

Diagnosis and Assessment of Dental Caries Using Novel Bioactive Caries Detecting Dye Solution
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical and Subject Selection
2.2. Sample Size
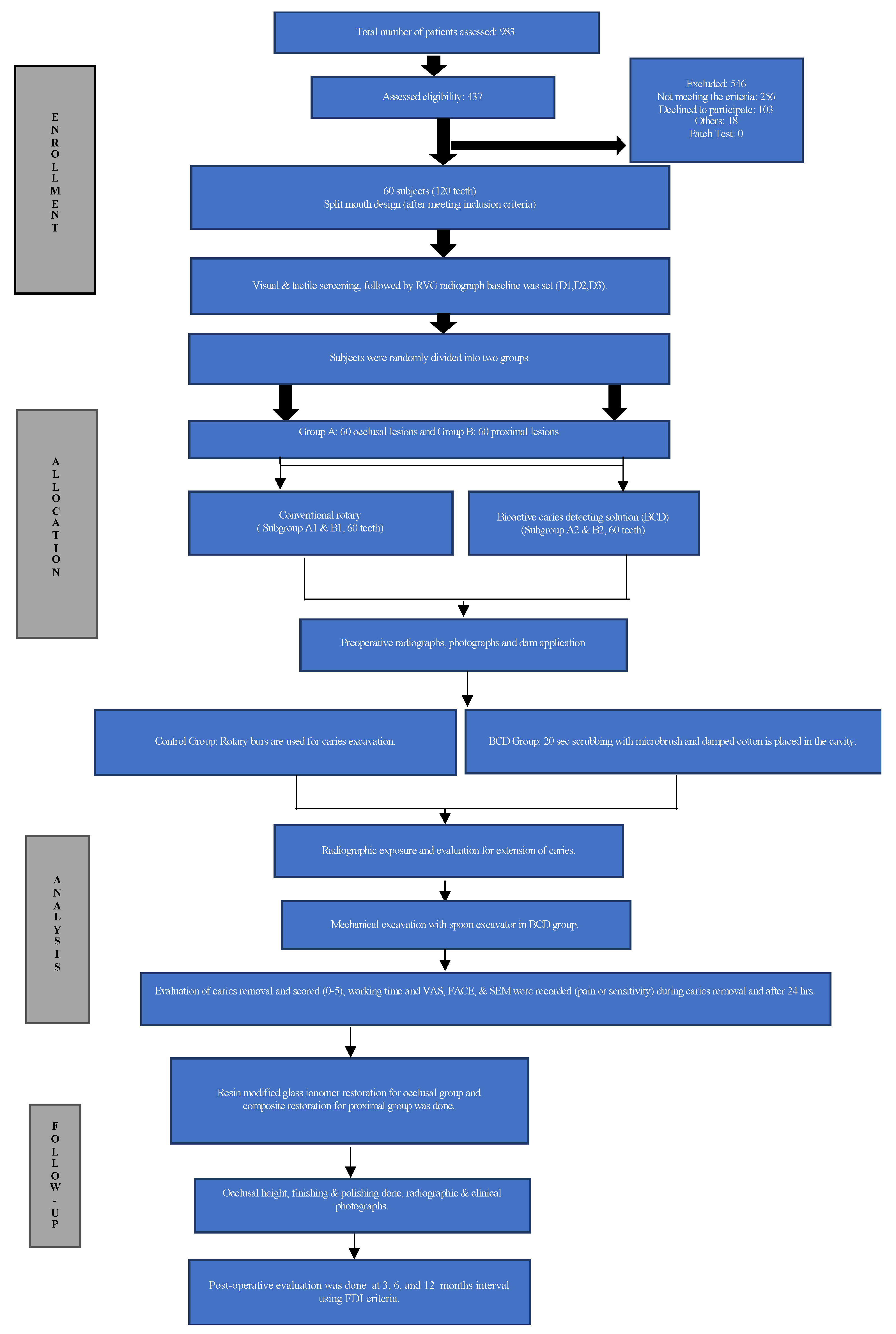
2.3. Study Design
2.4. Treatment
Caries Excavation and Treatment Time
2.5. Evaluations
3. Results
4. Discussion
5. Conclusions
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cury, J.A.; Tenuta, L.M.A. Enamel Remineralization: Controlling the Caries Disease or Treating Early Caries Lesions? Braz. Oral Res. 2009, 23 (Suppl. 1), 23–30. [Google Scholar] [CrossRef]
- Robinson, C.; Shore, R.C.; Brookes, S.J.; Strafford, S.; Wood, S.R.; Kirkham, J. The Chemistry of Enamel Caries. Crit. Rev. Oral Biol. Med. Off. Publ. Am. Assoc. Oral Biol. 2000, 11, 481–495. [Google Scholar] [CrossRef]
- Najibfard, K.; Ramalingam, K.; Chedjieu, I.; Amaechi, B.T. Remineralization of Early Caries by a Nano-Hydroxyapatite Dentifrice. J. Clin. Dent. 2011, 22, 139. [Google Scholar]
- Goldberg, M. Enamel and Dentin Carious Lesions. JSM Dent. 2020, 8, 1120. [Google Scholar]
- Alfaya, T.; Cardoso Guedes, C.; Fernandes, K.P.; Bussadori, S.; Matsumoto, S.F.; Motta, L. Assessment of Chemomechanical Removal of Carious Lesions Using Papacarie Duo TM: Randomized Longitudinal Clinical Trial. Indian J. Dent. Res. 2013, 24, 488. [Google Scholar] [CrossRef]
- Shashirekha, G.; Jena, A.; Mohanty, N.; Kamilla, S. Novel Bioactive Caries-Detecting Dye Solution: Cytotoxicity, Antimicrobial Activity, Scanning Electron Microscope, and Stereomicroscopic Analysis in Diagnosis of Dental Caries. J. Conserv. Dent. 2020, 23, 79. [Google Scholar] [CrossRef]
- Lesaffre, E.; Philstrom, B.; Needleman, I.; Worthington, H. The Design and Analysis of Split-Mouth Studies: What Statisticians and Clinicians Should Know. Stat. Med. 2009, 28, 3470–3482. [Google Scholar] [CrossRef]
- Hickel, R.; Peschke, A.; Tyas, M.; Mjör, I.; Bayne, S.; Peters, M.; Hiller, K.-A.; Randall, R.; Vanherle, G.; Heintze, S.D. FDI World Dental Federation: Clinical Criteria for the Evaluation of Direct and Indirect Restorations—Update and Clinical Examples. Clin. Oral Investig. 2010, 14, 349–366. [Google Scholar] [CrossRef]
- Zhu, H.; Zhang, S.; Ahn, C. Sample Size Considerations for Split-Mouth Design. Stat. Methods Med. Res. 2017, 26, 2543–2551. [Google Scholar] [CrossRef]
- Yousef, M.; Atwa, M.; Althubaitiy, R. Clinical and Radiographic Evaluation of Composite Restorations by Dental Students. Life Sci. J. 2014, 11, 869–872. [Google Scholar]
- Hosoya, Y.; Taguchi, T.; Tay, F.R. Evaluation of a New Caries Detecting Dye for Primary and Permanent Carious Dentin. J. Dent. 2007, 35, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Ericson, D.; Zimmerman, M.; Raber, H.; Götrick, B.; Bornstein, R.; Thorell, J. Clinical Evaluation of Efficacy and Safety of a New Method for Chemo-Mechanical Removal of Caries. A Multi-Centre Study. Caries Res. 1999, 33, 171–177. [Google Scholar] [CrossRef]
- Kumar, J.; Nayak, M.; Prasad, K.; Gupta, N. A Comparative Study of the Clinical Efficiency of Chemomechanical Caries Removal Using Carisolv ® and Papacarie ® - A Papain Gel. Indian J. Dent. Res. 2012, 23, 697. [Google Scholar] [CrossRef]
- Yildirim, C.; Akgun, O.; Polat, G.; Ok, M.; Altun, C.; Basak, F. Assessment of Dental Fear in Turkish Children with the Frankl Behavior Rating Scale (FS) and the Sound-Eye-Motor (SEM) Scale. Gulhane Med. J. 2017, 1. [Google Scholar] [CrossRef]
- Hamie, S.; Badr, S.; Ragab, H. Clinical and Radiographic Evaluation of Glass Ionomer Compared to Resin Composite in Restoring Primary Molars: A 1-Year Prospective Randomized Study. J. Pediatr. Dent. 2017, 5, 6. [Google Scholar] [CrossRef]
- Zanatta, R.F.; da Silva, T.M.; Esper, M.A.L.R.; Bresciani, E.; Caneppele, T.M.F.; de Paiva Gonçalves, S.E. Guidelines for Conducting Split-Mouth Clinical Studies in Restorative Dentistry. Braz. Dent. Sci. 2017, 20, 29. [Google Scholar] [CrossRef]
- Govind, S.; Kamilla, S.; Nanda, B.; Jena, A.; Mohanty, N. Physical and Chemical Characterizations of Novel Bioactive Caries Detecting Solution. Dent. Hypotheses 2021, 12, 8. [Google Scholar] [CrossRef]
- Lukacs, J.R. Gender Differences in Oral Health in South Asia: Metadata Imply Multifactorial Biological and Cultural Causes. Am. J. Hum. Biol. Off. J. Hum. Biol. Counc. 2011, 23, 398–411. [Google Scholar] [CrossRef]
- Ferraro, M.; Vieira, A.R. Explaining Gender Differences in Caries: A Multifactorial Approach to a Multifactorial Disease. Int. J. Dent. 2010, 2010, 649643. [Google Scholar] [CrossRef]
- Shaffer, J.R.; Leslie, E.J.; Feingold, E.; Govil, M.; McNeil, D.W.; Crout, R.J.; Weyant, R.J.; Marazita, M.L. Caries Experience Differs between Females and Males across Age Groups in Northern Appalachia. Int. J. Dent. 2015, 2015, e938213. [Google Scholar] [CrossRef]
- Kielbassa, A.M.; Paris, S.; Lussi, A.; Meyer-Lueckel, H. Evaluation of Cavitations in Proximal Caries Lesions at Various Magnification Levels in Vitro. J. Dent. 2006, 34, 817–822. [Google Scholar] [CrossRef]
- Chaussain-Miller, C.; Decup, F.; Domejean-Orliaguet, S.; Gillet, D.; Guigand, M.; Kaleka, R.; Laboux, O.; Lafont, J.; Medioni, E.; Serfaty, R.; et al. Clinical Evaluation of the Carisolv Chemomechanical Caries Removal Technique According to the Site/Stage Concept, a Revised Caries Classification System. Clin. Oral Investig. 2003, 7, 32–37. [Google Scholar] [CrossRef]
- Alshehri, D.F.A.; Aldossary, D.M.S. Chemomechanical Caries Removal: An Insight into the Agents’ Development and the Clinical Efficiency. Biol. Med. 2018, 5, 6. [Google Scholar]
- Shakya, V.K.; Chandra, A.; Tikku, A.P.; Verma, P.; Yadav, R.K. A Comparative Evaluation of Dentin Caries Removal with Polymer Bur and Conventional Burs—An in Vitro Study. Open J. Stomatol. 2012, 2, 12–15. [Google Scholar] [CrossRef] [Green Version]
- Kochhar, G.K.; Srivastava, N.; Pandit, I.; Gugnani, N.; Gupta, M. An Evaluation of Different Caries Removal Techniques in Primary Teeth: A Comparitive Clinical Study. J. Clin. Pediatr. Dent. 2011, 36, 5–10. [Google Scholar] [CrossRef]
- Boston, D.W. New Device for Selective Dentin Caries Removal. Quintessence Int. 2003, 34, 678–685. [Google Scholar]
- Hamama, H.; Yiu, C.; Burrow, M. Current Update of Chemomechanical Caries Removal Methods. Aust. Dent. J. 2014, 59, 446–456. [Google Scholar] [CrossRef]
- Ali, A.H.; Thani, F.B.; Foschi, F.; Banerjee, A.; Mannocci, F. Self-Limiting versus Rotary Subjective Carious Tissue Removal: A Randomized Controlled Clinical Trial—2-Year Results. J. Clin. Med. 2020, 9, 2738. [Google Scholar] [CrossRef]
- Pitts, N. Understanding Dental Caries – from Pathogenesis to Prevention and Therapy. In Understanding Dental Caries; Goldberg, M., Ed.; Springer International Publishing: Cham, Switzerland, 2016; pp. 3–9. ISBN 978-3-319-30550-9. [Google Scholar]
- Newbrun, E. Cariology; Williams & Wilkins: Baltimore, MD, USA, 1983; ISBN 978-0-683-06461-2. [Google Scholar]
- Lozano-Chourio, M.A.; Zambrano, O.; Gonzalez, H.; Quero, M. Clinical Randomized Controlled Trial of Chemomechanical Caries Removal (CarisolvTM). Int. J. Paediatr. Dent. 2006, 16, 161–167. [Google Scholar]
- Butera, A.; Pascadopoli, M.; Gallo, S.; Lelli, M.; Tarterini, F.; Giglia, F.; Scribante, A. SEM/EDS Evaluation of the Mineral Deposition on a Polymeric Composite Resin of a Toothpaste Containing Biomimetic Zn-Carbonate Hydroxyapatite (MicroRepair®) in Oral Environment: A Randomized Clinical Trial. Polymers 2021, 13, 2740. [Google Scholar] [CrossRef]
- Scanlan, C.A.; Rahmani, H.; Bowles, R.; Bennamoun, M. Three-Dimensional Scanning for Measurement of Bulk Density in Gravelly Soils. Soil Use Manag. 2018, 34, 380–387. [Google Scholar] [CrossRef]
- de A. Neves, A.; Coutinho, E.; De Munck, J.; Van Meerbeek, B. Caries-Removal Effectiveness and Minimal-Invasiveness Potential of Caries-Excavation Techniques: A Micro-CT Investigation. J. Dent. 2011, 39, 154–162. [Google Scholar] [CrossRef]
- Vusurumarthi, V.; Ballullaya, S.V.; Pushpa, S.; Veluvarti, V.R.K.; Loka, P.R.; Galla, P.K. Evaluation and Comparison of Caries Excavation Efficacy of Three Different Burs: A Micro-Computed Tomographic-Assisted Study. J. Int. Soc. Prev. Community Dent. 2020, 10, 213–219. [Google Scholar] [CrossRef]
- Husain, S.; Al-Samadani, K.H.; Najeeb, S.; Zafar, M.S.; Khurshid, Z.; Zohaib, S.; Qasim, S.B. Chitosan Biomaterials for Current and Potential Dental Applications. Materials 2017, 10, 602. [Google Scholar] [CrossRef]
- Maru, V.P.; Shakuntala, B.S.; Nagarathna, C. Caries Removal by Chemomechanical (CarisolvTM) vs. Rotary Drill: A Systematic Review. Open Dent. J. 2015, 9, 462–472. [Google Scholar] [CrossRef]
- Dermata, A.; Papageorgiou, S.N.; Fragkou, S.; Kotsanos, N. Comparison of Resin Modified Glass Ionomer Cement and Composite Resin in Class II Primary Molar Restorations: A 2-Year Parallel Randomised Clinical Trial. Eur. Arch. Paediatr. Dent. Off. J. Eur. Acad. Paediatr. Dent. 2018, 19, 393–401. [Google Scholar] [CrossRef] [Green Version]
- Donmez, S.B.; Uysal, S.; Dolgun, A.; Turgut, M.D. Clinical Performance of Aesthetic Restorative Materials in Primary Teeth According to the FDI Criteria. Eur. J. Paediatr. Dent. 2016, 17, 202–212. [Google Scholar]
- Banomyong, D.; Harnirattisai, C.; Burrow, M.F. Posterior Resin Composite Restorations with or without Resin-Modified, Glass-Ionomer Cement Lining: A 1-Year Randomized, Clinical Trial. J. Investig. Clin. Dent. 2011, 2, 63–69. [Google Scholar] [CrossRef]
- Yantcheva, S.M. Marginal Adaptation and Micropermeability of Class II Cavities Restored with Three Different Types of Resin Composites—A Comparative Ten-Month In Vitro Study. Polymers 2021, 13, 1660. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Occlusal | Control | BCD | p-Value | |
|---|---|---|---|---|
| Mean time (S) | 197.90 | 292.13 | <0.001 † | |
| Caries removal score | Score 0 | 24 (80.0) | 22 (73.3) | 0.542 |
| Color score | Black Brown Yellow | 2 (6.7) 4 (13.3) 24 (80.0) | 3 (10.0) 5 (16.7) 22 (73.3) | 0.820 |
| Consistency | Hard | 30 (100.0) | 30 (100.0) | - |
| Mean carious removal volume (mm3) | 1.10 | 0.82 | 0.003 † | |
| Mean VAS score | During | 4.03 | 1.96 | <0.001 † |
| Mean FACE score | During | 2.50 | 1.76 | 0.004 |
| Mean SEM score | During | 2.80 | 1.90 | <0.001 † |
| Proximal | Control | BCD | p-Value | |
|---|---|---|---|---|
| Mean time (S) | 273.06 | 411.86 | <0.001 † | |
| Caries removal score | Score 0 Score 1 Score 2 | 23 (76.7) 5 (16.7) 2 (6.7) | 20 (66.7) 9 (30.0) 1 (3.3) | 0.432 |
| Color score | Black Brown Yellow | 0 (0.0) 7 (23.3) 23 (76.7) | 0 (0.0) 11 (36.7) 19 (63.3) | 0.260 |
| Consistency | Hard | 30 (100.0) | 30 (100.0) | - |
| Mean carious removal volume (mm3) | 32.41 | 28.79 | 0.417 | |
| Mean VAS score | During | 4.23 | 2.73 | <0.001 † |
| Mean FACE score | During | 3.20 | 2.56 | 0.001 † |
| Mean SEM score | During | 3.03 | 2.03 | <0.001 † |
| Occlusal | Period (Months) | Clinically Excellent | Clinically Good | Clinically Satisfactory | Clinically Unsatisfactory | Clinically Poor | p-Value | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Control | BCD | Control | BCD | Control | BCD | Control | BCD | Control | BCD | |||
| Aesthetic | 3 | 5 (16.7) | 6 (20.0) | 11 (36.7) | 16 (53.3) | 8 (26.7) | 7 (23.3) | 4 (13.3) | 0 (0.0) | 2 (6.7) | 1 (3.3) | 0.247 |
| 6 | 14 (46.7) | 15 (50.0) | 6 (20.0) | 2 (6.7) | 3 (10.0) | 5 (16.7) | 0 (0.0) | 2 (6.7) | 7 (23.3) | 6 (20.0) | 0.330 | |
| 12 | 10 (37.0) | 13 (48.1) | 15 (55.6) | 14 (51.9) | 0 (0.0) | 0 (0.0) | 1 (3.7) | 0 (0.0) | 1 (3.7) | 0 (0.0) | 0.489 | |
| Functional | 3 | 12 (40.0) | 21 (70.0) | 16 (53.3) | 8 (26.7) | 2 (6.7) | 1 (3.3) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0.065 |
| 6 | 20 (66.7) | 17 (56.7) | 3 (10.0) | 5 (16.7) | 0 (0.0) | 1 (3.3) | 3 (10.0) | 3 (3.3) | 4 (13.3) | 4 (13.3) | 0.783 | |
| 12 | 11 (40.7) | 15 (55.6) | 14 (51.9) | 12 (44.4) | 0 (0.0) | 0 (0.0) | 1 (3.7) | 0 (0.0) | 1 (3.7) | 0 (0.0) | 0.429 | |
| Biological | 3 | 22 (73.3) | 23 (76.7) | 7 (23.3) | 7 (23.3) | 1 (3.3) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0.600 |
| 6 | 19 (63.3) | 17 (56.7) | 3 (10.0) | 3 (10.0) | 1 (3.3) | 4 (13.3) | 4 (13.3) | 3 (10.0) | 3 (10.0) | 3 (10.0) | 0.726 | |
| 12 | 13 (48.1) | 20 (74.1) | 12 (44.4) | 7 (25.9) | 0 (0.0) | 0 (0.0) | 2 (7.4) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0.091 | |
| Radiology | 3 | 30 (100.0) | 30 (100.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | - |
| 6 | 26 (86.7) | 23 (76.7) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 4 (13.3) | 7 (23.3) | 0.317 | |
| 12 | 25 (92.6) | 27 (100.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 2 (7.4) | 0 (0.0) | 0.150 | |
| Proximal | Period (months) | Clinically Excellent | Clinically Good | Clinically Satisfactory | Clinically Unsatisfactory | Clinically Poor | p-Value | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Control | BCD | Control | BCD | Control | BCD | Control | BCD | Control | BCD | |||
| Aesthetic | 3 | 19 (63.3) | 12 (40.0) | 8 (26.7) | 14 (46.7) | 0 (0.0) | 1 (3.3) | 1 (3.3) | 2 (6.7) | 2 (6.7) | 1 (3.3) | 0.299 |
| 6 | 20 (66.7) | 19 (63.3) | 3 (10.0) | 1 (3.3) | 3 (10.0) | 4 (13.3) | 2 (6.7) | 1 (3.3) | 2 (6.7) | 5 (16.7) | 0.594 | |
| 12 | 14 (51.9) | 13 (48.1) | 11 (40.7) | 14 (51.9) | 1 (3.7) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (3.7) | 0 (0.0) | 0.494 | |
| Functional | 3 | 22 (73.3) | 25 (83.3) | 4 (13.3) | 3 (10.0) | 0 (0.0) | 0 (0.0) | 1 (3.3) | 2 (6.7) | 3 (10.0) | 0 (0.0) | 0.300 |
| 6 | 16 (53.3) | 16 (53.3) | 5 (16.7) | 3 (10.0) | 1 (3.3) | 1 (3.3) | 3 (10.0) | 4 (13.3) | 5 (16.7) | 6 (20.0) | 0.947 | |
| 12 | 13 (48.1) | 11 (40.7) | 11 (40.7) | 15 (55.6) | 2 (7.4) | 1 (3.7) | 0 (0.0) | 0 (0.0) | 1 (3.7) | 0 (0.0) | 0.549 | |
| Biological | 3 | 25 (83.3) | 25 (83.3) | 2 (6.7) | 5 (16.7) | 0 (0.0) | 0 (0.0) | 2 (6.7) | 0 (0.0) | 1 (3.3) | 0 (0.0) | 0.232 |
| 6 | 18 (60.0) | 18 (60.0) | 4 (13.3) | 3 (10.0) | 2 (6.7) | 3 (10.0) | 4 (13.3) | 3 (10.0) | 2 (6.7) | 3 (10.0) | 0.953 | |
| 12 | 13 (48.1) | 11 (40.7) | 11 (40.7) | 13 (48.1) | 2 (7.4) | 3 (11.1) | 0 (0.0) | 0 (0.0) | 1 (3.7) | 0 (0.0) | 0.675 | |
| Radiology | 3 | 26 (89.7) | 28 (93.3) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (3.3) | 2 (6.9) | 0 (0.0) | 2 (6.9) | 1 (3.3) | 0.495 |
| 6 | 22 (73.3) | 19 (63.3) | 1 (3.3) | 0 (0.0) | 1 (3.3) | 5 (16.7) | 0 (0.0) | 0 (0.0) | 6 (20.0) | 6 (20.0) | 0.274 | |
| 12 | 16 (59.3) | 15 (55.6) | 8 (29.6) | 10 (37.0) | 2 (7.4) | 2 (7.4) | 0 (0.0) | 0 (0.0) | 1 (3.7) | 0 (0.0) | 0.740 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Govind, S.; Jena, A.; Kamilla, S.K.; Mohanty, N.; Mallikarjuna, R.M.; Nalawade, T.; Saraf, S.; Khaldi, N.A.; Jahdhami, S.A.; Shivagange, V. Diagnosis and Assessment of Dental Caries Using Novel Bioactive Caries Detecting Dye Solution. Biomedicines 2023, 11, 500. https://doi.org/10.3390/biomedicines11020500
Govind S, Jena A, Kamilla SK, Mohanty N, Mallikarjuna RM, Nalawade T, Saraf S, Khaldi NA, Jahdhami SA, Shivagange V. Diagnosis and Assessment of Dental Caries Using Novel Bioactive Caries Detecting Dye Solution. Biomedicines. 2023; 11(2):500. https://doi.org/10.3390/biomedicines11020500
Chicago/Turabian StyleGovind, Shashirekha, Amit Jena, Sushanta Kumar Kamilla, Neeta Mohanty, Rachappa M. Mallikarjuna, Triveni Nalawade, Sanjay Saraf, Naseer Al Khaldi, Salma Al Jahdhami, and Vinay Shivagange. 2023. "Diagnosis and Assessment of Dental Caries Using Novel Bioactive Caries Detecting Dye Solution" Biomedicines 11, no. 2: 500. https://doi.org/10.3390/biomedicines11020500