
Causative Agents of Ventilator-Associated Pneumonia and Resistance to Antibiotics in COVID-19 Patients: A Systematic Review


Abstract
:1. Introduction
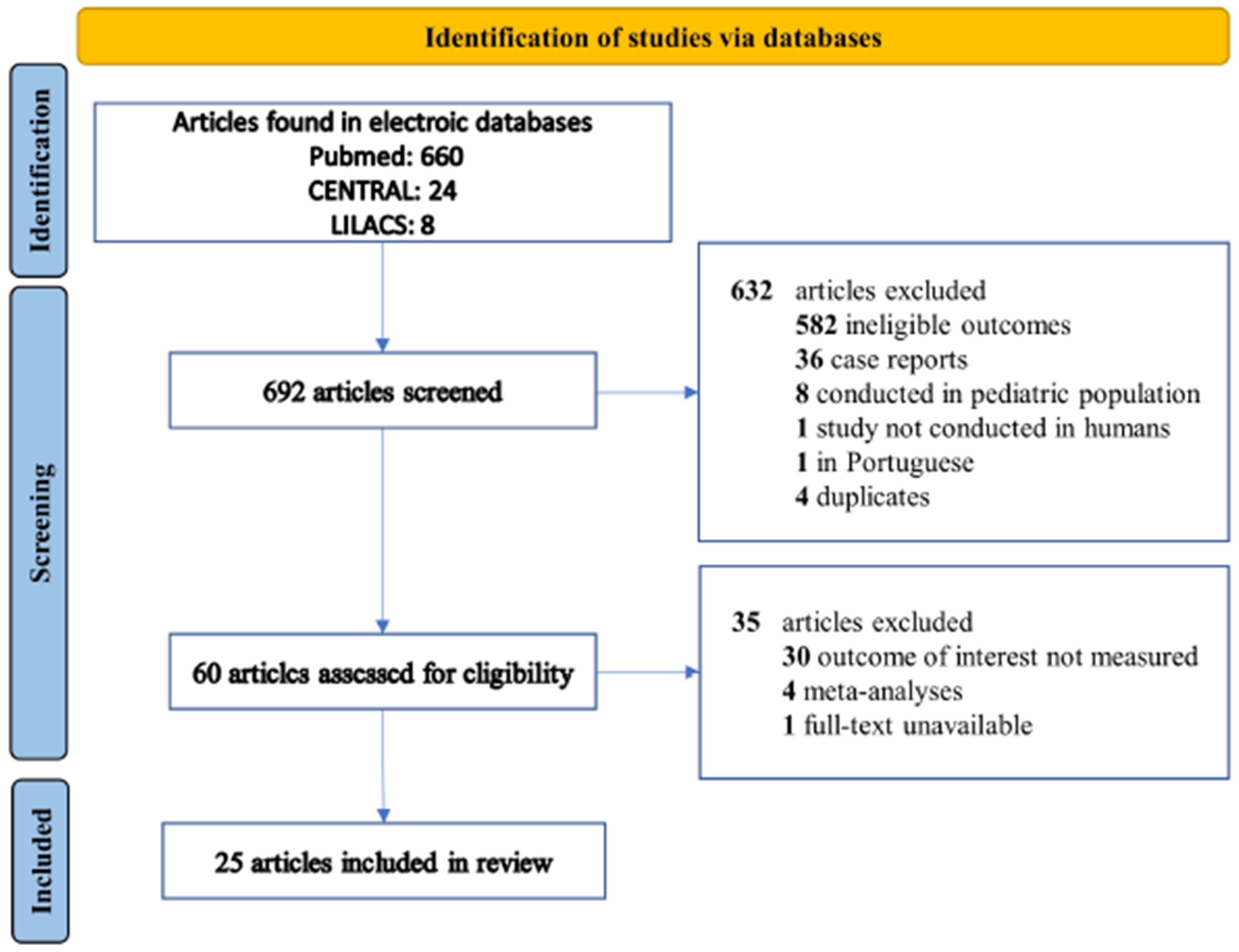
2. Materials and Methods
3. Results
3.1. Study Characteristics and Quality
3.2. VAP Caused by Gram-Negative Pathogens
3.3. VAP Caused by Gram-Positive Pathogens
3.4. Fungal VAP
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thakur, B.; Dubey, P.; Benitez, J.; Torres, J.P.; Reddy, S.; Shokar, N.; Aung, K.; Mukherjee, D.; Dwivedi, A.K. A systematic review and meta-analysis of geographic differences in comorbidities and associated severity and mortality among individuals with COVID-19. Sci. Rep. 2021, 11, 8562. [Google Scholar] [CrossRef] [PubMed]
- Meyerowitz-Katz, G.; Merone, L. A systematic review and meta-analysis of published research data on COVID-19 infection fatality rates. Int. J. Infect. Dis. 2020, 101, 138–148. [Google Scholar] [CrossRef] [PubMed]
- Bonanad, C.; García-Blas, S.; Tarazona-Santabalbina, F.; Sanchis, J.; Bertomeu-González, V.; Fácila, L.; Ariza, A.; Núñez, J.; Cordero, A. The Effect of Age on Mortality in Patients with COVID-19: A Meta-Analysis with 611,583 Subjects. J. Am. Med. Dir. Assoc. 2020, 21, 915–918. [Google Scholar] [CrossRef] [PubMed]
- Chang, R.; Elhusseiny, K.M.; Yeh, Y.-C.; Sun, W.-Z. COVID-19 ICU and mechanical ventilation patient characteristics and outcomes—A systematic review and meta-analysis. PLoS ONE 2021, 16, e0246318. [Google Scholar] [CrossRef]
- Sturm, L.K.; Saake, K.; Roberts, P.B.; Masoudi, F.A.; Fakih, M.G. Impact of COVID-19 pandemic on hospital onset bloodstream infections (HOBSI) at a large health system. Am. J. Infect. Control 2022, 50, 245–249. [Google Scholar] [CrossRef]
- DeVoe, C.; Segal, M.R.; Wang, L.; Stanley, K.; Madera, S.; Fan, J.; Schouest, J.; Graham-Ojo, R.; Nichols, A.; Prasad, P.A.; et al. Increased rates of secondary bacterial infections, including Enterococcus bacteremia, in patients hospitalized with coronavirus disease 2019 (COVID-19). Infect. Control Hosp. Epidemiol. 2021, 1–8. [Google Scholar] [CrossRef]
- Kalil, A.C.; Metersky, M.L.; Klompas, M.; Muscedere, J.; Sweeney, D.A.; Palmer, L.B.; Napolitano, L.M.; O’Grady, N.P.; Bartlett, J.G.; Carratalà, J.; et al. Management of adults with hospital- acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines by the infectious diseases society of America and the American thoracic society. Clin. Infect. Dis. 2016, 63, e61–e111. [Google Scholar] [CrossRef]
- Sandiumenge, A.; Rello, J. Ventilator-associated pneumonia caused by ESKAPE organisms: Cause, clinical features, and management. Curr. Opin. Pulm. Med. 2012, 18, 187–193. [Google Scholar] [CrossRef]
- Lim, S.M.S.; Zainal Abidin, A.; Liew, S.M.; Roberts, J.A.; Sime, F.B. The global prevalence of multidrug-resistance among Acinetobacter baumannii causing hospital-acquired and ventilator-associated pneumonia and its associated mortality: A systematic review and meta-analysis. J. Infect. 2019, 79, 593–600. [Google Scholar]
- Khan, S.; Hasan, S.S.; Bond, S.E.; Conway, B.R.; Aldeyab, M.A. Antimicrobial consumption in patients with COVID-19: A systematic review and meta-analysis. Expert Rev. Anti-Infect. Ther. 2022, 20, 749–772. [Google Scholar] [CrossRef]
- PAHO. Antimicrobial Resistance, Fueled by the COVID-19 Pandemic. Policy Brief November 2021. Available online: https://iris.paho.org/bitstream/handle/10665.2/55864/PAHOCDEAMRCOVID19220006_eng.pdf?sequence=5&isAllowed=y (accessed on 18 May 2022).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Beaucoté, V.; Plantefève, G.; Tirolien, J.A.; Desaint, P.; Fraissé, M.; Contou, D. Lung Abscess in Critically Ill Coronavirus Disease 2019 Patients with Ventilator-Associated Pneumonia: A French Monocenter Retrospective Study. Crit. Care Explor. 2021, 3, e0482. [Google Scholar] [CrossRef] [PubMed]
- Gragueb-Chatti, I.; Lopez, A.; Hamidi, D.; Guervilly, C.; Loundou, A.; Daviet, F.; Cassir, N.; Papazian, L.; Forel, J.M.; Leone, M.; et al. Impact of dexamethasone on the incidence of ventilator-associated pneumonia and blood stream infections in COVID-19 patients requiring invasive mechanical ventilation: A multicenter retrospective study. Ann. Intensive Care 2021, 11, 87. [Google Scholar] [CrossRef] [PubMed]
- De Pascale, G.; De Maio, F.; Carelli, S.; De Angelis, G.; Cacaci, M.; Montini, L.; Bello, G.; Cutuli, S.L.; Pintaudi, G.; Tanzarella, E.L.; et al. Staphylococcus aureus ventilator-associated pneumonia in patients with COVID-19: Clinical features and potential inference with lung dysbiosis. Crit. Care 2021, 25, 197. [Google Scholar] [CrossRef]
- De Santis, V.; Corona, A.; Vitale, D.; Nencini, C.; Potalivo, A.; Prete, A.; Zani, G.; Malfatto, A.; Tritapepe, L.; Taddei, S.; et al. Bacterial infections in critically ill patients with SARS-2-COVID-19 infection: Results of a prospective observational multicenter study. Infection 2021, 50, 139–148. [Google Scholar] [CrossRef]
- Karolyi, M.; Pawelka, E.; Hind, J.; Baumgartner, S.; Friese, E.; Hoepler, W.; Neuhold, S.; Omid, S.; Seitz, T.; Traugott, M.T.; et al. Detection of bacteria via multiplex PCR in respiratory samples of critically ill COVID-19 patients with suspected HAP/VAP in the ICU. Wien. Klin. Wochenschr. 2022, 134, 385–390. [Google Scholar] [CrossRef]
- Luque-Paz, D.; Tattevin, P.; Jaubert, P.; Reizine, F.; Kouatchet, A.; Camus, C. Selective digestive decontamination to reduce the high rate of ventilator-associated pneumonia in critical COVID-19. Anaesth. Crit. Care Pain Med. 2022, 41, 100987. [Google Scholar] [CrossRef]
- Meawed, T.E.; Ahmed, S.M.; Mowafy, S.M.; Samir, G.M.; Anis, R.H. Bacterial and fungal ventilator associated pneumonia in critically ill COVID-19 patients during the second wave. J. Infect. Public Health 2021, 14, 1375–1380. [Google Scholar] [CrossRef]
- Pickens, C.O.; Gao, C.A.; Cuttica, M.J.; Smith, S.B.; Pesce, L.L.; Grant, R.A.; Kang, M.; Morales-Nebreda, L.; Bavishi, A.A.; Arnold, J.M.; et al. NU COVID Investigators. Bacterial Superinfection Pneumonia in Patients Mechanically Ventilated for COVID-19 Pneumonia. Am. J. Respir. Crit. Care Med. 2021, 204, 921–932. [Google Scholar] [CrossRef]
- Risa, E.; Roach, D.; Budak, J.Z.; Hebert, C.; Chan, J.D.; Mani, N.S.; Bryson-Cahn, C.; Town, J.; Johnson, N.J. Characterization of Secondary Bacterial Infections and Antibiotic Use in Mechanically Ventilated Patients with COVID-19 Induced Acute Respiratory Distress Syndrome. J. Intensive Care Med. 2021, 36, 1167–1175. [Google Scholar] [CrossRef]
- Rouyer, M.; Strazzulla, A.; Youbong, T.; Tarteret, P.; Pitsch, A.; de Pontfarcy, A.; Cassard, B.; Vignier, N.; Pourcine, F.; Jochmans, S.; et al. Ventilator-Associated Pneumonia in COVID-19 Patients: A Retrospective Cohort Study. Antibiotics 2021, 10, 988. [Google Scholar] [CrossRef] [PubMed]
- Signorini, L.; Moioli, G.; Calza, S.; van Hauwermeiren, E.; Lorenzotti, S.; del Fabro, G.; Renisi, G.; Lanza, P.; Saccani, B.; Zambolin, G.; et al. Epidemiological and Clinical Characterization of Superinfections in Critically Ill Coronavirus Disease 2019 Patients. Crit. Care Explor. 2021, 3, e0430. [Google Scholar] [CrossRef] [PubMed]
- Bardi, T.; Pintado, V.; Gomez-Rojo, M.; Escudero-Sanchez, R.; Azzam Lopez, A.; Diez-Remesal, Y.; Martinez Castro, N.; Ruiz-Garbajosa, P.; Pestaña, D. Nosocomial infections associated to COVID-19 in the intensive care unit: Clinical characteristics and outcome. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 495–502. [Google Scholar] [CrossRef] [PubMed]
- Blonz, G.; Kouatchet, A.; Chudeau, N.; Pontis, E.; Lorber, J.; Lemeur, A.; Planche, L.; Lascarrou, J.B.; Colin, G. Epidemiology and microbiology of ventilator-associated pneumonia in COVID-19 patients: A multicenter retrospective study in 188 patients in an un-inundated French region. Crit. Care 2021, 25, 72. [Google Scholar] [CrossRef] [PubMed]
- Suarez-de-la-Rica, A.; Serrano, P.; de-la-Oliva, R.; Sánchez-Díaz, P.; Molinero, P.; Falces-Romero, I.; Ferrando, C.; Rello, J.; Maseda, E. Secondary infections in mechanically ventilated patients with COVID-19: An overlooked matter? Rev. Esp. Quimioter. 2021, 34, 330–336. [Google Scholar] [CrossRef]
- Luyt, C.E.; Sahnoun, T.; Gautier, M.; Vidal, P.; Burrel, S.; Pineton De Chambrun, M.; Chommeloux, J.; Desnos, C.; Arzoine, J.; Nieszkowska, A.; et al. Ventilator-associated pneumonia in patients with SARS-CoV-2-associated acute respiratory distress syndrome requiring ECMO: A retrospective cohort study. Ann. Intensive Care 2020, 10, 158. [Google Scholar] [CrossRef]
- Garcia-Vidal, C.; Sanjuan, G.; Moreno-García, E.; Puerta-Alcalde, P.; Garcia-Pouton, N.; Chumbita, M.; Fernandez-Pittol, M.; Pitart, C.; Inciarte, A.; Bodro, M.; et al. Incidence of co-infections and superinfections in hospitalized patients with COVID-19: A retrospective cohort study. Clin. Microbiol. Infect. 2021, 27, 83–88. [Google Scholar] [CrossRef]
- Giacobbe, D.R.; Battaglini, D.; Enrile, E.M.; Dentone, C.; Vena, A.; Robba, C.; Ball, L.; Bartoletti, M.; Coloretti, I.; Di Bella, S.; et al. Incidence and Prognosis of Ventilator-Associated Pneumonia in Critically Ill Patients with COVID-19: A Multicenter Study. J. Clin. Med. 2021, 10, 555. [Google Scholar] [CrossRef]
- Grasselli, G.; Scaravilli, V.; Mangioni, D.; Scudeller, L.; Alagna, L.; Bartoletti, M.; Bellani, G.; Biagioni, E.; Bonfanti, P.; Bottino, N.; et al. Hospital-Acquired Infections in Critically Ill Patients with COVID-19. Chest 2021, 160, 454–465. [Google Scholar] [CrossRef]
- Maes, M.; Higginson, E.; Pereira-Dias, J.; Curran, M.D.; Parmar, S.; Khokhar, F.; Cuchet-Lourenço, D.; Lux, J.; Sharma-Hajela, S.; Ravenhill, B.; et al. Ventilator-associated pneumonia in critically ill patients with COVID-19. Crit. Care 2021, 25, 25. [Google Scholar] [CrossRef]
- Martinez-Guerra, B.A.; Gonzalez-Lara, M.F.; de-Leon-Cividanes, N.A.; Tamez-Torres, K.M.; Roman-Montes, C.M.; Rajme-Lopez, S.; Villalobos-Zapata, G.I.; Lopez-Garcia, N.I.; Martínez-Gamboa, A.; Sifuentes-Osornio, J.; et al. Antimicrobial Resistance Patterns and Antibiotic Use during Hospital Conversion in the COVID-19 Pandemic. Antibiotics 2021, 10, 182. [Google Scholar] [CrossRef] [PubMed]
- Moretti, M.; van Laethem, J.; Minini, A.; Pierard, D.; Malbrain, M.L. Ventilator-associated bacterial pneumonia in coronavirus 2019 disease, a retrospective monocentric cohort study. J. Infect. Chemother. 2021, 27, 826–833. [Google Scholar] [CrossRef] [PubMed]
- Razazi, K.; Arrestier, R.; Haudebourg, A.F.; Benelli, B.; Carteaux, G.; Decousser, J.W.; Fourati, S.; Woerther, P.L.; Schlemmer, F.; Charles-Nelson, A.; et al. Risks of ventilator-associated pneumonia and invasive pulmonary aspergillosis in patients with viral acute respiratory distress syndrome related or not to Coronavirus 19 disease. Crit. Care 2020, 24, 699. [Google Scholar] [CrossRef] [PubMed]
- Rouzé, A.; Martin-Loeches, I.; Povoa, P.; Makris, D.; Artigas, A.; Bouchereau, M.; Lambiotte, F.; Metzelard, M.; Cuchet, P.; Boulle Geronimi, C.; et al. coVAPid study Group. Relationship between SARS-CoV-2 infection and the incidence of ventilator-associated lower respiratory tract infections: A European multicenter cohort study. Intensive Care Med. 2021, 47, 188–198. [Google Scholar] [CrossRef] [PubMed]
- Søgaard, K.K.; Baettig, V.; Osthoff, M.; Marsch, S.; Leuzinger, K.; Schweitzer, M.; Meier, J.; Bassetti, S.; Bingisser, R.; Nickel, C.H.; et al. Community-acquired and hospital-acquired respiratory tract infection and bloodstream infection in patients hospitalized with COVID-19 pneumonia. J. Intensive Care 2021, 9, 10. [Google Scholar] [CrossRef]
- Vacheron, C.H.; Lepape, A.; Savey, A.; Machut, A.; Timsit, J.F.; Vanhems, P.; Le, Q.V.; Egbeola, J.; Martin, M.; Maxime, V.; et al. Increased Incidence of Ventilator-Acquired Pneumonia in Coronavirus Disease 2019 Patients. Crit. Care Med. 2022, 50, 449–459. [Google Scholar] [CrossRef]
- Wu, D.; Wu, C.; Zhang, S.; Zhong, Y. Risk Factors of Ventilator-Associated Pneumonia in Critically III Patients. Front. Pharmacol. 2019, 10, 482. [Google Scholar] [CrossRef] [Green Version]
- Melsen, W.G.; Rovers, M.M.; Bonten, M.J. Ventilator-associated pneumonia and mortality: A systematic review of observational studies. Crit. Care Med. 2009, 37, 2709–2718. [Google Scholar]
- Melsen, W.G.; Rovers, M.M.; Groenwold, R.H.; Bergmans, D.C.; Camus, C.; Bauer, T.T.; Hanisch, E.W.; Klarin, B.; Koeman, M.; Krueger, W.A.; et al. Attributable mortality of ventilator-associated pneumonia: A meta-analysis of individual patient data from randomised prevention studies. Lancet Infect. Dis. 2013, 13, 665–671. [Google Scholar] [CrossRef]
- Ippolito, M.; Misseri, G.; Catalisano, G.; Marino, C.; Ingoglia, G.; Alessi, M.; Consiglio, E.; Gregoretti, C.; Giarratano, A.; Cortegiani, A. Ventilator-Associated Pneumonia in Patients with COVID-19: A Systematic Review and Meta-Analysis. Antibiotics 2021, 10, 545. [Google Scholar] [CrossRef]
- Luyt, C.E.; Hékimian, G.; Koulenti, D.; Chastre, J. Microbial cause of ICU-acquired pneumonia: Hospital-acquired pneumonia versus ventilator-associated pneumonia. Curr. Opin. Crit. Care 2018, 24, 332–338. [Google Scholar] [CrossRef] [PubMed]
- Govindaraj Vaithinathan, A.; Vanitha, A. WHO global priority pathogens list on antibiotic resistance: An urgent need for action to integrate One Health data. Perspect. Public Health 2018, 138, 87–88. [Google Scholar] [CrossRef] [PubMed]
- López-Jácome, L.E.; Fernández-Rodríguez, D.; Franco-Cendejas, R.; Camacho-Ortiz, A.; Morfin-Otero, M.D.R.; Rodríguez-Noriega, E.; Ponce-de-León, A.; Ortiz-Brizuela, E.; Rojas-Larios, F.; Velázquez-Acosta, M.D.C.; et al. Increment Antimicrobial Resistance During the COVID-19 Pandemic: Results from the Invifar Network. Microb. Drug Resist. 2022, 28, 338–345. [Google Scholar] [PubMed]
- Bahçe, Y.G.; Acer, Ö.; Özüdoğru, O. Evaluation of bacterial agents isolated from endotracheal aspirate cultures of COVID-19 general intensive care patients and their antibiotic resistance profiles compared to pre-pandemic conditions. Microb. Pathog. 2022, 164, 105409. [Google Scholar] [CrossRef] [PubMed]
- Dellière, S.; Dudoignon, E.; Fodil, S.; Voicu, S.; Collet, M.; Oillic, P.A.; Salmona, M.; Dépret, F.; Ghelfenstein-Ferreira, T.; Plaud, B.; et al. Risk factors associated with COVID-19-associated pulmonary aspergillosis in ICU patients: A French multicentric retrospective cohort. Clin. Microbiol. Infect. 2020, 27, 790.e1–790.e5. [Google Scholar] [CrossRef]
- Fekkar, A.; Lampros, A.; Mayaux, J.; Poignon, C.; Demeret, S.; Constantin, J.M.; Marcelin, A.G.; Monsel, A.; Luyt, C.E.; Blaize, M. Occurrence of Invasive Pulmonary Fungal Infections in Patients with Severe COVID-19 Admitted to the ICU. Am. J. Respir. Crit. Care Med. 2021, 203, 307–317. [Google Scholar] [CrossRef]
- Bartoletti, M.; Pascale, R.; Cricca, M.; Rinaldi, M.; Maccaro, A.; Bussini, L.; Fornaro, G.; Tonetti, T.; Pizzilli, G.; Francalanci, E.; et al. PREDICO Study Group. Epidemiology of Invasive Pulmonary Aspergillosis Among Intubated Patients with COVID-19: A Prospective Study. Clin. Infect. Dis. 2021, 73, e3606–e3614. [Google Scholar] [CrossRef]


{kind=link}
| First Author | Year | No. of Patients Requiring MV | No. of Patients with VAP | Immunosuppression | VAP Mortality | Main Causative Pathogens |
|---|---|---|---|---|---|---|
| Beaucote V, et al. [13] | 2021 | 161 | 119 | Corticosteroids 61%, immunosuppression (active solid cancer, hematologic cancer, organ transplant, HIV, or immunosuppressive drugs) 17%. | No information | P. aeruginosa (8%) K. aerogenes (4%) S. aureus (3%) |
| Gragueb–Chatti I, et al. [14] | 2021 | 151 | 127 | Immunosuppression 7%, history of neoplasm 12%, hydrocortisone for septic shock 18%, dexamethasone 55.6%. | No information | S. aureus (22%) P. aeruginosa (17%) K. aerogenes (9%) K. pneumoniae (8%) |
| De Pascale G, et al. [15] | 2021 | No information | 40 | Immunosuppression 6.7%, neoplasm 5.8%. | No information | S. aureus (100%) |
| De Santis V, et al. [16] | 2021 | No information | 62 | Neoplasm 6%, immunosuppression 3.6%, tocilizumab 28.6%. | No information | P. aeruginosa (22%) S. aureus (16%) E. coli (13%) K. pneumoniae (12%) |
| Karolyi M, et al. [17] | 2021 | 60 | 48 | Not specified. | 36.7% | S. aureus (22%) K. pneumoniae (20%) H. influenzae (10%) |
| Luque-Paz D, et al. [18] | 2021 | 178 | 66 | Not specified. | 28.3% | Enterobacteriaceae (65%) S. aureus (16%) P. aeruginosa (15%) |
| Meawed T, et al. [19] | 2021 | No information | 331 | Steroids 100%, tocilizumab 90%. | No information | K. pneumoniae (24.4%) C. albicans (17%) A. baumannii (16%) P. aeruginosa (12%) |
| Pickens C, et al. [20] | 2021 | 179 | 72 | Solid organ transplant 6.3%, bone marrow transplantation/malignancy 1.7%, other cancer 8.4%, anti-IL-6r 25.3%, corticosteroids 32%. | No information | S. aureus (18%) S. viridans (13%) |
| Risa E, et al. [21] | 2021 | 126 | 69 | Not specified. | No information | S. aureus (57%) K. aerogenes (15%) |
| Rouyer M, et al. [22] | 2021 | 79 | 42 | Corticosteroids 35%, neoplasm 5%, immunosuppressive treatment 5%. | 81% | Enterobacteriaceae (54%) P. aeruginosa (19%) |
| Signorini L, et al. [23] | 2021 | 92 | 75 | Steroids 98%. | No information | P. aeruginosa (34%) S. maltophila (18%) Enterococcus spp. (14%) |
| Bardi T, et al. [24] | 2021 | 134 | 21 | Steroids 90%, tocilizumab 68%. | No information | P. aeruginosa (38%) S. aureus (23%) |
| Blonz G, et al. [25] | 2021 | 194 | 92 | Cancer 5.9%, hematologic malignancies 2.7%, HIV 2.1%, immunosuppressive therapy 3.7%, long-term corticosteroid therapy 1.6%. | 30% | P. aeruginosa (33%) S. aureus (30%) E. coli (28%) K. pneumoniae (17%) |
| Suarez-de-la-Rica A, et al. [26] | 2021 | 107 | 35 | Solid tumor 10.3%, HIV 0.9%, corticosteroids 76.6%, tocilizumab 46.7%. | No information | P. aeruginosa (31%) Klebsiella spp. (25%) |
| Luyt C, et al. [27] | 2020 | 54 | 43 | Immunocompromised 2%. | 9% | P. aeruginosa (37%) K. aerogenes (25%) E. cloacae (7%) S. aureus (7%) |
| Garcia-Vidal C, et al. [28] | 2021 | 44 | 11 | Cancer 8.4%, tocilizumab 21.8%, methylprednisolone 26%, dexamethasone 2.5%. | No information | S. aureus (36%) P. aeruginosa (27%) |
| Giacobbe DR, et al. [29] | 2021 | 586 | 171 | Solid cancer 6%, hematological malignancy 2%, steroids 63%, anti-IL-6 64%, anti-IL-1 3%. | 45% | P. aeruginosa (15%) S. aureus (10.5%) K. pneumoniae (8.7%) |
| Grasselli G, et al. [30] | 2021 | 688 | 389 | Immunological comorbidity 12%, tocilizumab 24%. | No information | S. aureus (28%) P. aeruginosa (21%) Klebsiella species (11%) |
| Maes M, et al. [31] | 2021 | 82 | 39 | Immunocompromised 15%, corticosteroid use 13%. | No information | P. aeruginosa (14%) E. coli (14%) K. pneumoniae (12%) |
| Martinez-Guerra B, et al. [32] | 2021 | No information | 69 | Immunosuppression 5.7%, HIV 1.3%, steroid 9.2%. | No information | P. aeruginosa (14%) Klebsiella spp. (13%) E. coli (13%) |
| Moretti M, et al. [33] | 2021 | 39 | 27 | Immunosuppressant use 7.8%, neoplasm 7.8%. | 40% | K. pneumoniae (25%) P. aeruginosa (18%) |
| Razazi K, et al. [34] | 2020 | 90 | 58 | Solid cancer 5%, blood cancer 21%, organ transplant 11%, HIV 5%, sickle cell disease 2%, others 6%, corticosteroids 37%. | 56% | Enterobacter spp. (39%) E. coli (17%) |
| Rouze A, et al. [35] | 2021 | 568 | 205 | Immunosuppression 9.3%, corticosteroids 37%. | No information | P. aeruginosa (31%) Enterobacter spp. (26%) S. aureus (17%) |
| Sogaard KK, et al. [36] | 2021 | 34 | 5 | Not specified. | No information | A. fumigatus (40%) |
| Vacheron CH, et al. [37] | 2021 | No information | 550 | Not specified. | No information | P. aeruginosa (22%) Enterobacter spp. (14%) Klebsiella spp. (10%) S. aureus (10%) |
| Selection | Comparability * | Outcome | Overall | |
|---|---|---|---|---|
| Beaucote V, et al. [13] |  | | | 8 |
| Gragueb–Chatti I, et al. [14] | | | | 8 |
| De Pascale G, et al. [15] | | | | 8 |
| De Santis V, et al. [16] | | | | 8 |
| Karolyi M, et al. [17] | | | | 7 |
| Luque-Paz D, et al. [18] | | | | 7 |
| Meawed T, et al. [19] | | | | 8 |
| Pickens C, et al. [20] | | | | 8 |
| Risa E, et al. [21] | | | | 7 |
| Rouyer M, et al. [22] | | | | 9 |
| Signorini L, et al. [23] | | | | 7 |
| Bardi T, et al. [24] | | | | 8 |
| Blonz G, et al. [25] | | | | 8 |
| Suarez-de-la-Rica A, et al. [26] | | | | 7 |
| Luyt C, et al. [27] | | | | 7 |
| Garcia-Vidal C, et al. [28] | | | | 8 |
| Giacobbe DR, et al. [29] | | | | 8 |
| Grasselli G, et al. [30] | | | | 8 |
| Maes M, et al. [31] | | | | 9 |
| Martinez-Guerra B, et al. [32] | | | | 8 |
| Moretti M, et al. [33] | | | | 8 |
| Razazi K, et al. [34] | | | | 9 |
| Rouze A, et al. [35] | | | | 9 |
| Sogaard KK, et al. [36] | | | | 7 |
| Vacheron CH, et al. [37] | | | | 8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Velásquez-Garcia, L.; Mejia-Sanjuanelo, A.; Viasus, D.; Carratalà, J. Causative Agents of Ventilator-Associated Pneumonia and Resistance to Antibiotics in COVID-19 Patients: A Systematic Review. Biomedicines 2022, 10, 1226. https://doi.org/10.3390/biomedicines10061226
Velásquez-Garcia L, Mejia-Sanjuanelo A, Viasus D, Carratalà J. Causative Agents of Ventilator-Associated Pneumonia and Resistance to Antibiotics in COVID-19 Patients: A Systematic Review. Biomedicines. 2022; 10(6):1226. https://doi.org/10.3390/biomedicines10061226
Chicago/Turabian StyleVelásquez-Garcia, Larry, Ana Mejia-Sanjuanelo, Diego Viasus, and Jordi Carratalà. 2022. "Causative Agents of Ventilator-Associated Pneumonia and Resistance to Antibiotics in COVID-19 Patients: A Systematic Review" Biomedicines 10, no. 6: 1226. https://doi.org/10.3390/biomedicines10061226