Midday Napping and Successful Aging in Older People Living in the Mediterranean Region: The Epidemiological Mediterranean Islands Study (MEDIS)

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Bioethics
2.2. Measurements
2.2.1. Sociodemographic and Lifestyle Characteristics
2.2.2. Physical Activity Levels Physical
2.2.3. Anthropometric and Clinical Characteristics
2.2.4. Cognitive Function Assessment Cognitive
2.2.5. Dietary Habits Assessment
2.2.6. Successful Aging Index
2.3. Statistical Analysis
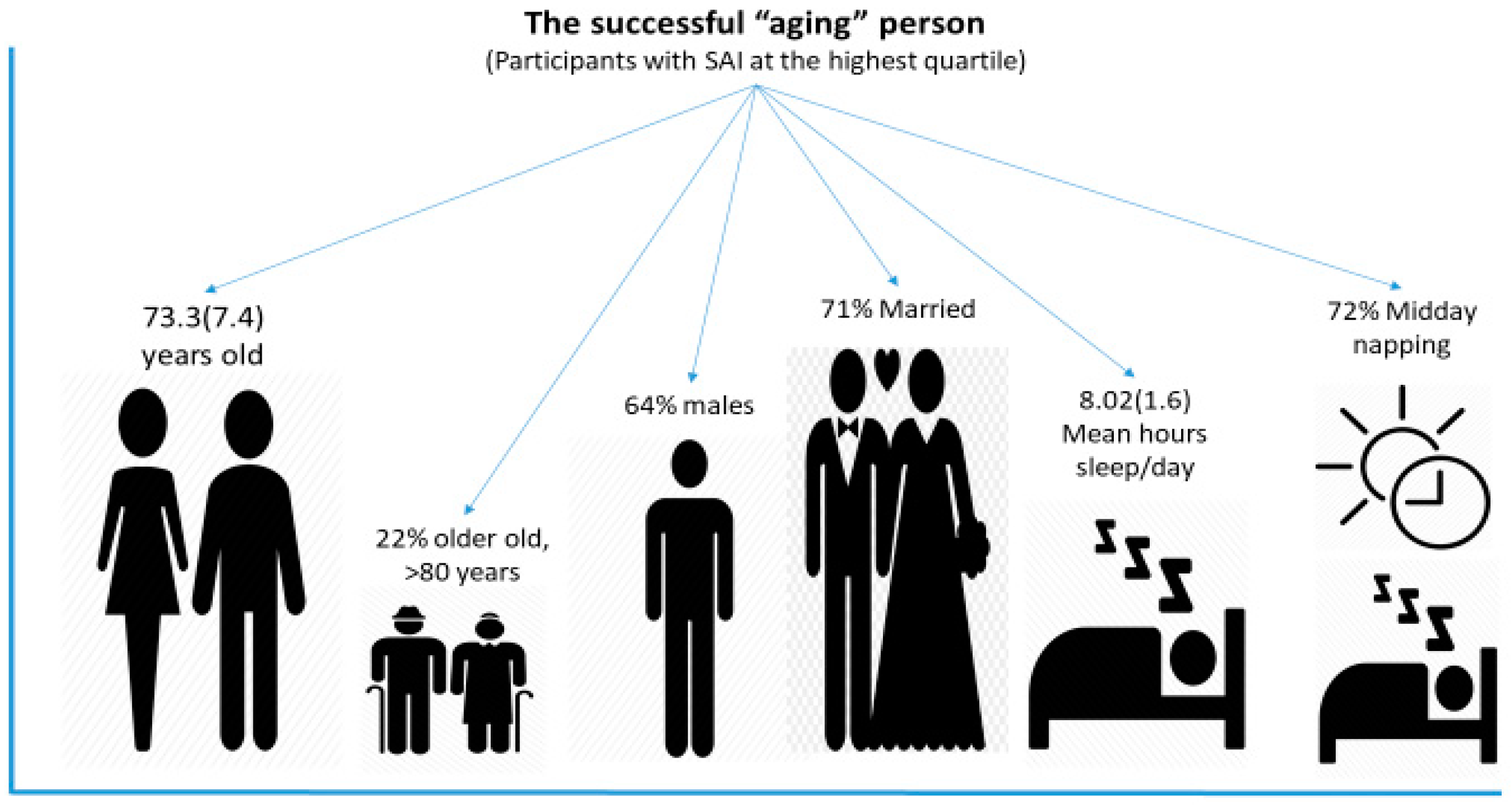
3. Results
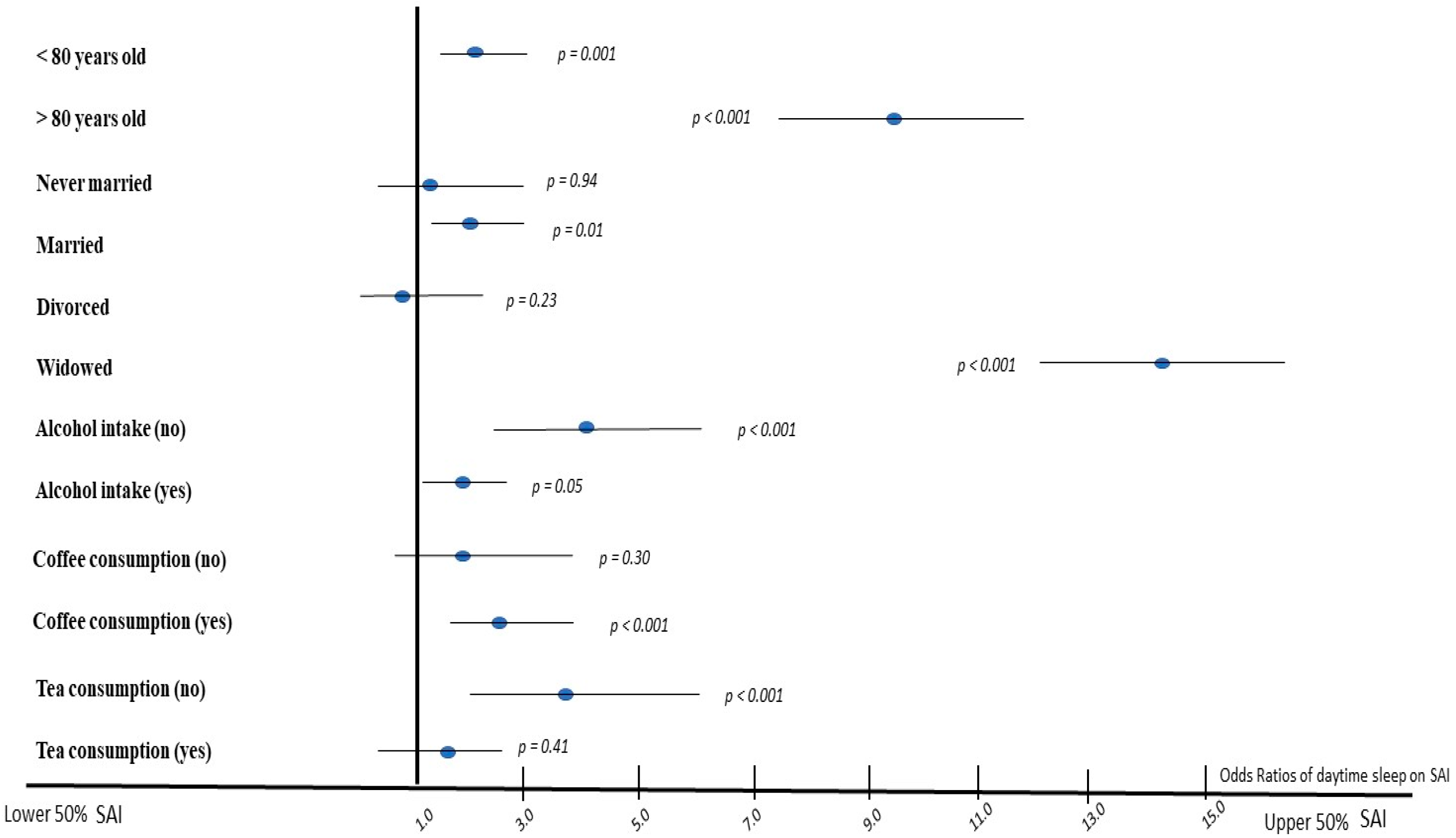
3.1. Midday Napping and Successful Aging
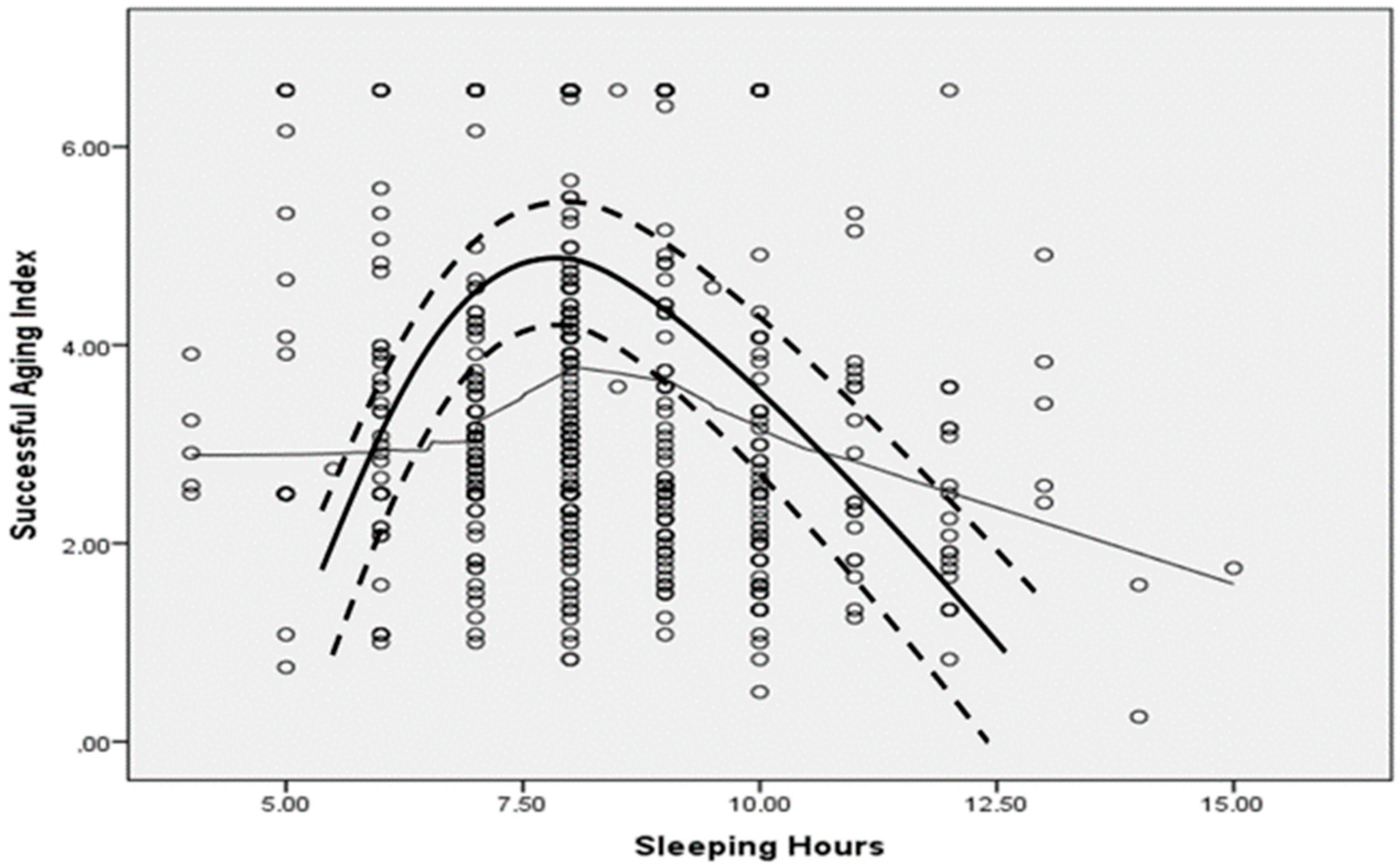
3.2. Sleeping Hours and Successful Aging
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Larcher, S.; Benhamou, P.-Y.; Pépin, J.-L.; Borel, A.-L. Sleep habits and diabetes. Diabetes Metab. 2015, 41, 263–271. [Google Scholar] [CrossRef]
- Wang, D.; Li, W.; Cui, X.; Meng, Y.; Zhou, M.; Xiao, L. Sleep duration and risk of coronary heart disease: A systematic review and meta-analysis of prospective cohort studies. Int. J. Cardiol. 2016, 219, 231–239. [Google Scholar] [CrossRef] [PubMed]
- Ogilvie, R.P.; Patel, S.R. The epidemiology of sleep and obesity. Sleep Health 2017, 3, 383–388. [Google Scholar] [CrossRef] [PubMed]
- Zhai, L.; Zhang, H.; Zhang, D. Sleep duration and depression among adults: A meta-analysis of prospective studies. Depress. Anxiety 2015, 32, 664–670. [Google Scholar] [CrossRef] [PubMed]
- Altena, E.; Chen, I.Y.; Daviaux, Y.; Ivers, H.; Philip, P.; Morin, C.M. How Hyperarousal and Sleep Reactivity Are Represented in Different Adult Age Groups: Results from a Large Cohort Study on Insomnia. Brain Sci. 2017, 7, 41. [Google Scholar] [CrossRef] [Green Version]
- Georgousopoulou, E.N.; Naumovski, N.; Mellor, D.D.; Tyrovolas, S.; Piscopo, S.; Valacchi, G. Association between Siesta (Daytime Sleep), Dietary Patterns and the Presence of Metabolic Syndrome in Elderly Living in Mediterranean Area (Medis Study): The Moderating Effect of Gender. J. Nutr. Health Aging 2017, 21, 1118–1124. [Google Scholar] [CrossRef] [Green Version]
- Dhand, R.; Sohal, H. Good sleep, bad sleep! The role of daytime naps in healthy adults. Curr. Opin. Pulm. Med. 2006, 12, 379–382. [Google Scholar] [CrossRef]
- Martin, P.; Kelly, N.; Kahana, B.; Kahana, E.; Willcox, B.J.; Willcox, D.C. Defining successful aging: A tangible or elusive concept? Gerontologist 2015, 55, 14–25. [Google Scholar] [CrossRef]
- Tyrovolas, S.; Polychronopoulos, E.; Morena, M.; Mariolis, A.; Piscopo, S.; Valacchi, G. Is car use related with successful aging of older adults? Results from the multinational Mediterranean islands study. Ann. Epidemiol. 2017, 27, 225–229. [Google Scholar] [CrossRef]
- Tyrovolas, S.; Haro, J.M.; Foscolou, A.; Tyrovola, D.; Mariolis, A.; Bountziouka, V. Anti-Inflammatory Nutrition and Successful Ageing in Elderly Individuals: The Multinational MEDIS Study. Gerontology 2018, 64, 3–10. [Google Scholar] [CrossRef]
- Foscolou, A.; Koloverou, E.; Matalas, A.-L.; Tyrovolas, S.; Chrysohoou, C.; Sidossis, L. Decomposition of Mediterranean Dietary Pattern on Successful Aging, Among Older Adults: A Combined Analysis of Two Epidemiological Studies. J. Aging Health 2019, 31, 1549–1567. [Google Scholar] [CrossRef] [PubMed]
- Foscolou, A.; Critselis, E.; Tyrovolas, S.; Chrysohoou, C.; Sidossis, L.S.; Naumovski, N. The Effect of Exclusive Olive Oil Consumption on Successful Aging: A Combined Analysis of the ATTICA and MEDIS Epidemiological Studies. Foods 2019, 8, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Booth, F.W.; Roberts, C.K.; Laye, M.J. Lack of exercise is a major cause of chronic diseases. Compr. Physiol. 2012, 2, 1143–1211. [Google Scholar] [PubMed] [Green Version]
- Tyrovolas, S.; Haro, J.M.; Mariolis, A.; Piscopo, S.; Valacchi, G.; Tsakountakis, N. Successful aging, dietary habits and health status of elderly individuals: A k-dimensional approach within the multi-national MEDIS study. Exp. Gerontol. 2014, 60, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Bursztyn, M.; Ginsberg, G.; Stessman, J. The siesta and mortality in the elderly: Effect of rest without sleep and daytime sleep duration. Sleep 2002, 25, 187–191. [Google Scholar] [CrossRef] [PubMed]
- Papathanasiou, G.; Georgoudis, G.; Papandreou, M.; Spyropoulos, P.; Georgakopoulos, D.; Kalfakakou, V. Reliability measures of the short International Physical Activity Questionnaire (IPAQ) in Greek young adults. Hell. J. Cardiol. 2009, 50, 283–294. [Google Scholar]
- Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA 2001, 285, 2486–2497. [Google Scholar] [CrossRef]
- Crum, R.M.; Anthony, J.C.; Bassett, S.S.; Folstein, M.F. Population-based norms for the Mini-Mental State Examination by age and education level. JAMA 1993, 269, 2386–2391. [Google Scholar] [CrossRef]
- Solias, A.; Skapinakis, P.; Degleris, N.; Pantoleon, M.; Katirtzoglou, E.; Politis, A. [Mini Mental State Examination (MMSE): Determination of cutoff scores according to age and educational level]. Psychiatriki 2014, 25, 245–256. [Google Scholar]
- Tyrovolas, S.; Pounis, G.; Bountziouka, V.; Polychronopoulos, E.; Panagiotakos, D.B. Repeatability and validation of a short, semi-quantitative food frequency questionnaire designed for older adults living in Mediterranean areas: The MEDIS-FFQ. J. Nutr. Elder. 2010, 29, 311–324. [Google Scholar] [CrossRef]
- Panagiotakos, D.B.; Pitsavos, C.; Stefanadis, C. Dietary patterns: A Mediterranean diet score and its relation to clinical and biological markers of cardiovascular disease risk. Nutr. Metab. Cardiovasc. Dis. 2006, 16, 559–568. [Google Scholar] [CrossRef] [PubMed]
- Tourlouki, E.; Matalas, A.-L.; Bountziouka, V.; Tyrovolas, S.; Zeimbekis, A.; Gotsis, E. Are current dietary habits in Mediterranean islands a reflection of the past? Results from the MEDIS study. Ecol. Food Nutr. 2013, 52, 371–386. [Google Scholar] [CrossRef] [PubMed]
- Maxfield, A.; Patil, S.; Cunningham, S.A. Globalization and Food Prestige among Indian Adolescents. Ecol. Food Nutr. 2016, 55, 341–364. [Google Scholar] [CrossRef] [PubMed]
- Mamalaki, E.; Anastasiou, C.A.; Ntanasi, E.; Tsapanou, A.; Kosmidis, M.H.; Dardiotis, E. Associations between the mediterranean diet and sleep in older adults: Results from the hellenic longitudinal investigation of aging and diet study. Geriatr. Gerontol. Int. 2018, 18, 1543–1548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Driscoll, H.C.; Serody, L.; Patrick, S.; Maurer, J.; Bensasi, S.; Houck, P.R.; Mazumdar, S.; Nofzinger, E.A.; Bell, B.; Nebes, R.D.; et al. Sleeping well, aging well: A descriptive and cross-sectional study of sleep in “successful agers” 75 and older. Am. J. Geriatr. Psychiatry 2008, 16, 74–82. [Google Scholar] [CrossRef] [Green Version]
- Luca, G.; Rubio, J.H.; Andries, D.; Tobback, N.; Vollenweider, P.; Waeber, G. Age and gender variations of sleep in subjects without sleep disorders. Ann. Med. 2015, 47, 482–491. [Google Scholar] [CrossRef]
- Mong, J.A.; Cusmano, D.M. Sex differences in sleep: Impact of biological sex and sex steroids. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2016, 371, 201501110. [Google Scholar] [CrossRef]
- Madrid-Valero, J.J.; Martínez-Selva, J.M.; Ribeiro do Couto, B.; Sánchez-Romera, J.F.; Ordoñana, J.R. Age and gender effects on the prevalence of poor sleep quality in the adult population. Gac. Sanit. 2017, 31, 18–22. [Google Scholar] [CrossRef] [Green Version]
- von Bonsdorff, M.B.; Strandberg, A.; von Bonsdorff, M.; Törmäkangas, T.; Pitkälä, K.H.; Strandberg, T.E. Working hours and sleep duration in midlife as determinants of health-related quality of life among older businessmen. Age Ageing 2017, 46, 108–112. [Google Scholar] [CrossRef] [Green Version]
- Carlson, M. Almost half of Americans Want the Bed to Themselves. 2018. Available online: https://www.mattressclarity.com/news/half-of-americans-want-bed-to-themselves/ (accessed on 12 December 2019).
- Strawbridge, W.J.; Shema, S.J.; Roberts, R.E. Impact of spouses’ sleep problems on partners. Sleep 2004, 27, 527–531. [Google Scholar] [CrossRef] [Green Version]
- Cooper, J.M.; Halter, K.A.; Prosser, R.A. Circadian rhythm and sleep-wake systems share the dynamic extracellular synaptic milieu. Neurobiol. Sleep Circadian Rhythm. 2018, 5, 15–36. [Google Scholar] [CrossRef] [PubMed]
- Clark, I.; Landolt, H.P. Coffee, caffeine, and sleep: A systematic review of epidemiological studies and randomized controlled trials. Sleep Med. Rev. 2017, 31, 70–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gooneratne, N.S.; Vitiello, M.V. Sleep in older adults: Normative changes, sleep disorders, and treatment options. Clin. Gertiatr. Med. 2014, 30, 591–627. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Callaghan, F.; Muurlink, O.; Reid, N. Effects of caffeine on sleep quality and daytime functioning. Risk Manag. Healthc Policy 2018, 11, 263–271. [Google Scholar] [CrossRef] [Green Version]
- Spadola, C.E.; Guo, N.; Johnson, D.A.; Sofer, T.; Bertisch, S.M.; Jackson, C.L.; Rueschman, M.; Mittleman, M.A.; Wilson, J.G.; Redline, S. Evening intake of alcohol, caffeine, and nicotine: Night-to-night associations with sleep duration and continuity among African Americans in the Jackson Heart Sleep Study. Sleep 2019, 42, 11. [Google Scholar] [CrossRef]
- Naumovski, N.; Foscolou, A.; D’Cunha, N.; Tyrovolas, S.; Chrysohoou, C.; Sidossis, L.S.; Rallidis, L.; Matalas, A.L.; Polychronopoulos, E.; Pitsavos, C.; et al. The association between green and black tea consumption on successful aging: A combined analysis of the ATTICA and MEDiterranean Islands (MEDIS) epidemiological studies. Molecules 2019, 24, 1862. [Google Scholar] [CrossRef] [Green Version]
- Hirshkowitz, M.; Whiton, K.; Albert, S.M.; Alessi, C.; Bruni, O.; DonCarlos, L. National Sleep Foundation’s sleep time duration recommendations: Methodology and results summary. Sleep Health 2015, 1, 40–43. [Google Scholar] [CrossRef]
- Liu, H.; Byles, J.E.; Xu, X.; Zhang, M.; Wu, X.; Hall, J.J. Association between nighttime sleep and successful aging among older Chinese people. Sleep Med. 2016, 22, 18–24. [Google Scholar] [CrossRef]
- Chaput, J.P.; Dutil, C.; Sampasa-Kanyinga, H. Sleeping hours: What is the ideal number and how does age impact this? Nat. Sci. Sleep 2018, 10, 421–430. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.C.; Espeland, M.A.; Brunner, R.L.; Lovato, L.C.; Wallace, R.B.; Leng, X.; Phillips, L.S.; Robinson, J.G.; Kotchen, J.M.; Johnson, K.C.; et al. Sleep duration, cognitive decline, and dementia risk in older women. Alzheimers Dement. 2016, 12, 21–33. [Google Scholar] [CrossRef]
- Rodriguez, J.C.; Dzierzewski, J.M.; Alessi, C.A. Sleep problems in the elderly. Med. Clin. N. Am. 2015, 99, 431–439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bazargan, M.; Mian, N.; Cobb, S.; Vargas, R.; Assari, S. Insomnia Symptoms among African-American Older Adults in Economically Disadvantaged Areas of South Los Angeles. Brain Sci. 2019, 9, 306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, Y.; Yu, B.Y.-M.; Liu, Y.; Liu, Y. Meta-Analysis of the Effect of Obstructive Sleep Apnea on Cardiovascular Events After Percutaneous Coronary Intervention. Am. J. Cardiol. 2017, 120, 1026–1030. [Google Scholar] [CrossRef] [PubMed]
- Lewis, O.; Odeyemi, Y.; Joseph, V.; Mehari, A.; Gillum, R.F. Screen Hours and Sleep Symptoms: The US National Health and Nutrition Examination Survey. Fam. Community Health 2017, 40, 231–235. [Google Scholar] [CrossRef] [PubMed]
- Schechter, A.; Kim, E.W.; St-Onge, M.P.; Westwood, A.J. Blocking nocturnal blue light for insomnia: A randomized controlled trial. J. Psychiatr. Res. 2018, 96, 196–202. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Non-Midday Nappers | Midday Nappers | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| All | Females | Males | All | Females | Males | p | p1 | p2 | |
| Males n (%) | 318 (47) | - | - | 1065 (56) | - | - | 0.02 | - | - |
| Age (years) | 72 ± 6.7 | 72 ± 6.3 | 73 ± 7.1 | 73 ± 7.3 | 73 ± 7.1 | 74 ± 7.5 | 0.37 | 0.48 | 0.69 |
| Smoking, %yes | 20 | 8 | 34 | 17 | 5 | 26 | 0.27 | 0.26 | 0.12 |
| Physically active, %active | 26 | 21 | 31 | 18 | 14 | 21 | 0.01 | 0.09 | 0.04 |
| BMI (kg/m2) | 28 ± 4.5 | 28 ± 5.3 | 28 ± 3.5 | 28 ± 4.2 | 29 ± 4.7 | 28 ± 3.8 | 0.72 | 0.24 | 0.59 |
| Coffee intake, %yes | 87 | 86 | 88 | 88 | 84 | 91 | 0.63 | 0.70 | 0.36 |
| Tea intake %yes | 43 | 53 | 32 | 57 | 59 | 54 | 0.001 | 0.25 | <0.001 |
| Alcohol intake %yes | 44 | 17 | 75 | 44 | 17 | 65 | 0.95 | 0.97 | 0.06 |
| MedDietScore (0–55) | 32 ± 5.0 | 32 ± 5.1 | 34 ± 4.5 | 34 ± 4.0 | 34 ± 3.8 | 34 ± 4.1 | 0.02 | 0.002 | 0.94 |
| Hypertension, %yes | 55 | 55 | 55 | 65 | 71 | 59 | 0.002 | 0.01 | 0.04 |
| Diabetes, %yes | 21 | 18 | 23 | 26 | 25 | 26 | 0.14 | 0.13 | 0.59 |
| Hypercholesterolemia, %yes | 50 | 51 | 48 | 45 | 47 | 44 | 0.28 | 0.48 | 0.47 |
| MMSE (0–30) | 24 ± 4 | 24 ± 4 | 25 ± 4 | 24 ± 4 | 24 ± 3 | 25 ± 4 | 0.97 | 0.43 | 0.72 |
| SAI (0–10) | 2.9 ± 1.3 | 2.5 ± 1.3 | 3.3 ± 1.3 | 3.5 ± 1.9 | 3.2 ± 2.1 | 3.8 ± 1.8 | 0.001 | 0.01 | 0.01 |
| b ± SE For Midday Napping (Yes/No) | 95% CI | p | |
|---|---|---|---|
| Model 1: Age | 0.577 ± 0.142 | 0.298–0.856 | <0.001 |
| Model 2: Model 1 + sex | 0.519 ± 0.140 | 0.244–0.795 | <0.001 |
| Model 3: Model 2 + smoking | 0.515 ± 0.141 | 0.238–0.792 | <0.001 |
| Model 4: Model 3 + coffee consumption | 0.521 ± 0.141 | 0.244–0.797 | <0.001 |
| Model 5: Model 4 + tea consumption | 0.667 ± 0.137 | 0.398–0.936 | <0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Foscolou, A.; D’Cunha, N.M.; Naumovski, N.; Tyrovolas, S.; Rallidis, L.; Matalas, A.-L.; Polychronopoulos, E.; Sidossis, L.S.; Panagiotakos, D. Midday Napping and Successful Aging in Older People Living in the Mediterranean Region: The Epidemiological Mediterranean Islands Study (MEDIS). Brain Sci. 2020, 10, 14. https://doi.org/10.3390/brainsci10010014
Foscolou A, D’Cunha NM, Naumovski N, Tyrovolas S, Rallidis L, Matalas A-L, Polychronopoulos E, Sidossis LS, Panagiotakos D. Midday Napping and Successful Aging in Older People Living in the Mediterranean Region: The Epidemiological Mediterranean Islands Study (MEDIS). Brain Sciences. 2020; 10(1):14. https://doi.org/10.3390/brainsci10010014
Chicago/Turabian StyleFoscolou, Alexandra, Nathan M. D’Cunha, Nenad Naumovski, Stefanos Tyrovolas, Loukianos Rallidis, Antonia-Leda Matalas, Evangelos Polychronopoulos, Labros S. Sidossis, and Demosthenes Panagiotakos. 2020. "Midday Napping and Successful Aging in Older People Living in the Mediterranean Region: The Epidemiological Mediterranean Islands Study (MEDIS)" Brain Sciences 10, no. 1: 14. https://doi.org/10.3390/brainsci10010014