
The Impact of Exercise Intervention with Rhythmic Auditory Stimulation to Improve Gait and Mobility in Parkinson Disease: An Umbrella Review


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Search Strategy and Study Selection
2.3. Quality Assessment
2.4. Data Extraction
3. Results
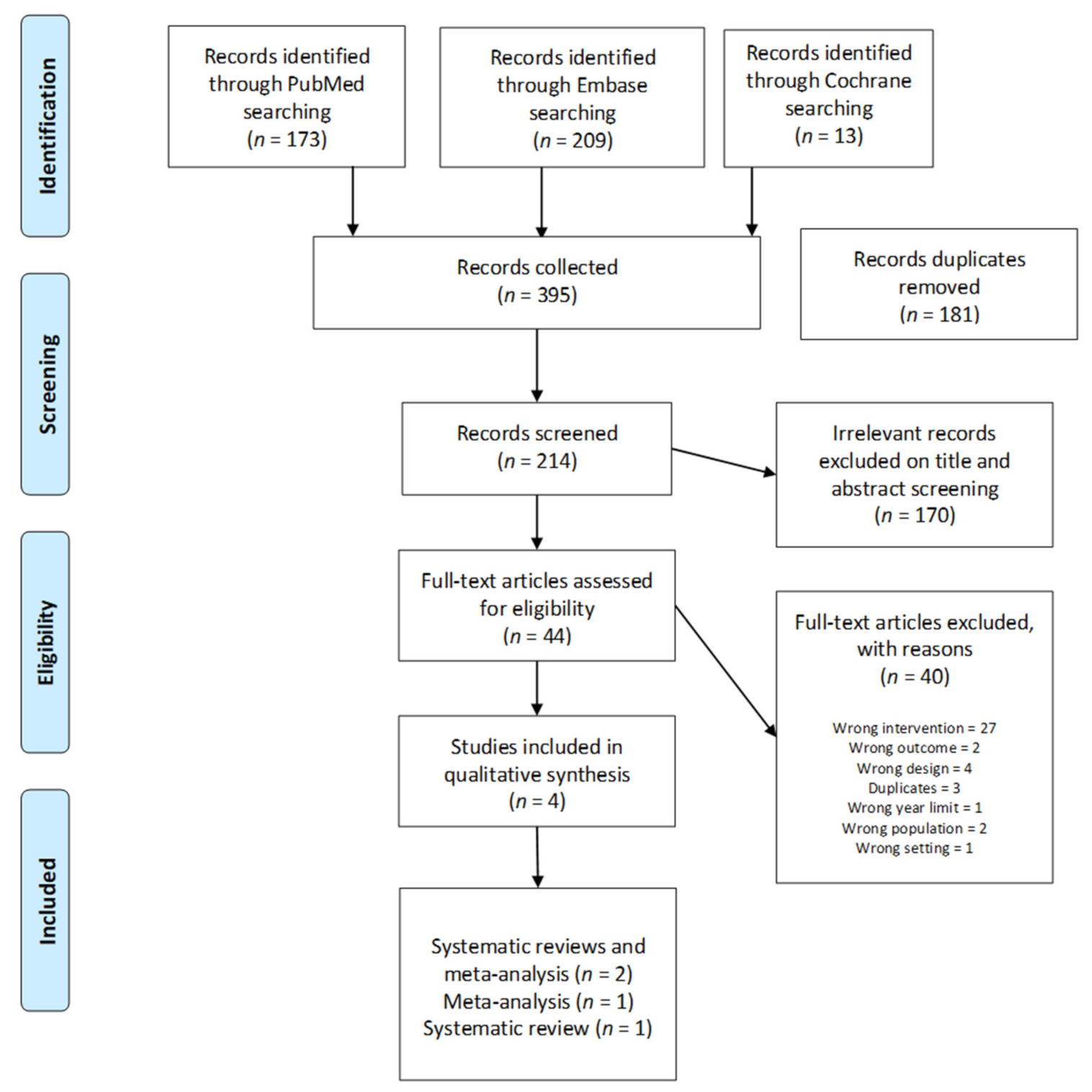
3.1. Study Selection
3.2. Study Characteristics
3.3. Study Outcomes
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Funding
Conflicts of Interest
References
- Dorsey, E.R.; Bloem, B.R. The Parkinson pandemic-a call to action. JAMA Neurol. 2018, 75, 9–10. [Google Scholar] [CrossRef] [PubMed]
- GBD 2016 Parkinson’s Disease Collaborators. Global, regional, and national burden of Parkinson’s disease, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2018, 17, 939–953. [Google Scholar] [CrossRef] [Green Version]
- Kouli, A.; Torsney, K.M.; Kuanin, W.L. Parkinson’s Disease: Etiology, Neuropathology, and Pathogenesis. In Pathogenesis and Clinical Aspects; Stoker, T.B., Greenland, J.C., Eds.; Codon Publications: Brisbane, QLD, Australia, 2018; pp. 4–26. [Google Scholar]
- Peterson, D.S.; Horak, F.B. Neural Control of Walking in People with Parkinsonism. Physiology 2016, 31, 95–107. [Google Scholar] [CrossRef] [Green Version]
- Hobert, M.A.; Nussbaum, S.A.; Heger, T.; Berg, D.; Maetzler, W.; Heinzel, S. Progressive Gait Deficits in Parkinson’s Disease: A Wearable-Based Biannual 5-Year Prospective Study. Front. Aging. Neurosci. 2019, 11, 22. [Google Scholar] [CrossRef]
- Silva de Lima, A.L.; Borm, C.; Vries, N.M.D.; Bloem, B.R. Falling among people with Parkinson’s disease: Motor, non-motor, or both? Arq. Neuropsiquiatr. 2019, 77, 759–760. [Google Scholar] [CrossRef] [Green Version]
- Smulders, K.; Dale, M.L.; Carlson-Kuhta, P.; Nutt, J.G.; Horak, F.B. Pharmacological treatment in Parkinson’s disease: Effects on gait. Parkinsonism Relat. Disord. 2016, 31, 3–13. [Google Scholar] [CrossRef] [Green Version]
- Greenland, J.C.; Barker, R.A. The Differential Diagnosis of Parkinson’s Disease. In Parkinson’s Disease: Etiology, Neuropathology, and Pathogenesis and Clinical Aspects; Stoker, T.B., Greenland, J.C., Eds.; Codon Publications: Brisbane, QLD, Australia, 2018; pp. 109–128. [Google Scholar]
- Zahoor, I.; Shafi, A.; Haq, E. Pharmacological Treatment of Parkinson’s Disease. In Pathogenesis and Clinical Aspects; Stoker, T.B., Greenland, J.C., Eds.; Codon Publications: Brisbane, QLD, Australia, 2018; pp. 129–143. [Google Scholar]
- PD Med Collaborative Group. Long-term effectiveness of dopamine agonists and monoamine oxidase B inhibitors compared with levodopa as initial treatment for Parkinson’s disease (PD MED): A large, open-label, pragmatic randomised trial. Lancet 2014, 384, 1196–1205. [Google Scholar] [CrossRef]
- Levy, G. The relationship of Parkinson disease with aging. Arch. Neurol. 2007, 64, 1242–1246. [Google Scholar] [CrossRef]
- Bryant, M.S.; Rintala, D.H.; Hou, J.G.; Lai, E.C.; Protas, E.J. Effects of levodopa on forward and backward gait patterns in persons with Parkinson’s disease. NeuroRehabilitation 2011, 29, 247–252. [Google Scholar] [CrossRef]
- Hou, L.; Chen, W.; Liu, X.; Qiao, D.; Zhou, F.M. Exercise-induced neuroprotection of the nigrostriatal dopamine system in Parkinson’s disease. Front Aging Neurosci. 2017, 9, 358. [Google Scholar] [CrossRef] [Green Version]
- Mak, M.K.; Wong-Yu, I.S.; Shen, X.; Chung, C.L. Long-term effects of exercise and physical therapy in people with Parkinson disease. Nat. Rev. Neurol. 2017, 13, 689. [Google Scholar] [CrossRef]
- Steiger, L.; Homann, C.N. Exercise therapy in Parkinson’s disease–An overview of current interventional studies. Physiother. Res. Rep. 2019, 2, 1–10. [Google Scholar] [CrossRef]
- Rafferty, M.R.; Schmidt, P.N.; Luo, S.T.; Li, K.; Marras, C.; Davis, T.L.; Guttman, M.; Cubillos, F.; Simuni, T. Regular Exercise, Quality of Life, and Mobility in Parkinson’s Disease: A Longitudinal Analysis of National Parkinson Foundation Quality Improvement Initiative Data. J. Parkinsons Dis. 2017, 7, 193–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bouça-Machado, R.; Rosário, A.; Caldeira, D.; Castro Caldas, A.; Guerreiro, D.; Venturelli, M.; Tinazzi, M.; Schena, F.; Ferreira, J. Physical activity, exercise, and physiotherapy in parkinson’s disease: Defining the concepts. Movem. Disord. Clin. Pract. 2020, 7, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Oliveira de Carvalho, A.; Souza Sá Filho, A.; Murillo-Rodriguez, E.; Barbosa Rocha, N.; Carta, M.G.; Machado, S. Physical Exercise For Parkinson’s Disease: Clinical And Experimental Evidence. Clin. Pract. Epidemiol. Ment. Health 2018, 30, 14. [Google Scholar] [CrossRef]
- Keus, S.H.J.; Bloem, B.R.; Hendriks, E.J.M.; Bredero-Cohen, A.B.; Munneke, M. Practice Recommendations Development Group Evidence-based analysis of physical therapy in Parkinson’s disease with recommendations for practice and research. Mov. Disord. 2007, 22, 451–460. [Google Scholar] [CrossRef]
- Choi, H.Y.; Cho, K.H.; Jin, C.; Lee, J.E.; Kim, T.H.; Jung, W.S.; Moon, S.K.; Ko, C.N.; Cho, S.Y.; Jeon, C.Y.; et al. Exercise Therapies for Parkinson’s Disease: A Systematic Review and Meta-Analysis. Parkinsons Dis. Sep. 2020, 8, 2565320. [Google Scholar] [CrossRef]
- Braunlich, K.; Seger, C.A.; Jentink, K.G.; Buard, I.; Kluger, B.M.; Thaut, M.H. Rhythmic auditory cues shape neural network recruitment in Parkinson’s disease during repetitive motor behavior. Eur. J. Neurosci. 2019, 49, 849–858. [Google Scholar] [CrossRef]
- Frazzitta, G.; Bertotti, G.; Riboldazzi, G.; Turla, M.; Uccellini, D.; Boveri, N.; Guaglio, G.; Perini, M.; Comi, C.; Balbi, P.; et al. Effectiveness of intensive inpatient rehabilitation treatment on disease progression in parkinsonian patients: A randomized controlled trial with 1-year follow-up. Neurorehabil. Neural. Repair. 2012, 26, 144–150. [Google Scholar] [CrossRef]
- Espay, A.J.; Baram, Y.; Dwivedi, A.K.; Shukla, R.; Gartner, M.; Gaines, L.; Duker, A.P.; Revilla, F.J. At-home training with closed-loop augmented-reality cueing device for improving gait in patients with Parkinson disease. J. Rehabil. Res. Dev. 2010, 47, 573–581. [Google Scholar] [CrossRef]
- Rochester, L.; Rafferty, D.; Dotchin, C.; Msuya, O.; Minde, V.; Walker, R.W. The effect of cueing therapy on single and dual-task gait in a drug naive population of people with Parkinson’s disease in Northern Tanzania. Mov. Disord. 2010, 25, 906–911. [Google Scholar] [CrossRef] [PubMed]
- Thaut, M.H.; Abiru, M. Rhythmic auditory stimulation in rehabilitation of movement disorders: A review of current research. Music Percept. 2010, 27, 263–269. [Google Scholar] [CrossRef] [Green Version]
- Spaulding, S.J.; Barber, B.; Colby, M.; Cormack, B.; Mick, T.; Jenkins, M. Cueing and gait improvement among people with Parkinson’s disease: A meta-analysis. Arch. Phys. Med. Rehabil. 2013, 94, 562–570. [Google Scholar] [CrossRef]
- Ashoori, A.; Eagleman, D.M.; Jankovic, J. Effects of Auditory Rhythm and Music on Gait Disturbances in Parkinson’s Disease. Front. Neurol. 2015, 11, 6–234. [Google Scholar] [CrossRef] [Green Version]
- Hove, M.J.; Keller, P.E. Impaired movement timing in neurological disorders: Rehabilitation and treatment strategies. Ann. N. Y. Acad. Sci. 2015, 1337, 111–117. [Google Scholar] [CrossRef] [Green Version]
- Kadivar, Z.; Corcos, D.M.; Foto, J.; Hondzinski, J.M. Effect of step training and rhythmic auditory stimulation on functional performance in Parkinson patients. Neurorehabil. Neural. Repair. 2011, 25, 626–635. [Google Scholar] [CrossRef] [Green Version]
- Thaut, M.H.; McIntosh, G.C.; Hoemberg, V. Neurobiological foundations of neurologic music therapy: Rhythmic entrainment and the motor system. Front. Psychol. 2015, 5, 1185. [Google Scholar] [CrossRef] [Green Version]
- Raglio, A. Music therapy interventions in Parkinson’s disease: The state-of-the-art. Front. Neurol. 2015, 6, 185. [Google Scholar] [CrossRef] [Green Version]
- Thaut, M.H.; Kenyon, G.P.; Schauer, M.L.; McIntosh, G.C. The connection between rhythmicity and brain function. IEEE Eng. Med. Biol. Mag. 1999, 18, 101–108. [Google Scholar] [CrossRef]
- Koshimori, Y.; Thaut, M.H. Future perspectives on neural mechanisms underlying rhythm and music based neurorehabilitation in Parkinson’s disease. Ageing Res. Rev. 2018, 47, 133–139. [Google Scholar] [CrossRef]
- Ford, M.P.; Malone, L.A.; Nyikos, I.; Yelisetty, R.; Bickel, C.S. Gait training with progressive external auditory cueing in persons with Parkinson’s disease. Arch. Phys. Med. Rehab. 2010, 91, 1255–1261. [Google Scholar] [CrossRef]
- Thaut, M.H.; McIntosh, G.C.; Rice, R.R.; Miller, R.A.; Rathbun, J.; Brault, J.M. Rhythmic auditory stimulation in gait training for Parkinson’s disease patients. Mov. Disord. 1996, 11, 193–200. [Google Scholar] [CrossRef]
- Cosentino, C.; Baccini, M.; Putzolu, M.; Ristori, D.; Avanzino, L.; Pelosin, E. Effectiveness of Physiotherapy on Freezing of Gait in Parkinson’s Disease: A Systematic Review and Meta-Analyses. Mov. Disord. 2020, 35, 523–536. [Google Scholar] [CrossRef]
- Delgado-Alvarado, M.; Marano, M.; Santurtún, A.; Urtiaga-Gallano, A.; Tordesillas-Gutierrez, D.; Infante, J. Nonpharmacological, nonsurgical treatments for freezing of gait in Parkinson’s disease: A systematic review. Mov. Disord. 2020, 35, 204–214. [Google Scholar] [CrossRef]
- Foster, E.R.; Bedekar, M.; Tickle-Degnen, L. Systematic review of the effectiveness of occupational therapy-related interventions for people with Parkinson’s disease. Am. J. Occup. Ther. 2014, 68, 39–49. [Google Scholar] [CrossRef] [Green Version]
- Tomlinson, C.L.; Patel, S.; Meek, C.; Herd, C.P.; Clarke, C.E.; Stowe, R.; Shah, L.; Sackley, C.M.; Deane, K.H.; Wheatley, K.; et al. Physiotherapy versus placebo or no intervention in Parkinson’s disease. Cochrane. Database. Syst. Rev. 2013, 10, CD002817. [Google Scholar] [CrossRef] [Green Version]
- Harrison, S.L.; Laver, K.E.; Ninnis, K.; Rowett, C.; Lannin, N.A.; Crotty, M. Effectiveness of external cues to facilitate task performance in people with neurological disorders: A systematic review and meta-analysis. Disabil. Rehabil. 2019, 41, 1874–1881. [Google Scholar] [CrossRef] [Green Version]
- Rutz, D.G.; Benninger, D.H. Physical Therapy for Freezing of Gait and Gait Impairments in Parkinson Disease: A Systematic Review. PM R. 2020, 12, 1140–1156. [Google Scholar] [CrossRef]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef] [Green Version]
- Pieper, D.; Antoine, S.L.; Mathes, T.; Neugebauer, E.A.M.; Eikermann, M. Systematic review finds overlapping reviews were not mentioned in every other overview. Clin. Epidemiol. 2014, 67, 368–375. [Google Scholar] [CrossRef]
- Cassimatis, C.; Liu, K.P.Y.; Fahey, P.; Bissett, M. The effectiveness of external sensory cues in improving functional performance in individuals with Parkinson’s disease: A systematic review with meta-analysis. Int. J. Rehabil. Res. 2016, 39, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Ghai, S.; Ghai, I.; Schmitz, G.; Effenberg, A.O. Effect of rhythmic auditory cueing on parkinsonian gait: A systematic review and meta-analysis. Sci. Rep. 2018, 8, 506. [Google Scholar] [CrossRef] [PubMed]
- Rocha, P.A.; Porfírio, G.M.; Ferraz, H.B.; Trevisani, V.F.M. Effects of external cues on gait parameters of Parkinson’s disease patients: A systematic review. Clin. Neurol. Neurosurg. 2014, 124, 127–134. [Google Scholar] [CrossRef]
- Rodríguez-Molinero, A.; Herrero-Larrea, A.; Miñarro, A.; Narvaiza, L.; Gálvez-Barrón, C.; Gonzalo León, N.; Valldosera, E.; de Mingo, E.; Macho, O.; Aivar, D.; et al. The spatial parameters of gait and their association with falls, functional decline and death in older adults: A prospective study. Sci. Rep. 2019, 9, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herssens, N.; Verbecque, E.; Hallemans, A.; Vereeck, L.; Van Rompaey, V.; Saeys, W. Do spatiotemporal parameters and gait variability differ across the lifespan of healthy adults? A systematic review. Gait. Posture 2018, 64, 181–190. [Google Scholar] [CrossRef] [PubMed]
- Mirelman, A.; Bonato, P.; Camicioli, R.; Ellis, T.D.; Giladi, N.; Hamilton, J.L.; Hass, C.J.; Hausdorff, J.M.; Pelosin, E.; Almeida, Q.J. Gait impairments in Parkinson’s disease. Lancet Neurol. 2019, 18, 697–708. [Google Scholar] [CrossRef]
- Leuk, J.S.P.; Low, L.L.N.; Teo, W.P. An Overview of Acoustic-Based Interventions to Improve Motor Symptoms in Parkinson’s Disease. Front. Aging Neurosci. 2020, 12, 243. [Google Scholar] [CrossRef]
- Woerd, E.S.; Oostenveld, R.; de Lange, F.P.; Praamstra, P. A shift from prospective to reactive modulation of beta-band oscillations in Parkinson’s disease. Neuroimage 2014, 100, 507–519. [Google Scholar] [CrossRef]
- Engel, A.K.; Fries, P. Beta-band oscillations--signalling the status quo? Curr. Opin. Neurobiol. 2010, 20, 156–165. [Google Scholar] [CrossRef]
- Gallo, P.M.; Garber, C.E. Parkinson’s disease: A comprehensive approach to exercise prescription for the health fitness professional. ACSM Health Fit. J. 2011, 15, 8–17. [Google Scholar] [CrossRef]
- Kelly, V.E.; Eusterbrock, A.J.; Shumway-Cook, A. A review of dual-task walking deficits in people with Parkinson’s disease: Motor and cognitive contributions, mechanisms, and clinical implications. Parkinsons Dis. 2012, 2012, 918719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, I.; van Wegen, E.; de Goede, C.; Deutekom, M.; Nieuwboer, A.; Willems, A.; Jones, D.; Rochester, L.; Kwakkel, G. Effects of external rhythmical cueing on gait in patients with Parkinson’s disease: A systematic review. Clin. Rehabil. 2005, 19, 695–713. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Inclusion Criteria for Reviews and Meta-Analyses | Exclusion Criteria for Reviews and Meta-Analyses |
|---|---|
| Studies on individuals with Parkinson disease of any age and level of severity | Studies with frail participants or with other neurological conditions, or cognitive impairment |
| Studies on physical exercise/activity interventions, applying music or other rhythmical or auditory stimulus | Studies on any form of dance or music therapy |
| Studies with primary outcomes related to mobility and gait (including FOG) and activities of daily living (ADL) | Studies with primary aims other than gait, mobility, and ADL |
| Studies in English | Narrative reviews |
| Studies published between 2010 and 2020 | Studies on other type of stimulus/their combination with auditory stimulus |
| Reviews including RCTs, CCTs and QRCT |
| Authors, Year | Aim of Study, Type of Study | Number of Included Studies, Type of Included Study | Participants: Number, Gender, Age Range, Disease Level/ Duration | Outcome | Intervention Protocols, Duration (Overall and Weekly Frequency) |
|---|---|---|---|---|---|
| Cassimatis et al., 2016 [44] | To verify the effects of external sensory cues in improving functional performance of ADL, walking, and daily tasks in PD; | 3 studies were included in the meta-analysis of pre-post treatment | 112, M&F, 63–73 years, II–IV | UPDRS II | 45–90 min 2–3 days per week 2–6 weeks Applied auditory stimuli: metronome, words, clunk, ding sounds Proposed Exercises with RAS: overground walking, treadmill walking, turning, stepping, sit to stand, performance of ADLs |
| Systematic review and meta-analysis | RCTs level II of the NHMRC Hierarchy of Evidence (National Health and Medical Research Council) | ||||
| Ghai et al., 2018 [45] | To analyze the effects of rhythmic auditory cueing on gait and postural performance in patients affected by Parkinson disease. | 51, RCT, CRCT, CCT | 1892, M = 1089, F = 745; 24–79 years; Duration of disease 3–14 years | Gait and postural parameters: Gait velocity Stride length Cadence Double limb support time Turn time | RAS and cadence: Preferred; +5%, +10%, +15%, +20% +25%; −10%; 105–144 bpm; 96–100 bpm. Metronome: preferred cadence, 80–124 steps min; −10, −20, +10, +20, +25% of preferred cadence;metronome embedded in music;30, 60, 90, 120, 150 bpm; Music: beat rhythm adjusted −10, +5, +10% preferred cadence;Musical instruments: Piano tones; percussions; Other sounds: Clicking sound generated with gait step; synthesized gravel step sound corresponding to plantar force; beep at preferred cadence; high pitched beep at preferred cadence; |
| Systematic review and meta-analysis | 7 Randomized controlled trials (RCT), 44 controlled clinical trials (CCT) | ||||
| Rocha et al., 2014 [46] | Evaluate the benefits of external cues on the gait of PD patients and their impact on the quality of life, freezing and psychomotor performance | 7 studies: 6 RCTs, 1 QRCT | 204, M&F mean age 68.8 years. The Hoehn Yahr, mean stage was 2.4. | Gait (step length, stride length, speed, cadence), freezing, psychomotor (UPDRS) | The authors did not include stimulus intensity and type of auditory cues in the session. |
| Systematic review of randomized clinical trials (RCTs) and quasi-randomized clinical trials (QRCTs) | Treadmill + visual cues × overground + visual cues × control (no intervention) 18 therapies 6 weeks 3 × week 30 min | ||||
| Conventional therapy + overground + visual cues × conventional therapy 20 therapies 01 h | |||||
| Treadmill + auditory cues × treadmill × home gait training 12 therapies 4 weeks 3 × week 30 min | |||||
| Overground + auditory cues × overground gait training × control (no intervention) NA 3 weeks NA 30 min Overground +verbal instruction × control (no intervention) 10 therapies 2 weeks 5 × week NA | |||||
| Spaulding et al., 2013 [26] | To compare the relative efficacy of visual versus auditory cueing on gait among individuals with Parkinson disease (PD). | 25 peer-reviewed publications. | 718, M&F, age mean 61.7–73.3. Duration of PD (mean) 6.5–10.0. MMSE > 24–29.0 (range 27–30) HY Stage (mean) 1 or 2–18/4. Medication On/Off. UPDRS range 10.9-44 | Kinematic gait parameters (cadence, velocity and stride length) | Prototype rhythmic auditory device, time of intervention to posttest: Immediate Pacer: Immediate. |
| Studies that reported pre-and post-outcome measures of gait parameters. |
| Authors, Year | Appraisal of Methodological Quality, Score | Statistical Method | Results/Summary Statistics (95% CI) |
|---|---|---|---|
| Cassimatis et al., 2016 [44] | PEDRO scale 4–8 low to moderate RCT | Random effect model (R the metafor package) | UPDRS II: post-treatment RE model: total (95% Cl) MD (95%CI) −2.27 (−4.03 to −052) Heterogeneity: Ƭ2 = 0; 2 = 1.3380, d.f. = 2 (p = 0.5122); I2 = 0% Test for overall effect: Z = −2.5353 (p = 0.0112) |
| high (7 or higher), moderate (4, 5 or 6) and low (less than 4) quality | Mean scores, associated SDs and sample sizes for treatment and control groups were extracted and analyzed. Mean difference (MD) in outcome between groups after treatment was computed. The MD could be applied as all studies used the same outcome measure. Results were considered statistically significant if the 95% confidence intervals (CIs) of the forest plot did not include 0. The statistical significance is summarized as a p-value, p < 0.05 considered statistically significant. | ||
| Systematic review of RCTs of level II (low risk of bias) of the NHMRC Hierarchy of Evidence (National Health and Medical Research Council) | Heterogeneity was tested with I2-test, values greater than 40% interpreted as considerable heterogeneity. A p-value < 0.05 indicates significant heterogeneity of intervention effects | ||
| Ghai et al., 2018 [45] | PEDro quality scale Included only ≥4, mean 5.4 (fair) range 4–8 | Random and fixed effect meta-analysis | Sub-group analyses were performed in case of unexplained heterogeneity (see text) Gait velocity (34 studies): small ES (g: 0.23, 95% C.I: 0.1 to 0.3) with substantial heterogeneity (I2: 87.4%, p > 0.01). On-off medication: “off”: positive small ES, (g: 0.43, 95% C.I: 0.11 to 0.75, I2: 18.8%, p = 0.29), negligible heterogeneity; “on”: positive medium ES (g: 0.55, 95% C.I: 0.23 to 0.87, I2: 0.0%, p = 0.44), negligible heterogeneity. Use of treadmill: positive large ES, negligible heterogeneity (g: 1.0, 95% C.I: 0.33 to 1.67, I2: 24.6%, p = 0.24). “Fast” and “Slow” auditory cueing: positive medium ES for “fast”, negligible heterogeneity (g: 0.7, 95% C.I: 0.50 to 0.89, I2: 0.0%, p = 0.44), negative small ES for “slow” group, negligible heterogeneity (g: −0.24, 95% C.I: 10.51 to 0.19, I2: 23.53%, p = 0.24). Acute effect of auditory stimulus (10 studies): negative small ES (g: −0.34, 95% C.I: −0.5 to −0.18, I2: 85.9%, p < 0.01), substantial heterogeneity. Disease duration: <9 years positive small ES (g: 0.16, 95% C.I: −0.12 to 0.44, I2: 0%, p = 0.56), negligible heterogeneity; >9 years negative small ES (g: −0.37, 95% C.I: −0.62 to −0.13, I2: 91%, p < 0.01), substantial heterogeneity. Training effect of RAS: positive medium ES with moderate heterogeneity (g: 0.64, 95% C.I: 0.37 to 0.92, I2: 36.08%, p = 0.34). Session duration: 30–45 min, positive medium ES with moderate heterogeneity (g: 0.52, 95% C.I: 0.38 to 0.66, I2: 33.8%, p > 0.05). 20 min, positive large ES with substantial heterogeneity (g: 1.09, 95% C.I: 0.7 to 1.47, I2: 80.9%, p < 0.01). Training duration: <5 weeks positive medium ES, substantial heterogeneity (g: 0.73, 95% C.I: 0.31 to 1.14, I2: 21.3%, p > 0.05). >5 weeks positive small ES, negligible heterogeneity (g: 0.46, 95% C.I: 0.2 to 0.72, I2: 0%, p > 0.05) Stride length (35 studies): positive small ES (g: 0.42, 95% C.I: 0.35 to 0.5, I2: 85.05%, p < 0.01) substantial heterogeneity; On-off medication: large positive ES for both “on” and “off” (g: 0.86, 95% C.I: 0.52 to 1.2, I2: 0%, p = 0.64), (g: 0.96, 95% C.I: 0.59 to 1.34, I2: 0%, p = 0.39), negligible heterogeneity. “Fast” and “Slow” auditory cueing: “fast” positive small ES (g: 0.30, 95% C.I: 0.08 to 0.52, I2: 0%, p = 0.7), negligible heterogeneity; “slow” positive medium ES (g: 0.69, 95% C.I: 0.35 to 1.03, I2: 20.03%, p = 0.29), negligible heterogeneity. Un-modulated RAS (23 studies): positive small ES (g: 0.35, 95% C.I: 0.22 to 0.48, I2: 35.3%, p = 0.04) moderate heterogeneity: Acute effect: a positive small ES (g: 0.12, 95% C.I: −0.11 to 0.35, I2: 0%, p = 0.72) negligible heterogeneity; Training effect: small EF (g: 0.37, 95% C.I: 0.23 to 0.51, I2: 26.2%, p = 0.16), moderate heterogeneity 30 min positive small ES (g: 0.36, 95% C.I: 0.21 to 0.51, I2: 42.5%, p = 0.07), moderate heterogeneity. Training frequency: <5 weekly session, small positive ES (g: 0.39, 95% C.I: 0.08 to 0.7, I2: 0%, p < 0.11), negligible heterogeneity. >5 weekly sessions, small positive ES (g: 0.4, 95% C.I: 0.1 to 0.68, I2: 0%, p > 0.5), negligible heterogeneity. Cadence (30 studies): negative small EF (g: −0.05, 95% C.I: −0.13 to 0.03, I2: 93.6%, p < 0.01) with substantial heterogeneity “On” and “off” medication: “off” negative small ES (g: −0.10, 95% C.I: −0.46 to −0.25, I2: 81.97%, p = 0.01), substantial heterogeneity; “on” positive small ES (g: −0.13, 95% C.I: −0.20 to 0.46, I2: 89.69%, p < 0.01), substantial heterogeneity. Fast-slow tempo: “fast” stimuli in less severe patients showed positive medium EF (g: 0.61, 95% C.I: 0.25 to 0.94, I2: 0%, p = 0.49), negligible heterogeneity; in severe patients, positive large ES (g: 1.4, 95% C.I: 0.89 to 1.91, I2: 27.6%, p = 0.24), moderate heterogeneity. “slow” <9 years duration (less severe) showed negative medium ES (g: −0.5, 95% C.I: −0.97 to −0.04, I2: 0%, p = 0.93), negligible heterogeneity; >9 years (severe) negative large ES (g: −1.54, 95% C.I: −2.06 to −1.02, I2: 0%, p = 0.37), substantial heterogeneity. Preferred cadence: positive small ES (g: 0.17, 95% C.I: 0.01 to 0.32, I2: 90.5%, p < 0.01), substantial heterogeneity. Acute effect: positive small EF (g: 0.30, 95% C.I: 0.07 to 0.53, I2: 0%, p = 0.45), negligible heterogeneity; Training effect: small negative EF (g: 0.04, 95% C.I: −0.1 to 0.2, I2: 93.6%, p < 0.01), substantial heterogeneity; Training of 30 min: small EF (g: 0.09, 95% C.I: −0.06 to 0.25, I2: 95.5%, p < 0.01), substantial heterogeneity. Weekly frequency: <5 weekly, positive medium ES (g: 0.65, 95% C.I: 0.33 to 0.96, I2: 0%, p = 0.94), negligible heterogeneity. >5 days weekly showed negative small ES (g: −0.22, 95% C.I: −1.16 to 0.71, I2: 23.6%, p > 0.05), negligible heterogeneity. Double limb support time (8 studies): positive medium ES (g: 0.5, 95% C.I: 0.34 to 0.67, I2: 93.46%, p < 0.01), substantial heterogeneity. “fast”-“slow” tempo”: fast shows a positive small ES (g: 0.46, 95% C.I: 0.05 to 0.87, I2: 92.3%, p < 0.01), negligible heterogeneity. Slow shows small positive ES (g: 0.33, 95% C.I: −0.18 to 0.85, I2: 92.8%, p < 0.01), substantial heterogeneity. Preferred cadence: reduction in double limb support phase, medium negative ES (g: −0.56, 95% C.I: −0.9 to −0.22, I2: 0%, p = 0.72), negligible heterogeneity. Turn time (3 studies): In freezers negative large ES (g: −2.08, 95% C.I: −2.5 to −1.66, I2: 93.7%, p < 0.01), substantial heterogeneity. In non-freezers negative large ES (g: −2.3, 95% C.I: −2.71 to −1.88, I2: 87.67%, p < 0.01), substantial heterogeneity. |
| Meta-analysis performed on pooled homogenous studies (CMA V2.0, USA). | |||
| Heterogeneity was assessed using I2 statistics with 0%, 25%, 75% interpreted as negligible, moderate and substantial heterogeneity, respectively | |||
| The ES were adjusted and reported as Hedge’s g interpreted as 0 = no change, 0.2 = small effect, 0.5 = medium effect, 0.8 = large effect, negative effect size = negative change. | |||
| Meta-analysis reports indicating heterogeneity among studies were evaluated to determine the reason of heterogeneity, and the included studies were then pooled separately and analyzed again | |||
| Publication bias was analyzed by plotting a Hedge’s g against standard error p < 0.05 was adopted. | |||
| Rocha et al., 2014 [46] | CONSORT Statement. All of the items were judged as adequate (low risk of bias), inadequate (high risk of bias) or unclear (high risk of bias). | If the data of the variables were continuous, analyses were performed with calculations of the difference of the mean values and the standard deviation. Sub-Group analyses were performed according to the cues used (visual, auditory, sensory, combined and verbal instruction) and the outcomes (step length, cadence, speed, stride length and UPDRS III). | Gait analysis Auditory cues:increased step length (p = 0.03) and speed (p < 0.00001). Auditory cues during overground and treadmill gait compared with no cues: improvements in speed (p = 0.05) and cadence (p = 0.003), but no statistically significant difference for stride length (p = 0.89). Only one study reported significant reduction in freezing episodes after the intervention (p = 0.04) |
| Heterogeneity was assessed in its clinical variations, and statistical methodology according to the principles of the Cochrane Collaboration. There was methodological heterogeneity in respect to the types of cues, but there was no compromise of the meta-analyses presented (≤40%). Statistical heterogeneity was assessed using the test I2 (“0% to 40%: might not be important; 30% to 60%: may represent moderate heterogeneity; 50% to 90%: may represent substantial heterogeneity; 75% to 100%: considerable heterogeneity”). The studies included were highly heterogeneous. Some variables could not be evaluated in all the comparisons because the outcomes were heterogeneous | |||
| All of the included studies were analyzed for risk of bias with a standardized table (Review Manager 5.2—Revman 5.2). | |||
| Spaulding et al., 2013 [26] | Appraisal declared but the used tool was not specified | Quantitative information was collected from each study: means and SDs or other statistical measures of difference before and after cueing, cadence, stride length, and velocity. | Cadence:auditory cueing resulted in a significant increase in cadence (Hedge g: 0.556; 95% CI, 0.291–0.893). Stride length: auditory cueing resulted in a significant improvement (Hedge g: 0.554; 95% CI, 0.072–1.036). Gait velocity:auditory cueing resulted in a significant improvement (Hedge g: 0.544; 95% CI, 0.294–0.795). |
| The data were synthesized using a meta-analysis, with the studies grouped based on cue type. The results from the meta-analysis were displayed in a random effects forest plot. An analysis based on random effects was used. It was chosen Hedge g is an effect size estimate. | |||
| The forest plots also provided statistics regarding the consistencies and strengths of the findings from each study and the overall effect when the results of the various studies were combined. |
| Authors, Year | Conclusions | Limitations |
|---|---|---|
| Cassimatis et al., 2016 [44] | Adding sensory cues to a rehabilitation program resulted in higher levels of improvement in ADL performance measured as UPDRS II | The limited number of studies included in the meta-analysis |
| Statistically significantly larger improvements on average for the UPDRS II were observed in the intervention group compared to the control group after treatment (p = 0.011) | ||
| Pre-post treatment means of UPDRS scores intervention 13.4–10.4 control 14.7–13.5 | ||
| Ghai et al., 2018 [45] | Evidence for positive effects of RAS on spatiotemporal gait parameters in PD patients. | The review attempted to be as comprehensive as possible. It mixes studies with different design, i.e., investigating both training effects and acute effects of RAS. |
| Overall, 88% of studies reported beneficial effects of RAS on gait parameters with significant small-to-large standardized effects: stride length (g: 0.42) gait velocity (g: 0.23), cadence (g: −0.13). | Sometimes difficult to read, some errors in reporting references, numbers of included studies and values of ES do not always match. | |
| Rocha et al., 2014 [46] | The present review corroborates the evidence that cues can promote significant gains in the PD gait, improve psychomotor performance and might reduce freezing episodes. Auditory cues could cause significant improvements in the step length and speed of the gait. Cadence improves with the use of auditory cues compared with interventions without the use of cues and compared to the use of cues (any type) during treadmill gait training versus gait training on the floor without cues. | Different treatment methodology regarding to stimulus intensity. Neither of them has the same number of therapies, distribution of therapies on the week, period of intervention and/or therapy time. |
| Spaulding et al., 2013 [26] | The findings of this meta-analysis infer that auditory forms of cueing are effective in improving important kinematic gait parameters, as cadence, velocity, and stride length. | The number of included studies and sample size were small. There were many different paradigms of cueing within each type, and therefore it is difficult to generalize the information to the rehabilitation setting. The study does not include use of gait assistive devices, which confines our results to people who had milder gait impairments. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Forte, R.; Tocci, N.; De Vito, G. The Impact of Exercise Intervention with Rhythmic Auditory Stimulation to Improve Gait and Mobility in Parkinson Disease: An Umbrella Review. Brain Sci. 2021, 11, 685. https://doi.org/10.3390/brainsci11060685
Forte R, Tocci N, De Vito G. The Impact of Exercise Intervention with Rhythmic Auditory Stimulation to Improve Gait and Mobility in Parkinson Disease: An Umbrella Review. Brain Sciences. 2021; 11(6):685. https://doi.org/10.3390/brainsci11060685
Chicago/Turabian StyleForte, Roberta, Nicoletta Tocci, and Giuseppe De Vito. 2021. "The Impact of Exercise Intervention with Rhythmic Auditory Stimulation to Improve Gait and Mobility in Parkinson Disease: An Umbrella Review" Brain Sciences 11, no. 6: 685. https://doi.org/10.3390/brainsci11060685