
A Survey on Socially Assistive Robotics: Clinicians’ and Patients’ Perception of a Social Robot within Gait Rehabilitation Therapies

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Hypothesis Formulation
2.2. Experimental Protocol
Procedure
2.3. Data Analysis
3. Results
3.1. Questionnaire Reliability
3.2. Overall User’s Perception
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Construct | No. | Questions |
|---|---|---|
| PF | 1 | I am afraid of damaging the robot. |
| 2 | I think that using the robot during the Lokomat sessions will be comfortable. | |
| 3 | Using the robot will generate stress. | |
| 4 | I think that the robot express emotions during the sessions will be uncomfortable. | |
| 5 | I think that the robot will increase the concentration during the therapy. | |
| 6 | I think that the robot speech could be weird. | |
| 7 | I think that using the robot will make me feel more secure. | |
| 8 | I think that the robot will give me confidence. | |
| SP | 1 | I think that using the robot in the rehabilitation could be more interesting. |
| 2 | I think that the interaction with the robot would be pleasant. | |
| 3 | I think that it is appropriate that the robot will use the data of the rehabilitation. | |
| 4 | Using the robot will give me satisfaction. | |
| 5 | I think that the robot’s instruction will be highly relevant. | |
| EL | 1 | I think that the therapy could turn boring with the use of the robot. |
| 2 | I think that I will enjoy more the therapy with the robot. | |
| 3 | I think that following-up with the robot’s instructions will be fun. | |
| 4 | I think that the robot company will make the therapy more enjoyable. | |
| EE | 1 | Following the robot’s instructions would be difficult. |
| 2 | I think that using the robot would improve Lokomat therapy. | |
| 3 | I think that I will be able to use the robot without external help. | |
| 4 | I think that use the robot will be easy. | |
| 5 | I think I will learn quickly how to use the robot. | |
| PE | 1 | I think that the robot will be helpful during the rehabilitation process. |
| 2 | The robot would help to decrease the fatigue during the therapies. | |
| 3 | I think that use the robot will make the therapies faster. | |
| 4 | I think that the presence of the robot is motivating. | |
| 5 | I think that the presence of the robot will affect over the engagement in the therapy. | |
| 6 | I think that using the robot is convenient for the rehabilitation procedure. | |
| 7 | I think that the use of the robot would become repetitive during the sessions. | |
| 8 | I think that the use of the robot will motivate the patients to perform better rehabilitation. | |
| 9 | I think that the use of the robot will make the session longer. | |
| FC | 1 | I consider that I must have previous training before using the robot. |
| 2 | I consider that the robot can be challenging to control. | |
| 3 | I consider that the robot could be adapted to any scenario. | |
| 4 | I consider that the robot could be used to assist patients with other pathologies. | |
| 5 | I would like the robot to reduce the workload I have during the rehabilitation procedure. | |
| Open Questions | 1 | How you perceive the robot?. |
| 2 | What does the robot inspire you?. | |
| 3 | What kind of interactions or gestures should a robot have for closer interaction?. | |
| 4 | Which physical changes would you make to the robot?. |
References
- World Health Organization. World Report On Disability; World Health Organization: Geneva, Switzerland, 2011; Volume 1, pp. 57–70. [Google Scholar]
- O’Sullivan, S.B.; Schmitz, T.J.; Fulk, G.D. Physical Rehabilitation, 6th ed.; FA Davis Company: Philadelphia, PA, USA, 2013; p. 1505. [Google Scholar]
- Hocoma. Lokomat Therapy Is Backed Up by Nearly 20 Years of Clinical Research; Knowledge Hocoma: Volketswil, Switzerland, 2020. [Google Scholar]
- Barbeau, H.; Wainberg, M.; Finch, L. Description and application of a system for locomotor rehabilitation. Med. Biol. Eng. Comput. 1987, 25, 341–344. [Google Scholar] [CrossRef] [PubMed]
- Mayr, A.; Kofler, M.; Quirbach, E.; Matzak, H.; Fröhlich, K.; Saltuari, L. Prospective, blinded, randomized crossover study of gait rehabilitation in stroke patients using the Lokomat gait orthosis. Neurorehabilit. Neural Repair 2007, 21, 307–314. [Google Scholar] [CrossRef]
- Hwang, S.; Kim, H.R.; Han, Z.A.; Lee, B.S.; Kim, S.; Shin, H.; Moon, J.G.; Yang, S.P.; Lim, M.H.; Cho, D.Y.; et al. Improved Gait Speed After Robot-Assisted Gait Training in Patients With Motor Incomplete Spinal Cord Injury: A Preliminary Study. Ann. Rehabil. Med. 2017, 41, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Vänni, K.J.; Salin, S.E. Attitudes of Professionals toward the Need for Assistive and Social Robots in the Healthcare Sector; Springer: Cham, Switzerland; New York, NY, USA, 2019; pp. 205–236. [Google Scholar] [CrossRef]
- Appelbaum, S.H.; Marchionni, A.; Fernandez, A. The multi-tasking paradox: Perceptions, problems and strategies. Manag. Decis. 2008, 46, 1313–1325. [Google Scholar] [CrossRef]
- Kalisch, B.J.; Aebersold, M. Interruptions and multitasking in nursing care. Jt. Comm. J. Qual. Patient Saf. 2010, 36, 126–132. [Google Scholar] [CrossRef]
- Céspedes, N.; Irfan, B.; Senft, E.; Cifuentes, C.A.; Gutierrez, L.F.; Rincon-Roncancio, M.; Belpaeme, T.; Múnera, M. A Socially Assistive Robot for Long-Term Cardiac Rehabilitation in the Real World. Front. Neurorobot. 2021, 15, 1–19. [Google Scholar] [CrossRef]
- Fasola, J.; Matarić, M.J. Using socially assistive human-robot interaction to motivate physical exercise for older adults. Proc. IEEE 2012, 100, 2512–2526. [Google Scholar] [CrossRef]
- Masvaure, P.; Ruggunan, S.; Maharaj, A. Work Engagement, Intrinsic Motivation and Job Satisfaction among Employees of a Diamond Mining Company in Zimbabwe. J. Econ. Behav. Stud. 2014, 6, 488–499. [Google Scholar] [CrossRef] [Green Version]
- Casas, J.; Cespedes, N.; Múnera, M.; Cifuentes, C.A. Human-Robot Interaction for Rehabilitation Scenarios; Academic Press: Cambridge, MA, USA, 2020; pp. 1–31. [Google Scholar] [CrossRef]
- Leite, I.; Martinho, C.; Paiva, A. Social Robots for Long-Term Interaction: A Survey; Springer: New York, NY, USA, 2013; pp. 291–308. [Google Scholar] [CrossRef]
- Cifuentes, C.A.; Pinto, M.J.; Céspedes, N.; Munera, M. Social Robots in Therapy and Care; Springer: Berlin/Heidelberg, Germany, 2020. [Google Scholar] [CrossRef]
- Heerink, M.; Vanderborght, B.; Broekens, J.; Albo-Canals, J. New Friends: Social Robots in Therapy and Education. Int. J. Soc. Robot. 2016, 8, 443–444. [Google Scholar] [CrossRef] [Green Version]
- Fischinger, D.; Einramhof, P.; Papoutsakis, K.; Wohlkinger, W.; Mayer, P.; Panek, P.; Hofmann, S.; Koertner, T.; Weiss, A.; Argyros, A.; et al. Hobbit, a care robot supporting independent living at home: First prototype and lessons learned. Robot. Auton. Syst. 2016, 75, 60–78. [Google Scholar] [CrossRef]
- Riek, L.D. Healthcare robotics. Commun. ACM 2017, 60, 68–78. [Google Scholar] [CrossRef]
- Céspedes Gómez, N.; Calderon Echeverria, A.V.; Munera, M.; Rocon, E.; Cifuentes, C.A. First Interaction Assessment between a Social Robot and Children Diagnosed with Cerebral Palsy in a Rehabilitation Context; Association for Computing Machinery: New York, NY, USA, 2021; pp. 484–488. [Google Scholar] [CrossRef]
- Martí Carrillo, F.; Butchart, J.; Knight, S.; Scheinberg, A.; Wise, L.; Sterling, L.; McCarthy, C. In-situ design and development of a socially assistive robot for paediatric rehabilitation. In Proceedings of the ACM/IEEE International Conference on Human-Robot Interaction, Vienna, Austria, 6–9 March 2017; pp. 199–200. [Google Scholar] [CrossRef]
- Matarić, M.J.; Eriksson, J.; Feil-Seifer, D.J.; Winstein, C.J. Socially assistive robotics for post-stroke rehabilitation. J. Neuroeng. Rehabil. 2007, 4, 5. [Google Scholar] [CrossRef] [PubMed]
- Munera, M.; Marroquin, A.; Jimenez, L.; Lara, J.S.; Gomez, C.; Rodriguez, S.; Rodriguez, L.E.; Cifuentes, C.A. Lokomat Therapy in Colombia: Current State and Cognitive Aspects; IEEE: London, UK, 2017; pp. 394–399. [Google Scholar] [CrossRef]
- Casas, J.A.; Céspedes, N.; Cifuentes, C.A.; Gutierrez, L.F.; Rincón-Roncancio, M.; Múnera, M. Expectation vs. reality: Attitudes towards a socially assistive robot in cardiac rehabilitation. Appl. Sci. 2019, 9, 4651. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.C.; Jones, C.; Moyle, W. Health Professional and Workers Attitudes Towards the Use of Social Robots for Older Adults in Long-Term Care. Int. J. Soc. Robot. 2019, 12, 1135–1147. [Google Scholar] [CrossRef]
- Cespedes, N.; Munera, M.; Gomez, C.; Cifuentes, C.A. Social Human-Robot Interaction for Gait Rehabilitation. IEEE Trans. Neural Syst. Rehabil. Eng. 2020, 28, 1299–1307. [Google Scholar] [CrossRef] [PubMed]
- Céspedes, N.; Raigoso, D.; Múnera, M.; Cifuentes, C. Long-Term Social Human-Robot Interaction for Neurorehabilitation: Robots as a Tool to Support Gait Therapy in the Pandemic. Front. Neurorobot. 2021, 15, 612034. [Google Scholar] [CrossRef] [PubMed]
- Broadbent, E.; Stafford, R.; MacDonald, B. Acceptance of healthcare robots for the older population: Review and future directions. Int. J. Soc. Robot. 2009, 1, 319–330. [Google Scholar] [CrossRef]
- Sierra, S.D.; Gomez, D.; Céspedes, N.; Múnera, M.; Roberti, F.; Barria, P.; Ramamoorthy, S.; Becker, M.; Carelli, R.; Cifuentes, C.A. Expectations and Perceptions of Healthcare Professionals for Robot Deployment in Hospital Environments during the COVID-19 Pandemic. Front. Robot. AI 2021, 8, 102. [Google Scholar] [CrossRef]
- Breazeal, C.; Dautenhahn, K.; Kanda, T. Social robotics. In Handbook of Robotics; Springer International Publishing: Berlin/Heidelberg, Germany, 2016; pp. 1935–1971. [Google Scholar] [CrossRef]
- Shamsuddin, S. Humanoid robot NAO: Review of control and motion exploration. In Proceedings of the 2011 IEEE International Conference on Control System, Computing and Engineering, Penang, Malaysia, 25–27 November 2011; Volume 75. [Google Scholar] [CrossRef]
- Heerink, M.; Kröse, B.; Evers, V.; Wielinga, B. Assessing Acceptance of Assistive Social Agent Technology by Older Adults: The Almere Model. Int. J. Soc. Robot. 2010, 2, 361–375. [Google Scholar] [CrossRef] [Green Version]
- Venkatesh, V.; Morris, M.G.; Davis, G.B.; Davis, F.D. User Acceptance of Information Technology: Toward a Unified View. MIS Q. 2003, 27, 425–478. [Google Scholar] [CrossRef] [Green Version]
- Tavakol, M.; Dennick, R. Making sense of Cronbach’s alpha. Int. J. Med Educ. 2011, 2, 53–55. [Google Scholar] [CrossRef]
- Jalessi, M.; Farhadi, M.; Kamrava, S.K.; Amintehran, E.; Asghari, A.; Rezaei Hemami, M.; Mobasseri, A.; Masroorchehr, M. The reliability and validity of the persian version of sinonasal outcome test 22 (SNOT 22) questionnaires. Iran. Red Crescent Med. J. 2013, 15, 404–408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vandemeulebroucke, T.; de Casterlé, B.D.; Gastmans, C. How do older adults experience and perceive socially assistive robots in aged care: A systematic review of qualitative evidence. Aging Ment. Health 2018, 22, 149–167. [Google Scholar] [CrossRef] [PubMed]
- Bartneck, C.; Belpaeme, T.; Eyssel, F.; Kanda, T.; Keijsers, M.; Šabanović, S. Human-Robot Interaction; Cambridge University Press: Cambridge, UK, 2020. [Google Scholar] [CrossRef] [Green Version]
- Stafford, R.Q.; MacDonald, B.A.; Jayawardena, C.; Wegner, D.M.; Broadbent, E. Does the Robot Have a Mind? Mind Perception and Attitudes Towards Robots Predict Use of an Eldercare Robot. Int. J. Soc. Robot. 2014, 6, 17–32. [Google Scholar] [CrossRef]
- Jokinen, K.; Wilcock, G. Multimodal Open-Domain Conversations with Robotic Platforms; Academic Press: Cambridge, MA, USA, 2018; pp. 9–26. [Google Scholar] [CrossRef]
- Hayashi, K.; Sakamoto, D.; Kanda, T.; Shiomi, M.; Koizumi, S.; Ishiguro, H.; Ogasawara, T.; Hagita, N. Humanoid Robots as a Passive-Social Medium: A Field Experiment at a Train Station; Association for Computing Machinery: New York, NY, USA, 2007; pp. 137–144. [Google Scholar] [CrossRef]
- Wu, Y.H.; Fassert, C.; Rigaud, A.S. Designing robots for the elderly: Appearance issue and beyond. Arch. Gerontol. Geriatr. 2012, 54, 121–126. [Google Scholar] [CrossRef] [PubMed]




| Clinicians (n = 77) | Patients (n = 11) | |
|---|---|---|
| Age (years), mean (SD) | 27.87, 9.43 | 33.63, 15.70 |
| Gender, (n) | Female (58) Male (19) | Female (8) Male (8) |
| Profession, Patients diagnosis | Physiotheraphist (50) Therapist (8) Physiatrist (1) Other professions (18) | Cerebral Palsy |
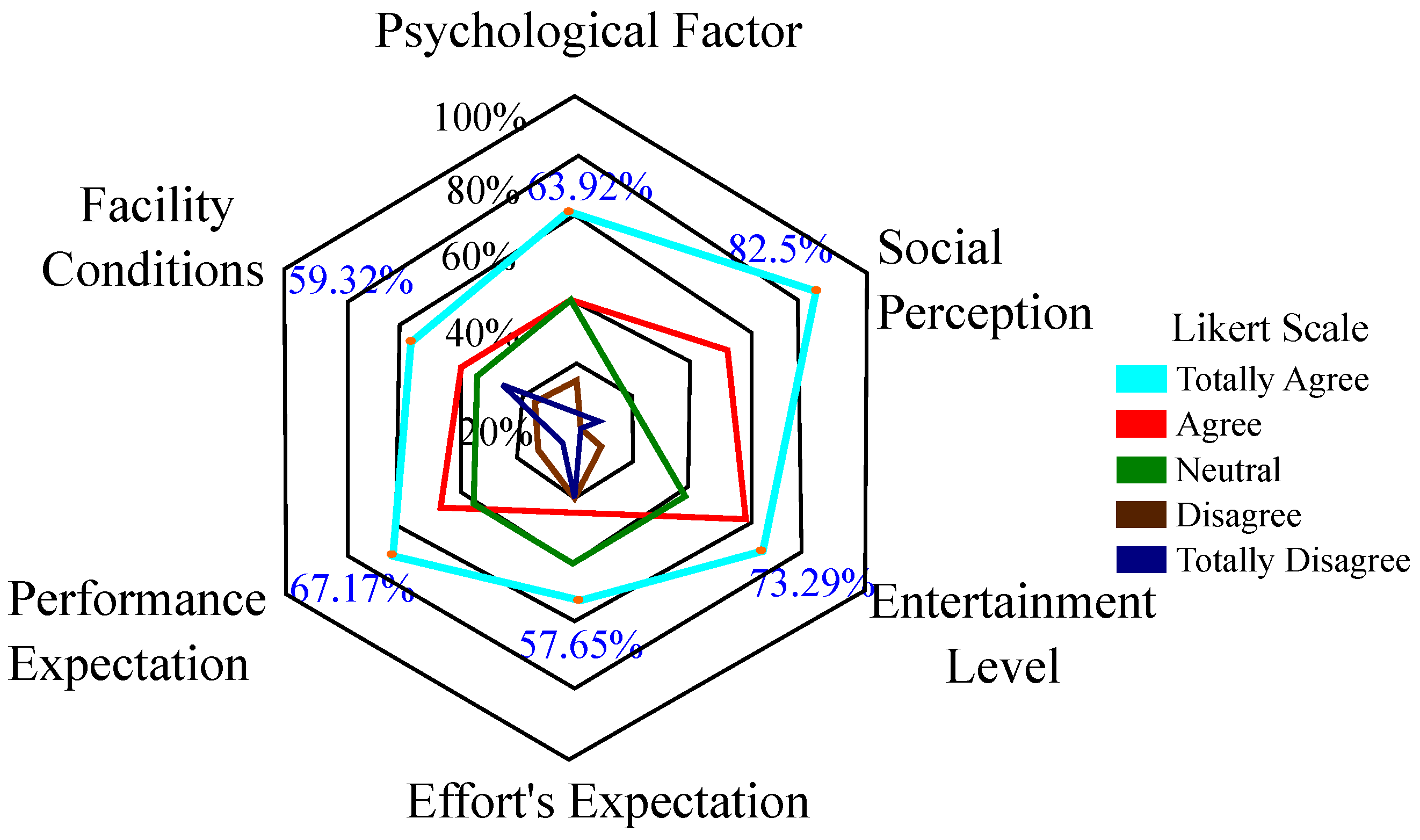
| Construct | Definition |
|---|---|
| Psychological Factor | The degree to which an individual believes that the use of technology will generate trust and comfort during its implementation. |
| Social Perception | The degree to which an individual perceives that others value the use of the system. |
| Entertainment Level | The degree to which an individual considers that the technology used provides fun and entertainment when it is used. |
| Effort’s Expectation | The ease of use perceived by the user towards the system. |
| Performance Expectation | The degree to which an individual believes that the use of the system will help to obtain a benefit in his/her self-performance. |
| Facility Conditions | The degree to which an individual considers an organized and technical structure helps her or him adapt to the technology. |
| Construct | Mean (Patients) ± SD | Mean (Clinicians) ± SD | p-Value |
|---|---|---|---|
| PF | 4.02 ± 0.32 | 4.87 ± 0.13 | 0.16 |
| SP | 4.85 ± 0.09 | 4.76 ± 0.24 | 0.06 |
| EL | 4.98 ± 0.18 | 4.29 ± 0.21 | |
| EE | 3.67 ± 0.52 | 2.98 ± 0.43 | 0.57 |
| PE | 3.99 ± 0.70 | 4.78 ± 0.56 | |
| FC | 4.23 ± 0.25 | 3.85 ± 0.28 | 0.27 |
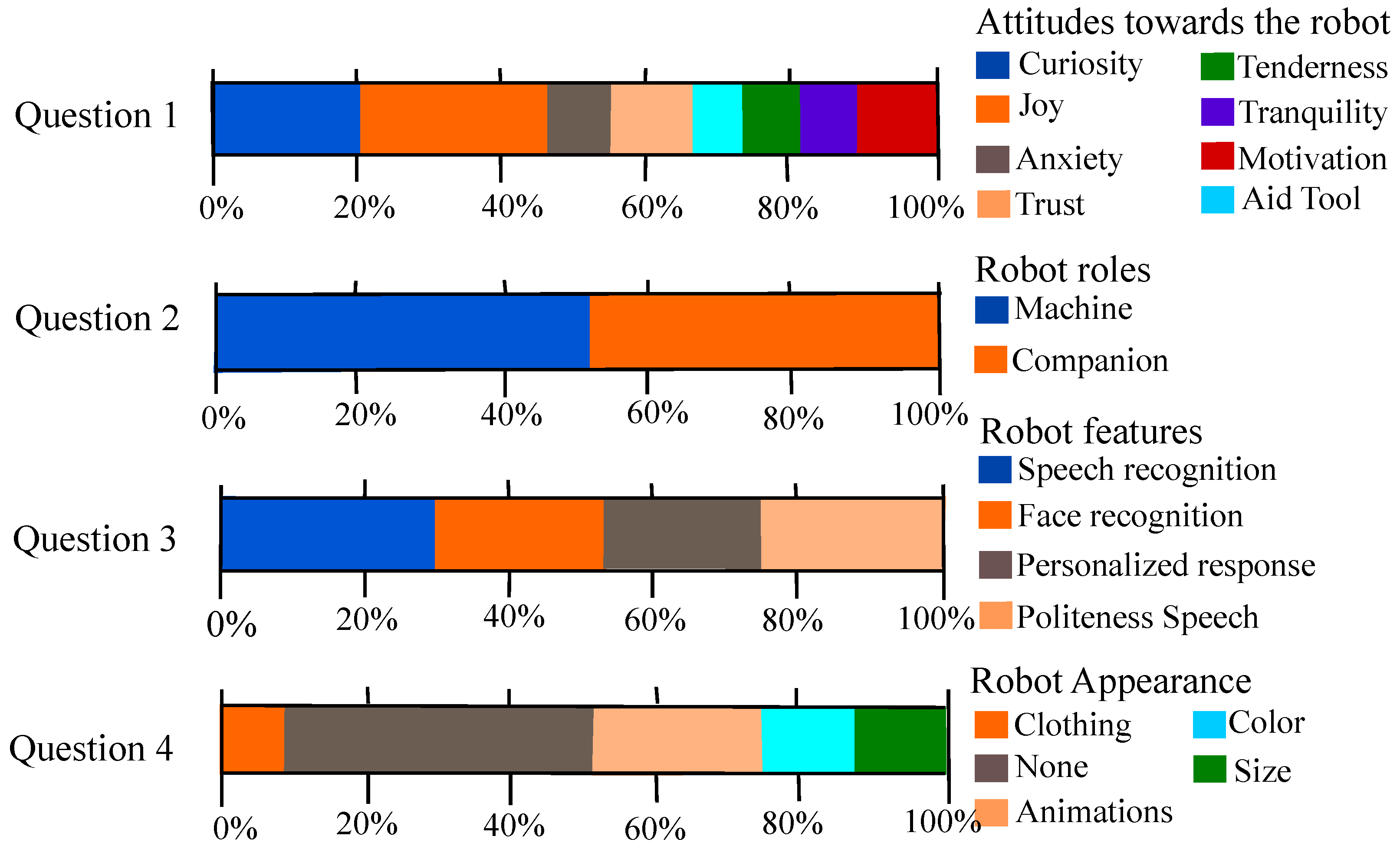
| Questions | Selected Vocabulary | Frecuency |
|---|---|---|
| What does the robot inspire you? | Curiosity | 13 |
| Joy | 16 | |
| Anxiety | 5 | |
| Trust | 8 | |
| Aid Tool | 3 | |
| Tenderness | 5 | |
| Tranquility | 5 | |
| Motivation | 6 | |
| How do you perceive the robot? | Machine | 46 |
| Companion | 42 | |
| What kind of interactions or gestures should a robot have for a closer interaction? | Politeness Speech | 17 |
| Speech Recognition | 23 | |
| Personalized Response | 17 | |
| Facial Recognition | 17 | |
| What physical changes would it make to the robot? | Animations | 15 |
| Clothing | 7 | |
| Color | 10 | |
| Size | 11 | |
| None | 32 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Raigoso, D.; Céspedes, N.; Cifuentes, C.A.; del-Ama, A.J.; Múnera, M. A Survey on Socially Assistive Robotics: Clinicians’ and Patients’ Perception of a Social Robot within Gait Rehabilitation Therapies. Brain Sci. 2021, 11, 738. https://doi.org/10.3390/brainsci11060738
Raigoso D, Céspedes N, Cifuentes CA, del-Ama AJ, Múnera M. A Survey on Socially Assistive Robotics: Clinicians’ and Patients’ Perception of a Social Robot within Gait Rehabilitation Therapies. Brain Sciences. 2021; 11(6):738. https://doi.org/10.3390/brainsci11060738
Chicago/Turabian StyleRaigoso, Denniss, Nathalia Céspedes, Carlos A. Cifuentes, Antonio J. del-Ama, and Marcela Múnera. 2021. "A Survey on Socially Assistive Robotics: Clinicians’ and Patients’ Perception of a Social Robot within Gait Rehabilitation Therapies" Brain Sciences 11, no. 6: 738. https://doi.org/10.3390/brainsci11060738