
Intensive Care Unit-Acquired Weakness and Positioning-Related Peripheral Nerve Injuries in COVID-19: A Case Series of Three Patients and the Latest Literature Review

 , ,
, ,  , , and
, , and
Abstract
:1. Introduction
2. Case Presentation
2.1. Case 1
2.2. Cases 2 and 3
3. Discussion
3.1. COVID-19-Related ICUAW
3.1.1. Epidemiology of COVID-19-Related ICUAW
3.1.2. Utility of Electrophysiological Studies in Diagnosing ICUAW
3.1.3. Functional Outcome of COVID-19-Related ICUAW
3.1.4. Utility of Muscle MRI in COVID-19-Related ICUAW
3.2. Peripheral Nerve Injuries and COVID-19-Related ICUAW
3.2.1. Epidemiology of Peripheral Nerve Injuries in COVID 19 Cases
3.2.2. ICU Care and Peripheral Nerve Injuries in COVID-19
3.2.3. Diagnostic Challenges of Peripheral Nerve Injuries and Utility of NUS
3.2.4. Functional Outcome of Peripheral Nerve Injuries and Appropriate Interventions
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Stevens, R.D.; Marshall, S.A.; Cornblath, D.R.; Hoke, A.; Needham, D.M.; De Jonghe, B.; Ali, N.A.; Sharshar, T. A framework for diagnosing and classifying intensive care unit-acquired weakness. Crit. Care Med. 2009, 37, 299–308. [Google Scholar] [CrossRef]
- Latronico, N.; Bolton, C.F. Critical illness polyneuropathy and myopathy: A major cause of muscle weakness and paralysis. Lancet Neurol. 2011, 10, 931–941. [Google Scholar] [CrossRef]
- Zhou, C.; Wu, L.; Ni, F.; Ji, W.; Wu, J.; Zhang, H. Critical illness polyneuropathy and myopathy: A systematic review. Neural Regen. Res. 2014, 9, 101–110. [Google Scholar] [CrossRef]
- Sidiras, G.; Patsaki, I.; Karatzanos, E.; Dakoutrou, M.; Kouvarakos, A.; Mitsiou, G.; Routsi, C.; Stranjalis, G.; Nanas, S.; Gerovasili, V. Long term follow-up of quality of life and functional ability in patients with ICU acquired Weakness—A post hoc analysis. J. Crit. Care 2019, 53, 223–230. [Google Scholar] [CrossRef]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. Baseline Characteristics and Outcomes of 1591 Patients Infected with SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy. J. Am. Med. Assoc. 2020, 323, 1574–1581. [Google Scholar] [CrossRef] [Green Version]
- Stam, H.J.; Stucki, G.; Bickenbach, J. Covid-19 and post intensive care syndrome: A call for action. J. Rehabil. Med. 2020, 52, 19–22. [Google Scholar] [CrossRef]
- Cabañes-martínez, L.; Villadóniga, M.; González-rodríguez, L.; Araque, L.; Díaz-cid, A.; Ruz-caracuel, I.; Pian, H.; Sánchez-alonso, S.; Fanjul, S.; Regidor, I. Neuromuscular involvement in COVID-19 critically ill patients. Clin. Neurophysiol. 2020, 131, 2809–2816. [Google Scholar] [CrossRef] [PubMed]
- Van Aerde, N.; Van den Berghe, G.; Wilmer, A.; Gosselink, R.; Hermans, G.; Meersseman, P.; Gunst, J.; Aerts, V.; Balthazar, T.; Barbé, A.; et al. Intensive care unit acquired muscle weakness in COVID-19 patients. Intensive Care Med. 2020, 26, 2083–2085. [Google Scholar] [CrossRef]
- Frithiof, R.; Rostami, E.; Kumlien, E.; Virhammar, J.; Fällmar, D.; Hultström, M.; Lipcsey, M.; Ashton, N.; Blennow, K.; Zetterberg, H.; et al. Critical illness polyneuropathy, myopathy and neuronal biomarkers in COVID-19 patients: A prospective study. Clin. Neurophysiol. 2021, 132, 1733–1740. [Google Scholar] [CrossRef]
- Alhazzani, W.; Møller, M.H.; Arabi, Y.M.; Loeb, M.; Gong, M.N.; Fan, E.; Oczkowski, S.; Levy, M.M.; Derde, L.; Dzierba, A.; et al. Surviving Sepsis Campaign: Guidelines on the Management of Critically Ill Adults with Coronavirus Disease 2019 (COVID-19); Springer: Berlin/Heidelberg, Germany, 2020; Volume 46. [Google Scholar]
- McClafferty, B.; Umer, I.; Fye, G.; Kepko, D.; Kalayanamitra, R.; Shahid, Z.; Ramgobin, D.; Cai, A.; Groff, A.; Bhandari, A.; et al. Approach to critical illness myopathy and polyneuropathy in the older SARS-CoV-2 patients. J. Clin. Neurosci. 2020, 79, 241–245. [Google Scholar] [CrossRef] [PubMed]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef]
- Bagnato, S.; Boccagni, C.; Marino, G.; Prestandrea, C.; Agostino, T.D.; Rubino, F. Critical illness myopathy after COVID-19. Int. J. Infect. Dis. 2020, 99, 276–278. [Google Scholar] [CrossRef]
- Tankisi, H.; Tankisi, A.; Harbo, T.; Markvardsen, L.K.; Andersen, H.; Pedersen, T.H. Critical illness myopathy as a consequence of Covid-19 infection. Clin. Neurophysiol. 2020, 131, 1931–1932. [Google Scholar] [CrossRef]
- Fernandez, C.E.; Franz, C.K.; Ko, J.H.; Walter, J.M.; Koralnik, I.J.; Ahlawat, S.; Deshmukh, S. Imaging Review of Peripheral Nerve Injuries in Patients with COVID-19. Radiology 2021, 298, E117–E130. [Google Scholar] [CrossRef] [PubMed]
- Malik, G.R.; Wolfe, A.R.; Soriano, R.; Rydberg, L.; Wolfe, L.F.; Deshmukh, S.; Ko, J.H.; Nussbaum, R.P.; Dreyer, S.D.; Jayabalan, P.; et al. Injury-prone: Peripheral nerve injuries associated with prone positioning for COVID-19-related acute respiratory distress syndrome. Br. J. Anaesth. 2020, 125, e478–e480. [Google Scholar] [CrossRef]
- Nasuelli, N.A.; Pettinaroli, R.; Godi, L.; Savoini, C.; De Marchi, F.; Mazzini, L.; Crimaldi, F.; Pagni, A.; Pompa, C.P.; Colombo, D. Critical illness neuro-myopathy (CINM) and focal amyotrophy in intensive care unit (ICU) patients with SARS-CoV-2: A case series. Neurol. Sci. 2020, 42, 1119–1121. [Google Scholar] [CrossRef]
- Rubinos, C.; Ruland, S. Neurologic Complications in the Intensive Care Unit. Curr. Neurol. Neurosci. Rep. 2016, 16. [Google Scholar] [CrossRef] [PubMed]
- Winfree, C.J.; Kline, D.G. Intraoperative positioning nerve injuries. Surg. Neurol. 2005, 63, 5–18. [Google Scholar] [CrossRef]
- Le, M.Q.; Rosales, R.; Shapiro, L.T.; Huang, L.Y. The down Side of Prone Positioning: The Case of a Coronavirus 2019 Survivor. Am. J. Phys. Med. Rehabil. 2020, 99, 870–872. [Google Scholar] [CrossRef]
- Agergaard, J.; Leth, S.; Pedersen, T.H.; Harbo, T.; Blicher, J.U.; Karlsson, P.; Østergaard, L.; Andersen, H.; Tankisi, H. Myopathic changes in patients with long-term fatigue after COVID-19. Clin. Neurophysiol. 2021, 132, 1974–1981. [Google Scholar] [CrossRef]
- Tankisi, H. Critical illness myopathy and polyneuropathy in Covid-19: Is it a distinct entity? Clin. Neurophysiol. 2021, 132, 1716–1717. [Google Scholar] [CrossRef] [PubMed]
- Berlit, P.; Bösel, J.; Gahn, G.; Isenmann, S.; Meuth, S.G.; Nolte, C.H.; Pawlitzki, M.; Rosenow, F.; Schoser, B.; Thomalla, G.; et al. “Neurological manifestations of COVID-19”—Guideline of the German society of neurology. Neurol. Res. Pract. 2020, 2. [Google Scholar] [CrossRef] [PubMed]
- Pinzon, R.T.; Wijaya, V.O.; Buana, R.B.; Al Jody, A.; Nunsio, P.N. Neurologic characteristics in coronavirus disease 2019 (COVID-19): A systematic review and meta-analysis. Front. Neurol. 2020, 11, 565. [Google Scholar] [CrossRef] [PubMed]
- Tatu, L.; Nono, S.; Grácio, S.; Koçer, S. Guillain–Barré syndrome in the COVID-19 era: Another occasional cluster? J. Neurol. 2020, 268, 1198–1200. [Google Scholar] [CrossRef]
- Harapan, B.N.; Yoo, H.J. Neurological symptoms, manifestations, and complications associated with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease 19 (COVID-19). J. Neurol. 2021, 268, 3059–3071. [Google Scholar] [CrossRef]
- Bolton, C.F. Neuromuscular manifestations of critical illness. Muscle Nerve 2005, 32, 140–163. [Google Scholar] [CrossRef]
- Bax, F.; Lettieri, C.; Marini, A.; Pellitteri, G.; Surcinelli, A.; Valente, M.; Budai, R.; Patruno, V.; Gigli, G.L. Clinical and neurophysiological characterization of muscular weakness in severe COVID-19. Neurol. Sci. 2021, 42, 2173–2178. [Google Scholar] [CrossRef]
- Guarneri, B.; Bertolini, G.; Latronico, N. Long-term outcome in patients with critical illness myopathy or neuropathy: The Italian multicentre CRIMYNE study. J. Neurol. Neurosurg. Psychiatry 2008, 79, 838–840. [Google Scholar] [CrossRef]
- Vanhorebeek, I.; Latronico, N.; Van den Berghe, G. ICU-acquired weakness. Intensive Care Med. 2020, 46, 637–653. [Google Scholar] [CrossRef] [PubMed]
- Goodman, B.P.; Harper, C.M.; Boon, A.J. Prolonged compound muscle action potential duration in critical illness myopathy. Muscle Nerve 2009, 40, 1040–1042. [Google Scholar] [CrossRef]
- Curci, C.; Negrini, F.; Ferrillo, M.; Bergonzi, R.; Bonacci, E.; Camozzi, D.M.; Ceravolo, C.; De Franceschi, S.; Guarnieri, R.; Moro, P.; et al. Functional outcome after inpatient rehabilitation in post-intensive care unit COVID-19 patients: Findings and clinical implications from a real-practice retrospective study. Eur. J. Phys. Rehabil. Med. 2021, 57, 443–450. [Google Scholar] [CrossRef]
- Fan, E.; Cheek, F.; Chlan, L.; Gosselink, R.; Hart, N.; Herridge, M.S.; Hopkins, R.O.; Hough, C.L.; Kress, J.P.; Latronico, N.; et al. An official American Thoracic Society Clinical Practice guideline: The diagnosis of intensive care unit-acquired weakness in adults. Am. J. Respir. Crit. Care Med. 2014, 190, 1437–1446. [Google Scholar] [CrossRef]
- Dinh, A.; Carlier, R.; Descatha, A. Critical illness myopathy and whole body mri. Intensive Care Med. 2016, 42, 587. [Google Scholar] [CrossRef] [Green Version]
- Ten Dam, L.; van der Kooi, A.J.; Verhamme, C.; Wattjes, M.P.; de Visser, M. Muscle imaging in inherited and acquired muscle diseases. Eur. J. Neurol. 2016, 23, 688–703. [Google Scholar] [CrossRef]
- Kayim Yildiz, O.; Yildiz, B.; Avci, O.; Hasbek, M.; Kanat, S. Clinical, Neurophysiological and Neuroimaging Findings of Critical Illness Myopathy after COVID-19. Cureus 2021, 13. [Google Scholar] [CrossRef]
- Coraci, D.; Fusco, A.; Frizziero, A.; Giovannini, S.; Biscotti, L.; Padua, L. Global approaches for global challenges: The possible support of rehabilitation in the management of COVID-19. J. Med. Virol. 2020, 92, 1739–1740. [Google Scholar] [CrossRef] [Green Version]
- Needham, E.; Newcombe, V.; Michell, A.; Thornton, R.; Grainger, A.; Anwar, F.; Warburton, E.; Menon, D.; Trivedi, M.; Sawcer, S. Mononeuritis multiplex: An unexpectedly frequent feature of severe COVID-19. J. Neurol. 2020, 268, 2685–2689. [Google Scholar] [CrossRef] [PubMed]
- Bickler, P.E.; Schapera, A.; Bainton, C.R. Acute Radial Nerve Injury from Use of an Automatic Blood Pressure Monitor. Obstet. Anesth. Dig. 1991, 10, 235. [Google Scholar] [CrossRef]
- Jang, A.Y.; Oh, Y.J.; Lee, S.I.; Lim, O.K.; Suh, S.Y. Femoral neuropathy following venoarterial-extracorporeal membrane oxygenation therapy: A case report. BMC Cardiovasc. Disord. 2020, 20, 393. [Google Scholar] [CrossRef] [PubMed]
- Rieg, S.; von Cube, M.; Kalbhenn, J.; Utzolino, S.; Pernice, K.; Bechet, L.; Baur, J.; Lang, C.N.; Wagner, D.; Wolkewitz, M.; et al. COVID-19 in-hospital mortality and mode of death in a dynamic and non-restricted tertiary care model in Germany. PLoS ONE 2020, 15, e0242127. [Google Scholar] [CrossRef]
- Go, J.Y.; Min, Y.S.; Jung, T. Du Delayed onset of acute limb compartment syndrome with neuropathy after venoarterial extracorporeal membrane oxygenation therapy. Ann. Rehabil. Med. 2014, 38, 575–580. [Google Scholar] [CrossRef] [PubMed]
- Aydin, Ş.; Pazarci, N.; Akan, O.; Büyükkale, S.; Bakan, N.D.; Sayar, A. A case report of a drop foot developed after common femoral artery cannulation for venoarterial extracorporeal membrane Oxygenation. Arch. Neuropsychiatry 2019, 56, 75–78. [Google Scholar] [CrossRef]
- Hobson-Webb, L.D.; Padua, L. Ultrasound of Focal Neuropathies. J. Clin. Neurophysiol. 2016, 33, 94–102. [Google Scholar] [CrossRef]
- Padua, L.; Coraci, D.; Erra, C.; Pazzaglia, C.; Paolasso, I.; Loreti, C.; Caliandro, P.; Hobson-Webb, L.D. Carpal tunnel syndrome: Clinical features, diagnosis, and management. Lancet Neurol. 2016, 15, 1273–1284. [Google Scholar] [CrossRef]
- Kwee, M.M.; Ho, Y.H.; Rozen, W.M. The prone position during surgery and its complications: A systematic review and evidence-based guidelines. Int. Surg. 2015, 100, 292–303. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Case 1 | Case 2 | Case 3 | |
|---|---|---|---|
| Age | 52 | 77 | 52 |
| Sex | Male | Male | Male |
| ICU stay (days) | 82 | 70 | 44 |
| Mechanical ventilation (days) | 60 | 50 | 39 |
| Comorbidities | ARDS, septic shock, MOF | ARDS, septic shock, MOF | ARDS |
| NBA | + | + | + |
| Corticosteroids | + | + | + |
| Additional treatment | ECMO | CHDF | None |
| Type of ICUAW | CINM | CINM | CINM |
| Peripheral nerve injury | bilateral fibular nerve | left radial nerve | bilateral ulnar nerve |
| (site) | (fibular head) | (spiral groove) | (cubital tunnel) |
| Focal neurological deficits | bilateral foot drop | left wrist drop | bilateral FDI atrophy |
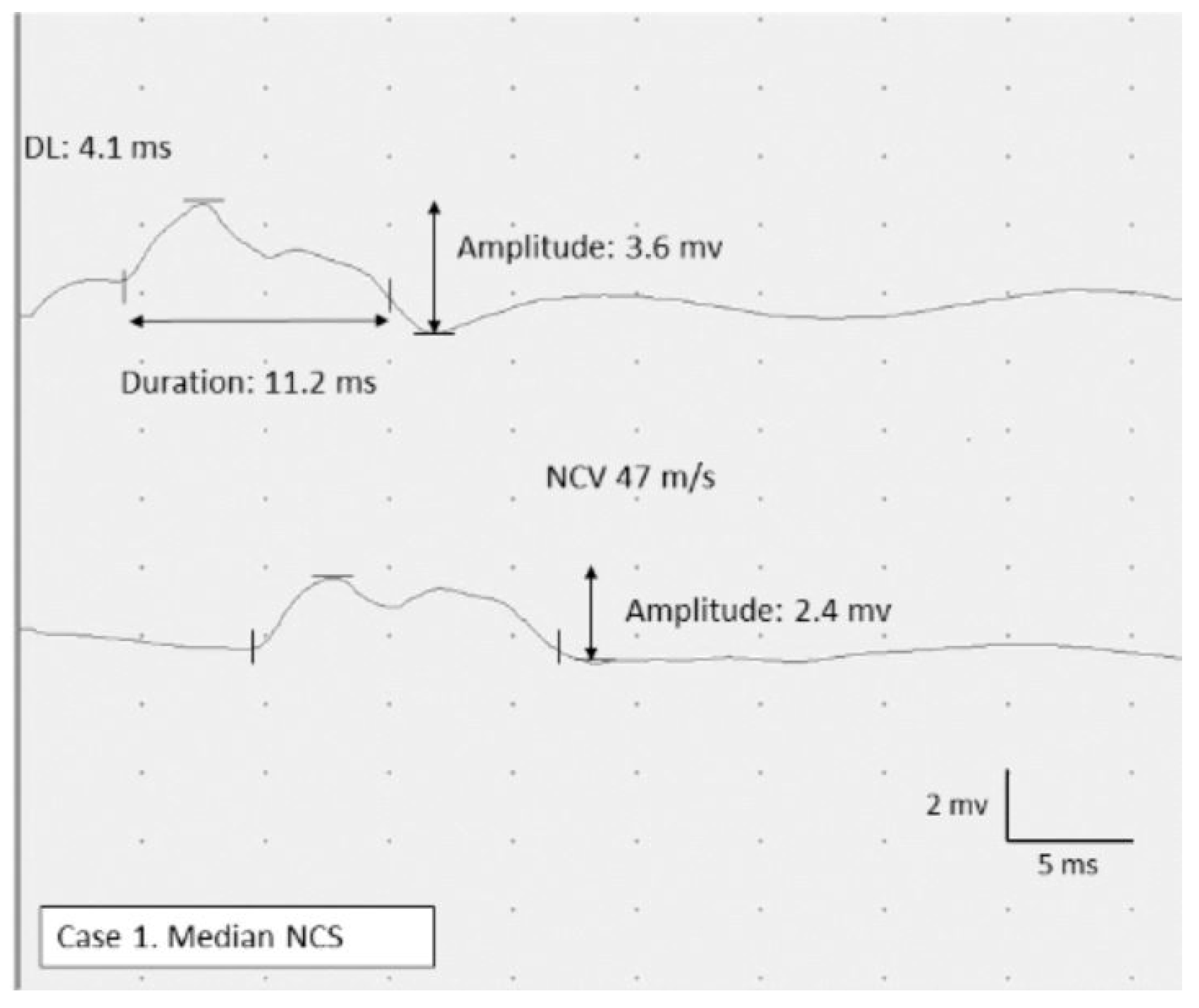
| Nerve conduction study | sensorimotor poly neuropathy | sensorimotor poly neuropathy | sensorimotor poly neuropathy |
| Prolonged CMAP duration | + | + | + |
| Electromyography | neurogenic changes with Fib/PSW | myopathic changes with Fib/PSW | myopathic changes with Fib/PSW |
| Nerve ultrasound | focal enlargement in the bilateral fibular nerve | focal enlargement in the left radial nerve | focal enlargement in the left ulnar nerve |
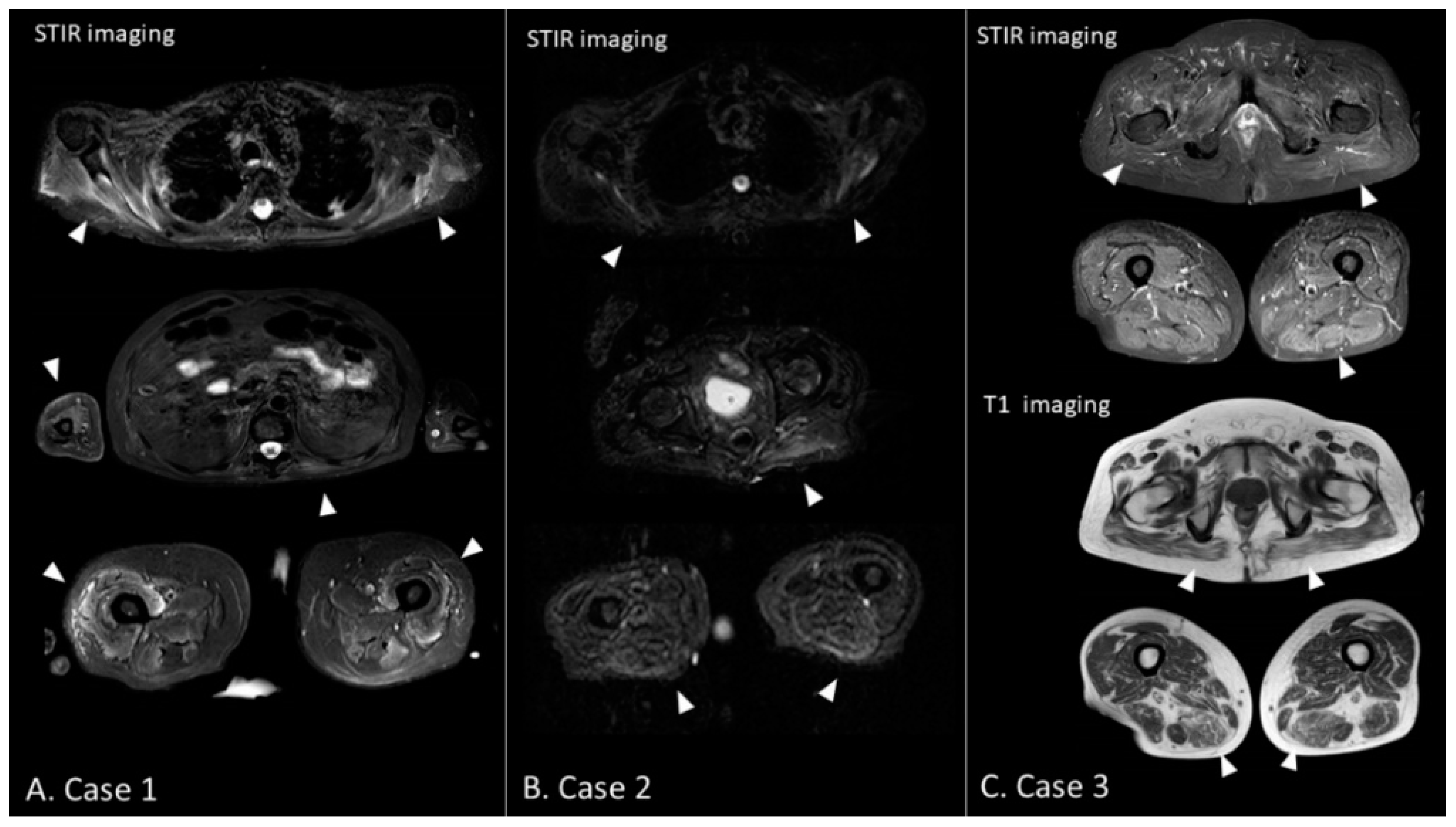
| Muscle MRI (STIR image) | diffuse hyperintense lesions | diffuse hyperintense lesions | diffuse hyperintense lesions |
| MRC sum-score | |||
| On admission | 34 | 27 | 38 |
| Three months later | 51 | 41 | 54 |
| Barthel index | |||
| On admission | 5 | 5 | 11 |
| Three months later | 95 | 90 | 95 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hokkoku, K.; Erra, C.; Cuccagna, C.; Coraci, D.; Gatto, D.M.; Glorioso, D.; Padua, L. Intensive Care Unit-Acquired Weakness and Positioning-Related Peripheral Nerve Injuries in COVID-19: A Case Series of Three Patients and the Latest Literature Review. Brain Sci. 2021, 11, 1177. https://doi.org/10.3390/brainsci11091177
Hokkoku K, Erra C, Cuccagna C, Coraci D, Gatto DM, Glorioso D, Padua L. Intensive Care Unit-Acquired Weakness and Positioning-Related Peripheral Nerve Injuries in COVID-19: A Case Series of Three Patients and the Latest Literature Review. Brain Sciences. 2021; 11(9):1177. https://doi.org/10.3390/brainsci11091177
Chicago/Turabian StyleHokkoku, Keiichi, Carmen Erra, Cristina Cuccagna, Daniele Coraci, Dario Mattia Gatto, Davide Glorioso, and Luca Padua. 2021. "Intensive Care Unit-Acquired Weakness and Positioning-Related Peripheral Nerve Injuries in COVID-19: A Case Series of Three Patients and the Latest Literature Review" Brain Sciences 11, no. 9: 1177. https://doi.org/10.3390/brainsci11091177