
Coping Strategies, Anxiety and Depression in OCD and Schizophrenia: Changes during COVID-19

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
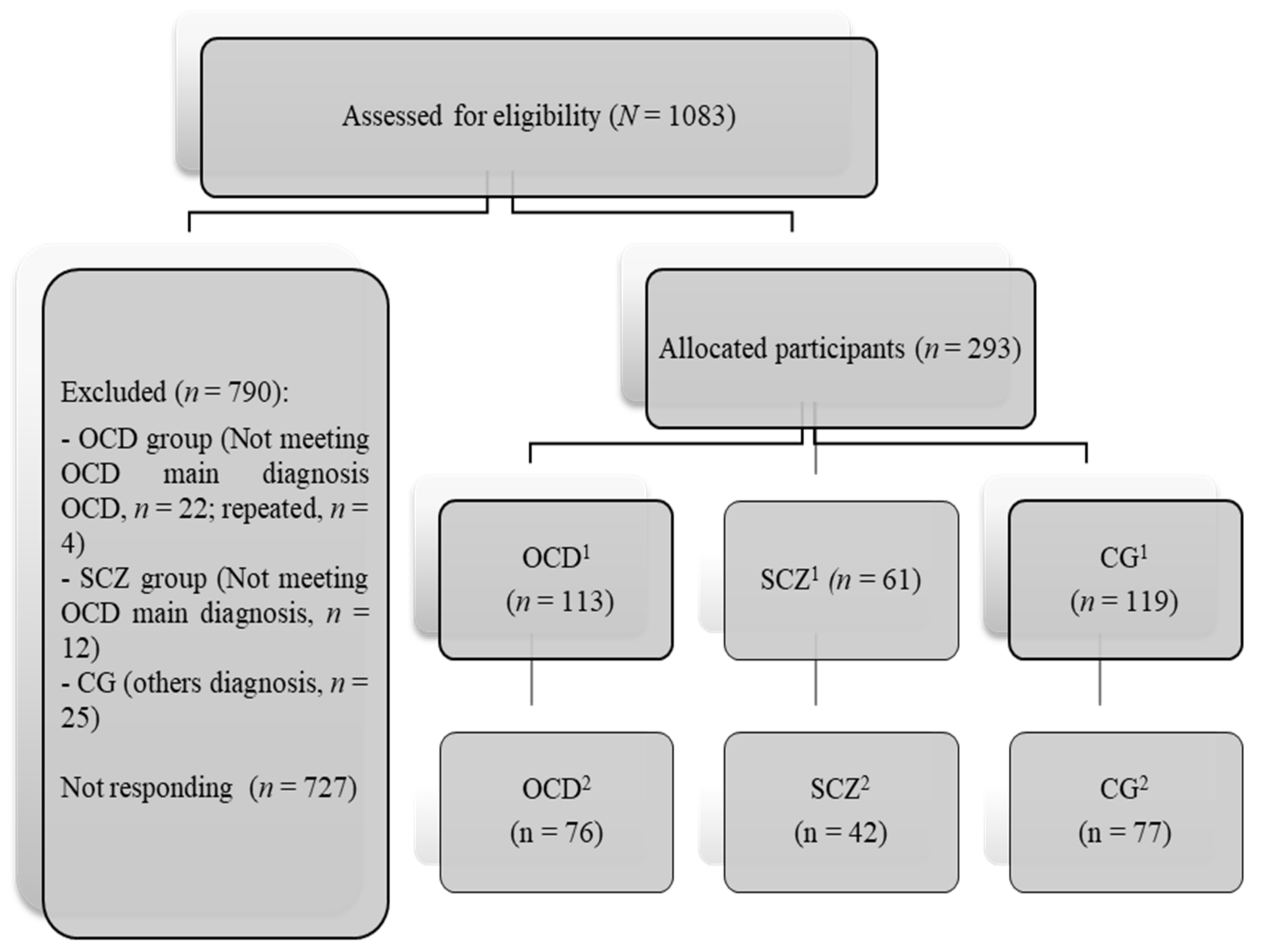
2.1. Participants
2.2. Procedure
2.3. Measures
2.4. Data Analysis
3. Results
3.1. Changes in Coping Strategies, Anxiety and Depression
3.2. Coping Strategies Controlling Level of Intolerance to Uncertainty and Experiential Avoidance during Second Time
3.3. Intragroup Comparison Based on Coping Strategies and Clinical and Sociodemographic
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Monroe, S.M.; Slavich, G.M.; Torres, L.D.; Gotlib, I.H. Severe life events predict specific patterns of change in cognitive biases in major depression. Psychol. Med. 2007, 37, 863–871. [Google Scholar] [CrossRef] [Green Version]
- Slavich, G.M. Life stress and health: A review of conceptual issues and recent findings. Teach. Psychol. 2016, 43, 346–355. [Google Scholar] [CrossRef] [Green Version]
- Duan, H.; Yan, L.; Ding, X.; Gan, Y.; Kohn, N.; Wu, J. Impact of the COVID-19 pandemic on mental health in the general Chinese population: Changes, predictors and psychosocial correlates. Psychiatry Res. 2020, 293, 113396. [Google Scholar] [CrossRef] [PubMed]
- Fiorillo, A.; Gorwood, P. The consequences of the COVID-19 pandemic on mental health and implications for clinical practice. Eur. Psychiatry 2020, 63, e32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fontenelle, L.F.; Miguel, E.C. The impact of coronavirus (COVID-19) in the diagnosis and treatment of obsessive-compulsive disorder. Depress. Anxiety 2020, 37, 510–511. [Google Scholar] [CrossRef]
- Pozza, A.; Mucci, F.; Marazziti, D. Risk for pathological contamination fears at coronavirus time: Proposal of early intervention and prevention strategies. Clin. Neuropsychiatry 2020, 17, 100–102. [Google Scholar] [CrossRef]
- Silva, R.M.; Shavitt, R.G.; Costa, D.L. Obsessive-compulsive disorder during the COVID-19 pandemic. Rev. Bras. Psiquiatr. 2021, 43, 108. [Google Scholar] [CrossRef]
- Maguire, P.A.; Reay, R.E.; Looi, J.C. A sense of dread: Affect and risk perception in people with schizophrenia during an influenza pandemic. Australas. Psychiatry 2019, 27, 450–455. [Google Scholar] [CrossRef]
- Fineberg, N.A.; Van Ameringen, M.; Drummond, L.; Hollander, E.; Stein, D.J.; Geller, D.; Pallanti, S.; Pellegrini, L.; Zohar, J.; Rodriguez, C.I.; et al. How to manage obsessive-compulsive disorder (OCD) under COVID-19: A clinician’s guide from the International College of Obsessive Compulsive Spectrum Disorders (ICOCS) and the Obsessive-Compulsive Research Network (OCRN) of the European College of Neuropsychopharmacology. Compr. Psychiat. 2020, 100, 152174. [Google Scholar] [CrossRef]
- Rivera, R.M.; Carballea, D. Coronavirus: A trigger for OCD and illness anxiety disorder? Psychol. Trauma Theory, Res. Pr. Policy 2020, 12, S66. [Google Scholar] [CrossRef] [PubMed]
- Bornheimer, L.A.; Li, J.; Im, V.; Taylor, M.; Himle, J.A. The Role of Social Isolation in the Relationships between Psychosis and Suicidal Ideation. Clin. Soc. Work. J. 2019, 48, 54–62. [Google Scholar] [CrossRef]
- Reddy, L.F.; Irwin, M.R.; Breen, E.C.; Reavis, E.A.; Green, M.F. Social exclusion in schizophrenia: Psychological and cognitive consequences. J. Psychiatr. Res. 2019, 114, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Carleton, R.N. Into the unknown: A review and synthesis of contemporary models involving uncertainty. J. Anxiety Disord. 2016, 39, 30–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rettie, H.; Daniels, J. Coping and tolerance of uncertainty: Predictors and mediators of mental health during the COVID-19 pandemic. Am. Psychol. 2021, 76, 427–437. [Google Scholar] [CrossRef]
- Wheaton, M.G.; Messner, G.R.; Marks, J.B. Intolerance of uncertainty as a factor linking obsessive-compulsive symptoms, health anxiety and concerns about the spread of the novel coronavirus (COVID-19) in the United States. J. Obs. Compuls. Relat. Disord. 2021, 28, 100605. [Google Scholar] [CrossRef] [PubMed]
- Larsen, E.M.; Donaldson, K.; Mohanty, A. Conspiratorial Thinking during COVID-19: The Roles of Paranoia, Delusion-Proneness, and Intolerance to Uncertainty. PsyArXiv. 2020. Available online: psyarxiv.com/mb65f/ (accessed on 9 July 2021).
- Seçer, I.; Ulaş, S. An Investigation of the Effect of COVID-19 on OCD in Youth in the Context of Emotional Reactivity, Experiential Avoidance, Depression and Anxiety. Int. J. Ment. Health Addict. 2020, 1–14. [Google Scholar] [CrossRef]
- Melin, K.; Skarphedinsson, G.; Thomsen, P.H.; Weidle, B.; Torp, N.C.; Valderhaug, R.; Højgaard, D.R.; Hybel, K.A.; Nissen, J.B.; Jensen, S.; et al. Treatment Gains Are Sustainable in Pediatric Obsessive-Compulsive Disorder: Three-Year Follow-Up From the NordLOTS. J. Am. Acad. Child Adolesc. Psychiatry 2020, 59, 244–253. [Google Scholar] [CrossRef]
- Lazarus, R.S.; Folkman, S. Estrés y Procesos Cognitivos; Martínez Roca: Madrid, Spain, 1986. [Google Scholar]
- Morán, C.; Landero, R.; González, T. COPE-28: Un análisis psicométrico de la versión en español del Brief COPE. Univ. Psychol. 2020, 9, 543–552. [Google Scholar] [CrossRef] [Green Version]
- Rosa-Alcázar, Á.; García-Hernández, M.D.; Parada-Navas, J.L.; Olivares-Olivares, P.J.; Martínez-Murillo, S.; Rosa-Alcázar, A.I. Coping strategies in obsessive-compulsive patients during Covid-19 lockdown. Int. J. Clin. Health Psychol. 2021, 21, 100223. [Google Scholar] [CrossRef]
- Mazza, M.G.; De Lorenzo, R.; Conte, C.; Poletti, S.; Vai, B.; Bollettini, I.; Melloni, E.M.T.; Furlan, R.; Ciceri, F.; Rovere-Querini, P.; et al. Anxiety and depression in COVID-19 survivors: Role of inflammatory and clinical predictors. Brain Behav. Immun. 2020, 89, 594–600. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gámez, W.; Chmielewski, M.; Kotov, R.; Ruggero, C.; Suzuki, N.; Watson, D. The Brief Experiential Avoidance Questionnaire: Development and initial validation. Psychol. Assess. 2014, 26, 35–45. [Google Scholar] [CrossRef] [PubMed]
- Freeston, M.H.; Rhéaume, J.; Letarte, H.; Dugas, M.; Ladouceur, R. Why do people worry? Pers. Individ. Differ. 1994, 17, 791–802. [Google Scholar] [CrossRef]
- Prasko, J.; Holubova, M.; Hruby, R.; Kamaradova, D.; Ociskova, M.; Latalova, K.; Grambal, A. Coping strategies and quality of life in schizophrenia: Cross-sectional study. Neuropsychiatr. Dis. Treat. 2015, 11, 3041–3048. [Google Scholar] [CrossRef] [Green Version]
- Kommescher, M.; Gross, S.; Pützfeld, V.; Klosterkötter, J.; Bechdolf, A. Coping and the stages of psychosis: An investigation into the coping styles in people at risk of psychosis, in people with first-episode and multiple-episode psychoses. Early Interv. Psychiatry 2015, 11, 147–155. [Google Scholar] [CrossRef]
- Freeston, M.; Tiplady, A.; Mawn, L.; Bottesi, G.; Thwaites, S. Towards a model of uncertainty distress in the context of Coronavirus (COVID-19). Cogn. Behav. Ther. 2020, 13, 1–32. [Google Scholar] [CrossRef]
- Bueno-Notivol, J.; Gracia-García, P.; Olaya, B.; Lasheras, I.; López-Antón, R.; Santabárbara, J. Prevalence of depression during the COVID-19 outbreak: A meta-analysis of community-based studies. Int. J. Clin. Health Psychol. 2021, 21, 100196. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | OCD (n = 113) | SCZ (n = 61) | CG (n = 119) | ANOVA/χ2 |
|---|---|---|---|---|
| Age (Mean ± SD) | 34.54 ± 10.31 | 43.98 ± 10.59 | 35.05 ± 13.58 | F (2;277,08) = 14,53; p < 0.001 |
| Sex n (%) | Χ2 (2) = 25,57; p < 0.001 | |||
| Men | 61 (54) | 21(34.4) | 67 (56.3) | |
| Women | 52 (46) | 40 (65.6) | 52 (43.7) | |
| Marital status n (%) | Χ2 (6) = 42,32; p <.001 | |||
| Single | 65 (57.5) | 45 (73.7) | 61 (51.2) | |
| Married | 39 (34.5) | 2 (3.3) | 49 (41.1) | |
| Divorced | 9 (8) | 12 (19.7) | 6 (5.2) | |
| Widower | 0 (0) | 2 (3.3) | 3 (2.5) | |
| Educational level n (%) | Χ2 (6) = 10.95; p = 0.012 | |||
| Elementary | 6 (5.7) | 32 (52.4) | 2 (2) | |
| Secundary education | 22 (19.5) | 13 (21.3) | 6 (5.2) | |
| High school | 29 (25.2) | 11 (18) | 51 (24.4) | |
| University student | 56 (49.6) | 5 (8.3) | 60 (72.3) | |
| Who did you spend quarantine with n (%) | Χ2 (2) = 10.95; p = 0.012 | |||
| Alone | 9 (7.9) | 13 (21.3) | 9 (7.6) | |
| Accompanied | 104 (92.1) | 48 (78.9) | 110 (92.4) | |
| COVID-19 patient | ns | |||
| Yes | 5 (4.8) | 4 (6.6) | 5 (4) | |
| No | 108 (95.2) | 57 (93.4) | 114 (96) |
| Time | OCD | SCZ | CG | F | p | η2 | |
|---|---|---|---|---|---|---|---|
| (napril = 113; nnovember = 85) | (napril = 61; nnovember = 42) | (nabril = 119; nnoviembre = 77) | |||||
| M ± SD | M ± SD | M ± SD | |||||
| Cognitive C. | F(time)= | 44.27 | <0.001 | 0.1 | |||
| T1 | 16.48 ± 5.76 | 19.68 ± 6.24 | 18.96 ± 5.01 | F(interaction)= | 19.62 | <0.001 | 0.1 |
| T2 | 16.02 ± 5.32 | 17.65 ± 5.54 | 18.98 ± 4.97 | F(group)= | 11.59 | <0.001 | 0.06 |
| Social C. | F(time)= | 10.99 | 0.001 | 0.03 | |||
| T1 | 8.95 ± 4.49 | 10.88 ± 3.66 | 8.00 ± 3.95 | F(interaction)= | 3.09 | 0.047 | 0.02 |
| T2 | 9.09 ± 4.41 | 11.29 ± 3.84 | 8.03 ± 3.92 | F(group)= | 9.58 | <0.001 | 0.05 |
| Avoidance C. | F(time)= | 2.28 | >0.05 | 0.01 | |||
| T1 | 8.68 ± 3.86 | 8.34 ± 3.18 | 6.68 ± 3.23 | F(interaction)= | 5.65 | 0.004 | 0.03 |
| T2 | 8.96 ± 3.77 | 8.45 ± 3.01 | 6.59 ± 3.09 | F(group)= | 19.07 | <0.001 | 0.1 |
| Spiritual C. | F(time)= | 35.57 | <0.001 | 0.08 | |||
| T1 | 1.93 ± 1.98 | 2.69 ± 2.36 | 1.28 ± 1.69 | F(interaction)= | 23.81 | <0.001 | 0.11 |
| T2 | 1.95 ± 1.97 | 3.12 ± 2.19 | 1.27 ± 1.66 | F(group)= | 14.65 | <0.001 | 0.07 |
| Anxiety | F(time)= | 24.41 | <0.001 | 0.06 | |||
| T1 | 11.69 ± 4.45 | 8.41 ± 4.81 | 7.44 ± 3.76 | F(interaction)= | 6.96 | 0.001 | 0.03 |
| T2 | 11.85 ± 4.22 | 9.06 ± 4.35 | 7.51 ± 3.69 | F(group)= | 48.13 | <0.001 | 0.19 |
| Depression | F(time)= | 102.98 | <0.001 | 0.2 | |||
| T1 | 8.09 ± 4.27 | 5.52 ± 4.08 | 5.00 ± 3.57 | F(interaction)= | 31.33 | <0.001 | 0.14 |
| T2 | 8.61 ± 3.94 | 7.67 ± 2.34 | 5.17 ± 3.52 | F(group)= | 33.03 | <0.001 | 0.14 |
| Variables | OCD (n = 76) | SCZ (n = 42) | CG (n = 77) | F |
|---|---|---|---|---|
| Experiential avoidance | F = 22.55; p < 0.001 | |||
| (Mean ± SD) | 56.47 ± 13.92 | 57.12 ± 12.95 | 48.14 ± 11.47 | |
| Uncertainty intolerance | F = 37.22; p < 0.001 | |||
| (Mean ± SD) | 82.60 ± 19.24 | 74.75 ± 23.70 | 62.28 ± 21.21 | |
| Uncertainty to prospective intolerance | F = 14.29; p < 0.001 | |||
| (Mean ± SD) | 31.61 ± 8.93 | 30.62 ± 10.14 | 26.23 ± 9.30 | |
| Uncertainty to inhibitory uncertainty | F = 54.06; p < 0.001 | |||
| (Mean ± SD) | 51.00 ± 11.57 | 44.12 ± 14.42 | 35.93 ± 13.31 |
| Variables | OCD (n = 113) M Adjusted | SCZ (n = 61) M Adjusted | CG (n = 119) M Adjusted | F | p |
|---|---|---|---|---|---|
| Cognitive coping | 16.48 | 18.72 | 18.70 | 6.03 | 0.003 |
| Social coping | 8.53 | 11.81 | 8.37 | 7.95 | <0.001 |
| Avoidance coping | 7.89 | 8.19 | 7.14 | 2.99 | 0.05 |
| Spiritual coping | 1.93 | 3.10 | 1.26 | 13,04 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rosa-Alcázar, Á.; Parada-Navas, J.L.; García-Hernández, M.D.; Martínez-Murillo, S.; Olivares-Olivares, P.J.; Rosa-Alcázar, A.I. Coping Strategies, Anxiety and Depression in OCD and Schizophrenia: Changes during COVID-19. Brain Sci. 2021, 11, 926. https://doi.org/10.3390/brainsci11070926
Rosa-Alcázar Á, Parada-Navas JL, García-Hernández MD, Martínez-Murillo S, Olivares-Olivares PJ, Rosa-Alcázar AI. Coping Strategies, Anxiety and Depression in OCD and Schizophrenia: Changes during COVID-19. Brain Sciences. 2021; 11(7):926. https://doi.org/10.3390/brainsci11070926
Chicago/Turabian StyleRosa-Alcázar, Ángel, José Luis Parada-Navas, María Dolores García-Hernández, Sergio Martínez-Murillo, Pablo J. Olivares-Olivares, and Ana I. Rosa-Alcázar. 2021. "Coping Strategies, Anxiety and Depression in OCD and Schizophrenia: Changes during COVID-19" Brain Sciences 11, no. 7: 926. https://doi.org/10.3390/brainsci11070926