
Neurosurgical Anesthesia: Optimizing Outcomes with Agent Selection
 , ,
, ,
Abstract
:1. Development and Adoption of Anesthesia in Neurosurgery
2. Physiological Effects of Anesthesia during Neurosurgery
3. Overview of Classes of Neuroanesthesia
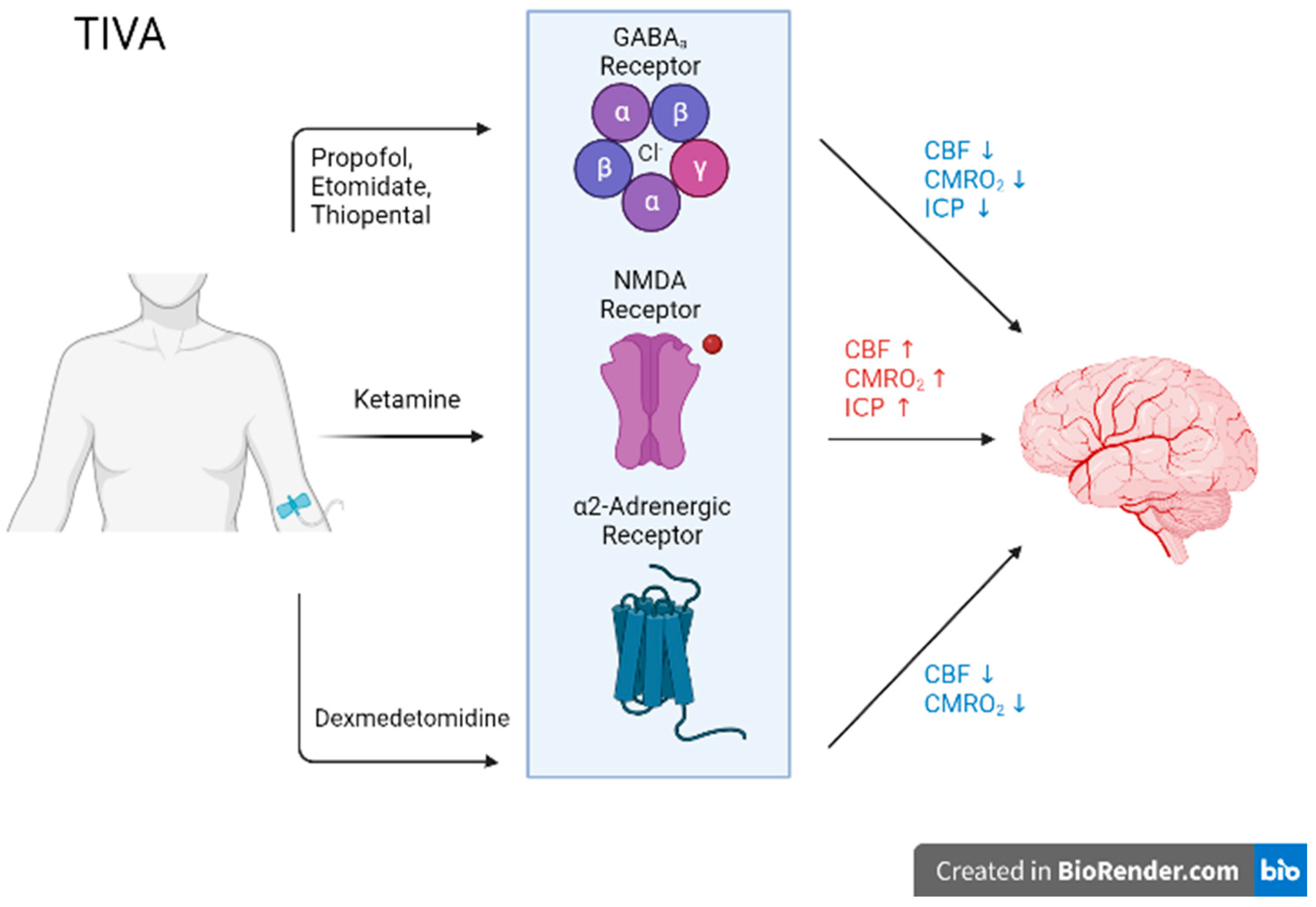
3.1. Total Intravenous Anesthetics
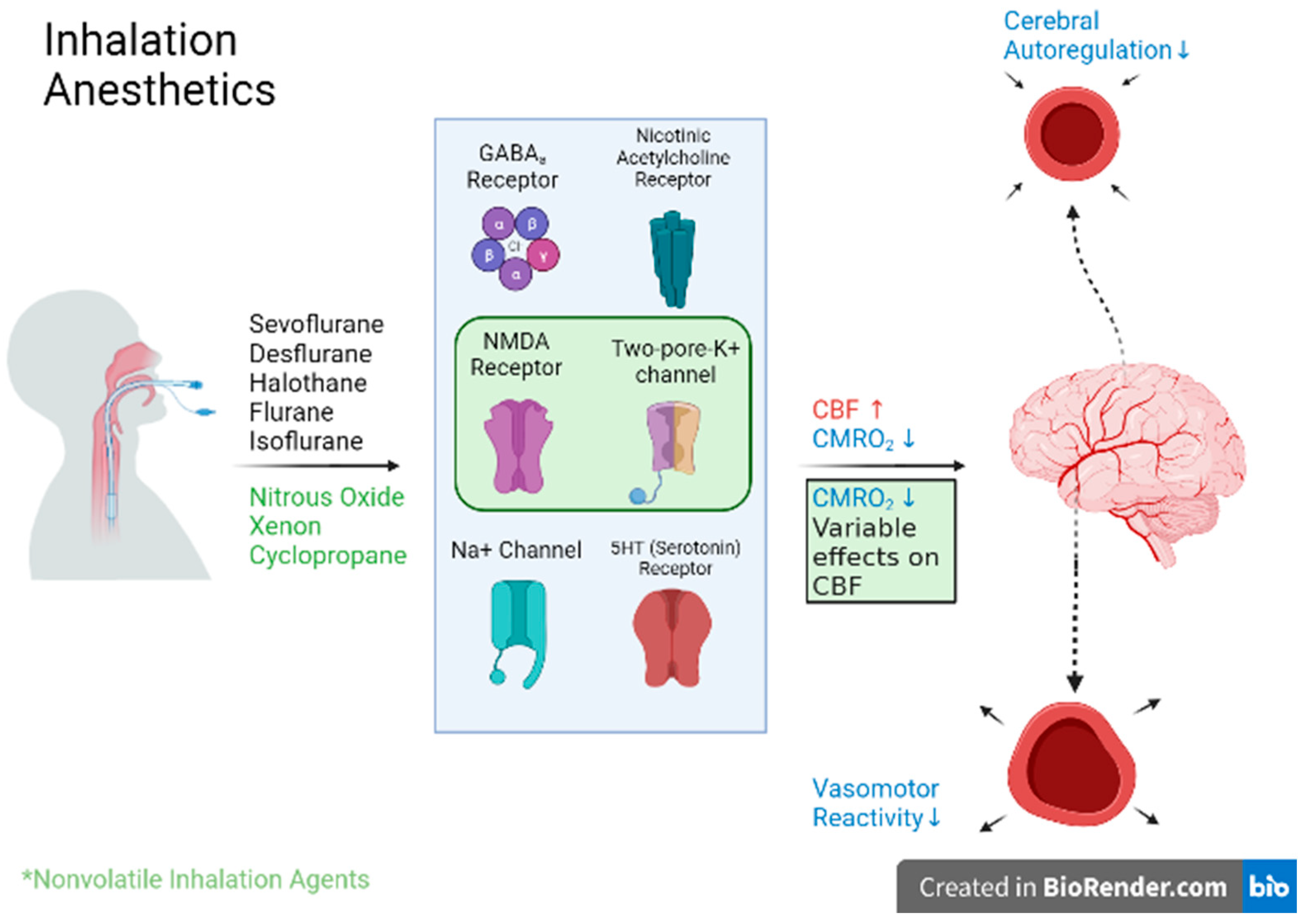
3.2. Volatile Anesthetics
3.3. Advantages and Disadvantages of Anesthetic Options
3.4. Systematic Review of Randomized-Controlled Trials Comparing Neuroanesthetic Agents (Spine or Spinal or Vertebrae or Vertebra) and (Brain or Cranial or Cranium) and (Surgery or Operation or Operative) and (Anaesthesia or Anesthesia or Sedative) and (ICP or Intracranial Pressure)
4. Biological Mechanism of Widespread, Select TIVA Agents
4.1. Thiopental
4.2. Propofol
4.3. Ketamine
5. Biological Mechanism of Widespread, Select Inhaled Agents
5.1. Sevoflurane
5.2. Desflurane
5.3. Isoflurane
6. Neuroanesthesia in Cranial Operations
6.1. Craniotomies
6.2. Functional Interventions
7. Neuroanesthesia in Spinal Operations
7.1. Spinal Cord Injuries
7.2. Elective Procedures
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Chivukula, S.; Grandhi, R.; Friedlander, R.M. A brief history of early neuroanesthesia. Neurosurg. Focus. 2014, 36, E2. [Google Scholar] [CrossRef] [Green Version]
- Lanier, W.L. The history of neuroanesthesiology: The people, pursuits, and practices. J. Neurosurg. Anesthesiol. 2012, 24, 281–299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slupe, A.M.; Kirsch, J.R. Effects of anesthesia on cerebral blood flow, metabolism, and neuroprotection. J. Cereb. Blood Flow. Metab. 2018, 38, 2192–2208. [Google Scholar] [CrossRef]
- Son, Y. Molecular mechanisms of general anesthesia. Korean J. Anesthesiol. 2010, 59, 3–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gruss, M.; Bushell, T.J.; Bright, D.P.; Lieb, W.R.; Mathie, A.; Franks, N.P. Two-pore-domain K+ channels are a novel target for the anesthetic gases xenon, nitrous oxide, and cyclopropane. Mol. Pharmacol. 2004, 65, 443–452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orser, B.A.; Pennefather, P.S.; MacDonald, J.F. Multiple mechanisms of ketamine blockade of N-methyl-D-aspartate receptors. Anesthesiology 1997, 86, 903–917. [Google Scholar] [CrossRef] [PubMed]
- Frost, E.A.M. Central Nervous System Effects of Anesthetic Agents. In Clinical Anesthesia in Neurosurgery, 2nd ed.; Butterworth-Heinemann, Ed.; Elsevier Inc.: Amsterdam, The Netherlands, 1991; pp. 129–145. [Google Scholar]
- Deng, J.; Lei, C.; Chen, Y.; Fang, Z.; Yang, Q.; Zhang, H.; Cai, M.; Shi, L.; Dong, H.; Xiong, L. Neuroprotective gases—Fantasy or reality for clinical use? Prog. Neurobiol. 2014, 115, 210–245. [Google Scholar] [CrossRef] [PubMed]
- Silverman, A.; Petersen, N.H. Physiology, Cerebral Autoregulation. In StatPearls; StatsPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Armstead, W.M. Cerebral Blood Flow Autoregulation and Dysautoregulation. Anesthesiol. Clin. 2016, 34, 465–477. [Google Scholar] [CrossRef] [Green Version]
- Bazin, J.E. Effects of anesthetic agents on intracranial pressure. Ann. Fr. Anesth. Reanim. 1997, 16, 445–452. [Google Scholar] [CrossRef]
- Masamoto, K.; Kanno, I. Anesthesia and the quantitative evaluation of neurovascular coupling. J. Cereb. Blood Flow. Metab. 2012, 32, 1233–1247. [Google Scholar] [CrossRef] [Green Version]
- Tomas Partington, A.F. Intracranial pressure and cerebral blood flow. Anaesth. Intensive Care Med. 2014, 15, 189–194. [Google Scholar] [CrossRef]
- Jorgensen, P.B.; Henriksen, H.T. The effect of fluroxene on intracranial pressure in patients with intracranial space-occupying lesions. Br. J. Anaesth. 1973, 45, 599–603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Searles, P.W. Intravenous Anesthesia. JAMA 1942, 118, 117–119. [Google Scholar] [CrossRef]
- Kay, B.; Rolly, G.I.C.I. 35868, a new intravenous induction agent. Acta Anaesthesiol. Belg. 1977, 28, 303–316. [Google Scholar] [PubMed]
- Antkowiak, B.; Rammes, G. GABA(A) receptor-targeted drug development -New perspectives in perioperative anesthesia. Expert Opin. Drug Discov. 2019, 14, 683–699. [Google Scholar] [CrossRef]
- Hans, P.; Bonhomme, V. Why we still use intravenous drugs as the basic regimen for neurosurgical anaesthesia. Curr. Opin. Anaesthesiol. 2006, 19, 498–503. [Google Scholar] [CrossRef]
- Cole, C.D.; Gottfried, O.N.; Gupta, D.K.; Couldwell, W.T. Total intravenous anesthesia: Advantages for intracranial surgery. Neurosurgery 2007, 61, 369–377; discussion 377–368. [Google Scholar] [CrossRef]
- Dershwitz, M.; Michalowski, P.; Chang, Y.; Rosow, C.E.; Conlay, L.A. Postoperative nausea and vomiting after total intravenous anesthesia with propofol and remifentanil or alfentanil: How important is the opioid? J. Clin. Anesth. 2002, 14, 275–278. [Google Scholar] [CrossRef]
- Demirbilek, S.; Ganidagli, S.; Aksoy, N.; Becerik, C.; Baysal, Z. The effects of remifentanil and alfentanil-based total intravenous anesthesia (TIVA) on the endocrine response to abdominal hysterectomy. J. Clin. Anesth. 2004, 16, 358–363. [Google Scholar] [CrossRef]
- Whalen, F.X.; Bacon, D.R.; Smith, H.M. Inhaled anesthetics: An historical overview. Best Pract. Res. Clin. Anaesthesiol. 2005, 19, 323–330. [Google Scholar] [CrossRef]
- Gaya da Costa, M.; Kalmar, A.F.; Struys, M. Inhaled Anesthetics: Environmental Role, Occupational Risk, and Clinical Use. J. Clin. Med. 2021, 10, 1306. [Google Scholar] [CrossRef]
- Thwaites, A.; Edmends, S.; Smith, I. Inhalation induction with sevoflurane: A double-blind comparison with propofol. Br. J. Anaesth. 1997, 78, 356–361. [Google Scholar] [CrossRef]
- Ergun, R.; Akdemir, G.; Sen, S.; Tasci, A.; Ergungor, F. Neuroprotective effects of propofol following global cerebral ischemia in rats. Neurosurg. Rev. 2002, 25, 95–98. [Google Scholar] [CrossRef]
- Paulson, O.B.; Strandgaard, S.; Edvinsson, L. Cerebral autoregulation. Cerebrovasc. Brain Metab. Rev. 1990, 2, 161–192. [Google Scholar]
- Dagal, A.; Lam, A.M. Cerebral autoregulation and anesthesia. Curr. Opin. Anaesthesiol. 2009, 22, 547–552. [Google Scholar] [CrossRef] [PubMed]
- Hughey, A.B.; Lesniak, M.S.; Ansari, S.A.; Roth, S. What will anesthesiologists be anesthetizing? Trends in neurosurgical procedure usage. Anesth. Analg. 2010, 110, 1686–1697. [Google Scholar] [CrossRef] [PubMed]
- Strebel, S.; Lam, A.M.; Matta, B.; Mayberg, T.S.; Aaslid, R.; Newell, D.W. Dynamic and static cerebral autoregulation during isoflurane, desflurane, and propofol anesthesia. Anesthesiology 1995, 83, 66–76. [Google Scholar] [CrossRef] [PubMed]
- Van Hemelrijck, J.; Van Aken, H.; Merckx, L.; Mulier, J. Anesthesia for craniotomy: Total intravenous anesthesia with propofol and alfentanil compared to anesthesia with thiopental sodium, isoflurane, fentanyl, and nitrous oxide. J. Clin. Anesth. 1991, 3, 131–136. [Google Scholar] [CrossRef]
- Petersen, K.D.; Landsfeldt, U.; Cold, G.E.; Petersen, C.B.; Mau, S.; Hauerberg, J.; Holst, P.; Olsen, K.S. Intracranial pressure and cerebral hemodynamic in patients with cerebral tumors: A randomized prospective study of patients subjected to craniotomy in propofol-fentanyl, isoflurane-fentanyl, or sevoflurane-fentanyl anesthesia. Anesthesiology 2003, 98, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Magni, G.; Baisi, F.; La Rosa, I.; Imperiale, C.; Fabbrini, V.; Pennacchiotti, M.L.; Rosa, G. No difference in emergence time and early cognitive function between sevoflurane-fentanyl and propofol-remifentanil in patients undergoing craniotomy for supratentorial intracranial surgery. J. Neurosurg. Anesthesiol. 2005, 17, 134–138. [Google Scholar] [CrossRef]
- Talke, P.; Caldwell, J.E.; Brown, R.; Dodson, B.; Howley, J.; Richardson, C.A. A comparison of three anesthetic techniques in patients undergoing craniotomy for supratentorial intracranial surgery. Anesth. Analg. 2002, 95, 430–435. [Google Scholar] [CrossRef] [PubMed]
- Chui, J.; Mariappan, R.; Mehta, J.; Manninen, P.; Venkatraghavan, L. Comparison of propofol and volatile agents for maintenance of anesthesia during elective craniotomy procedures: Systematic review and meta-analysis. Can. J. Anaesth. 2014, 61, 347–356. [Google Scholar] [CrossRef]
- Van Aken, H.; Van Hemelrijck, J.; Merckx, L.; Mollhoff, T.; Mulier, J.; Lubbesmeyer, H.J. Total intravenous anesthesia using propofol and alfentanil in comparison with balanced anesthesia in neurosurgery. Anasth Intensiv. Notf. 1990, 25, 54–58. [Google Scholar] [CrossRef]
- Ornstein, E.; Young, W.L.; Fleischer, L.H.; Ostapkovich, N. Desflurane and isoflurane have similar effects on cerebral blood flow in patients with intracranial mass lesions. Anesthesiology 1993, 79, 498–502. [Google Scholar] [CrossRef]
- Talke, P.; Caldwell, J.; Dodsont, B.; Richardson, C.A. Desflurane and isoflurane increase lumbar cerebrospinal fluid pressure in normocapnic patients undergoing transsphenoidal hypophysectomy. Anesthesiology 1996, 85, 999–1004. [Google Scholar] [CrossRef] [PubMed]
- Artru, A.A.; Lam, A.M.; Johnson, J.O.; Sperry, R.J. Intracranial pressure, middle cerebral artery flow velocity, and plasma inorganic fluoride concentrations in neurosurgical patients receiving sevoflurane or isoflurane. Anesth. Analg. 1997, 85, 587–592. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, W.E.; Charbel, F.T.; Edelman, G.; Ausman, J.I. Thiopental and desflurane treatment for brain protection. Neurosurgery 1998, 43, 1050–1053. [Google Scholar] [CrossRef] [PubMed]
- Talke, P.; Caldwell, J.E.; Richardson, C.A. Sevoflurane increases lumbar cerebrospinal fluid pressure in normocapnic patients undergoing transsphenoidal hypophysectomy. Anesthesiology 1999, 91, 127–130. [Google Scholar] [CrossRef] [PubMed]
- Iwata, T.; Inoue, S.; Kawaguchi, M.; Takahashi, M.; Sakamoto, T.; Kitaguchi, K.; Furuya, H.; Sakaki, T. Comparison of the effects of sevoflurane and propofol on cooling and rewarming during deliberate mild hypothermia for neurosurgery. Br. J. Anaesth. 2003, 90, 32–38. [Google Scholar] [CrossRef]
- Fraga, M.; Rama-Maceiras, P.; Rodino, S.; Aymerich, H.; Pose, P.; Belda, J. The effects of isoflurane and desflurane on intracranial pressure, cerebral perfusion pressure, and cerebral arteriovenous oxygen content difference in normocapnic patients with supratentorial brain tumors. Anesthesiology 2003, 98, 1085–1090. [Google Scholar] [CrossRef]
- Günes, Y.; Gündüz, M.; Özcengiz, D.; Özbek, H.; Isik, G. Dexmedetomidine-Remifentanil or Propofol-Remifentanil Anesthesia in Patients Undergoing Intracranial Surgery. Neurosurg. Q. 2005, 15, 122–126. [Google Scholar] [CrossRef]
- Sekimoto, K.; Nishikawa, K.; Ishizeki, J.; Kubo, K.; Saito, S.; Goto, F. The effects of volatile anesthetics on intraoperative monitoring of myogenic motor-evoked potentials to transcranial electrical stimulation and on partial neuromuscular blockade during propofol/fentanyl/nitrous oxide anesthesia in humans. J. Neurosurg. Anesthesiol. 2006, 18, 106–111. [Google Scholar] [CrossRef]
- Djian, M.C.; Blanchet, B.; Pesce, F.; Sermet, A.; Disdet, M.; Vazquez, V.; Gury, C.; Roux, F.X.; Raggueneau, J.L.; Coste, J.; et al. Comparison of the time to extubation after use of remifentanil or sufentanil in combination with propofol as anesthesia in adults undergoing nonemergency intracranial surgery: A prospective, randomized, double-blind trial. Clin. Ther. 2006, 28, 560–568. [Google Scholar] [CrossRef]
- Bhagat, H.; Dash, H.H.; Bithal, P.K.; Chouhan, R.S.; Pandia, M.P. Planning for early emergence in neurosurgical patients: A randomized prospective trial of low-dose anesthetics. Anesth. Analg. 2008, 107, 1348–1355. [Google Scholar] [CrossRef] [PubMed]
- Bonhomme, V.; Demoitie, J.; Schaub, I.; Hans, P. Acid-base status and hemodynamic stability during propofol and sevoflurane-based anesthesia in patients undergoing uncomplicated intracranial surgery. J. Neurosurg. Anesthesiol. 2009, 21, 112–119. [Google Scholar] [CrossRef]
- Ali, Z.; Prabhakar, H.; Bithal, P.K.; Dash, H.H. Bispectral index-guided administration of anesthesia for transsphenoidal resection of pituitary tumors: A comparison of 3 anesthetic techniques. J. Neurosurg. Anesthesiol. 2009, 21, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Bilotta, F.; Doronzio, A.; Cuzzone, V.; Caramia, R.; Rosa, G.; Group, P.S. Early postoperative cognitive recovery and gas exchange patterns after balanced anesthesia with sevoflurane or desflurane in overweight and obese patients undergoing craniotomy: A prospective randomized trial. J. Neurosurg. Anesthesiol. 2009, 21, 207–213. [Google Scholar] [CrossRef]
- Lauta, E.; Abbinante, C.; Del Gaudio, A.; Aloj, F.; Fanelli, M.; de Vivo, P.; Tommasino, C.; Fiore, T. Emergence times are similar with sevoflurane and total intravenous anesthesia: Results of a multicenter RCT of patients scheduled for elective supratentorial craniotomy. J. Neurosurg. Anesthesiol. 2010, 22, 110–118. [Google Scholar] [CrossRef]
- Yildiz, K.; Bicer, C.; Aksu, R.; Dogru, K.; Madenoglu, H.; Boyaci, A. A comparison of 1 minimum alveolar concentration desflurane and 1 minimum alveolar concentration isoflurane anesthesia in patients undergoing craniotomy for supratentorial lesions. Curr. Ther. Res. Clin. Exp. 2011, 72, 49–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghoneim, A.A.; Azer, M.S.; Ghobrial, H.Z.; El Beltagy, M.A. Awakening properties of isoflurane, sevoflurane, and desflurane in pediatric patients after craniotomy for supratentorial tumours. J. Neurosurg. Anesthesiol. 2015, 27, 1–6. [Google Scholar] [CrossRef]
- Hernandez-Palazon, J.; Fuentes-Garcia, D.; Domenech-Asensi, P.; Piqueras-Perez, C.; Falcon-Arana, L.; Burguillos-Lopez, S. A comparison of equivolume, equiosmolar solutions of hypertonic saline and mannitol for brain relaxation during elective supratentorial craniotomy. Br. J. Neurosurg. 2016, 30, 70–75. [Google Scholar] [CrossRef]
- Goettel, N.; Bharadwaj, S.; Venkatraghavan, L.; Mehta, J.; Bernstein, M.; Manninen, P.H. Dexmedetomidine vs propofol-remifentanil conscious sedation for awake craniotomy: A prospective randomized controlled trial. Br. J. Anaesth. 2016, 116, 811–821. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gokcek, E.; Kaydu, A.; Akdemir, M.S.; Akil, F.; Akinci, I.O. Early postoperative recovery after intracranial surgical procedures. Comparison of the effects of sevoflurane and desflurane. Acta Cir. Bras. 2016, 31, 638–644. [Google Scholar] [CrossRef] [Green Version]
- Lin, N.; Han, R.; Zhou, J.; Gelb, A.W. Mild Sedation Exacerbates or Unmasks Focal Neurologic Dysfunction in Neurosurgical Patients with Supratentorial Brain Mass Lesions in a Drug-specific Manner. Anesthesiology 2016, 124, 598–607. [Google Scholar] [CrossRef] [PubMed]
- Rajan, S.; Hutcherson, M.T.; Sessler, D.I.; Kurz, A.; Yang, D.; Ghobrial, M.; Liu, J.; Avitsian, R. The Effects of Dexmedetomidine and Remifentanil on Hemodynamic Stability and Analgesic Requirement After Craniotomy: A Randomized Controlled Trial. J Neurosurg. Anesthesiol. 2016, 28, 282–290. [Google Scholar] [CrossRef] [Green Version]
- Thongrong, C.; Sirikannarat, P.; Kasemsiri, P.; Duangthongphon, P. Comparison of dexmedetomidine and fentanyl to prevent haemodynamic response to skull pin application in neurosurgery: Double blind randomized controlled trial. Anaesthesiol. Intensive Ther. 2017, 49, 268–273. [Google Scholar] [CrossRef] [PubMed]
- Bhardwaj, A.; Bhagat, H.; Grover, V.K.; Panda, N.B.; Jangra, K.; Sahu, S.; Singla, N. Comparison of propofol and desflurane for postanaesthetic morbidity in patients undergoing surgery for aneurysmal SAH: A randomized clinical trial. J. Anesth. 2018, 32, 250–258. [Google Scholar] [CrossRef]
- Gracia, C.Z.; Hanafie, A.; Nasution, A.H. Comparison of hemodynamic response between propofol and thiopental as an induction agent in neurosurgery anesthesia at Haji Adam Malik General Hospital Medan-Indonesa. Bali Med. J. 2018, 7, 712–722. [Google Scholar]
- Suero Molina, E.; Schipmann, S.; Mueller, I.; Wolfer, J.; Ewelt, C.; Maas, M.; Brokinkel, B.; Stummer, W. Conscious sedation with dexmedetomidine compared with asleep-awake-asleep craniotomies in glioma surgery: An analysis of 180 patients. J. Neurosurg. 2018, 129, 1223–1230. [Google Scholar] [CrossRef] [Green Version]
- Xinyan, Z.; Xuekang, Z.; Sisi, L.; Xinhua, F.; Shi, S.; Zhiyi, L. Effects of dexmedetomidine, propofol and etomidate on the intraoperative wake-up in the cerebral functional area under the guidance of entropy index. Pharmazie 2018, 73, 647–650. [Google Scholar] [CrossRef]
- Khallaf, M.; Thabet, A.M.; Ali, M.; Sharkawy, E.; Abdel-rehim, S. The effect of dexmedetomidine versus propofol in traumatic brain injury: Evaluation of some hemodynamic and intracranial pressure changes. Egypt. J. Neurosurg. 2019, 34, 17. [Google Scholar] [CrossRef]
- Preethi, J.; Bidkar, P.U.; Cherian, A.; Dey, A.; Srinivasan, S.; Adinarayanan, S.; Ramesh, A.S. Comparison of total intravenous anesthesia vs. inhalational anesthesia on brain relaxation, intracranial pressure, and hemodynamics in patients with acute subdural hematoma undergoing emergency craniotomy: A randomized control trial. Eur. J. Trauma Emerg. Surg. 2021, 47, 831–837. [Google Scholar] [CrossRef]
- Balasubramanian, M.; Kuberan, A.; Rawat, A.; Dhandapani, S.; Panda, N.; Kumar, A.; Sahoo, A.K.; Kumar, M.; Sharma, T.; Garcia, P.S.; et al. Effect of General Anesthetics on Caspase-3 Levels in Patients With Aneurysmal Subarachnoid Hemorrhage: A Preliminary Study. J. Neurosurg. Anesthesiol. 2021, 33, 172–176. [Google Scholar] [CrossRef]
- Laureau, E.; Marciniak, B.; Hebrard, A.; Herbaux, B.; Guieu, J.D. Comparative study of propofol and midazolam effects on somatosensory evoked potentials during surgical treatment of scoliosis. Neurosurgery 1999, 45, 69–74. [Google Scholar] [CrossRef]
- Inoue, Y.; Koga, K.; Sata, T.; Shigematsu, A. Effects of fentanyl on emergence characteristics from anesthesia in adult cervical spine surgery: A comparison of fentanyl-based and sevoflurane-based anesthesia. J. Anesth. 2005, 19, 12–16. [Google Scholar] [CrossRef] [PubMed]
- Kurt, F.; Derbent, A.; Demirag, K.; Eris, O.; Uyar, M.; Islekel, S. Old method, new drugs: Comparison of the efficacy of sevoflurane, isoflurane, and desflurane in achieving controlled hypotension in spinal surgery. Adv. Ther. 2005, 22, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Albertin, A.; La Colla, L.; Gandolfi, A.; Colnaghi, E.; Mandelli, D.; Gioia, G.; Fraschini, G. Greater peripheral blood flow but less bleeding with propofol versus sevoflurane during spine surgery: A possible physiologic model? Spine 2008, 33, 2017–2022. [Google Scholar] [CrossRef]
- Turgut, N.; Turkmen, A.; Gokkaya, S.; Altan, A.; Hatiboglu, M.A. Dexmedetomidine-based versus fentanyl-based total intravenous anesthesia for lumbar laminectomy. Minerva Anestesiol. 2008, 74, 469–474. [Google Scholar]
- Güneş, Y.; Türktan, M.; Erman, T.; Özbek, H.; Işik, G. Anesthesia for craniotomy: Comparison of sevoflurane, desflurane, or isoflurane anesthesia supplemented with an infusion of dexmedetomidine during supratentorial craniotomy. Neurosurg. Q. 2009, 19, 110–115. [Google Scholar] [CrossRef]
- Magni, G.; La Rosa, I.; Melillo, G.; Savio, A. and Rosa, G. A comparison between sevoflurane and desflurane anesthesia in patients undergoing craniotomy for supratentorial intracranial surgery. Anesth Analg. 2009, 109, 567–571. [Google Scholar] [CrossRef] [PubMed]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [Green Version]
- Skibiski, J.; Abdijadid, S. Barbiturates. In StatPearls; StatsPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Brohan, J.; Goudra, B.G. The Role of GABA Receptor Agonists in Anesthesia and Sedation. CNS Drugs 2017, 31, 845–856. [Google Scholar] [CrossRef] [PubMed]
- Hara, M.; Kai, Y.; Ikemoto, Y. Propofol activates GABAA receptor-chloride ionophore complex in dissociated hippocampal pyramidal neurons of the rat. Anesthesiology 1993, 79, 781–788. [Google Scholar] [CrossRef]
- Sahinovic, M.M.; Struys, M.; Absalom, A.R. Clinical Pharmacokinetics and Pharmacodynamics of Propofol. Clin. Pharm. 2018, 57, 1539–1558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goetz, T.; Arslan, A.; Wisden, W.; Wulff, P. GABA(A) receptors: Structure and function in the basal ganglia. Prog. Brain Res. 2007, 160, 21–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jayakar, S.S.; Zhou, X.; Chiara, D.C.; Dostalova, Z.; Savechenkov, P.Y.; Bruzik, K.S.; Dailey, W.P.; Miller, K.W.; Eckenhoff, R.G.; Cohen, J.B. Multiple propofol-binding sites in a gamma-aminobutyric acid type A receptor (GABAAR) identified using a photoreactive propofol analog. J. Biol. Chem. 2014, 289, 27456–27468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mikkelsen, M.L.; Ambrus, R.; Miles, J.E.; Poulsen, H.H.; Moltke, F.B.; Eriksen, T. Effect of propofol and remifentanil on cerebral perfusion and oxygenation in pigs: A systematic review. Acta Vet. Scand. 2016, 58, 42. [Google Scholar] [CrossRef] [Green Version]
- Wu, M.; Yin, X.; Chen, M.; Liu, Y.; Zhang, X.; Li, T.; Long, Y.; Wu, X.; Pu, L.; Zhang, M.; et al. Effects of propofol on intracranial pressure and prognosis in patients with severe brain diseases undergoing endotracheal suctioning. BMC Neurol. 2020, 20, 394. [Google Scholar] [CrossRef]
- Giovannitti, J.A., Jr.; Thoms, S.M.; Crawford, J.J. Alpha-2 adrenergic receptor agonists: A review of current clinical applications. Anesth. Prog. 2015, 62, 31–39. [Google Scholar] [CrossRef] [Green Version]
- Godoy, D.A.; Badenes, R.; Pelosi, P.; Robba, C. Ketamine in acute phase of severe traumatic brain injury “an old drug for new uses?”. Crit. Care 2021, 25, 19. [Google Scholar] [CrossRef]
- Rueda Carrillo, L.; Garcia, K.A.; Yalcin, N.; Shah, M. Ketamine and Its Emergence in the Field of Neurology. Cureus 2022, 14, e27389. [Google Scholar] [CrossRef]
- Farag, E.; Kot, M.; Podolyak, A.; Argalious, M.; Deogaonkar, M.; Mascha, E.J.; Xu, Z.; Katzan, I.; Ebrahim, Z. The relative effects of dexmedetomidine and propofol on cerebral blood flow velocity and regional brain oxygenation: A randomised noninferiority trial. Eur. J. Anaesthesiol. 2017, 34, 732–739. [Google Scholar] [CrossRef]
- Bowles, E.D.; Gold, M.E. Rethinking the paradigm: Evaluation of ketamine as a neurosurgical anesthetic. AANA J. 2012, 80, 445–452. [Google Scholar] [PubMed]
- Ankur Luthra, G.R. The relative effects of dexmedetomidine and propofol on cerebral blood flow velocity and regional brain oxygenation. J. Neuroanaesth. Crit. Care 2018, 34, 732–739. [Google Scholar] [CrossRef] [Green Version]
- Zeiler, F.A.; Teitelbaum, J.; West, M.; Gillman, L.M. The ketamine effect on ICP in traumatic brain injury. Neurocrit Care 2014, 21, 163–173. [Google Scholar] [CrossRef]
- Tasbihgou, S.R.; Barends, C.R.M.; Absalom, A.R. The role of dexmedetomidine in neurosurgery. Best Pr. Res. Clin. Anaesthesiol. 2021, 35, 221–229. [Google Scholar] [CrossRef] [PubMed]
- Schomer, K.J.; Sebat, C.M.; Adams, J.Y.; Duby, J.J.; Shahlaie, K.; Louie, E.L. Dexmedetomidine for Refractory Intracranial Hypertension. J. Intensive Care Med. 2019, 34, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Tsaousi, G.G.; Bilotta, F. Is dexmedetomidine a favorable agent for cerebral hemodynamics? Indian J. Crit. Care Med. 2016, 20, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Edgington, T.L.; Muco, E.; Maani, C.V. Sevoflurane. In StatPearls; Stats Pearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Duffy, C.M.; Matta, B.F. Sevoflurane and anesthesia for neurosurgery: A review. J. Neurosurg. Anesthesiol. 2000, 12, 128–140. [Google Scholar] [CrossRef] [Green Version]
- Gauthier, A.; Girard, F.; Boudreault, D.; Ruel, M.; Todorov, A. Sevoflurane provides faster recovery and postoperative neurological assessment than isoflurane in long-duration neurosurgical cases. Anesth. Analg. 2002, 95, 1384–1388. [Google Scholar] [CrossRef]
- Singh, D.; Rath, G.P.; Dash, H.H.; Bithal, P.K. Sevoflurane provides better recovery as compared with isoflurane in children undergoing spinal surgery. J. Neurosurg. Anesthesiol. 2009, 21, 202–206. [Google Scholar] [CrossRef]
- Shan, J.; Sun, L.; Wang, D.; Li, X. Comparison of the neuroprotective effects and recovery profiles of isoflurane, sevoflurane and desflurane as neurosurgical pre-conditioning on ischemia/reperfusion cerebral injury. Int. J. Clin. Exp. Pathol. 2015, 8, 2001–2009. [Google Scholar]
- Zhou, Z.; Ying, M.; Zhao, R. Efficacy and safety of sevoflurane vs propofol in combination with remifentanil for anesthesia maintenance during craniotomy: A meta-analysis. Medicine 2021, 100, e28400. [Google Scholar] [CrossRef] [PubMed]
- Moshchev, D.A.; Lubnin, A. Application of desflurane in anaesthesiology. Anesteziol. Reanimatol. 2014, 1, 71–78. [Google Scholar]
- Baker, K.Z. Desflurane and sevoflurane are valuable additions to the practice of neuroanesthesiology: Pro. J. Neurosurg. Anesthesiol 1997, 9, 66–68. [Google Scholar] [CrossRef]
- Xiang, B.; Jiao, S.; Zhang, Y.; Wang, L.; Yao, Y.; Yuan, F.; Chen, R.; Zhou, Q. Effects of desflurane and sevoflurane on somatosensory-evoked and motor-evoked potential monitoring during neurosurgery: A randomized controlled trial. BMC Anesthesiol. 2021, 21, 240. [Google Scholar] [CrossRef]
- Hoffman, W.E.; Charbel, F.T.; Edelman, G. Desflurane increases brain tissue oxygenation and pH. Acta Anaesthesiol. Scand. 1997, 41, 1162–1166. [Google Scholar] [CrossRef]
- Hawkley, T.F.; Preston, M.; Maani, C.V. Isoflurane. In StatPearls; StatsPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Altay, O.; Suzuki, H.; Hasegawa, Y.; Ostrowski, R.P.; Tang, J.; Zhang, J.H. Isoflurane on brain inflammation. Neurobiol. Dis. 2014, 62, 365–371. [Google Scholar] [CrossRef] [Green Version]
- Altay, O.; Suzuki, H.; Altay, B.N.; Calisir, V.; Tang, J.; Zhang, J.H. Isoflurane versus sevoflurane for early brain injury and expression of sphingosine kinase 1 after experimental subarachnoid hemorrhage. Neurosci. Lett. 2020, 733, 135142. [Google Scholar] [CrossRef]
- Lemkuil, B.P.; Head, B.P.; Pearn, M.L.; Patel, H.H.; Drummond, J.C.; Patel, P.M. Isoflurane neurotoxicity is mediated by p75NTR-RhoA activation and actin depolymerization. Anesthesiology 2011, 114, 49–57. [Google Scholar] [CrossRef] [Green Version]
- Xia, Y.; Sun, X.; Luo, Y.; Stary, C.M. Ferroptosis Contributes to Isoflurane Neurotoxicity. Front. Mol. Neurosci. 2018, 11, 486. [Google Scholar] [CrossRef] [PubMed]
- Cheng, F.; Chang, H.; Yan, F.; Yang, A.; Liu, J.; Liu, Y. Agomelatine Attenuates Isoflurane-Induced Inflammation and Damage in Brain Endothelial Cells. Drug. Des. Devel. Ther. 2020, 14, 5589–5598. [Google Scholar] [CrossRef]
- Adams, R.W.; Cucchiara, R.F.; Gronert, G.A.; Messick, J.M.; Michenfelder, J.D. Isoflurane and cerebrospinal fluid pressure in neurosurgical patients. Anesthesiology 1981, 54, 97–99. [Google Scholar] [CrossRef]
- Massei, R.; Calappi, E.; Parma, A.; Granata, G. Effects of inhalation anesthetics on intracranial pressure and cerebral blood flow velocity. Minerva Anestesiol. 1994, 60, 643–647. [Google Scholar]
- Waaben, J.; Husum, B.; Hansen, A.J.; Gjedde, A. Hypocapnia prevents the decrease in regional cerebral metabolism during isoflurane-induced hypotension. J. Neurosurg. Anesthesiol. 1989, 1, 29–34. [Google Scholar] [CrossRef]
- Meng, L.; McDonagh, D.L.; Berger, M.S.; Gelb, A.W. Anesthesia for awake craniotomy: A how-to guide for the occasional practitioner. Can. J. Anaesth. 2017, 64, 517–529. [Google Scholar] [CrossRef] [Green Version]
- Stevanovic, A.; Rossaint, R.; Veldeman, M.; Bilotta, F.; Coburn, M. Anaesthesia Management for Awake Craniotomy: Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0156448. [Google Scholar] [CrossRef] [Green Version]
- Osborn, I.; Sebeo, J. “Scalp block” during craniotomy: A classic technique revisited. J. Neurosurg. Anesthesiol. 2010, 22, 187–194. [Google Scholar] [CrossRef] [Green Version]
- Sokhal, N.; Rath, G.P.; Chaturvedi, A.; Dash, H.H.; Bithal, P.K.; Chandra, P.S. Anaesthesia for awake craniotomy: A retrospective study of 54 cases. Indian J. Anaesth. 2015, 59, 300–305. [Google Scholar] [CrossRef]
- Shen, S.L.; Zheng, J.Y.; Zhang, J.; Wang, W.Y.; Jin, T.; Zhu, J.; Zhang, Q. Comparison of dexmedetomidine and propofol for conscious sedation in awake craniotomy: A prospective, double-blind, randomized, and controlled clinical trial. Ann. Pharmacother. 2013, 47, 1391–1399. [Google Scholar] [CrossRef]
- Rasmussen, K.G. Propofol for ECT anesthesia a review of the literature. J. ECT 2014, 30, 210–215. [Google Scholar] [CrossRef]
- Souter, M.J.; Rozet, I.; Ojemann, J.G.; Souter, K.J.; Holmes, M.D.; Lee, L.; Lam, A.M. Dexmedetomidine sedation during awake craniotomy for seizure resection: Effects on electrocorticography. J. Neurosurg. Anesthesiol. 2007, 19, 38–44. [Google Scholar] [CrossRef]
- Sakamoto, A.; Hoshino, T.; Suzuki, N.; Suzuki, H.; Kimura, M.; Ogawa, R. Effects of propofol anesthesia on cognitive recovery of patients undergoing electroconvulsive therapy. Psychiatry Clin. Neurosci. 1999, 53, 655–660. [Google Scholar] [CrossRef]
- Geretsegger, C.; Nickel, M.; Judendorfer, B.; Rochowanski, E.; Novak, E.; Aichhorn, W. Propofol and methohexital as anesthetic agents for electroconvulsive therapy: A randomized, double-blind comparison of electroconvulsive therapy seizure quality, therapeutic efficacy, and cognitive performance. J. ECT 2007, 23, 239–243. [Google Scholar] [CrossRef]
- Wang, X.; Chen, Y.; Zhou, X.; Liu, F.; Zhang, T.; Zhang, C. Effects of propofol and ketamine as combined anesthesia for electroconvulsive therapy in patients with depressive disorder. J. ECT 2012, 28, 128–132. [Google Scholar] [CrossRef]
- Bao, F.P.; Zhang, H.G.; Zhu, S.M. Anesthetic considerations for patients with acute cervical spinal cord injury. Neural. Regen. Res. 2017, 12, 499–504. [Google Scholar] [CrossRef]
- Ahuja, C.S.; Wilson, J.R.; Nori, S.; Kotter, M.R.N.; Druschel, C.; Curt, A.; Fehlings, M.G. Traumatic spinal cord injury. Nat. Rev. Dis. Prim. 2017, 3, 17018. [Google Scholar] [CrossRef] [Green Version]
- Claydon, V.E.; Krassioukov, A.V. Orthostatic hypotension and autonomic pathways after spinal cord injury. J. Neurotrauma 2006, 23, 1713–1725. [Google Scholar] [CrossRef]
- Blake, D.W.; Donnan, G.; Novella, J.; Hackman, C. Cardiovascular effects of sedative infusions of propofol and midazolam after spinal anaesthesia. Anaesth. Intensive Care 1988, 16, 292–298. [Google Scholar] [CrossRef] [Green Version]
- Kumar, N.; Rajan, S.; Kumar, L. Efficacy of Ketofol in Blunting Hypotensive Effects of Propofol during Induction and Its Effect on Intraoperative Anesthetic Requirements and Recovery Profile. Anesth Essays Res. 2020, 14, 605–610. [Google Scholar] [CrossRef]
- Park, J.H.; Hyun, S.J. Intraoperative neurophysiological monitoring in spinal surgery. World J. Clin. Cases 2015, 3, 765–773. [Google Scholar] [CrossRef]
- McPherson, R.W.; Mahla, M.; Johnson, R.; Traystman, R.J. Effects of enflurane, isoflurane, and nitrous oxide on somatosensory evoked potentials during fentanyl anesthesia. Anesthesiology 1985, 62, 626–633. [Google Scholar] [CrossRef]
- Strahm, C.; Min, K.; Boos, N.; Ruetsch, Y.; Curt, A. Reliability of perioperative SSEP recordings in spine surgery. Spinal Cord 2003, 41, 483–489. [Google Scholar] [CrossRef]
- Kalkman, C.J.; Traast, H.; Zuurmond, W.W.; Bovill, J.G. Differential effects of propofol and nitrous oxide on posterior tibial nerve somatosensory cortical evoked potentials during alfentanil anaesthesia. Br. J. Anaesth. 1991, 66, 483–489. [Google Scholar] [CrossRef]
- Lotto, M.L.; Banoub, M.; Schubert, A. Effects of anesthetic agents and physiologic changes on intraoperative motor evoked potentials. J. Neurosurg. Anesthesiol. 2004, 16, 32–42. [Google Scholar] [CrossRef] [Green Version]
- Scheufler, K.M.; Zentner, J. Total intravenous anesthesia for intraoperative monitoring of the motor pathways: An integral view combining clinical and experimental data. J. Neurosurg. 2002, 96, 571–579. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Hu, H.; Yan, R.; Li, T.; Wang, W.; Yang, W. Effects of rocuronium dosage on intraoperative neurophysiological monitoring in patients undergoing spinal surgery. J. Clin. Pharm. Ther. 2022, 47, 313–320. [Google Scholar] [CrossRef]
- Chung, Y.H.; Chung, I.S.; Kim, M.H.; Shin, J.; Park, J.; Lee, J.J. Comparing the effects of vecuronium and cisatracurium on electrophysiologic monitoring during neurosurgery: A randomized controlled study. Anesth. Pain Med. 2017, 12, 213–219. [Google Scholar] [CrossRef] [Green Version]
- Sloan, T.B. Muscle relaxant use during intraoperative neurophysiologic monitoring. J. Clin. Monit. Comput. 2013, 27, 35–46. [Google Scholar] [CrossRef]
- Lurie, J.; Tomkins-Lane, C. Management of lumbar spinal stenosis. BMJ 2016, 352, h6234. [Google Scholar] [CrossRef]
- Virk, S.S.; Niedermeier, S.; Yu, E.; Khan, S.N. Adjacent segment disease. Orthopedics 2014, 37, 547–555. [Google Scholar] [CrossRef] [Green Version]
- Silvers, H.R.; Lewis, P.J.; Asch, H.L. Decompressive lumbar laminectomy for spinal stenosis. J. Neurosurg. 1993, 78, 695–701. [Google Scholar] [CrossRef]
- Jiang, S.; Li, W. Biomechanical study of proximal adjacent segment degeneration after posterior lumbar interbody fusion and fixation: A finite element analysis. J. Orthop. Surg. Res. 2019, 14, 135. [Google Scholar] [CrossRef]
- Burch, M.B.; Wiegers, N.W.; Patil, S.; Nourbakhsh, A. Incidence and risk factors of reoperation in patients with adjacent segment disease: A meta-analysis. J. Craniovertebr. Junction Spine 2020, 11, 9–16. [Google Scholar] [CrossRef]
- Irmola, T.M.; Hakkinen, A.; Jarvenpaa, S.; Marttinen, I.; Vihtonen, K.; Neva, M. Reoperation Rates Following Instrumented Lumbar Spine Fusion. Spine 2018, 43, 295–301. [Google Scholar] [CrossRef]
- Apfelbaum, J.L.; Hagberg, C.A.; Connis, R.T.; Abdelmalak, B.B.; Agarkar, M.; Dutton, R.P.; Fiadjoe, J.E.; Greif, R.; Klock, P.A.; Mercier, D.; et al. 2022 American Society of Anesthesiologists Practice Guidelines for Management of the Difficult Airway. Anesthesiology 2022, 136, 31–81. [Google Scholar] [CrossRef]
- Mordecai, M.M.; Brull, S.J. Spinal anesthesia. Curr. Opin. Anaesthesiol. 2005, 18, 527–533. [Google Scholar] [CrossRef]
- Mohta, M. Ropivacaine: Is it a good choice for spinal anesthesia? J. Anaesthesiol. Clin. Pharmacol. 2015, 31, 457–458. [Google Scholar] [CrossRef]
- Hartmann, B.; Junger, A.; Klasen, J.; Benson, M.; Jost, A.; Banzhaf, A.; Hempelmann, G. The incidence and risk factors for hypotension after spinal anesthesia induction: An analysis with automated data collection. Anesth. Analg. 2002, 94, 1521–1529, table of contents. [Google Scholar] [CrossRef]
- McLain, R.F.; Kalfas, I.; Bell, G.R.; Tetzlaff, J.E.; Yoon, H.J.; Rana, M. Comparison of spinal and general anesthesia in lumbar laminectomy surgery: A case-controlled analysis of 400 patients. J. Neurosurg. Spine 2005, 2, 17–22. [Google Scholar] [CrossRef]
- Pierce, J.T.; Kositratna, G.; Attiah, M.A.; Kallan, M.J.; Koenigsberg, R.; Syre, P.; Wyler, D.; Marcotte, P.J.; Kofke, W.A.; Welch, W.C. Efficiency of spinal anesthesia versus general anesthesia for lumbar spinal surgery: A retrospective analysis of 544 patients. Local. Reg. Anesth. 2017, 10, 91–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sekerak, R.; Mostafa, E.; Morris, M.T.; Nessim, A.; Vira, A.; Sharan, A. Comparative outcome analysis of spinal anesthesia versus general anesthesia in lumbar fusion surgery. J. Clin. Orthop. Trauma 2021, 13, 122–126. [Google Scholar] [CrossRef] [PubMed]
- Sarkar, S.; Banerji, A.; Chattopadhyaya, A.; Banerjee, S. Lumbar spine instrumented fusion surgery under spinal anaesthesia versus general anaesthesia-A retrospective study of 239 cases. J. Clin. Orthop. Trauma 2021, 18, 205–208. [Google Scholar] [CrossRef] [PubMed]
- Scheinin, B.; Lindgren, L.; Randell, T.; Scheinin, H.; Scheinin, M. Dexmedetomidine attenuates sympathoadrenal responses to tracheal intubation and reduces the need for thiopentone and peroperative fentanyl. Br. J. Anaesth. 1992, 68, 126–131. [Google Scholar] [CrossRef] [PubMed]
- De Rojas, J.O.; Syre, P.; Welch, W.C. Regional anesthesia versus general anesthesia for surgery on the lumbar spine: A review of the modern literature. Clin. Neurol. Neurosurg. 2014, 119, 39–43. [Google Scholar] [CrossRef]
- Garg, B.; Ahuja, K.; Khanna, P.; Sharan, A.D. Regional Anesthesia for Spine Surgery. Clin. Spine Surg. 2020, 34, 163–170. [Google Scholar] [CrossRef]
- Kurnutala, L.N.; Dibble, J.E.; Kinthala, S.; Tucci, M.A. Enhanced Recovery After Surgery Protocol for Lumbar Spinal Surgery With Regional Anesthesia: A Retrospective Review. Cureus 2021, 13, e18016. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Authors and Year | Surgical Procedure | Comparison | Findings |
|---|---|---|---|
| Aken et al., 1990 [35] | Unspecified cranial procedure | Balanced anesthesia (loading thiopental and fentanyl + maintenance fentanyl, droperidol, thiopental, and isoflurane in nitrous oxide, n = 20) vs. TIVA (loading propofol + alfentanil infusion, n = 20) | During induction, TIVA had a significantly greater hemodynamic stability. Balance anesthesia was associated with a significantly longer emergence time than TIVA. |
| Hemelrijck et al., 1991 [30] | Craniotomy for resection of brain tumor | Propofol (n = 20) vs. thiopental (n = 20) | Postoperative return to orientation time was shorter in the propofol group (7 +/− 5 min vs. 27 +/− 23 min). |
| Ornstein et al., 1993 [36] | Craniotomy for resection of supratentorial lesion | Anesthetic maintenance via desflurane (n = 12) vs. isoflurane (n = 12) | CBF values were non-significantly different as measured at 1 MAC and 1.5 MAC concentrations for both desflurane and isoflurane (p > 0.05), as well as at 1.25 MAC as measured in n = 15 patients (p > 0.05). |
| Talke et al., 1996 [37] | Hypophysectomy | Propofol (n = 10) vs. loading propofol + maintenance desflurane (n = 10) vs. loading propofol + maintenance isoflurane (n = 10) | Minimum CPP was significantly lower in desflurane (p < 0.05) and isoflurane (p < 0.05) groups compared to propofol-only control. Minimum SBP was significantly lower in desflurane (p < 0.05) and isoflurane (p < 0.05) compared to propofol-only control. |
| Artru et al., 1997 [38] | Unspecified cranial procedure | Anesthetic maintenance via sevoflurane (n = 8) and isoflurane (n = 6) following induction via mannitol | Neither sevoflurane or isoflurane significantly altered ICP, and both decreased middle cerebral artery flow velocity (Vmca). Notably, decreased Vmca with sevoflurane was related to decreased CPP at 0.5 MAC (p < 0.05), and increased CVRe at 1.0 and 1.5 MAC (p < 0.05). The CPP decreased from baseline at 0.5, 1.0, and 1.5 MACs of isoflurane (p < 0.05). |
| Hoffman et al., 1998 [39] | Craniotomy for unspecified pathology | Thiopental induction (n = 10) vs. desflurane (n = 10) | Neither thiopental nor desflurane changed tissue gases or pH, but desflurane increased PO2 70% (p < 0.05), whereas thiopental decreased PO2 30% during temporary brain artery occlusion. |
| Talke et al., 1999 [40] | Transsphenoidal Hypophysectomy | Anesthetic maintenance via propofol (n = 10) vs. sevoflurane (n = 20) | Sevoflurane increased lumbar CSF pressure and decreased CPP and systolic blood pressure following infusion while propofol did not affect lumbar CSF pressure, CPP, nor systolic blood pressure. |
| Talke et al., 2002 [33] | Craniotomy for resection of supratentorial lesion | Propofol (n = 20) vs. isoflurane (n = 20) | Emergence time to eyes opening was not different between anesthetic agents (p > 0.05). There was no difference in occurrence of hypertension (p > 0.05). |
| Iwata et al., 2003 [41] | Unspecified intracranial surgery | Propofol (n = 13) vs. sevoflurane (n = 13) | There was no difference in the rate of temperature decrease and recovery in induced hypothermia (p < 0.05). |
| Fraga et al., 2003 [42] | Craniotomy for resection of supratentorial lesion | Inhalation of isoflurane (n = 30) vs. desflurane (n = 30) following induction via fentanyl, thiopental, and vecuronium maintained with 60% nitrous oxide in oxygen | There were no significant differences between MAP, ICP, and CPP between use of desflurane and isoflurane, but notable decreases (p < 0.05) in both groups from baseline values with regard to MAP and CPP. The ratio between the cerebral metabolic oxygen requirement and cerebral blood flow decreased significantly for both groups as well. |
| Petersen et al., 2003 [31] | Craniotomy for resection of supratentorial tumor | Propofol (n = 41) vs. isoflurane (n = 38) vs. sevoflurane (n = 38) | No differences in ICP or CPP between anesthetic agents (p > 0.05). |
| Günes et al., 2005 [43] | Unspecified intracranial procedure | Anesthetic maintenance via propofol (n = 39) vs. dexmedetomidine (n = 39) | Systolic blood pressure and MAP were not different between the two agents. Extubation time was shorter for propofol (p < 0.05). Analgesic requirements were higher for propofol (p = 0.013). |
| Magni et al., 2005 [32] | Supratentorial craniotomy for unspecified pathology | Propofol (n = 64) vs. sevoflurane (n = 64) | Emergence time was not different between anesthetic agents. Occurrence of hypertension was higher in propofol than sevoflurane use (p = 0.0046), and hypotension was higher in propofol than sevoflurane (p = 0.02). |
| Sekimoto et al., 2006 [44] | Craniotomy for resection of brain tumor | Anesthetic maintenance via halothane vs. isoflurane vs. sevoflurane after induction via propofol/fentanyl/nitrous oxide | Halothane, isoflurane, and sevoflurane were all found to reduce systolic blood pressure, but only sevoflurane and isoflurane decreased train-of-four ratios significantly at 1.0 MAC (p < 0.001). Amplitudes of transcranial motor-evoked potentials were reduced by isoflurane and sevoflurane at 0.5 MACs, but not halothane, reflecting the reduced extent of the neuromuscular blockade initiated by halothane. |
| Djian et al., 2006 [45] | Unspecified intracranial procedure | Remifentanil vs. sufentanil in combination with propofol for maintenance of anesthesia | Remifentanil was associated with the need for less adjustments with regard to hemodynamic stability (p = 0.037), greater use of morphine (p = 0.01), and higher intraoperative opioid costs. However, there was no significant differences in extubation times between groups. |
| Bhagat et al., 2008 [46] | Craniotomy for unspecified pathology | Anesthetic maintenance via propofol (n = 50) vs. isoflurane (n = 50) | Hypertension occurrence and MAP change were not different between the two agents. Emergence time was higher for propofol (p = 0.008). |
| Bonhomme et al., 2009 [47] | Unspecified intracranial procedure | Propofol (n = 30) vs. sevoflurane (n = 31) | Propofol was associated with higher occurrence of intraoperative hypertension (p < 0.001) and sevoflurane was associated with higher occurrence of intraoperative hypotension (p = 0.015). |
| Ali et al., 2009 [48] | Resection of pituitary tumor | Propofol (n = 30), isoflurane (n = 30), sevoflurane (n = 30) | Emergence time was significantly longer with use of isoflurane (p < 0.001). Hypertension occurrence was higher in isoflurane than in propofol or sevoflurane, and higher in sevoflurane than propofol (p < 0.001). Hypotension was not difference between anesthetics (p = 0.36). |
| Bilotta et al., 2009 [49] | Craniotomy for resection of supratentorial lesion | Sevoflurane (n = 28) vs. desflurane (n = 28) | Significant delays in cognitive “awakening” for obese and overweight patients receiving sevoflurane-based anesthesia as compared to those receiving desflurane-based anesthesia as measured by post-operative short orientation memory concentration test scores at 15 and 30 min (p < 0.005, p < 0.005) as well as with the Rancho Los Amigos scale (p < 0.005) |
| Güneş et al., 2009 [71] | Craniotomy for resection of supratentorial lesion | Anesthetic maintenance with dexmedetomidine in addition to sevoflurane (n = 30), desflurane (n = 30), and isoflurane (n = 30) | MAP was elevated following intubation for all groups. Rates of eyes opening and responsiveness following verbal commands were lower in desflurane–dexmedetomidine than in other groups (p = 0.001). |
| Magni et al., 2009 [72] | Craniotomy for resection of supratentorial lesion | Anesthetic maintenance via sevoflurane (n = 60) vs. desflurane (n = 60) | Mean emergence was similar between the two groups, but extubation and recovery time were lower (p < 0.001) in the desflurane group. Hemodynamic stability differences were non-significant between the two groups. |
| Lauta et al., 2010 [50] | Craniotomy for resection of supratentorial lesion | Anesthetic maintenance via propofol (n = 153) vs. sevoflurane (n = 149) | Propofol was associated with a significantly longer emergence time to eyes opening (p < 0.014. Sevoflurane was associated with higher occurrence of hypotension (p < 0.0167). |
| Yildiz et al., 2011 [51] | Craniotomy for resection of supratentorial lesion | Anesthetic maintenance via desflurane (n = 35) vs. isoflurane (n = 35) | Heart rate was not different between the two agents. MAP was higher for desflurane (p < 0.05). Extubation time and eyes opening time was shorter for desflurane (p < 0.05). |
| Ghoneim et al., 2015 [52] | Craniotomy for resection of supratentorial tumors | Anesthetic maintenance via isoflurane (n = 20) vs. sevoflurane (n = 20) vs. desflurane (n = 20) | Emergence times were significantly shorter for desflurane or sevoflurane than with isoflurane in pediatric patients following a craniotomy for supratentorial tumors. |
| Hernandez et al., 2015 [53] | Craniotomy for hematoma | Anesthetic maintenance via propofol (n = 20) or sevoflurane (n = 20) | SSEPs amplitudes and latencies were not different between the two agents. TceMEPs amplitudes were higher for propofol (p < 0.05). Latencies were shorter in the propofol group (p < 0.05). |
| Goettel et al., 2016 [54] | Awake craniotomy for unspecified pathology | Dexmedetomidine (n = 25) vs. propofol (n = 25) | There were no differences in level of sedation (OAA) (p = 0.13). There were no differences in intraoperative hypertension (p = 0.60), hypotension (p = 0.50), or complications (p = 0.99). There was no difference in postoperative complications (p > 0.05). |
| Gokcek et al., 2016 [55] | Unspecified intracranial procedure | Anesthetic maintenance via sevoflurane (n = 25) vs. desflurane (n = 25) | Emergence time and time to eyes opening were higher with sevoflurane (p < 0.001). |
| Lin et al., 2016 [56] | Resection of supratentorial lesion | Anesthetic maintenance via propofol (n = 31) vs. dexmedetomidine (n = 31) | NIHSS-positive change was higher in propofol than dexmedetomidine (p < 0.001). Focal neurologic deficits were higher in propofol than dexmedetomidine (p < 0.05). |
| Rajan et al., 2016 [57] | Craniotomy or transsphenoidal approach for resection of brain tumor | Dexmedetomidine (n = 68) vs. remifentanil (n = 71) | Dexmedetomidine was associated with significantly lower postoperative MAP (p < 0.001). Dexmedetomidine was associated with significantly longer emergence time to open eyes (p < 0.001). |
| Thongrong et al., 2017 [58] | Craniotomy for unspecified pathology | Anesthetic maintenance via fentanyl (n = 30) vs. dexmedetomidine (n = 30) after propofol induction | Dexmedetomidine infusions reduced adverse effects, with signs of effectively controlled systolic blood pressure one minute prior to skull pin insertion (p < 0.05), as well as during skull pin insertion (p < 0.01) in comparison to fentanyl. Similarly, dexmedetomidine infusions were related to reduced adverse hypertensive and hypotensive responses in patients. |
| Bhardwaj et al., 2018 [59] | Surgical clipping for aneurysmal subarachnoid hemorrhage | Propofol (n = 35) vs. desflurane (n = 35) | There was no difference in blood loss (p < 0.05), hypotension (p < 0.05), hypertension (p < 0.05), or emergence time for eyes opening (p < 0.05). |
| Gracia et al., 2018 [60] | Unspecified intracranial procedure | Anesthetic induction via propofol (n = 20) vs. thiopental (n = 20) | There was no difference in heart rate (p > 0.05). MAP was significantly higher in thiopental groups (p < 0.05). Systolic and diastolic blood pressure was significantly lower in thiopental groups (p < 0.05). |
| Molina et al., 2018 [61] | Craniotomy for resection of tumor | Propofol–remifentanil (n = 105) for asleep sedation vs. conscious sedation with dexmedetomidine (n = 75) | Patients sedated with dexmedetomidine used less opiates, antihypertensive drugs, and had a lower postoperative duration and length of stay (all p < 0.001). |
| Xinyan et al., 2018 [62] | Awake craniotomy for unspecified pathology | Dexmedetomidine (n = 20), propofol (n = 20), etomidate (n = 20) | There was no significant difference in perioperative wake up duration (p > 0.05) and postoperative emergence time (p > 0.05). The rate of adverse events was lower in dexmedetomidine than propofol and etomidate (p < 0.05). The rate of adverse events was lower in propofol than etomidate (p < 0.05). |
| Khallaf et al., 2019 [63] | Craniotomy for hematoma | Anesthetic maintenance via propofol (n = 20) vs. dexmedetomidine (n = 20) | Tachycardia, bradycardia, and hypertension occurrences were not different between the two agents. IPP and CPP changes were not different between the two agents. Hypotension occurrences were higher in the propofol group (p = 0.024). |
| Preethi et al., 2021 [64] | Craniotomy for hematoma | Anesthetic maintenance via propofol (n = 45) vs. isoflurane | Change in heart rate, systolic blood pressure, diastolic blood pressure, and MAP were not different between the two agents. Brain relaxation was higher for propofol (p < 0.05). ICP was higher for isoflurane (p = 0.01). |
| Balasubramanian et al., 2021 [65] | Surgical clipping/endovascular coiling for aneurysmal subarachnoid hemorrhage | Propofol (n = 8) vs. isoflurane (n = 8) vs. sevoflurane (n = 8), vs. desflurane (n = 8) | There was no significant difference found between anesthetic on levels of CSF caspase-3 levels. |
| Authors and Year | Surgical Procedure | Comparison | Findings |
|---|---|---|---|
| Laureau et al., 1999 [66] | Posterior instrumentation for treatment of idiopathic scoliosis | Induction via intravenous propofol (n = 15) vs. midazolam (n = 15) | Cortical somatosensory-evoked potentials did not deteriorate in either the propofol or the midazolam induction groups. |
| Inoue et al., 2005 [67] | Cervical spine surgery for unspecified pathology | Anesthetic maintenance via fentanyl and propofol (n = 25) vs. fentanyl and <1% sevoflurane (n = 25) vs. sevoflurane (n = 25) | Perception of pain and bucking scores following emergence- were greater for patients exposed to sevoflurane versus propofol and fentanyl and fentanyl and sevoflurane in combination. |
| Kurt et al., 2005 [68] | Unspecified spinal procedure | Anesthetic maintenance via isoflurane (n = 12) vs. sevoflurane (n = 10) vs. desflurane (n = 10) | Sevoflurane and isoflurane administered via volatile anesthetics were able to achieve controlled hypotension in comparison to desflurane with systolic blood pressures outside the target range of 32% and 26% for isoflurane and sevoflurane, respectively, and 44% with desflurane. |
| Albertin et al., 2008 [69] | Lumbar spine surgery for unspecified pathology | Induction via sevoflurane (n = 14) or propofol (n = 14) as main anesthetic agents | Peripheral blood flow was greater in the propofol group before and during the hypotensive period, but had reduced blood loss and intra-operative bleeding as compared to the sevoflurane group (p < 0.005). |
| Turgut et al., 2008 [70] | Lumbar laminectomy | Pre-operative bolus and anesthetic maintenance via dexmedetomidine (n = 25) vs. fentanyl (n = 25) following induction via propofol as well as maintenance | Extubation and discharge times were similar between dexmedetomidine and fentanyl, but MAP values after intubation for those exposed to dexmedetomidine were higher for those exposed to fentanyl before and after extubation. Supplemental analgesia was required earlier for fentanyl group patients (34.8 +/− 1.35 min vs. 60.4 +/− 1.04 min). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nguyen, A.; Mandavalli, A.; Diaz, M.J.; Root, K.T.; Patel, A.; Casauay, J.; Perisetla, P.; Lucke-Wold, B. Neurosurgical Anesthesia: Optimizing Outcomes with Agent Selection. Biomedicines 2023, 11, 372. https://doi.org/10.3390/biomedicines11020372
Nguyen A, Mandavalli A, Diaz MJ, Root KT, Patel A, Casauay J, Perisetla P, Lucke-Wold B. Neurosurgical Anesthesia: Optimizing Outcomes with Agent Selection. Biomedicines. 2023; 11(2):372. https://doi.org/10.3390/biomedicines11020372
Chicago/Turabian StyleNguyen, Andrew, Akhil Mandavalli, Michael Joseph Diaz, Kevin Thomas Root, Aashay Patel, Jed Casauay, Priyanka Perisetla, and Brandon Lucke-Wold. 2023. "Neurosurgical Anesthesia: Optimizing Outcomes with Agent Selection" Biomedicines 11, no. 2: 372. https://doi.org/10.3390/biomedicines11020372