
Regenerative Effect of Mesenchymal Stem Cell on Cartilage Damage in a Porcine Model
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
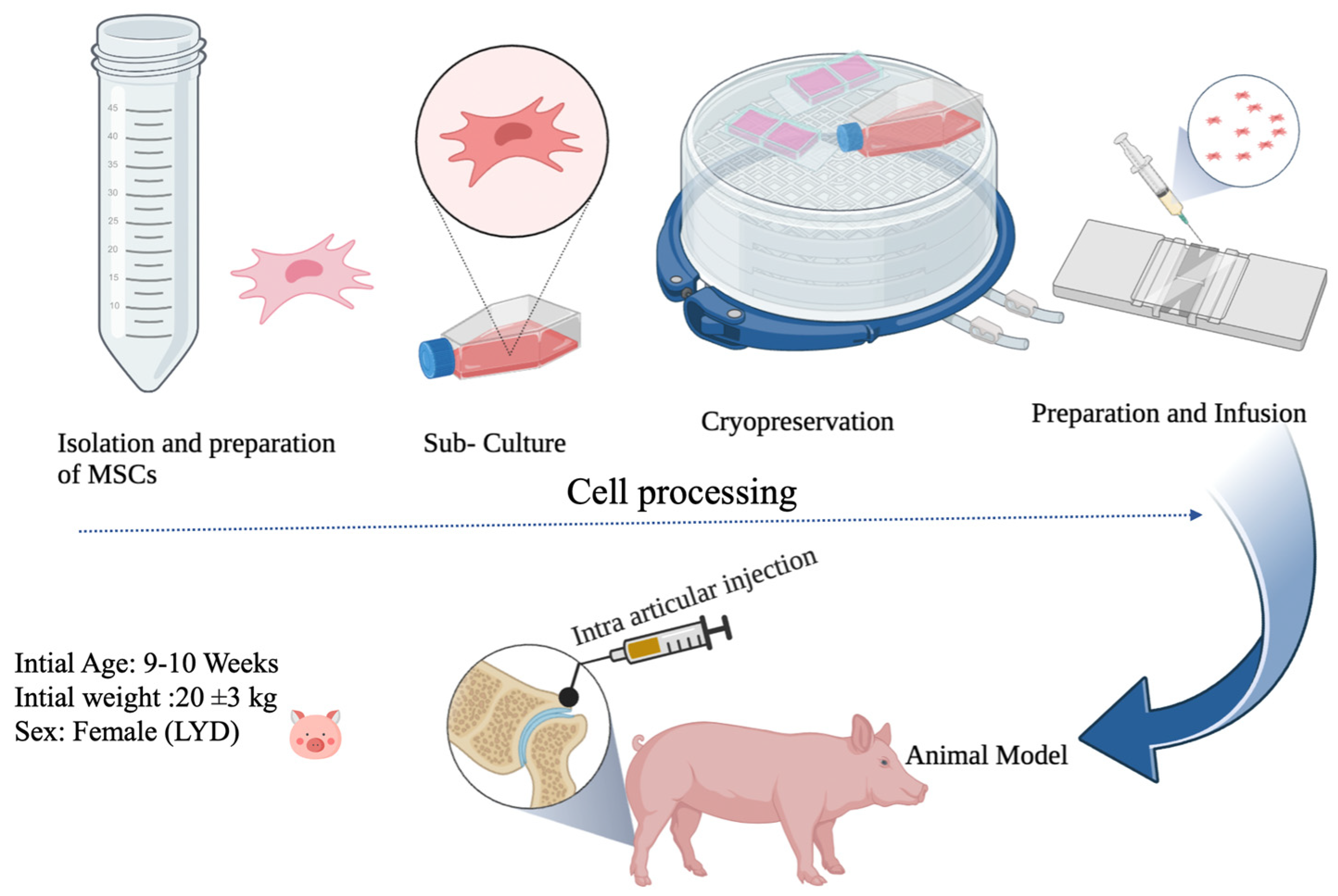
2.1. Preparation of MSCs
2.2. Experimental Animals
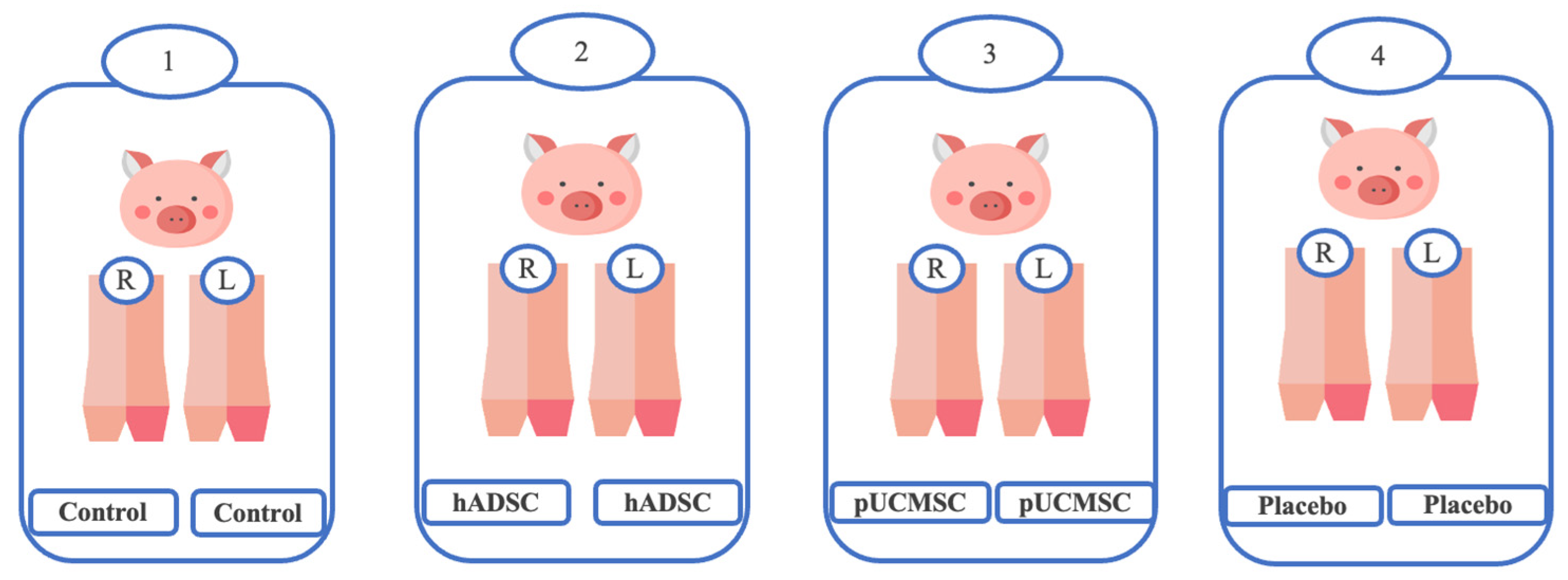
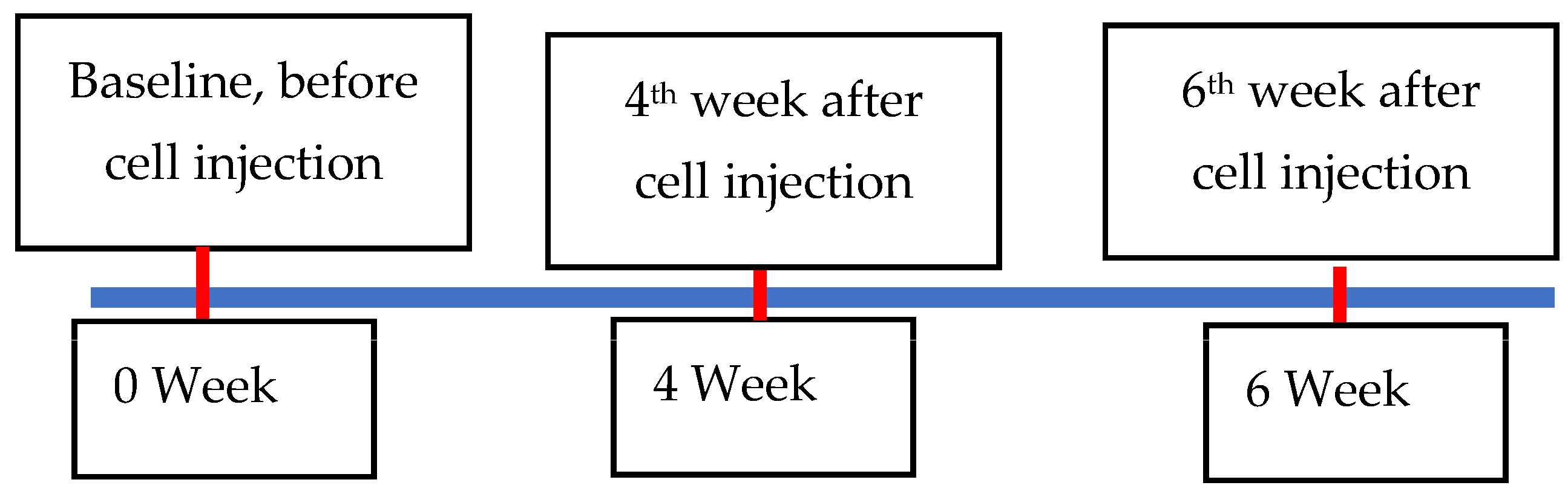
2.3. Experimental Design
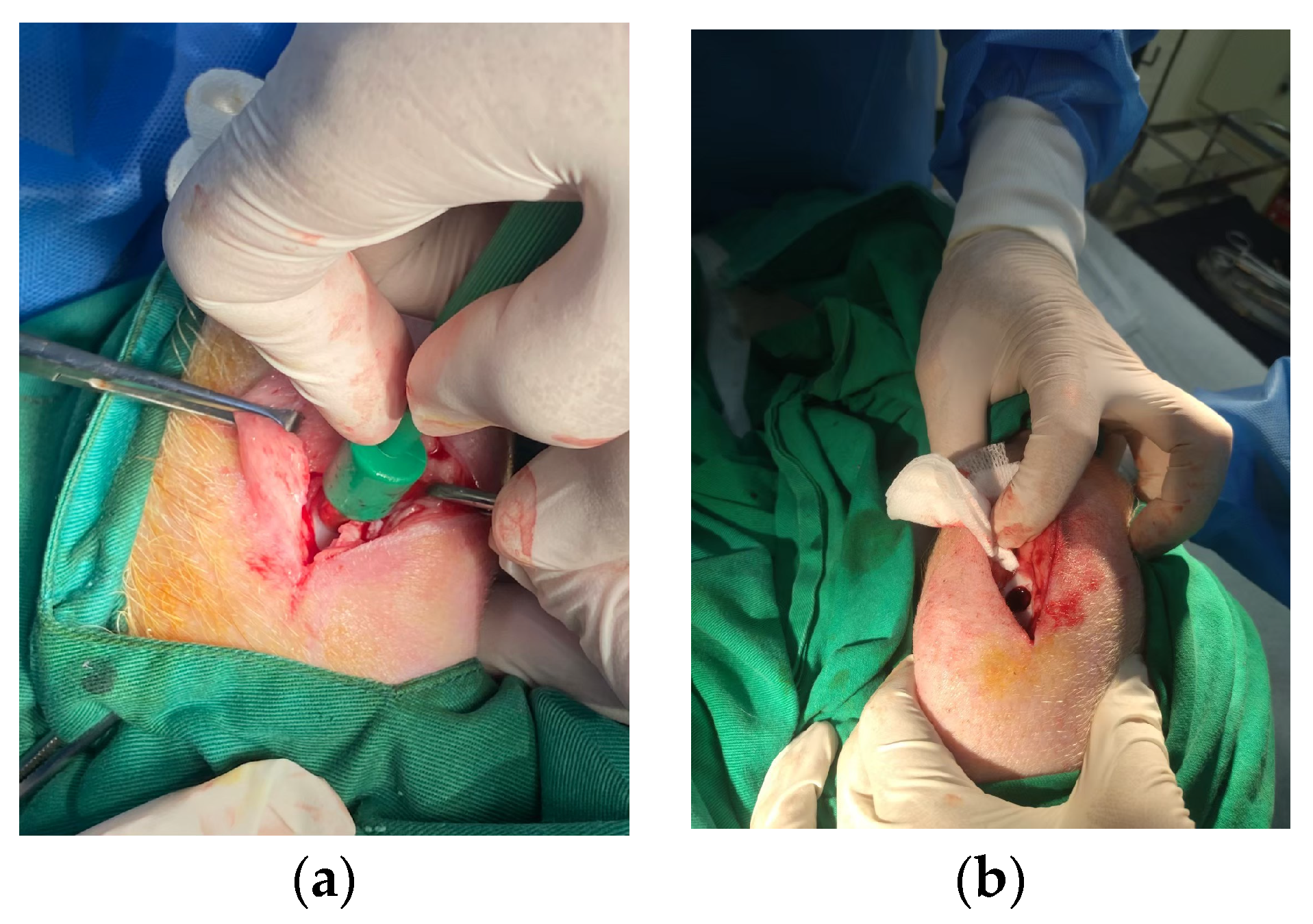
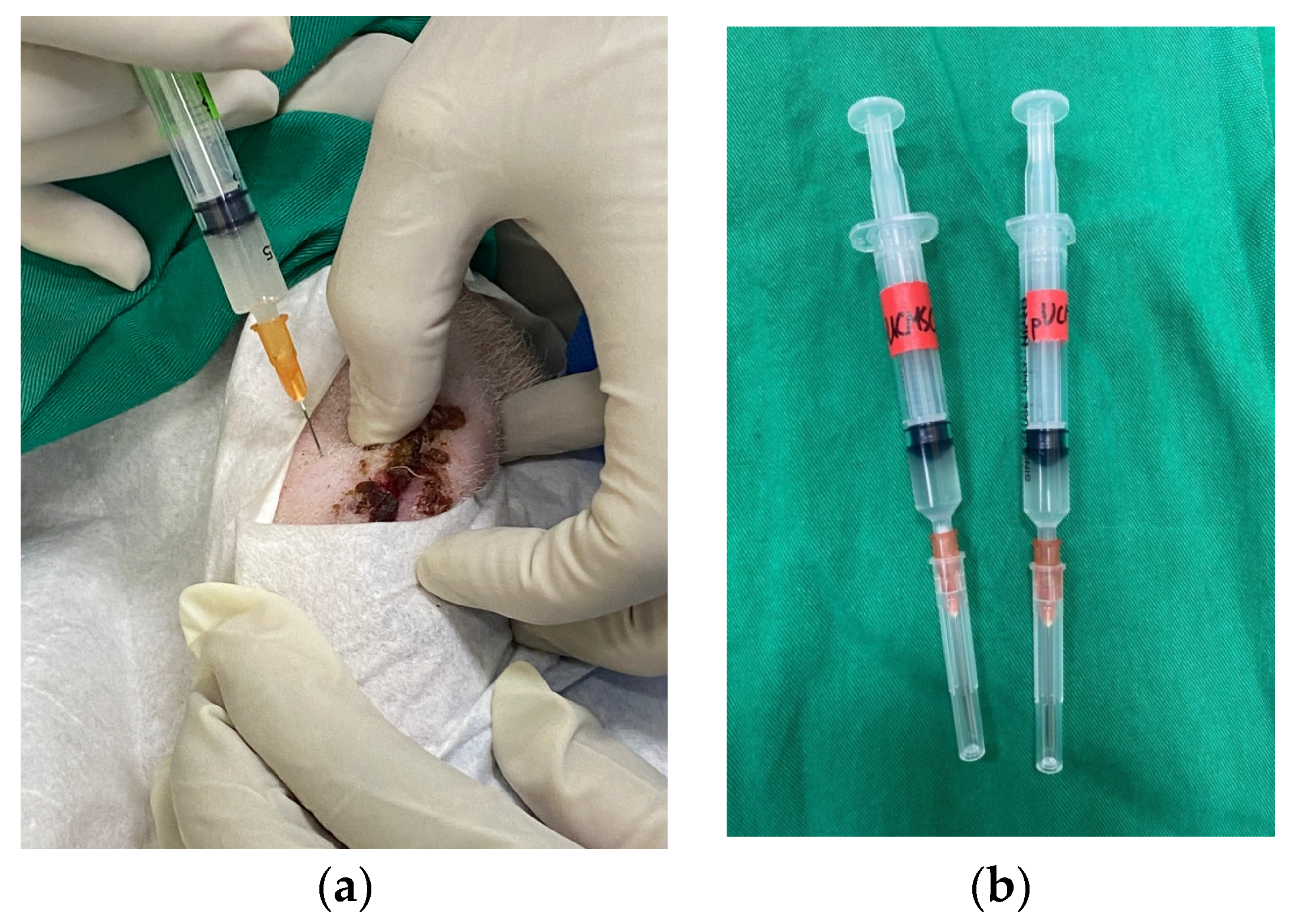
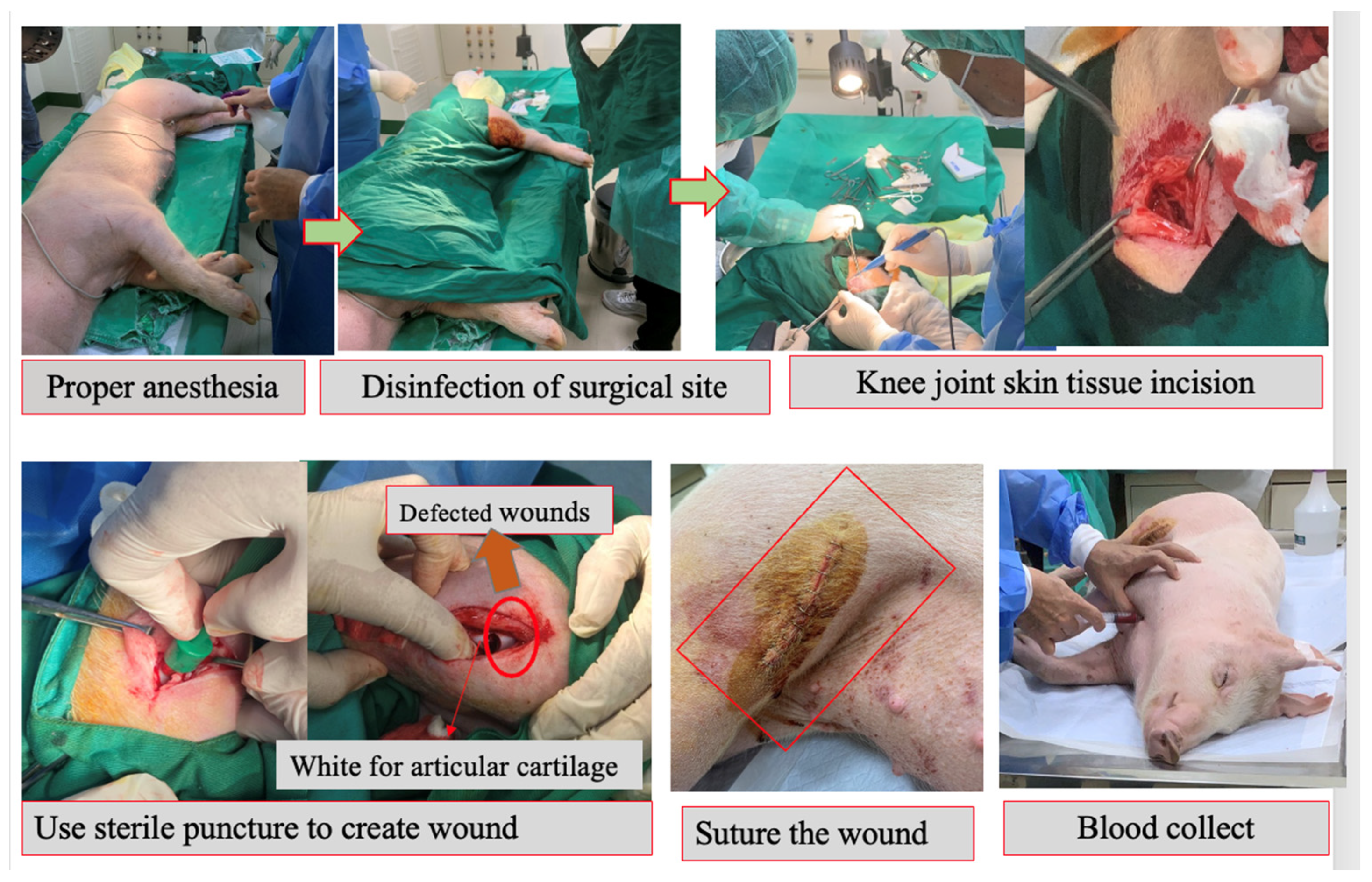
2.4. Surgical Procedure
2.5. MRI and CT Examinations
2.6. Macroscopic Images
2.7. Microscopic Evaluation
2.8. Enzyme-Linked Immunosorbent Assay for Cytokine Concentrations
2.9. Statistical Analysis
3. Results
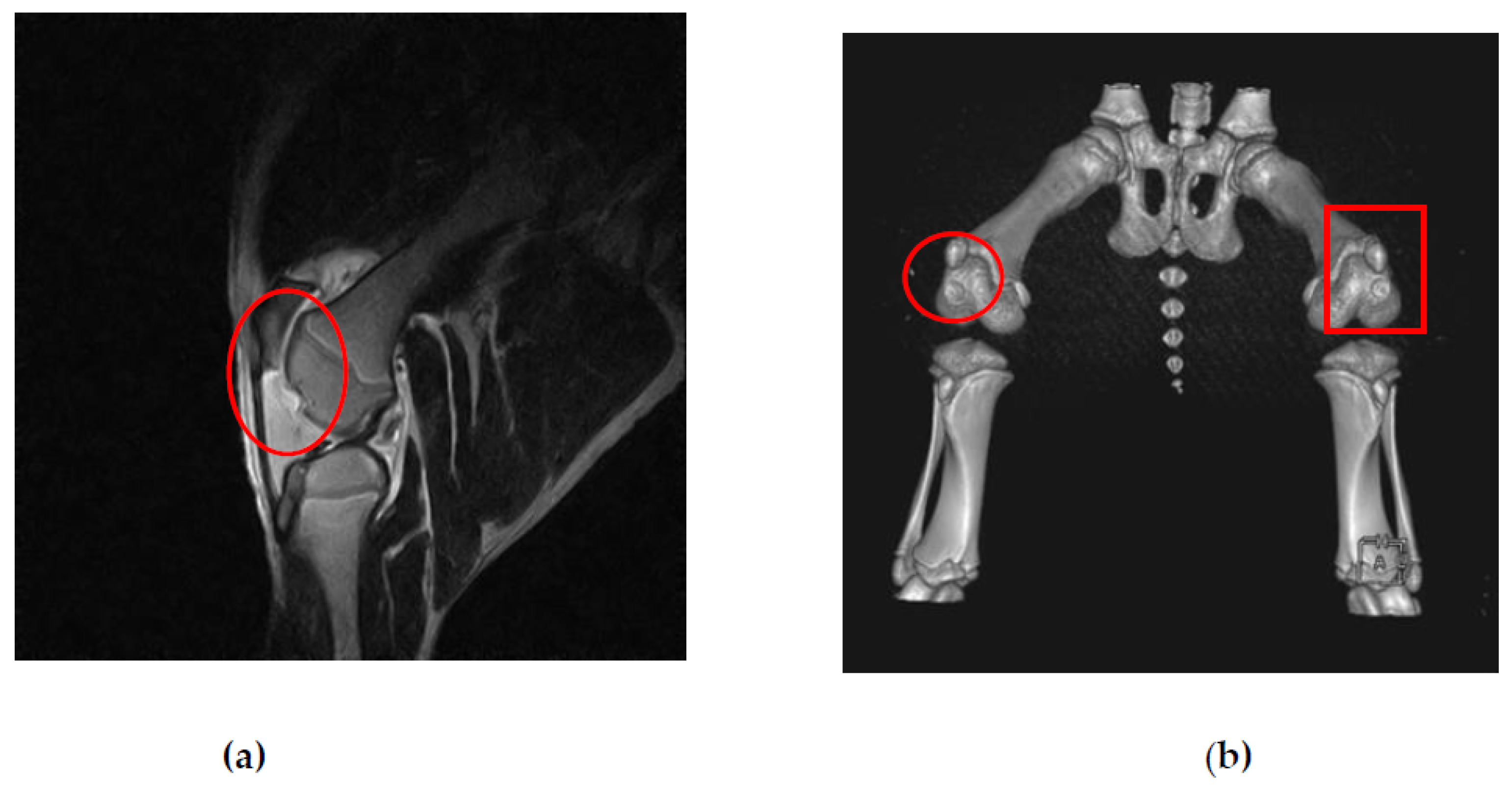
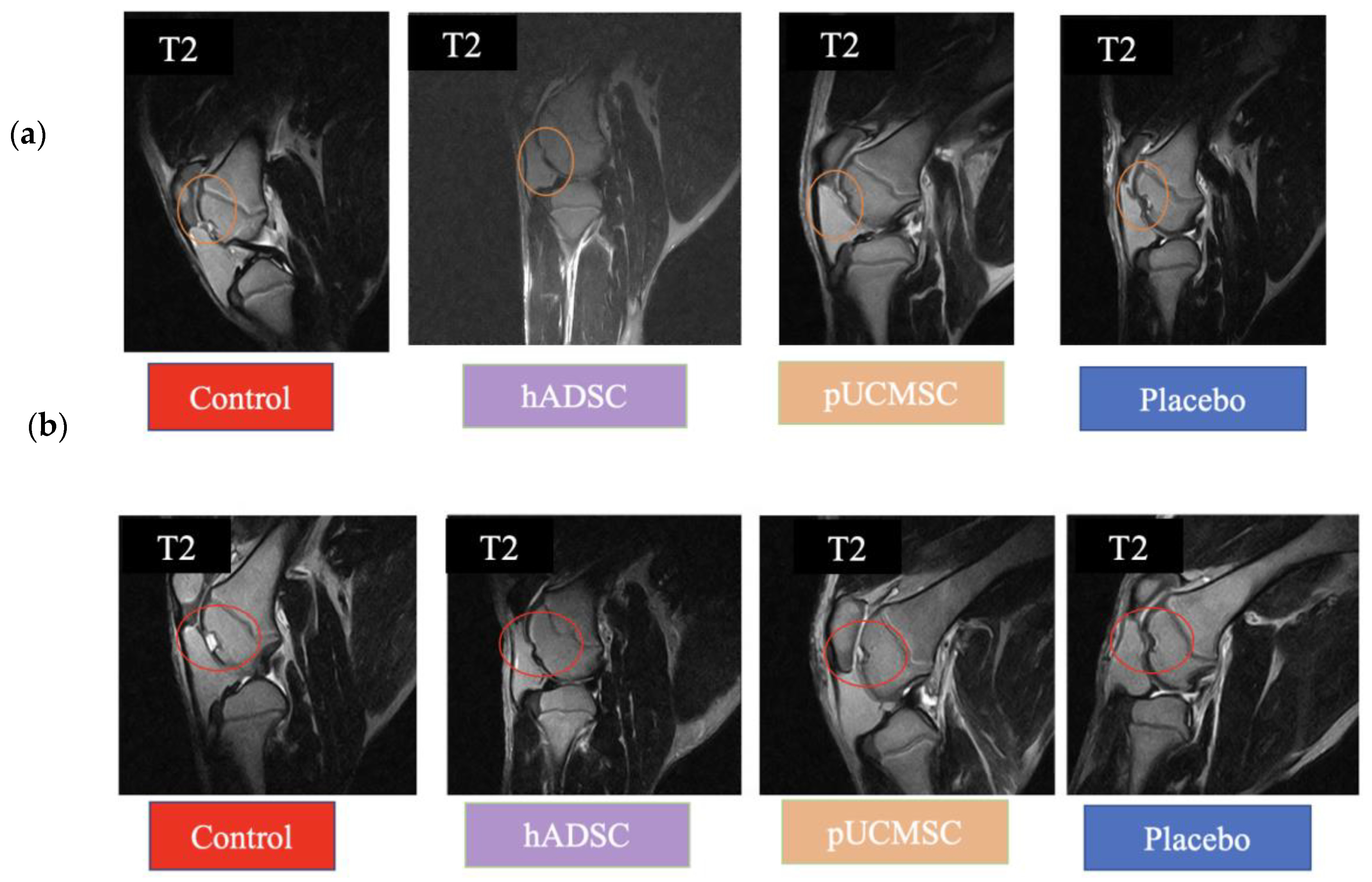
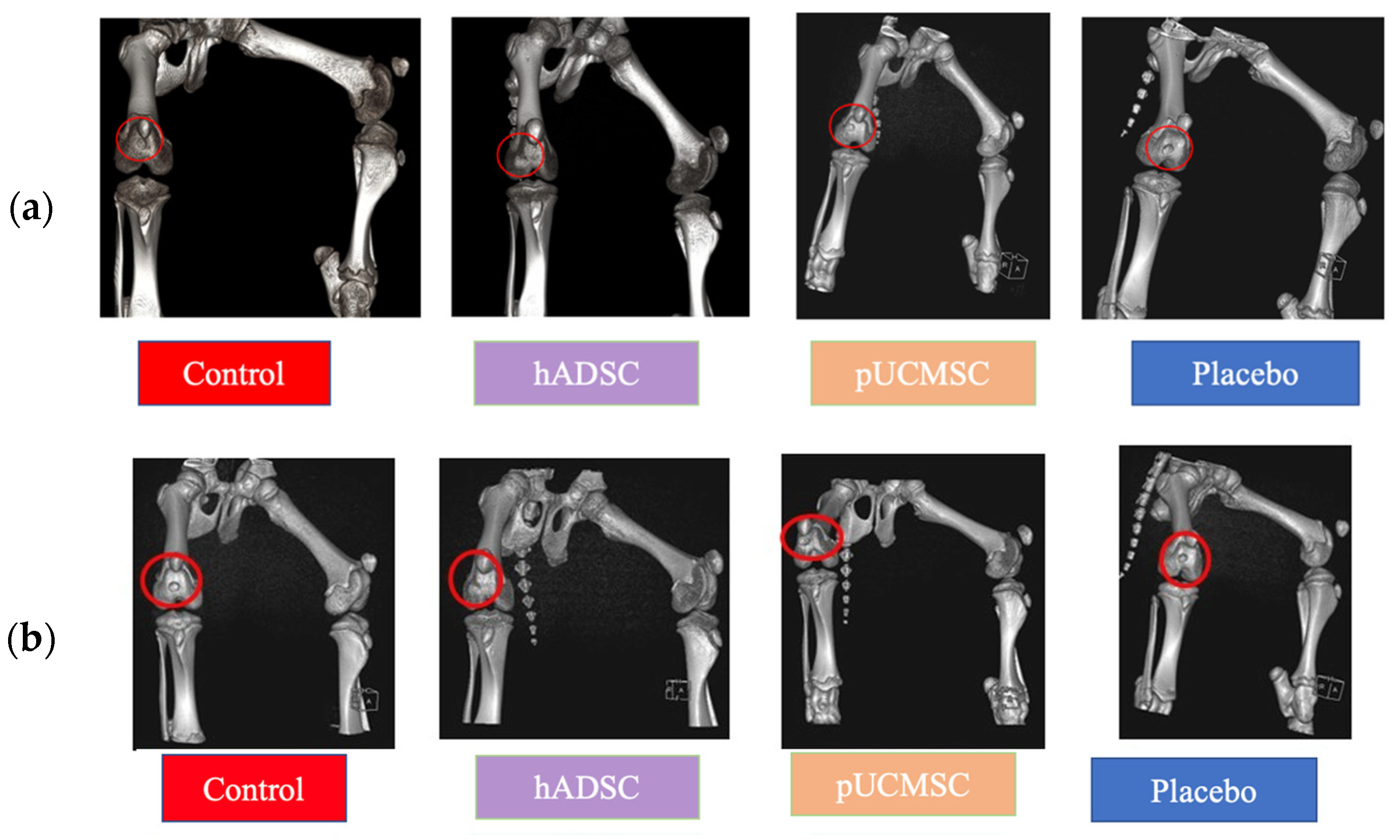
3.1. MRI and CT Observations
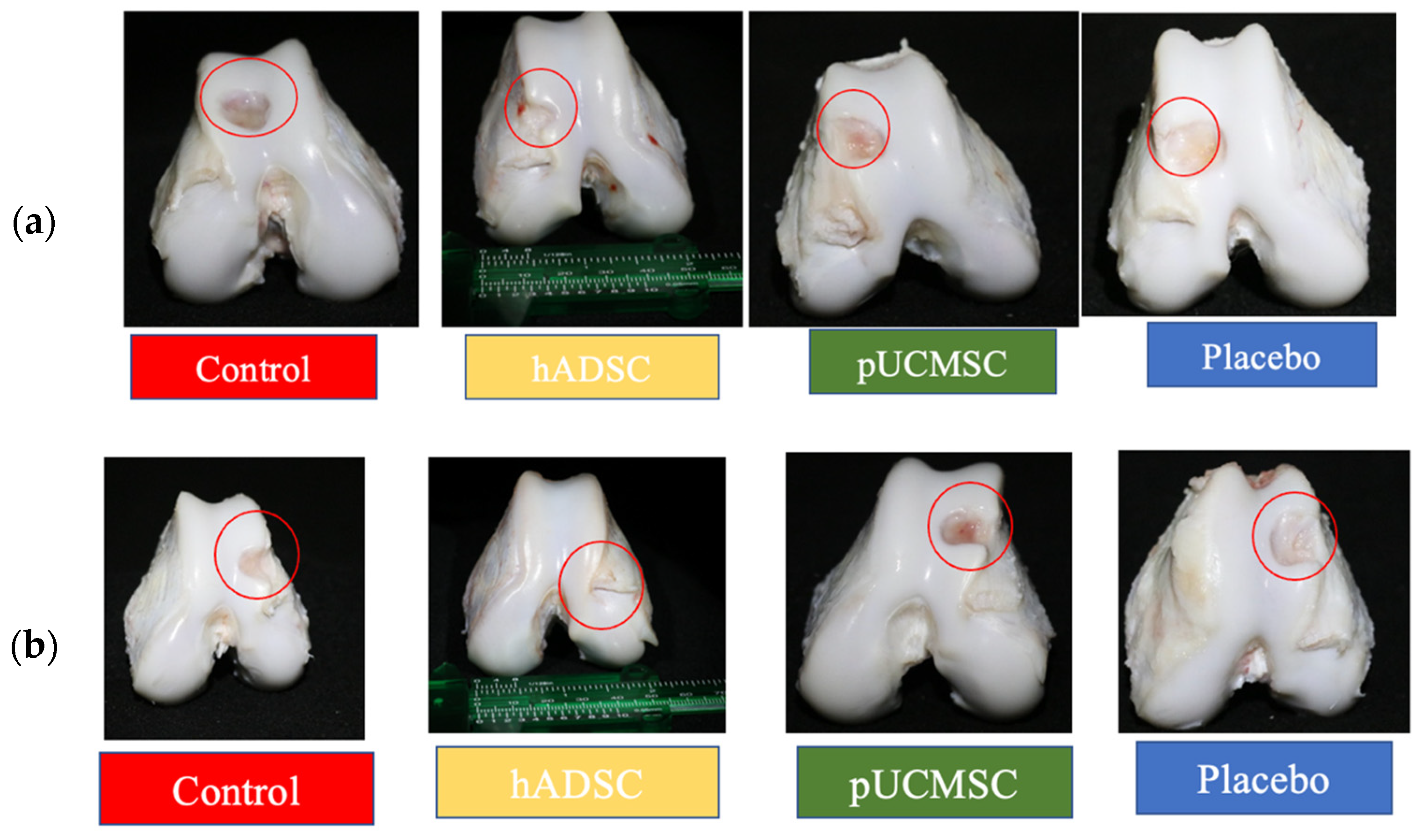
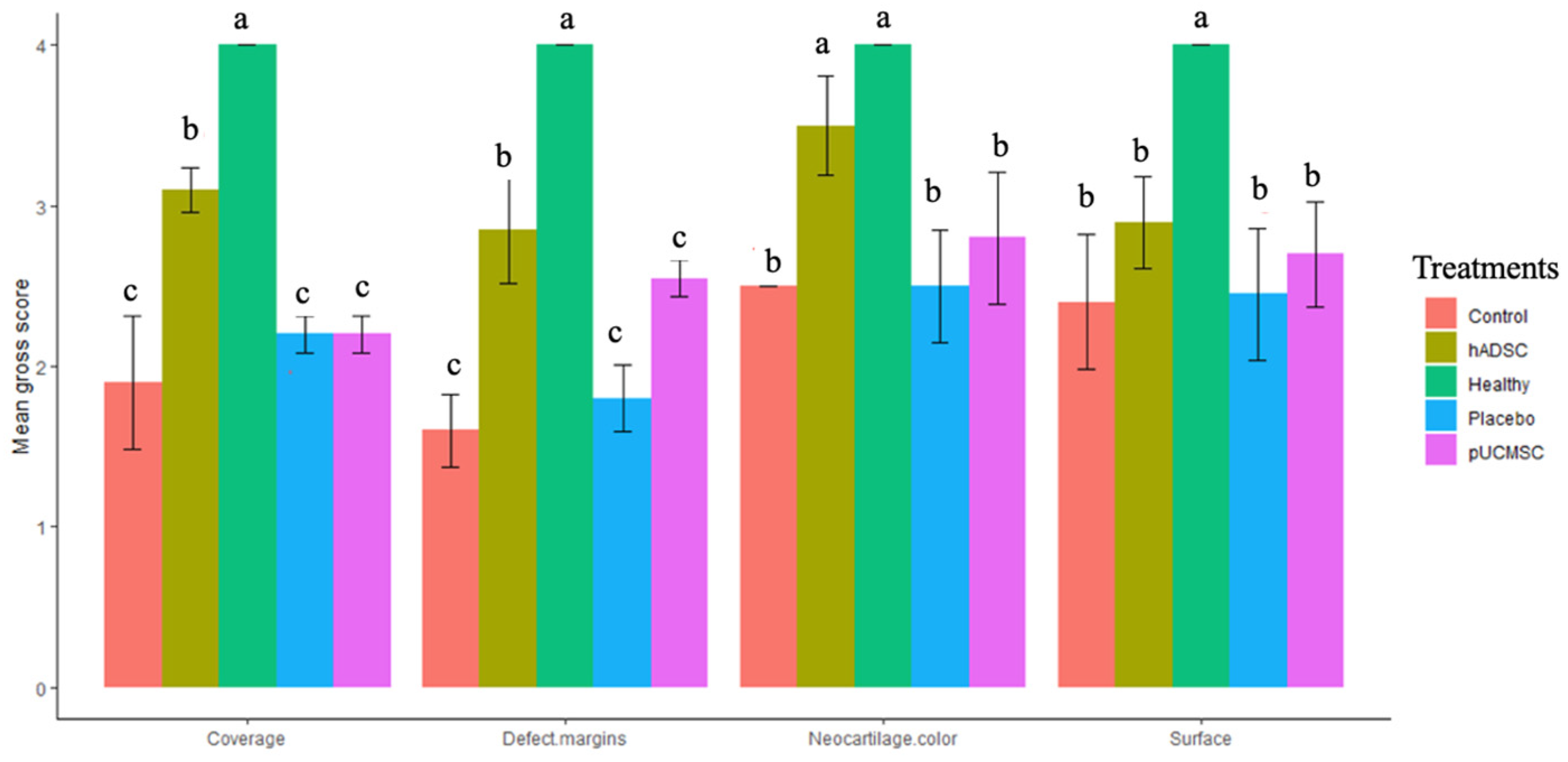
3.2. Gross Observations
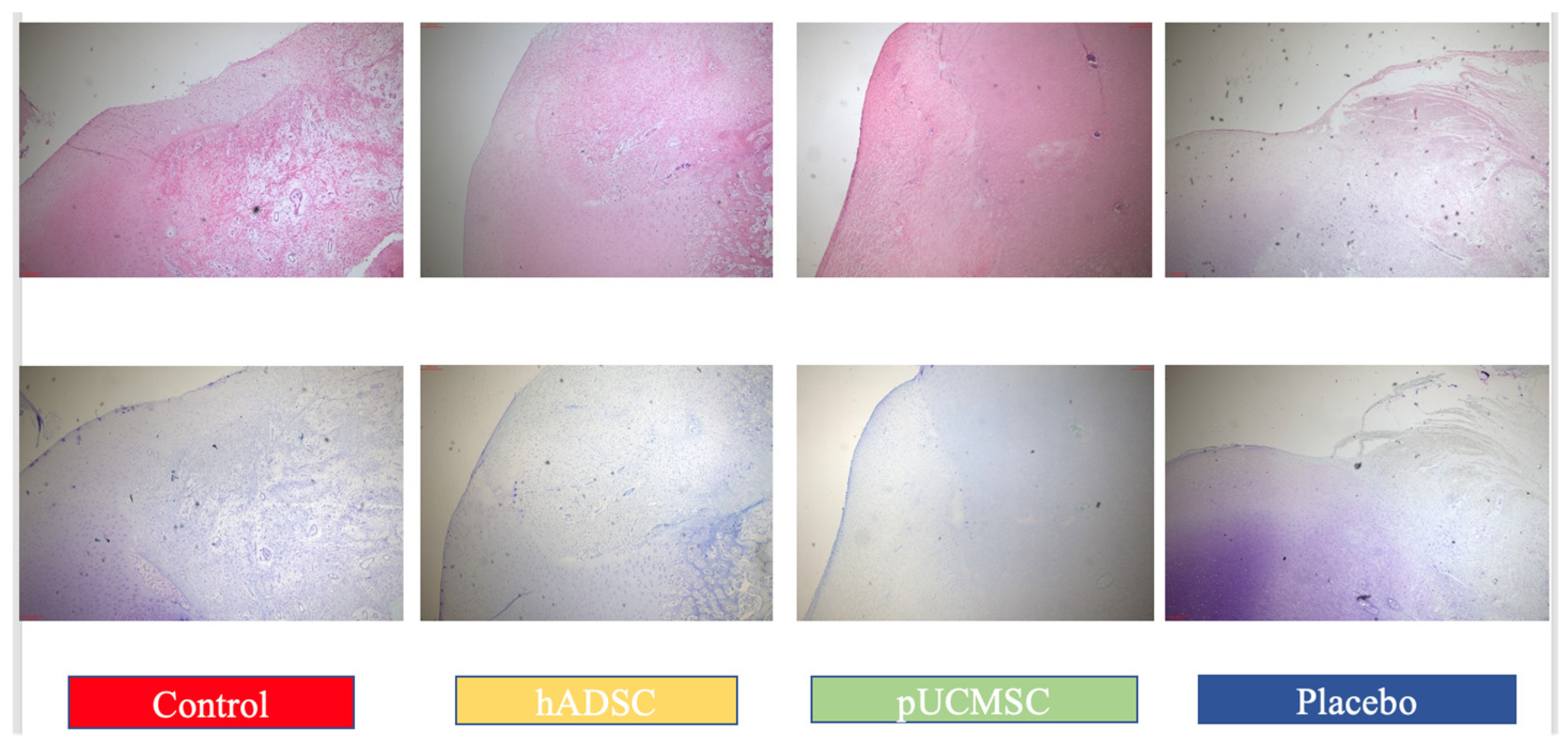
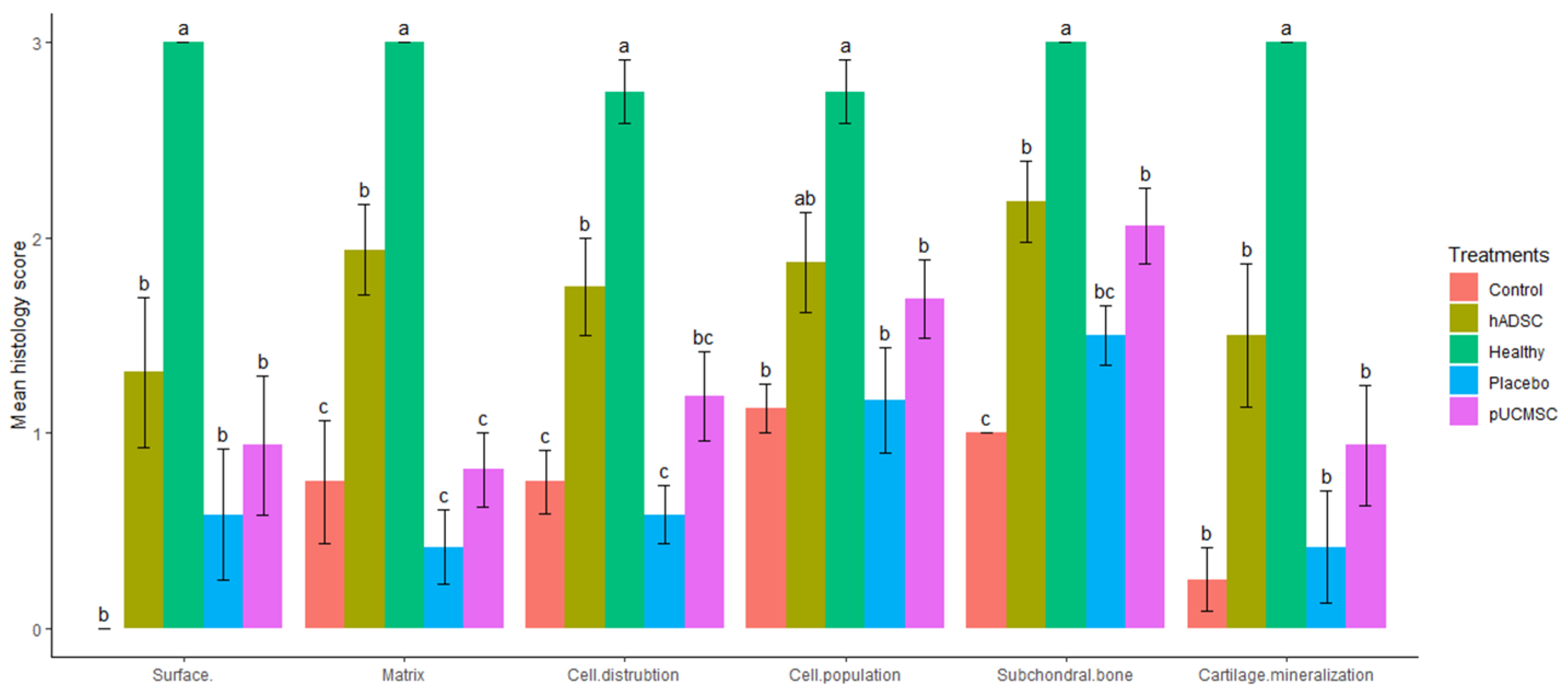
3.3. Histological Observations
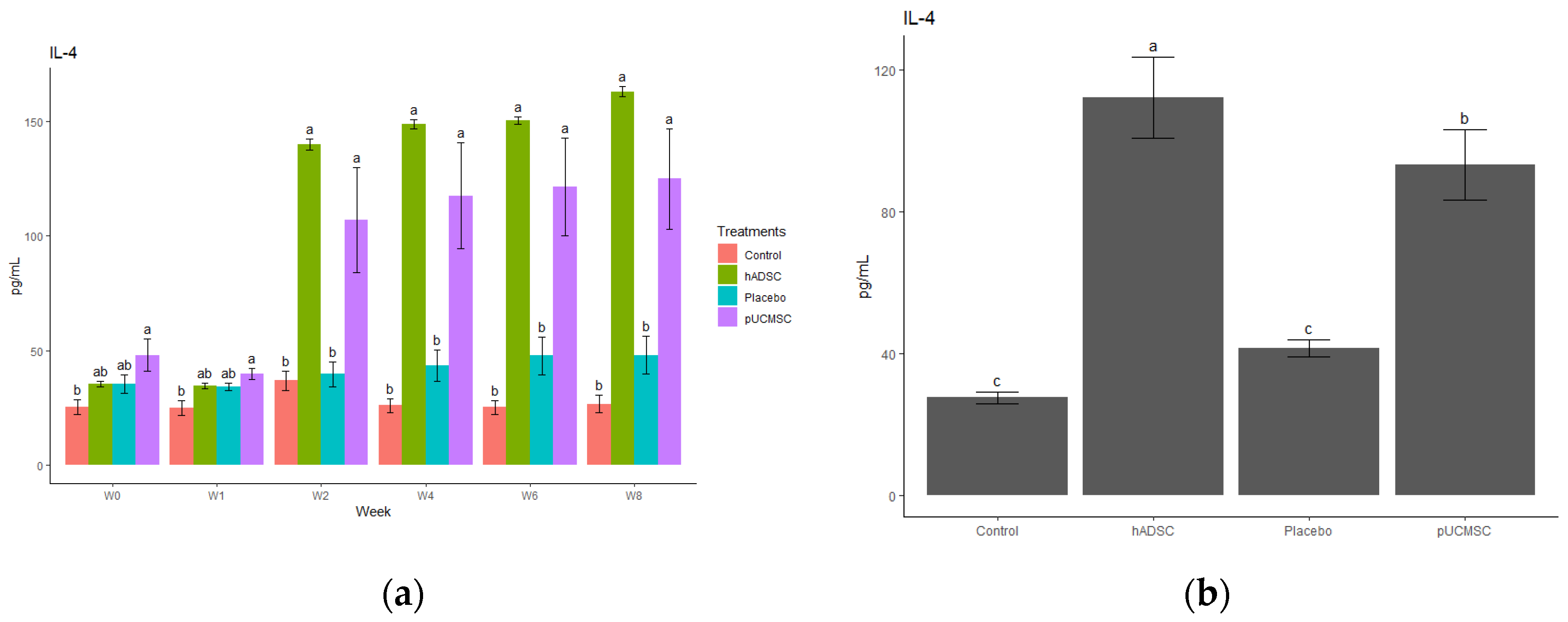
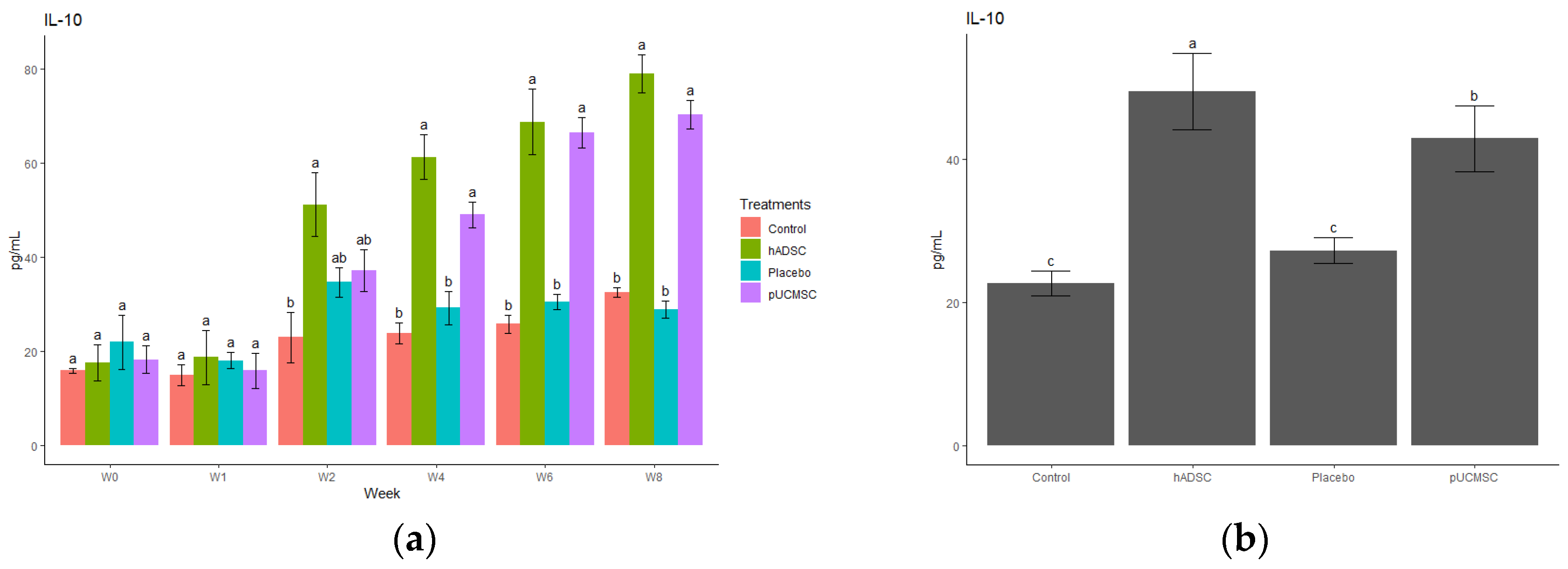
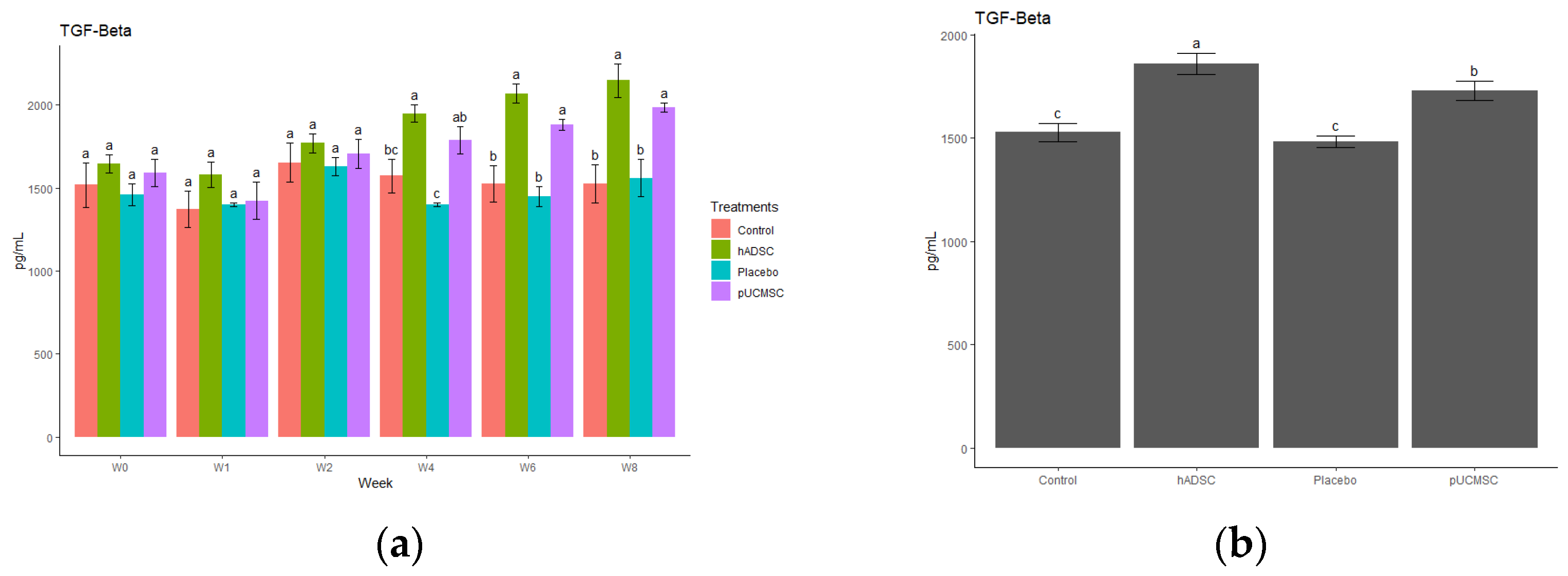
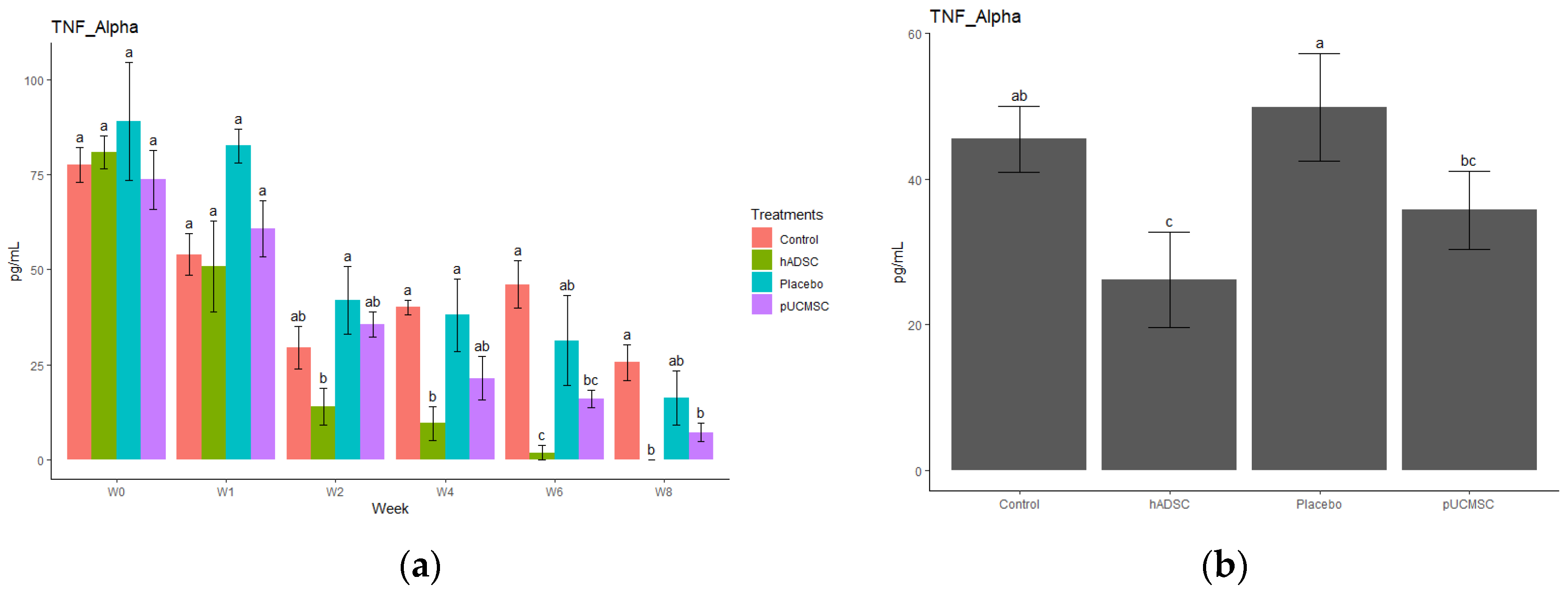
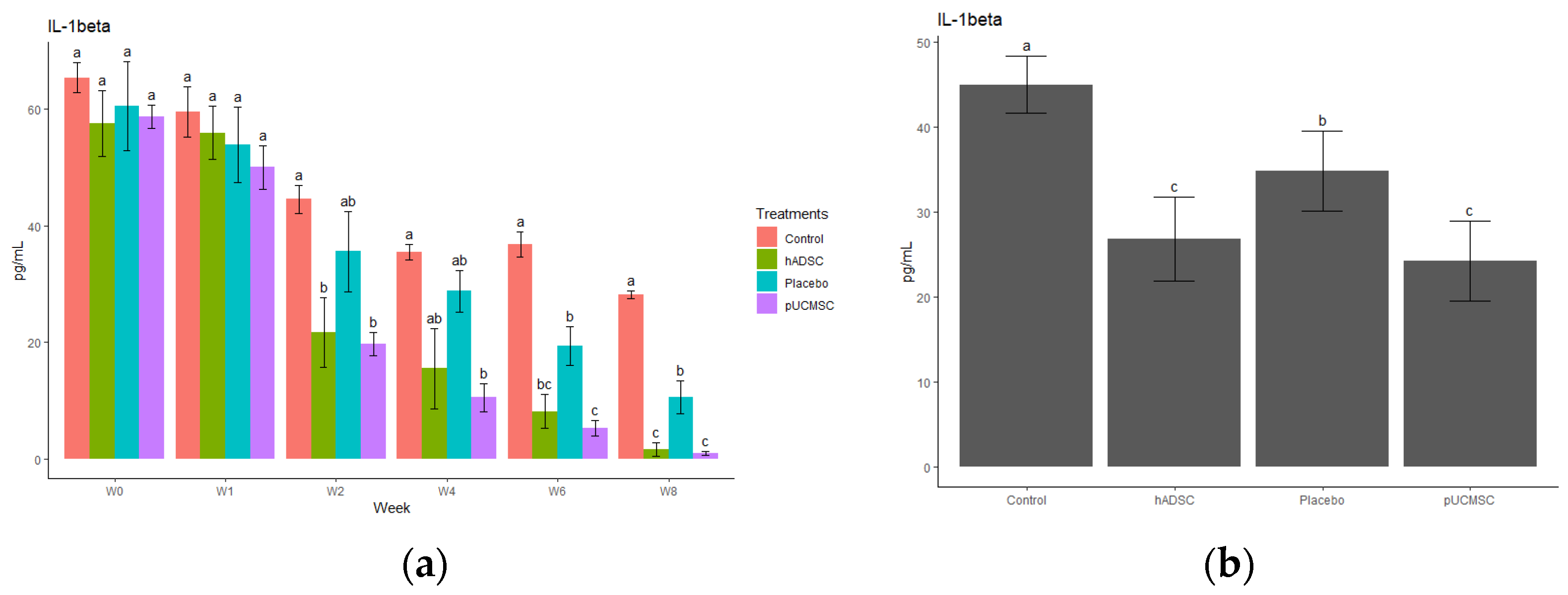
3.4. Cytokine Observations
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mille, M.A.; McClement, J.; Lauer, S. Physiotherapeutic Strategies and Their Current Evidence for Canine Osteoarthritis. Vet. Sci. 2023, 10, 2. [Google Scholar] [CrossRef]
- Camargo Garbin, L.; Morris, M.J. A Comparative Review of Autologous Conditioned Serum and Autologous Protein Solution for Treatment of Osteoarthritis in Horses. Front. Vet. Sci. 2021, 8, 602978. [Google Scholar] [CrossRef] [PubMed]
- Rios, J.L.; Sapède, D.; Djouad, F.; Rapp, A.E.; Lang, A.; Larkin, J.; Ladel, C.; Mobasheri, A. Animal Models of Osteoarthritis Part 1—Preclinical Small Animal Models: Challenges and Opportunities for Drug Development. Curr. Protoc. 2022, 2, e596. [Google Scholar] [CrossRef]
- Hulshof, C.T.J.; Colosio, C.; Daams, J.G.; Ivanov, I.D.; Prakash, K.C.; Kuijer, P.P.F.M.; Leppink, N.; Mandic-Rajcevic, S.; Masci, F.; van der Molen, H.F.; et al. WHO/ILO Work-Related Burden of Disease and Injury: Protocol for Systematic Reviews of Exposure to Occupational Ergonomic Risk Factors and of the Effect of Exposure to Occupational Ergonomic Risk Factors on Osteoarthritis of Hip or Knee and Selected Other. Environ. Int. 2019, 125, 554–566. [Google Scholar] [CrossRef] [PubMed]
- Manlapaz, D.G.; Sole, G.; Jayakaran, P.; Chapple, C.M. Risk Factors for Falls in Adults with Knee Osteoarthritis: A Systematic Review. PM&R 2019, 11, 745–757. [Google Scholar] [CrossRef]
- Tschon, M.; Contartese, D.; Pagani, S.; Borsari, V.; Fini, M. Gender and Sex Are Key Determinants in Osteoarthritis Not Only Confounding Variables. A Systematic Review of Clinical Data. J. Clin. Med. 2021, 10, 3178. [Google Scholar] [CrossRef] [PubMed]
- Long, H.; Liu, Q.; Yin, H.; Wang, K.; Diao, N.; Zhang, Y.; Lin, J.; Guo, A. Prevalence Trends of Site-Specific Osteoarthritis from 1990 to 2019: Findings from the Global Burden of Disease Study 2019. Arthritis Rheumatol. 2022, 74, 1172–1183. [Google Scholar] [CrossRef]
- Hunter, D.J.; March, L.; Chew, M. Osteoarthritis in 2020 and beyond: A Lancet Commission. Lancet 2020, 396, 1711–1712. [Google Scholar] [CrossRef]
- Safiri, S.; Kolahi, A.A.; Smith, E.; Hill, C.; Bettampadi, D.; Mansournia, M.A.; Hoy, D.; Ashrafi-Asgarabad, A.; Sepidarkish, M.; Almasi-Hashiani, A.; et al. Global, Regional and National Burden of Osteoarthritis 1990–2017: A Systematic Analysis of the Global Burden of Disease Study 2017. Ann. Rheum. Dis. 2020, 79, 819–828. [Google Scholar] [CrossRef]
- Giorgino, R.; Albano, D.; Fusco, S.; Peretti, G.M.; Mangiavini, L.; Messina, C. Knee Osteoarthritis: Epidemiology, Pathogenesis, and Mesenchymal Stem Cells: What Else Is New? An Update. Int. J. Mol. Sci. 2023, 24, 6405. [Google Scholar] [CrossRef]
- Sasaki, A.; Mizuno, M.; Mochizuki, M.; Sekiya, I. Mesenchymal Stem Cells for Cartilage Regeneration in Dogs. World J. Stem Cells 2019, 11, 254–269. [Google Scholar] [CrossRef] [PubMed]
- Nganvongpanit, K.; Soponteerakul, R.; Kaewkumpai, P.; Punyapornwithaya, V.; Buddhachat, K.; Nomsiri, R.; Kaewmong, P.; Kittiwatanawong, K.; Chawangwongsanukun, R.; Angkawanish, T.; et al. Osteoarthritis in Two Marine Mammals and 22 Land Mammals: Learning from Skeletal Remains. J. Anat. 2017, 231, 140–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, J.; Kim, J.; Cheon, S. A Deep Neural Network-Based Method for Early Detection of Osteoarthritis Using Statistical Data. Int. J. Environ. Res. Public Health 2019, 16, 1281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pap, T.; Korb-Pap, A. Cartilage Damage in Osteoarthritis and Rheumatoid Arthritis—Two Unequal Siblings. Nat. Rev. Rheumatol. 2015, 11, 606–615. [Google Scholar] [CrossRef]
- Evenbratt, H.; Andreasson, L.; Bicknell, V.; Brittberg, M.; Mobini, R.; Simonsson, S. Insights into the Present and Future of Cartilage Regeneration and Joint Repair. Cell Regen. 2022, 11, 3. [Google Scholar] [CrossRef]
- Wu, K.C.; Chang, Y.H.; Liu, H.W.; Ding, D.C. Transplanting Human Umbilical Cord Mesenchymal Stem Cells and Hyaluronate Hydrogel Repairs Cartilage of Osteoarthritis in the Minipig Model. Tzu Chi Med. J. 2019, 31, 11–19. [Google Scholar] [CrossRef]
- Sato, M.; Uchida, K.; Nakajima, H.; Miyazaki, T.; Guerrero, A.R.; Watanabe, S.; Roberts, S.; Baba, H. Direct Transplantation of Mesenchymal Stem Cells into the Knee Joints of Hartley Strain Guinea Pigs with Spontaneous Osteoarthritis. Arthritis Res. Ther. 2012, 14, R31. [Google Scholar] [CrossRef] [Green Version]
- Sheu, S.Y.; Wang, C.H.; Pao, Y.H.; Fu, Y.T.; Liu, C.H.; Yao, C.H.; Kuo, T.F. The Effect of Platelet-Rich Fibrin on Autologous Osteochondral Transplantation: An In Vivo Porcine Model. Knee 2017, 24, 1392–1401. [Google Scholar] [CrossRef]
- Lv, Z.; Cai, X.; Bian, Y.; Wei, Z.; Zhu, W.; Zhao, X.; Weng, X. Advances in Mesenchymal Stem Cell Therapy for Osteoarthritis: From Preclinical and Clinical Perspectives. Bioengineering 2023, 10, 195. [Google Scholar] [CrossRef]
- Hunter, D.J.; Bierma-Zeinstra, S. Osteoarthritis. Lancet 2019, 393, 1745–1759. [Google Scholar] [CrossRef]
- Wong, R.S.Y. Disease-Modifying Effects of Long-Term and Continuous Use of Nonsteroidal Anti-Inflammatory Drugs (NSAIDs) in Spondyloarthritis. Adv. Pharmacol. Sci. 2019, 2019, 5324170. [Google Scholar] [CrossRef]
- Abraham, N.S.; El-Serag, H.B.; Hartman, C.; Richardson, P.; Deswal, A. Cyclooxygenase-2 Selectivity of Non-Steroidal Anti-Inflammatory Drugs and the Risk of Myocardial Infarction and Cerebrovascular Accident. Aliment. Pharmacol. Ther. 2007, 25, 913–924. [Google Scholar] [CrossRef]
- Le, H.; Xu, W.; Zhuang, X.; Chang, F.; Wang, Y.; Ding, J. Mesenchymal Stem Cells for Cartilage Regeneration. J. Tissue Eng. 2020, 11, 2041731420943839. [Google Scholar] [CrossRef]
- Brown, C.; McKee, C.; Bakshi, S.; Walker, K.; Hakman, E.; Halassy, S.; Svinarich, D.; Dodds, R.; Govind, C.K.; Chaudhry, G.R. Mesenchymal Stem Cells: Cell Therapy and Regeneration Potential. J. Tissue Eng. Regen. Med. 2019, 13, 1738–1755. [Google Scholar] [CrossRef] [PubMed]
- Xie, M.; Li, C.; She, Z.; Wu, F.; Mao, J.; Hun, M.; Luo, S.; Wan, W.; Tian, J.; Wen, C. Human Umbilical Cord Mesenchymal Stem Cells Derived Extracellular Vesicles Regulate Acquired Immune Response of Lupus Mouse in Vitro. Sci. Rep. 2022, 12, 13101. [Google Scholar] [CrossRef] [PubMed]
- Ribitsch, I.; Baptista, P.M.; Lange-Consiglio, A.; Melotti, L.; Patruno, M.; Jenner, F.; Schnabl-Feichter, E.; Dutton, L.C.; Connolly, D.J.; van Steenbeek, F.G.; et al. Large Animal Models in Regenerative Medicine and Tissue Engineering: To Do or Not to Do. Front. Bioeng. Biotechnol. 2020, 8, 972. [Google Scholar] [CrossRef] [PubMed]
- Zhu, M.; Heydarkhan-Hagvall, S.; Hedrick, M.; Benhaim, P.; Zuk, P. Manual Isolation of Adipose-Derived Stem Cells from Human Lipoaspirates. J. Vis. Exp. 2013, 79, e50585. [Google Scholar] [CrossRef] [Green Version]
- Lee, F.Y.; Chen, K.H.; Wallace, C.G.; Sung, P.H.; Sheu, J.J.; Chung, S.Y.; Chen, Y.L.; Lu, H.I.; Ko, S.F.; Sun, C.K.; et al. Xenogeneic Human Umbilical Cord-Derived Mesenchymal Stem Cells Reduce Mortality in Rats with Acute Respiratory Distress Syndrome Complicated by Sepsis. Oncotarget 2017, 8, 45626–45642. [Google Scholar] [CrossRef] [Green Version]
- Hoemann, C.; Kandel, R.; Roberts, S.; Saris, D.B.F.; Creemers, L.; Mainil-Varlet, P.; Méthot, S.; Hollander, A.P.; Buschmann, M.D. International Cartilage Repair Society (ICRS) Recommended Guidelines for Histological Endpoints for Cartilage Repair Studies in Animal Models and Clinical Trials. Cartilage 2011, 2, 153–172. [Google Scholar] [CrossRef] [Green Version]
- van den Borne, M.P.J.; Raijmakers, N.J.H.; Vanlauwe, J.; Victor, J.; de Jong, S.N.; Bellemans, J.; Saris, D.B.F. International Cartilage Repair Society (ICRS) and Oswestry Macroscopic Cartilage Evaluation Scores Validated for Use in Autologous Chondrocyte Implantation (ACI) and Microfracture. Osteoarthr. Cartil. 2007, 15, 1397–1402. [Google Scholar] [CrossRef] [Green Version]
- Cone, S.G.; Warren, P.B.; Fisher, M.B. Biomechanical Considerations of Animal Models Used in Tissue Engineering of Bone. Tissue Eng.—Part C Methods 2017, 23, 763–780. [Google Scholar] [CrossRef]
- Liu, T.P.; Ha, P.; Xiao, C.Y.; Kim, S.Y.; Jensen, A.R.; Easley, J.; Yao, Q.; Zhang, X. Updates on Mesenchymal Stem Cell Therapies for Articular Cartilage Regeneration in Large Animal Models. Front. Cell Dev. Biol. 2022, 10, 982199. [Google Scholar] [CrossRef] [PubMed]
- Uto, S.; Nishizawa, S.; Hikita, A.; Takato, T.; Hoshi, K. Application of Induced Pluripotent Stem Cells for Cartilage Regeneration in CLAWN Miniature Pig Osteochondral Replacement Model. Regen. Ther. 2018, 9, 58–70. [Google Scholar] [CrossRef]
- Boguszewski, D.V.; Shearn, J.T.; Wagner, C.T.; Butler, D.L. Investigating the Effects of Anterior Tibial Translation on Anterior Knee Force in the Porcine Model: Is the Porcine Knee ACL Dependent? J. Orthop. Res. 2011, 29, 641–646. [Google Scholar] [CrossRef]
- Takroni, T.; Laouar, L.; Adesida, A.; Elliott, J.A.W.; Jomha, N.M. Anatomical Study: Comparing the Human, Sheep and Pig Knee Meniscus. J. Exp. Orthop. 2016, 3, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, F.; Hu, Y.; He, D.; Zhou, G.; Ellis, E. Scaffold-Free Cartilage Cell Sheet Combined with Bone-Phase BMSCs-Scaffold Regenerate Osteochondral Construct in Mini-Pig Model. Am. J. Transl. Res. 2018, 10, 2997–3010. [Google Scholar]
- Zhang, R.; Ma, J.; Han, J.; Zhang, W.; Ma, J. Mesenchymal Stem Cell Related Therapies for Cartilage Lesions and Osteoarthritis. Am. J. Transl. Res. 2019, 11, 6275–6289. [Google Scholar] [PubMed]
- Zhang, S.; Wong, K.L.; Ren, X.; Teo, K.Y.W.; Afizah, H.; Choo, A.B.H.; Lai, R.C.; Lim, S.K.; Hui, J.H.P.; Toh, W.S. Mesenchymal Stem Cell Exosomes Promote Functional Osteochondral Repair in a Clinically Relevant Porcine Model. Am. J. Sport. Med. 2022, 50, 788–800. [Google Scholar] [CrossRef]
- International, B.M.R. Retracted: Side-by-Side Comparison of the Biological Characteristics of Human Umbilical Cord and Adipose Tissue-Derived Mesenchymal Stem Cells. BioMed Res. Int. 2020, 2020, 3176431. [Google Scholar] [CrossRef]
- Kondo, T.; Ishida, Y. Molecular Pathology of Wound Healing. Forensic Sci. Int. 2010, 203, 93–98. [Google Scholar] [CrossRef]
- Baiguera, S.; Jungebluth, P.; Mazzanti, B.; MacChiarini, P. Mesenchymal Stromal Cells for Tissue-Engineered Tissue and Organ Replacements. Transpl. Int. 2012, 25, 369–382. [Google Scholar] [CrossRef]
- Boomsma, R.A.; Geenen, D.L. Mesenchymal Stem Cells Secrete Multiple Cytokines That Promote Angiogenesis and Have Contrasting Effects on Chemotaxis and Apoptosis. PLoS ONE 2012, 7, e35685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gugliandolo, A.; Fonticoli, L.; Trubiani, O.; Rajan, T.S.; Marconi, G.D.; Bramanti, P.; Mazzon, E.; Pizzicannella, J.; Diomede, F. Oral Bone Tissue Regeneration: Mesenchymal Stem Cells, Secretome, and Biomaterials. Int. J. Mol. Sci. 2021, 22, 5236. [Google Scholar] [CrossRef] [PubMed]
- Molnar, V.; Matišić, V.; Kodvanj, I.; Bjelica, R.; Jeleč, Ž.; Hudetz, D.; Rod, E.; Čukelj, F.; Vrdoljak, T.; Vidović, D.; et al. Cytokines and Chemokines Involved in Osteoarthritis Pathogenesis. Int. J. Mol. Sci. 2021, 22, 9208. [Google Scholar] [CrossRef]
- Kyurkchiev, D. Secretion of Immunoregulatory Cytokines by Mesenchymal Stem Cells. World J. Stem Cells 2014, 6, 552. [Google Scholar] [CrossRef] [PubMed]
- Uccelli, A.; de Rosbo, N.K. The Immunomodulatory Function of Mesenchymal Stem Cells: Mode of Action and Pathways. Ann. N. Y. Acad. Sci. 2015, 1351, 114–126. [Google Scholar] [CrossRef]
- Wang, Z.; Zhu, H.; Dai, S.; Liu, K.; Ge, C. Alleviation of Medial Meniscal Transection-Induced Osteoarthritis Pain in Rats by Human Adipose Derived Mesenchymal Stem Cells. Stem Cell Investig. 2020, 7, 6–13. [Google Scholar] [CrossRef]
- Saito, T.; Kuang, J.Q.; Bittira, B.; Al-Khaldi, A.; Chiu, R.C.J. Xenotransplant Cardiac Chimera: Immune Tolerance of Adult Stem Cells. Ann. Thorac. Surg. 2002, 74, 19–24. [Google Scholar] [CrossRef]



















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Ear Tag | Received |
|---|---|---|
| Treatment | P51, P72 | hADSC 1 |
| Treatment | P61, P71 | pUCMSC 1 |
| Control | P62 | Nothing |
| Placebo | P52, P63 | Medium |
| Gross Appearance | Grade |
|---|---|
| Coverage | |
| N > 75% fill | 4 |
| 50–75% fill | 3 |
| 25–50% fill | 2 |
| <25% fill | 1 |
| No fill | 0 |
| Neocartilage color | |
| Normal | 4 |
| 25% yellow/brown | 3 |
| 50% yellow/brown | 2 |
| 75% yellow/brown | 1 |
| 100% yellow/brown | 0 |
| Defect margins | |
| Invisible | 4 |
| 25% circumference visible | 3 |
| 50% circumference visible | 2 |
| 75% circumference visible | 1 |
| Entire circumference visible | 0 |
| Surface | |
| Smooth/level with normal | 4 |
| Smooth but raised. | 3 |
| Irregular 25–50% | 2 |
| Irregular 50–75% | 1 |
| Irregular > 75% | 0 |
| Features | Score |
|---|---|
| Surface | |
| Smooth/continuous | 3 |
| Discontinuities/irregularities | 0 |
| Matrix | |
| Hyaline | 3 |
| Mixture: hyaline/fibrocartilage | 2 |
| Fibrocartilage | 1 |
| Fibrous tissue | 0 |
| Cell distribution | |
| Columnar | 3 |
| Mixed: columnar/cluster | 2 |
| Cluster | 1 |
| Individual cells/disorganized | 0 |
| Subchondral bone | |
| Normal | 3 |
| Increased remodeling | 2 |
| Bone necrosis/granulation tissue | 1 |
| Detached/fracture/callus at base | 0 |
| Cartilage mineralization (calcified cartilage) | |
| Normal | 3 |
| Abnormal/inappropriate | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, S.-C.; Panthi, S.; Hsuuw, Y.-H.; Chen, S.-H.; Huang, M.-J.; Sieber, M.; Hsuuw, Y.-D. Regenerative Effect of Mesenchymal Stem Cell on Cartilage Damage in a Porcine Model. Biomedicines 2023, 11, 1810. https://doi.org/10.3390/biomedicines11071810
Lin S-C, Panthi S, Hsuuw Y-H, Chen S-H, Huang M-J, Sieber M, Hsuuw Y-D. Regenerative Effect of Mesenchymal Stem Cell on Cartilage Damage in a Porcine Model. Biomedicines. 2023; 11(7):1810. https://doi.org/10.3390/biomedicines11071810
Chicago/Turabian StyleLin, Sheng-Chuan, Sankar Panthi, Yu-Her Hsuuw, Shih-Hsien Chen, Ming-Ju Huang, Martin Sieber, and Yan-Der Hsuuw. 2023. "Regenerative Effect of Mesenchymal Stem Cell on Cartilage Damage in a Porcine Model" Biomedicines 11, no. 7: 1810. https://doi.org/10.3390/biomedicines11071810