
From Cerebrospinal Fluid Neurochemistry to Clinical Diagnosis of Alzheimer’s Disease in the Era of Anti-Amyloid Treatments. Report of Four Patients

 ,
,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Neuropsychological Approach
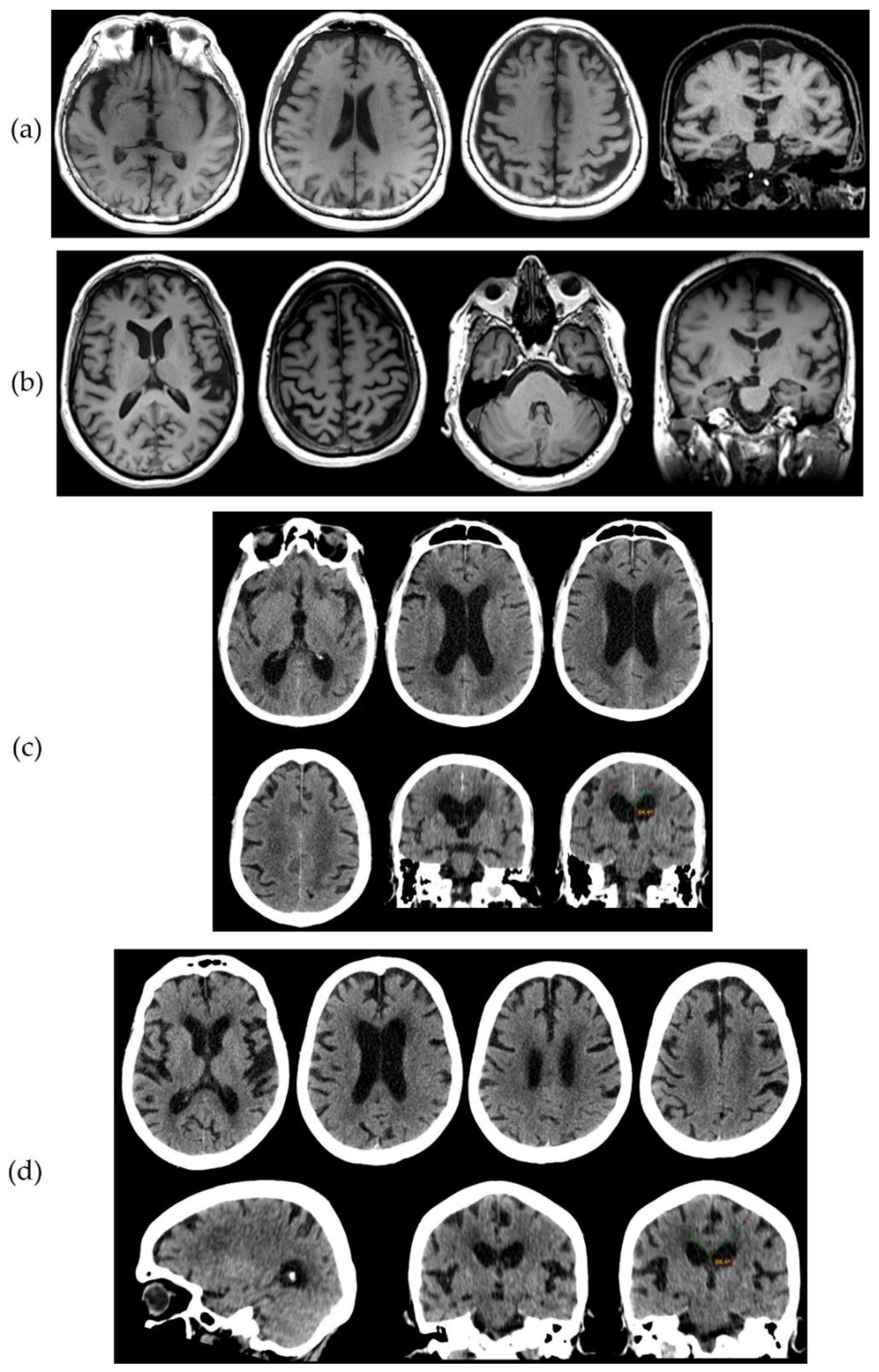
2.3. Neuroimaging
2.4. Lumbar Puncture and CSF Biomarker Measurements
3. Results
3.1. Patient 1
3.2. Patient 2
3.3. Patient 3
3.4. Patient 4
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hyman, B.T.; Phelps, C.H.; Beach, T.G.; Bigio, E.H.; Cairns, N.J.; Carrillo, M.C.; Dickson, D.W.; Duyckaerts, C.; Frosch, M.P.; Masliah, E.; et al. National Institute on Aging-Alzheimer’s Association guidelines for the neuropathologic assessment of Alzheimer’s disease. Alzheimers Dement. 2012, 8, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Jellinger, K.A.; Bancher, C. Neuropathology of Alzheimer’s disease: A critical update. J. Neural. Transm. Suppl. 1998, 54, 77–95. [Google Scholar]
- Braak, H.; Braak, E. Neuropathological staging of Alzheimer-related changes. Acta Neuropathol. 1991, 82, 239–259. [Google Scholar] [CrossRef]
- Sperling, R.A.; Aisen, P.S.; Beckett, L.A.; Bennett, D.A.; Craft, S.; Fagan, A.M.; Iwatsubo, T.; Jack, C.R., Jr.; Kaye, J.; Montine, T.J.; et al. Toward defining the preclinical stages of Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011, 7, 280–292. [Google Scholar] [CrossRef] [Green Version]
- Dubois, B.; Feldman, H.H.; Jacova, C.; Hampel, H.; Molinuevo, J.L.; Blennow, K.; DeKosky, S.T.; Gauthier, S.; Selkoe, D.; Bateman, R.; et al. Advancing research diagnostic criteria for Alzheimer’s disease: The IWG-2 criteria. Lancet Neurol. 2014, 13, 614–629. [Google Scholar] [CrossRef]
- Albert, M.S.; DeKosky, S.T.; Dickson, D.; Dubois, B.; Feldman, H.H.; Fox, N.C.; Gamst, A.; Holtzman, D.M.; Jagust, W.J.; Petersen, R.C.; et al. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011, 7, 270–279. [Google Scholar] [CrossRef] [Green Version]
- McKhann, G.M.; Knopman, D.S.; Chertkow, H.; Hyman, B.T.; Jack, C.R., Jr.; Kawas, C.H.; Klunk, W.E.; Koroshetz, W.J.; Manly, J.J.; Mayeux, R.; et al. The diagnosis of dementia due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011, 7, 263–269. [Google Scholar] [CrossRef] [Green Version]
- Wagner, M.; Wolf, S.; Reischies, F.M.; Daerr, M.; Wolfsgruber, S.; Jessen, F.; Popp, J.; Maier, W.; Hüll, M.; Frölich, L.; et al. Biomarker validation of a cued recall memory deficit in prodromal Alzheimer disease. Neurology 2012, 78, 379–386. [Google Scholar] [CrossRef] [PubMed]
- Mendez, M.F. Early-onset Alzheimer disease. Neurol. Clin. 2017, 35, 263–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grossman, M. Primary progressive aphasia: Clinicopathological correlations. Nat. Rev. Neurol. 2010, 6, 88–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mendez, M.F.; Joshi, A.; Tassniyom, K.; Teng, E.; Shapira, J.S. Clinicopathologic differences among patients with behavioral variant frontotemporal dementia. Neurology 2013, 80, 561–568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boeve, B.F.; Josephs, K.A.; Drubach, D.A. Current and future management of the corticobasal syndrome and corticobasal degeneration. Handb. Clin. Neurol. 2008, 89, 533–548. [Google Scholar]
- Crutch, S.J.; Lehmann, M.; Schott, J.M.; Rabinovici, G.D.; Rossor, M.N.; Fox, N.C. Posterior cortical atrophy. Lancet Neurol. 2012, 11, 170–178. [Google Scholar] [CrossRef] [Green Version]
- Wallin, A.; Nordlund, A.; Jonsson, M.; Blennow, K.; Zetterberg, H.; Öhrfelt, A.; Stålhammar, J.; Eckerström, M.; Carlsson, M.; Olsson, E.; et al. Alzheimer’s disease–subcortical vascular disease spectrum in a hospital-based setting: Overview of results from the Gothenburg MCI and dementia studies. J. Cereb. Blood Flow Metab. 2016, 36, 95–113. [Google Scholar] [CrossRef] [PubMed]
- Peavy, G.M.; Edland, S.D.; Toole, B.M.; Hansen, L.A.; Galasko, D.R.; Mayo, A.M. Phenotypic differences based on staging of Alzheimer’s neuropathology in autopsy-confirmed dementia with Lewy bodies. Parkinsonism Relat. Disord. 2016, 31, 72–78. [Google Scholar] [CrossRef] [Green Version]
- Müller-Schmitz, K.; Krasavina-Loka, N.; Yardimci, T.; Lipka, T.; Kolman, A.G.J.; Robbers, S.; Menge, T.; Kujovic, M.; Seitz, R.J. Normal Pressure Hydrocephalus Associated with Alzheimer’s Disease. Ann. Neurol. 2020, 88, 703–711. [Google Scholar] [CrossRef]
- Graff-Radford, J.; Yong, K.X.X.; Apostolova, L.G.; Bouwman, F.H.; Carrillo, M.; Dickerson, B.C.; Rabinovici, G.D.; Schott, J.M.; Jones, D.T.; Murray, M.E. New insights into atypical Alzheimer’s disease in the era of biomarkers. Lancet Neurol. 2021, 20, 222–234. [Google Scholar] [CrossRef]
- Jack, C.R., Jr.; Bennett, D.A.; Blennow, K.; Carrillo, M.C.; Dunn, B.; Haeberlein, S.B.; Holtzman, D.M.; Jagust, W.; Jessen, F.; Karlawish, J.; et al. NIA-AA Research Framework: Toward a biological definition of Alzheimer’s disease. Alzheimers Dement. 2018, 14, 535–562. [Google Scholar] [CrossRef]
- McKhann, G.; Drachman, D.; Folstein, M.; Katzman, R.; Price, D.; Stadlan, E.M. Clinical diagnosis of Alzheimer’s disease: Report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer’s Disease. Neurology 1984, 34, 939–944. [Google Scholar] [CrossRef] [Green Version]
- Lopez, O.L.; Becker, J.T.; Klunk, W.; Saxton, J.; Hamilton, R.L.; Kaufer, D.I.; Sweet, R.A.; Cidis Meltzer, C.; Wisniewski, S.; Kamboh, M.I.; et al. Research evaluation and diagnosis of probable Alzheimer’s disease over the last two decades: I. Neurology 2000, 55, 1854–1862. [Google Scholar] [CrossRef]
- Mendez, M.; Mastri, A.R.; Sung, J.H.; Frey, W.H. Clinically diagnosed Alzheimer’s disease: Neuropathologic findings in 650 cases. Alzheimer Dis. Assoc. Disord. 1992, 6, 35–43. [Google Scholar] [CrossRef]
- Nelson, P.T.; Head, E.; Schmitt, F.A.; Davis, P.R.; Neltner, J.H.; Jicha, G.A.; Abner, E.L.; Smith, C.D.; Van Eldik, L.J.; Kryscio, R.J.; et al. Alzheimer’s disease is not "brain aging": Neuropathological, genetic, and epidemiological human studies. Acta Neuropathol. 2011, 121, 571–587. [Google Scholar] [CrossRef] [Green Version]
- Galasko, D.; Hansen, L.A.; Katzman, R.; Wiederholt, W.; Masliah, E.; Terry, R.; Hill, L.R.; Lessin, P.; Thal, L.J. Clinical-neuropathological correlations in Alzheimer’s disease and related dementias. Arch. Neurol. 1994, 51, 888–895. [Google Scholar] [CrossRef] [PubMed]
- Johnell, K.; Religa, D.; Eriksdotter, M. Differences in drug therapy between dementia disorders in the Swedish dementia registry: A nationwide study of over 7000 patients. Dement. Geriatr. Cogn. Disord. 2013, 35, 239–248. [Google Scholar] [CrossRef] [PubMed]
- Thomas, A.J.; Mahin-Babaei, F.; Saidi, M.; Lett, D.; Taylor, J.P.; Walker, L.; Attems, J. Improving the identification of dementia with Lewy bodies in the context of an Alzheimer’s-type dementia. Alzheimers Res. Ther. 2018, 10, 27. [Google Scholar] [CrossRef] [PubMed]
- Tagliavini, F.; Tiraboschi, P.; Federico, A. Alzheimer’s disease: The controversial approval of Aducanumab. Neurol. Sci. 2021, 42, 3069–3070. [Google Scholar] [CrossRef]
- McGrowder, D.A.; Miller, F.; Vaz, K.; Nwokocha, C.; Wilson-Clarke, C.; Anderson-Cross, M.; Brown, J.; Anderson-Jackson, L.; Williams, L.; Latore, L.; et al. Cerebrospinal Fluid Biomarkers of Alzheimer’s Disease: Current Evidence and Future Perspectives. Brain Sci. 2021, 11, 215. [Google Scholar] [CrossRef]
- Lewczuk, P.; Riederer, P.; O’Bryant, S.E.; Verbeek, M.M.; Dubois, B.; Visser, P.J.; Jellinger, K.A.; Engelborghs, S.; Ramirez, A.; Parnetti, L.; et al. Cerebrospinal fluid and blood biomarkers for neurodegenerative dementias: An update of the Consensus of the Task Force on Biological Markers in Psychiatry of the World Federation of Societies of Biological Psychiatry. World J. Biol. Psychiatry 2018, 19, 244–328. [Google Scholar] [CrossRef]
- Sjögren, M.; Minthon, L.; Davidsson, P.; Granérus, A.K.; Clarberg, A.; Vanderstichele, H.; Vanmechelen, E.; Wallin, A.; Blennow, K. CSF levels of tau, beta-amyloid(1-42) and GAP-43 in frontotemporal dementia, other types of dementia and normal aging. J. Neural Transm. 2000, 107, 563–579. [Google Scholar]
- Vanderstichele, H.; De Vreese, K.; Blennow, K.; Andreasen, N.; Sindic, C.; Ivanoiu, A.; Hampel, H.; Bürger, K.; Parnetti, L.; Lanari, A.; et al. Analytical performance and clinical utility of the INNOTEST PHOSPHO-TAU181P assay for discrimination between Alzheimer’s disease and dementia with Lewy bodies. Clin. Chem. Lab. Med. 2006, 44, 1472–1480. [Google Scholar] [CrossRef]
- Blennow, K.; Wallin, A.; Agren, H.; Spenger, C.; Siegfried, J.; Vanmechelen, E. Tau protein in cerebrospinal fluid: A biochemical marker for axonal degeneration in Alzheimer disease? Mol. Chem. Neuropathol. 1995, 26, 231–245. [Google Scholar] [CrossRef]
- Niemantsverdriet, E.; Ottoy, J.; Somers, C.; De Roeck, E.; Struyfs, H.; Soetewey, F.; Verhaeghe, J.; Van den Bossche, T.; Van Mossevelde, S.; Goeman, J.; et al. The Cerebrospinal Fluid Aβ1-42/Aβ1-40 Ratio Improves Concordance with Amyloid-PET for Diagnosing Alzheimer’s Disease in a Clinical Setting. J. Alzheimers Dis. 2017, 60, 561–576. [Google Scholar] [CrossRef] [Green Version]
- Simonsen, A.H.; Herukka, S.K.; Andreasen, N.; Baldeiras, I.; Bjerke, M.; Blennow, K.; Engelborghs, S.; Frisoni, G.B.; Gabryelewicz, T.; Galluzzi, S.; et al. Recommendations for CSF AD biomarkers in the diagnostic evaluation of dementia. Alzheimers Dement. 2017, 13, 274–284. [Google Scholar] [CrossRef] [Green Version]
- Seeburger, J.L.; Holder, D.J.; Combrinck, M.; Joachim, C.; Laterza, O.; Tanen, M.; Dallob, A.; Chappell, D.; Snyder, K.; Flynn, M.; et al. Cerebrospinal fluid biomarkers distinguish postmortem-confirmed Alzheimer’s disease from other dementias and healthy controls in the OPTIMA cohort. J. Alzheimers Dis. 2015, 44, 525–539. [Google Scholar] [CrossRef]
- Jack, C.R., Jr.; Bennett, D.A.; Blennow, K.; Carrillo, M.C.; Feldman, H.H.; Frisoni, G.B.; Hampel, H.; Jagust, W.J.; Johnson, K.A.; Knopman, D.S.; et al. A/T/N: An unbiased descriptive classification scheme for Alzheimer disease biomarkers. Neurology 2016, 87, 539–547. [Google Scholar] [CrossRef]
- Delmotte, K.; Schaeverbeke, J.; Poesen, K.; Vandenberghe, R. Prognostic value of amyloid/tau/neurodegeneration (ATN) classification based on diagnostic cerebrospinal fluid samples for Alzheimer’s disease. Alzheimers Res. Ther. 2021, 13, 84. [Google Scholar] [CrossRef]
- Konstantinopoulou, E.; Kosmidis, M.H.; Ioannidis, P.; Kiosseoglou, G.; Karacostas, D.; Taskos, N. Adaptation of Addenbrooke’s Cognitive Examination-Revised for the Greek population. Eur. J. Neurol. 2011, 18, 442–447. [Google Scholar] [CrossRef] [PubMed]
- Fountoulakis, K.N.; Tsolaki, M.; Chantzi, H.; Kazis, A. Mini Mental State Examination (MMSE): A validation study in Greece. Am. J. Alzheimers Dis. Other Demen. 2000, 15, 342–345. [Google Scholar] [CrossRef]
- Theotoka, I.; Kapaki, E.; Vagenas, V.; Ilias, I.; Paraskevas, G.P.; Liappas, I. Preliminary report of a validation study of Instrumental Activities of Daily Living in a Greek sample. Percept. Mot. Skills 2007, 104, 958–960. [Google Scholar] [CrossRef] [PubMed]
- Dubois, B.; Touchon, J.; Portet, F.; Ousset, P.J.; Vellas, B.; Michel, B. “The 5 words”: A simple and sensitive test for the diagnosis of Alzheimer’s disease. Presse. Med. 2002, 31, 1696–1699. [Google Scholar]
- Dubois, B.; Slachevsky, A.; Litvan, I.; Pillon, B. The FAB: A Frontal Assessment Battery at bedside. Neurology 2000, 55, 1621–1626. [Google Scholar] [CrossRef] [Green Version]
- Royall, D.R.; Cordes, J.A.; Polk, M. CLOX: An executive clock drawing task. J. Neurol. Neurosurg. Psychiatry 1998, 64, 588–594. [Google Scholar] [CrossRef] [PubMed]
- Sheikh, J.I.; Yesavage, J.A. Geriatric Depression Scale (GDS): Recent evidence and development of a shorter version. Clin. Gerontol. 1986, 5, 165–173. [Google Scholar]
- Morris, J.C. The Clinical Dementia Rating (CDR): Current version and scoring rules. Neurology 1993, 43, 2412–2414. [Google Scholar] [CrossRef]
- Scheltens, P.; Leys, D.; Barkhof, F.; Huglo, D.; Weinstein, H.C.; Vermersch, P.; Kuiper, M.; Steinling, M.; Wolters, E.C.; Valk, J. Atrophy of medial temporal lobes on MRI in “probable” Alzheimer’s disease and normal ageing: Diagnostic value and neuropsychological correlates. J. Neurol. Neurosurg. Psychiatry 1992, 55, 967–972. [Google Scholar] [CrossRef] [PubMed]
- Kockum, K.; Lilja-Lund, O.; Larsson, E.M.; Rosell, M.; Söderström, L.; Virhammar, J.; Laurell, K. The idiopathic normal-pressure hydrocephalus Radscale: A radiological scale for structured evaluation. Eur. J. Neurol. 2018, 25, 569–576. [Google Scholar] [CrossRef] [PubMed]
- Del Campo, M.; Mollenhauer, B.; Bertolotto, A.; Engelborghs, S.; Hampel, H.; Simonsen, A.H.; Kapaki, E.; Kruse, N.; Le Bastard, N.; Lehmann, S.; et al. Recommendations to standardize preanalytical confounding factors in Alzheimer’s and Parkinson’s disease cerebrospinal fluid biomarkers: An update. Biomark. Med. 2012, 6, 419–430. [Google Scholar] [CrossRef]
- Constantinides, V.C.; Paraskevas, G.P.; Boufidou, F.; Bourbouli, M.; Stefanis, L.; Kapaki, E. Cerebrospinal fluid biomarker profiling in corticobasal degeneration: Application of the AT(N) and other classification systems. Parkinsonism Relat. Disord. 2021, 82, 44–49. [Google Scholar] [CrossRef] [PubMed]
- Gorno-Tempini, M.L.; Hillis, A.E.; Weintraub, S.; Kertesz, A.; Mendez, M.; Cappa, S.F.; Ogar, J.M.; Rohrer, J.D.; Black, S.; Boeve, B.F.; et al. Classification of primary progressive aphasia and its variants. Neurology 2011, 76, 1006–1014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armstrong, M.J.; Litvan, I.; Lang, A.E.; Bak, T.H.; Bhatia, K.P.; Borroni, B.; Boxer, A.L.; Dickson, D.W.; Grossman, M.; Hallett, M.; et al. Criteria for the diagnosis of corticobasal degeneration. Neurology 2013, 80, 496–503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paraskevas, G.P.; Kasselimis, D.; Kourtidou, E.; Constantinides, V.; Bougea, A.; Potagas, C.; Evdokimidis, I.; Kapaki, E. Cerebrospinal Fluid Biomarkers as a Diagnostic Tool of the Underlying Pathology of Primary Progressive Aphasia. J. Alzheimers Dis. 2017, 55, 1453–31461. [Google Scholar] [CrossRef] [PubMed]
- Bech-Azeddine, R.; Hogh, P.; Juhler, M.; Gjerris, F.; Waldemar, G. Idiopathic normal-pressure hydrocephalus: Clinical comorbidity correlated with cerebral biopsy findings and outcome of cerebrospinal fluid shunting. J. Neurol. Neurosurg. Psychiatry 2007, 78, 157–161. [Google Scholar] [CrossRef] [Green Version]
- Golomb, J.; Wisoff, J.; Miller, D.C.; Boksay, I.; Kluger, A.; Weiner, H.; Salton, J.; Graves, W. Alzheimer’s disease comorbidity in normal pressure hydrocephalus: Prevalence and shunt response. J. Neurol. Neurosurg. Psychiatry 2000, 68, 778–781. [Google Scholar] [CrossRef] [Green Version]
- Hamilton, R.; Patel, S.; Lee, E.B.; Jackson, E.M.; Lopinto, J.; Arnold, S.E.; Clark, C.M.; Basil, A.; Shaw, L.M.; Xie, S.X.; et al. Lack of shunt response in suspected idiopathic normal pressure hydrocephalus with Alzheimer disease pathology. Ann. Neurol. 2010, 68, 535–540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schoonenboom, N.S.; Reesink, F.E.; Verwey, N.A.; Kester, M.I.; Teunissen, C.E.; van de Ven, P.M.; Pijnenburg, Y.A.; Blankenstein, M.A.; Rozemuller, A.J.; Scheltens, P.; et al. Cerebrospinal fluid markers for differential dementia diagnosis in a large memory clinic cohort. Neurology 2012, 78, 47–354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Engelborghs, S.; De Vreese, K.; Van de Casteele, T.; Vanderstichele, H.; Van Everbroeck, B.; Cras, P.; Martin, J.J.; Vanmechelen, E.; De Deyn, P.P. Diagnostic performance of a CSF-biomarker panel in autopsy-confirmed dementia. Neurobiol. Aging 2008, 29, 1143–1159. [Google Scholar] [CrossRef]
- Benvenutto, A.; Guedj, E.; Felician, O.; Eusebio, A.; Azulay, J.P.; Ceccaldi, M.; Koric, L. Clinical Phenotypes in Corticobasal Syndrome with or without Amyloidosis Biomarkers. J. Alzheimers Dis. 2020, 74, 331–343. [Google Scholar] [CrossRef] [PubMed]
- Winkel, I.; Ermann, N.; Żelwetro, A.; Sambor, B.; Mroczko, B.; Kornhuber, J.; Paradowski, B.; Lewczuk, P. Cerebrospinal fluid α synuclein concentrations in patients with positive AD biomarkers and extrapyramidal symptoms. J. Neural Transm. 2021, 128, 817–825. [Google Scholar] [CrossRef] [PubMed]
- Wallin, A.; Kapaki, E.; Boban, M.; Engelborghs, S.; Hermann, D.M.; Huisa, B.; Jonsson, M.; Kramberger, M.G.; Lossi, L.; Malojcic, B.; et al. Biochemical markers in vascular cognitive impairment associated with subcortical small vessel disease—A consensus report. BMC Neurol. 2017, 17, 102. [Google Scholar] [CrossRef] [PubMed]
- Bommarito, G.; Van De Ville, D.; Frisoni, G.B.; Garibotto, V.; Ribaldi, F.; Stampacchia, S.; Assal, F.; Allali, G.; Griffa, A. Alzheimer’s Disease Biomarkers in Idiopathic Normal Pressure Hydrocephalus: Linking Functional Connectivity and Clinical Outcome. J. Alzheimers Dis. 2021. [Google Scholar] [CrossRef] [PubMed]
- Stiffel, M.; Bergeron, D.; Amari, K.M.; Poulin, É.; Roberge, X.; Meilleur-Durand, S.; Sellami, L.; Molin, P.; Nadeau, Y.; Fortin, M.P.; et al. Use of Alzheimer’s Disease Cerebrospinal Fluid Biomarkers in A Tertiary Care Memory Clinic. Can. J. Neurol. Sci. 2021, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.; Lee, E.B.; Xie, S.X.; Law, A.; Jackson, E.M.; Arnold, S.E.; Clark, C.M.; Shaw, L.M.; Grady, M.S.; Trojanowski, J.Q.; et al. Phosphorylated tau/amyloid beta 1–42 ratio in ventricular cerebrospinal fluid reflects outcome in idiopathic normal pressure hydrocephalus. Fluids Barriers C.N.S. 2012, 9, 7. [Google Scholar] [CrossRef] [Green Version]
- Contador, J.; Pérez-Millán, A.; Tort-Merino, A.; Balasa, M.; Falgàs, N.; Olives, J.; Castellví, M.; Borrego-Écija, S.; Bosch, B.; Fernández-Villullas, G.; et al. Longitudinal brain atrophy and CSF biomarkers in early-onset Alzheimer’s disease. Neuroimage Clin. 2021, 32, 102804. [Google Scholar] [CrossRef] [PubMed]
- Gouilly, D.; Tisserand, C.; Nogueira, L.; Saint-Lary, L.; Rousseau, V.; Benaiteau, M.; Rafiq, M.; Carlier, J.; Milongo-Rigal, E.; Pagès, J.C.; et al. Taking the A Train? Limited Consistency of Aβ42 and the Aβ42/40 Ratio in the AT(N) Classification. J. Alzheimers Dis. 2021. [Google Scholar] [CrossRef] [PubMed]
- Lewczuk, P.; Lelental, N.; Spitzer, P.; Maler, J.M.; Kornhuber, J. Amyloid-β 42/40 CSF concentration ratio in the diagnostics of Alzheimer’s disease: Validation of two novel assays. J. Alzheimers Dis. 2015, 43, 183–191. [Google Scholar] [CrossRef]
- Mattsson, N.; Andreasson, U.; Persson, S.; Arai, H.; Batish, S.D.; Bernardini, S.; Bocchio-Chiavetto, L.; Blankenstein, M.A.; Carrillo, M.C.; Chalbot, S.; et al. The Alzheimer’s Association external quality control program for cerebrospinal fluid biomarkers. Alzheimers Dement. 2011, 7, 386–395. [Google Scholar] [CrossRef] [Green Version]
- Mattsson, N.; Andreasson, U.; Persson, S.; Carrillo, M.C.; Collins, S.; Chalbot, S.; Cutler, N.; Dufour-Rainfray, D.; Fagan, A.M.; Heegaard, N.H.; et al. CSF biomarker variability in the Alzheimer’s Association quality control program. Alzheimers Dement. 2013, 9, 251–261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- EU Joint Programme—Neurodegenerative Disease Research. Biomarkers for Alzheimer’s Disease and Parkinson’s Disease (BIOMARKAPD). Available online: https://www.neurodegenerationresearch.eu/fileadmin/Project_Fact_Sheets/PDFs/Biomarkers/BIOMARKAPD_Fact_Sheet_Template.pdf (accessed on 11 September 2021).
- Niemantsverdriet, E.; Goossens, J.; Struyfs, H.; Martin, J.J.; Goeman, J.; De Deyn, P.P.; Vanderstichele, H.; Engelborghs, S. Diagnostic Impact of Cerebrospinal Fluid Biomarker (Pre-)Analytical Variability in Alzheimer’s Disease. J. Alzheimers Dis. 2016, 51, 97–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vogelgsang, J.; Vukovich, R.; Wedekind, D.; Wiltfang, J. Higher Level of Mismatch in APOEε4 Carriers for Amyloid-Beta Peptide Alzheimer’s Disease Biomarkers in Cerebrospinal Fluid. ASN Neuro. 2019, 11, 1759091419845524. [Google Scholar] [CrossRef]
- Toledo, J.B.; Brettschneider, J.; Grossman, M.; Arnold, S.E.; Hu, W.T.; Xie, S.X.; Lee, V.M.; Shaw, L.M.; Trojanowski, J.Q. CSF biomarkers cutoffs: The importance of coincident neuropathological diseases. Acta Neuropathol. 2012, 124, 23–35. [Google Scholar] [CrossRef] [Green Version]
- Piccio, L.; Deming, Y.; Del-Águila, J.L.; Ghezzi, L.; Holtzman, D.M.; Fagan, A.M.; Fenoglio, C.; Galimberti, D.; Borroni, B.; Cruchaga, C. Cerebrospinal fluid soluble TREM2 is higher in Alzheimer disease and associated with mutation status. Acta Neuropathol. 2016, 131, 925–933. [Google Scholar] [CrossRef]
- Kester, M.I.; Teunissen, C.E.; Sutphen, C.L.; Herries, E.M.; Ladenson, J.H.; Xiong, C.; Scheltens, P.; Van Der Flier, W.M.; Morris, J.C.; Holtzman, D.M.; et al. Cerebrospinal fluid VILIP-1 and YKL-40, candidate biomarkers to diagnose, predict and monitor Alzheimer’s disease in a memory clinic cohort. Alzheimer Res. 2015, 7, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Suárez-Calvet, M.; Capell, A.; Caballero, M.; Ángel, A.; Morenas-Rodríguez, E.; Fellerer, K.; Franzmeier, N.; Kleinberger, G.; Eren, E.; Deming, Y.; et al. CSF progranulin increases in the course of Alzheimer’s disease and is associated with sTREM 2, neurodegeneration and cognitive decline. EMBO Mol. Med. 2018, 10, e9712. [Google Scholar] [CrossRef]
- Wellington, H.; Paterson, R.W.; Portelius, E.; Törnqvist, U.; Magdalinou, N.; Fox, N.C.; Blennow, K.; Schott, J.M.; Zetterberg, H. Increased CSF neurogranin concentration is specific to Alzheimer disease. Neurology 2016, 86, 829–835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, A.; Rao, M.V.; Nixon, R.A. Neurofilaments and Neurofilament Proteins in Health and Disease. Cold Spring Harb. Perspect. Biol. 2017, 9, a018309. [Google Scholar] [CrossRef] [Green Version]
- McKeever, P.M.; Schneider, R.; Taghdiri, F.; Weichert, A.; Multani, N.; Brown, R.A.; Boxer, A.L.; Karydas, A.; Miller, B.; Robertson, J.; et al. MicroRNA Expression Levels Are Altered in the Cerebrospinal Fluid of Patients with Young-Onset Alzheimer’s Disease. Mol. Neurobiol. 2018, 55, 8826–8841. [Google Scholar] [CrossRef] [Green Version]
- Phan, L.M.; Cho, S. A Multi-Chamber Paper-Based Platform for the Detection of Amyloid β Oligomers 42 via Copper-Enhanced Gold Immunoblotting. Biomolecules 2021, 11, 948. [Google Scholar] [CrossRef] [PubMed]
- Mollenhauer, B.; El-Agnaf, O.M.; Marcus, K.; Trenkwalder, C.; Schlossmacher, M.G. Quantification of α-synuclein in cerebrospinal fluid as a biomarker candidate: Review of the literature and considerations for future studies. Biomark. Med. 2010, 4, 683–699. [Google Scholar] [CrossRef] [PubMed]
- Junttila, A.; Kuvaja, M.; Hartikainen, P.; Siloaho, M.; Helisalmi, S.; Moilanen, V.; Kiviharju, A.; Jansson, L.; Tienari, P.J.; Remes, A.M.; et al. Cerebrospinal fluid TDP-43 in frontotemporal lobar degeneration and amyotrophic lateral sclerosis patients with and without the C9ORF72 hexanucleotide expansion. Dement. Geriatr. Cogn. Dis. Extra 2016, 6, 142–149. [Google Scholar] [CrossRef]
- Chalatsa, I.; Melachroinou, K.; Emmanouilidou, E.; Vekrellis, K. Assesment of cerebrospinal fluid α-synuclein as a potential biomarker in Parkinson’s disease and synucleinopathies. Neuroimmunol. Neuroinflammation 2020, 7, 132–140. [Google Scholar]
- Oeckl, P.; Metzger, F.; Nagl, M.; von Arnim, C.A.; Halbgebauer, S.; Steinacker, P.; Ludolph, A.C.; Otto, M. Alpha-, Beta-, and Gamma-synuclein Quantification in Cerebrospinal Fluid by Multiple Reaction Monitoring Reveals Increased Concentrations in Alzheimer’s and Creutzfeldt-Jakob Disease but No Alteration in Synucleinopathies. Mol. Cell Proteom. 2016, 15, 3126–3138. [Google Scholar] [CrossRef] [Green Version]
- Li, J.Q.; Bi, Y.L.; Shen, X.N.; Wang, H.F.; Xu, W.; Tan, C.C.; Dong, Q.; Wang, Y.J.; Tan, L.; Yu, J.T.; et al. Cerebrospinal fluid α-synuclein predicts neurodegeneration and clinical progression in non-demented elders. Transl. Neurodegener. 2020, 9, 41. [Google Scholar] [CrossRef] [PubMed]
- Halbgebauer, S.; Oeckl, P.; Steinacker, P.; Yilmazer-Hanke, D.; Anderl-Straub, S.; von Arnim, C.; Froelich, L.; Gomes, L.A.; Hausner, L.; Huss, A.; et al. Beta-synuclein in cerebrospinal fluid as an early diagnostic marker of Alzheimer’s disease. J. Neurol. Neurosurg. Psychiatry. 2020. [Google Scholar] [CrossRef]
- Shim, K.H.; Kang, M.J.; Suh, J.W.; Pyun, J.M.; Ryoo, N.; Park, Y.H.; Youn, Y.C.; Jang, J.W.; Jeong, J.H.; Park, K.W.; et al. CSF total tau/α-synuclein ratio improved the diagnostic performance for Alzheimer’s disease as an indicator of tau phosphorylation. Alzheimers Res. Ther. 2020, 12, 83. [Google Scholar] [CrossRef]
- Alcolea, D.; Delaby, C.; Muñoz, L.; Torres, S.; Estellés, T.; Zhu, N.; Barroeta, I.; Carmona-Iragui, M.; Illán-Gala, I.; Santos-Santos, M.Á.; et al. Use of plasma biomarkers for AT(N) classification of neurodegenerative dementias. J. Neurol. Neurosurg. Psychiatry. 2021. [Google Scholar] [CrossRef]
- Ashton, N.J.; Leuzy, A.; Karikari, T.K.; Mattsson-Carlgren, N.; Dodich, A.; Boccardi, M.; Corre, J.; Drzezga, A.; Nordberg, A.; Ossenkoppele, R.; et al. The validation status of blood biomarkers of amyloid and phospho-tau assessed with the 5-phase development framework for AD biomarkers. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 2140–2156. [Google Scholar] [CrossRef]
- Kim, K.Y.; Shin, K.Y.; Chang, K.A. Brain-Derived Exosomal Proteins as Effective Biomarkers for Alzheimer’s Disease: A Systematic Review and Meta-Analysis. Biomolecules 2021, 11, 980. [Google Scholar] [CrossRef] [PubMed]
- Hampel, H.; Cummings, J.; Blennow, K.; Gao, P.; Jack, C.R., Jr.; Vergallo, A. Developing the ATX(N) classification for use across the Alzheimer disease continuum. Nat. Rev. Neurol. 2021, 17, 580–589. [Google Scholar] [CrossRef] [PubMed]
- Blennow, K.; Zetterberg, H. The past and the future of Alzheimer’s disease fluid biomarkers. J. Alzheimers Dis. 2018, 62, 1125–1140. [Google Scholar] [CrossRef] [Green Version]
- Molinuevo, J.L.; Ayton, S.; Batrla, R.; Bednar, M.M.; Bittner, T.; Cummings, J.; Fagan, A.M.; Hampel, H.; Mielke, M.M.; Mikulskis, A.; et al. Current state of Alzheimer’s fluid biomarkers. Acta Neuropathol. 2018, 136, 821–853. [Google Scholar] [CrossRef] [Green Version]
- Álvarez, I.; Diez-Fairen, M.; Aguilar, M.; González, J.M.; Ysamat, M.; Tartari, J.P.; Carcel, M.; Alonso, A.; Brix, B.; Arendt, P.; et al. Added value of cerebrospinal fluid multimarker analysis in diagnosis and progression of dementia. Eur. J. Neurol. 2021, 28, 1142–1152. [Google Scholar] [CrossRef] [PubMed]
- Ossenkoppele, R.; Mattsson, N.; Teunissen, C.E.; Barkhof, F.; Pijnenburg, Y.; Scheltens, P.; van der Flier, W.M.; Rabinovici, G.D. Cerebrospinal fluid biomarkers and cerebral atrophy in distinct clinical variants of probable Alzheimer’s disease. Neurobiol. Aging 2015, 36, 2340–2347. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Patient 1 | Patient 2 | Patient 3 | Patient 4 | |
|---|---|---|---|---|
| Gender | Female | Female | Male | Female |
| Age (years) | 76 | 76 | 81 | 83 |
| Education (years) | 6 | 12 | 12 | 12 |
| Disease duration (years) | 4 | 3 | 4 | 3 |
| ACE-R [37] | 77/100 | 51/100 | 49/100 | 44/100 |
| MMSE [38] | 29/30 | 23/30 | 15/30 | 14/30 |
| IADL [39] | 7/8 | 8/8 | 3/8 | 2/8 |
| 5-words delayed recall [40] | 2 + 3/5 | 0 + 0/5 | 0 + 2/5 | 1 + 1/5 |
| FAB [41] | 9/18 | 10/18 | 5/18 | 3/18 |
| CLOX1 [42] | 9/15 | 12/15 | 0/15 | 4/15 |
| CLOX2 [42] | 10/15 | 12/15 | 0/15 | 6/15 |
| GDS [43] | 5/15 | 4/15 | 3/15 | 2/15 |
| CDR sum of boxes [44] | 1 | 0 | 10 | 12 |
| CDR overall [44] | 0.5 | 0 | 2 | 2 |
| Clinical diagnosis | Incipient dementia (frontal-like?) | PPA logopenic | NPH; VCI | CBS-like; VCI; NPH (?) |
| Aβ42 (pg/mL) (normal > 500) | 492.8 ↓ | 864.5 | 262.1 ↓ | 627.9 |
| Aβ40 (pg/mL) | 13938 | 12185 | NA | 11648 |
| Aβ42/Aβ40 (normal > 0.09) | 0.035 ↓ | 0.071 ↓ | NA | 0.054 ↓ |
| τP-181 (pg/mL) (normal < 60) | 161.6 ↑ | 110.1 ↑ | 62.3 ↑ | 82.6 ↑ |
| τT (pg/mL) (normal < 400) | 557.7 ↑ | 490.5 ↑ | 420.1 ↑ | 427.1 ↑ |
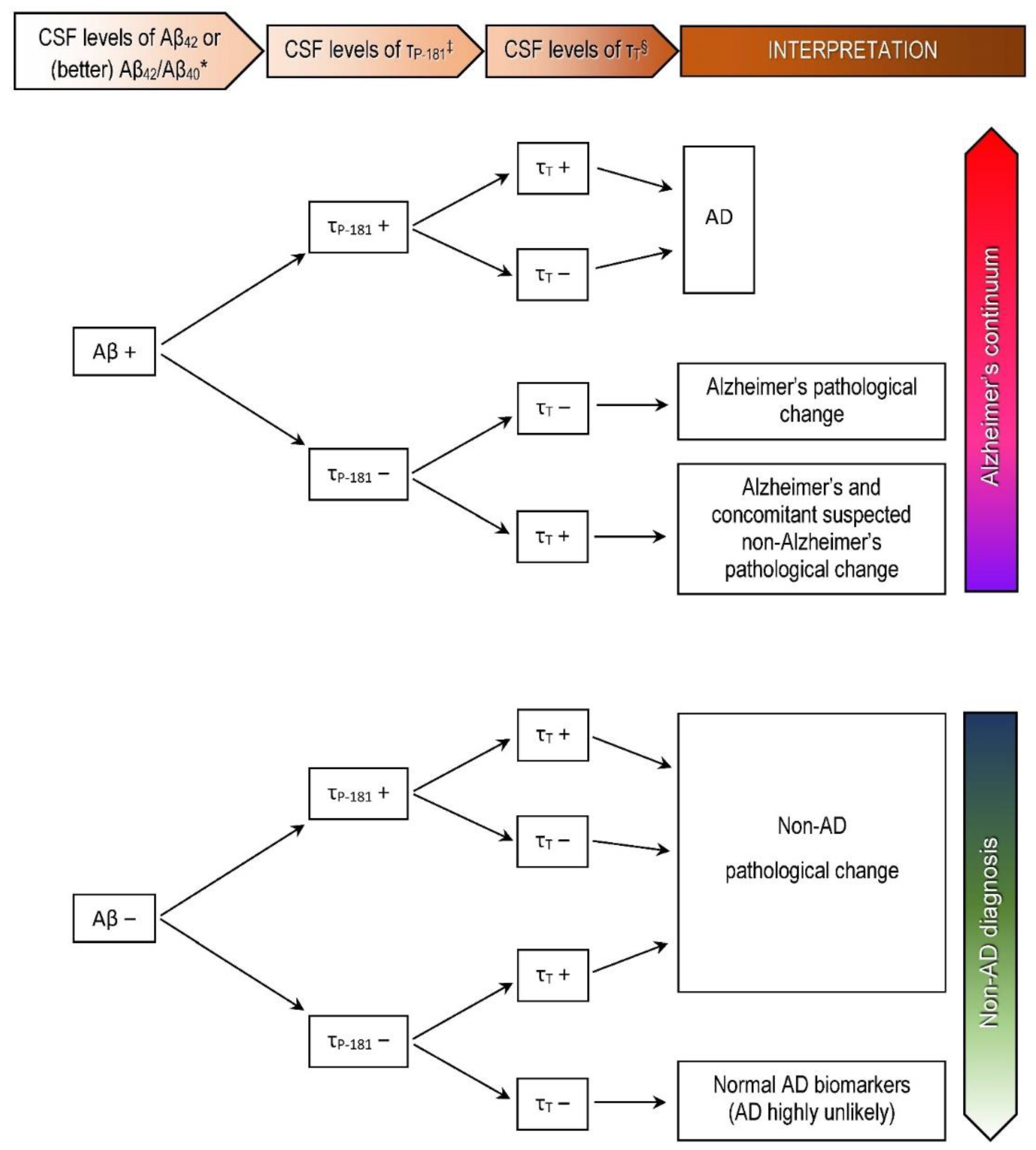
| AT(N) profile [18] | A+T+(N)+ | A+T+(N)+ | A+T+(N)+ | A+T+(N)+ |
| Final diagnosis | AD | AD | NPH + VCI + AD | AD mixed |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsantzali, I.; Boufidou, F.; Sideri, E.; Mavromatos, A.; Papaioannou, M.G.; Foska, A.; Tollos, I.; Paraskevas, S.G.; Bonakis, A.; Voumvourakis, K.I.; et al. From Cerebrospinal Fluid Neurochemistry to Clinical Diagnosis of Alzheimer’s Disease in the Era of Anti-Amyloid Treatments. Report of Four Patients. Biomedicines 2021, 9, 1376. https://doi.org/10.3390/biomedicines9101376
Tsantzali I, Boufidou F, Sideri E, Mavromatos A, Papaioannou MG, Foska A, Tollos I, Paraskevas SG, Bonakis A, Voumvourakis KI, et al. From Cerebrospinal Fluid Neurochemistry to Clinical Diagnosis of Alzheimer’s Disease in the Era of Anti-Amyloid Treatments. Report of Four Patients. Biomedicines. 2021; 9(10):1376. https://doi.org/10.3390/biomedicines9101376
Chicago/Turabian StyleTsantzali, Ioanna, Fotini Boufidou, Eleni Sideri, Antonis Mavromatos, Myrto G. Papaioannou, Aikaterini Foska, Ioannis Tollos, Sotirios G. Paraskevas, Anastasios Bonakis, Konstantinos I. Voumvourakis, and et al. 2021. "From Cerebrospinal Fluid Neurochemistry to Clinical Diagnosis of Alzheimer’s Disease in the Era of Anti-Amyloid Treatments. Report of Four Patients" Biomedicines 9, no. 10: 1376. https://doi.org/10.3390/biomedicines9101376