
The Impact of Metabolic Syndrome and Obesity on the Evolution of Diastolic Dysfunction in Apparently Healthy Patients Suffering from Post-COVID-19 Syndrome

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Study Protocol, Clinical and Laboratory Assessments
2.3. Echocardiographic Assessments
- (a)
- Left ventricular (LV) systolic performance, was evaluated in 2D mode, from the apical 2-, 3-, and 4-chamber views, by determining the LV ejection fraction (LVEF) using the modified Simpson rule (values less than 50% were considered abnormal) and the lateral mitral annular plane systolic excursion (MAPSE) measure (values under 10 mm were considered pathological). LV global longitudinal strain (LV-GLS) was quantified from apical 2-, 3-, and 4-chamber views, the region of interest being automatically generated and, after tracing the LV endocardial border, manual corrections were performed to fit the thickness of the LV myocardial wall [18,25,26]. Values under −18% suggested impaired LV systolic function (LV-SF).
- (b)
- Right ventricular (RV) function (RVF) was determined from an apical 4-chamber view by measuring tricuspid annular plane systolic excursion (TAPSE), assessed in M-mode, at the level of the lateral tricuspid valve annulus, by calculating the fractional area change and by determining in apical 4-chamber view the RV global longitudinal strain (RV-GLS), RVD being certified by either TAPSE < 17 mm, FAC ˂ 35%, and/or RV-GLS < −28% [18,26].
- (c)
- To appreciate the systolic pressure in the pulmonary artery (sPAP), we determined the peak tricuspid regurgitation velocity (TRV) in continuous-wave Doppler, from the apical window at the level of the tricuspid valves, and we employed Bernouli’s equation to calculate the pressure gradient, to which we added the estimated right atrial pressure, based on the inferior vena cava diameter, and its respiratory variations. We considered that sPAP values of ≥35 mmHg at rest indicated pulmonary hypertension (PH), with severities ranging from mild (35–44 mmHg) to moderate (45–60 mmHg) to severe (>60 mmHg) [23,27].
- (d)
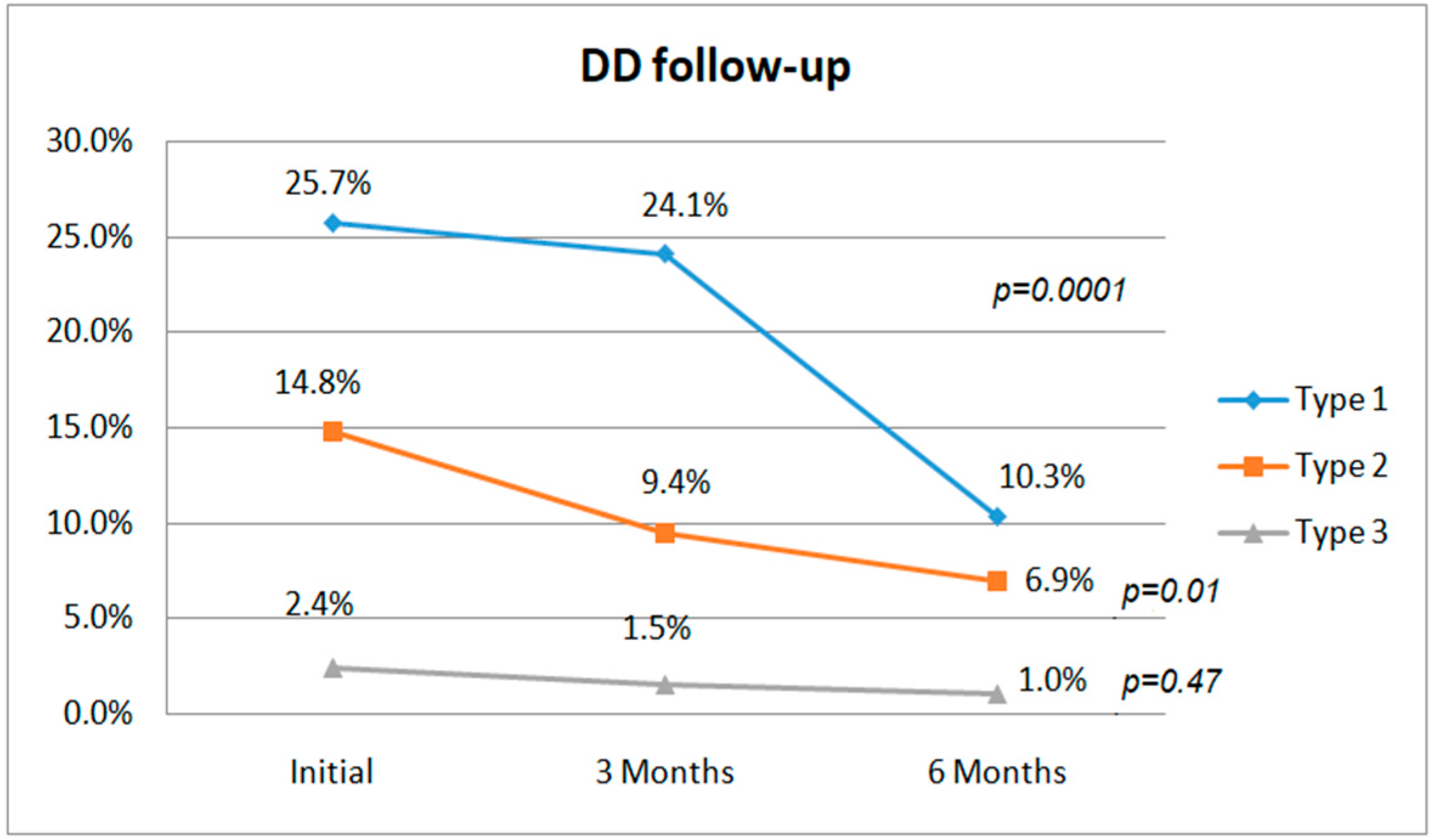
- To evaluate DD, the apical 4-chamber view was employed to determine the left atrial volume index (LAVI), then pulsed Doppler was used to register the peak early diastolic velocity (E), and the late diastolic velocity (A) at the level of the mitral valve annulus, and, subsequently, the E/A ratio was calculated. Afterwards, tissue Doppler imaging (TDI) was employed to record the early (e’) and the late diastolic velocity (a’) at the level of the septal and lateral mitral annulus, and an average E/e’ ratio was calculated. According to guidelines [24], DD is classified as mild or grade 1 (impaired relaxation pattern), moderate or grade 2, and severe (restrictive filling) or grade 3. An E/A ratio ≤ 0.8 and E < 50 cm/s defines DD of type 1, while an E/A ratio over 2 indicates a DD of type 3 DD. In the case of an E/A ratio ≤ 0.8 but with an E of over 50 cm/s, or an E/A ratio between 0.8 and 2, type 2 DD was presumed and certified if at least two of the following criteria were fulfilled: an average E/e’ > 14, LAVI of over 34 mL/m2, and/or a TRV over 2.8 m/s. If only one of these three criteria was fulfilled, a DD of type 1 was diagnosed [24].
2.4. Statistical Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239. [Google Scholar] [CrossRef] [PubMed]
- Bovolini, A.; Garcia, J.; Andrade, M.A.; Duarte, J.A. Metabolic Syndrome Pathophysiology and Predisposing Factors. Int. J. Sports Med. 2021, 42, 199–214. [Google Scholar] [CrossRef] [PubMed]
- Batabyal, R.; Freishtat, N.; Hill, E.; Rehman, M.; Freishtat, R.; Koutroulis, I. Metabolic Dysfunction and Immunometabolism in COVID-19 Pathophysiology and Therapeutics. Int. J. Obes. 2021, 45, 1163–1169. [Google Scholar] [CrossRef] [PubMed]
- Bornstein, S.R.; Rubino, F.; Ludwig, B.; Rietzsch, H.; Schwarz, P.E.H.; Rodionov, R.N.; Khunti, K.; Hopkins, D.; Birkenfeld, A.L.; Boehm, B.; et al. Consequences of the COVID-19 Pandemic for Patients with Metabolic Diseases. Nat. Metab. 2021, 3, 289–292. [Google Scholar] [CrossRef]
- de Siqueira, J.V.V.; Almeida, L.G.; Zica, B.O.; Brum, I.B.; Barceló, A.; de Siqueira Galil, A.G. Impact of Obesity on Hospitalizations and Mortality, Due to COVID-19: A Systematic Review. Obes. Res. Clin. Pract. 2020, 14, 398–403. [Google Scholar] [CrossRef]
- Martínez-Colón, G.J.; Ratnasiri, K.; Chen, H.; Jiang, S.; Zanley, E.; Rustagi, A.; Verma, R.; Chen, H.; Andrews, J.R.; Mertz, K.D.; et al. SARS-CoV-2 Infects Human Adipose Tissue and Elicits an Inflammatory Response Consistent with Severe COVID-19. bioRxiv 2021. [Google Scholar] [CrossRef]
- Oronsky, B.; Larson, C.; Hammond, T.C.; Oronsky, A.; Kesari, S.; Lybeck, M.; Reid, T.R. A Review of Persistent Post-COVID Syndrome (PPCS). Clin. Rev. Allerg. Immunol. 2021, 1–9. [Google Scholar] [CrossRef]
- Kalligeros, M.; Shehadeh, F.; Mylona, E.K.; Benitez, G.; Beckwith, C.G.; Chan, P.A.; Mylonakis, E. Association of Obesity with Disease Severity Among Patients with Coronavirus Disease 2019. Obesity 2020, 28, 1200–1204. [Google Scholar] [CrossRef]
- Tessier, C.M.; Kokkinos, A.; Mingrone, G.; Koliaki, C.; Zierath, J.R.; Mantzoros, C.S. COVID-19 Editorial: Mechanistic Links and Therapeutic Challenges for Metabolic Diseases One Year into the COVID-19 Pandemic. Metabolism 2021, 119, 154769. [Google Scholar] [CrossRef]
- Reiterer, M.; Rajan, M.; Gómez-Banoy, N.; Lau, J.D.; Gomez-Escobar, L.G.; Ma, L.; Gilani, A.; Alvarez-Mulett, S.; Sholle, E.T.; Chandar, V.; et al. Hyperglycemia in Acute COVID-19 Is Characterized by Insulin Resistance and Adipose Tissue Infectivity by SARS-CoV-2. Cell Metab. 2021, 33, 2174–2188.e5. [Google Scholar] [CrossRef]
- Freaney, P.M.; Shah, S.J.; Khan, S.S. COVID-19 and Heart Failure with Preserved Ejection Fraction. JAMA 2020, 324, 1499. [Google Scholar] [CrossRef] [PubMed]
- Xiong, T.-Y.; Redwood, S.; Prendergast, B.; Chen, M. Coronaviruses and the Cardiovascular System: Acute and Long-Term Implications. Eur. Heart J. 2020, 41, 1798–1800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, R.; Wang, H.; Ma, F.; Cui, G.; Peng, L.; Li, C.; Zeng, H.; Marian, A.J.; Wang, D. Widespread Myocardial Dysfunction in COVID-19 Patients Detected by Myocardial Strain Imaging Using 2-D Speckle-Tracking Echocardiography. Acta Pharm. Sin. 2021, 42, 1567–1574. [Google Scholar] [CrossRef]
- Asadi-Pooya, A.A.; Akbari, A.; Emami, A.; Lotfi, M.; Rostamihosseinkhani, M.; Nemati, H.; Barzegar, Z.; Kabiri, M.; Zeraatpisheh, Z.; Farjoud-Kouhanjani, M.; et al. Risk Factors Associated with Long COVID Syndrome: A Retrospective Study. Iran. J. Med. Sci. 2021, 46, 428–436. [Google Scholar] [CrossRef] [PubMed]
- Madjid, M.; Safavi-Naeini, P.; Solomon, S.D.; Vardeny, O. Potential Effects of Coronaviruses on the Cardiovascular System: A Review. JAMA Cardiol. 2020, 5, 831. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chung, M.K.; Zidar, D.A.; Bristow, M.R.; Cameron, S.J.; Chan, T.; Harding, C.V.; Kwon, D.H.; Singh, T.; Tilton, J.C.; Tsai, E.J.; et al. COVID-19 and Cardiovascular Disease. Circ. Res. 2021, 128, 1214–1236. [Google Scholar] [CrossRef]
- 2020 Research Reveals Heart Complications in COVID-19 Patients. Available online: https://www.cidrap.umn.edu/news-perspective/2020/07/research-reveals-heart-complications-covid-19-patients (accessed on 31 October 2020).
- Szekely, Y.; Lichter, Y.; Taieb, P.; Banai, A.; Hochstadt, A.; Merdler, I.; Gal Oz, A.; Rothschild, E.; Baruch, G.; Peri, Y.; et al. Spectrum of Cardiac Manifestations in COVID-19: A Systematic Echocardiographic Study. Circulation 2020, 142, 342–353. [Google Scholar] [CrossRef]
- Becker, R.C. Anticipating the Long-Term Cardiovascular Effects of COVID-19. J. Thromb. Thrombolysis. 2020, 50, 512–524. [Google Scholar] [CrossRef]
- Iqubal, A.; Iqubal, M.K.; Hoda, F.; Najmi, A.K.; Haque, S.E. COVID-19 and Cardiovascular Complications: An Update from the Underlying Mechanism to Consequences and Possible Clinical Intervention. Expert Rev. Anti Infect. Ther. 2021, 19, 1083–1092. [Google Scholar] [CrossRef]
- del Rio, C.; Collins, L.F.; Malani, P. Long-Term Health Consequences of COVID-19. JAMA 2020, 324, 1723. [Google Scholar] [CrossRef]
- Carfì, A.; Bernabei, R.; Landi, F. For the Gemelli Against COVID-19 Post-Acute Care Study Group Persistent Symptoms in Patients After Acute COVID-19. JAMA 2020, 324, 603. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Bierig, M.; Devereux, R.B.; Flachskampf, F.A.; Foster, E.; Pellikka, P.A.; Picard, M.H.; Roman, M.J.; Seward, J.; Shanewise, J.S.; et al. Recommendations for Chamber Quantification: A Report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, Developed in Conjunction with the European Association of Echocardiography, a Branch of the European Society of Cardiology. J. Am. Soc. Echocardiogr. 2005, 18, 1440–1463. [Google Scholar] [CrossRef]
- Nagueh, S.F.; Appleton, C.P.; Gillebert, T.C.; Marino, P.N.; Oh, J.K.; Smiseth, O.A.; Waggoner, A.D.; Flachskampf, F.A.; Pellikka, P.A.; Evangelista, A. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography. J. Am. Soc. Echocardiogr. 2009, 22, 107–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Croft, L.B.; Krishnamoorthy, P.; Ro, R.; Anastasius, M.; Zhao, W.; Buckley, S.; Goldman, M.; Argulian, E.; Sharma, S.K.; Kini, A.; et al. Abnormal Left Ventricular Global Longitudinal Strain by Speckle Tracking Echocardiography in COVID-19 Patients. Future Cardiol. 2020, 17, 655–661. [Google Scholar] [CrossRef] [PubMed]
- Baycan, O.F.; Barman, H.A.; Atici, A.; Tatlisu, A.; Bolen, F.; Ergen, P.; Icten, S.; Gungor, B.; Caliskan, M. Evaluation of Biventricular Function in Patients with COVID-19 Using Speckle Tracking Echocardiography. Int. J. Cardiovasc. Imaging 2021, 37, 135–144. [Google Scholar] [CrossRef]
- Pagnesi, M.; Baldetti, L.; Beneduce, A.; Calvo, F.; Gramegna, M.; Pazzanese, V.; Ingallina, G.; Napolano, A.; Finazzi, R.; Ruggeri, A.; et al. Pulmonary Hypertension and Right Ventricular Involvement in Hospitalised Patients with COVID-19. Heart 2020, 106, 1324–1331. [Google Scholar] [CrossRef]
- Klok, F.A.; Boon, G.J.a.M.; Barco, S.; Endres, M.; Geelhoed, J.J.M.; Knauss, S.; Rezek, S.A.; Spruit, M.A.; Vehreschild, J.; Siegerink, B. The Post-COVID-19 Functional Status (PCFS) Scale: A Tool to Measure Functional Status over Time after COVID-19. Eur. Respir. J. 2020, 56, 2001494. [Google Scholar] [CrossRef]
- Statistics How To. Available online: https://www.statisticshowto.com/spearman-correlation-in-spss/ (accessed on 2 February 2022).
- Inciardi, R.M.; Lupi, L.; Zaccone, G.; Italia, L.; Raffo, M.; Tomasoni, D.; Cani, D.S.; Cerini, M.; Farina, D.; Gavazzi, E.; et al. Cardiac Involvement in a Patient with Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. 2020, 5, 819. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-Month Consequences of COVID-19 in Patients Discharged from Hospital: A Cohort Study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Seeßle, J.; Waterboer, T.; Hippchen, T.; Simon, J.; Kirchner, M.; Lim, A.; Müller, B.; Merle, U. Persistent Symptoms in Adult Patients 1 Year After Coronavirus Disease 2019 (COVID-19): A Prospective Cohort Study. Clin. Infect. Dis. 2022, 74, 1191–1198. [Google Scholar] [CrossRef]
- Tudoran, M.; Tudoran, C.; Lazureanu, V.; Marinescu, A.; Pop, G.; Pescariu, A.; Enache, A.; Cut, T. Alterations of Left Ventricular Function Persisting during Post-Acute COVID-19 in Subjects without Previously Diagnosed Cardiovascular Pathology. J. Pers. Med. 2021, 11, 225. [Google Scholar] [CrossRef]
- Simonnet, A.; Chetboun, M.; Poissy, J.; Raverdy, V.; Noulette, J.; Duhamel, A.; Labreuche, J.; Mathieu, D.; Pattou, F.; Jourdain, M.; et al. High Prevalence of Obesity in Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2) Requiring Invasive Mechanical Ventilation. Obesity 2020, 28, 1195–1199. [Google Scholar] [CrossRef] [PubMed]
- Lighter, J.; Phillips, M.; Hochman, S.; Sterling, S.; Johnson, D.; Francois, F.; Stachel, A. Obesity in Patients Younger Than 60 Years Is a Risk Factor for COVID-19 Hospital Admission. Clin. Infect. Dis. 2020, 71, 896–897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raman, B.; Bluemke, D.A.; Lüscher, T.F.; Neubauer, S. Long COVID: Post-Acute Sequelae of COVID-19 with a Cardiovascular Focus. Eur. Heart J. 2022, 43, 1157–1172. [Google Scholar] [CrossRef] [PubMed]
- Thompson, E.J.; Williams, D.M.; Walker, A.J.; Mitchell, R.E.; Niedzwiedz, C.L.; Yang, T.C.; Huggins, C.F.; Kwong, A.S.F.; Silverwood, R.J.; Gessa, G.D.; et al. Risk Factors for Long COVID: Analyses of 10 Longitudinal Studies and Electronic Health Records in the UK. medRxiv 2021. [Google Scholar] [CrossRef]
- Steenblock, C.; Schwarz, P.E.H.; Ludwig, B.; Linkermann, A.; Zimmet, P.; Kulebyakin, K.; Tkachuk, V.A.; Markov, A.G.; Lehnert, H.; de Angelis, M.H.; et al. COVID-19 and Metabolic Disease: Mechanisms and Clinical Management. Lancet Diabetes Endocrinol. 2021, 9, 786–798. [Google Scholar] [CrossRef]
- Bende, F.; Tudoran, C.; Sporea, I.; Fofiu, R.; Bâldea, V.; Cotrău, R.; Popescu, A.; Sirli, R.; Ungureanu, B.S.; Tudoran, M. A Multidisciplinary Approach to Evaluate the Presence of Hepatic and Cardiac Abnormalities in Patients with Post-Acute COVID-19 Syndrome—A Pilot Study. J. Clin. Med. 2021, 10, 2507. [Google Scholar] [CrossRef]
- Puntmann, V.O.; Carerj, M.L.; Wieters, I.; Fahim, M.; Arendt, C.; Hoffmann, J.; Shchendrygina, A.; Escher, F.; Vasa-Nicotera, M.; Zeiher, A.M.; et al. Outcomes of Cardiovascular Magnetic Resonance Imaging in Patients Recently Recovered from Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. 2020, 5, 1265–1273. [Google Scholar] [CrossRef]
- Knight, D.S.; Kotecha, T.; Razvi, Y.; Chacko, L.; Brown, J.T.; Jeetley, P.S.; Goldring, J.; Jacobs, M.; Lamb, L.E.; Negus, R.; et al. COVID-19: Myocardial Injury in Survivors. Circulation 2020, 142, 1120–1122. [Google Scholar] [CrossRef]
- Dini, F.L.; Fabiani, I.; Miccoli, M.; Galeotti, G.G.; Pugliese, N.R.; D’Agostino, A.; Scartabelli, A.; Conte, L.; Salvetti, G.; Santini, F.; et al. Prevalence and Determinants of Left Ventricular Diastolic Dysfunction in Obese Subjects and the Role of Left Ventricular Global Longitudinal Strain and Mass Normalized to Height. Echocardiography 2018, 35, 1124–1131. [Google Scholar] [CrossRef]
- Rayner, J.J.; Banerjee, R.; Holloway, C.J.; Lewis, A.J.M.; Peterzan, M.A.; Francis, J.M.; Neubauer, S.; Rider, O.J. The Relative Contribution of Metabolic and Structural Abnormalities to Diastolic Dysfunction in Obesity. Int. J. Obes. 2018, 42, 441–447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burroughs Peña, M.; Swett, K.; Schneiderman, N.; Spevack, D.M.; Ponce, S.G.; Talavera, G.A.; Kansal, M.M.; Daviglus, M.L.; Cai, J.; Hurwitz, B.E.; et al. Cardiac Structure and Function with and without Metabolic Syndrome: The Echocardiographic Study of Latinos (Echo-SOL). BMJ Open Diab. Res. Care 2018, 6, e000484. [Google Scholar] [CrossRef] [PubMed]
- Tudoran, C.; Tudoran, M.; Cut, T.G.; Lazureanu, V.E.; Oancea, C.; Marinescu, A.R.; Pescariu, S.A.; Pop, G.N.; Bende, F. Evolution of Echocardiographic Abnormalities Identified in Previously Healthy Individuals Recovering from COVID-19. J. Pers. Med. 2022, 12, 46. [Google Scholar] [CrossRef] [PubMed]
- Augustin, M.; Schommers, P.; Stecher, M.; Dewald, F.; Gieselmann, L.; Gruell, H.; Horn, C.; Vanshylla, K.; Cristanziano, V.D.; Osebold, L.; et al. Post-COVID Syndrome in Non-Hospitalised Patients with COVID-19: A Longitudinal Prospective Cohort Study. Lancet Reg. Health Eur. 2021, 6, 100122. [Google Scholar] [CrossRef]
- Tian, L.; Duan, F.; Li, X.; Zhou, C. Incidence, Risk Factors and Prognostic Effect of Imaging Left Ventricular Diastolic Dysfunction in Patients with COVID-19: Protocol for a Systematic Review. BMJ Open 2022, 12, e059281. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Group A N = 59 | Group B N = 53 | Group C N = 91 | p-Value | |||
|---|---|---|---|---|---|---|
| A/B | B/C | A/C | ||||
| Gender: | ||||||
| Men | 25 (42.37%) | 20 (37.73%) | 37 (40.65%) | 0.7388 | 0.3858 | 0.7288 |
| Women | 34 (57.62%) | 33 (62.26%) | 54 (59.34%) | 0.7588 | 0.9114 | 0.9954 |
| Age (year) | 49.55 ± 5.62 | 46.98 ± 4.74 | 41.67 ± 7.45 | 0.0106 | <0.0001 | <0.0001 |
| BMI (Kg/m2) | 32.28 (30.47–33.6) | 27.7 (26.5–29.98) | 24.38 (22.56–26.8) | <0.0001 | <0.0001 | <0.0001 |
| Waist circumference (cm) | 100 (94–110) | 90 (89–103) | 86 (78–98) | <0.0001 | 0.0002 | <0.0001 |
| SPB (mmHg) | 130 (130–140) | 130 (120–132.5) | 120 (100–120) | 0.0234 | <0.0001 | <0.0001 |
| DBP (mmHg) | 80 (70–90) | 80 (70–80) | 70 (60–70) | 0.0133 | <0.0001 | <0.0001 |
| Heart rate (b/min) | 75 (70–80) | 75 (75–80) | 80 (75–85) | 0.5030 | 0.0017 | 0.0004 |
| Weeks since COVID-19 infection | 8 (8–10) | 8 (8–10) | 9 (9–10) | 0.8324 | 0.0147 | 0.0329 |
| Number of symptoms | 6 (4–7) | 5 (3–6) | 3 (3–6) | 0.0962 | 0.0162 | <0.0001 |
| PCFS scale | 2 (1–3) | 2 (1–2) | 1 (1–2) | <0.0001 | 0.0044 | <0.0001 |
| Self-assessed exercise level | 0.5 (0.4–1) | 1.1 (1–2) | 2.3 (1.5–3) | <0.0001 | <0.0001 | <0.0001 |
| Results of the initial COVID-19 evaluation | ||||||
| COVID-19 severity: | ||||||
| Moderate | 25 (42.37%) | 12 (22.64%) | 16 (17.58%) | 0.0439 | 0.6019 | 0.0017 |
| Mild | 34 (57.62%) | 41 (77.35%) | 75 (82.41%) | 0.0439 | 0.6287 | 0.0030 |
| Lung injury on CCT (%) | 15 (15–30) | 8 (0–29) | 0 (0–6) | 0.1737 | 0.0023 | <0.0001 |
| CRP (mg/dL) | 30.28(27.6–36.75) | 27.89 (23.9–36.4) | 26.23(16.84–30.2) | 0.0686 | 0.0119 | <0.0001 |
| Laboratory results at baseline | ||||||
| Basal blood glucose (mg/dL) | 104 (100 -118) | 100 (100–110) | 90 (89–95) | 0.0026 | <0.0001 | <0.0001 |
| Uric acid (mg/dL) | 7.6 (7.3–8) | 7.3 (7.2–7.5) | 6.3 (6–6.8) | 0.0019 | <0.0001 | <0.0001 |
| LDL cholesterol (mg/dL) | 140 (130–150) | 120 (120–140) | 100 (90–120) | <0.0001 | <0.0001 | <0.0001 |
| HDL cholesterol (mg/dL) | 30 (30–35) | 35 (30–40) | 45 (40–50) | 0.0917 | <0.0001 | <0.0001 |
| Triglycerides (mg/dL) | 170 (160–190) | 160 (160–170) | 140 (130–145) | <0.0001 | <0.0001 | <0.0001 |
| Group A N = 59 | Group B N = 53 | Group C N = 91 | p-Value | |||
|---|---|---|---|---|---|---|
| A/B | B/C | A/C | ||||
| LVMI (g/m2) | 100 (95.98–114.53) | 96.12(88.3–108) | 87.7 (70.45–97.54) | 0.0011 | 0.0002 | <0.0001 |
| LVEF (%) | 53 (50–55) | 55 (52.5–60) | 60 (55–65) | 0.0025 | 0.0002 | <0.0001 |
| MAPSE lateral (mm) | 14 (12–16) | 15 (12–16) | 17 (15–18) | 0.5595 | <0.0001 | <0.0001 |
| LV-GLS (%) | −19 (−20–−18) | −20 (−21–−19) | −21 (−22–−19) | 0.0002 | 0.2227 | <0.0001 |
| LAVI (mL/m2) | 30.21(23.43–30.67) | 20 (17.6–27.23) | 15.76 (13.3–21.34) | <0.0001 | 0.0002 | <0.0001 |
| E/A | 0.98 (0.81–1.29) | 1.01 (0.77–1.27) | 1.11 (0.9–1.34) | 0.8429 | 0.1397 | 0.2263 |
| E/e’ average | 14.12 (12.23–14.4) | 12.83 (11.4–14.14) | 11.94 (9.8–13) | 0.0098 | 0.0023 | <0.0001 |
| TRV max (m/s) | 2.69 (2.6–2.87) | 2.67 (2.41–2.71) | 2.51 (2–2.7) | 0.0400 | 0.0045 | <0.0001 |
| sPAP (mmHg) | 33.94 (32–37.94) | 33.5 (28.23–34.37) | 30.2 (21–34.16) | 0.0400 | 0.0045 | <0.0001 |
| TAPSE lateral (mm) | 20 (17–21) | 20 (19–22) | 24 (21–26) | 0.0079 | <0.0001 | <0.0001 |
| FAC (%) | 36.56 (35.47–37.9) | 36.23 (35–37.89) | 37.89 (35.7–39) | 0.8841 | 0.0042 | 0.0002 |
| RV-GLS (%) | −28 (−30–−27) | −29 (−30–−28) | −31 (−33–−29) | 0.5364 | <0.0001 | <0.0001 |
| Age | BMI | MS Factors | CCT Injury | CRP | Weeks | Number of Symptoms | PCFS Scale | LVMI | Level of Exercise | |
|---|---|---|---|---|---|---|---|---|---|---|
| R | 0.46 | 0.36 | 0.46 | 0.63 | 0.75 | −0.49 | 0.61 | 0.63 | 0.52 | −0.63 |
| 95%CI | 0.347–0.564 | 0.237–0.477 | 0.345–0.563 | 0.542–0.708 | 0.687–0.807 | −0.589–−0.380 | 0.524–0.696 | 0.548–0.712 | 0.413–0.615 | −0.708–−0.541 |
| p | ˂0.001 | ˂0.001 | ˂0.001 | ˂0.001 | ˂0.001 | ˂0.001 | ˂0.001 | ˂0.001 | ˂0.001 | ˂0.001 |
| Age | BMI | CCT Injury | CRP | Weeks | Number of Symptoms | PCFS Scale | LVMI | E/e’ Average | TRV | LAVI | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| R | 0.695 | 0.684 | 0.414 | 0.446 | −0.359 | 0.280 | 0.519 | 0.554 | 0.461 | 0.518 | 0.580 |
| 95%CI | 0.616–0.760 | 0.603–0.751 | 0.293–0.522 | 0.329–0.550 | −0.474–−0.233 | 0.149–0.403 | 0.410–0.612 | 0.450–0.642 | 0.345–0.563 | 0.410–0.512 | 0.480–0.664 |
| p | ˂0.001 | ˂0.001 | ˂0.001 | ˂0.001 | ˂0.001 | ˂0.001 | ˂0.001 | ˂0.001 | ˂0.001 | ˂0.001 | ˂0.001 |
| Variable | β | ±SE | p |
|---|---|---|---|
| Multivariate linear regression analysis of DD | |||
| Pulmonary injury on CCT | 0.035 | ±0.0028 | <0.0001 |
| SBP values | 0.007926 | ±0.003122 | 0.0119 |
| MS factors | 0.080 | ±0.022 | 0.0004 |
| LVMI values | β = 0.00606 | ±0.002353 | p = 0.0107 |
| Multivariate linear regression analysis of E/e’ values | |||
| LVMI values | 0.0236 | ±0.0059 | 0.0001 |
| CRP levels | 0.1139 | ±0.01166 | <0.0001 |
| PCFS | 0.6048 | ±0.157 | 0.0002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tudoran, C.; Tudoran, M.; Cut, T.G.; Lazureanu, V.E.; Bende, F.; Fofiu, R.; Enache, A.; Pescariu, S.A.; Novacescu, D. The Impact of Metabolic Syndrome and Obesity on the Evolution of Diastolic Dysfunction in Apparently Healthy Patients Suffering from Post-COVID-19 Syndrome. Biomedicines 2022, 10, 1519. https://doi.org/10.3390/biomedicines10071519
Tudoran C, Tudoran M, Cut TG, Lazureanu VE, Bende F, Fofiu R, Enache A, Pescariu SA, Novacescu D. The Impact of Metabolic Syndrome and Obesity on the Evolution of Diastolic Dysfunction in Apparently Healthy Patients Suffering from Post-COVID-19 Syndrome. Biomedicines. 2022; 10(7):1519. https://doi.org/10.3390/biomedicines10071519
Chicago/Turabian StyleTudoran, Cristina, Mariana Tudoran, Talida Georgiana Cut, Voichita Elena Lazureanu, Felix Bende, Renata Fofiu, Alexandra Enache, Silvius Alexandru Pescariu, and Dorin Novacescu. 2022. "The Impact of Metabolic Syndrome and Obesity on the Evolution of Diastolic Dysfunction in Apparently Healthy Patients Suffering from Post-COVID-19 Syndrome" Biomedicines 10, no. 7: 1519. https://doi.org/10.3390/biomedicines10071519