
The Role of Probiotics in Inducing and Maintaining Remission in Crohn’s Disease and Ulcerative Colitis: A Systematic Review of the Literature

 , , , ,
, , , ,  and
and
Abstract
:1. Introduction
- Examine if probiotic treatment can induce and maintain remission in adults.
- Examine differences in efficacy between various probiotic strains, as well as differences between symbiotic treatment and therapeutic formulas containing only one type of microorganism.
- Compare treatment options concerning the duration of treatment, examining their possible role in the long-term maintenance of remission.
- Compare probiotic treatment with approved therapeutic options, such as mesalazine.
- Examine differences in the efficacy of probiotics when provided in active and inactive stages of the disease.
2. Materials and Methods
2.1. Ethical Considerations
2.2. Search Strategy
2.3. Eligibility Criteria
- Randomized controlled trials (RCTs).
- Studies about participants diagnosed with inflammatory bowel diseases.
- Studies published in the English language.
- Studies including at least one comparison between a patients group receiving probiotics and a control group which did not.
- Studies examining remission using endoscopic and clinical scores as well as inflammation markers and clinical relapse rate.
- Reviews, case reports, correspondences, and non-randomized clinical trials (non-RCTs).
- Not providing measurement methods and outcomes.
- Studies conducted on animals.
- Studies conducted on children and adolescents.
- Studies measuring changes in microflora and not providing results about remission of disease.
2.4. Data Extraction and Quality Assessment
- Were the research question and primary outcomes clearly stated?
- Was the sample number >100?
- Were the characteristics of the sample well stated without significant differences between the test and control groups?
- Was the treatment method for probiotics clearly stated? (Type, duration, dose, other treatments).
- Was the patient’s status of disease clearly stated before intervention? (Active disease, diagnosis criteria).
3. Results
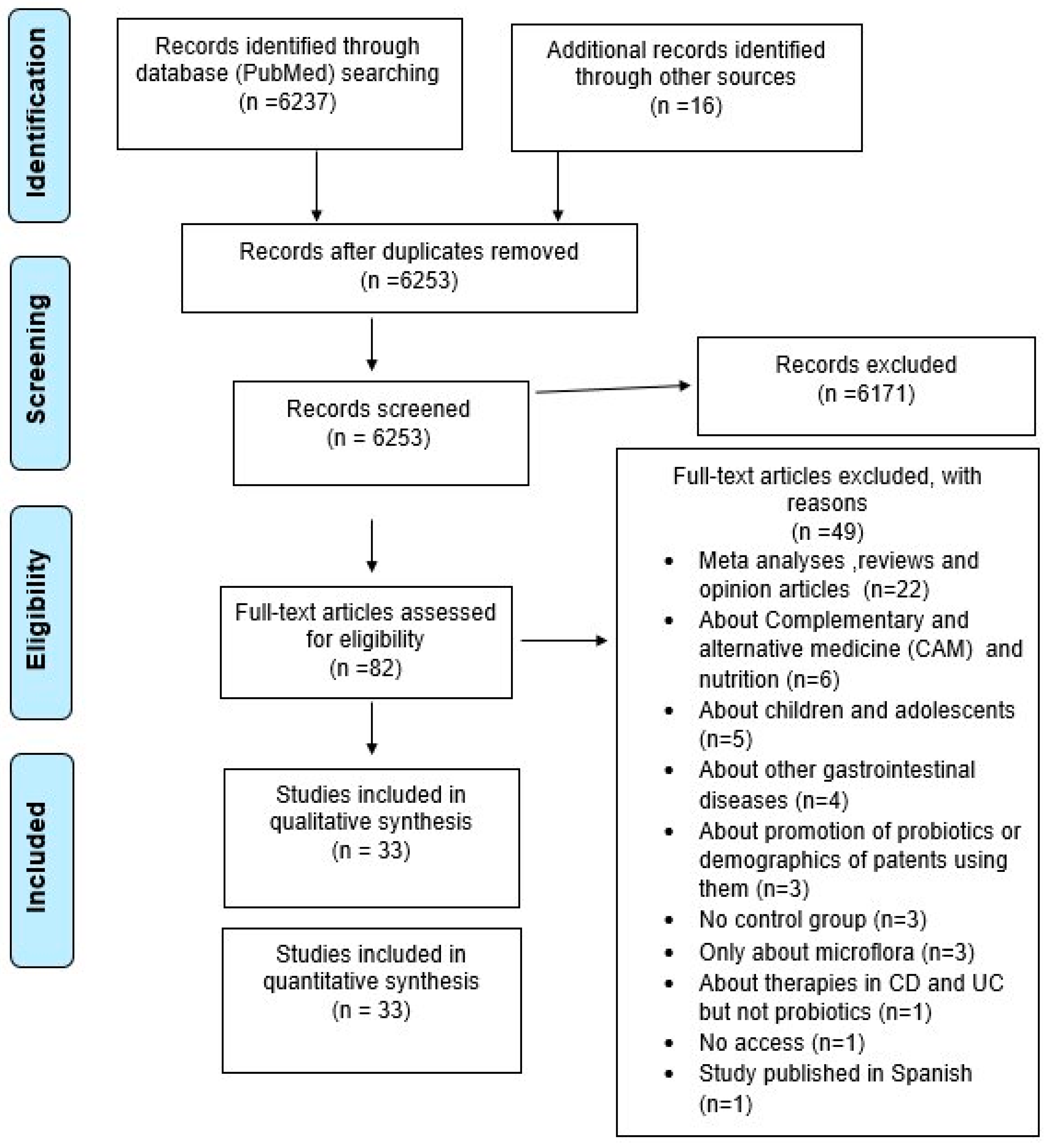
3.1. Search Results and Primary Outcomes
3.1.1. Role of Probiotics in UC
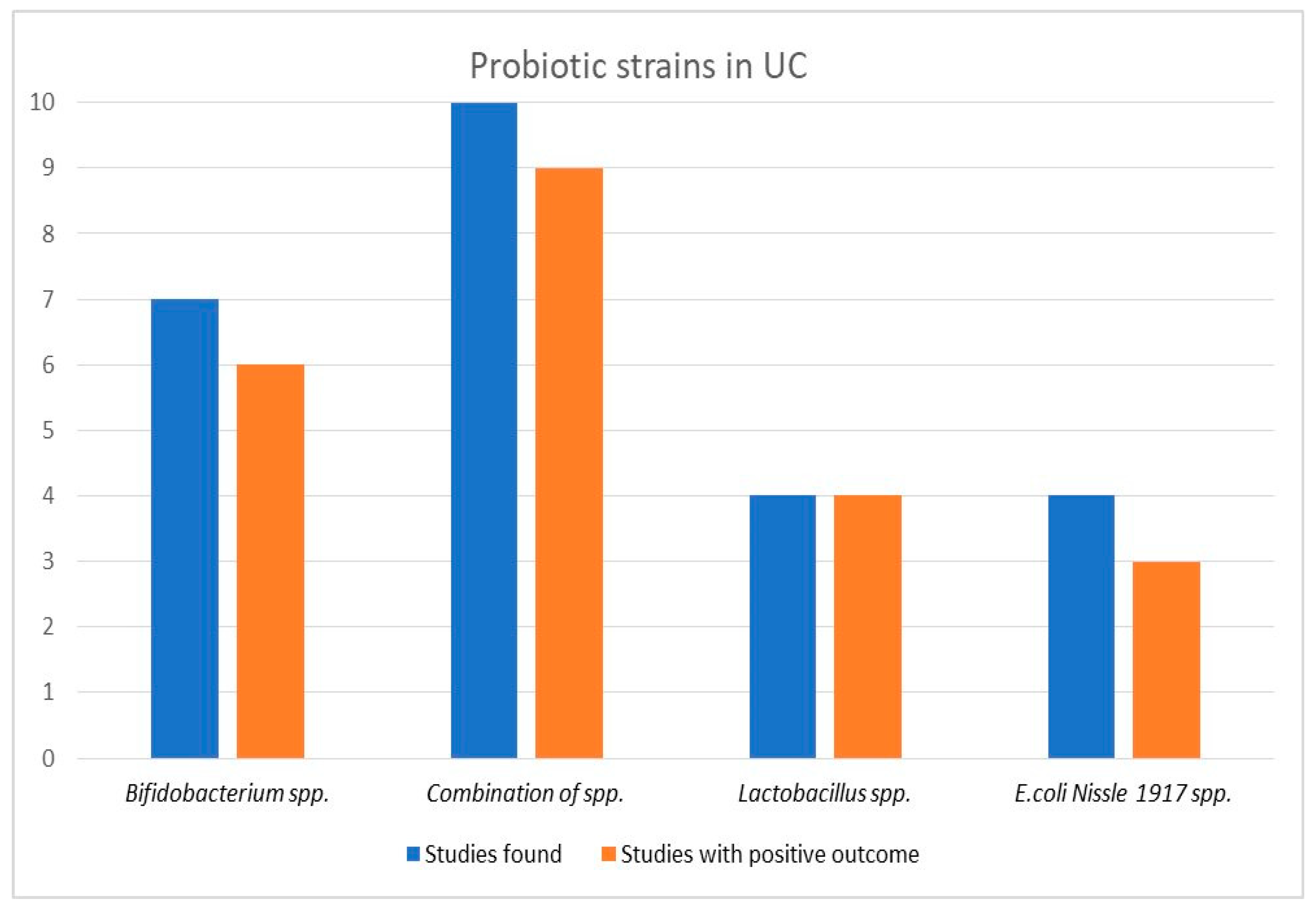
3.1.2. Efficacy of Probiotics Type in UC
3.1.3. Efficacy of Probiotics Concerning Treatment Duration
3.1.4. Efficacy of Probiotics in Comparison with the Control Group
3.1.5. Role of Probiotics in CD
3.1.6. Efficacy of Probiotics Type in CD
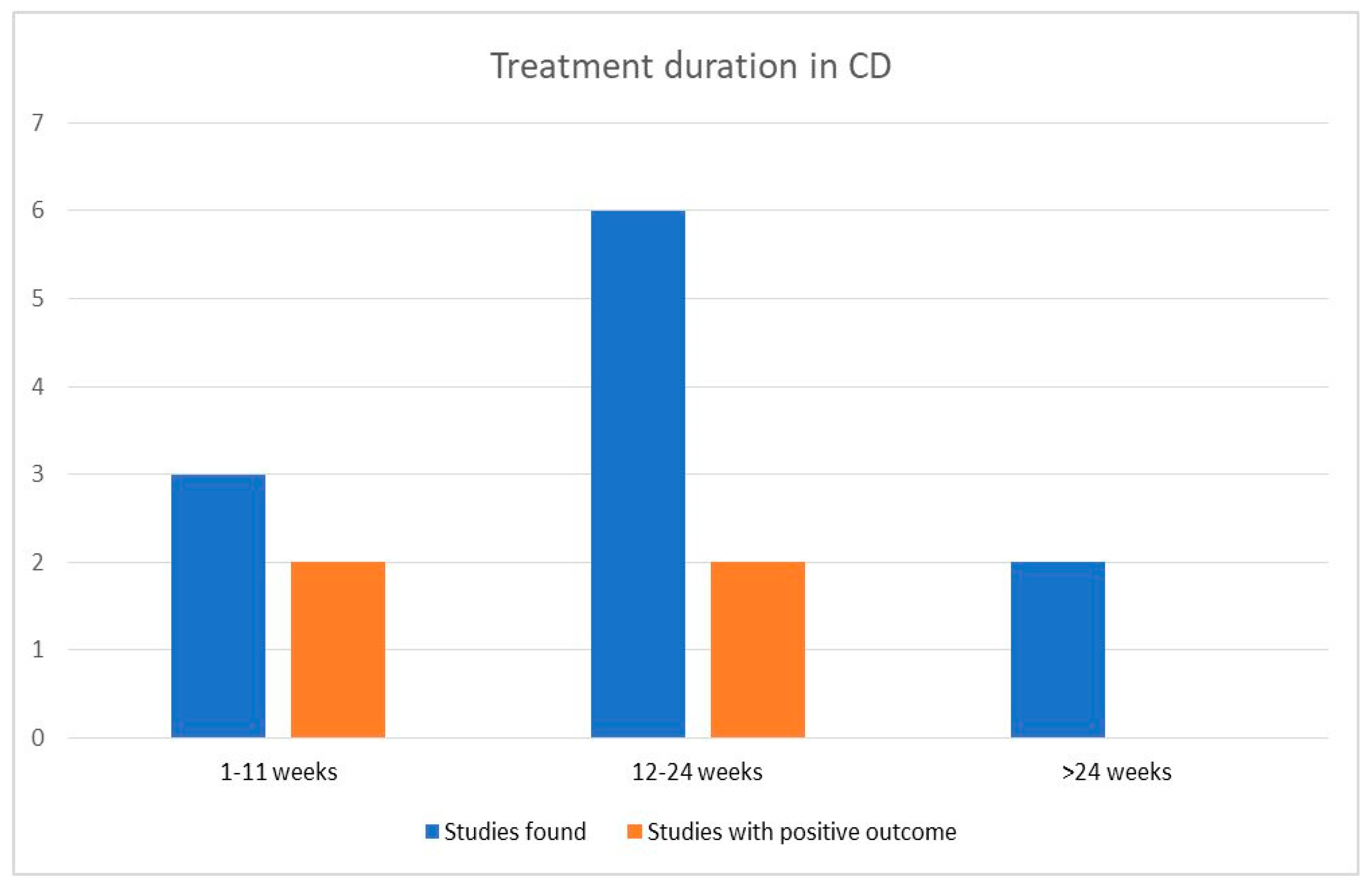
3.1.7. Efficacy of Probiotics Concerning Treatment Duration
3.1.8. Efficacy of Probiotics in Comparison with the Control Group
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jairath, V.; Feagan, B.G. Global burden of inflammatory bowel disease. Lancet Gastroenterol. Hepatol. 2020, 5, 2–3. [Google Scholar] [CrossRef] [PubMed]
- Kappelman, M.D.; Rifas–Shiman, S.L.; Kleinman, K.; Ollendorf, D.; Bousvaros, A.; Grand, R.J.; Finkelstein, J.A. The prevalence and geographic distribution of Crohn’s disease and ulcerative colitis in the United States. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2007, 5, 1424–1429. [Google Scholar] [CrossRef]
- Seyedian, S.S.; Nokhostin, F.; Malamir, M.D. A review of the diagnosis, prevention, and treatment methods of inflammatory bowel disease. J. Med. Life 2019, 12, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Mak, W.Y.; Zhao, M.; Nig, S.C.; Burisch, J. The epidemiology of inflammatory bowel disease: East meets west. J. Gastroenterol. Hepatol. 2020, 35, 380–389. [Google Scholar] [CrossRef] [PubMed]
- Abraham, C.; Cho, J.H. Inflammatory bowel disease. N. Engl. J. Med. 2009, 361, 2066–2078. [Google Scholar] [CrossRef]
- Kornbluth, A.; Sachar, D.B. Ulcerative colitis practice guidelines in adults: American College Of Gastroenterology, Practice Parameters Committee. Am. J. Gastroenterol. 2010, 105, 501–523, quiz 524. [Google Scholar] [CrossRef]
- Lichtenstein, G.R.; Hanauer, S.B.; Sandborn, W.J. Management of Crohn’s disease in adults. Am. J. Gastroenterol. 2009, 104, 465–483, quiz 464, 484. [Google Scholar] [CrossRef]
- Yoshimatsu, Y.; Yamada, A.; Furukawa, R.; Sono, K.; Osamura, A.; Nakamura, K.; Aoki, H.; Tsuda, Y.; Hosoe, N.; Takada, N.; et al. Effectiveness of probiotic therapy for the prevention of relapse in patients with inactive ulcerative colitis. World J. Gastroenterol. 2015, 21, 5985–5994. [Google Scholar] [CrossRef]
- Singh, P.; Rawat, A.; Alwakeel, M.; Sharif, E.; Al Khodor, S. The potential role of vitamin D supplementation as a gut microbiota modifier in healthy individuals. Sci. Rep. 2020, 10, 21641. [Google Scholar] [CrossRef]
- Cashman, K.D.; Dowling, K.G.; Cashman, K.D.; Škrabáková, Z.; Gonzalez-Gross, M.; Valtueña, J.; De Henauw, S.; Moreno, L.; Damsgaard, C.T.; Michaelsen, K.F.; et al. Vitamin D deficiency in Europe: Pandemic? Am. J. Clin. Nutr. 2016, 103, 1033–1044. [Google Scholar] [CrossRef] [Green Version]
- Akimbekov, N.S.; Digel, I.; Sherelkhan, D.K.; Lutfor, A.B.; Razzaque, M.S. Vitamin D and the Host-Gut Microbiome: A Brief Overview. Acta Histochem. Cytochem. 2020, 53, 33–42. [Google Scholar] [CrossRef]
- Manes, N.P.; Shulzhenko, N.; Nuccio, A.G.; Azeem, S.; Morgun, A.; Nita-Lazar, A. Multi-omics Comparative Analysis Reveals Multiple Layers of Host Signaling Pathway Regulation by the Gut Microbiota. mSystems 2017, 2, e00107-17. [Google Scholar] [CrossRef]
- Garg, M.; Hendy, P.; Ding, J.N.; Shaw, S.; Hold, G.; Hart, A. The Effect of Vitamin D on Intestinal Inflammation and Faecal Microbiota in Patients with Ulcerative Colitis. J. Crohn’s Colitis 2018, 12, 963–972. [Google Scholar] [CrossRef]
- Singh, P.; Kumar, M.; Al Khodor, S. Vitamin D deficiency in the gulf cooperation council: Exploring the triad of genetic predisposition, the gut microbiome and the immune system. Front. Immunol. 2019, 10, 1042. [Google Scholar] [CrossRef]
- Chatterjee, I.; Lu, R.; Zhang, Y.; Zhang, J.; Dai, Y.; Xia, Y.; Sun, J. Vitamin D receptor promotes healthy microbial metabolites and microbiome. Sci. Rep. 2020, 10, 7340. [Google Scholar] [CrossRef]
- Bellerba, F.; Muzio, V.; Gnagnarella, P.; Facciotti, F.; Chiocca, S.; Bossi, P.; Cortinovis, D.; Chiaradonna, F.; Serrano, D.; Raimondi, S.; et al. The Association between Vitamin D and Gut Microbiota: A Systematic Review of Human Studies. Nutrients 2021, 13, 3378. [Google Scholar] [CrossRef]
- Roager, H.M.; Licht, T.R.; Poulsen, S.K.; Larsen, T.M.; Bahl, M.I. Microbial enterotypes, inferred by the prevotella-to-bacteroides ratio, remained stable during a 6-month randomized controlled diet intervention with the new nordic diet. Appl. Environ. Microbiol. 2014, 80, 1142–1149. [Google Scholar] [CrossRef]
- Glassner, K.L.; Abraham, B.P.; Quigley, E.M.M. The microbiome and inflammatory bowel disease. J. Allergy Clin. Immunol. 2020, 145, 16–27. [Google Scholar] [CrossRef]
- Gálvez, J. Role of Th17 Cells in the Pathogenesis of Human IBD. ISRN Inflamm. 2014, 2014, 928461. [Google Scholar] [CrossRef]
- Shreiner, A.B.; Kao, J.Y.; Young, V.B. The gut microbiome in health and in disease. Curr. Opin. Gastroenterol. 2015, 31, 69–75. [Google Scholar] [CrossRef]
- Bezirtzoglou, E.; Stavropoulou, E.; Kantartzi, K.; Tsigalou, C.; Voidarou, C.; Mitropoulou, G.; Prapa, I.; Santarmaki, V.; Kompoura, V.; Amalia; et al. Maintaining Digestive Health in Diabetes: The Role of the Gut Microbiome and the Challenge of Functional Foods. Microorganisms 2021, 9, 516. [Google Scholar] [CrossRef] [PubMed]
- Papadopoulos, P.D.; Tsigalou, C.; Valsamaki, P.N.; Konstantinidis, T.G.; Voidarou, C.; Bezirtzoglou, E. The Emerging Role of the Gut Microbiome in Cardiovascular Disease: Current Knowledge and Perspectives. Biomedicines 2022, 10, 948. [Google Scholar] [CrossRef]
- Stavropoulou, E.; Kantartzi, K.; Tsigalou, C.; Konstantinidis, T.; Romanidou, G.; Voidarou, C.; Bezirtzoglou, E. Focus on the Gut-Kidney Axis in Health and Disease. Front. Med. (Lausanne) 2021, 7, 620102. [Google Scholar] [CrossRef] [PubMed]
- Monteleone, I.; Sarra, M.; Pallone, F.; Monteleone, G. Th17-related cytokines in inflammatory bowel diseases: Friends or foes? Curr. Mol. Med. 2012, 12, 592–597. [Google Scholar] [CrossRef]
- Gareau, M.G.; Sherman, P.M.; Walker, W.A. Probiotics and the gut microbiota in intestinal health and disease. Nat. Rev. Gastroenterol. Hepatol. 2010, 7, 503–514. [Google Scholar] [CrossRef] [PubMed]
- Carlsson, A.H.; Yakymenko, O.; Olivier, I.; Håkansson, F.; Postma, E.; Keita, Å.V.; Söderholm, J.D. Faecalibacterium prausnitzii supernatant improves intestinal barrier function in mice DSS colitis. Scand. J. Gastroenterol. 2013, 48, 1136–1144. [Google Scholar] [CrossRef] [PubMed]
- Fedorak, R.N.; Feagan, B.G.; Hotte, N.; Leddin, D.; Dieleman, L.A.; Petrunia, D.M.; Enns, R.; Bitton, A.; Chiba, N.; Paré, P.; et al. The probiotic VSL#3 has anti-inflammatory effects and could reduce endoscopic recurrence after surgery for Crohn’s disease. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2015, 13, 928–935.e2. [Google Scholar]
- Kato, K.; Mizuno, S.; Umesaki, Y.; Ishii, Y.; Sugitani, M.; Imaoka, A.; Otsuka, M.; Hasunuma, O.; Kurihara, R.; Iwasaki, A.; et al. Randomized placebo-controlled trial assessing the effect of bifidobacteria-fermented milk on active ulcerative colitis. Aliment. Pharmacol. Ther. 2004, 20, 1133–1141. [Google Scholar] [CrossRef]
- Kruis, W.; Schütz, E.; Fric, P.; Fixa, B.; Judmaier, G.; Stolte, M. Double-blind comparison of an oral Escherichia coli preparation and mesalazine in maintaining remission of ulcerative colitis. Aliment. Pharmacol. Ther. 1997, 11, 853–858. [Google Scholar] [CrossRef]
- Derwa, Y.; Gracie, D.J.; Hamlin, P.J.; Ford, A.C. Systematic review with meta-analysis: The efficacy of probiotics in inflammatory bowel disease. Aliment Pharm. 2017, 46, 389–400. [Google Scholar] [CrossRef]
- Kazemi, A.; Soltani, S.; Ghorabi, S.; Keshtkar, A.; Daneshzad, E.; Nasri, F.; Mazloomi, S.M. Effect of probiotic and synbiotic supplementation on inflammatory markers in health and disease status: A systematic review and meta-analysis of clinical trials. Clin. Nutr. (Edinb. Scotl.) 2020, 39, 789–819. [Google Scholar] [CrossRef] [PubMed]
- Fan, H.; Du, J.; Liu, X.; Zheng, W.-W.; Zhuang, Z.-H.; Wang, C.-D.; Gao, R. Effects of pentasa-combined probiotics on the microflora structure and prognosis of patients with inflammatory bowel disease. Turk. J. Gastroenterol. Off. J. Turk. Soc. Gastroenterol. 2019, 30, 680–685. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Lee, H.J. Research trend visualization By MeSH terms from Pub-Med. Int. J. Environ. Res. Public Health 2018, 15, 1113. [Google Scholar] [CrossRef] [PubMed]
- Falagas, M.E.; Pitsouni, E.I.; Malietzis, G.A.; Pappas, G. Comparison of PubMed, Scopus, web of science, and google scholar: Strengths and weaknesses. FASEB J. 2008, 22, 338–342. [Google Scholar] [CrossRef]
- Lu, Z. PubMed and beyond: A survey of web tools for searching biomedical literature. Database 2011, 2011, baq036. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ (Clin. Res. Ed.) 2008, 336, 924–926. [Google Scholar] [CrossRef]
- Bourreille, A.; Cadiot, G.; Le Dreau, G.; Laharie, D.; Beaugerie, L.; Dupas, J.L.; Marteau, P.; Rampal, P.; Moyse, D.; Saleh, A.; et al. Saccharomyces boulardii does not prevent relapse of Crohn’s disease. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2013, 11, 982–987. [Google Scholar] [CrossRef]
- Guslandi, M.; Mezzi, G.; Sorghi, M.; Testoni, P.A. Saccharomyces boulardii in maintenance treatment of Crohn’s disease. Dig. Dis. Sci. 2000, 45, 1462–1464. [Google Scholar] [CrossRef]
- Marteau, P.; Lémann, M.; Seksik, P.; Laharie, D.; Colombel, J.F.; Bouhnik, Y.; Cadiot, G.; Soulé, J.; Bourreille, A.; Metman, E. Ineffectiveness of Lactobacillus johnsonii LA1 for prophylaxis of postoperative recurrence in Crohn’s disease: A randomised, double blind, placebo controlled GETAID trial. Gut 2006, 55, 842–847. [Google Scholar] [CrossRef]
- Prantera, C.; Scribano, M.L.; Falasco, G.; Andreoli, A.; Luzi, C. Ineffectiveness of probiotics in preventing recurrence after curative resection for Crohn’s disease: A randomised controlled trial with Lactobacillus GG. Gut 2002, 51, 405–409. [Google Scholar] [CrossRef] [Green Version]
- Schultz, M.; Timmer, A.; Herfarth, H.H.; Sartor, R.B.; Vanderhoof, J.A.; Rath, H.C. Lactobacillus GG in inducing and maintaining remission of Crohn’s disease. BMC Gastroenterol. 2004, 4, 5. [Google Scholar] [CrossRef]
- Steed, H.; Macfarlane, G.T.; Blackett, K.L.; Bahrami, B.; Reynolds, N.; Walsh, S.V.; Cummings, J.H.; Macfarlane, S. Clinical trial: The microbiological and immunological effects of synbiotic consumption—A randomized double-blind placebo-controlled study in active Crohn’s disease. Aliment. Pharmacol. Ther. 2010, 32, 872–883. [Google Scholar] [CrossRef]
- Van Gossum, A.; Dewit, O.; Louis, E.; de Hertogh, G.; Baert, F.; Fontaine, F.; DeVos, M.; Enslen, M.; Paintin, M.; Franchimont, D. Multicenter randomized-controlled clinical trial of probiotics (Lactobacillus johnsonii, LA1) on early endoscopic recurrence of Crohn’s disease after lleo-caecal resection. Am. J. Physiol. Gastrointest. Liver Physiol. 2007, 13, 135–142. [Google Scholar]
- Cui, H.-H.; Chen, C.-L.; Wang, J.-D.; Yang, Y.-J.; Cun, Y.; Wu, J.-B.; Liu, Y.-H.; Dan, H.-L.; Jian, Y.-T.; Chen, X.-Q. Effects of probiotic on intestinal mucosa of patients with ulcerative colitis. World J. Gastroenterol. 2004, 10, 1521–1525. [Google Scholar] [CrossRef]
- D’Incà, R.; Barollo, M.; Scarpa, M.; Grillo, A.R.; Brun, P.; Vettorato, M.G.; Castagliuolo, I.; Sturniolo, G.C. Rectal administration of Lactobacillus casei DG modifies flora composition and Toll-like receptor expression in colonic mucosa of patients with mild ulcerative colitis. Dig. Dis. Sci. 2011, 56, 1178–1187. [Google Scholar] [CrossRef]
- Furrie, E.; Macfarlane, S.; Kennedy, A.; Cummings, J.H.; Walsh, S.V.; O’neil, D.A.; Macfarlane, G.T. Synbiotic therapy (Bifidobacterium longum/Synergy 1) initiates resolution of inflammation in patients with active ulcerative colitis: A randomised controlled pilot trial. Gut 2005, 54, 242–249. [Google Scholar] [CrossRef]
- Ishikawa, H.; Akedo, I.; Umesaki, Y.; Tanaka, R.; Imaoka, A.; Otani, T. Randomized controlled trial of the effect of bifidobacteria-fermented milk on ulcerative colitis. J. Am. Coll. Nutr. 2003, 22, 56–63. [Google Scholar] [CrossRef]
- Ishikawa, H.; Matsumoto, S.; Ohashi, Y.; Imaoka, A.; Setoyama, H.; Umesaki, Y.; Tanaka, R.; Otani, T. Beneficial effects of probiotic bifidobacterium and galacto-oligosaccharide in patients with ulcerative colitis: A randomized controlled study. Digestion 2011, 84, 128–133. [Google Scholar] [CrossRef]
- Huang, M.; Chen, Z.; Lang, C.; Chen, J.; Yang, B.; Xue, L.; Zhang, Y. Efficacy of mesalazine in combination with bifid triple viable capsules on ulcerative colitis and the resultant effect on the inflammatory factors. Pak. J. Pharm. Sci. 2018, 31, 2891–2895. [Google Scholar]
- Kamarlı, A.H.; Yıldız, E.A.; Akın, M. Effects of synbiotic therapy in mild-to-moderately active ulcerative colitis: A randomized placebo-controlled study. Turk. J. Gastroenterol. Off. J. Turk. Soc. Gastroenterol. 2019, 30, 313–320. [Google Scholar] [CrossRef]
- Li, S.; Yin, Y.; Xiao, D.; Zou, Y. Supplemental bifid triple viable capsule treatment improves inflammatory response and T cell frequency in ulcerative colitis patients. BMC Gastroenterol. 2021, 21, 314. [Google Scholar] [CrossRef]
- Matsuoka, K.; Uemura, Y.; Kanai, T.; Kunisaki, R.; Suzuki, Y.; Yokoyama, K.; Yoshimura, N.; Hibi, T. Efficacy of Bifidobacterium breve Fermented Milk in Maintaining Remission of Ulcerative Colitis. Dig. Dis. Sci. 2018, 63, 1910–1919. [Google Scholar] [CrossRef] [Green Version]
- Matthes, H.; Krummenerl, T.; Giensch, M.; Wolff, C.; Schulze, J. Clinical trial: Probiotic treatment of acute distal ulcerative colitis with rectally administered Escherichia coli Nissle 1917 (EcN). BMC Complement. Altern. Med. 2010, 10, 13. [Google Scholar] [CrossRef]
- Ng, S.C.; Plamondon, S.; Kamm, M.A.; Hart, A.L.; Al-Hassi, H.O.; Guenther, T.; Stagg, A.J.; Knight, S.C. Immunosuppressive effects via human intestinal dendritic cells of probiotic bacteria and steroids in the treatment of acute ulcerative colitis. Inflamm. Bowel Dis. 2010, 16, 1286–1298. [Google Scholar] [CrossRef]
- Palumbo, V.D.; Romeo, M.; Marino Gammazza, A.; Carini, F.; Damiani, P.; Damiano, G.; Buscemi, S.; Monte, A.I.L.; Gerges-Geageac, A.; Jurjus, A.; et al. The long-term effects of probiotics in the therapy of ulcerative colitis: A clinical study. Biomed. Pap. Med. Fac. Univ. Palacky Olomouc Czechoslov. 2016, 160, 372–377. [Google Scholar] [CrossRef]
- Petersen, A.M.; Mirsepasi, H.; Halkjær, S.I.; Mortensen, E.M.; Nordgaard-Lassen, I.; Krogfelt, K.A. Ciprofloxacin and probiotic Escherichia coli Nissle add-on treatment in active ulcerative colitis: A double-blind randomized placebo controlled clinical trial. J. Crohn’s Colitis 2014, 8, 1498–1505. [Google Scholar] [CrossRef]
- Rembacken, B.J.; Snelling, A.M.; Hawkey, P.M.; Chalmers, D.M.; Axon, A.T. Non-pathogenic Escherichia coli versus mesalazine for the treatment of ulcerative colitis: A randomised trial. Lancet 1999, 354, 635–639. [Google Scholar] [CrossRef]
- Sood, A.; Midha, V.; Makharia, G.K.; Ahuja, V.; Singal, D.; Goswami, P.; Tandon, R.K. The probiotic preparation, VSL#3 induces remission in patients with mild-to-moderately active ulcerative colitis. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2009, 7, 1202–1209.e1. [Google Scholar]
- Tamaki, H.; Nakase, H.; Inoue, S.; Kawanami, C.; Itani, T.; Ohana, M.; Kusaka, T.; Uose, S.; Hisatsune, H.; Tojo, M.; et al. Efficacy of probiotic treatment with Bifidobacterium longum 536 for induction of remission in active ulcerative colitis: A randomized, double-blinded, placebo-controlled multicenter trial. Dig. Endosc. Off. J. Jpn. Gastroenterol. Endosc. Soc. 2016, 28, 67–74. [Google Scholar] [CrossRef]
- Tursi, A.; Brandimarte, G.; Papa, A.; Giglio, A.; Elisei, W.; Giorgetti, G.M.; Forti, G.; Morini, S.; Hassan, C.; Antonietta, M. Pistoia Treatment of relapsing mild-to-moderate ulcerative colitis with the probiotic VSL#3 as adjunctive to a standard pharmaceutical treatment: A double-blind, randomized, placebo-controlled study. Am. J. Gastroenterol. 2010, 105, 2218–2227. [Google Scholar]
- Wildt, S.; Nordgaard, I.; Hansen, U.; Brockmann, E.; Rumessen, J.J. A randomised double-blind placebo-controlled trial with Lactobacillus acidophilus La-5 and Bifidobacterium animalis subsp. lactis BB-12 for maintenance of remission in ulcerative colitis. J. Crohn’s Colitis 2011, 5, 115–121. [Google Scholar] [CrossRef]
- Yılmaz, İ.; Dolar, M.E.; Özpınar, H. Effect of administering kefir on the changes in fecal microbiota and symptoms of inflammatory bowel disease: A randomized controlled trial. Turk. J. Gastroenterol. Off. J. Turk. Soc. Gastroenterol. 2019, 30, 242–253. [Google Scholar] [CrossRef]
- LaPointe, G.; Rogers, M.A. Microorganisms Special Issue “How Do Food and Probiotics Influence the Composition and Activity of the Gut Microbiota?”. Microorganisms 2022, 22, 2097. [Google Scholar] [CrossRef]
- Zocco, M.A.; dal Verme, L.Z.; Cremonini, F.; Piscaglia, A.C.; Nista, E.C.; Candelli, M.; Novi, M.; Rigante, D.; Cazzato, I.A.; Ojetti, V.; et al. Efficacy of Lactobacillus GG in maintaining remission of ulcerative colitis. J. Appl. Microbiol. 2006, 23, 1567–1574. [Google Scholar] [CrossRef]
- McInnes, I.B.; Porter, B.; Das Gupta, A.; Pricop, L.; Fox, T.; Bjarnason, I. A randomised, double-blind, placebo-controlled trial of a multi-strain probiotic in patients with asymptomatic ulcerative colitis and Crohn’s disease. Ann. Rheum. Dis. 2019, 27, 465–473. [Google Scholar]
- Martini, E.; Krug, S.; Siegmund, B.; Neurath, M.F.; Becker, C. Mend Your Fences: The Epithelial Barrier and its Relationship with Mucosal Immunity in Inflammatory Bowel Disease. Cell Mol. Gastroenterol Hepatol. 2017, 4, 33–46. [Google Scholar] [CrossRef]
- Generoso, S.V.; Viana, M.L.; Santos, R.G.; Arantes, R.M.; Martins, F.S.; Nicoli, J.R.; Machado, J.A.; Correia, M.I.; Cardoso, V.N. Protection against increased intestinal permeability and bacterial translocation induced by intestinal obstruction in mice treated with viable and heat-killed Saccharomyces boulardii. Eur. J. Nutr. 2011, 50, 261–269. [Google Scholar] [CrossRef]
- Coqueiro, A.Y.; Raizel, R.; Bonvini, A.; Tirapegui, J.; Rogero, M.M. Probiotics for inflammatory bowel diseases: A promising adjuvant treatment. Int. J. Food Sci. Nutr. 2019, 70, 20–29. [Google Scholar] [CrossRef]
- Pavel, F.M.; Vesa, C.M.; Gheorghe, G.; Diaconu, C.C.; Stoicescu, M.; Munteanu, M.A.; Babes, E.E.; Tit, D.M.; Toma, M.M.; Bungau, S. Highlighting the Relevance of Gut Microbiota Manipulation in Inflammatory Bowel Disease. Diagnostics 2021, 11, 1090. [Google Scholar] [CrossRef]
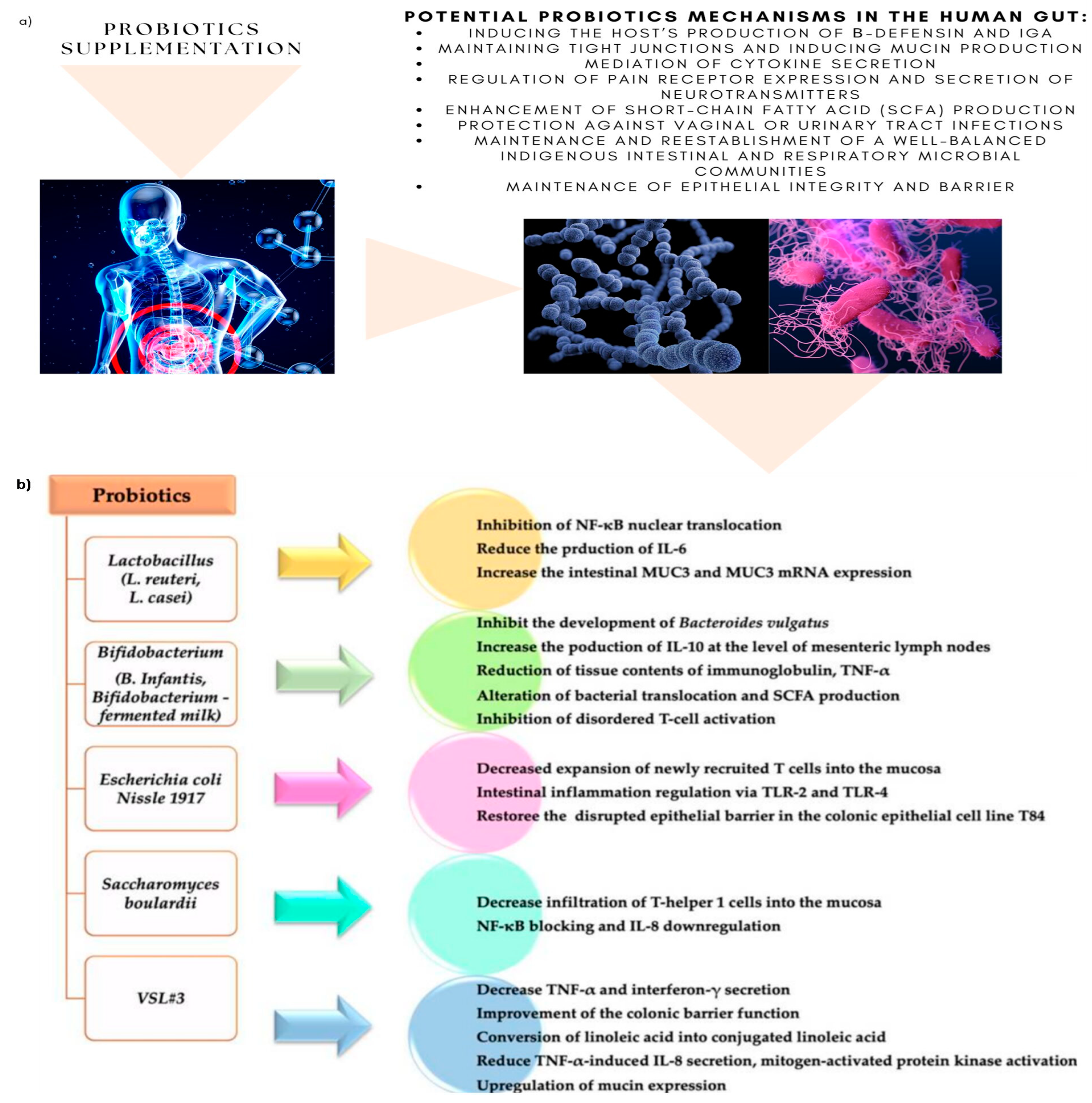
- Hemarajata, P.; Versalovic, J. Effects of probiotics on gut microbiota: Mechanisms of intestinal immunomodulation and neuromodulation. Ther. Adv. Gastroenterol. 2013, 6, 39–51. [Google Scholar] [CrossRef]
- Stefanis, C.; Mantzourani, I.; Plessas, S.; Alexopoulos, A.; Galanis, A.; Bezirtzoglou, E.; Kandylis, P.; Varzakas, T. Reviewing Classical and Molecular Techniques Regarding Profiling of Probiotic Character of Microorganisms. Curr. Res. Nutr. Food Sci. 2016, 4, 27–47. [Google Scholar] [CrossRef]
- Plaza-Díaz, J.; Ruiz-Ojeda, F.J.; Vilchez-Padial, L.M.; Gil, A. Evidence of the Anti-Inflammatory Effects of Probiotics and Synbiotics in Intestinal Chronic Diseases. Nutrients 2017, 9, 555. [Google Scholar] [CrossRef]
- Dahiya, D.; Nigam, P.S. The Gut Microbiota Influenced by the Intake of Probiotics and Functional Foods with Prebiotics Can Sustain Wellnes and Alleviate Certain Ailments like Gut-Inflammation and Colon-Cancer. Microorganisms 2022, 20, 665. [Google Scholar] [CrossRef]
- Banerjee, P.; Choudhury, S.; Jalan, K.; Das, A.; Ghosh, N.; Bagchi, D. Beneficial role of gut microbiome in metabolic syndrome, obesity, and cardiovascular diseases. In Microbiome, Immunity, Digestive Health and Nutrition: Epidemiology, Pathophysiology, Prevention and Treatment; Academic Press: Cambridge, MA, USA, 2022; pp. 149–166. [Google Scholar] [CrossRef]
- Cuervo, A.; Valdés, L.; Salazar, N.; De Los Reyes-Gavilán, C.G.; Ruas-Madiedo, P.; Gueimonde, M.; González, S. Pilot study of diet and microbiota: Interactive associations of fibers and polyphenols with human intestinal bacteria. J. Agric. Food Chem. 2014, 62, 5330–5336. [Google Scholar] [CrossRef]
- Manach, C.; Scalbert, A.; Morand, C.; Rémésy, C.; Jiménez, L. Polyphenols: Food sources and bioavailability. Am. J. Clin. Nutr. 2004, 79, 727–747. [Google Scholar] [CrossRef]
- Régnier, M.; van Hul, M.; Knauf, C.; Cani, P.D. Gut microbiome, endocrine control of gut barrier function and metabolic diseases. J. Endocrinol. 2021, 248, R67–R82. [Google Scholar] [CrossRef]
- Anhê, F.F.; Choi, B.S.Y.; Dyck, J.R.B.; Schertzer, J.D.; Marette, A. Host–Microbe Interplay in the Cardiometabolic Benefits of Dietary Polyphenols. Trends Endocrinol. Metab. 2019, 30, 384–395. [Google Scholar] [CrossRef]
- Malinowsk, B.; Wiciński, M.; Sokołowska, M.M.; Hill, N.A.; Szambelan, M. The rundown of dietary supplements and their effects on inflammatory bowel disease—A review. Nutrients 2020, 12, 1423. [Google Scholar] [CrossRef]
- Pesce, M.; Seguella, L.; Del Re, A.; Lu, J.; Palenca, I.; Corpetti, C.; Rurgo, S.; Sanseverino, W.; Sarnelli, G.; Esposito, G. Next-Generation Probiotics for Inflammatory Bowel Disease. Int. J. Mol. Sci. 2022, 23, 5466. [Google Scholar] [CrossRef]
- Behl, T.; Bungau, S.; Kumar, K.; Zengin, G.; Khan, F.; Kumar, A.; Kaur, R.; Venkatachalam, T.; Tit, D.M.; Vesa, S.M.; et al. Pleotropic effects of polyphenols in cardiovascular system. Biomed. Pharmacother. 2020, 130, 110714. [Google Scholar] [CrossRef] [PubMed]
- Araújo, J.R.; Tomas, J.; Brenner, C.; Sansonetti, P.J. Impact of high-fat diet on the intestinal microbiota and small intestinal physiology before and after the onset of obesity. Biochimie 2017, 141, 97–106. [Google Scholar] [CrossRef] [PubMed]
- Bernardi, S.; Del Bo’, C.; Marino, M.; Gargari, G.; Cherubini, A.; Andrés-Lacueva, C.; Hidalgo-Liberona, N.; Peron, G.; González-Dominguez, R.; Kroon, P.; et al. Polyphenols and Intestinal Permeability: Rationale and Future Perspectives. J. Agric. Food Chem. 2020, 68, 1816–1829. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Feng, Y.; Liu, W. Efficacy and safety of probiotics in the induction and maintenance of inflammatory bowel disease remission: A systematic review and meta-analysis. Ann. Palliat. Med. 2021, 10, 11821–11829. [Google Scholar] [CrossRef]
- Zhang, X.F.; Guan, X.X. Clinical effects and gut microbiota changes of using probiotics, prebiotics or synbiotics in inflammatory bowel disease: A systematic review and meta-analysis. Eur. J. Nutr. 2021, 60, 2855–2875. [Google Scholar] [CrossRef]
- Sepehri, S.; Kotlowski, R.; Bernstein, C.N.; Krause, D.O. Microbial diversity of inflamed and noninflamed gut biopsy tissues in inflammatory bowel disease. Inflamm. Bowel Dis. 2007, 1, 675–683. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ref. | Were the Research Question and Primary Outcomes Clearly Stated? | Was the Sample Number >100? | Were the Characteristics of Sample Well Stated without Major Differences between Test and Control Groups? | Was the Treatment Method about Probiotics Clearly Stated? (Type, Duration, Dose, Other Treatments) | Was the Patient’s Status of Disease Clearly Stated before Intervention? (Active Disease, Diagnosis Criteria) | Quality Assessment |
|---|---|---|---|---|---|---|
| [35] | + | + | + | + | + | High |
| [27] | + | + | + | + | + | High |
| [36] | + | - | + | + | + | High |
| [37] | + | - | + | + | + | High |
| [38] | + | - | + | + | + | High |
| [39] | + | - | + | + | + | High |
| [40] | + | - | + | + | + | High |
| [41] | + | - | + | + | + | High |
| [42] | + | - | - | - | - | Low |
| [43] | + | - | - | + | + | Moderate |
| [44] | + | - | + | + | + | High |
| [45] | + | - | + | + | + | High |
| [46] | + | - | + | + | + | High |
| [47] | + | + | + | + | + | High |
| [48] | + | - | + | + | + | High |
| [28] | + | - | + | + | + | High |
| [29] | + | + | + | + | + | High |
| [49] | + | - | + | - | + | Moderate |
| [50] | + | + | + | + | + | High |
| [51] | + | - | + | + | + | High |
| [52] | + | - | + | + | + | High |
| [53] | + | - | + | + | + | High |
| [54] | + | + | + | + | + | High |
| [55] | + | + | + | + | + | High |
| [56] | + | + | + | + | + | High |
| [57] | + | - | + | + | + | High |
| [58] | + | + | + | + | + | High |
| [59] | + | - | + | + | + | High |
| [8] | + | - | + | + | + | High |
| [60] | + | + | + | + | + | High |
| [17] | + | - | + | + | + | High |
| [61] | + | + | + | + | + | High |
| [62] | + | - | - | + | + | Moderate |
| Ref. | Year | Country | Sample Size | Duration Weeks | Type of Disease |
|---|---|---|---|---|---|
| [35] | 2013 | France | 165 | 52 | Crohn’s disease |
| [63] | 2015 | Canada | 119 | 13 | |
| [36] | 2000 | Italy | 32 | 26 | |
| [37] | 2005 | France | 98 | 26 | |
| [38] | 2001 | Portugal | 45 | 52 | |
| [39] | 2004 | Germany | 11 | 26 | |
| [40] | 2010 | UK | 35 | 26 | |
| [41] | 2007 | Belgium | 70 | 12 | |
| [42] | 2004 | China | 30 | 8 | Ulcerative colitis |
| [43] | 2010 | Italy | 26 | 8 | |
| [44] | 2015 | UK | 18 | 4 | |
| [45] | 2003 | Japan | 21 | 52 | |
| [46] | 2010 | Japan | 41 | 52 | |
| [47] | 2018 | China | 360 | 8 | |
| [48] | 2018 | Turkey | 40 | 8 | |
| [64] | 2004 | Japan | 20 | 12 | |
| [29] | 1997 | Germany, Czechia, and Austria | 120 | 12 | |
| [49] | 2012 | China | 82 | 4 | |
| [50] | 2008 | Japan | 192 | 48 | |
| [51] | 2010 | Germany | 90 | 2 | |
| [52] | 2010 | UK | 28 | 8 | |
| [53] | 2016 | Italy | 60 | 104 | |
| [54] | 2014 | Denmark | 50 | 7 | |
| [55] | 1999 | UK | 120 | 52 | |
| [56] | 2009 | India | 147 | 6 | |
| [57] | 2015 | Japan | 56 | 8 | |
| [58] | 2010 | Italy | 144 | 8 | |
| [59] | 2011 | Denmark | 32 | 52 | |
| [8] | 2015 | Japan | 46 | 52 | |
| [60] | 2006 | Italy | 187 | 26 and 52 | |
| [32] | 2019 | China | 40 | 5 | Both diseases |
| [61] | 2019 | UK | 143 | 4 | |
| [62] | 2018 | Turkey | 45 | 4 |
| Author | Disease Severity | Groups | Type of Probiotics | Species Used | Main Clinical Outcome |
|---|---|---|---|---|---|
| Cui H. [45] | I | P | Bifidobacterium spp. | Bifid Triple Viable Capsules | IL-1, TNF-α, and IL-10 had higher decrease in test group |
| D’Inca R. [46] | MA | No | LGC | Lactobacillus casei DG | Both orally and rectally given probiotics have shown SS improvement in clinical and histological scores |
| Furrie E. [47] | A | P | Bifidobacterium spp. | Bifidobacterium longum | Sigmoidoscopy scores (SS) and blood-serological markers (TNF-a) and (IL-1a)were reduced. Both clinical activity index (CAI) and bowel habit index (BHI) were reduced in test group |
| Hideki Ishikawa [48] | MMA | P | Combination of species | Bifidobacterium breve, Bifidobacterium bifidum, Lactobacillus acidophillus YIT 0168 | Exacerbation of symptoms were seen in fewer patients in test group than control. No difference was seen in the colonoscopy findings |
| Hideki Ishikawa [49] | A/I | P | Bifidobacterium spp. | Bifidobacterium breve | Endoscopic score of the treatment group was significantly lower. Myeloperoxidase analysis (MPO) amounts in the lavage solution (LS) significantly decreased |
| Huang M. [50] | A | P | Bifidobacterium spp. | Bifid Triple Viable Capsules | Higher decrease in UCDAI score and symptoms in test group. TNF-α and IL-8 were decreased in test group |
| Kamarli H. [51] | MMA | P | Combination of species | Enterococcus faecium, Lactobacillus plantarum, Streptococcus thermophilus, Bifidobacterium lactis, Lactobacillus acidophilus, Bifidobacterium longum | SS differences in decrease of endoscopic and clinical index score. Test group achieved higher decrease |
| Kato K. [28] | MMA | P | Combination of species | Bifidobacterium breve, Bifidobacterium bifidum, Lactobacillus acidophillus YIT 0168 | CAI score, endoscopic score, and histological score were significantly lower in treatment group |
| Kruis W. [29] | I | M | E.coli Nissle 1917 | E.coli Nissle 1917 (Serotype O6: K5: H1) | No significant differences both in CAI scores and relapse rate. Relapse free time differences were also NS |
| Li S. [52] | A | No | Bifidobacterium spp. | Bifid Triple Viable Capsules | NS differences in decrease of clinical symptoms and blood-serological markers between groups. Both groups had decreased inflammation markers and symptoms |
| Matsuoka K. [53] | I | P | Combination of species | Bifidobacterium breve,
Bifidobacterium bifidum, Lactobacillus acidophillus YIT 0168 | NS differences in both relapse-free survival and clinical deterioration |
| Matthes H. [54] | MMA | P | E.coli Nissle 1917 | E.coli Nissle 1917 (Serotype O6: K5: H1) | Dose depended efficacy in both remission time and endoscopic findings |
| Ng S. [55] | MMA | P | Combination of species | L. paracasei, L. plantarum, L. acidophilus, L. delbrueckii subsp bulgaricus, B. longum, B. breve, B. infantis, Streptococcus thermophilus | More patients achieved remission in test group |
| Palumbo V. [56] | MS | M | Combination of species | Lactobacillus salivarius, Lactobacillus acidophilus, Bifidobacterium bifidus strain BGN4 | Better improvement compared to control |
| Petersen A. [57] | MMA | P | E.coli Nissle 1917 | E.coli Nissle 1917 (Serotype O6: K5: H1) | Group receiving probiotics had fewer patients achieving remission and higher numbers in withdrawals |
| Rembacken B.J. [58] | A | M | E.coli Nissle 1917 | E.coli Nissle 1917 (Serotype O6: K5: H1) | Equal effect of mesalazine and EcN in attaining remission, time, and duration of remission |
| Sood A. [59] | MMA | P | Combination of species | L. paracasei, L. plantarum, L. acidophilus, L. delbrueckii subsp bulgaricus, B. longum, B. breve, B. infantis, Streptococcus thermophilus | Individual UCDAI score decrease was higher in test group. More patients achieved remission and mean decrease rate was higher in test group |
| Tamaki H. [60] | MMA | P | Bifidobacterium spp. | Bifidobacterium longum BB536 | Significant decrease of UCDAI scores and endoscopic index in test group |
| Tursi A. [61] | MMA | P | Combination of species | L. paracasei, L. plantarum,
L. acidophilus, L. delbrueckiisubspbulgaricus, B. longum, B. breve, B. infantis, Streptococcus thermophilus | In test group more patients achieved remission, had decreased UCDAI score, in endoscopic scores and symptoms |
| Wildt S. [62] | I | P | Combination of species | L. acidophilus strain LA-5 and B. animalis subsp. lactis strain BB-12 | More patients in test group achieved remission. Median relapse time was longer in test group |
| Yoshimatsu Y. [8] | A/I | P | Combination of species | Streptococcus faecalis (T-110), Clostridium butyricum (TO-A), Bacillus mesentericus (TO-A) | Remission rate was higher in test group and relapse was presented more often in control group |
| Zocco A. [65] | I | M | LGC | Lactobacillus GG | No difference in relapse rate between groups. Differences between groups were NS |
| Fan H. [32] | MMA | No | Bifidobacterium spp. | Bifid Triple Viable Capsules | Observation group had significantly lower scores in CDAI and UCAI as well as recurrence rate |
| McInnes I. [66] | I | P | LGC | Lactobacillus rhamnosus NCIMB 30174, Lactobacillus plantarum NCIMB 30173, Lactobacillus acidophilus NCIMB 30175 and Enterococcus faecium NCIMB 30176 | Reduced fecal calprotectin (FCAL) in UC patients. No differences in IBD-QOL scores and blood-serological markers |
| Yilmaz Il. [63] | A/I | No | LGC | Lactobacillus spp. | Significant decrease in ESR and CRP in test group. Bloating scores significantly reduced and feeling good scores increased |
| First Author’s Name | Disease Severity before Intervention | Control | Type of Probiotics | Species Used | Main Clinical Outcome |
|---|---|---|---|---|---|
| Bourreille A. [38] | I | P | Saccharomyces | Saccharomyces boulardii | Median time of relapse and achievement of remission differences were NS. Differences in decrease of CDAI were also NS |
| Fedorak R. [27] | I | P | Combination of species | L. paracasei,L. plantarum, L. acidophilus, L. delbrueckiisubspbulgaricus, B. longu, B. breve, B. infantis, Streptococcus thermophilus | Recurrence rates and CDAI and IBQD were similar in both groups |
| Guslandi M. [39] | I | No | Saccharomyces | Saccharomyces boulardii | Fewer patients had relapse episodes in test group (SS results) |
| Marteau P. [40] | I | No | LGC | Lactobacillus johnsonii LA1 | NS differences in recurrence rates and endoscopic score |
| Prantera C. [41] | I | P | LGC | Lactobacillus casei subspecies rhamnosus | Clinical recurrence was ascertained in more patients in test group. Endoscopic score was better in control group |
| Schultz M. [42] | MMA | P | LGC | Lactobacillus GG | NS differences in recurrence rates and relapse time |
| Steed H. [43] | MMA | P | Bifidobacterium spp. | Bifidobacterium longum | Symbiotic group had improvement in CDAI scores and histological score |
| Van Gossum A. [44] | A | P | LGC | Lactobacillus johnsonii LA1 | Mean endoscopic score, relapse rate, and mean histological score differences were NS for two groups |
| Fan H. [32] | MMA | No | Bifidobacterium spp. | Bifid Triple Viable Capsules | Observation group had significantly lower scores in CDAI and UCAI as well as recurrence rate |
| McInnes I. [66] | I | P | LGC | Lactobacillus rhamnosus NCIMB 30174, Lactobacillus plantarum NCIMB 30173, Lactobacillus acidophilus NCIMB 30175 and Enterococcus faecium NCIMB 30176 | Reduced fecal calprotectin (FCAL) differences in CD patients were NS. No differences in IBD-QOL scores and blood-serological markers |
| Yilmaz Il. [63] | A/I | No | LGC | Lactobacillus spp. | Significant decrease in ESR and CRP in test group. Bloating scores significantly reduced and feeling good scores increased |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vakadaris, G.; Stefanis, C.; Giorgi, E.; Brouvalis, M.; Voidarou, C.; Kourkoutas, Y.; Tsigalou, C.; Bezirtzoglou, E. The Role of Probiotics in Inducing and Maintaining Remission in Crohn’s Disease and Ulcerative Colitis: A Systematic Review of the Literature. Biomedicines 2023, 11, 494. https://doi.org/10.3390/biomedicines11020494
Vakadaris G, Stefanis C, Giorgi E, Brouvalis M, Voidarou C, Kourkoutas Y, Tsigalou C, Bezirtzoglou E. The Role of Probiotics in Inducing and Maintaining Remission in Crohn’s Disease and Ulcerative Colitis: A Systematic Review of the Literature. Biomedicines. 2023; 11(2):494. https://doi.org/10.3390/biomedicines11020494
Chicago/Turabian StyleVakadaris, Georgios, Christos Stefanis, Elpida Giorgi, Merkourios Brouvalis, Chrysoula (Chrysa) Voidarou, Yiannis Kourkoutas, Christina Tsigalou, and Eugenia Bezirtzoglou. 2023. "The Role of Probiotics in Inducing and Maintaining Remission in Crohn’s Disease and Ulcerative Colitis: A Systematic Review of the Literature" Biomedicines 11, no. 2: 494. https://doi.org/10.3390/biomedicines11020494