
Mortality in Severe Antibody Deficiencies Patients during the First Two Years of the COVID-19 Pandemic: Vaccination and Monoclonal Antibodies Efficacy

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Statistical Analysis of Numerical Data
3. Results
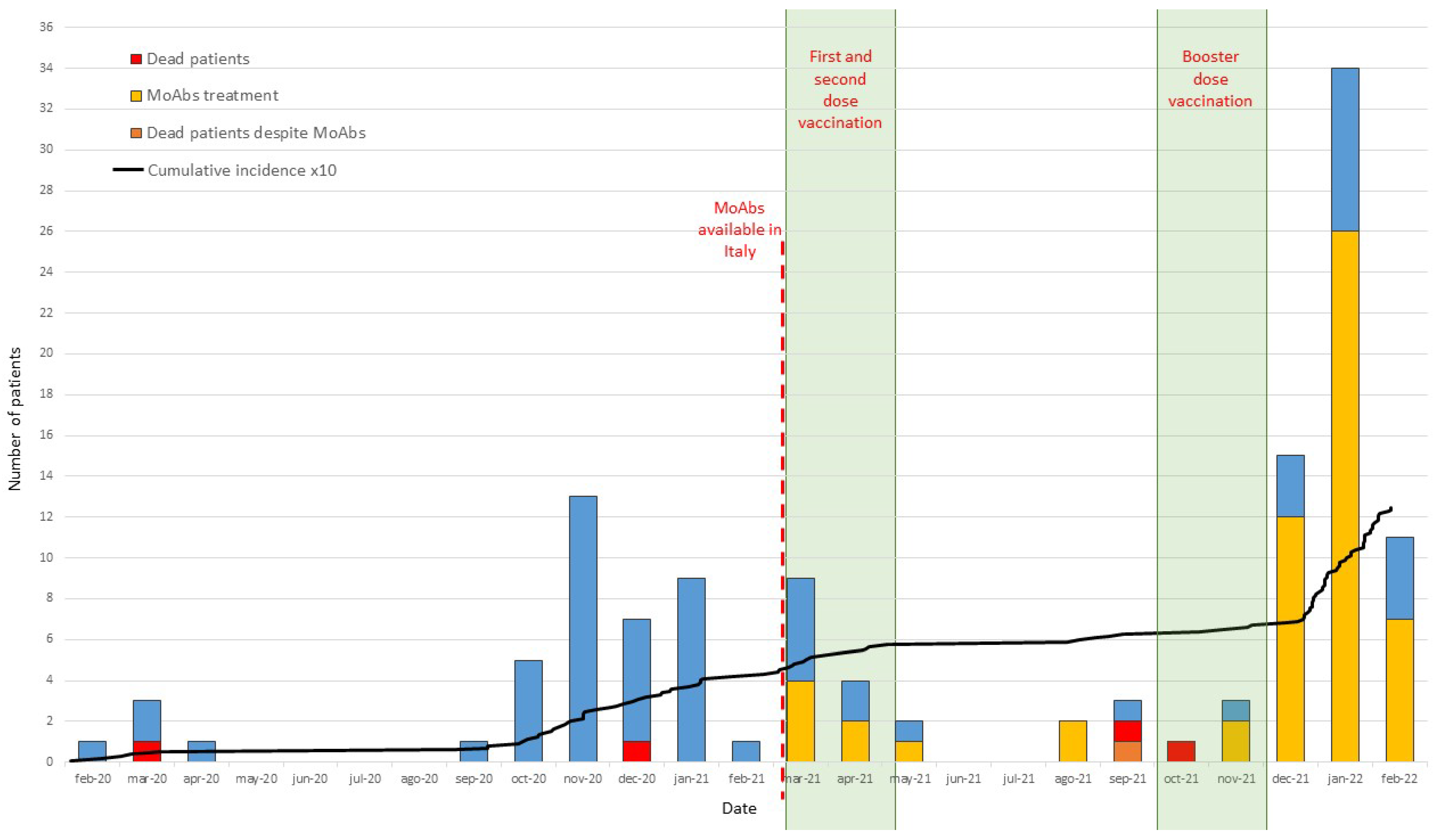
3.1. Incidence/Infection Rate
3.2. Vaccination and Monoclonal Antibodies Treatment
3.3. COVID-19 Disease Severity and Fatality Rate
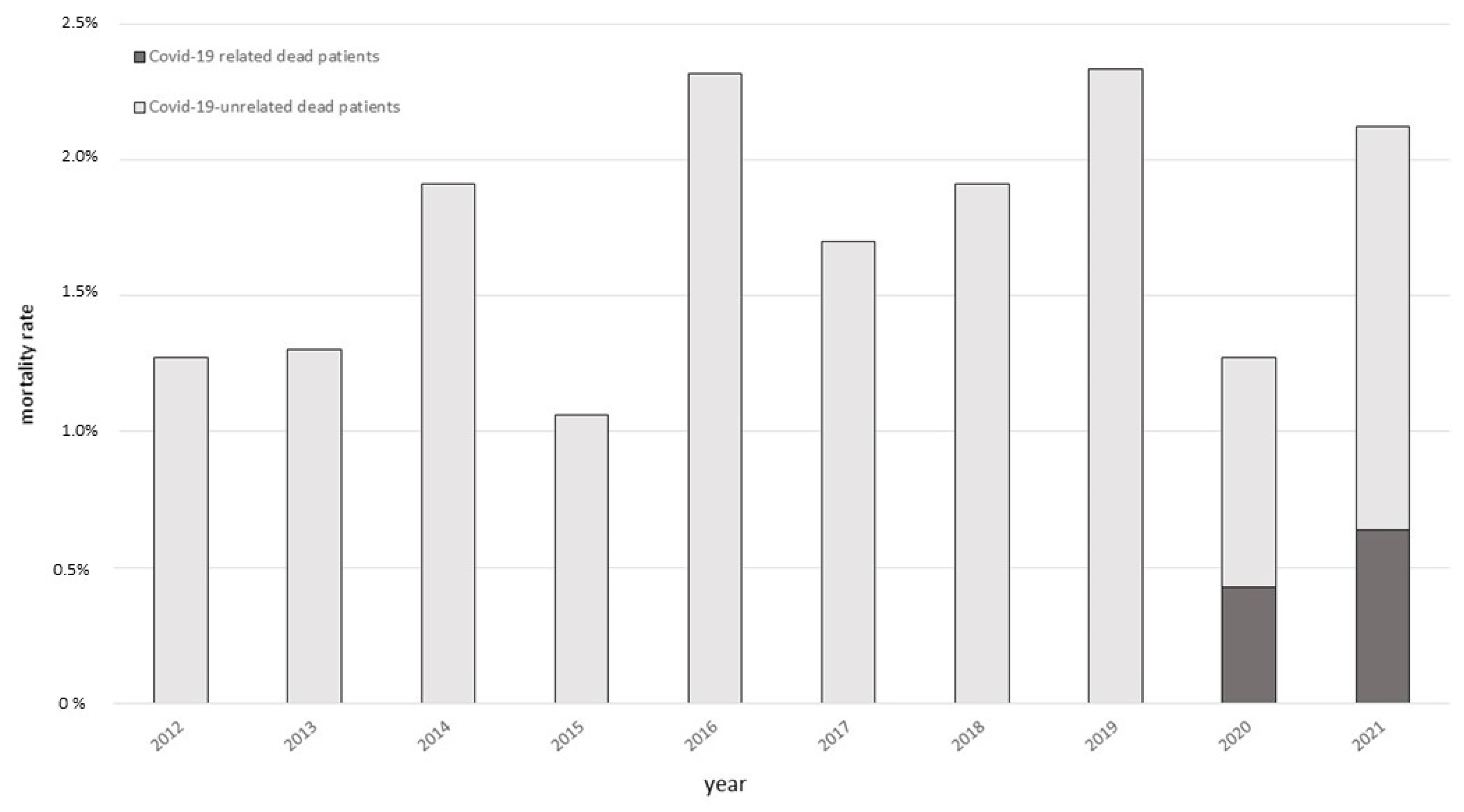
3.4. PADs Fatality Rate
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bucciol, G.; Tangye, S.G.; Meyts, I. Coronavirus disease 2019 in patients with inborn errors of immunity: Lessons learned. Curr. Opin. Pediatr. 2021, 33, 648–656. [Google Scholar] [CrossRef]
- Koerber, N.; Priller, A.; Yazici, S.; Bauer, T.; Cheng, C.C.; Mijočević, H.; Wintersteller, H.; Jeske, S.; Vogel, E.; Feuerherd, M.; et al. Dynamics of spike-and nucleocapsid specific immunity during long-term follow-up and vaccination of SARS-CoV-2 convalescents. Nat. Commun. 2022, 13, 153. [Google Scholar] [CrossRef] [PubMed]
- Terpos, E.; Karalis, V.; Sklirou, A.D.; Apostolakou, F.; Ntanasis-Stathopoulos, I.; Bagratuni, T.; Iconomidou, V.A.; Malandrakis, P.; Korompoki, E.; Papassotiriou, I.; et al. Third dose of the BNT162b2 vaccine results in very high levels of neutralizing antibodies against SARS-CoV-2: Results of a prospective study in 150 health professionals in Greece. Am. J. Hematol. 2022, 97, E147–E150. [Google Scholar] [CrossRef] [PubMed]
- Delmonte, O.M.; Bergerson, J.R.E.; Burbelo, P.D.; Durkee-Shock, J.R.; Dobbs, K.; Bosticardo, M.; Keller, M.D.; McDermott, D.H.; Rao, V.K.; Dimitrova, D.; et al. Antibody responses to the SARS-CoV-2 vaccine in individuals with various inborn errors of immunity. J. Allergy Clin. Immunol. 2021, 148, 1192–1197. [Google Scholar] [CrossRef] [PubMed]
- Bousfiha, A.; Jeddane, L.; Picard, C.; Ailal, F.; Bobby Gaspar, H.; Al-Herz, W.; Chatila, T.; Crow, Y.J.; Cunningham-Rundles, C.; Etzioni, A.; et al. The 2017 IUIS Phenotypic Classification for Primary Immunodeficiencies. J. Clin. Immunol. 2018, 38, 129–143. [Google Scholar] [CrossRef] [Green Version]
- Levin, E.G.; Lustig, Y.; Cohen, C.; Fluss, R.; Indenbaum, V.; Amit, S.; Doolman, R.; Asraf, K.; Mendelson, E.; Ziv, A.; et al. Waning Immune Humoral Response to BNT162b2 Covid-19 Vaccine over 6 Months. N. Engl. J. Med. 2021, 385, e84. [Google Scholar] [CrossRef]
- Fernandez Salinas, A.; Piano Mortari, E.; Terreri, S.; Milito, C.; Zaffina, S.; Perno, C.F.; Locatelli, F.; Quinti, I.; Carsetti, R. Impaired memory B-cell response to the Pfizer-BioNTech COVID-19 vaccine in patients with common variable immunodeficiency. J. Allergy Clin. Immunol. 2022, 149, 76–77. [Google Scholar] [CrossRef]
- Fernandez Salinas, A.; Mortari, E.P.; Terreri, S.; Quintarelli, C.; Pulvirenti, F.; Di Cecca, S.; Guercio, M.; Milito, C.; Bonanni, L.; Auria, S.; et al. SARS-CoV-2 Vaccine Induced Atypical Immune Responses in Antibody Defects: Everybody Does their Best. J. Clin. Immunol. 2021, 41, 1709–1722. [Google Scholar] [CrossRef]
- Meyts, I.; Bucciol, G.; Quinti, I.; Neven, B.; Fischer, A.; Seoane, E.; Lopez-Granados, E.; Gianelli, C.; Robles-Marhuenda, A.; Jeandel, P.Y.; et al. Coronavirus disease 2019 in patients with inborn errors of immunity: An international study. J. Allergy Clin. Immunol. 2021, 147, 520–531. [Google Scholar] [CrossRef]
- Ameratunga, R.; Longhurst, H.; Steele, R.; Lehnert, K.; Leung, E.; Brooks, A.E.S.; Woon, S.T. Common Variable Immunodeficiency Disorders, T-Cell Responses to SARS-CoV-2 Vaccines, and the Risk of Chronic COVID-19. J. Allergy Clin. Immunol. Pract. 2021, 9, 3575–3583. [Google Scholar] [CrossRef]
- WHO Working Group on the Clinical Characterisation and Management of COVID-19 Infection. A minimal common outcome measure set for COVID-19 clinical research. Lancet Infect. Dis. 2020, 20, e192–e197. [Google Scholar] [CrossRef]
- Milito, C.; Lougaris, V.; Giardino, G.; Punziano, A.; Vultaggio, A.; Carrabba, M.; Cinetto, F.; Scarpa, R.; DellePiane, R.M.; Baselli, L.; et al. Clinical outcome, incidence, and SARS-CoV-2 infection-fatality rates in Italian patients with inborn errors of immunity. J. Allergy Clin. Immunol. Pract. 2021, 9, 2904–2906.E2. [Google Scholar] [CrossRef] [PubMed]
- Planas, D.; Saunders, N.; Maes, P.; Guivel-Benhassine, F.; Planchais, C.; Buchrieser, J.; Bolland, W.H.; Porrot, F.; Staropoli, I.; Lemoine, F.; et al. Considerable escape of SARS-CoV-2 Omicron to antibody neutralization. Nature 2022, 602, 671–675. [Google Scholar] [CrossRef] [PubMed]
- Pulvirenti, F.; Milito, C.; Cinetto, F.; Salinas, A.F.; Terreri, S.; Mortari, E.P.; Auria, S.; Soccodato, V.; Miriam, L.; Nicastri, E.; et al. SARS-CoV-2 monoclonal antibody combination therapy in patients with COVID-19 and primary antibody deficiency. J. Infect. Dis. 2021, 225, 820–824. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Gonzalez-Rojas, Y.; Juarez, E.; Crespo Casal, M.; Moya, J.; Falci, D.R.; Sarkis, E.; Solis, J.; Zheng, H.; Scott, N.; et al. COMET-ICE Investigators. Early Treatment for Covid-19 with SARS-CoV-2 Neutralizing Antibody Sotrovimab. N. Engl. J. Med. 2021, 385, 1941–1950. [Google Scholar] [CrossRef]
- Cinetto, F.; Scarpa, R.; Pulvirenti, F.; Quinti, I.; Agostini, C.; Milito, C. Appropriate lung management in patients with primary antibody deficiencies. Expert. Rev. Respir. Med. 2019, 13, 823–838. [Google Scholar] [CrossRef] [Green Version]
- Quinti, I.; Soresina, A.; Guerra, A.; Rondelli, R.; Spadaro, G.; Agostini, C.; Milito, C.; Trombetta, A.C.; Visentini, M.; Martini, H.; et al. IPINet Investigators. Effectiveness of immunoglobulin replacement therapy on clinical outcome in patients with primary antibody deficiencies: Results from a multicenter prospective cohort study. J. Clin. Immunol. 2011, 31, 315–322. [Google Scholar] [CrossRef]
- Grau-Expósito, J.; Sánchez-Gaona, N.; Massana, N.; Suppi, M.; Astorga-Gamaza, A.; Perea, D.; Rosado, J.; Falcó, A.; Kirkegaard, C.; Torrella, A.; et al. Peripheral and lung resident memory T cell responses against SARS-CoV-2. Nat. Commun. 2021, 12, 3010. [Google Scholar] [CrossRef]
- Sette, A.; Crotty, S. Adaptive immunity to SARS-CoV-2 and COVID-19. Cell 2021, 184, 861–880. [Google Scholar] [CrossRef]
- Hoffmann, M.; Krüger, N.; Schulz, S.; Cossmann, A.; Rocha, C.; Kempf, A.; Nehlmeier, I.; Graichen, L.; Moldenhauer, A.S.; Winkler, M.S.; et al. The Omicron variant is highly resistant against antibody-mediated neutralization: Implications for control of the COVID-19 pandemic. Cell 2022, 185, 447–456.E11. [Google Scholar] [CrossRef]
- Friedmann, D.; Goldacker, S.; Peter, H.H.; Warnatz, K. Preserved Cellular Immunity Upon Influenza Vaccination in Most Patients with Common Variable Immunodeficiency. J. Allergy Clin. Immunol. Pract. 2020, 8, 2332–2340.E5. [Google Scholar] [CrossRef] [PubMed]
- Pizzolla, A.; Nguyen, T.H.O.; Smith, J.M.; Brooks, A.G.; Kedzieska, K.; Heath, W.R.; Reading, P.C.; Wakim, L.M. Resident memory CD8+ T cells in the upper respiratory tract prevent pulmonary influenza virus infection. Sci. Immunol. 2017, 2, eaam6970. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, H.; Durkee-Shock, J.; Jensen-Wachspress, M.; Kankate, V.V.; Lang, H.; Lazarski, C.A.; Keswani, A.; Webber, K.C.; Montgomery-Recht, K.; Walkiewicz, M.; et al. Robust Antibody and T Cell Responses to SARS-CoV-2 in Patients with Antibody Deficiency. J. Clin. Immunol. 2021, 41, 1146–1153. [Google Scholar] [CrossRef] [PubMed]
- Steiner, S.; Sotzny, F.; Bauer, S.; Na, I.K.; Schmueck-Henneresse, M.; Corman, V.M.; Schwarz, T.; Drosten, C.; Wendering, D.J.; Behrends, U.; et al. HCoV- and SARS-CoV-2 Cross-Reactive T Cells in CVID Patients. Front. Immunol. 2020, 11, 607918. [Google Scholar] [CrossRef]
- Sauerwein, K.M.T.; Geier, C.B.; Stemberger, R.F.; Akyaman, H.; Illes, P.; Fischer, M.B.; Eibl, M.M.; Walter, J.E.; Wolf, H.M. Antigen-Specific CD4+ T-Cell Activation in Primary Antibody Deficiency After BNT162b2 mRNA COVID-19 Vaccination. Front. Immunol. 2022, 13, 827048. [Google Scholar] [CrossRef]
- Quinti, I.; Locatelli, F.; Carsetti, R. The Immune Response to SARS-CoV-2 Vaccination: Insights Learned From Adult Patients With Common Variable Immune Deficiency. Front. Immunol. 2022, 12, 815404. [Google Scholar] [CrossRef]
- Stravalaci, M.; Pagani, I.; Paraboschi, E.M.; Pedotti, M.; Doni, A.; Scavello, F.; Mapelli, S.N.; Sironi, M.; Perucchini, C.; Varani, L.; et al. Recognition and inhibition of SARS-CoV-2 by humoral innate immunity pattern recognition molecules. Nat. Immunol. 2022, 23, 275–286. [Google Scholar] [CrossRef]
- Zhang, Q.; Bastard, P.; COVID Human Genetic Effort; Cobat, A.; Casanova, J.L. Human genetic and immunological determinants of critical COVID-19 pneumonia. Nature 2022, 603, 587–598. [Google Scholar] [CrossRef]
- Quinti, I.; Mitrevski, M. Modulatory Effects of Antibody Replacement Therapy to Innate and Adaptive Immune Cells. Front. Immunol. 2017, 8, 697. [Google Scholar] [CrossRef] [Green Version]
- Volk, A.; Covini-Souris, C.; Kuehnel, D.; De Mey, C.; Römisch, J.; Schmidt, T. SARS-CoV-2 Neutralization in Convalescent Plasma and Commercial Lots of Plasma-Derived Immunoglobulin. BioDrugs 2022, 36, 41–53. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Asymptomatic/Mild n (%) | Moderate/Severe n (%) | Hospitalizations n (%) | Deaths n (%) | ||
|---|---|---|---|---|---|
| 1st YEAR (n = 41) | All PADs | 25 (60.98%) | 16 (39.02%) | 16 (39.02%) | 2 (4.87%) |
| CVID only | 22 (59.5%) | 15 (40.5%) | 15 (40.5%) | 2 (5.4%) | |
| 2nd YEAR (n = 84) | All PADs | 70 (83.33%) | 14 (16.67%) | 14 (16.67%) | 3 (3.57%) |
| CVID only | 64 (85.3%) | 11 (14.7%) | 11 (14.7%) | 2 (2.67%) |
| Hospitalization | n (%) | Unadjusted OR (95% CI) | Adjusted OR (95% CI) | ||
|---|---|---|---|---|---|
| Vaccinated vs. not vaccinated | 9 (15.5) vs. 6 (24.0) | 0.582 (0.182–1.857) | p = 0.360 * | 0.453 (0.131–1.561) | p = 0.210 § |
| MoAbs vs. not MoAbs | 6 (10.7) vs. 9 (32.1) | 0.253 (0.079–0.808) | p = 0.020 * | 0.187 (0.053–0.653) | p = 0.009 # |
| Severe Disease | n(%) | Unadjusted OR (95% CI) | Adjusted OR (95% CI) | ||
| Vaccinated vs. not vaccinated | 3 (5.2) vs. 2 (8.0) | 0.627 (0.098–4.006) | p = 0.622 * | 0.664 (0.096–4.564) | p = 0.677 § |
| MoAbs vs. not MoAbs | 1 (1.8) vs. 4 (14.3) | 0.109 (0.012–1.028) | p = 0.053 * | 0.095 (0.009–0.951) | p = 0.045 # |
| Mortality | n(%) | Unadjusted OR (95% CI) | Adjusted OR (95% CI) | ||
| Vaccinated vs. not vaccinated | 2 (3.4) vs. 1 (4) | 0.857 (0.074–9.909) | p = 0.902 * | 0.781 (0.059–10.294) | p = 0.851 § |
| MoAbs vs. not MoAbs | 1 (81.8) vs. 2 (7.1) | 0.236 (0.020–2.726) | p = 0.248 * | 0.110 (0.013–2.147) | p = 0.167 # |
| Patient | Sex | Age | PID | Comorbidity | Date of Infection | Vaccination Status | MoABs Therapy |
|---|---|---|---|---|---|---|---|
| 1 | F | 59 | CVID | GLILD, chronic respiratory failure | March 2020 | Not done | No |
| 2 | M | 52 | CVID | GLILD, bilateral lung transplantation, chronic respiratory failure | December 2020 | Not done | No |
| 3 | F | 48 | CVID | GLILD, chronic respiratory failure | September 2021 | 2 doses | Yes |
| 4 | M | 78 | CVID | Chronic heart failure, bronchiectasis | September 2021 | 2 doses | No |
| 5 | M | 46 | XLA | Post-poliomyelitis flaccid paralysis. Chronic obstructive pulmonary disease | October 2021 | Refused | No |
| Year | All Causes of Death |
|---|---|
| 2012 | 4, cancer; 1, CMV disseminated infection; 1, autoimmune cytopenias |
| 2013 | 2, cancer; 1, chronic lung disease *; 1, CMV disseminated infection; 2, enteropathy |
| 2014 | 4, cancer; 3, chronic lung disease *; 1, autoimmune cytopenias; 1, enteropathy |
| 2015 | 2, cancer; 2, chronic lung disease *, 1, enteropathy |
| 2016 | 5, cancer; 3, autoimmune cytopenias; 2, chronic lung disease *; 1, hepatic disease |
| 2017 | 2, cancer; 2, autoimmune cytopenias; 1, chronic lung disease *; 3, enteropathy |
| 2018 | 3, cancer; 3, autoimmune cytopenias; 2, chronic lung disease *; 1, hepatic disease |
| 2019 | 3, cancer; 3, hepatic diseases; 3, chronic lung disease *; 1, autoimmune cytopenias; 1 enteropathy |
| 2020 | 3, chronic lung disease *; 1, hepatic disease; 2, COVID-19 |
| 2021 | 2, cancer; 3, chronic lung disease *; 1, meningitis; 1, autoimmune cytopenias; 3, COVID-19 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Milito, C.; Cinetto, F.; Palladino, A.; Garzi, G.; Punziano, A.; Lagnese, G.; Scarpa, R.; Rattazzi, M.; Pesce, A.M.; Pulvirenti, F.; et al. Mortality in Severe Antibody Deficiencies Patients during the First Two Years of the COVID-19 Pandemic: Vaccination and Monoclonal Antibodies Efficacy. Biomedicines 2022, 10, 1026. https://doi.org/10.3390/biomedicines10051026
Milito C, Cinetto F, Palladino A, Garzi G, Punziano A, Lagnese G, Scarpa R, Rattazzi M, Pesce AM, Pulvirenti F, et al. Mortality in Severe Antibody Deficiencies Patients during the First Two Years of the COVID-19 Pandemic: Vaccination and Monoclonal Antibodies Efficacy. Biomedicines. 2022; 10(5):1026. https://doi.org/10.3390/biomedicines10051026
Chicago/Turabian StyleMilito, Cinzia, Francesco Cinetto, Andrea Palladino, Giulia Garzi, Alessandra Punziano, Gianluca Lagnese, Riccardo Scarpa, Marcello Rattazzi, Anna Maria Pesce, Federica Pulvirenti, and et al. 2022. "Mortality in Severe Antibody Deficiencies Patients during the First Two Years of the COVID-19 Pandemic: Vaccination and Monoclonal Antibodies Efficacy" Biomedicines 10, no. 5: 1026. https://doi.org/10.3390/biomedicines10051026