Emerging Biosensing Technologies towards Early Sepsis Diagnosis and Management

 , ,
, ,  , and
, and 
Abstract
:1. Introduction
2. Pathogens, Biomarkers, and Conventional Diagnostic Techniques
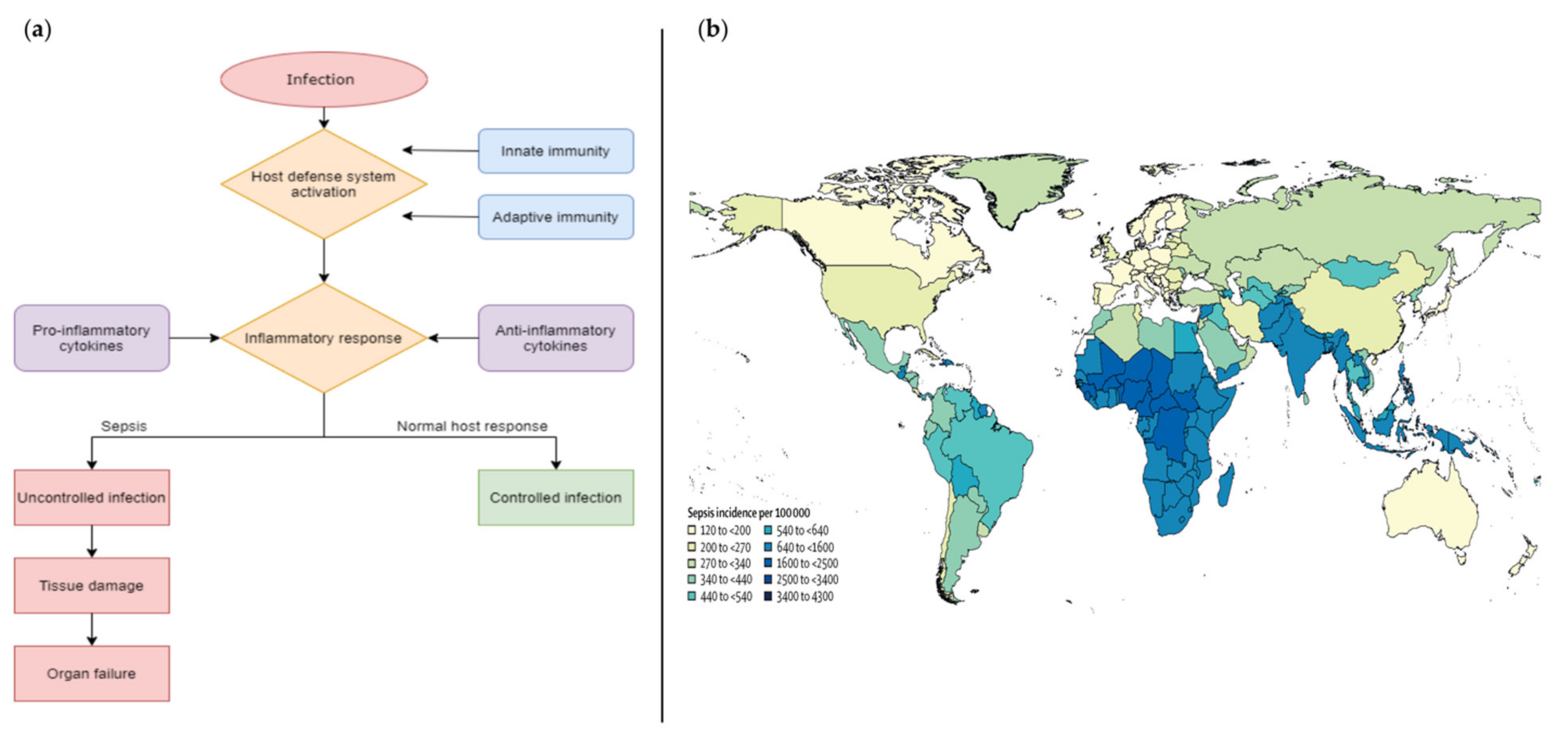
2.1. Pathogens
2.2. Biomarkers
2.2.1. C-Reactive Protein (CRP)
2.2.2. Procalcitonin (PCT)
2.2.3. Lipopolysaccharide Binding Protein (LPB)
2.2.4. D-Dimer (DD)
2.2.5. Interleukins (ILs) and Other Cytokines
2.2.6. Surface Markers of Circulating Leukocytes
2.2.7. Fibronectin (FN)
2.2.8. Lactate Dehydrogenase (LDH)
2.2.9. MicroRNAs (miRNAs)
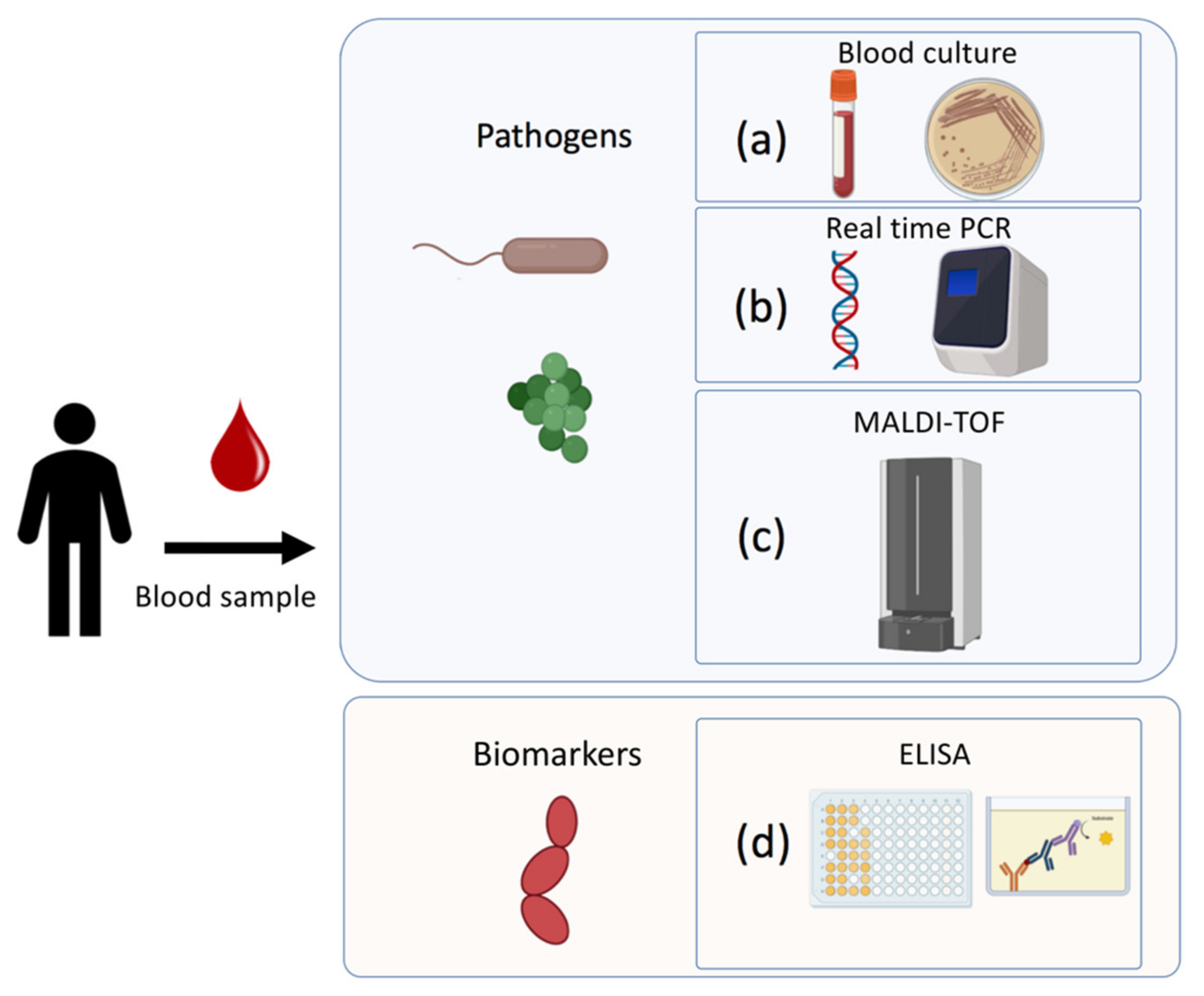
2.3. Traditional Laboratory Techniques
2.3.1. Blood Cultures (BCs)
2.3.2. Molecular Methods
Nucleic Acid Amplification-Based Techniques
Matrix-Assisted Laser Desorption/Ionization Time-of-Flight Mass Spectrometry (MALDI-TOF)
2.3.3. Serological Methods
3. Biosensor as an Alternative Device for Sepsis
3.1. Electrochemical Biosensors
3.1.1. Procalcitonin (PCT), C-Reactive Protein (CRP) Detection
3.1.2. Cytokines
3.1.3. Pathogens
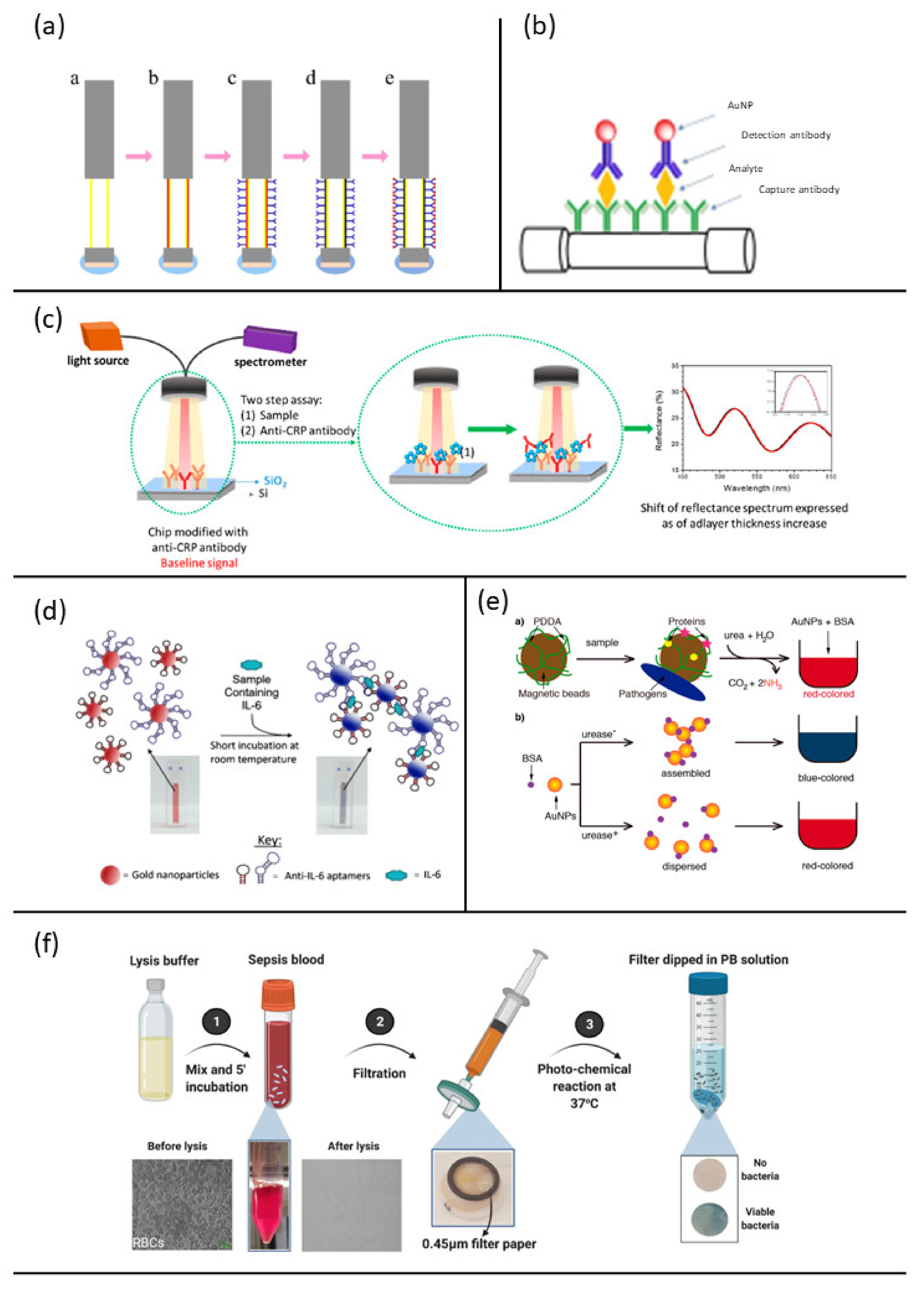
3.2. Optical Biosensors
3.2.1. Procalcitonin (PCT), C-Reactive Protein (CRP) Detection and Interleukins
3.2.2. Pathogens
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Singer, M.; Deutschman, C.S.; Seymour, C.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- O’Brien, J.M.; Ali, N.A.; Aberegg, S.K.; Abraham, E. Sepsis. Am. J. Med. 2007, 120, 1012–1022. [Google Scholar] [CrossRef]
- World Health Organization. Sepsis. Available online: https://www.who.int/news-room/fact-sheets/detail/sepsis (accessed on 23 July 2022).
- Paoli, C.J.; Reynolds, M.A.; Sinha, M.; Gitlin, M.; Crouser, E. Epidemiology and Costs of Sepsis in the United States—An Analysis Based on Timing of Diagnosis and Severity Level. Crit. Care Med. 2018, 46, 1889. [Google Scholar] [CrossRef]
- Abbas, A.K.; Lichtman, A.H.; Pillai, S. Cellular and Molecular Immunology; Elsevier Health Sciences: Philadelphia, PA, USA, 2014; ISBN 9780323757508. [Google Scholar]
- Braunwald, E.; Fauci, A.S.; Hauser, S.L.; Longo, D.L.; Jameson, J.L. Harrison’s Principles of Internal Medicine; McGraw-Hill Companies, Inc.: New York, NY, USA, 2005. [Google Scholar]
- Minasyan, H. Sepsis and Septic Shock: Pathogenesis and Treatment Perspectives. J. Crit. Care 2017, 40, 229–242. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention; National Center for Emerging and Zoonotic Infectious Diseases (NCEZID); Division of Healthcare Quality Promotion (DHQP). What Is Sepsis? Available online: https://www.cdc.gov/sepsis/what-is-sepsis.html (accessed on 23 July 2022).
- Rudd, K.E.; Johnson, S.C.; Agesa, K.M.; Shackelford, K.A.; Tsoi, D.; Kievlan, D.R.; Colombara, D.V.; Ikuta, K.S.; Kissoon, N.; Finfer, S.; et al. Global, Regional, and National Sepsis Incidence and Mortality, 1990–2017: Analysis for the Global Burden of Disease Study. Lancet 2020, 395, 200–211. [Google Scholar] [CrossRef] [Green Version]
- Levy, M.M.; Evans, L.E.; Rhodes, A. The Surviving Sepsis Campaign Bundle: 2018 Update. Intensive Care Med. 2018, 44, 925–928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, S.; Tripathy, S.; Jyoti, A.; Singh, S.G. Recent Advances in Biosensors for Diagnosis and Detection of Sepsis: A Comprehensive Review. Biosens. Bioelectron. 2019, 124–125, 205–215. [Google Scholar] [CrossRef]
- Reddy, B.; Hassan, U.; Seymour, C.; Angus, D.C.; Isbell, T.S.; White, K.; Weir, W.; Yeh, L.; Vincent, A.; Bashir, R. Point-of-Care Sensors for the Management of Sepsis. Nat. Biomed. Eng. 2018, 2, 640–648. [Google Scholar] [CrossRef]
- Tsounidi, D.; Petrou, P.S.; Raptis, I. Current Progress on Biosensors and Point-of-Care Devices for Sepsis Diagnosis. IEEE Sens. J. 2021, 21, 12840–12855. [Google Scholar] [CrossRef]
- Prucha, M.; Bellingan, G.; Zazula, R. Sepsis Biomarkers. Clin. Chim. Acta 2015, 440, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Parlato, M.; Cavaillon, J.M. Host Response Biomarkers in the Diagnosis of Sepsis: A General Overview. Methods Molecular Biology 2014, 1237, 149–211. [Google Scholar] [CrossRef]
- Oduncu, A.F.; Kıyan, G.S.; Yalçınlı, S. Comparison of QSOFA, SIRS, and NEWS Scoring Systems for Diagnosis, Mortality, and Morbidity of Sepsis in Emergency Department. Am. J. Emergency Medicine 2021, 48, 54–59. [Google Scholar] [CrossRef]
- Kundu, S. Overview of Sepsis and Sepsis Biomarker Detection. Master’s Thesis, Iowa State University, Ames, IA, USA, 2019. [Google Scholar]
- List of Microorganisms. Available online: https://www.ecdc.europa.eu/en/healthcare-associated-infections-acute-care-hospitals/database/microorganisms-and-antimicrobial-resistance/list (accessed on 23 July 2022).
- Tan, M.; Lu, Y.; Jiang, H.; Zhang, L. The Diagnostic Accuracy of Procalcitonin and C-Reactive Protein for Sepsis: A Systematic Review and Meta-Analysis. J. Cell Biochem. 2019, 120, 5852–5859. [Google Scholar] [CrossRef] [PubMed]
- Kondo, Y.; Umemura, Y.; Hayashida, K.; Hara, Y.; Aihara, M.; Yamakawa, K. Diagnostic Value of Procalcitonin and Presepsin for Sepsis in Critically Ill Adult Patients: A Systematic Review and Meta-Analysis. J. Intensive Care 2019, 7, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, K.F.; Chaou, C.H.; Jiang, J.Y.; Yu, H.W.; Meng, Y.H.; Tang, W.C.; Wu, C.C. Diagnostic Accuracy of Lipopolysaccharide-Binding Protein as Biomarker for Sepsis in Adult Patients: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0153188. [Google Scholar] [CrossRef]
- García de Guadiana Romualdo, L.; Albaladejo Otón, M.D.; Rebollo Acebes, S.; Esteban Torrella, P.; Hernando Holgado, A.; Jiménez Santos, E.; Jiménez Sánchez, R.; Ortón Freire, A. Diagnostic Accuracy of Lipopolysaccharide-Binding Protein for Sepsis in Patients with Suspected Infection in the Emergency Department. Ann. Clin. Biochem. 2017, 55, 143–148. [Google Scholar] [CrossRef]
- Semeraro, F.; Ammollo, C.T.; Caironi, P.; Masson, S.; Latini, R.; Panigada, M.; Pesenti, A.; Semeraro, N.; Gattinoni, L.; Colucci, M. D-Dimer Corrected for Thrombin and Plasmin Generation Is a Strong Predictor of Mortality in Patients with Sepsis. Blood Transfus. 2020, 18, 304. [Google Scholar] [CrossRef]
- Raymond, S.L.; Hawkins, R.B.; Stortz, J.A.; Murphy, T.J.; Ungaro, R.; Dirain, M.L.; Nacionales, D.C.; Hollen, M.K.; Rincon, J.C.; Larson, S.D.; et al. Sepsis Is Associated with Reduced Spontaneous Neutrophil Migration Velocity in Human Adults. PLoS ONE 2018, 13, e0205327. [Google Scholar] [CrossRef] [Green Version]
- Schenck, E.J.; Ma, K.C.; Price, D.R.; Nicholson, T.; Oromendia, C.; Gentzler, E.R.; Sanchez, E.; Baron, R.M.; Fredenburgh, L.E.; Huh, J.W.; et al. Circulating Cell Death Biomarker TRAIL Is Associated with Increased Organ Dysfunction in Sepsis. JCI Insight 2019, 4, e127143. [Google Scholar] [CrossRef]
- Patnaik, R.; Azim, A.; Agarwal, V. Neutrophil CD64 a Diagnostic and Prognostic Marker of Sepsis in Adult Critically Ill Patients: A Brief Review. Indian J. Crit. Care Med. 2020, 24, 1242. [Google Scholar] [CrossRef]
- Gad, G.I.; Shinkar, D.M.; Kamel El-Din, M.M.; Nagi, H.M. The Utility of Soluble CD14 Subtype in Early Diagnosis of Culture-Proven Early-Onset Neonatal Sepsis and Prediction of Outcome. Am. J. Perinatol. 2020, 37, 497–502. [Google Scholar] [CrossRef] [PubMed]
- Abd Elkareem, R.M.; Ahmed, H.M.; Meabed, M.H.; Elias, S.S.; Elmaraghy, M.A. Diagnostic Value of CD64 in Early Detection of Neonatal Sepsis. Comp. Clin. Path 2020, 29, 639–643. [Google Scholar] [CrossRef]
- Hulett, M.D.; Hogarth, P.M. The Second and Third Extracellular Domains of FcγRI (CD64) Confer the Unique High Affinity Binding of IgG2a. Mol. Immunol. 1998, 35, 989–996. [Google Scholar] [CrossRef]
- Tian, H.Y.; Chen, J.Y.; Lin, J.; Liang, Q.R.; Lei, Y.; Li, X.; Wu, Y.; Yang, L.Y.; Lin, X.H.; Liu, A.L.; et al. Sepsis Progression Monitoring via Human Serum Fibronectin Detection Based on Sandwich-Type Electrochemical Immunosensor. Anal. Chim. Acta 2020, 1100, 225–231. [Google Scholar] [CrossRef]
- Nelson, D.L.; Cox, M.M. I Principi di Biochimica di Lehninger; Zanichelli: Bologna, Italy, 2002. [Google Scholar]
- Ryoo, S.M.; Lee, J.; Lee, Y.S.; Lee, J.H.; Lim, K.S.; Huh, J.W.; Hong, S.B.; Lim, C.M.; Koh, Y.; Kim, W.Y. Lactate Level versus Lactate Clearance for Predicting Mortality in Patients with Septic Shock Defined by Sepsis-3. Crit. Care Med. 2018, 46, E489–E495. [Google Scholar] [CrossRef]
- Ghimenti, S.; Lomonaco, T.; Bellagambi, F.G.; Biagini, D.; Salvo, P.; Trivella, M.G.; Scali, M.C.; Barletta, V.; Marzilli, M.; di Francesco, F.; et al. Salivary Lactate and 8-Isoprostaglandin F2α as Potential Non-Invasive Biomarkers for Monitoring Heart Failure: A Pilot Study. Sci. Rep. 2020, 10, 1–11. [Google Scholar] [CrossRef]
- Lu, J.; Wei, Z.; Jiang, H.; Cheng, L.; Chen, Q.; Chen, M.; Yan, J.; Sun, Z. Lactate Dehydrogenase Is Associated with 28-Day Mortality in Patients with Sepsis: A Retrospective Observational Study. J. Surg. Res. 2018, 228, 314–321. [Google Scholar] [CrossRef]
- Zein, J.G.; Lee, G.L.; Tawk, M.; Dabaja, M.; Kinasewitz, G.T. Prognostic Significance of Elevated Serum Lactate Dehydrogenase (LDH) in Patients with Severe Sepsis. Chest 2004, 126, 873S. [Google Scholar] [CrossRef]
- Benz, F.; Roy, S.; Trautwein, C.; Roderburg, C.; Luedde, T. Circulating MicroRNAs as Biomarkers for Sepsis. Int. J. Mol. Sci. 2016, 17, 78. [Google Scholar] [CrossRef] [Green Version]
- Peker, N.; Couto, N.; Sinha, B.; Rossen, J.W. Diagnosis of Bloodstream Infections from Positive Blood Cultures and Directly from Blood Samples: Recent Developments in Molecular Approaches. Clin. Microbiol. Infect. 2018, 24, 944–955. [Google Scholar] [CrossRef]
- Loonen, A.J.M.; Wolffs, P.F.G.; Bruggeman, C.A.; van den Brule, A.J.C. Developments for Improved Diagnosis of Bacterial Bloodstream Infections. Eur. J. Clin. Microbiol. Infect. Dis. 2014, 33, 1687–1702. [Google Scholar] [CrossRef]
- Cheng, M.P.; Stenstrom, R.; Paquette, K.; Stabler, S.N.; Akhter, M.; Davidson, A.C.; Gavric, M.; Lawandi, A.; Jinah, R.; Saeed, Z.; et al. Blood Culture Results Before and After Antimicrobial Administration in Patients With Severe Manifestations of Sepsis: A Diagnostic Study. Ann. Intern. Med. 2019, 171, 547–554. [Google Scholar] [CrossRef]
- Sautter, R.L.; Bills, A.R.; Lang, D.L.; Ruschell, G.; Heiter, B.J.; Bourbeau, P.P. Effects of Delayed-Entry Conditions on the Recovery and Detection of Microorganisms from BacT/ALERT and BACTEC Blood Culture Bottles. J. Clin. Microbiol. 2006, 44, 1245–1249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fenollar, F.; Raoult, D. Molecular Diagnosis of Bloodstream Infections Caused by Non-Cultivable Bacteria. Int. J. Antimicrob. Agents 2007, 30, 7–15. [Google Scholar] [CrossRef] [PubMed]
- La Scola, B.; Raoult, D. Direct Identification of Bacteria in Positive Blood Culture Bottles by Matrix-Assisted Laser Desorption Ionisation Time-of-Flight Mass Spectrometry. PLoS ONE 2009, 4, e8041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Opota, O.; Jaton, K.; Greub, G. Microbial Diagnosis of Bloodstream Infection: Towards Molecular Diagnosis Directly from Blood. Clin. Microbiol. Infection 2015, 21, 323–331. [Google Scholar] [CrossRef] [Green Version]
- Mwaigwisya, S.; Assiri, R.A.M.; O’Grady, J. Emerging Commercial Molecular Tests for the Diagnosis of Bloodstream Infection. Expert Rev. Mol. Diagn. 2015, 15, 681–692. [Google Scholar] [CrossRef]
- Seng, P.; Rolain, J.M.; Fournier, P.E.; la Scola, B.; Drancourt, M.; Raoult, D. MALDI-TOF-Mass Spectrometry Applications in Clinical Microbiology. Future Microbiol. 2010, 5, 1733–1754. [Google Scholar] [CrossRef]
- Panda, A.; Kurapati, S.; Samantaray, J.C.; Srinivasan, A.; Khalil, S. MALDI-TOF Mass Spectrometry Proteomic Based Identification of Clinical Bacterial Isolates. Indian J. Med. Res. 2014, 140, 770. [Google Scholar]
- Chen, H.; Liu, K.; Li, Z.; Wang, P. Point of Care Testing for Infectious Diseases. Clin. Chim. Acta 2019, 493, 138–147. [Google Scholar] [CrossRef]
- Kempf, M.; Bakour, S.; Flaudrops, C.; Berrazeg, M.; Brunel, J.M.; Drissi, M.; Mesli, E.; Touati, A.; Rolain, J.M. Rapid Detection of Carbapenem Resistance in Acinetobacter Baumannii Using Matrix-Assisted Laser Desorption Ionization-Time of Flight Mass Spectrometry. PLoS ONE 2012, 7, e31676. [Google Scholar] [CrossRef]
- Rychert, J. Benefits and Limitations of MALDI-TOF Mass Spectrometry for the Identification of Microorganisms. J. Infect. Epidemiol. 2019, 2, 1–5. [Google Scholar] [CrossRef]
- Rifai, N. Tietz Textbook of Clinical Chemistry and Molecular Diagnostics; Elsevier Health Sciences: St. Louis, MI, USA, 2017. [Google Scholar]
- Mancini, N. Diagnostic Methods and Protocols; Springer: New York, NY, USA, 2015. [Google Scholar]
- Hosseini, S.; Vázquez-Villegas, P.; Rito-Palomares, M.; Martinez-Chapa, S.O. Advantages, Disadvantages and Modifications of Conventional ELISA. In Enzyme-Linked Immunosorbent Assay (ELISA); Springer Briefs in Applied Sciences and Technology; Springer: Singapore, 2018; pp. 67–115. [Google Scholar] [CrossRef]
- Gan, S.D.; Patel, K.R. Enzyme Immunoassay and Enzyme-Linked Immunosorbent Assay. J. Investig. Dermatol. 2013, 133, 1–3. [Google Scholar] [CrossRef] [Green Version]
- Grieshaber, D.; MacKenzie, R.; Vörös, J.; Reimhult, E. Electrochemical Biosensors—Sensor Principles and Architectures. Sensors 2008, 8, 1400–1458. [Google Scholar] [CrossRef]
- Labuda, J.; Bowater, R.P.; Fojta, M.; Gauglitz, G.; Glatz, Z.; Hapala, I.; Havliš, J.; Kilar, F.; Kilar, A.; Malinovská, L.; et al. Terminology of Bioanalytical Methods (IUPAC Recommendations 2018). Pure Applied Chemistry 2018, 90, 1121–1198. [Google Scholar] [CrossRef] [Green Version]
- Pandey, C.M.; Malhotra, B.D. Biosensors: Fundamentals and Applications; Walter de Gruyter GmbH & Co KG: Berlin, Germany, 2019. [Google Scholar]
- Salvo, P.; Vivaldi, F.M.; Bonini, A.; Biagini, D.; Bellagambi, F.G.; Miliani, F.M.; Di Francesco, F.; Lomonaco, T. Biosensors for Detecting Lymphocytes and Immunoglobulins. Biosensors 2020, 10, 155. [Google Scholar] [CrossRef] [PubMed]
- Land, K.J.; Boeras, D.I.; Chen, X.S.; Ramsay, A.R.; Peeling, R.W. REASSURED Diagnostics to Inform Disease Control Strategies, Strengthen Health Systems and Improve Patient Outcomes. Nat. Microbiol. 2018, 4, 46–54. [Google Scholar] [CrossRef]
- Quesada-González, D.; Merkoçi, A. Nanomaterial-Based Devices for Point-of-Care Diagnostic Applications. Chem. Soc. Rev. 2018, 47, 4697–4709. [Google Scholar] [CrossRef]
- Bonini, A.; Vivaldi, F.M.; Herrera, E.; Melai, B.; Kirchhain, A.; Sajama, N.V.P.; Mattonai, M.; Caprioli, R.; Lomonaco, T.; Di Francesco, F.; et al. A Graphenic Biosensor for Real-Time Monitoring of Urea during Dialysis. IEEE Sens. J. 2020, 20, 4571–4578. [Google Scholar] [CrossRef]
- Poma, N.; Vivaldi, F.; Bonini, A.; Salvo, P.; Kirchhain, A.; Ates, Z.; Melai, B.; Bottai, D.; Tavanti, A.; di Francesco, F. Microbial Biofilm Monitoring by Electrochemical Transduction Methods. TrAC Trends Anal. Chem. 2021, 134, 116134. [Google Scholar] [CrossRef]
- Kirchhain, A.; Bonini, A.; Vivaldi, F.; Poma, N.; di Francesco, F. Latest Developments in Non-Faradic Impedimetric Biosensors: Towards Clinical Applications. TrAC Trends in Anal. Chem. 2020, 133, 116073. [Google Scholar] [CrossRef]
- Dincer, C.; Bruch, R.; Costa-Rama, E.; Fernández-Abedul, M.T.; Merkoçi, A.; Manz, A.; Urban, G.A.; Güder, F. Disposable Sensors in Diagnostics, Food, and Environmental Monitoring. Adv. Mater. 2019, 31, 1806739. [Google Scholar] [CrossRef]
- Vivaldi, F.M.; Dallinger, A.; Bonini, A.; Poma, N.; Sembranti, L.; Biagini, D.; Salvo, P.; Greco, F.; di Francesco, F. Three-Dimensional (3D) Laser-Induced Graphene: Structure, Properties, and Application to Chemical Sensing. ACS Appl. Mater. Interfaces 2021, 13, 30245–30260. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.M.; Ryu, M.Y.; Kim, J.H.; Cho, C.H.; Park, T.J.; Park, J.P. An Electrochemical Biosensor for Detection of the Sepsis-Related Biomarker Procalcitonin. RSC Adv. 2017, 7, 36562–36565. [Google Scholar] [CrossRef] [Green Version]
- Molinero-Fernández, Á.; Moreno-Guzmán, M.; López, M.Á.; Escarpa, A. Magnetic Bead-Based Electrochemical Immunoassays On-Drop and On-Chip for Procalcitonin Determination: Disposable Tools for Clinical Sepsis Diagnosis. Biosensors 2020, 10, 66. [Google Scholar] [CrossRef]
- Molinero-Fernández, Á.; Arruza, L.; López, M.Á.; Escarpa, A. On-the-Fly Rapid Immunoassay for Neonatal Sepsis Diagnosis: C-Reactive Protein Accurate Determination Using Magnetic Graphene-Based Micromotors. Biosens. Bioelectron. 2020, 158, 112156. [Google Scholar] [CrossRef]
- Guillem, P.; Bustos, R.H.; Garzon, V.; Munoz, A.; Juez, G. A Low-Cost Electrochemical Biosensor Platform for C-Reactive Protein Detection. Sens. Biosens. Res. 2021, 31, 100402. [Google Scholar] [CrossRef]
- Ge, X.Y.; Zhang, J.X.; Feng, Y.G.; Wang, A.J.; Mei, L.P.; Feng, J.J. Label-Free Electrochemical Biosensor for Determination of Procalcitonin Based on Graphene-Wrapped Co Nanoparticles Encapsulated in Carbon Nanobrushes Coupled with AuPtCu Nanodendrites. Microchim. Acta 2022, 189, 110. [Google Scholar] [CrossRef]
- Wang, X.Y.; Feng, Y.G.; Wang, A.J.; Mei, L.P.; Luo, X.; Xue, Y.; Feng, J.J. Facile Construction of Ratiometric Electrochemical Immunosensor Using Hierarchical PtCoIr Nanowires and Porous SiO2@Ag Nanoparticles for Accurate Detection of Septicemia Biomarker. Bioelectrochemistry 2021, 140, 107802. [Google Scholar] [CrossRef]
- Miao, J.; Du, K.; Li, X.; Xu, X.; Dong, X.; Fang, J.; Cao, W.; Wei, Q. Ratiometric Electrochemical Immunosensor for the Detection of Procalcitonin Based on the Ratios of SiO2-Fc–COOH–Au and UiO-66-TB Complexes. Biosens. Bioelectron. 2021, 171, 112713. [Google Scholar] [CrossRef]
- Tanak, A.S.; Jagannath, B.; Tamrakar, Y.; Muthukumar, S.; Prasad, S. Non-Faradaic Electrochemical Impedimetric Profiling of Procalcitonin and C-Reactive Protein as a Dual Marker Biosensor for Early Sepsis Detection. Anal. Chim. Acta X 2019, 3, 100029. [Google Scholar] [CrossRef]
- Zupančič, U.; Jolly, P.; Estrela, P.; Moschou, D.; Ingber, D.E. Graphene Enabled Low-Noise Surface Chemistry for Multiplexed Sepsis Biomarker Detection in Whole Blood. Adv. Funct. Mater. 2021, 31, 2010638. [Google Scholar] [CrossRef]
- Russell, C.; Ward, A.C.; Vezza, V.; Hoskisson, P.; Alcorn, D.; Steenson, D.P.; Corrigan, D.K. Development of a Needle Shaped Microelectrode for Electrochemical Detection of the Sepsis Biomarker Interleukin-6 (IL-6) in Real Time. Biosens. Bioelectron. 2019, 126, 806–814. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Gopinath, S.C.B.; Anbu, P. Longitudinal Zeolite-Iron Oxide Nanocomposite Deposited Capacitance Biosensor for Interleukin-3 in Sepsis Detection. Nanoscale Res. Lett. 2021, 16, 68. [Google Scholar] [CrossRef]
- Min, J.; Nothing, M.; Coble, B.; Zheng, H.; Park, J.; Im, H.; Weber, G.F.; Castro, C.M.; Swirski, F.K.; Weissleder, R.; et al. Integrated Biosensor for Rapid and Point-of-Care Sepsis Diagnosis. ACS Nano 2018, 12, 3378–3384. [Google Scholar] [CrossRef] [PubMed]
- Tanak, A.S.; Muthukumar, S.; Krishnan, S.; Schully, K.L.; Clark, D.V.; Prasad, S. Multiplexed Cytokine Detection Using Electrochemical Point-of-Care Sensing Device towards Rapid Sepsis Endotyping. Biosens. Bioelectron. 2021, 171, 112726. [Google Scholar] [CrossRef] [PubMed]
- Tanak, A.S.; Sardesai, A.; Muthukumar, S.; Krishnan, S.; Striegel, D.A.; Schully, K.L.; Clark, D.V.; Prasad, S. Multiplexed Host Immune Response Biosensor for Rapid Sepsis Stratification and Endotyping at Point-of-Care. Biosens. Bioelectron. X 2022, 10, 100144. [Google Scholar] [CrossRef]
- Gao, J.; Jeffries, L.; Mach, K.E.; Craft, D.W.; Thomas, N.J.; Gau, V.; Liao, J.C.; Wong, P.K. A Multiplex Electrochemical Biosensor for Bloodstream Infection Diagnosis. SLAS Technol. 2017, 22, 466–474. [Google Scholar] [CrossRef] [Green Version]
- Sharma, R.; Lakshmi, G.B.V.S.; Kumar, A.; Solanki, P. Polypyrrole Based Molecularly Imprinted Polymer Platform for Klebsiella Pneumonia Detection. ECS Sens. Plus 2022, 1, 010603. [Google Scholar] [CrossRef]
- Bonini, A.; Poma, N.; Vivaldi, F.; Biagini, D.; Bottai, D.; Tavanti, A.; di Francesco, F. A Label-Free Impedance Biosensing Assay Based on CRISPR/Cas12a Collateral Activity for Bacterial DNA Detection. J. Pharm. Biomed. Anal. 2021, 204, 114268. [Google Scholar] [CrossRef]
- Oved, K.; Cohen, A.; Boico, O.; Navon, R.; Friedman, T.; Etshtein, L.; Kriger, O.; Bamberger, E.; Fonar, Y.; Yacobov, R.; et al. A Novel Host-Proteome Signature for Distinguishing between Acute Bacterial and Viral Infections. PLoS ONE 2015, 10, e0120012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonini, A.; Poma, N.; Vivaldi, F.; Kirchhain, A.; Salvo, P.; Bottai, D.; Tavanti, A.; di Francesco, F. Advances in Biosensing: The CRISPR/Cas System as a New Powerful Tool for the Detection of Nucleic Acids. J. Pharm. Biomed. Anal. 2021, 192, 113645. [Google Scholar] [CrossRef]
- Damborský, P.; Švitel, J.; Katrlík, J. Optical Biosensors. Essays Biochem. 2016, 60, 91–100. [Google Scholar] [PubMed] [Green Version]
- Vivaldi, F.; Salvo, P.; Poma, N.; Bonini, A.; Biagini, D.; del Noce, L.; Melai, B.; Lisi, F.; di Francesco, F. Recent Advances in Optical, Electrochemical and Field Effect PH Sensors. Chemosensors 2021, 9, 33. [Google Scholar] [CrossRef]
- Chen, C.; Wang, J. Optical Biosensors: An Exhaustive and Comprehensive Review. Analyst 2020, 145, 1605–1628. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.T.; Lee, Y.C.; Lai, Y.H.; Lim, J.C.; Huang, N.T.; Lin, C.T.; Huang, J.J. Review of Integrated Optical Biosensors for Point-of-Care Applications. Biosensors 2020, 10, 209. [Google Scholar] [CrossRef]
- Guo, X. Surface Plasmon Resonance Based Biosensor Technique: A Review. J. Biophotonics 2012, 5, 483–501. [Google Scholar] [CrossRef]
- Wang, W.; Mai, Z.; Chen, Y.; Wang, J.; Li, L.; Su, Q.; Li, X.; Hong, X. A Label-Free Fiber Optic SPR Biosensor for Specific Detection of C-Reactive Protein. Sci. Rep. 2017, 7, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Chiang, C.Y.; Huang, T.T.; Wang, C.H.; Huang, C.J.; Tsai, T.H.; Yu, S.N.; Chen, Y.T.; Hong, S.W.; Hsu, C.W.; Chang, T.C.; et al. Fiber Optic Nanogold-Linked Immunosorbent Assay for Rapid Detection of Procalcitonin at Femtomolar Concentration Level. Biosens. Bioelectron. 2020, 151, 111871. [Google Scholar] [CrossRef]
- Giorgi-Coll, S.; Marín, M.J.; Sule, O.; Hutchinson, P.J.; Carpenter, K.L.H. Aptamer-Modified Gold Nanoparticles for Rapid Aggregation-Based Detection of Inflammation: An Optical Assay for Interleukin-6. Microchim. Acta 2020, 187, 13. [Google Scholar] [CrossRef]
- Fabri-Faja, N.; Calvo-Lozano, O.; Dey, P.; Terborg, R.A.; Estevez, M.C.; Belushkin, A.; Yesilköy, F.; Duempelmann, L.; Altug, H.; Pruneri, V.; et al. Early Sepsis Diagnosis via Protein and MiRNA Biomarkers Using a Novel Point-of-Care Photonic Biosensor. Anal. Chim. Acta 2019, 1077, 232–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santopolo, G.; Doménech-Sánchez, A.; Russell, S.M.; de La Rica, R. Ultrafast and Ultrasensitive Naked-Eye Detection of Urease-Positive Bacteria with Plasmonic Nanosensors. ACS Sens. 2019, 4, 961–967. [Google Scholar] [CrossRef]
- Zhou, X.; Li, P.; Wu, X.; Lin, X.; Zhao, L.; Huang, H.; Wu, J.; Cai, H.; Xu, M.; Zhou, H.; et al. Multifunctional Biosensor Constructed by Ag-Coating Magnetic-Assisted Unique Urchin Core Porous Shell Structure for Dual SERS Enhancement, Enrichment, and Quantitative Detection of Multi-Components Inflammatory Markers. Biosens. Bioelectron. 2022, 210, 114257. [Google Scholar] [CrossRef] [PubMed]
- Narayana Iyengar, S.; Dietvorst, J.; Ferrer-Vilanova, A.; Guirado, G.; Muñoz-Berbel, X.; Russom, A. Toward Rapid Detection of Viable Bacteria in Whole Blood for Early Sepsis Diagnostics and Susceptibility Testing. ACS Sens. 2021, 6, 3357–3366. [Google Scholar] [CrossRef] [PubMed]
- Kundu, A.; Rani, R.; Ahmad, A.; Kumar, A.; Raturi, M.; Gupta, T.; Khan, R.; Hazra, K.S. Ultrasensitive and Label-Free Detection of Prognostic and Diagnostic Biomarkers of Sepsis on a AgNP-Laden Black Phosphorous-Based SERS Platform. Sens. Diagn. 2022, 1, 449–459. [Google Scholar] [CrossRef]
- Tsounidi, D.; Koukouvinos, G.; Christianidis, V.; Legaki, E.; Giogli, V.; Panagiotopoulou, K.; Taka, S.; Ekaterinidi, Z.; Kakabakos, S.; Raptis, I.; et al. Development of a Point-of-Care System Based on White Light Reflectance Spectroscopy: Application in Crp Determination. Biosensors 2021, 11, 268. [Google Scholar] [CrossRef]
- Willets, K.A.; van Duyne, R.P. Localized Surface Plasmon Resonance Spectroscopy and Sensing. Annu. Rev. Phys. Chem. 2007, 58, 267–297. [Google Scholar] [CrossRef] [Green Version]
- Cao, J.; Galbraith, E.K.; Sun, T.; Grattan, K.T.V. Comparison of Surface Plasmon Resonance and Localized Surface Plasmon Resonance-Based Optical Fibre Sensors. J. Phys. Conf. Ser. 2011, 307, 012050. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Bacteria | Gram | Respiration |
|---|---|---|
| Staphylococcus aureus | Aerobic/Facultative anaerobic | |
| Enterococcus faecalis | Aerobic/Facultative anaerobic | |
| Streptococcus pneumoniae | Aerobic/Facultative anaerobic | |
| Neisseria meningitidis | Aerobic | |
| Klebsiella pneumoniae | Aerobic/Facultative anaerobic | |
| Acinetobacter baumannii | Aerobic | |
| Escherichia coli | Aerobic/Facultative anaerobic | |
| Salmonella enterica | Aerobic/Facultative anaerobic | |
| Shigella dysenteriae | Aerobic/Facultative anaerobic | |
| Citrobacter freundii | Aerobic/Facultative anaerobic | |
| Serratia marcescens | Aerobic/Facultative anaerobic | |
| Proteus mirabilis | Aerobic/Facultative anaerobic | |
| Pseudomonas aeruginosa | Aerobic/Facultative anaerobic | |
| Bacteroides fragilis | Obligate anaerobic | |
| Haemophilus influenzae b | Aerobic/Facultative anaerobic |
| Electrode | Biorecognition Element | Biomarker | Technique | LOD | Working Range | Sample | Response Time | Year | Ref. |
|---|---|---|---|---|---|---|---|---|---|
| Gold | BP3 peptide | PCT | EIS | 12.5 ng/mL | 0.013–0.25 g/mL | Buffer | / | 2017 | [65] |
| Carbon screen printed | Antibody | PCT | Amperometric | 0.1 ng/mL | 0.5–1000 ng/mL | Human serum | <20 min | 2020 | [66] |
| Gold | Antibody | PCT | Amperometric | 0.04 ng/mL | 0.1–20 ng/mL | Plasma | <20 min | 2020 | |
| Carbon screen printed | Antibody | CRP | Amperometric | 0.80 g/mL | 2–100 g/mL | Plasma | 5 min | 2020 | [67] |
| Carbon screen printed | Antibody | CRP | Amperometric | 0.058 g/mL | 1–100 g/mL | Plasma | 5 min | 2021 | [68] |
| Glassy carbon electrode | Antibody | PCT | Amperometric | 0.011 pg/mL | 0.0001–100 ng/mL | Diluted serum | 50 min | 2022 | [69] |
| Glassy carbon electrode | Antibody | PCT | DPV | 0.46 pg/mL | 0.001–100 ng/mL | Diluted human serum | / | 2021 | [70] |
| Glassy carbon electrode | Antibody | PCT | DPV | 0.3 pg/mL | 1 pg/mL–100 ng/mL | Human serum | / | 2021 | [71] |
| Gold interdigitated electrode | Antibody | PCT, CRP | EIS | 10 ng/mL | 0.01–10 ng/mL | Human Serum | <15 min | 2019 | [72] |
| Gold electrode | Antibody | PCT, CRP | Amperometric | 10 ng/mL | 0.01–10 ng/mL | Clinical sample | <15 min | 2021 | [73] |
| Gold electrode on microneedle | Antibody | IL-6 | DPV | / | 20–100 pg/mL | Human Serum spiked | 3 min | 2018 | [74] |
| Gold interdigitated | Antibody | IL-3 | Capacitive | 3.0 pg/mL | 3.0–100 pg/mL | Human Serum spiked | / | 2021 | [75] |
| Gold screen printed | Antibody | IL-3 | Chronoamperometry | 10 pg/mL | 10–104 pg/mL | Plasma/serum from clinical sample | <1 h | 2018 | [76] |
| Gold | Antibody | IL-6, IL-8, IL-10, TRAIL, IP 10 | EIS | 0.1, 0.1, 1.0, 1.0, 1.0 pg/mL | 0.01–104, 0.1–5000, 0.1–103, 1.0–2103 pg/mL | Plasma | 5 min | 2021 | [77] |
| Disposable sensor cartridge with a gold-based array electrodes | Antibody | IL-6, IL-8, IL-10, TRAIL, IP 10 | Label-free non faradic impedence spetroscopy | 0.1, 0.1, 1.0, 1.0, 1.0 pg/mL | 0.01–104, 0.1–5000, 0.1–103, 1.0–2103 pg/mL | Clinical samples | 5 min | 2022 | [78] |
| Gold | RNA specific probe | 16S RNA from S. aureus, E coli, P aeruginosa, P. mirabilis | Amperometry | 290 CFU/mL | / | Human blood | <1 h | 2017 | [79] |
| Indium tin oxide coated glass | Conductive MIP | K. pneumoniae | DPV | 1.35 CFU/mL | 1.0–1.0105 CFU/mL | Spiked human urine | 3 min | 2022 | [80] |
| Gold | CRISPR/Cas12a | DNA from E. coli, S. aureus | EIS | 3.0 nM | 3 –18 nM | Buffer solution spiked clinical strains | 1 h | 2022 | [81] |
| Substrate | Biorecognition Element | Biomarker | Technique | LOD | Working Range | Sample | Response Time | Year | Ref. |
|---|---|---|---|---|---|---|---|---|---|
| Optic fiber | Antibody | CRP | SPR | 1.17 μg/mL | 0.01–20 ug/mL | PBS buffer | / | 2017 | [89] |
| Optic fiber | Antibody | PCT | LSPR | 95 fg/mL | 1–100 ng/mL | Human serum | <15 min | 2019 | [90] |
| AuNPs | Aptamers | IL-6 | LSPR | 1.95 μg/mL | 3.3–125 μg/mL | mixed protein solution | 5 min | 2020 | [91] |
| gold nanohole array (Au-NHA) | Antibody | CRP | Interferometry | 18 mg/mL | 0–250 μg/mL | spiked PBS sample | 1 min after sample incubation | 2019 | [92] |
| Antibody | IL-6 | 88 mg/mL | 0–400 μg/mL | ||||||
| DNA capture probe | miRNA-16 | 6 mg/mL | 0.8–12.5 μg/mL | ||||||
| AuNPs | electrostatic | urease | LSPR | 0.8 μg/mL | 0.8–12.5 μg/mL | broth culture | 40 min | 2019 | [93] |
| AgNPs@BP | Aptamers | CRP | SERS | 100 fg/mL | 10−4–10 ng/mL | Human serum | / | 2022 | [94] |
| IL-6 | 0.1 fg/mL | 10−7–10−2 ng/mL | |||||||
| PCT | 1.0 fg/mL | 10−6–10−1 ng/mL | |||||||
| / | Photocatalysis | S. capitis | Colorimetry | 103 CFU/mL | 102–108 CFU/mL | Whole blood | <5 h | 2021 | [95] |
| E. coli | |||||||||
| AgMNPs/CPs | Label-free | IL-3 | SERS | 1000 fM | 1 pM–100 nM | Sterile human serum | Real time | 2022 | [96] |
| PCT | 100 fM | 100 fM–100 nM | |||||||
| Silicon chip | Antibody | CRP | WLRS | 1 ng/mL | 0.05–200 μg/mL | Human plasma | 12 min | 2021 | [97] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bonini, A.; Carota, A.G.; Poma, N.; Vivaldi, F.M.; Biagini, D.; Bottai, D.; Lenzi, A.; Tavanti, A.; Di Francesco, F.; Lomonaco, T. Emerging Biosensing Technologies towards Early Sepsis Diagnosis and Management. Biosensors 2022, 12, 894. https://doi.org/10.3390/bios12100894
Bonini A, Carota AG, Poma N, Vivaldi FM, Biagini D, Bottai D, Lenzi A, Tavanti A, Di Francesco F, Lomonaco T. Emerging Biosensing Technologies towards Early Sepsis Diagnosis and Management. Biosensors. 2022; 12(10):894. https://doi.org/10.3390/bios12100894
Chicago/Turabian StyleBonini, Andrea, Angela Gilda Carota, Noemi Poma, Federico Maria Vivaldi, Denise Biagini, Daria Bottai, Alessio Lenzi, Arianna Tavanti, Fabio Di Francesco, and Tommaso Lomonaco. 2022. "Emerging Biosensing Technologies towards Early Sepsis Diagnosis and Management" Biosensors 12, no. 10: 894. https://doi.org/10.3390/bios12100894