

MmpL3 Inhibition as a Promising Approach to Develop Novel Therapies against Tuberculosis: A Spotlight on SQ109, Clinical Studies, and Patents Literature
 , , , ,
, , , ,  , , ,
, , ,
Abstract
:1. Introduction
2. Mycobacterial Membrane Protein Large 3 (MmpL3)
3. Literature on MmpL3 Inhibitors
4. Clinical Studies on MmpL3 Inhibitors
5. SQ109
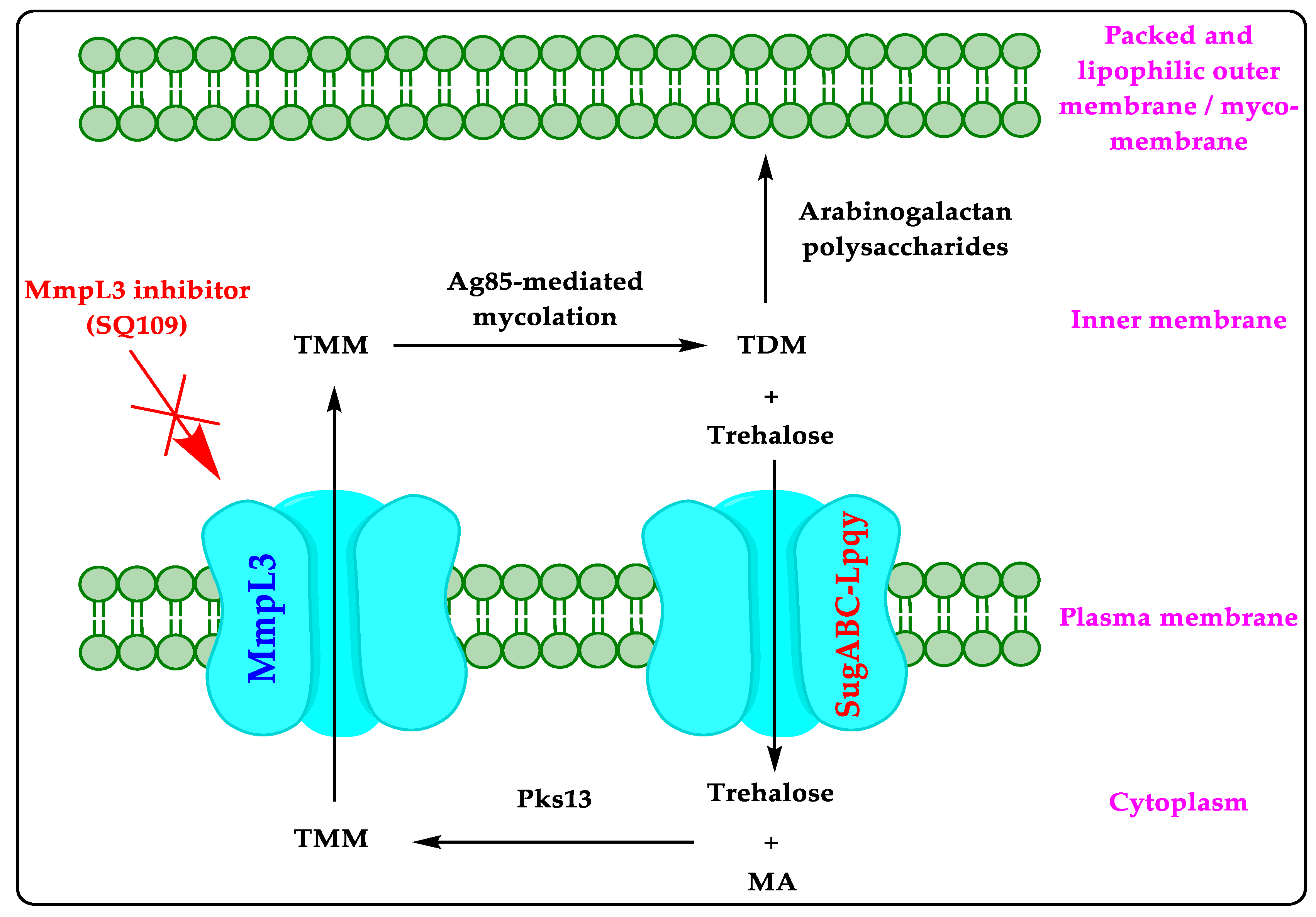
5.1. Mechanism of Action
5.2. Preclinical Studies
5.3. Clinical Studies on SQ109
6. Patent Searching and Analysis

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| S. No. | Patent/Patent Application Number (Assignee; Status) | Summary of the Claimed Invention |
|---|---|---|
| 1 | WO2021090283A1 (Foundation for Neglected Disease Research; No national phase entry) | A method of reducing the duration of TB treatment in patients suffering from DS-TB or DR-TB utilizing a combination of chloroquine/hydroxychloroquine and an anti-TB agent (SQ109, BNQ, macozinone, CFZ, etc.). The use of the claimed combination to reduce the relapse of TB in patients co-infected with HIV-1 is also claimed [51]. |
| 2 | WO2018191628A1 (University of California; No national phase entry) | An anti-TB pharmaceutical composition of CFZ, BZQ, and PZA that may optionally contain a therapeutically effective amount of SQ109 [52]. |
| 3 | WO2017191444A1 (UCL Business PLC; No national phase entry) | The polymersome (vesicles formed from amphiphilic block copolymers) composition of anti-TB drugs (INH, RIF, SQ109, etc.) with improved in vivo anti-TB activity over the free drug [53]. |
| 4 | US20170189474A1 (Cedars-Sinai Medical Center; Abandoned) | A method of treating Hirschsprung-associated fungal enterocolitis with an antifungal agent (SQ109, posaconazole, itraconazole, etc.) [54]. |
| 5 | US2017136102A1 (GangaGen Inc.; Abandoned) | A method of treating Mtb infection with a combination of an outer membrane acting biologic and an anti-TB drug (SQ109, INH, RIF, EMB, PZA, etc.), wherein the outer membrane acting biologic increases the permeability of the mycobacteria outer membrane for the anti-TB drug [55]. |
| 6 | EP2340022B1 (Pfizer; Invalid due to non-payment of fee) | A combination of sutezolid with at least two anti-TB drugs selected from the groups consisting of INH, RIF, PZA, CFZ, SQ109 etc., to treat TB [56]. |
| 7 | US2021069156A1 (Cornell University; Non-final action mailed) | A method of treating inflammatory disease (inflammatory bowel disease) in a subject diagnosed with one or more loss-or-function mutations in the CX3CR1 gene using a therapeutically effective amount of an anti-fungal agent (SQ109, voriconazole, fluconazole, etc.) [57]. |
| 8 | US10624893B2 (GlaxoSmithKline; Patented case) | A method for the treatment of TB using a therapeutically effective amount of GSK2556286 optionally in combination with other drugs (SQ109, INH, RIF, and PZA) [58]. |
| 9 | US9572809B2 (Spero Trinem; Patented case) | A method of controlling, treating, or reducing the advancement, severity or effects of a mycobacterium disease (TB) using a combination of VXc-486 and another antibiotic (SQ109, CFZ, sutezolid, PZA, and INH) [59]. |
7. Discussion
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Miggiano, R.; Rizzi, M.; Ferraris, D.M. Mycobacterium tuberculosis Pathogenesis, Infection Prevention and Treatment. Pathogens 2020, 9, 385. [Google Scholar] [CrossRef] [PubMed]
- Blumberg, H.M.; Ernst, J.D. The Challenge of Latent TB Infection. JAMA 2016, 316, 931–933. [Google Scholar] [CrossRef] [PubMed]
- Marais, B.J.; Gie, R.P.; Obihara, C.C.; Hesseling, A.C.; Schaaf, H.S.; Beyers, N. Well defined symptoms are of value in the diagnosis of childhood pulmonary tuberculosis. Arch. Dis. Child. 2005, 90, 1162–1165. [Google Scholar] [CrossRef] [PubMed]
- Global Tuberculosis Report 2021. Available online: https://www.who.int/publications/i/item/9789240037021 (accessed on 1 October 2022).
- Feske, M.L.; Teeter, L.D.; Musser, J.M.; Graviss, E.A. Giving TB wheels: Public transportation as a risk factor for tuberculosis transmission. Tuberculosis 2011, 91 (Suppl. 1), S16–S23. [Google Scholar] [CrossRef] [PubMed]
- Oommen, S.; Banaji, N. Laboratory Diagnosis of Tuberculosis: Advances in Technology and Drug Susceptibility Testing. Indian J. Med. Microbiol. 2017, 35, 323–331. [Google Scholar] [CrossRef]
- Hawn, T.R.; Day, T.A.; Scriba, T.J.; Hatherill, M.; Hanekom, W.A.; Evans, T.G.; Churchyard, G.; Kublin, J.G.; Bekker, L.-G.; Self, S.G. Tuberculosis Vaccines and Prevention of Infection. Microbiol. Mol. Biol. Rev. 2014, 78, 650–671. [Google Scholar] [CrossRef] [Green Version]
- Leibert, E.; Rom, W. New drugs and regimens for treatment of TB. Expert Rev. Anti-Infective Ther. 2010, 8, 801–813. [Google Scholar] [CrossRef]
- Rendon, A.; Tiberi, S.; Scardigli, A.; D’Ambrosio, L.; Centis, R.; Caminero, J.A.; Migliori, G.B. Classification of drugs to treat multidrug-resistant tuberculosis (MDR-TB): Evidence and perspectives. J. Thorac. Dis. 2016, 8, 2666–2671. [Google Scholar] [CrossRef] [Green Version]
- WHO Consolidated Guidelines on Tuberculosis: Module 4: Treatment: Drug-Resistant Tuberculosis Treatment. Available online: https://www.who.int/publications/i/item/9789240007048 (accessed on 1 October 2022).
- Prasad, R. Multidrug and extensively drug-resistant TB (M/XDR-TB): Problems and solutions. Indian J. Tuberc. 2010, 57, 180–191. [Google Scholar]
- Imran, M.; Alshrari, A.S.; Thabet, H.K.; Abida; Bakht, A. Synthetic molecules as DprE1 inhibitors: A patent review. Expert Opin. Ther. Patents 2021, 31, 759–772. [Google Scholar] [CrossRef]
- Imran, M.; Alam Khan, S.; Asdaq, S.M.B.; Almehmadi, M.; Abdulaziz, O.; Kamal, M.; Alshammari, M.K.; Alsubaihi, L.I.; Hussain, K.H.; Alharbi, A.S.; et al. An insight into the discovery, clinical studies, compositions, and patents of macozinone: A drug targeting the DprE1 enzyme of Mycobacterium tuberculosis. J. Infect. Public Health 2022, 15, 1097–1107. [Google Scholar] [CrossRef] [PubMed]
- Bolla, J.R. Targeting MmpL3 for anti-tuberculosis drug development. Biochem. Soc. Trans. 2020, 48, 1463–1472. [Google Scholar] [CrossRef] [PubMed]
- Su, C.-C.; Klenotic, P.A.; Bolla, J.R.; Purdy, G.E.; Robinson, C.V.; Yu, E.W. MmpL3 is a lipid transporter that binds trehalose monomycolate and phosphatidylethanolamine. Proc. Natl. Acad. Sci. USA 2019, 116, 11241–11246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Umare, M.D.; Khedekar, P.B.; Chikhale, R.V. Mycobacterial Membrane Protein Large 3 (MmpL3) Inhibitors: A Promising Approach to Combat Tuberculosis. Chem. Med. Chem. 2021, 16, 3136–3148. [Google Scholar] [CrossRef]
- Belardinelli, J.M.; Yazidi, A.; Yang, L.; Fabre, L.; Li, W.; Jacques, B.; Angala, S.K.; Rouiller, I.; Zgurskaya, H.I.; Sygusch, J.; et al. Structure-function profile of MmpL3, the essential mycolic acid transporter from Mycobacterium tuberculosis. ACS Infect. Dis. 2016, 2, 702–713. [Google Scholar] [CrossRef] [Green Version]
- Su, C.-C.; Klenotic, P.A.; Cui, M.; Lyu, M.; Morgan, C.E.; Yu, E.W. Structures of the mycobacterial membrane protein MmpL3 reveal its mechanism of lipid transport. PLoS Biol. 2021, 19, e3001370. [Google Scholar] [CrossRef]
- Xu, Z.; Meshcheryakov, V.A.; Poce, G.; Chng, S.-S. MmpL3 is the flippase for mycolic acids in mycobacteria. Proc. Natl. Acad. Sci. USA 2017, 114, 7993–7998. [Google Scholar] [CrossRef] [Green Version]
- Bajad, N.G.; Singh, S.K.; Singh, S.K.; Singh, T.D.; Singh, M. Indole: A promising scaffold for the discovery and development of potential anti-tubercular agents. Curr. Res. Pharmacol. Drug Discov. 2022, 3, 100119. [Google Scholar] [CrossRef]
- Addison, W.; Frederickson, M.; Coyne, A.G.; Abell, C. Potential therapeutic targets from Mycobacterium abscessus (Mab): Recently reported efforts towards the discovery of novel antibacterial agents to treat Mab infections. RSC Med. Chem. 2022, 13, 392–404. [Google Scholar] [CrossRef]
- Black, T.A.; Buchwald, U.K. The pipeline of new molecules and regimens against drug-resistant tuberculosis. J. Clin. Tuberc. Other Mycobact. Dis. 2021, 25, 100285. [Google Scholar] [CrossRef]
- Sethiya, J.P.; Sowards, M.A.; Jackson, M.; North, E.J. MmpL3 Inhibition: A New Approach to Treat Nontuberculous Mycobacterial Infections. Int. J. Mol. Sci. 2020, 21, 6202. [Google Scholar] [CrossRef] [PubMed]
- Shao, M.; McNeil, M.; Cook, G.M.; Lu, X. MmpL3 inhibitors as antituberculosis drugs. Eur. J. Med. Chem. 2020, 200, 112390. [Google Scholar] [CrossRef] [PubMed]
- Dey, R.; Nandi, S.; Samadder, A.; Saxena, A.; Saxena, A.K. Exploring the potential inhibition of candidate drug molecules for clinical investigation based on their docking or crystallographic analyses against M. tuberculosis enzyme targets. Curr. Top. Med. Chem. 2020, 20, 2662–2680. [Google Scholar] [CrossRef] [PubMed]
- Goldman, R.C. Target Discovery for New Antitubercular Drugs Using a Large Dataset of Growth Inhibitors from PubChem. Infect. Disord. Drug Targets 2020, 20, 352–366. [Google Scholar] [CrossRef]
- Saxena, A.K.; Singh, A. Mycobacterial tuberculosis Enzyme Targets and their Inhibitors. Curr. Top. Med. Chem. 2019, 19, 337–355. [Google Scholar] [CrossRef]
- Campaniço, A.; Moreira, R.; Lopes, F. Drug discovery in tuberculosis. New drug targets and antimycobacterial agents. Eur. J. Med. Chem. 2018, 150, 525–545. [Google Scholar] [CrossRef]
- Rayasam, G.V. MmpL3 a potential new target for development of novel anti-tuberculosis drugs. Expert Opin. Ther. Targets 2014, 18, 247–256. [Google Scholar] [CrossRef]
- NIH. Available online: https://clinicaltrials.gov/ (accessed on 1 October 2022).
- Heinrich, N.; Dawson, R.; du Bois, J.; Narunsky, K.; Horwith, G.; Phipps, A.J.; Nacy, C.A.; Aarnoutse, R.E.; Boeree, M.J.; Gil-lespie, S.H.; et al. Pan African Consortium for the Evaluation of Antituberculosis Antibiotics (PanACEA); Pan African Consortium for the Evaluation of Antituberculosis Antibiotics PanACEA. Early phase evaluation of SQ109 alone and in combination with rifampicin in pulmonary TB patients. J. Antimicrob. Chemother. 2015, 70, 1558–1566. [Google Scholar]
- Boeree, M.J.; Heinrich, N.; Aarnoutse, R.; Diacon, A.H.; Dawson, R.; Rehal, S.; Kibiki, G.S.; Churchyard, G.; Sanne, I.; E Ntinginya, N.; et al. High-dose rifampicin, moxifloxacin, and SQ109 for treating tuberculosis: A multi-arm, multi-stage randomised controlled trial. Lancet Infect. Dis. 2016, 17, 39–49. [Google Scholar] [CrossRef] [Green Version]
- Kayigire, X.A.; Friedrich, S.O.; van der Merwe, L.; Donald, P.R.; Diacon, A.H. Simultaneous staining of sputum smears for acid-fast and lipid-containing Myobacterium tuberculosis can enhance the clinical evaluation of antituberculosis treatments. Tuberculosis 2015, 95, 770–779. [Google Scholar] [CrossRef]
- Lee, R.E.; Protopopova, M.; Crooks, E.; Slayden, R.A.; Terrot, M.; Barry, C.E., 3rd. Combinatorial Lead Optimization of [1,2]-Diamines Based on Ethambutol as Potential Antituberculosis Preclinical Candidates. J. Comb. Chem. 2003, 5, 172–187. [Google Scholar] [CrossRef] [PubMed]
- Protopopova, M.; Hanrahan, C.; Nikonenko, B.; Samala, R.; Chen, P.; Gearhart, J.; Einck, L.; Nacy, C.A. Identification of a new antitubercular drug candidate, SQ109, from a combinatorial library of 1,2-ethylenediamines. J. Antimicrob. Chemother. 2005, 56, 968–974. [Google Scholar] [CrossRef] [PubMed]
- Bahuguna, A.; Rawat, D.S. An overview of new antitubercular drugs, drug candidates, and their targets. Med. Res. Rev. 2020, 40, 263–292. [Google Scholar] [CrossRef] [PubMed]
- SQ109. Available online: https://infectex.ru/en/products/sq-109/ (accessed on 1 October 2022).
- Sacksteder, K.A.; Protopopova, M.; Barry, C.E., 3rd; Andries, K.; Nacy, C.A. Discovery and development of SQ109: A new an-titubercular drug with a novel mechanism of action. Future Microbiol. 2012, 7, 823–837. [Google Scholar] [CrossRef] [Green Version]
- SQ109. Tuberculosis (Edinb) 2008, 88, 159–161. [CrossRef]
- Iqbal, I.; Bajeli, S.; Akela, A.; Kumar, A. Bioenergetics of Mycobacterium: An Emerging Landscape for Drug Discovery. Pathogens 2018, 7, 24. [Google Scholar] [CrossRef] [Green Version]
- Imran, M.; Alam Khan, S.; Alshammari, M.K.; Alreshidi, M.A.; Alreshidi, A.A.; Alghonaim, R.S.; Alanazi, F.A.; Alshehri, S.; Ghoneim, M.M.; Shakeel, F. Discovery, Development, Inventions, and Patent Trends on Mobocertinib Succinate: The First-in-Class Oral Treatment for NSCLC with EGFR Exon 20 Insertions. Biomedicines 2021, 9, 1938. [Google Scholar] [CrossRef]
- Imran, M.; Thabet, H.K.; Alaqel, S.I.; Alzahrani, A.R.; Abida, A.; Alshammari, M.K.; Kamal, M.; Diwan, A.; Asdaq, S.M.B.; Alshehri, S. The Therapeutic and Prophylactic Potential of Quercetin against COVID-19: An Outlook on the Clinical Studies, Inventive Compositions, and Patent Literature. Antioxidants 2022, 11, 876. [Google Scholar] [CrossRef]
- Imran, M.; Fatima, W.; Alzahrani, A.K.; Suhail, N.; Alshammari, M.K.; Alghitran, A.A.; Alshammari, F.N.; Ghoneim, M.M.; Alshehri, S.; Shakeel, F. Development of Therapeutic and Prophylactic Zinc Compositions for Use against COVID-19: A Glimpse of the Trends, Inventions, and Patents. Nutrients 2022, 14, 1227. [Google Scholar] [CrossRef]
- Imran, M.; Khan, S.A.; Abida; Alshrari, A.S.; Eltahir Mudawi, M.M.; Alshammari, M.K.; Harshan, A.A.; Alshammari, N.A. Small molecules as kinetoplastid specific proteasome inhibitors for leishmaniasis: A patent review from 1998 to 2021. Expert Opin. Ther. Pat. 2022, 32, 591–604. [Google Scholar] [CrossRef]
- Protopopova, M.N.; Lee, R.E.; Slayden, R.A.; Barry, C.E., 3rd; Einck, L. Anti-Tubercular Drug: Compositions and Methods. WO Patent Application No. 200,309,698,9A2, 27 November 2003. [Google Scholar]
- Protopopova, M.N.; Bogatcheva, E.; Einck, L.; Lee, R.E.; Slayden, R.A.; Barry, C.E., 3rd. Compositions and Methods for the Treatment of Infectious Diseases. U.S. Patent Application No. 826,889,4B2, 18 September 2012. [Google Scholar]
- Protopopova, M.N.; Lee, R.E.; Slayden, R.A.; Barry, C.E., 3rd; Bogatcheva, E.; Einck, L. Anti-Tubercular Drug: Compositions and Methods. U.S. Patent Application No. 784,272,9B2, 30 November 2010. [Google Scholar]
- Protopopova, M.N.; Lee, R.E.; Slayden, R.A.; Barry, C.E., 3rd; Bogatcheva, E.; Einck, L. Anti-Tubercular Drug: Compositions and Methods. U.S. Patent Application No. 745,622,2B2, 25 November 2008. [Google Scholar]
- Protopopova, M.N.; Einck, L.; Nikonenko, B.; Chen, P. Compositions and Methods for Treatment of Infectious Disease. U.S. Patent Application No. 820,291,0B2, 19 June 2012. [Google Scholar]
- Ho, C.M.; Clemens, D.L.; Clemens, B.Y.L.; Horwitz, M.A.; Vite, A.M.S.; Kee, T.; Ding, X. Multi-Drug Therapies for Tuberculosis Treatment. U.S. Patent Application No. 105,760,79B2, 3 March 2020. [Google Scholar]
- Singh, A.; Mishra, R.; Shandil, R.K.; Narayanan, S. Shortening Tuberculosis Therapy and Reducing Relapse by Co-Administering Chloroquine in TB and HIV-TB Co-Infected Conditions. WO Patent Application No. 202,109,028,3A1, 14 May 2021. [Google Scholar]
- Ho, C.M.; Horwitz, M.A.; Vite, A.M.S.; Ding, X.; Clemens, D.L.; Clemens, B.Y.L. Multi-Drug Therapies for Tuberculosis Treatment. WO Patent Application No. 201,819,162,8A1, 18 October 2018. [Google Scholar]
- Battaglia, G.; Rizzello, L.; Cecchin, D. Anti-Tuberculous Polymersomes. WO Patent Application No. 201,719,144,4A1, 9 November 2017. [Google Scholar]
- Frykman, P.K. Antifungal Therapy for the Treatment of Hirschsprung-Associated Enterocolitis. U.S. Patent Application No. 201,701,894,74A1, 6 July 2017. [Google Scholar]
- Sharma, U.K. Phage-Derived Compositions for Improved Mycobacterial Therapy. U.S. Patent Application No. 201,713,610,2A1, 18 May 2017. [Google Scholar]
- Brickner, S.J.; Nuermberger, E.; Stover, C.K. Combination Therapy for Tuberculosis. EP Patent Application No. 234,002,2B1, 20 November 2013. [Google Scholar]
- Iliev, I.; Leonardi, I. Theranostic Test for Antifungal Treatment of Inflammatory Diseases. U.S. Patent Application No. 202,106,915,6A1, 11 March 2021. [Google Scholar]
- Pages, L.B.; Aguirre, D.B.; Bates, R.H.; Pichel, J.C.; Provencio, J.E.; Pethe, K. Antituberculosis Agent. U.S. Patent Application No. 106,248,93B2, 21 April 2020. [Google Scholar]
- Locher, C.P.; Bennani, Y.L.; Grillot, A.L.; O’Dowd, H.; Perola, E.; Tiran, A.L.; Charifson, P.S. Combination Therapy to Treat Mycobacterium Diseases. U.S. Patent Application No. 957,280,9B2, 21 February 2017. [Google Scholar]
- North, J.; Pandya, A.N.; Jackson, M.; Li, W.; Juarrero, M.G. Chemical Probes to Identify Anti-Mycobacterial MmpL3 Inhibitors. U.S. Patent Application No. 202,033,189,7A1, 22 October 2020. [Google Scholar]
- Jiricek, J.; Kondreddi, R.R.; Smith, P.W. Indole Carboxamide Derivatives and Uses Thereof. U.S. Patent Application No. 944,703,9B2, 20 September 2016. [Google Scholar]
- Kaneko, T.; Fotouhi, N. Indole Carboxamide Compounds and Use Thereof for the Treatment of Mycobacterial Infections. WO Patent Application No. 202,106,231,9A1, 1 April 2021. [Google Scholar]
- North, J.; Jackson, M.C. Indole-Based Therapeutics. U.S. Patent Application No. 103,838,48B2, 20 August 2019. [Google Scholar]
- Reddy, D.S.; Chopra, S.; Shingare, R.D.; Ramana, S.R.; Dasgupta, A. Indole Compounds, Process for the Preparation and Use Thereof. WO Patent Application No. 201,922,046,1A1, 21 November 2019. [Google Scholar]
- Freundlich, J.S.; Alland, D.; Neiditch, M.B.; Inoyama, D.; Capodagli, G.; Kumar, P. Therapeutic Indoles. WO Patent Application No. 201,904,646,5A2, 7 March 2019. [Google Scholar]
- Liu, D.; Kuang, G.; Zhou, Y. 4-iodo-indole Compound and Preparation Method Thereof. CN Patent Application No. 112,028,811B, 22 March 2022. [Google Scholar]
- Liu, D.; Kuang, G.; Zhou, Y. 4-Bromoindole Compound and Preparation Method Thereof. CN Patent Application No. 112,028,812B, 22 March 2022. [Google Scholar]
- Bishai, W.R.; Lun, S.; Guo, H. Inhibitors of Drug-Resistant Mycobacterium Tuberculosis. WO Patent Application No. 201,516,448,2A1, 2 October 2015. [Google Scholar]
- Freundlich, J.S.; Alland, D.; Neiditch, M.B.; Kumar, P.; Capodagli, G.; Awasthi, D.; Ekins, S. Therapeutic Indazoles. U.S. Patent Application No. 111,865,49B2, 30 November 2021. [Google Scholar]
- Rao, Z.; Li, J.; Zhang, B.; Yang, H. Mmpl3 Inhibitors, Compositions and Uses Thereof. WO Patent Application No. 202,010,385,6A1, 28 May 2020. [Google Scholar]
- Oldfield, E.; Li, K. Anti-Microbial Compounds and Compositions. WO Patent Application No. 201,503,523,4A2, 12 March 2015. [Google Scholar]
- Liu, S.; Hickey, B.M.E.; Blivtao, J.R.; Xu, Y.; Huang, W.; Guo, X.; Wang, J. Application of Compound, Antibacterial Composition and Application of Antibacterial Composition. CN Patent Application No. 113,768,909A, 10 December 2021. [Google Scholar]
- Zhong, W.; Li, S.; Xiao, H.; Zhou, M. Ethylenediamine Compound and Use Thereof. U.S. Patent Application No. 202,208,952,1A1, 24 March 2022. [Google Scholar]
- Swarts, B.M. Trehalose Analogues. U.S. Patent Application No. 107,598,21B2, 1 September 2020. [Google Scholar]
- Joshua, D.; James, G.; Thale, J.; Mcfaddin, E.; Urs, O.; Xicheng, S.; Weng, C. Novel Anti-Mycobacterial Heterocyclic Amides. CN Patent Application No. 112,423,746A, 26 February 2021. [Google Scholar]
- Malwal, S.R.; Zimmerman, M.D.; Alvarez, N.; Sarathy, J.P.; Dartois, V.; Nacy, C.A.; Oldfield, E. Structure, In Vivo Detection, and Antibacterial Activity of Metabolites of SQ109, an Anti-Infective Drug Candidate. ACS Infect. Dis. 2021, 7, 2492–2507. [Google Scholar] [CrossRef] [PubMed]
- Imran, M.; Asdaq, S.M.B.; Alam Khan, S.; Meenakshi, D.U.; Alamri, A.S.; Alsanie, W.F.; Alhomrani, M.; Mohzari, Y.; Alrashed, A.; AlMotairi, M.; et al. Innovations and Patent Trends in the Development of USFDA Approved Protein Kinase Inhibitors in the Last Two Decades. Pharmaceuticals 2021, 14, 710. [Google Scholar] [CrossRef] [PubMed]




| Ref. No. | Year | Summary of the Review Article |
|---|---|---|
| [14] | 2020 | Reviews MmpL3 (physiological role, structure, and properties) and ligands/inhibitors of MmpL3 (AU1235, ICA38, SQ109, rimonabant, SPIRO, and NITD-349). |
| [16] | 2021 | Describes MmpL3 as a drug target, different chemical classes of MmpL3 inhibitors (derivatives of indole carboxamide, pyrrole/pyrazole, quinoline/quinolone, adamantane, benzimidazole, acetamide, and spiro-compound) and different ligands of MmpL3 like ICA38 (PDB ID: 6AJJ), rimonabant (PDB ID: 6AJI), SQ109 (PDB ID: 6AJG), and U1235 (PDB ID: 6AJH). |
| [20] | 2022 | Reviews indole derivatives as MmpL3 inhibitors (NITD-349, indolamide, adamantanol analogs, and indole-2-carboxamides) and inhibitors of other anti-TB drug targets (InhA, DprE1, KasA, chorismate mutase, DNA replication, DNA gyrase, dihydrofolate reductase). |
| [21] | 2022 | Describes MmpL3 as a promiscuous drug target and also spotlights the MmpL3 inhibitors of different chemical classes (adamantyl derivatives, piperidinol derivatives, and benzimidazole derivatives). It also highlights other anti-TB drug targets (TrmD, Ag85C, GyrB, and ClpC1). |
| [22] | 2021 | Briefly explains clinical study data (NCT01785186) of SQ109 (an MmpL3 inhibitor) and comments on the improved anti-TB activity of SQ109 with MDR regimens. |
| [23] | 2020 | Talks about MmpL3, the preclinical/clinical development of MmpL3 inhibitors (BM212, THPP, SQ109, Spiro, NITD-349, NITD-304, AU1235, C215, and HC2091), and different chemical classes of MmpL3 inhibitors (derivatives of indole, benzimidazole, benzothiazole, piperidine, 4-Thiophen-2-yloxane-4-carboxamide, benzofuran, quinoline/quinolone, naphthalene, acetamide, and pyrrole). |
| [24] | 2020 | Explores the current development of MmpL3 inhibitors (ethylenediamine derivatives, carboxamide derivatives, benzothiazole amides, adamantyl ureas, pyrroles and pyrazoles, benzimidazoles, spiropiperidines, and piperidinol), along with their structure-activity relationship (SAR) and challenges in developing them. It also provides the chemical structure of many MmpL3 inhibitors (AU1235, CRS400393, BM212, THPP, spiropiperidine, TBL-140, ICA38, HC2091, BM533, BM635, rimonabant, C215, PIPD1, NITD-349, NITD-304, and SQ109,). |
| [25] | 2020 | Surveys the new targets for TB, including MmpL3 and the chemistry of MmpL3 inhibitors (design and structural features) in clinical/preclinical trials. |
| [26] | 2020 | Identified lead compounds from PubChem database targeting MmpL3 and other anti-TB drug targets by high-throughput screening. |
| [27] | 2019 | Underlines the chemical structures and designs of MmpL3 inhibitors. |
| [28] | 2018 | Highlights the target validation, discovery, hit-optimization, and SAR of MmpL3 inhibitors of different chemical classes (ethylenediamine, adamantyl ureas, phenyl pyrroles, benzimidazoles, indole carboxamides, and spiropiperidines). |
| [29] | 2014 | Discloses MmpL3 as a validated target for developing anti-TB medications. It also discloses SQ109 and BM212 as MmpL3 inhibitors. |
| The Anti-TB Activity of SQ109 | The Anti-TB Activity of SQ109 Combinations in Mice | ||||
|---|---|---|---|---|---|
| Susceptibility Profile | Assay | MIC (μg/mL) | Drug Regimen | Log10 CFU in Lung | Log Decrease |
| H37Rv (pan-susceptible) | BACTEC | ≤0.2 | Two weeks | ||
| H37Rv (pan-susceptible) | Alamar | ≤0.39 | Untreated | 6.16 ± 0.02 | - |
| Erdman (pan-susceptible) | Alamar | ≤0.39 | INH + RIF + EMB | 4.64 ± 0.23 | 1.52 |
| EMB-resistant | Alamar | 0.78 | INH + RIF + SQ109 | 4.46 ± 0.12 | 1.70 |
| INH-resistant | Alamar | 0.78 | Four weeks | ||
| RIF-resistant | Alamar | ≤0.39 | Untreated | 6.42 ± 0.76 | - |
| XDR plus EMB-resistant | Microbroth | 0.20 | INH + RIF + EMB | 3.86 ± 0.14 | 2.56 |
| INH + RIF + SQ109 | 3.26 ± 0.12 | 3.16 | |||
| Title (Allocation; Intervention Model; Masking; Purpose) | Intervention and Active Comparator (AC) | NCT Number (Status; Phase; Number Enrolled; Results; Outcome Measures) | Sponsor/Collaborator (Location; Study Start Date (SSD); Study Completion Date (SCD); Last Update Date (LUD)) |
|---|---|---|---|
| Pharmacokinetics and early bactericidal activity (EBA) of SQ109 in adult subjects with pulmonary TB (Randomized; Parallel assignment; None (Open-label); Treatment of TB) | SQ109 monotherapy (75 mg, 150 mg, and 300 mg tablet daily) or a combination of RIF with SQ109 (RIF standard dose + 150 mg or 300 mg of SQ109) for 14 days; AC: RIF capsule (150 mg) | NCT01218217 (Completed; 2; 90; Not available; EBA of SQ109 monotherapy and combination therapy of SQ109 with RIF) | Michael Hoelscher and Sequella, Inc. (South Africa; November 2010: May 2012; 14 January 2013) |
| Evaluation of SQ109 plus PPI in urea breath test-positive volunteers (Not mentioned; Single group assignment; None (Open-label); Treatment of H. pylori infection) | SQ109 (300 mg) daily for two weeks; AC: Not mentioned | NCT01252108 (Withdrawn due to lack of funding: 2: 0: Not available; safety and efficacy of SQ109 against H. pylori infection in adult patients) | Sequella, Inc. (Not mentioned; March 2012; August 2015; 17 November 2015) |
| Evaluation of SQ109, high-dose RIF, and moxifloxacin in adults with smear-positive pulmonary TB in a MAMS design (Randomized: Single group assignment: None (Open-label): Treatment of TB) | Combinations of SQ109 (300 mg) with RIF (10 to 35 mg/kg), INH (75 mg), PZA (400 mg) and pyridoxine (25 mg); AC: Combination of INH, RIF, PZA, and EMB | NCT01785186 (Completed: 2: 365; Available; Two negative sputum cultures utilizing liquid media) | Michael Hoelscher and Sequella, Inc. (South Africa; April 2013; March 2015; 20 September 2017) |
| Escalating single-dose safety, tolerability, and pharmacokinetics of SQ109 in healthy volunteers (Randomized; Single group assignment; Quadruple (participant, care provider, investigator, outcomes assessor); Treatment of TB) | A single oral dose of SQ109 (10 mg, 20 mg, 50 mg, 100 mg, 200 mg, 300 mg, and the combination of fatty food with 300 mg of SQ109); AC: Placebo | NCT01585636 (Completed; 1; 62; Not available; Safety and pharmacokinetics of single dose of SQ109 for seven days) | Sequella, Inc. and Quintiles, Inc. (United States; September 2006; February 2007; 19 August 2013) |
| Dose escalation study of SQ109 in healthy adult volunteers (Randomized; Parallel assignment; Double (participant, investigator); Treatment of MDR-TB) | SQ109 (75 mg and 150 mg) daily for 14 days and SQ109 (150 mg) daily on days 1–5, 9, and 14; AC: Placebo | NCT00866190 (Completed; 1; 10; Not available; Safety and tolerability evaluation of SQ109) | National Institute of Allergy and Infectious Diseases (NIAID) (United States; April 2009; November 2009; 6 November 2011) |
| Phase IC study of safety and PK of SQ109 300 mg daily (Randomized; Parallel assignment; Triple (participant, investigator, outcomes assessor); Treatment of TB) | A single dose of SQ109 (300 mg) daily for two weeks; AC: Placebo | NCT01358162 (Completed: 1: 10: Not available: Safety and tolerability evaluation of SQ109) | NIAID (United States; November 2010; April 2011; 14 May 2013) |
| Effects of SQ109 on QTc interval in healthy subjects (Randomized; Crossover assignment; None (Open-label); Treatment of TB) | Oral SQ109 (300 mg or 450 mg daily) for seven days; AC: Placebo | NCT01874314 (Withdrawn due to undisclosed reason; 1; 0; Not available; Effect of SQ109 on QTc interval) | NIAID (United States; Not available; December 2015; 24 March 2014) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Imran, M.; Arora, M.K.; Chaudhary, A.; Khan, S.A.; Kamal, M.; Alshammari, M.M.; Alharbi, R.M.; Althomali, N.A.; Alzimam, I.M.; Alshammari, A.A.; et al. MmpL3 Inhibition as a Promising Approach to Develop Novel Therapies against Tuberculosis: A Spotlight on SQ109, Clinical Studies, and Patents Literature. Biomedicines 2022, 10, 2793. https://doi.org/10.3390/biomedicines10112793
Imran M, Arora MK, Chaudhary A, Khan SA, Kamal M, Alshammari MM, Alharbi RM, Althomali NA, Alzimam IM, Alshammari AA, et al. MmpL3 Inhibition as a Promising Approach to Develop Novel Therapies against Tuberculosis: A Spotlight on SQ109, Clinical Studies, and Patents Literature. Biomedicines. 2022; 10(11):2793. https://doi.org/10.3390/biomedicines10112793
Chicago/Turabian StyleImran, Mohd., Mandeep Kumar Arora, Anurag Chaudhary, Shah Alam Khan, Mehnaz Kamal, Manal Mutlaq Alshammari, Raghad Mohammad Alharbi, Nuha Abdullah Althomali, Ibrahim Mohammed Alzimam, Abdullah Ayed Alshammari, and et al. 2022. "MmpL3 Inhibition as a Promising Approach to Develop Novel Therapies against Tuberculosis: A Spotlight on SQ109, Clinical Studies, and Patents Literature" Biomedicines 10, no. 11: 2793. https://doi.org/10.3390/biomedicines10112793