Predictive Values of Location and Volumetric MRI Injury Patterns for Neurodevelopmental Outcomes in Hypoxic-Ischemic Encephalopathy Neonates


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subject Selection
Secondary Outcome (Follow-Up at 18–24 Months)
2.2. Imaging Methods
2.3. Image Assessment
2.4. Statistical Analysis
3. Results
3.1. Demographic Characteristics
3.2. MRI NICHD Scoring System for ND Outcome at 18–24 Months
3.3. Total Lesion Count and Size in the Brain MRI in Association with ND Outcome at 18–24 Months
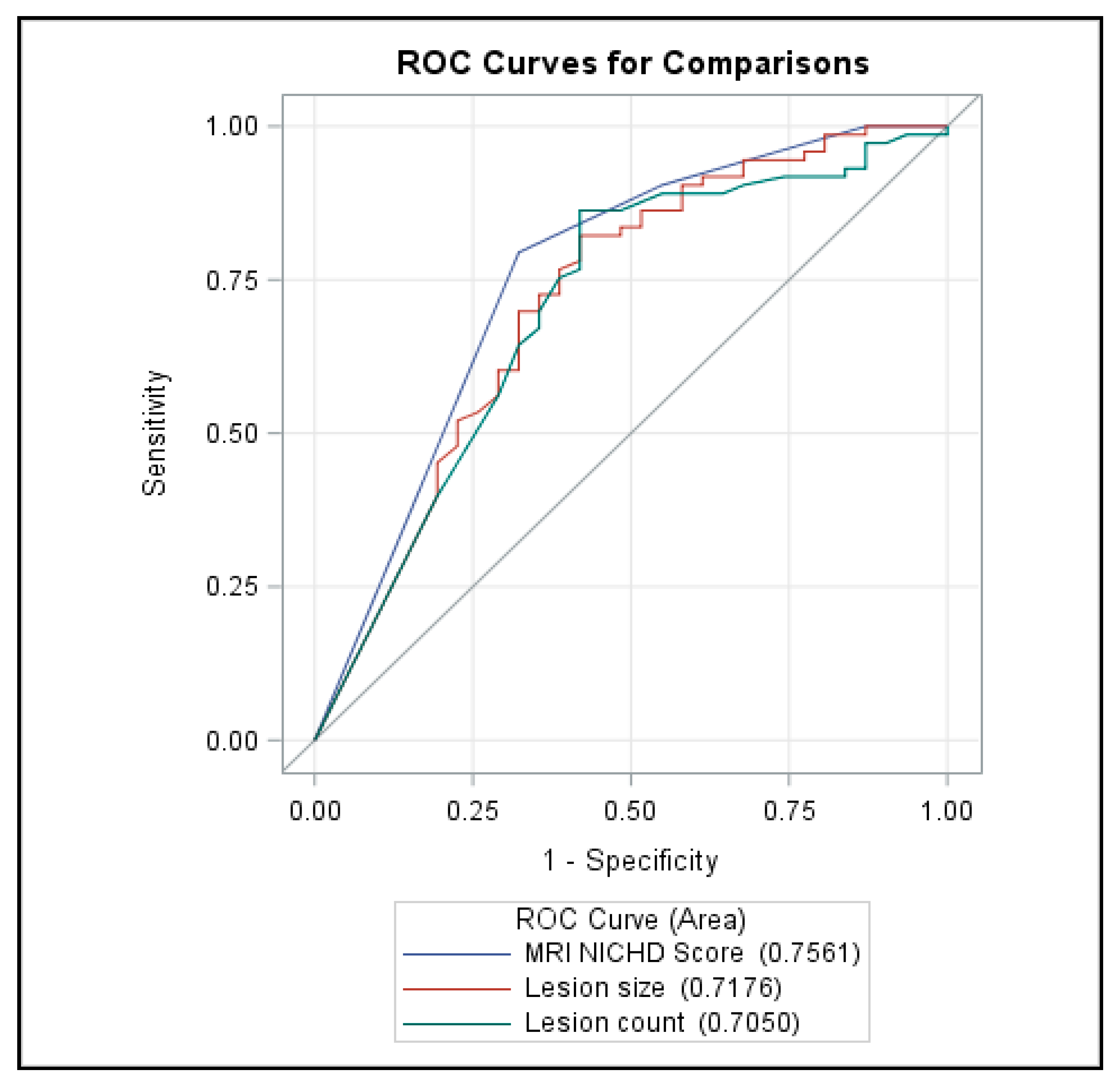
3.4. Receiver Operating Characteristic (ROC) Curve
3.5. Interreader Reliability
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A TH Management for HIE
References
- Finer, N.N.; Robertson, C.M.; Richards, R.T.; Pinnell, L.E.; Peters, K.L. Hypoxic-ischemic encephalopathy in term neonates: Perinatal factors and outcome. J. Pediatr. 1981, 98, 112–117. [Google Scholar] [CrossRef]
- Nelson, K.B. Neonatal encephalopathy: Etiology and outcome. Dev. Med. Child Neurol. 2005, 47, 292. [Google Scholar] [CrossRef]
- Badawi, N.; Felix, J.F.; Kurinczuk, J.J.; Dixon, G.; Watson, L.; Keogh, J.M.; Valentine, J.; Stanley, F.J. Cerebral palsy following term newborn encephalopathy: A population-based study. Dev. Med. Child Neurol. 2005, 47, 293–298. [Google Scholar] [CrossRef]
- Haataja, L.; Mercuri, E.; Guzzetta, A.; Rutherford, M.; Counsell, S.; Frisone, M.F.; Cioni, G.; Cowan, F.; Dubowitz, L. Neurologic examination in infants with hypoxic-ischemic encephalopathy at age 9 to 14 months: Use of optimality scores and correlation with magnetic resonance imaging findings. J. Pediatr. 2001, 138, 332–337. [Google Scholar] [CrossRef]
- Sie, L.T.L.; Van Der Knaap, M.S.; Oosting, J.; De Vries, L.S.; Lafeber, H.N.; Valk, J. MR Patterns of Hypoxic-Ischemic Brain Damage After Prenatal, Perinatal or Postnatal Asphyxia*. Neuropediatrics 2000, 31, 128–136. [Google Scholar] [CrossRef]
- Miller, S.P.; Ramaswamy, V.; Michelson, D.; Barkovich, A.J.; Holshouser, B.; Wycliffe, N.; Glidden, D.V.; Deming, D.; Partridge, J.C.; Wu, Y.W.; et al. Patterns of brain injury in term neonatal encephalopathy. J. Pediatr. 2005, 146, 453–460. [Google Scholar] [CrossRef]
- Azzopardi, D.; Edwards, A.D. Magnetic resonance biomarkers of neuroprotective effects in infants with hypoxic ischemic encephalopathy. Semin. Fetal Neonatal Med. 2010, 15, 261–269. [Google Scholar] [CrossRef]
- Okereafor, A.; Allsop, J.; Counsell, S.J.; Fitzpatrick, J.; Azzopardi, D.; Rutherford, M.A.; Cowan, F.M. Patterns of Brain Injury in Neonates Exposed to Perinatal Sentinel Events. Pediatrics 2008, 121, 906–914. [Google Scholar] [CrossRef]
- Mercuri, E.; Haataja, L.; Guzzetta, A.; Anker, S.; Cowan, F.; Rutherford, M.; Andrew, R.; Braddick, O.; Cioni, G.; Dubowitz, L.; et al. Visual function in term infants with hypoxic-ischaemic insults: Correlation with neurodevelopment at 2 years of age. Arch. Dis. Child.-Fetal Neonatal Ed. 1999, 80, F99–F104. [Google Scholar] [CrossRef] [Green Version]
- Shankaran, S.; Barnes, P.D.; Hintz, S.R.; Laptook, A.R.; Zaterka-Baxter, K.M.; McDonald, S.A.; Ehrenkranz, R.A.; Walsh, M.C.; Tyson, J.E.; Donovan, E.F.; et al. Brain injury following trial of hypothermia for neonatal hypoxic–ischemic encephalopathy. Arch. Dis. Child.-Fetal Neonatal Ed. 2012, 97, F398–F404. [Google Scholar]
- Cowan, F.; Rutherford, M.; Groenendaal, F.; Eken, P.; Mercuri, E.; Bydder, G.M.; Meiners, L.C.; Dubowitz, L.M.S.; De Vries, L.S. Origin and timing of brain lesions in term infants with neonatal encephalopathy. Lancet 2003, 361, 736–742. [Google Scholar] [CrossRef]
- Rutherford, M.J.; Pennock, J.M.; Counsell, S.J.; Mercuri, E.; Cowan, F.; Dubowitz, L.M.S.; Edwards, A.D. Abnormal magnetic resonance signal in the internal capsule predicts poor neurodevelopmental outcome in infants with hypoxic-ischemic encephalopathy. Pediatrics 1998, 102, 323–328. [Google Scholar] [CrossRef] [PubMed]
- Natarajan, G.; Pappas, A.; Shankaran, S. Outcomes in childhood following therapeutic hypothermia for neonatal hypoxic-ischemic encephalopathy (HIE). Semin. Perinatol. 2016, 40, 549–555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shankaran, S.; McDonald, S.A.; Laptook, A.R.; Hintz, S.R.; Barnes, P.D.; Das, A.; Pappas, A.; Higgins, R.D.; Ehrenkranz, R.A.; Goldberg, R.N.; et al. Neonatal Magnetic Resonance Imaging Pattern of Brain Injury as a Biomarker of Childhood Outcomes following a Trial of Hypothermia for Neonatal Hypoxic-Ischemic Encephalopathy. J. Pediatr. 2015, 167, 987–993.e3. [Google Scholar] [CrossRef] [Green Version]
- Rutherford, M.; Ramenghi, L.A.; Edwards, A.D.; Brocklehurst, P.; Halliday, H.; Levene, M.; Strohm, B.; Thoresen, M.; Whitelaw, A.; Azzopardi, D. Assessment of brain tissue injury after moderate hypothermia in neonates with hypoxic–ischaemic encephalopathy: A nested substudy of a randomised controlled trial. Lancet Neurol. 2010, 9, 39–45. [Google Scholar] [CrossRef] [Green Version]
- Lansberg, M.G.; Straka, M.; Kemp, S.; Mlynash, M.; Wechsler, L.R.; Jovin, T.G.; Wilder, M.J.; Lutsep, H.L.; Czartoski, T.J.; Bernstein, R.A.; et al. MRI profile and response to endovascular reperfusion after stroke (DEFUSE 2): A prospective cohort study. Lancet Neurol. 2012, 11, 860–867. [Google Scholar] [CrossRef] [Green Version]
- Rex, P.E.A.B.; Iccarelli, O.L.C.; O’Riordan, J.I.; Ailer, M.I.S.; Hompson, A.L.J.T.; Iller, D.A.H.M. A Longitudinal Study of Abnormalities on MRI and Disability from Multiple Sclerosis. N. Engl. J. Med. 2002, 346, 158–164. [Google Scholar] [CrossRef] [Green Version]
- Scher, M.S. Neonatal seizure classification: A fetal perspective concerning childhood epilepsy. Epilepsy Res. 2006, 70, 41–57. [Google Scholar] [CrossRef]
- Thoresen, M. Patient selection and prognostication with hypothermia treatment. Semin. Fetal Neonatal Med. 2010, 15, 247–252. [Google Scholar] [CrossRef]
- Mercuri, E.; Ricci, D.; Cowan, F.; Lessing, D.; Frisone, M.F.; Haataja, L.; Counsell, S.; Dubowitz, L.M.; Rutherford, M.A. Head growth in infants with hypoxic-ischemic encephalopathy: Correlation with neonatal magnetic resonance imaging. Pediatrics 2000, 106, 235–243. [Google Scholar] [CrossRef]
- Parikh, N.A.; Lasky, R.E.; Garza, C.N.; Bonfante-Mejia, E.; Shankaran, S.; Tyson, J.E. Volumetric and anatomical MRI for hypoxic–ischemic encephalopathy: Relationship to hypothermia therapy and neurosensory impairments. J. Perinatol. 2008, 29, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Barnett, A.; Mercuri, E.; Rutherford, M.J.; Haataja, L.; Frisone, M.F.; Henderson, S.; Cowan, F.; Dubowitz, L. Neurological and Perceptual-Motor Outcome at 5–6 Years of Age in Children with Neonatal Encephalopathy: Relationship with Neonatal Brain MRI. Neuropediatrics 2002, 33, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Mulkey, S.B.; Ramakrishnaiah, R.H.; McKinstry, R.C.; Chang, T.; Mathur, A.M.; Mayock, D.E.; Van Meurs, K.; Schaefer, G.B.; Luo, C.; Bai, S.; et al. Erythropoietin and Brain Magnetic Resonance Imaging Findings in Hypoxic-Ischemic Encephalopathy: Volume of Acute Brain Injury and 1-Year Neurodevelopmental Outcome. J. Pediatr. 2017, 186, 196–199. [Google Scholar] [CrossRef] [PubMed]
- Markus, R.; Reutens, D.C.; Kazui, S.; Read, S.J.; Wright, P.; Pearce, D.C.; Tochon-Danguy, H.J.; Sachinidis, J.I.; Donnan, G.A. Hypoxic tissue in ischaemic stroke: Persistence and clinical consequences of spontaneous survival. Brain 2004, 127, 1427–1436. [Google Scholar] [CrossRef] [Green Version]
- Andronikou, S.; Simpson, E.; Klemm, M.; Vedajallam, S.; Chacko, A.; Thai, N.J. Technical report: 3D printing of the brain for use as a visual-aid tool to communicate MR imaging features of hypoxic ischaemic injury at term with non-physicians. Child’s Nerv. Syst. 2018, 34, 1573–1577. [Google Scholar] [CrossRef] [Green Version]
- Gluckman, P.D.; Wyatt, J.S.; Azzopardi, D.; Ballard, R.; Edwards, A.D.; Ferriero, D.M.; Polin, R.A.; Robertson, C.M.; Theoresen, M.; Whitelaw, A.; et al. Selective head cooling with mild systemic hypothermia after neonatal encephalopathy: Multicentre randomised trial. Lancet 2005, 365, 663–670. [Google Scholar] [CrossRef]
- Azzopardi, D.; Strohm, B.; Edwards, A.D.; Dyet, L.; Halliday, H.L.; Juszczak, E.; Kapellou, O.; Levene, M.; Marlow, N.; Porter, E.; et al. Moderate Hypothermia to Treat Perinatal Asphyxial Encephalopathy. N. Engl. J. Med. 2009, 361, 1349–1358. [Google Scholar] [CrossRef] [Green Version]
- Sarnat, H.B. Neonatal Encephalopathy Following Fetal Distress. Arch. Neurol. 1976, 33, 696–705. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Normal Neurodevelopment (n = 76) | Abnormal Neurodevelopment (n = 31) | p-Value | |
|---|---|---|---|
| Gestational age, weeks | 39.9 (38.8~40.2) | 39.3 (38.2~40.0) | 0.072 |
| Birth weight, g | 3230 (3030~3510) | 3200 (2955~3370) | 0.153 |
| Delivery mode, emergent C/S | 22 (26.5) | 9 (25.7) | 0.113 |
| Apgar score at 1 min | 4.90 (2.39) | 4.69 (2.03) | 0.638 |
| Apgar score at 5 min | 6.81 (2.01) | 6.71 (1.87) | 0.815 |
| Male, n (%) | 35 (42.2) | 11 (31.4) | 0.376 |
| Sarnat Stage 1, mild | 11 (14.5) | 0 (0) | 0.471 |
| Sarnat Stage 2, moderate | 54 (71.0) | 26 (83.9) | |
| Sarnat Stage 3, severe | 11 (14.5) | 5 (16.1) | |
| Clinical seizure | 55 (73.3) | 31 (96.9) | 0.011 |
| Ventilator care, days | 3.86 (4.82) | 3.66 (2.06) | 0.822 |
| Full feeding (100 cc/kg/day) | 8.53 (5.28) | 8.18 (3.14) | 0.724 |
| Hospital days | 13.80 (7.62) | 13.54 (4.82) | 0.857 |
| Early intervention | 22 (28.9) | 20 (64.5) | 0.002 |
| MRI NICHD Score, n (%) | Normal Neurodevelopment (n = 76) | Abnormal Neurodevelopment (n = 31) | p-Value |
|---|---|---|---|
| 0 | 30 (39.47) | 5 (16.13) | <0.001 |
| 1A | 31 (40.79) | 5 (16.13) | <0.001 |
| 1B | 8 (10.53) | 7 (22.58) | <0.001 |
| 2A | 7 (9.21) | 10 (32.26) | <0.001 |
| 2B | 0 (0) | 4 (12.90) | <0.001 |
| 3 | 0 (0) | 0 (0) | NA |
| Brain MRI | Normal ND (n = 76) | Abnormal ND (n = 31) | p-Value |
|---|---|---|---|
| size (mean (SD)) | 91.25 (179.63) | 384.77 (527.18) | <0.001 |
| lesion size < 100 | 59 (77.6) | 12 (38.7) | <0.001 |
| lesion size 100–200 | 5 (6.8) | 3 (9.7) | 0.926 |
| lesion size 200–500 | 8 (11) | 7 (22.6) | 0.216 |
| lesion n size > 500 | 4 (5.5) | 9 (29) | <0.001 |
| Total lesion count (mean (SD)) | 5.29 (9.29) | 14.16 (12.49) | <0.001 |
| counts < 2 | 44 (57.9) | 9 (29.03) | 0.0113 |
| count between 2–14 | 22 (30.14) | 4 (12.90) | 0.0634 |
| count between 14–40 | 9 (12) | 16 (51) | <0.001 |
| count > 40 | 1 (1.37) | 2 (6.45) | 0.1567 |
| Number of lesions with volume size between 0–100 (mean (SD)) | 5.29 (9.29) | 14.16 (12.49) | <0.001 |
| between 100–200 (mean (SD)) | 0.18 (0.54) | 0.52(0.81) | 0.014 |
| between 200–500 (mean (SD)) | 0.07 (0.38) | 0.10 (0.40) | 0.735 |
| above 500 (mean (SD)) | 0.00 (0.00) | 0.06 (0.25) | 0.028 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, P.D.; Chow, D.S.; Alber, A.; Lin, Y.-K.; Youn, Y.A. Predictive Values of Location and Volumetric MRI Injury Patterns for Neurodevelopmental Outcomes in Hypoxic-Ischemic Encephalopathy Neonates. Brain Sci. 2020, 10, 991. https://doi.org/10.3390/brainsci10120991
Chang PD, Chow DS, Alber A, Lin Y-K, Youn YA. Predictive Values of Location and Volumetric MRI Injury Patterns for Neurodevelopmental Outcomes in Hypoxic-Ischemic Encephalopathy Neonates. Brain Sciences. 2020; 10(12):991. https://doi.org/10.3390/brainsci10120991
Chicago/Turabian StyleChang, Peter D., Daniel S. Chow, Anna Alber, Yen-Kuang Lin, and Young Ah Youn. 2020. "Predictive Values of Location and Volumetric MRI Injury Patterns for Neurodevelopmental Outcomes in Hypoxic-Ischemic Encephalopathy Neonates" Brain Sciences 10, no. 12: 991. https://doi.org/10.3390/brainsci10120991