises therapy | -Home: 30 min endurance 2× week; 3× week strength training lower extremity + 2 functional exercises per week -in-person: 30 endurance-tr + 30 resistance + home exercise for 8 weeks | 20 MS patients 48 (8) years old 90% of female | RRMS: 16, SPMS: 1, PPMS: 1 | X | X | |||
| Flachenecker et al., 2020 [45] | 23 | RCT | Behavior-oriented exercise and physical activity promotion program via web and telephone-based program | 12 weeks on intervention -Strength training (1–2 times per week) -Endurance training (10–60 min/1–2 times per week) | 64 MS patients 47 (9) years old 62% of female | RRMS: 39, SPMS: 25 EDSS: 4.3 (3.5; 5.0) | X | X | X | ||
| Manns et al., 2020 [46] | 22 | Pre–post intervention (single group) | SitLess+ MoveMore FitBit on (tracking instrument-self monitoring tool) ActivPAL3 (tracking for activity level during 7 days after each time point) | 15 weeks of training -7 weeks with SitLess -7 weeks with MoveMore | 41 MS patients (39 post intervention and 36 complete follow-up) 50 (10) years old 90% of female | RRMS: 26, SPMS: 11, PPMS: 4 EDSS: 5.5 (3.7) | X | X | |||
| Donkers et al., 2020 [47] | 24 | RCT (pilot) | Web-based exercise webbasedphysio.com | 26 weeks of training Adaptation of the exercises every two weeks | 48 MS patients 54 (12) years old 65% of female | Type and EDSS not available | X | X | |||
| Messinis et al., 2020 [48] | 24 | RCT | RehaCom | 8 weeks of training (3 × 45 min/week) | 36 MS patients 46 (4) years old 66% of female | SPMS: 36 EDSS: 5.5 (4.5; 7.0) | X | X | X | ||
| Minen et al., 2020 [49] | 23 | RCT | RELAXaHEAD | 90 days Self-paced training | 62 MS patients 40 (10) years old 89% female | Type and EDSS not available | X | ||||
| Van Geel et al., 2020 [50] | 25 | Cohort study | Walk-With-Me app | 10 weeks of training | 12 participants 43 (38.5; 50) years old 100% female | RRMS: 11, SPMS: 1 EDSS not available | X | X | X | X | |
| Bove et al., 2020 [51] | 26 | RCT | AKL-T03 (web-based) | 6 weeks of training (5 × 25 min/weeks) | 44 MS patients 51 (13) years old 80% female | RRMS: 33, SPMS: 7, PPMS: 2, CIS: 1, undetermined: 1 EDSS: 3.5 (2.5; 4.5) | X | X | |||
| Tarakci et al., 2021 [52] | 24 | RCT | Web-based and telphone delivered exercises therapy | 12 weeks program (3 × 60 min/week) | 30 MS patients 41 (11) years old 77% of female | RRMS: 30 EDSS: 3.4 (1.5) | X | X | X | ||
| Williams et al., 2021 [53] | 23 | RCT | Phone instruction and illustrated training booklet and activity diary | 8 weeks of training (2 × 60 min/week) | 50 MS patients 51 (10) years old 76% females | RRMS: 31, SPMS: 6, PPMS: 7, undetermined: 6 EDSS not available | X | ||||
| Study | D&B (/28) | Study Design | Intervention | Duration | Participants | Type of MS and Disability Level | ICF | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Motor Function | Activity Level | Cognition | Fatigue | Quality of Life | |||||||
| Miller et al., 2011 [54] | 24 | RCT | MCCO-enhanced (Web-Based) | 12 months: self-monitoring functioning at any moment, comparing MCCO-original with MCCO-enhanced | 206 MS patients | Not available | X | ||||
| Greiner et al., 2015 [55] | 18 | Pilot study | MSdialog (Web-Based and App) | 6-week study, following stages: 5-min online survey, training teleconference, weekly health reports, 5-min usability survey at weeks 3 and 6, follow-up call interview with selected patients | 76 MS patients 68% female | Not available | X | X | |||
| D’Hooghe et al., 2018 [56] | 21 | Cohort study | MS TeleCoach (Web-Based) | 2-week run-in period: assess baseline activity level per patient 12-week period: target number of activity counts gradually increased through telecoaching | 75 MS patients 67% female | RRMS: 75 EDSS: 2 | X | ||||
| Midaglia et al., 2019 [57] | 20 | Observational study | Floodlight (App) | Active monitoring for 24 weeks: Daily Mood Question: daily, MSIS-29: fortnightly, SDMT: weekly, pinching test: daily, Draw a Shape Test: daily, 5UTT: daily, 2MWT: daily Passive monitoring: gait behavior: continuous, mobility pattern: continuous | 101 participants (76 MS patients) 40 years old 70% female | RRMS: 69, SPMS: 4, PPMS: 3 EDSS: 2.4 (1.4) | X | X | |||
| Newland et al., 2019 [58] | 18 | Pilot study | FatigueApp.com (App) | FatigueApp.com: collect data for 5 weeks on Patient-Reported Outcomes Measurement Information System (PROMIS) | 32 MS patients 49 (11) years old 81% female | RRMS: 30, SPMS: 2 EDSS: 3 (2; 4.8) | X | ||||
| Pratap et al., 2020 [59] | 21 | Observational pilot study | ElevateMS (App) | 12 weeks Completed baseline assessments, including self-reported physical ability and longitudinal assessments of quality of life and daily health Completed functional tests as an independent assessment of MS-related motor activity | 629 participants (490 MS patients) 47 (11) years old 50% female | RRMS: 423, SPMS: 30, PPMS: 42, undetermined: 2 | X | X | |||
| Functioning (ICF) | mHealth | |
|---|---|---|
| Rehabilitation | Self-Assessment | |
| Cognition | BrainHQ [27,32,39,41,42] Lumosity [26] RehaCom [24,30,33] BrainStim [28] COGNI-TRAcK [31] MAPPS-MS * [35] APT [25] MS-HAT [43] Walk-With-Me [50] AKL-T03 [51] | MSdialog [55] Floodlight [57] |
| Fatigue | RehaCom [24,33] ELEVEDIA [37] MAPPS-MS [35] SitLess and MoveMore [46] Walk-With-Me [50] AKL-T03 [51] | MSdialog [55] MS TeleCoach [56] FatigueApp.com [58] |
| Quality of Life | ELEVEDIA [37] MBSR [38] MS-HAT [43] webbasedphysio.com [47] RehaCom [48] RELAXaHEAD [49] Walk-With-Me [50] | MCCO-enhanced [54] ElevateMS [59] |
| Activity Level | MS-HAT system [34] SitLess and MoveMore [46] Walk-With-Me [50] | Floodlight [57] ElevateMS [59] |
| Motor Function | MS-HAT system [34,43] webbasedphysio.com [47] | / |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bonnechère, B.; Rintala, A.; Spooren, A.; Lamers, I.; Feys, P. Is mHealth a Useful Tool for Self-Assessment and Rehabilitation of People with Multiple Sclerosis? A Systematic Review. Brain Sci. 2021, 11, 1187. https://doi.org/10.3390/brainsci11091187
Bonnechère B, Rintala A, Spooren A, Lamers I, Feys P. Is mHealth a Useful Tool for Self-Assessment and Rehabilitation of People with Multiple Sclerosis? A Systematic Review. Brain Sciences. 2021; 11(9):1187. https://doi.org/10.3390/brainsci11091187
Chicago/Turabian StyleBonnechère, Bruno, Aki Rintala, Annemie Spooren, Ilse Lamers, and Peter Feys. 2021. "Is mHealth a Useful Tool for Self-Assessment and Rehabilitation of People with Multiple Sclerosis? A Systematic Review" Brain Sciences 11, no. 9: 1187. https://doi.org/10.3390/brainsci11091187