
Optimized Manufacture of Lyophilized Dermal Fibroblasts for Next-Generation Off-the-Shelf Progenitor Biological Bandages in Topical Post-Burn Regenerative Medicine

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Establishment and Qualification of Dermal FPC Sources in GMP Settings
2.2. Manufacturing Optimization of Dermal FPC Types in GMP Settings
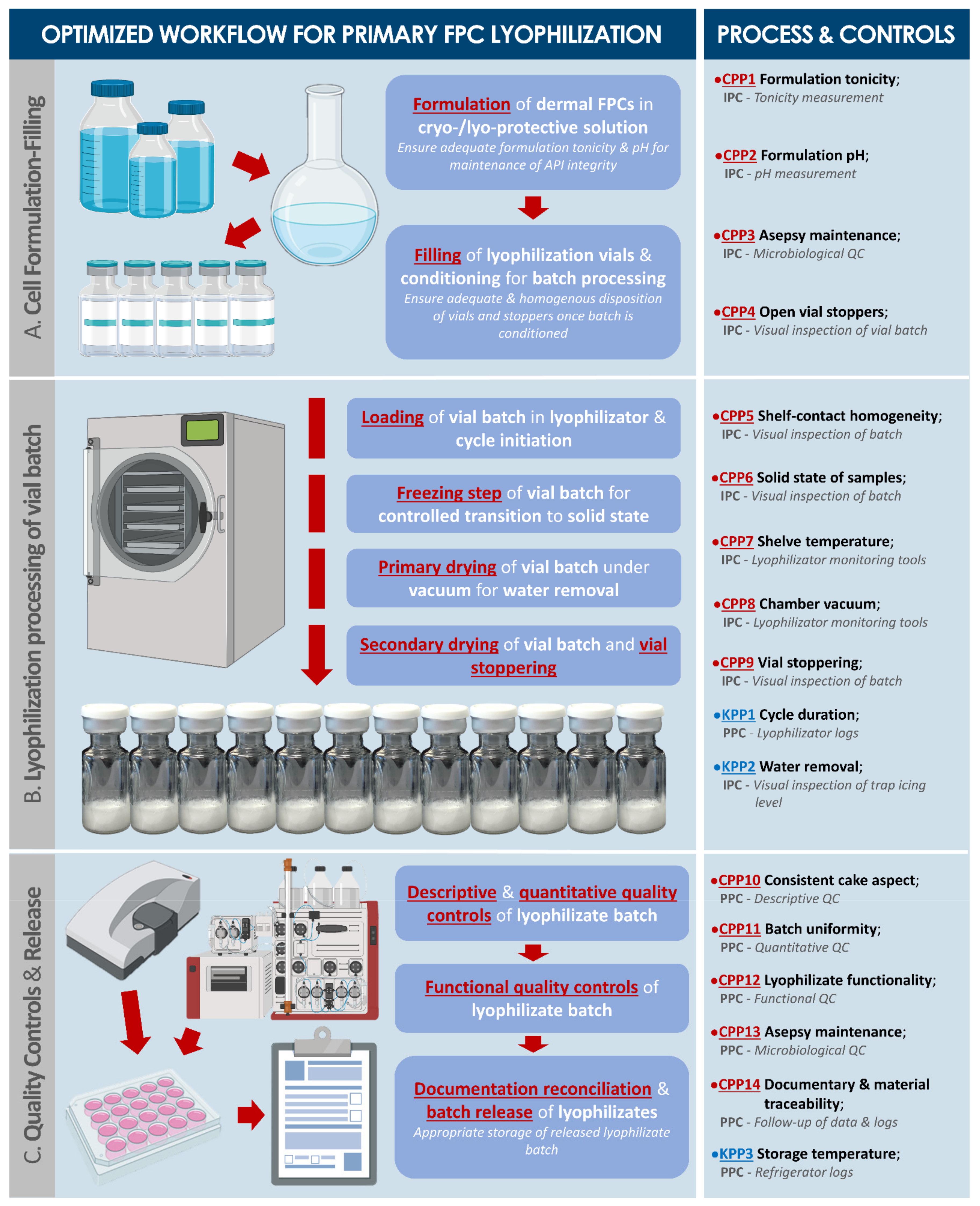
2.3. Optimization of Lyophilization Parameters for Stabilization of Dermal FPCs
2.4. Qualitative and Functional Characterization of Lyophilized Dermal FPCs
2.5. Statistical Analysis
3. Results
3.1. Establishment and Qualification of Dermal FPC Sources in GMP Settings
3.2. Optimization of Technical Specifications for Dermal FPC Industrial GMP Manufacture
3.3. Optimization of Dermal FPC Stabilization by Lyophilization
3.3.1. Protective Formula Benchmarking and Lyophilization Cycle Optimization
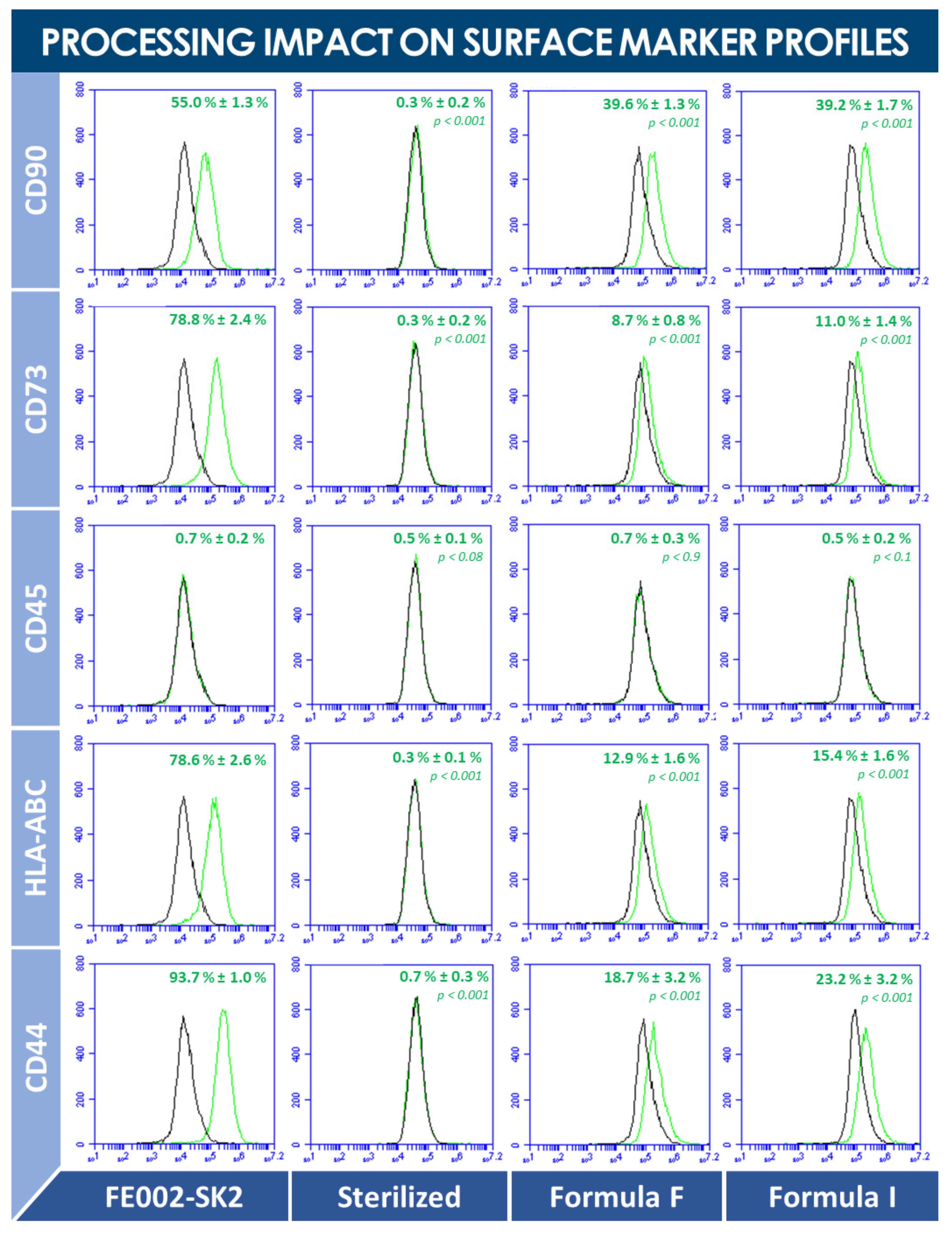
3.3.2. Qualitative and Quantitative Study of Lyophilized Dermal FPCs
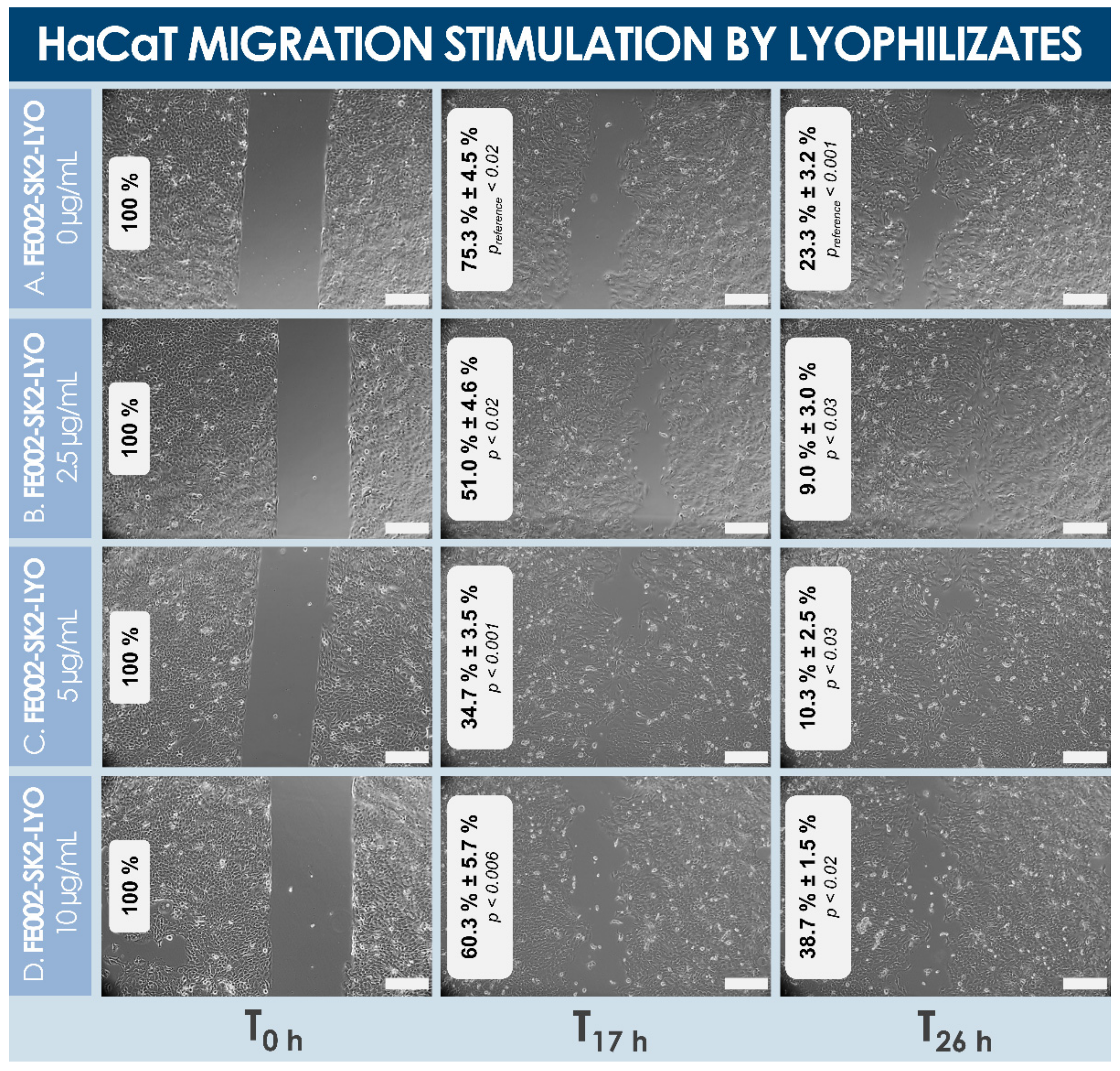
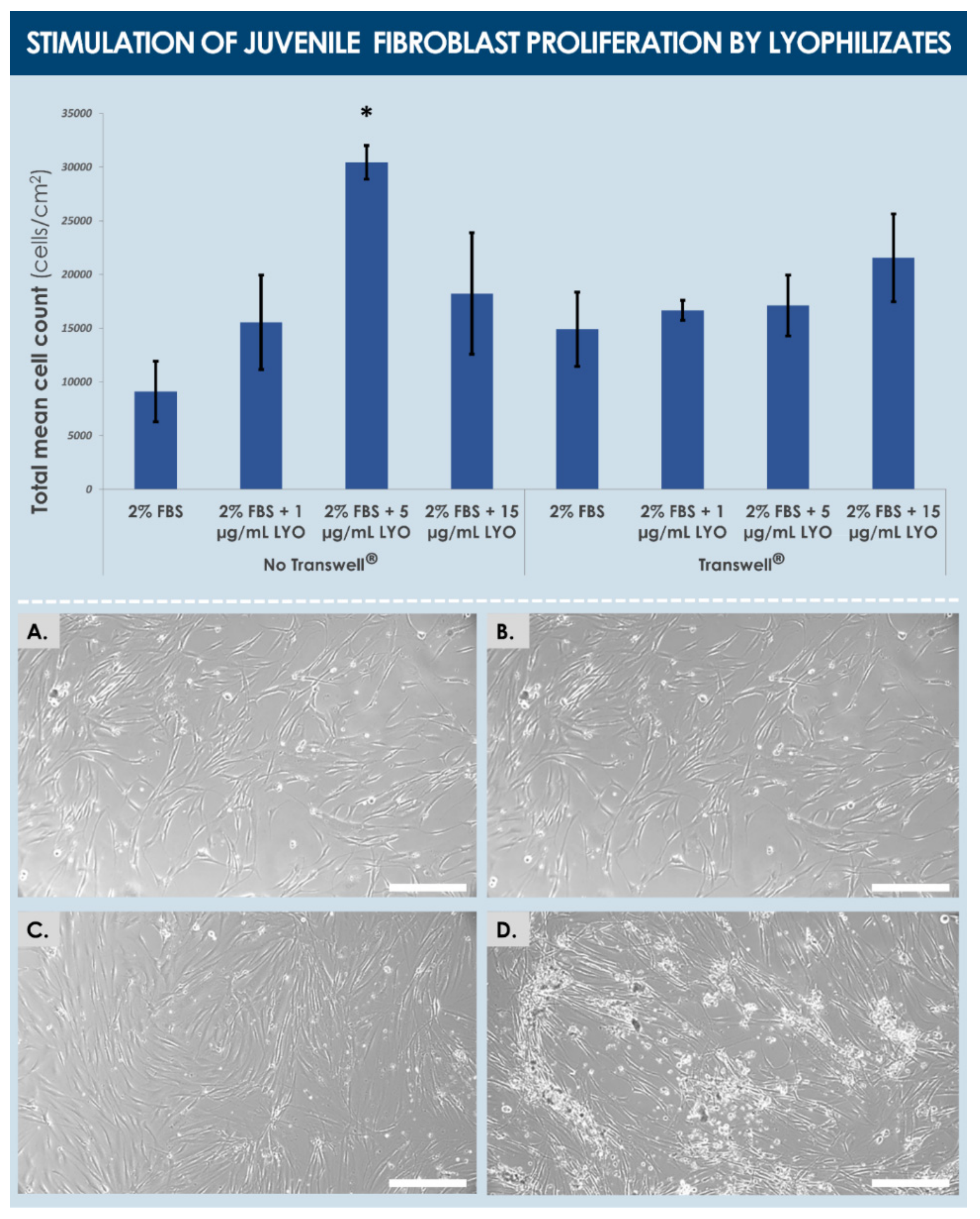
3.3.3. Functional Quality Control of Lyophilized Dermal FPCs
4. Discussion
4.1. Optimized Dermal FPC Multi-Tiered Cell Banking for Regenerative Medicine Products
4.2. Benchmarking of Materials and Consumables for Efficient Large-Scale Primary FPC Manufacturing
4.3. Lyophilization as an Effective Stabilization Method for Therapeutic FPC Biological Materials
4.4. Tangible Advantages of Off-the-Shelf FPC-Based Therapeutic Products
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| API | active pharmaceutical ingredient |
| ATMP | advanced therapy medicinal product |
| BCA | bicinchoninic acid assay |
| BPyV | bovine polyomavirus |
| BSA | bovine serum albumin |
| CD | cluster of differentiation |
| CHUV | Centre hospitalier universitaire Vaudois |
| CPP | critical process parameter |
| CQA | critical quality attribute |
| DMEM | Dulbecco’s modified Eagle medium |
| DMSO | dimethyl sulfoxide |
| DNA | deoxyribonucleic acid |
| EBV | Epstein-Barr virus |
| EC | European Commission |
| ECACC | European collection of authenticated cell cultures |
| EDQM | European Directorate for the Quality of Medicines & Healthcare |
| EDTA | ethylenediaminetetraacetic acid |
| ELISA | enzyme-linked immunosorbent assay |
| EOPCB | end of production cell bank |
| EP | European Pharmacopoeia |
| ESC | embryonic stem cells |
| FACS | fluorescence activated cell-sorting |
| FBS | fetal bovine serum |
| FDA | US Food and Drug Administration |
| FPC | fibroblast progenitor cells |
| FT | freeze-thaw |
| GMP | good manufacturing practices |
| HAV | hepatitis A virus |
| HBV | hepatitis B virus |
| HBoV | human bocavirus |
| hCMV | human cytomegalovirus |
| HCV | hepatitis C virus |
| HHV | human herpes virus |
| HIV | human immunodeficiency virus |
| HPV | human papilloma virus |
| HTLV | human T-cell lymphotropic virus |
| IPC | in-process control |
| KIPyV | KI polyomavirus |
| KPP | key process parameter |
| LYO | lyophilizate |
| MCB | master cell bank |
| MoA | mechanism of action |
| MSC | mesenchymal stem cells |
| PBB | Progenitor Biological Bandage |
| PBS | phosphate-buffered saline |
| PCB | parental cell bank |
| PDT | population doubling time |
| PDV | population doubling value |
| PPC | post-process control |
| RH | relative humidity |
| SD | standard deviation |
| SV40 | simian virus 40 |
| TEM | transmission electron microscopy |
| TEP | tissue engineering product |
| TrSt | standardized transplant product |
| USA | United States of America |
| WCB | working cell bank |
| WUPyV | WU polyomavirus |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Formula ID | Individual Components of Cryo- and Lyo-Protective Solutions Used for Lyophilization of FPCs | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Saccharose | Mannitol | Lactose | Dextran | PVP | DMSO | PBS | NaCl | Water | |
| A | 5 | 2 | 3 | 0 | 0 | 0.2 | 0 | 0 | Ad. 100 |
| B | 5 | 1 | 4 | 0 | 0 | 0.2 | 0 | 0 | Ad. 100 |
| C | 5 | 0 | 3 | 2 | 0 | 0.2 | 0 | 0 | Ad. 100 |
| D | 5 | 0 | 3 | 0 | 2 | 0.2 | 0 | 0 | Ad. 100 |
| E | 6.5 | 0 | 0 | 3.5 | 0 | 0.2 | 0 | 0 | Ad. 100 |
| F | 6.5 | 3.5 | 0 | 0 | 0 | 0.2 | 0 | 0 | Ad. 100 |
| G | 6.5 | 0 | 0 | 0 | 3.5 | 0.2 | 0 | 0 | Ad. 100 |
| H | 6.5 | 0 | 3.5 | 0 | 0 | 0.2 | 0 | 0 | Ad. 100 |
| I | 8 | 0 | 0 | 2 | 0 | 0.2 | 0 | 0 | Ad. 100 |
| J | 8 | 0 | 0 | 0 | 2 | 0.2 | 0 | 0 | Ad. 100 |
| K | 0 | 0 | 0 | 0 | 0 | 2 | 0 | 0 | Ad. 100 |
| L | 0 | 0 | 0 | 0 | 0 | 10 | 0 | 0 | Ad. 100 |
| M | 0 | 0 | 0 | 0 | 0 | 0 | 100 | 0 | 0 |
| N | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 100 | 0 |
| Process Phase ID | Investigated Parameter | Lyophilization Formula ID | ||
|---|---|---|---|---|
| N°B | N°F | N°I | ||
| Freezing/cooling phase | Subcooling temperature (°C) | −11 ± 2 | −13 ± 2 | −12 ± 2 |
| Crystallization temperature (°C) | −2 ± 2 | −2 ± 2 | −2 ± 2 | |
| Temperature when Zsinφ = 0 MΩ (°C) | −7 ± 2 | −10 ± 2 | −10 ± 2 | |
| Temperature when Zsinφ = 1 MΩ (°C) | −15 ± 2 | −16 ± 2 | −18 ± 2 | |
| Heating phase | Temperature at beginning of fusion (°C) | −10 ± 2 | −11 ± 2 | −11 ± 2 |
| Temperature when Zsinφ = 0 MΩ (°C) | −4 ± 2 | −3 ± 2 | −3 ± 2 | |
| Temperature when Zsinφ = 1 MΩ (°C) | −13 ± 2 | −14 ± 2 | −11 ± 2 | |
| Process Phase ID | Optimized Parameters (Temperature, Pressure, and Time) |
|---|---|
| A. Loading | Ambient temperature; 1 atm |
| B. Freezing | −45 °C; 1 atm; 2 h |
| C. Chamber vacuum | 0.08 mbar |
| D. Primary drying | Ramp from −10 °C to −30 °C and then ramp from −30 °C to 25 °C; 0.08 mbar; 39 h |
| E. Secondary drying | Ramp from 25 °C to 20 °C; maximal vacuum; 9 h |
References
- Johnson, P.C.; Bertram, T.A.; Tawil, B.; Hellman, K.B. Hurdles in tissue engineering/regenerative medicine product commercialization: A survey of North American academia and industry. Tissue Eng. Part A 2011, 17, 5–15. [Google Scholar] [CrossRef]
- Voltz-Girolt, C.; Celis, P.; Boucaumont, M.; D’Apote, L.; Pinheiro, M.H.; Papaluca-Amati, M. The advanced therapy classification procedure. Overview of experience gained so far. Bundesgesundheitsblatt-Gesundheitsforschung-Gesundheitsschutz 2011, 54, 811–815. [Google Scholar] [CrossRef]
- Bertram, T.A.; Tentoff, E.; Johnson, P.C.; Tawil, B.; Van Dyke, M.; Hellman, K.B. Hurdles in tissue engineering/regenerative medicine product commercialization: A pilot survey of governmental funding agencies and the financial industry. Tissue Eng. Part A 2012, 18, 2187–2194. [Google Scholar] [CrossRef] [PubMed]
- Fisher, M.B.; Mauck, R.L. Tissue engineering and regenerative medicine: Recent innovations and the transition to translation. Tissue Eng. Part B 2013, 19, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Gaspar, B.; Swift, S. ‘Special Exemptions’: Should they be put on trial? Mol. Ther. 2013, 21, 261–262. [Google Scholar] [CrossRef] [Green Version]
- Pirnay, J.P.; Vanderkelen, A.; De Vos, D.; Draye, J.P.; Rose, T.; Ceulemans, C.; Ectors, N.; Huys, I.; Jennes, S.; Verbeken, G. Business oriented EU human cell and tissue product legislation will adversely impact Member States’ health care systems. Cell Tissue Bank 2013, 14, 525–560. [Google Scholar] [CrossRef] [PubMed]
- Cuende, N.; Boniface, C.; Bravery, C.; Forte, M.; Giordano, R.; Hildebrandt, M.; Izeta, A.; Dominici, M. Legal and Regulatory Affairs Committee—Europe, International Society for Cellular Therapy. The puzzling situation of hospital exemption for advanced therapy medicinal products in Europe and stakeholders’ concerns. Cryotherapy 2014, 16, 1597–1600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pearce, K.F.; Hildebrandt, M.; Greinix, H.; Scheding, S.; Koehl, U.; Worel, N.; Apperley, J.; Edinger, M.; Hauser, A.; Mischak-Weissinger, E.; et al. Regulation of advanced therapy medicinal products in Europe and the role of academia. Cytotherapy 2014, 16, 289–297. [Google Scholar] [CrossRef] [Green Version]
- De Wilde, S.; Veltrop-Duits, L.; Hoozemans-Strik, M.; Ras, T.; Blom-Veenman, J.; Guchelaar, H.J.; Zandvliet, M.; Meij, P. Hurdles in clinical implementation of academic Advanced Therapy Medicinal Product: A national evaluation. Cythotherapy 2016, 18, 797–805. [Google Scholar] [CrossRef]
- Dimitropoulos, G.; Jafari, P.; De Buys Roessingh, A.S.; Hirt-Burri, N.; Raffoul, W.; Applegate, L.A. Burn patient care lost in Good Manufacturing Practices? Ann. Burns Fire Disaster 2016, 29, 111–115. [Google Scholar]
- Ramezankhani, R.; Torabi, S.; Minaei, N.; Madani, H.; Rezaeiani, S.; Hassani, S.N.; Gee, A.P.; Dominici, M.; Silva, D.N.; Baharvand, H.; et al. Two decades of global progress in authorized advanced therapy medicinal products: An emerging revolution in therapeutic strategies. Front. Cell Dev. Biol. 2020, 8, 547653. [Google Scholar] [CrossRef]
- Iglesias-Lopez, C.; Obach, M.; Vallano, A.; Agustí, A. Comparison of regulatory pathways for the approval of advanced therapies in the European Union and the United States. Cytotherapy 2021, 23, 261–274. [Google Scholar] [CrossRef]
- Green, H. The birth of therapy with cultured cells. BioEssays 2008, 30, 897–903. [Google Scholar] [CrossRef]
- Phinney, D.G.; Pittenger, M.F. Concise review: MSC-derived exosomes for cell-free therapy. Stem Cells 2017, 35, 851–858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doyle, L.M.; Wang, M.Z. Overview of extracellular vesicles, their origin, composition, purpose, and methods for exosome isolation and analysis. Cells 2019, 8, 727. [Google Scholar] [CrossRef] [Green Version]
- Lenihan, C.; Rogers, C.; Metcalfe, A.D.; Martin, Y.H. The effect of isolation and culture methods on epithelial stem cell populations and their progeny-toward an improved cell expansion protocol for clinical application. Cytotherapy 2014, 16, 1750–1759. [Google Scholar] [CrossRef] [PubMed]
- Marks, P.; Gottlieb, S. Balancing safety and innovation for cell-based regenerative medicine. N. Engl. J. Med. 2018, 378, 954–959. [Google Scholar] [CrossRef] [PubMed]
- Doulgkeroglou, M.N.; Di Nubila, A.; Niessing, B.; König, N.; Schmitt, R.H.; Damen, J.; Szilvassy, S.J.; Chang, W.; Csontos, L.; Louis, S.; et al. Automation, monitoring, and standardization of cell product manufacturing. Front. Bioeng. Biotechnol. 2020, 8, 811. [Google Scholar] [CrossRef]
- Lavrentieva, A.; Hoffmann, A.; Lee-Thedieck, C. Limited potential or unfavorable manipulations? Strategies toward efficient mesenchymal stem/stromal cell applications. Front. Cell Dev. Biol. 2020, 8, 316. [Google Scholar] [CrossRef] [PubMed]
- Hohlfeld, J.; de Buys Roessingh, A.S.; Hirt-Burri, N.; Chaubert, P.; Gerber, S.; Scaletta, C.; Holhlfeld, P.; Applegate, L.A. Tissue engineered fetal skin constructs for pediatric burns. Lancet 2005, 366, 840–842. [Google Scholar] [CrossRef]
- De Buys Roessingh, A.S.; Hohlfeld, J.; Scaletta, C.; Hirt-Burri, N.; Gerber, S.; Hohlfeld, P.; Gebbers, J.O.; Applegate, L.A. Development, characterization, and use of a fetal skin cell bank for tissue engineering in wound healing. Cell Transplant. 2006, 15, 823–834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quintin, A.; Hirt-Burri, N.; Scaletta, C.; Schizas, C.; Pioletti, D.P.; Applegate, L.A. Consistency and safety of cell banks for research and clinical use: Preliminary analysis of fetal skin banks. Cell Transplant. 2007, 16, 675–684. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramelet, A.A.; Hirt-Burri, N.; Raffoul, W.; Scaletta, C.; Pioletti, D.P.; Offord, E.; Mansourian, R.; Applegate, L.A. Chronic wound healing by fetal cell therapy may be explained by differential gene profiling observed in fetal versus old skin cells. Exp. Gerontol. 2009, 44, 208–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Buys Roessingh, A.S.; Hirt-Burri, N.; Raffoul, W.; Scaletta, C.; Applegate, L.A. A decade after fetal skin progenitor cell therapy in pediatric burn treatment. J. Regen. Med. 2015, 4, 1. [Google Scholar] [CrossRef]
- Laurent, A.; Lin, P.; Scaletta, C.; Hirt-Burri, N.; Michetti, M.; De Buys Roessingh, A.S.; Raffoul, W.; She, B.R.; Applegate, L.A. Bringing safe and standardized cell therapies to industrialized processing for burns and wounds. Front. Bioeng. Biotechnol. 2020, 8, 581. [Google Scholar] [CrossRef]
- Laurent, A.; Hirt-Burri, N.; Scaletta, C.; Michetti, M.; Raffoul, W.; De Buys Roessingh, A.S.; Applegate, L.A. Holistic approach of Swiss fetal progenitor cell banking: Optimizing safe and sustainable substrates for regenerative medicine and biotechnology. Front. Bioeng. Biotechnol. 2020, 8, 557758. [Google Scholar] [CrossRef]
- Abdel-Sayed, P.; Hirt-Burri, N.; De Buys Roessingh, A.S.; Raffoul, W.; Applegate, L.A. Evolution of biological bandages as first cover for burn patients. Adv. Wound Care 2019, 8, 555–564. [Google Scholar] [CrossRef]
- Dwenger, A.; Strassburger, J.; Schwerdtfeger, W. European Parliament and Council. Regulation (EC) No 1394/2007 on Advanced Therapy Medicinal Products and amending Directive 2001/83/EC and Regulation (EC) No 726/2004. Off. J. Eur. Union 2007, 53, 14–19. [Google Scholar]
- Switzerland’s Federal Council. Federal Assembly of the Swiss Confederation: Federal Act on the Transplantation of Organs, Tissues and Cells (Transplantation Act); SR 810: 21; Switzerland’s Federal Council: Bern, Switzerland, 2004.
- Hayflick, L.; Plotkin, S.A.; Norton, T.W.; Koprowski, H. Preparation of poliovirus vaccines in a human fetal diploid cell strain. Am. J. Hyg. 1962, 75, 240–258. [Google Scholar] [CrossRef]
- European Directorate for the Quality of Medicines & Health Care. General Chapter 5.2.3. “Cell Substrates for the Production of Vaccines for Human Use”. In European Pharmacopoeia; EDQM, Ph. Eur. Version 6.0.; European Directorate for the Quality of Medicines & HealthCare: Strasbourg, France, 2008. [Google Scholar]
- Verbeken, G.; Draye, J.P.; Fauconnier, A.; Vanlaere, I.; Huys, I.; De Corte, P.; Verween, G.; Pascual, B.; Delmotte, N.; Pierlot, A.; et al. The magistral preparation of Advanced Therapy Medicinal Products (ATMPs). J. Surg. Pract. 2020, 2, 16. [Google Scholar]
- Hayflick, L. The limited in vitro lifetime of human diploid cell strains. Exp. Cell Res. 1965, 37, 614–636. [Google Scholar] [CrossRef]
- Jacobs, J.P.; Jones, C.M.; Baille, J.P. Characteristics of a human diploid cell designated MRC-5. Nature 1970, 227, 168–170. [Google Scholar] [CrossRef]
- Ma, B.; He, L.F.; Zhang, Y.L.; Chen, M.; Wang, L.L.; Yang, H.W.; Yan, T.; Sun, M.X.; Zheng, C.Y. Characteristics and viral propagation properties of a new human diploid cell line, Walvax-2, and its suitability as a candidate cell substrate for vaccine production. Hum. Vaccines Immunother. 2015, 11, 998–1009. [Google Scholar] [CrossRef] [PubMed]
- Al-Dourobi, K.; Laurent, A.; Deghayli, L.; Flahaut, M.; Abdel-Sayed, P.; Scaletta, C.; Michetti, M.; Waselle, L.; Simon, J.P.; Ezzi, O.E.; et al. Retrospective evaluation of Progenitor Biological Bandage use: A complementary and safe therapeutic management option for prevention of hypertrophic scarring in pediatric burn care. Pharmaceuticals 2021, 14, 201. [Google Scholar] [CrossRef]
- Ghamari, S.H.; Abbasi-Kangevari, M.; Tayebi, T.; Bahrami, S.; Niknejad, H. The bottlenecks in translating placenta-derived amniotic epithelial and mesenchymal stromal cells into the clinic: Current discrepancies in marker reports. Front. Bioeng. Biotechnol. 2020, 8, 180. [Google Scholar] [CrossRef] [Green Version]
- Kabat, M.; Bobkov, I.; Kumar, S.; Grumet, M. Trends in mesenchymal stem cell clinical trials 2004-2018: Is efficacy optimal in a narrow dose range? Stem Cells Transl. Med. 2020, 9, 17–27. [Google Scholar] [CrossRef] [Green Version]
- Racchi, M.; Govoni, S.; Lucchelli, A.; Capone, L.; Giovagnoni, E. Insights into the definition of terms in European medical device regulation. Exp. Rev. Med. Dev. 2016, 13, 907–917. [Google Scholar] [CrossRef] [PubMed]
- Gatlin, L.A.; Nail, S.L. Protein purification process engineering. Freeze drying: A practical overview. Bioprocess Technol. 1994, 18, 317–367. [Google Scholar]
- Puhlev, I.; Guo, N.; Brown, D.R.; Levine, F. Desiccation tolerance in human cells. Cryobiology 2001, 42, 207–217. [Google Scholar] [CrossRef] [Green Version]
- Massie, I.; Selden, C.; Hodgson, H.; Fuller, B.; Gibbons, S.; Morris, G.J. GMP cryopreservation of large volumes of cells for regenerative medicine: Active control of the freezing process. Tissue Eng. Part C 2014, 20, 693–702. [Google Scholar] [CrossRef] [Green Version]
- Davis, K.E.; Killeen, A.L.; Farrar, D.; Raspovic, K.M.; Berriman-Rozen, Z.D.; Malone, M.; Lavery, L.A. Lyopreserved amniotic membrane is cellularly and clinically similar to cryopreserved construct for treating foot ulcers. Int. Wound J. 2020, 17, 1893–1901. [Google Scholar] [CrossRef]
- Whaley, D.; Damyar, K.; Witek, R.P.; Mendoza, A.; Alexander, M.; Lakey, J.R. Cryopreservation: An overview of principles and cell-specific considerations. Cell Transpl. 2021, 30, 963689721999617. [Google Scholar] [CrossRef] [PubMed]
- El Baradie, K.; Nouh, M.; O’Brien, F., III; Liu, Y.; Fulzele, S.; Eroglu, A.; Hamrick, M.W. Freeze-dried extracellular vesicles from adipose-derived stem cells prevent hypoxia-induced muscle cell injury. Front. Cell Dev. Biol. 2020, 8, 181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soejima, K.; Shimoda, K.; Kashimura, T.; Yamaki, T.; Kono, T.; Sakurai, H.; Nakazawa, H. Wound dressing material containing lyophilized allogeneic cultured cells. Cryobiology 2013, 66, 210–214. [Google Scholar] [CrossRef] [PubMed]
- Strong, D.M. The US Navy Tissue Bank: 50 years on the cutting edge. Cell Tissue Bank 2000, 1, 9–16. [Google Scholar] [CrossRef]
- Kennedy, J.F.; Turan, N. Freeze-Drying/ Lyophilization of pharmaceutical and biological products Louis Rey and Joan, C. May. Bioseparation 2000, 9, 118. [Google Scholar] [CrossRef]
- Pisano, R.; Rasetto, V.; Barresi, A.A.; Kuntz, F.; Aoude-Werner, D.; Rey, L. Freeze-drying of enzymes in case of water-binding and non-water-binding substrates. Eur. J. Pharm. Biopharm. 2013, 85, 974–983. [Google Scholar] [CrossRef] [PubMed]
- Gresham, R.B. Freeze-drying of human tissue for clinical use. Cryobiology 1964, 1, 150–156. [Google Scholar] [CrossRef]
- Daller, S.; Friess, W.; Schroeder, R. Energy transfer in vials nested in a rack system during lyophilization. Pharmaceutics 2020, 12, 61. [Google Scholar] [CrossRef] [Green Version]
- Ehlers, S.; Schroeder, R.; Friess, W. Process optimization and transfer of freeze-drying in nested vial systems. Eur. J. Pharm. Biopharm. 2021, 159, 143–150. [Google Scholar] [CrossRef]
- Antsiferova, M.; Klatte, J.E.; Bodó, E.; Paus, R.; Jorcano, J.L.; Matzuk, M.M.; Werner, S.; Kögel, H. Keratinocyte-derived follistatin regulates epidermal homeostasis and wound repair. Lab. Investig. 2009, 89, 131–141. [Google Scholar] [CrossRef] [Green Version]
- Akita, S.; Akino, K.; Hirano, A. Basic fibroblast growth factor in scarless wound healing. Adv. Wound Care 2013, 2, 44–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shibuya, M. Vascular endothelial growth factor and its receptor system: Physiological functions in angiogenesis and pathological roles in various diseases. J. Biochem. 2013, 153, 13–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, J.F.; Duan, H.F.; Wu, C.T.; Zhang, D.J.; Deng, Y.; Yin, H.L.; Han, B.; Gong, H.C.; Wang, H.W.; Wang, Y.L. HGF accelerates wound healing by promoting the dedifferentiation of epidermal cells through β1-integrin/ILK pathway. Biomed. Res. Int. 2013, 470418. [Google Scholar] [CrossRef] [Green Version]
- Tadokoro, S.; Ide, S.; Tokuyama, R.; Umeki, H.; Tatehara, S.; Kataoka, S.; Satomura, K. Leptin promotes wound healing in the skin. PLoS ONE 2015, 10, e0121242. [Google Scholar] [CrossRef] [PubMed]
- Frank, S.; Stallmeyer, B.; Kämpfer, H.; Kolb, N.; Pfeilschifter, J. Leptin enhances wound re-epithelialization and constitutes a direct function of leptin in skin repair. J. Clin. Investig. 2000, 106, 501–509. [Google Scholar] [CrossRef] [Green Version]
- Jiang, W.G.; Sanders, A.J.; Ruge, F.; Harding, K.G. Influence of interleukin-8 (IL-8) and IL-8 receptors on the migration of human keratinocytes, the role of PLC-γ and potential clinical implications. Exp. Ther. Med. 2012, 3, 231–236. [Google Scholar] [CrossRef] [Green Version]
- Penn, J.W.; Grobbelaar, A.O.; Rolfe, K.J. The role of the TGF-β family in wound healing, burns and scarring: A review. Int. J. Burns Trauma 2012, 2, 18–28. [Google Scholar]
- Pakyari, M.; Farrokhi, A.; Maharlooei, M.K.; Ghahary, A. Critical role of transforming growth factor beta in different phases of wound healing. Adv. Wound Care 2013, 2, 215–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramirez, H.; Patel, S.B.; Pastar, I. The role of TGFβ signaling in wound epithelialization. Adv. Wound Care 2014, 3, 482–491. [Google Scholar] [CrossRef] [Green Version]
- Scharenberg, M.A.; Pippenger, B.E.; Sack, R.; Zingg, D.; Ferralli, J.; Schenk, S.; Martin, I.; Chiquet-Ehrismann, R. TGF-β-induced differentiation into myofibroblasts involves specific regulation of two MKL1 isoforms. J. Cell Sci. 2014, 127, 1079–1091. [Google Scholar] [CrossRef] [Green Version]
- Grafe, I.; Alexander, S.; Peterson, J.R.; Snider, T.N.; Levi, B.; Lee, B.; Mishina, Y. TGF-β family signaling in mesenchymal differentiation. Cold Spring Harb. Perspect. Biol. 2018, 10, a022202. [Google Scholar] [CrossRef]
- Rho, S.B.; Chung, B.M.; Lee, J.H. TIMP-1 regulates cell proliferation by interacting with the ninth zinc finger domain of PLZF. J. Cell. Biochem. 2007, 101, 57–67. [Google Scholar] [CrossRef]
- Caley, M.P.; Martins, V.L.; O’Toole, E.A. Metalloproteinases and wound healing. Adv. Wound Care 2015, 4, 225–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miyoshi, H.; Kanekura, T.; Aoki, T.; Kanzaki, T. Beneficial effects of tissue inhibitor of metalloproteinases-2 (TIMP-2) on chronic dermatitis. J. Dermatol. 2005, 32, 346–353. [Google Scholar] [CrossRef] [PubMed]
- Bonnans, C.; Chou, J.; Werb, Z. Remodelling the extracellular matrix in development and disease. Nat. Rev. Mol. Cell Biol. 2014, 15, 786–801. [Google Scholar] [CrossRef]
- Jostock, T.; Müllberg, J.; Ozbek, S.; Atreya, R.; Blinn, G.; Voltz, N.; Fischer, M.; Neurath, M.F.; Rose-John, S. Soluble gp130 is the natural inhibitor of soluble interleukin-6 receptor transsignaling responses. Eur. J. Biochem. 2001, 268, 160–167. [Google Scholar] [CrossRef] [PubMed]
- Baran, P.; Hansen, S.; Waetzig, G.H.; Akbarzadeh, M.; Lamertz, L.; Huber, H.J.; Ahmadian, M.R.; Moll, J.M.; Scheller, J. The balance of interleukin (IL)-6, IL-6·soluble IL-6 receptor (sIL-6R), and IL-6·sIL-6R·sgp130 complexes allows simultaneous classic and trans-signaling. J. Biol. Chem. 2018, 293, 6762–6775. [Google Scholar] [CrossRef] [Green Version]
- Rose-John, S. IL-6 trans-signaling via the soluble IL-6 receptor: Importance for the pro-inflammatory activities of IL-6. Int. J. Biol. Sci. 2012, 8, 1237–1247. [Google Scholar] [CrossRef]
- Johnson, K.E.; Wilgus, T.A. Vascular endothelial growth factor and angiogenesis in the regulation of cutaneous wound repair. Adv. Wound Care 2014, 3, 647–661. [Google Scholar] [CrossRef] [Green Version]
- Eming, S.A.; Lauer, G.; Cole, M.; Jurk, S.; Christ, H.; Hornig, C.; Krieg, T.; Weich, H.A. Increased levels of the soluble variant of the vascular endothelial growth factor receptor VEGFR-1 are associated with a poor prognosis in wound healing. J. Investig. Dermatol. 2004, 123, 799–802. [Google Scholar] [CrossRef] [Green Version]
- Jacobi, J.; Tam, B.; Sundram, U.; von Degenfeld, G.; Blau, H.; Kuo, C.; Cooke, J. Discordant effects of a soluble VEGF receptor on wound healing and angiogenesis. Gene Ther. 2004, 11, 302–309. [Google Scholar] [CrossRef] [Green Version]
- Deshmane, S.L.; Kremlev, S.; Amini, S.; Sawaya, B.E. Monocyte chemoattractant protein-1 (MCP-1): An overview. J. Interf. Cytokine Res. 2009, 29, 313–326. [Google Scholar] [CrossRef]
- Ahuja, S.K.; Murphy, P.M. The CXC chemokines growth-regulated oncogene (GRO) alpha, GRObeta, GROgamma, neutrophil-activating peptide-2, and epithelial cell-derived neutrophil-activating peptide-78 are potent agonists for the type B, but not the type A, human interleukin-8 receptor. J. Biol. Chem. 1996, 271, 20545–20550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muehlhoefer, A.; Saubermann, L.J.; Gu, X.; Luedtke-Heckenkamp, K.; Xavier, R.; Blumberg, R.S.; Podolsky, D.K.; MacDermott, R.P.; Reinecker, H.C. Fractalkine is an epithelial and endothelial cell-derived chemoattractant for intraepithelial lymphocytes in the small intestinal mucosa. J. Immunol. 2000, 164, 3368–3376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeisberger, S.M.; Schulz, J.C.; Mairhofer, M.; Ponsaerts, P.; Wouters, G.; Doerr, D.; Katsen-Globa, A.; Ehrbar, M.; Hescheler, J.; Hoerstrup, S.P.; et al. Biological and physicochemical characterization of a serum- and xeno-free chemically defined cryopreservation procedure for adult human progenitor cells. Cell Transplant. 2011, 20, 1241–1257. [Google Scholar] [CrossRef] [PubMed]
- Emami, F.; Vatanara, A.; Park, E.J.; Na, D.H. Drying technologies for the stability and bioavailability of biopharmaceuticals. Pharmaceutics 2018, 10, 131. [Google Scholar] [CrossRef] [Green Version]
- Hanna, J.; Hubel, A. Preservation of stem cells. Organogenesis 2009, 5, 134–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thirumala, S.; Goebel, W.S.; Woods, E.J. Clinical grade adult stem cell banking. Organogenesis 2009, 5, 143–154. [Google Scholar] [CrossRef] [Green Version]
- Hunt, C.J. Cryopreservation of human stem cells for clinical application: A review. Transfus. Med. Hemother. 2011, 38, 107–123. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Ma, T. Bioprocessing of cryopreservation for large-scale banking of human pluripotent stem cells. Biores. Open Access 2012, 1, 205–214. [Google Scholar] [CrossRef] [PubMed]
- Kartoglu, U.H.; Moore, K.L.; Lloyd, J.S. Logistical challenges for potential SARS-CoV-2 vaccine and a call to research institutions, developers and manufacturers. Vaccine 2020, 38, 5393–5395. [Google Scholar] [CrossRef]
- Peng, Y.; Xuan, M.; Zou, J.; Liu, H.; Zhuo, Z.; Wan, Y.; Cheng, B. Freeze-dried rat bone marrow mesenchymal stem cell paracrine factors: A simplified novel material for skin wound therapy. Tissue Eng. Part A 2015, 21, 1036–1046. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahangar, P.; Mills, S.J.; Cowin, A.J. Mesenchymal stem cell secretome as an emerging cell-free alternative for improving wound repair. Int. J. Mol. Sci. 2020, 21, 7038. [Google Scholar] [CrossRef]
- Faruqu, F.N.; Liam-Or, R.; Zhou, S.; Nip, R.; Al-Jamal, K.T. Defined serum-free three-dimensional culture of umbilical cord-derived mesenchymal stem cells yields exosomes that promote fibroblast proliferation and migration in vitro. FASEB J. 2021, 35, e21206. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association. Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [Green Version]









| Optimized Parameter | Considered Indicators and Endpoints | Parameter-Specific Targets | Tested Options | Grading 1 |
|---|---|---|---|---|
| Culture vessel surface (cm2) |
|
| 175 cm2—T175 225 cm2—T225 500 cm2—T500 | +++ +++ + |
| FBS source & lot identity |
|
| Sigma®—lot A Sigma®—lot B Sigma®—lot C Invitrogen®—lot A Invitrogen®—lot B HyClone™—lot A | +++ + +++ ++ – + |
| Seeding densities (viable cells/cm2) |
|
| 1.5 × 103 cells/cm2 3.0 × 103 cells/cm2 5.0 × 103 cells/cm2 104 cells/cm2 | +++ +++ ++ + |
| Culture medium volume (mL/cm2) |
|
| 0.05 mL/cm2 0.10 mL/cm2 0.15 mL/cm2 0.20 mL/cm2 0.25 mL/cm2 0.30 mL/cm2 | – + +++ +++ ++ + |
| Culture periods (days) |
|
| 8 days 10 days 12 days 15 days | – + +++ +++ |
| Parameter | Target | Acceptance Criteria (Cumulative) | Grading of Optimal Formulas | ||
|---|---|---|---|---|---|
| N°B | N°F | N°I | |||
| Presence of cake * |
|
| + | + | +++ |
| Batch uniformity * |
|
| ++ | ++ | +++ |
| Cake colour |
|
| ++ | ++ | +++ |
| Cake structure |
|
| + | + | +++ |
| Cake density |
|
| ++ | ++ | +++ |
| Cake finish |
|
| ++ | ++ | ++ |
| Cake friability |
|
| + | – | +++ |
| Cake topography |
|
| – | – | ++ |
| Cake shrinkage |
|
| – | + | +++ |
| Cake collapse/ meltback |
|
| + | ++ | +++ |
| Residual material presence |
|
| +++ | +++ | +++ |
| Particle presence |
|
| +++ | +++ | +++ |
| Residual moisture level * |
|
| +++ | +++ | +++ |
| Cake reconstitution * |
|
| +++ | +++ | +++ |
| Cell structural integrity maintenance |
|
| ++ | +++ | +++ |
| Cellular viability upon reconstitution |
|
| +++ | +++ | +++ |
| Product Dosage Final Concentration in the Culture Medium (µg/mL) 1 | Keratinocyte Count in Product-Supplemented Homeostasis Medium (103 Cells) | Keratinocyte Count in Product-Supplemented Proliferation Medium (103 Cells) | ||
|---|---|---|---|---|
| FE002-SK2-FT | FE002-SK2-LYO | FE002-SK2-FT | FE002-SK2-LYO | |
| 0 | 194 ± 10 | 194 ± 10 | 68 ± 3 | 68 ± 3 |
| 5 | 218 ± 20 | 202 ± 6 | 116 ± 8 | 98 ± 12 |
| 15 | 239 ± 29 | 247 ± 32 | 131 ± 9 | 128 ± 14 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laurent, A.; Scaletta, C.; Abdel-Sayed, P.; Michetti, M.; Flahaut, M.; Simon, J.-P.; Roessingh, A.d.B.; Raffoul, W.; Hirt-Burri, N.; Applegate, L.A. Optimized Manufacture of Lyophilized Dermal Fibroblasts for Next-Generation Off-the-Shelf Progenitor Biological Bandages in Topical Post-Burn Regenerative Medicine. Biomedicines 2021, 9, 1072. https://doi.org/10.3390/biomedicines9081072
Laurent A, Scaletta C, Abdel-Sayed P, Michetti M, Flahaut M, Simon J-P, Roessingh AdB, Raffoul W, Hirt-Burri N, Applegate LA. Optimized Manufacture of Lyophilized Dermal Fibroblasts for Next-Generation Off-the-Shelf Progenitor Biological Bandages in Topical Post-Burn Regenerative Medicine. Biomedicines. 2021; 9(8):1072. https://doi.org/10.3390/biomedicines9081072
Chicago/Turabian StyleLaurent, Alexis, Corinne Scaletta, Philippe Abdel-Sayed, Murielle Michetti, Marjorie Flahaut, Jeanne-Pascale Simon, Anthony de Buys Roessingh, Wassim Raffoul, Nathalie Hirt-Burri, and Lee Ann Applegate. 2021. "Optimized Manufacture of Lyophilized Dermal Fibroblasts for Next-Generation Off-the-Shelf Progenitor Biological Bandages in Topical Post-Burn Regenerative Medicine" Biomedicines 9, no. 8: 1072. https://doi.org/10.3390/biomedicines9081072