
Efficacy and Tolerability of Perampanel in Brain Tumor-Related Epilepsy: A Systematic Review
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods
2.1. Primary and Secondary Objectives
2.2. Search Strategy
2.3. Study Selection and Data Extraction
3. Results
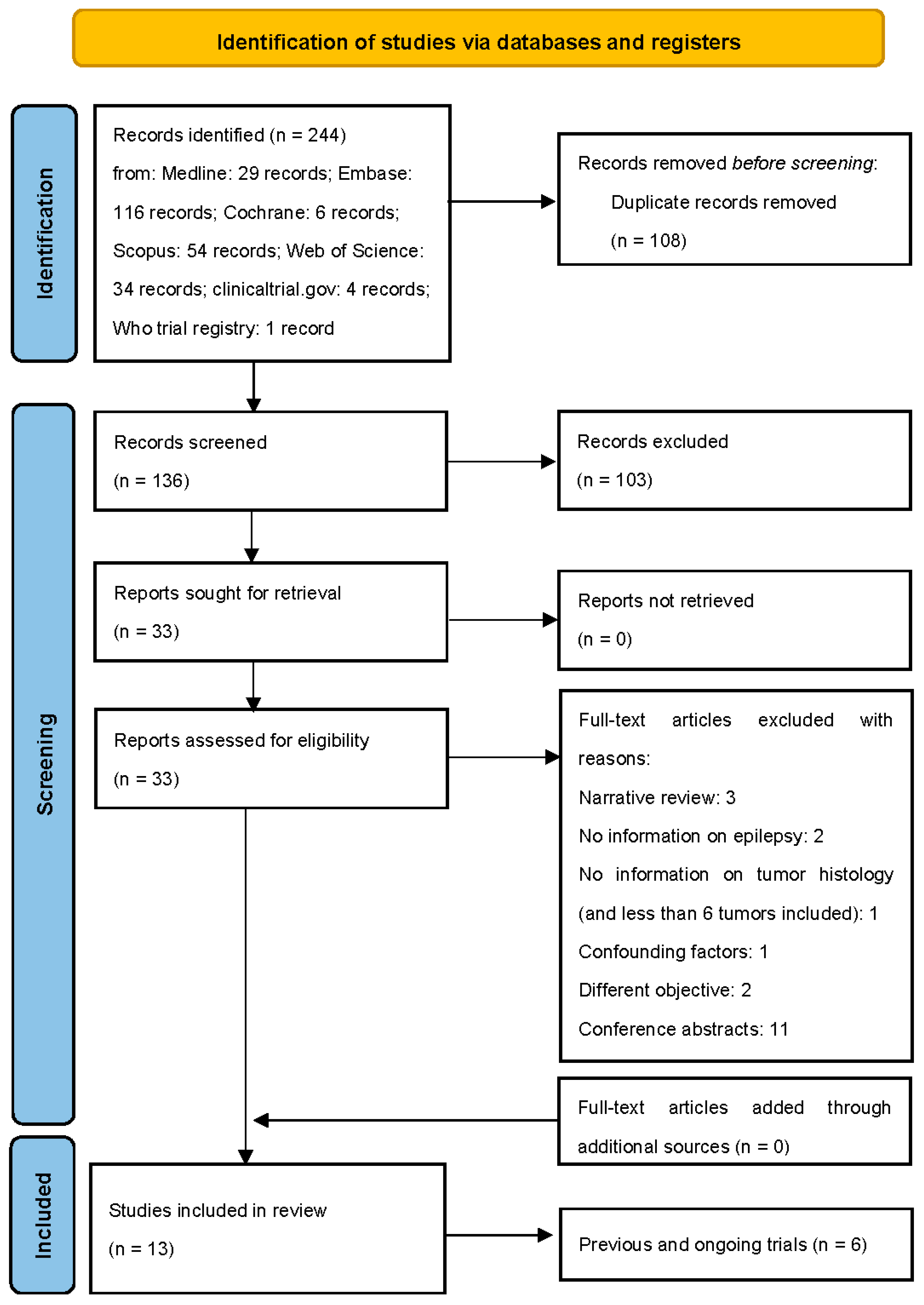
3.1. Results of the Search
3.2. Qualitative Review
3.2.1. Studies on Brain Tumor-Related Epilepsy (BTRE)
3.2.2. Studies on Glioma-Related Epilepsy

{kind=link}
| Author, Year | Study Design | Sample Size | Male/ Female | Age | Tumor Histology | IDH Mutation | mgmt Methylation | GTR N Patients | CT N Patients | Type of CT | RT N Patients | Seizure Semeiology | AED Monotherapy N Patients | AED Polytherapy N Patients | Final Dosage of Perampanel (mg/Day) | Follow-Up (Months) | N Patients at the End of Follow-Up | Primary Outcome | Secondary Outcome | Means of Cognitive Function Evaluation |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Coppola, 2020 | Single arm prospective | 36 | 23/13 | Median: 46 Range: 15–75 | LGG: 11 HGG 14 GBM: 7 Unclassified: 4 | Mutated: 6 Unmutated: 10 Unknown: 20 | Unmethylated: 4 Unknown: 25 | 13 | 29 | TMZ: 16 Fotoemustine: 4 Bevacizumab: 1 Other: 5 Unknown: 3 | 17 | Focal aware: 14 Focal unaware: 7 Focal to bilateral: 11 Generalized: 4 | 19 | 17 | 2 mg: 1; 4 mg: 7; 6 mg: 14; 7 mg: 1; 8 mg: 9; 10 mg: 3; 12 mg: 1 | 12 | 21 | Efficacy of PER (Responder rate: ≥50% reduction in seizure frequency; seizure freedom) | Retention rate; quality of life modification | QOLIE 31-P test |
| Maschio, 2020 | Single arm prospective | 26 | 16/10 | Mean: 47.5 Range: 32–75 | LGG: 8 HGG: 8 GBM: 7 Meningioma: 2 Metastasis: 1 | Mutated: 6 Unmutated: 11 Unknown: 9 | Unmethylated: 4 Unknown: 15 | 11 | 25 | TMZ: 13 Fotoemustine: 4 Bevacizumab: 1 Other: 4 Unknown: 3 | 11 | Focal aware: 1 Focal unaware: 6 Focal to bilateral: 7 | 11 | 15 | 2 mg: 1; 4 mg: 6; 6 mg: 9; 8 mg: 7; 10 mg: 2; 12 mg: 1 | 6 | 21 | Efficacy of PER (Responder rate: ≥50% reduction in seizure frequency; seizure freedom) | PER-related side effects; PER impact on cognition, mood, and quality of life | Battery of cognitive tests |
| Maschio, 2019 | Retrospective | 11 | 9/2 | Mean: 54 Range: 31–76 | AOA: 2 AA: 2 GBM: 3; LGA: 4 | Mutated: 3 Unmutated: 7 Unknown: 1 | Unmethylated: 5 Unknown: 1 | 6 | 7 | TMZ: 3 Fotoemustine: 2 Bevacizumab:1 Other:1 | 3 | Focal: 6 Focal to bilateral: 5 | 5 | 6 | 6 mg: 5 8 mg: 4 10 mg: 2 | 12 | 11 | Efficacy of PER (Responder rate: ≥50% reduction in seizure frequency; seizure freedom) | PER-related side effects | Not assessed |
| Chonan, 2020 | Retrospective | 18 | 9/9 | Mean: 50 Range 24–76 | DA: 2 AA: 5 OL G2: 3; AO: 1 GBM: 7 | Mutated: 10 Unmutated: 5 Unknown: 3 | NA | 2 | 16 | Nimustine hydrochloride (ACNU), TMZ, and bevacizumab: 15 TMZ: 1 Bevacizumab: 1 (for recurrence) | 17 (1 for recurrence) | Focal: 8 Focal to bilateral: 10 | 18 | 0 | 2 mg: 2 4 mg: 15 8 mg: 1 | 1–21 months (median, 10.6 months) | 18 | Efficacy of PER (number of patients achieving seizure freedom) | Time to seizure freedom; number and type of adverse events | Not assessed |
| Izumoto, 2018 | Single arm prospective | 12 | 8/4 | Mean: 57.8 Range: 31–84 | DA: 1 Oligoastrocytoma: 1 AA: 3 AO: 5 GBM: 2 | NA | NA | NA | 9 | TMZ: 6 Bevacizumab: 3 | 11 | Focal: 7 Focal to bilateral: 5 | 10 | 2 | 4 mg: 9 8 mg: 3 | 6 | 12 | Efficacy of PER (responder rate: ≥50% reduction in seizure frequency; seizure freedom) | tumor volume and peritumoral edema after 6 months of PER treatment | Not assessed |
| Dunn-Pirio, 2018 | Single arm prospective | 8 | 6/2 | Median: 45 Range: 35–61 | GBM: 2 AA: 2 OL: 2 DA: 2 | Mutated: 5 Unmutated: 2 Unknown: 1 | Unmethylated: 0 Unknown:1 | NA | NA | NA | NA | Focal: 8 | 2 | 6 | 6 mg: 4 8 mg: 4 | 6 | 6 | Seizure frequency | percentage of subjects with unacceptable adverse events | Not assessed |
| Vecht, 2017 | Single arm prospective | 12 | 9/3 | Median: 41 Range: 31–65 | Ganglioglioma: 1 Low-grade astro- or oligo(astro)dendroglioma: 6 Anaplastic astro- or oligo(astro)dendroglioma: 3 GBM: 2 | NA | NA | NA | 6 | NA | NA | Focal aware: 7 Focal unaware: 4 Generalized: 1 Focal SE: 2. | 0 | 12 | 2 mg: 1 4 mg: 2; 6 mg: 3; 8 mg: 3; 10 mg: 1; 12 mg: 2 | 6 | 12 | Efficacy of PER (Responder rate: ≥50% reduction in seizure frequency; seizure freedom) | Outcome on cognition | CTCS |
| Author, Year | Seizure Freedom N Patients (%) | ≥50% Re-Duction in Seizure Frequency N Patients (%) | <50% Re-Duction in Seizure Frequency N Patients (%) | Unchanged Seizure Frequency N Patients (%) | Worsening Seizure Frequency N Patients (%) | Adverse Events N Patients (%) | Type of Adverse Events | Retention Rate, N Patients (%) | Effect on Cognitive Function |
|---|---|---|---|---|---|---|---|---|---|
| Coppola, 2020 | 7 (33.3) | 12 (57.1) | 1 (4.8) | 1 (4.8) | 0 (0) | 11 (52.4) | Anxiety: 2 Aggressiveness: 2 Dizziness: 5 Fatigue: 2 | 21/36 (58.3) | Improvement |
| Maschio, 2020 | 7 (33.3) | 13 (61.9) | 0 (0) | 1 (4.8) | 0 (0) | 4 (19.1) | Vertigo: 4 Aggressiveness: 1 | 16/26 (61.5) | Stability |
| Maschio, 2019 | 5 (45.5) | 4 (36.4) | 0 (0) | 2 (18.2) | 0 (0) | 2 (18.2) | Anxiety: 2 Agitation: 2 | 11/11 (100) | NA |
| Chonan, 2020 | 17 (94.4) | NA | NA | NA | NA | 2 (11.1) | Irritability: 2 | 10/18 (55.6) | NA |
| Izumoto, 2018 | 6 (50) | 4 (33.3) | NA | NA | 0 (0) | 2 (16.7) | Dizziness: 2 (one after concomitant alcohol intake) | 10/12 (83.3) | NA |
| Dunn-Pirio, 2018 | 0 (0) | 6 (75) | 0 (0) | 0 (0) | 2 (25) | 8 (100) | Nausea: 1 Fatigue: 5 Dizziness: 2 Somnolence: 1 Confusion: 1 | 6/8 (75) | NA |
| Vecht, 2017 | 6 (50) | 3 (25) | 0 (0) | 2 (16.7) | 1 (8.3) | 6 (50) | Dizziness/vertigo: 4 Drowsiness: 2 | 10/12 (75) | Improvement: 6 Stability: 1 Worsening: 1 |
3.2.3. Overview of Registered Clinical Trials
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Maschio, M. Brain Tumor-Related Epilepsy. Curr. Neuropharmacol. 2012, 10, 124–133. [Google Scholar] [CrossRef]
- Coppola, A.; Zarabla, A.; Maialetti, A.; Villani, V.; Koudriavtseva, T.; Russo, E.; Nozzolillo, A.; Sueri, C.; Belcastro, V.; Balestrini, S.; et al. Perampanel Confirms to Be Effective and Well-Tolerated as an Add-On Treatment in Patients With Brain Tumor-Related Epilepsy (PERADET Study). Front. Neurol. 2020, 11, 592. [Google Scholar] [CrossRef]
- de Bruin, M.E.; van der Meer, P.B.; Dirven, L.; Taphoorn, M.J.B.; Koekkoek, J.A.F. Efficacy of Antiepileptic Drugs in Glioma Patients with Epilepsy: A Systematic Review. Neuro-Oncol. Pract. 2021, 8, 501–517. [Google Scholar] [CrossRef]
- Chen, J.-S.; Clarke, R.; Haddad, A.F.; Wang, E.J.; Lacroix, M.; Sarkar, I.N.; Zand, R.; Chen, E.S.; Toms, S.A. The Effect of Levetiracetam Treatment on Survival in Patients with Glioblastoma: A Systematic Review and Meta-Analysis. J. Neurooncol. 2022, 156, 257–267. [Google Scholar] [CrossRef] [PubMed]
- Rossi, J.; Cavallieri, F.; Biagini, G.; Rizzi, R.; Russo, M.; Cozzi, S.; Giaccherini, L.; Pisanello, A.; Valzania, F. Epileptogenesis and Tumorigenesis in Glioblastoma: Which Relationship? Medicina 2022, 58, 1349. [Google Scholar] [CrossRef]
- Pallud, J.; Capelle, L.; Huberfeld, G. Tumoral Epileptogenicity: How Does It Happen? Epilepsia 2013, 54 (Suppl. S9), 30–34. [Google Scholar] [CrossRef] [Green Version]
- Elbadry Ahmed, R.; Tang, H.; Asemota, A.; Huang, L.; Boling, W.; Bannout, F. Meningioma Related Epilepsy- Pathophysiology, Pre/Postoperative Seizures Predicators and Treatment. Front. Oncol. 2022, 12, 905976. [Google Scholar] [CrossRef] [PubMed]
- Rudà, R.; Mo, F.; Pellerino, A. Epilepsy in Brain Metastasis: An Emerging Entity. Curr. Treat. Options Neurol. 2020, 22, 6. [Google Scholar] [CrossRef]
- Steinhoff, B.J.; Ben-Menachem, E.; Ryvlin, P.; Shorvon, S.; Kramer, L.; Satlin, A.; Squillacote, D.; Yang, H.; Zhu, J.; Laurenza, A. Efficacy and Safety of Adjunctive Perampanel for the Treatment of Refractory Partial Seizures: A Pooled Analysis of Three Phase III Studies. Epilepsia 2013, 54, 1481–1489. [Google Scholar] [CrossRef] [PubMed]
- French, J.A.; Krauss, G.L.; Biton, V.; Squillacote, D.; Yang, H.; Laurenza, A.; Kumar, D.; Rogawski, M.A. Adjunctive Perampanel for Refractory Partial-Onset Seizures: Randomized Phase III Study 304. Neurology 2012, 79, 589–596. [Google Scholar] [CrossRef] [PubMed]
- Krauss, G.L.; Perucca, E.; Ben-Menachem, E.; Kwan, P.; Shih, J.J.; Clément, J.-F.; Wang, X.; Bagul, M.; Gee, M.; Zhu, J.; et al. Long-Term Safety of Perampanel and Seizure Outcomes in Refractory Partial-Onset Seizures and Secondarily Generalized Seizures: Results from Phase III Extension Study 307. Epilepsia 2014, 55, 1058–1068. [Google Scholar] [CrossRef] [Green Version]
- Lavu, A.; Aboulatta, L.; Abou-Setta, A.M.; Aloud, B.; Askin, N.; Rabbani, R.; Shouman, W.; Zarychanski, R.; Eltonsy, S. Efficacy and Safety of Perampanel in Epilepsy: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Seizure 2022, 102, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Yagi, C.; Tatsuoka, J.; Sano, E.; Hanashima, Y.; Ozawa, Y.; Yoshimura, S.; Yamamuro, S.; Sumi, K.; Hara, H.; Katayama, Y.; et al. Anti-tumor Effects of Anti-epileptic Drugs in Malignant Glioma Cells. Oncol. Rep. 2022, 48, 1–12. [Google Scholar] [CrossRef]
- Lange, F.; Hartung, J.; Liebelt, C.; Boisserée, J.; Resch, T.; Porath, K.; Hörnschemeyer, J.; Reichart, G.; Sellmann, T.; Neubert, V.; et al. Perampanel Add-on to Standard Radiochemotherapy in Vivo Promotes Neuroprotection in a Rodent F98 Glioma Model. Front. Neurosci. 2020, 14, 598266. [Google Scholar] [CrossRef] [PubMed]
- Maschio, M.; Zarabla, A.; Maialetti, A.; Giannarelli, D.; Koudriavtseva, T.; Villani, V.; Zannino, S. Perampanel in Brain Tumor-Related Epilepsy: Observational Pilot Study. Brain Behav. 2020, 10, e01612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maschio, M.; Pauletto, G.; Zarabla, A.; Maialetti, A.; Lus, T.; Villani, V.; Fabi, A.; Koudriavtseva, T.; Giannarelli, D. Perampanel in Patients with Brain Tumor-Related Epilepsy in Real-Life Clinical Practice: A Retrospective Analysis. Int. J. Neurosci. 2019, 129, 593–597. [Google Scholar] [CrossRef] [PubMed]
- Chonan, M.; Saito, R.; Kanamori, M.; Osawa, S.-I.; Watanabe, M.; Suzuki, H.; Nakasato, N.; Tominaga, T. Experience of Low Dose Perampanel to Add-on in Glioma Patients with Levetiracetam-Uncontrollable Epilepsy. Neurol. Med. Chir. 2020, 60, 37–44. [Google Scholar] [CrossRef] [Green Version]
- Izumoto, S.; Miyauchi, M.; Tasaki, T.; Okuda, T.; Nakagawa, N.; Nakano, N.; Kato, A.; Fujita, M. Seizures and Tumor Progression in Glioma Patients with Uncontrollable Epilepsy Treated with Perampanel. Anticancer Res. 2018, 38, 4361–4366. [Google Scholar] [CrossRef]
- Dunn-Pirio, A.M.; Woodring, S.; Lipp, E.; Herndon, J.E.; Healy, P.; Weant, M.; Randazzo, D.; Desjardins, A.; Friedman, H.S.; Peters, K.B. Adjunctive Perampanel for Glioma-Associated Epilepsy. Epilepsy Behav. Case Rep. 2018, 10, 114–117. [Google Scholar] [CrossRef] [PubMed]
- Vecht, C.; Duran-Peña, A.; Houillier, C.; Durand, T.; Capelle, L.; Huberfeld, G. Seizure Response to Perampanel in Drug-Resistant Epilepsy with Gliomas: Early Observations. J. Neurooncol. 2017, 133, 603–607. [Google Scholar] [CrossRef]
- French, J.A.; Krauss, G.L.; Steinhoff, B.J.; Squillacote, D.; Yang, H.; Kumar, D.; Laurenza, A. Evaluation of Adjunctive Perampanel in Patients with Refractory Partial-Onset Seizures: Results of Randomized Global Phase III Study 305. Epilepsia 2013, 54, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Krauss, G.L.; Serratosa, J.M.; Villanueva, V.; Endziniene, M.; Hong, Z.; French, J.; Yang, H.; Squillacote, D.; Edwards, H.B.; Zhu, J.; et al. Randomized Phase III Study 306: Adjunctive Perampanel for Refractory Partial-Onset Seizures. Neurology 2012, 78, 1408–1415. [Google Scholar] [CrossRef] [PubMed]
- Trinka, E.; Steinhoff, B.J.; Nikanorova, M.; Brodie, M.J. Perampanel for Focal Epilepsy: Insights from Early Clinical Experience. Acta Neurol. Scand. 2016, 133, 160–172. [Google Scholar] [CrossRef] [Green Version]
- Vazquez, B.; Yang, H.; Williams, B.; Zhou, S.; Laurenza, A. Perampanel Efficacy and Safety by Gender: Subanalysis of Phase III Randomized Clinical Studies in Subjects with Partial Seizures. Epilepsia 2015, 56, e90–e94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lattanzi, S.; Cagnetti, C.; Foschi, N.; Ciuffini, R.; Osanni, E.; Chiesa, V.; Dainese, F.; Dono, F.; Canevini, M.P.; Evangelista, G.; et al. Adjunctive Perampanel in Older Patients With Epilepsy: A Multicenter Study of Clinical Practice. Drugs Aging 2021, 38, 603–610. [Google Scholar] [CrossRef]
- Witt, J.-A.; Helmstaedter, C. The Impact of Perampanel on Cognition: A Systematic Review of Studies Employing Standardized Tests in Patients with Epilepsy. Seizure 2022, 94, 107–111. [Google Scholar] [CrossRef] [PubMed]
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A Summary. Neuro-Oncol. 2021, 23, 1231–1251. [Google Scholar] [CrossRef]

| Name (ID) (Year) | Study Design | Status | Population | Intervention | Comparison | Outcome |
|---|---|---|---|---|---|---|
| NCT02363933 (2015) | Phase 2 single-arm study | Completed (see Dunn-Pirio et al.) [19] | 9 patients diagnosed with glioma and refractory partial onset seizure activity (defined as 3 or more seizures in a 28-day period) on levetiracetam monotherapy | Perampanel + current anti-epileptic drug | Current anti-epileptic drug | Percentage of patients with ≥50% seizure reduction during the maintenance period compared with seizure frequency before initiation of perampanel |
| JPRN-UMIN000026095 (2017) | Single arm non-randomized | Pending | 20 post-operative glioma patients with epilepsy | Addition of 8 mg of perampanel on the patients treated with 1000 mg of levetiracetam for 1 year | NA (single arm non-randomized) | Seizure free rate (Time Frame: 12 months after treatment); Overall survival; Progression-free survival |
| ACTRN12617000078358 (2017) | Randomized controlled trial | Stopped early | 40 patients with radiological diagnosis of a supratentorial WHO grade II-III glioma who experienced a pre-operative seizure attributed to glioma | Perampanel increased to 6 mg/d | Levetiracetam | Proportion of patients seizure-free for 24 or more continuous weeks in assessment phase (weeks 5–52)—assessed by seizure diary; Time to first seizure in assessment phase (weeks 5–52)—assessed by seizure diary |
| NCT04497142 (2020) | Non-randomized interventional | Recruiting | 20 patients with radiologic evidence of anaplastic astrocytoma or GBM. | Predetermined first dose of perampanel on the day before their tumor surgery | Standard of care | Rate of high frequency oscillations [Time Frame: Peri-operative] |
| NCT04650204 (2020) | Non-randomized interventional | Recruiting | 40 patients with a diagnosis of biopsy-proven high-grade glioma and epilepsy refractory to at least 1, drug. | Perampanel | Conventional antiepileptic treatment | Number of patients with a high-grade glioma who achieve a >50% reduction in focal seizures with perampanel after failing 1 or more anti-seizure drugs at 3 and 6 months; overall survival; decline in neuropsychological function. |
| NCT03636958 (2021) | Randomized controlled trial | Withdrawn (concomitant decision of the sponsor and the PI, lack of patients) | Patients with a diagnosis of glioma-refractory epilepsy | Perampanel | Conventional antiepileptic treatment | Monthly frequency of seizures |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rossi, J.; Cavallieri, F.; Bassi, M.C.; Biagini, G.; Rizzi, R.; Russo, M.; Bondavalli, M.; Iaccarino, C.; Pavesi, G.; Cozzi, S.; et al. Efficacy and Tolerability of Perampanel in Brain Tumor-Related Epilepsy: A Systematic Review. Biomedicines 2023, 11, 651. https://doi.org/10.3390/biomedicines11030651
Rossi J, Cavallieri F, Bassi MC, Biagini G, Rizzi R, Russo M, Bondavalli M, Iaccarino C, Pavesi G, Cozzi S, et al. Efficacy and Tolerability of Perampanel in Brain Tumor-Related Epilepsy: A Systematic Review. Biomedicines. 2023; 11(3):651. https://doi.org/10.3390/biomedicines11030651
Chicago/Turabian StyleRossi, Jessica, Francesco Cavallieri, Maria Chiara Bassi, Giuseppe Biagini, Romana Rizzi, Marco Russo, Massimo Bondavalli, Corrado Iaccarino, Giacomo Pavesi, Salvatore Cozzi, and et al. 2023. "Efficacy and Tolerability of Perampanel in Brain Tumor-Related Epilepsy: A Systematic Review" Biomedicines 11, no. 3: 651. https://doi.org/10.3390/biomedicines11030651