
Clinical Significance of Preoperative Hematological Parameters in Patients with D2-Resected, Node-Positive Stomach Cancer

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Treatment
2.3. Preoperative Blood Cell Counts and Ratios
2.4. Evaluation and Statistical Analysis
2.5. Ethical Statement
3. Results
3.1. Patient Characteristics
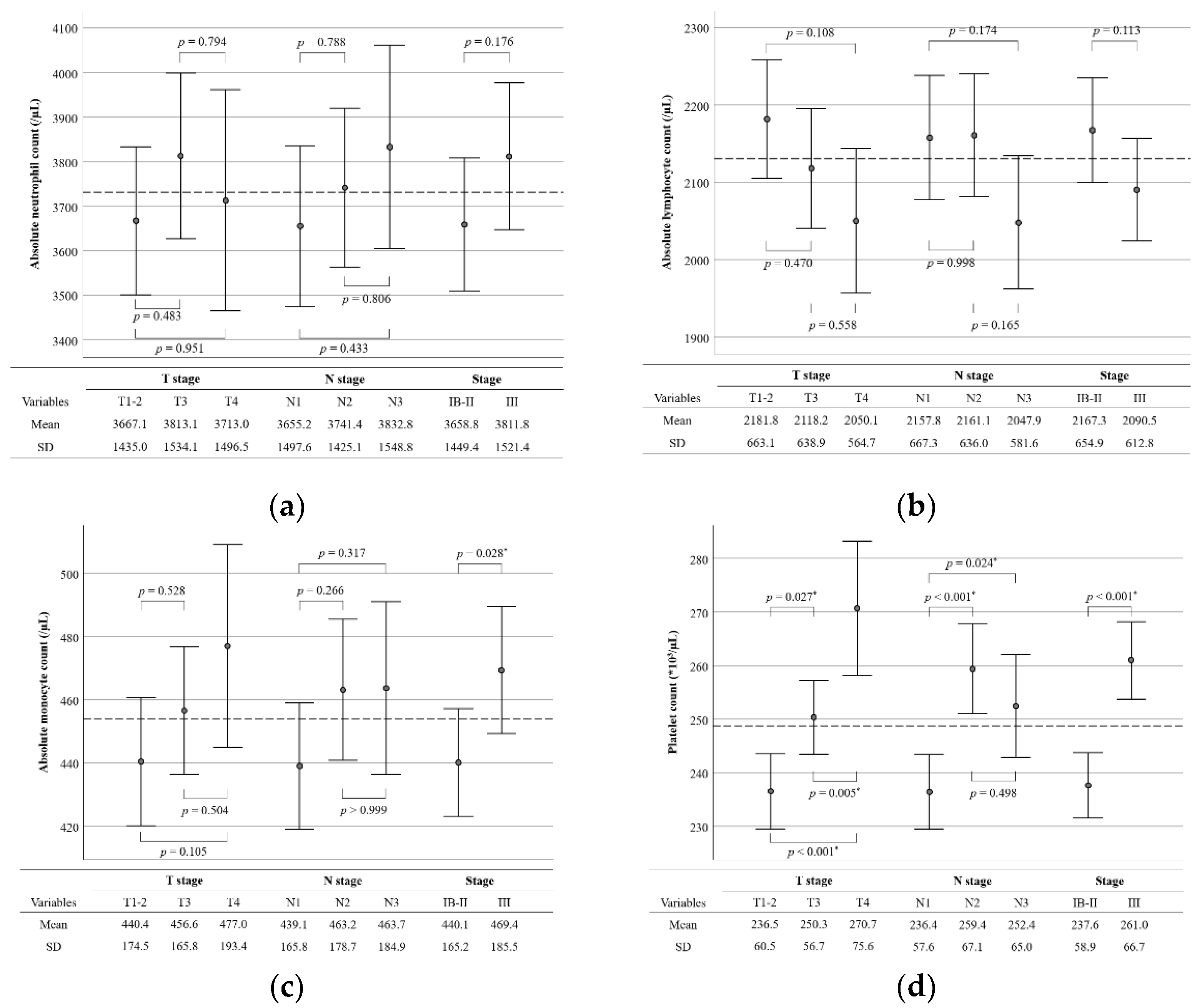
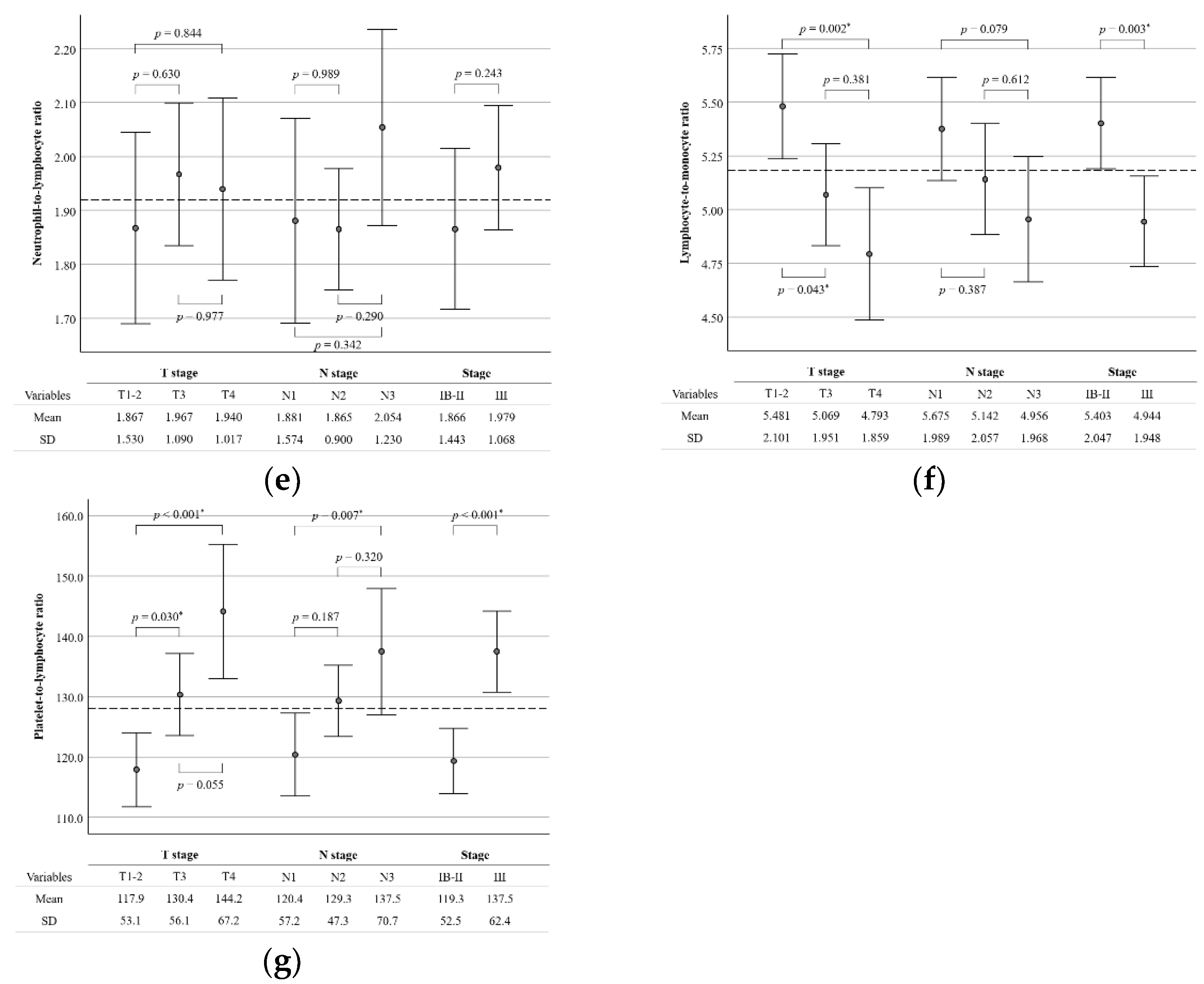
3.2. Preoperative Blood Cell Counts and Ratios
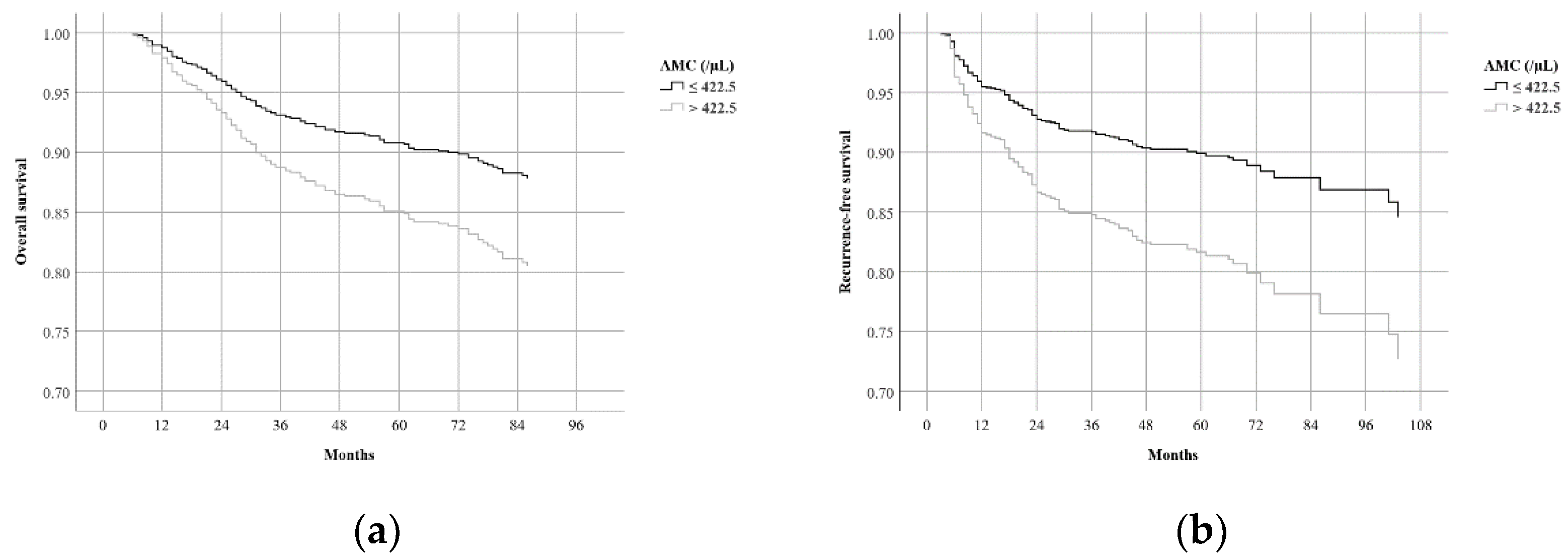
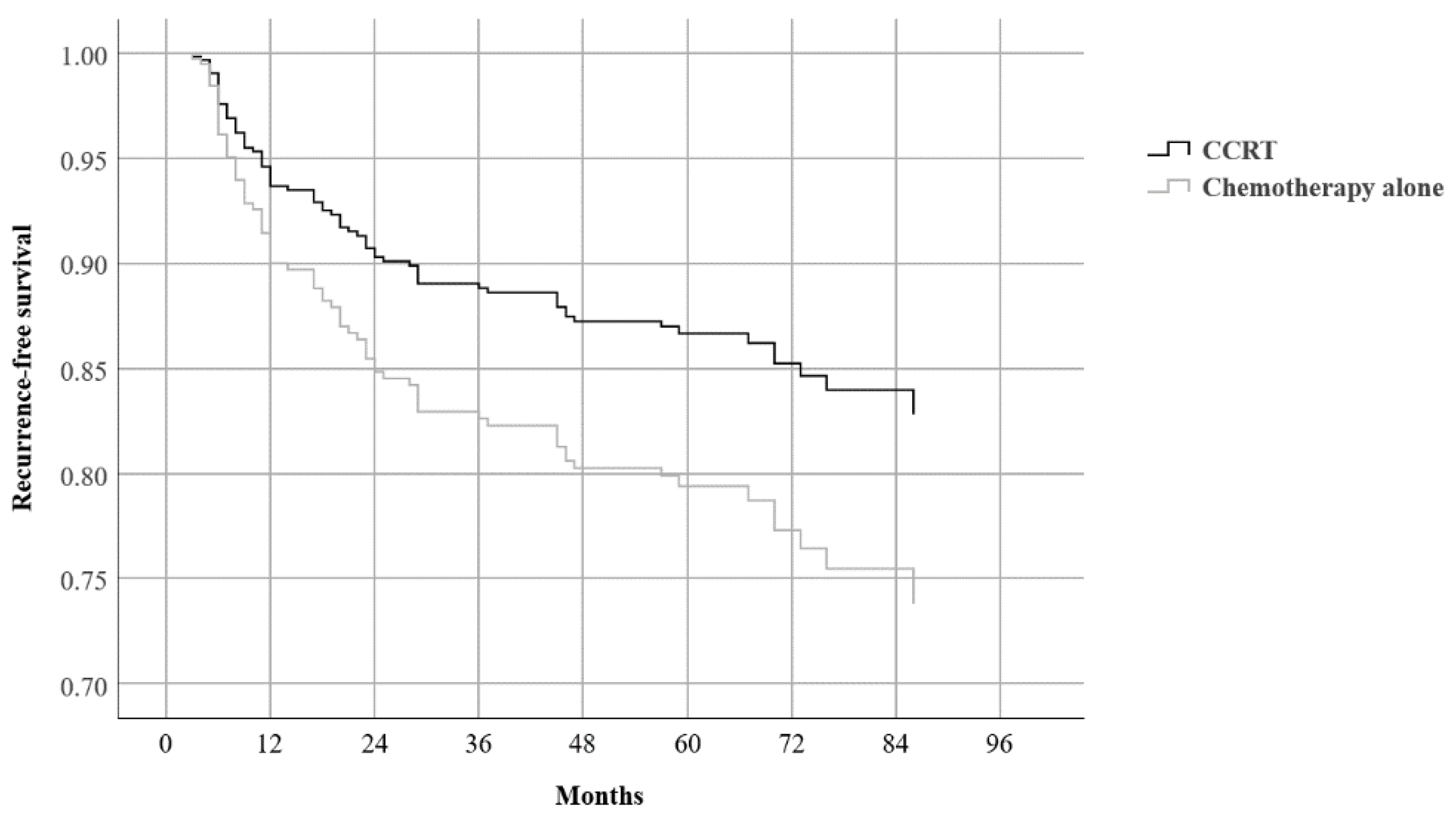
3.3. Survival Results
3.4. Subgroup Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Sakuramoto, S.; Sasako, M.; Yamaguchi, T.; Kinoshita, T.; Fujii, M.; Nashimoto, A.; Furukawa, H.; Nakajima, T.; Ohashi, Y.; Imamura, H.; et al. Adjuvant chemotherapy for gastric cancer with S-1, an oral fluoropyrimidine. N. Engl. J. Med. 2007, 357, 1810–1820. [Google Scholar] [CrossRef] [PubMed]
- Bang, Y.J.; Kim, Y.W.; Yang, H.K.; Chung, H.C.; Park, Y.K.; Lee, K.H.; Lee, K.W.; Kim, Y.H.; Noh, S.I.; Cho, J.Y.; et al. Adjuvant capecitabine and oxaliplatin for gastric cancer after D2 gastrectomy (CLASSIC): A phase 3 open-label, randomised controlled trial. Lancet 2012, 379, 315–321. [Google Scholar] [CrossRef]
- Sasako, M.; Sakuramoto, S.; Katai, H.; Kinoshita, T.; Furukawa, H.; Yamaguchi, T.; Nashimoto, A.; Fujii, M.; Nakajima, T.; Ohashi, Y. Five-year outcomes of a randomized phase III trial comparing adjuvant chemotherapy with S-1 versus surgery alone in stage II or III gastric cancer. J. Clin. Oncol. 2011, 29, 4387–4393. [Google Scholar] [CrossRef] [Green Version]
- Noh, S.H.; Park, S.R.; Yang, H.K.; Chung, H.C.; Chung, I.J.; Kim, S.W.; Kim, H.H.; Choi, J.H.; Kim, H.K.; Yu, W.; et al. Adjuvant capecitabine plus oxaliplatin for gastric cancer after D2 gastrectomy (CLASSIC): 5-year follow-up of an open-label, randomised phase 3 trial. Lancet Oncol. 2014, 15, 1389–1396. [Google Scholar] [CrossRef]
- Macdonald, J.S.; Smalley, S.R.; Benedetti, J.; Hundahl, S.A.; Estes, N.C.; Stemmermann, G.N.; Haller, D.G.; Ajani, J.A.; Gunderson, L.L.; Jessup, J.M.; et al. Chemoradiotherapy after surgery compared with surgery alone for adenocarcinoma of the stomach or gastroesophageal junction. N. Engl. J. Med. 2001, 345, 725–730. [Google Scholar] [CrossRef]
- Lee, J.; Lim, D.H.; Kim, S.; Park, S.H.; Park, J.O.; Park, Y.S.; Lim, H.Y.; Choi, M.G.; Sohn, T.S.; Noh, J.H.; et al. Phase III trial comparing capecitabine plus cisplatin versus capecitabine plus cisplatin with concurrent capecitabine radiotherapy in completely resected gastric cancer with D2 lymph node dissection: The ARTIST trial. J. Clin. Oncol. 2012, 30, 268–273. [Google Scholar] [CrossRef]
- Park, S.H.; Sohn, T.S.; Lee, J.; Lim, D.H.; Hong, M.E.; Kim, K.M.; Sohn, I.; Jung, S.H.; Choi, M.G.; Lee, J.H.; et al. Phase III Trial to Compare Adjuvant Chemotherapy with Capecitabine and Cisplatin Versus Concurrent Chemoradiotherapy in Gastric Cancer: Final Report of the Adjuvant Chemoradiotherapy in Stomach Tumors Trial, Including Survival and Subset Analyses. J. Clin. Oncol. 2015, 33, 3130–3136. [Google Scholar] [CrossRef] [Green Version]
- Yu, J.I.; Lim, D.H.; Ahn, Y.C.; Lee, J.; Kang, W.K.; Park, S.H.; Park, J.O.; Park, Y.S.; Lim, H.Y.; Kim, S.T.; et al. Effects of adjuvant radiotherapy on completely resected gastric cancer: A radiation oncologist’s view of the ARTIST randomized phase III trial. Radiother. Oncol. 2015, 117, 171–177. [Google Scholar] [CrossRef]
- Cupp, M.A.; Cariolou, M.; Tzoulaki, I.; Aune, D.; Evangelou, E.; Berlanga-Taylor, A.J. Neutrophil to lymphocyte ratio and cancer prognosis: An umbrella review of systematic reviews and meta-analyses of observational studies. BMC Med. 2020, 18, 360. [Google Scholar] [CrossRef]
- Nishijima, T.F.; Muss, H.B.; Shachar, S.S.; Tamura, K.; Takamatsu, Y. Prognostic value of lymphocyte-to-monocyte ratio in patients with solid tumors: A systematic review and meta-analysis. Cancer Treat. Rev. 2015, 41, 971–978. [Google Scholar] [CrossRef]
- Tan, D.; Fu, Y.; Tong, W.; Li, F. Prognostic significance of lymphocyte to monocyte ratio in colorectal cancer: A meta-analysis. Int. J. Surg. 2018, 55, 128–138. [Google Scholar] [CrossRef]
- Cao, W.; Yao, X.; Cen, D.; Zhi, Y.; Zhu, N.; Xu, L. The prognostic role of platelet-to-lymphocyte ratio on overall survival in gastric cancer: A systematic review and meta-analysis. BMC Gastroenterol. 2020, 20, 16. [Google Scholar] [CrossRef] [Green Version]
- Sherry, A.D.; von Eyben, R.; Newman, N.B.; Gutkin, P.; Mayer, I.; Horst, K.; Chakravarthy, A.B.; Rafat, M. Systemic Inflammation After Radiation Predicts Locoregional Recurrence, Progression, and Mortality in Stage II-III Triple-Negative Breast Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2020, 108, 268–276. [Google Scholar] [CrossRef]
- Liang, Z.G.; Zhang, F.; Li, Y.; Li, L.; Qu, S.; Su, F.; Yu, B.B.; Guan, Y.; Han, L.; Li, K.G.; et al. The Integration of the Pre-Treatment Neutrophil-to-Lymphocyte Ratio in the Eighth Edition of the AJCC Staging System for Nasopharynx Cancer. Front. Oncol. 2021, 11, 724467. [Google Scholar] [CrossRef]
- Eastern Rectal Cancer Response Collaborative, Ireland. A multicentre cohort study assessing the utility of routine blood tests as adjuncts to identify complete responders in rectal cancer following neoadjuvant chemoradiotherapy. Int. J. Colorectal. Dis. 2022, 37, 957–965. [Google Scholar] [CrossRef]
- Eo, W.K.; Jeong, D.W.; Chang, H.J.; Won, K.Y.; Choi, S.I.; Kim, S.H.; Chun, S.W.; Oh, Y.L.; Lee, T.H.; Kim, Y.O.; et al. Absolute monocyte and lymphocyte count prognostic score for patients with gastric cancer. World J. Gastroenterol. 2015, 21, 2668–2676. [Google Scholar] [CrossRef]
- Feng, F.; Zheng, G.; Wang, Q.; Liu, S.; Liu, Z.; Xu, G.; Wang, F.; Guo, M.; Lian, X.; Zhang, H. Low lymphocyte count and high monocyte count predicts poor prognosis of gastric cancer. BMC Gastroenterol. 2018, 18, 148. [Google Scholar] [CrossRef] [Green Version]
- Ma, J.Y.; Liu, Q. Clinicopathological and prognostic significance of lymphocyte to monocyte ratio in patients with gastric cancer: A meta-analysis. Int. J. Surg. 2018, 50, 67–71. [Google Scholar] [CrossRef]
- Kim, M.R.; Kim, A.S.; Choi, H.I.; Jung, J.H.; Park, J.Y.; Ko, H.J. Inflammatory markers for predicting overall survival in gastric cancer patients: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0236445. [Google Scholar] [CrossRef]
- Du, S.; Fang, Z.; Ye, L.; Sun, H.; Deng, G.; Wu, W.; Zeng, F. Pretreatment neutrophil-to-lymphocyte ratio predicts the benefit of gastric cancer patients with systemic therapy. Aging 2021, 13, 17638–17654. [Google Scholar] [CrossRef]
- Peng, X.; Zeng, W.; Tang, B.; He, A.; Zhang, M.; Luo, R. Utility of Pretreatment Blood Platelet-To-Lymphocyte Ratio in Prediction of Clinical Outcomes and Chemosensitivity in Patients with Advanced Gastric Cancer: A Meta-Analysis. Med. Sci. Monit. 2022, 28, e933449. [Google Scholar] [CrossRef]
- Schiefer, S.; Wirsik, N.M.; Kalkum, E.; Seide, S.E.; Nienhüser, H.; Müller, B.; Billeter, A.; Büchler, M.W.; Schmidt, T.; Probst, P. Systematic Review of Prognostic Role of Blood Cell Ratios in Patients with Gastric Cancer Undergoing Surgery. Diagnostics 2022, 12, 593. [Google Scholar] [CrossRef]
- Lee, J.S.; Kim, N.Y.; Na, S.H.; Youn, Y.H.; Shin, C.S. Reference values of neutrophil-lymphocyte ratio, lymphocyte-monocyte ratio, platelet-lymphocyte ratio, and mean platelet volume in healthy adults in South Korea. Medicine 2018, 97, e11138. [Google Scholar] [CrossRef]
- Xiong, S.; Dong, L.; Cheng, L. Neutrophils in cancer carcinogenesis and metastasis. J. Hematol. Oncol. 2021, 14, 173. [Google Scholar] [CrossRef]
- Yang, L.; Zhang, Y. Tumor-associated macrophages: From basic research to clinical application. J. Hematol. Oncol. 2017, 10, 58. [Google Scholar] [CrossRef] [Green Version]
- Palacios-Acedo, A.L.; Mège, D.; Crescence, L.; Dignat-George, F.; Dubois, C.; Panicot-Dubois, L. Platelets, Thrombo-Inflammation, and Cancer: Collaborating with the Enemy. Front. Immunol. 2019, 10, 1805. [Google Scholar] [CrossRef] [Green Version]
- Zhao, J.; Huang, W.; Wu, Y.; Luo, Y.; Wu, B.; Cheng, J.; Chen, J.; Liu, D.; Li, C. Prognostic role of pretreatment blood lymphocyte count in patients with solid tumors: A systematic review and meta-analysis. Cancer Cell Int. 2020, 20, 15. [Google Scholar] [CrossRef]
- Park, S.H.; Lim, D.H.; Sohn, T.S.; Lee, J.; Zang, D.Y.; Kim, S.T.; Kang, J.H.; Oh, S.Y.; Hwang, I.G.; Ji, J.H.; et al. A randomized phase III trial comparing adjuvant single-agent S1, S-1 with oxaliplatin, and postoperative chemoradiation with S-1 and oxaliplatin in patients with node-positive gastric cancer after D2 resection: The ARTIST 2 trial✩. Ann. Oncol. 2021, 32, 368–374. [Google Scholar] [CrossRef]
- Pietrantonio, F.; Miceli, R.; Raimondi, A.; Kim, Y.W.; Kang, W.K.; Langley, R.E.; Choi, Y.Y.; Kim, K.M.; Nankivell, M.G.; Morano, F.; et al. Individual Patient Data Meta-Analysis of the Value of Microsatellite Instability as a Biomarker in Gastric Cancer. J. Clin. Oncol. 2019, 37, 3392–3400. [Google Scholar] [CrossRef]
- McEachron, J.; Zhou, N.; Spencer, C.; Chatterton, C.; Shanahan, L.; Katz, J.; Naegele, S.; Singhal, P.K.; Lee, Y.-C. Adjuvant chemoradiation associated with improved outcomes in patients with microsatellite instability-high advanced endometrial carcinoma. Int. J. Gynecol. Cancer 2021, 31, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Vaes, R.D.W.; Hendriks, L.E.L.; Vooijs, M.; De Ruysscher, D. Biomarkers of Radiotherapy-Induced Immunogenic Cell Death. Cells 2021, 10, 930. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | All Patients (n = 692) | CCRT (n = 346) | Chemotherapy Alone (n = 346) | p-Value |
|---|---|---|---|---|
| Age | ||||
| ≤65 | 550 (79.5%) | 282 (81.5%) | 268 (77.5%) | 0.188 |
| >65 | 142 (20.5%) | 64 (18.5%) | 78 (22.5%) | |
| Sex | ||||
| Male | 417 (60.3%) | 216 (62.4%) | 201 (58.1%) | 0.244 |
| Female | 275 (39.7%) | 130 (37.6%) | 145 (41.9%) | |
| T stage | ||||
| T1–2 | 288 (41.6%) | 147 (42.5%) | 141 (40.8%) | 0.820 |
| T3 | 262 (37.9%) | 127 (36.7%) | 135 (39.0%) | |
| T4 | 142 (20.5%) | 72 (20.8%) | 70 (20.2%) | |
| N stage | ||||
| N1 | 266 (38.4%) | 132 (38.2%) | 134 (38.7%) | 0.788 |
| N2 | 248 (35.8%) | 128 (37.0%) | 120 (34.7%) | |
| N3 | 178 (25.7%) | 86 (24.9%) | 92 (26.6%) | |
| Stage | ||||
| IB–II | 362 (52.3%) | 182 (52.6%) | 180 (52.0%) | 0.879 |
| III | 330 (47.7%) | 164 (47.4%) | 166 (48.0%) | |
| Lauren classification | ||||
| Non-intestinal | 458 (66.2%) | 228 (65.9%) | 230 (66.5%) | 0.872 |
| Intestinal | 234 (33.8%) | 118 (34.1%) | 116 (33.5%) | |
| Surgical extent | ||||
| STG | 479 (69.2%) | 242 (69.96%) | 237 (68.5%) | 0.681 |
| TG | 213 (30.8%) | 104 (30.1%) | 109 (31.5%) | |
| ANC (/µL) | ||||
| ≤3448.5 | 346 (50.0%) | 172 (49.7%) | 174 (50.3%) | 0.879 |
| >3448.5 | 346 (50.0%) | 174 (50.3%) | 172 (49.7%) | |
| ALC (/µL) | ||||
| ≤2074.0 | 347 (50.1%) | 163 (47.1%) | 184 (53.2%) | 0.110 |
| >2074.0 | 345 (49.9%) | 183 (52.9%) | 162 (46.8%) | |
| AMC (/µL) | ||||
| ≤422.5 | 346 (50.0%) | 174 (50.3%) | 172 (49.7%) | 0.879 |
| >422.5 | 346 (50.0%) | 172 (49.7%) | 174 (50.3%) | |
| PC (×103/µL) | ||||
| ≤240.5 | 346 (50.0%) | 170 (49.1%) | 176 (50.9%) | 0.648 |
| >240.5 | 346 (50.0%) | 176 (50.9%) | 170 (49.1%) | |
| NLR | ||||
| ≤1.657 | 347 (50.1%) | 188 (54.3%) | 159 (46.7%) | 0.027 * |
| >1.657 | 345 (49.9%) | 158 (45.7%) | 187 (54.0%) | |
| LMR | ||||
| ≤4.956 | 346 (50.0%) | 159 (46.0%) | 187 (54.0%) | 0.033 * |
| >4.956 | 346 (50.0%) | 187 (54.0%) | 159 (46.0%) | |
| PLR | ||||
| ≤117.6 | 346 (50.0%) | 180 (52.0%) | 166 (48.0%) | 0.287 |
| >117.6 | 346 (50.0%) | 166 (48.0%) | 180 (52.0%) |
| Variables | 5-Year OS | p-Value | 5-Year RFS | p-Value |
|---|---|---|---|---|
| Age | ||||
| ≤65 | 87.5% | <0.001 * | 83.8% | <0.001 * |
| >65 | 67.5% | 67.8% | ||
| Sex | ||||
| Male | 81.8% | 0.255 | 78.9% | 0.123 |
| Female | 85.8% | 83.2% | ||
| T stage | ||||
| T1–2 | 94.8% | 94.0% | ||
| T3 | 81.7% | <0.001 * | 78.7% | <0.001 * |
| T4 | 63.3% | <0.001 * | 56.8% | <0.001 * |
| N stage | ||||
| N1 | 91.3% | 92.9% | ||
| N2 | 85.1% | 0.002 * | 80.7% | <0.001 * |
| N3 | 69.1% | <0.001 * | 61.4% | <0.001 * |
| Stage | ||||
| IB–II | 93.1% | 93.1% | ||
| III | 72.7% | <0.001 * | 66.6% | <0.001 * |
| Lauren classification | ||||
| Non-intestinal | 84.7% | 81.4% | ||
| Intestinal | 80.8% | 0.332 | 79.2% | 0.704 |
| Surgical extent | ||||
| STG | 87.0% | <0.001 * | 84.1% | 0.001 * |
| TG | 75.1% | 72.8% | ||
| Adjuvant treatment | ||||
| CCRT | 84.4% | 0.821 | 83.8% | 0.097 |
| Chemotherapy alone | 82.3% | 77.5% | ||
| ANC (/µL) | ||||
| ≤3448.5 | 82.7% | 0.791 | 81.5% | 0.567 |
| >3448.5 | 84.1% | 79.8% | ||
| ALC (/µL) | ||||
| ≤2074.0 | 84.1% | 0.622 | 82.3% | 0.344 |
| >2074.0 | 82.6% | 79.0% | ||
| AMC (/µL) | ||||
| ≤422.5 | 87.9% | 0.001 * | 86.7% | <0.001 * |
| >422.5 | 78.9% | 74.6% | ||
| PC (×103/µL) | ||||
| ≤240.5 | 85.3% | 0.211 | 83.7% | 0.058 |
| >240.5 | 81.5% | 77.5% | ||
| NLR | ||||
| ≤1.657 | 82.4% | 0.921 | 80.5% | 0.992 |
| >1.657 | 84.3% | 80.8% | ||
| LMR | ||||
| ≤4.956 | 80.0% | 0.008* | 76.6% | 0.013 * |
| >4.956 | 86.7% | 84.6% | ||
| PLR | ||||
| ≤117.6 | 84.7% | 0.1449 | 82.8% | 0.153 |
| >117.6 | 82.1% | 78.5% |
| OS | RFS | |||||
|---|---|---|---|---|---|---|
| Variables | HR | 95% CI | p-Value | HR | 95% CI | p-Value |
| Age | ||||||
| ≤65 | 1.000 | 1.000 | ||||
| >65 | 2.806 | 1.981–3.976 | <0.001 * | 2.089 | 1.462–2.983 | <0.001 |
| Sex | ||||||
| Male | 1.000 | 1.000 | ||||
| Female | 0.815 | 0.573–1.160 | 0.257 | 0.764 | 0.542–1.078 | 0.764 |
| T stage | <0.001 * | <0.001 * | ||||
| T1–2 | 1.000 | 1.000 | ||||
| T3 | 2.844 | 1.730–4.675 | <0.001 * | 3.229 | 1.974–5.281 | <0.001 * |
| T4 | 7.287 | 4.466–11.888 | <0.001 * | 7.658 | 4.712–12.447 | <0.001 * |
| N stage | <0.001 * | <0.001 * | ||||
| N1 | 1.000 | 1.000 | ||||
| N2 | 2.105 | 1.293–3.426 | 0.003 * | 2.933 | 1.769–4.861 | <0.001 * |
| N3 | 4.599 | 2.895–7.304 | <0.001 * | 6.249 | 3.830–10.196 | <0.001 * |
| Stage | <0.001 * | <0.001 * | ||||
| IB–II | 1.000 | 1.000 | ||||
| III | 4.518 | 3.010–6.782 | <0.001 * | 5.081 | 3.393–7.607 | <0.001 * |
| Lauren classification | 0.498 | |||||
| Intestinal | 1.000 | 1.000 | ||||
| Non-intestinal | 0.842 | 0.595–1.193 | 0.333 | 0.935 | 0.662–1.321 | 0.705 |
| Surgical extent | ||||||
| STG | 1.000 | 1.000 | ||||
| TG | 2.204 | 1.572–3.090 | <0.001 * | 1.773 | 1.273–2.470 | 0.001 * |
| Adjuvant treatment | ||||||
| CCRT | 1.000 | 1.000 | ||||
| Chemotherapy alone | 1.040 | 0.742–1.457 | 0.821 | 1.319 | 0.949–1.835 | 0.100 |
| ANC (/µL) | ||||||
| ≤3448.5 | 1.000 | 1.000 | ||||
| >3448.5 | 1.047 | 0.747–1.467 | 0.792 | 1.100 | 0.792–1.527 | 0.568 |
| ALC (/µL) | ||||||
| ≤2074.0 | 0.919 | 0.655–1.288 | 0.623 | 0.854 | 0.615–1.186 | 0.347 |
| >2074.0 | 1.000 | 1.000 | ||||
| AMC (/µL) | ||||||
| ≤422.5 | 1.000 | 1.000 | ||||
| >422.5 | 1.802 | 1.270–2.555 | 0.001 * | 2.023 | 1.434–2.853 | <0.001 * |
| PC (× 103/µL) | ||||||
| ≤240.5 | 1.000 | 1.000 | ||||
| >240.5 | 1.241 | 0.884–1.741 | 0.213 | 1.374 | 0.987–1.913 | 0.060 |
| NLR | ||||||
| ≤1.657 | 1.000 | 1.000 | ||||
| >1.657 | 0.983 | 0.701–1.378 | 0.921 | 0.998 | 0.719–1.386 | 0.992 |
| LMR | ||||||
| ≤4.956 | 1.583 | 1.122–2.234 | 0.009 * | 1.514 | 1.085–2.113 | 0.015 * |
| >4.956 | 1.000 | 1.000 | ||||
| PLR | ||||||
| ≤117.6 | 1.000 | 1.000 | ||||
| >117.6 | 1.282 | 0.913–1.801 | 0.151 | 1.270 | 0.913–1.766 | 0.155 |
| OS | RFS | |||||
|---|---|---|---|---|---|---|
| Variables | HR | 95% CI | p-Value | HR | 95% CI | p-Value |
| Age | ||||||
| ≤65 | 1.000 | 1.000 | ||||
| >65 | 2.190 | 1.531–3.132 | <0.001 | 1.444 | 1.001–2.084 | 0.049 |
| T stage | <0.001 | <0.001 | ||||
| T1–2 | 1.000 | 1.000 | ||||
| T3 | 2.099 | 1.261–3.492 | 0.004 | 2.509 | 1.521–4.141 | <0.001 |
| T4 | 4.346 | 2.587–7.300 | <0.001 | 4.717 | 2.829–7.865 | <0.001 |
| N stage | 0.003 | <0.001 | ||||
| N1 | 1.000 | 1.000 | ||||
| N2 | 1.770 | 1.081–2.896 | 0.023 | 2.496 | 1.500–4.155 | <0.001 |
| N3 | 2.340 | 1.436–3.814 | 0.001 | 3.591 | 2.150–5.999 | <0.001 |
| Surgical extent | ||||||
| STG | 1.000 | |||||
| TG | 1.548 | 1.094–2.191 | 0.014 | |||
| AMC (/µL) | ||||||
| ≤422.5 | 1.000 | 1.000 | ||||
| >422.5 | 1.674 | 1.180–2.376 | 0.004 | 1.908 | 1.650–2.695 | <0.001 |
| Variables | Hazard Ratio | 95% Confidence Interval | p-Value |
|---|---|---|---|
| T stage | <0.001 | ||
| T1–2 | 1.000 | ||
| T3 | 2.285 | 1.202–4.344 | 0.012 |
| T4 | 4.315 | 2.223–8.375 | <0.001 |
| N stage | 0.001 | ||
| N1 | 1.000 | ||
| N2 | 1.991 | 1.046–3.790 | 0.036 |
| N3 | 3.374 | 1.751–6.499 | <0.001 |
| Adjuvant treatment | |||
| CCRT | 0.620 | 0.393–0.980 | 0.040 |
| Chemotherapy alone | 1.000 |
| Author | Inclusion | Hazard Ratio (95% Confidence Interval) | Cut-Off |
|---|---|---|---|
| Kim et al. (2020) [20] | 41 studies with 18,348 stage I–IV patients | High NLR, 1.605 (1.449–1.779) for OS | 1.44–5.00 |
| Du et al. (2021) [21] | 36 studies with 8614 patients, inoperable | High NLR, 1.78 (1.59–1.99) for OS; 1.63 (1.39–1.91) for progression-free survival | 0.4–5.0 (3.0 in 10 studies) |
| Ma et al. (2018) [19] | 6 studies with 4908 stage I–IV patients | High LMR, 0.66 (0.54–0.82) for OS; not for DFS 0.71 (0.38–1.32) | 3.15–5.15 |
| Cao et al. (2020) [13] | 28 studies with 15,617 stage I–IV patients | High PLR, 1.19 (1.08–1.33) for OS | 108–305 |
| Peng et al. (2022) [22] | 17 studies with 3499 stage III–IV patients | High PLR, 1.429 (1.246–1.639) for OS; 1.47 (1.14–1.88) for DFS | 107.7–284 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, J.S.; Yu, J.I.; Lim, D.H.; Nam, H.; Kim, Y.I.; Lee, J.; Kang, W.K.; Park, S.H.; Kim, S.T.; Hong, J.Y.; et al. Clinical Significance of Preoperative Hematological Parameters in Patients with D2-Resected, Node-Positive Stomach Cancer. Biomedicines 2022, 10, 1565. https://doi.org/10.3390/biomedicines10071565
Park JS, Yu JI, Lim DH, Nam H, Kim YI, Lee J, Kang WK, Park SH, Kim ST, Hong JY, et al. Clinical Significance of Preoperative Hematological Parameters in Patients with D2-Resected, Node-Positive Stomach Cancer. Biomedicines. 2022; 10(7):1565. https://doi.org/10.3390/biomedicines10071565
Chicago/Turabian StylePark, Jun Su, Jeong Il Yu, Do Hoon Lim, Heerim Nam, Young Il Kim, Jeeyun Lee, Won Ki Kang, Se Hoon Park, Seung Tae Kim, Jung Yong Hong, and et al. 2022. "Clinical Significance of Preoperative Hematological Parameters in Patients with D2-Resected, Node-Positive Stomach Cancer" Biomedicines 10, no. 7: 1565. https://doi.org/10.3390/biomedicines10071565