1. Introduction
Secondary lymphedema is the most common long-term complication of cancer treatment, particularly following axillary lymph node dissection for breast cancer (15–50% of patients) and treatment of other solid tumors (15–20% of patients), such as melanoma, sarcoma, and gynecological and urologic malignancies [
1,
2,
3,
4]. The number of patients with this lifelong disease increases each year due to improved long-term survival following cancer treatment and rising rates of important risk factors for the disease such as obesity, adjuvant radiation therapy, and advanced age [
5,
6,
7].
Although lymphedema is a highly morbid, progressive disease that significantly impairs function and quality of life, there is no medical or surgical cure. Instead, patients are treated with palliative measures using compression garments and physical therapy to prevent disease progression and relieve symptoms [
8,
9,
10,
11]. These treatments are time-consuming and expensive, leading to a high degree of non-compliance and disease progression [
9]. Surgical treatments for lymphedema have recently been developed and are helpful in some patients, but these treatments are invasive and not very effective for patients with advanced lymphedema.
The development of novel therapies for secondary lymphedema has been limited because the pathophysiology of this disease is poorly understood. We know that lymphatic injury resulting from cancer surgery is a critical initiator of this disease, but it is not clear why some patients develop lymphedema while others do not. Although many studies have identified clinical risk factors for lymphedema, the mechanisms by which these comorbid conditions modulate the pathophysiology of the disease are less well-defined. Perhaps most intriguingly, it is not fully understood why, in most cases, lymphedema develops in a delayed manner, months or years after surgery [
12]. These epidemiologic features suggest that additional pathologic events (i.e., “second hits”) are necessary for lymphedema to develop. Therefore, identifying the sequence of events that translates lymphatic injury to lymphedema may provide effective therapeutic targets.
Several research groups have hypothesized that chronic inflammation may be an important regulator in the pathological sequence of lymphedema development. Although chronic inflammation is a histologic feature of lymphedema, Rockson and colleagues were the first to demonstrate that persistent inflammation may also serve as a critical pathologic driver of the disease [
13]. Our group also analyzed clinical lymphedema biopsy specimens and mouse models of lymphedema to identify the inflammatory signature of lymphedema. By comparing the normal and lymphedematous limbs of women with unilateral breast cancer–related lymphedema (BCRL), we found that the severity of lymphedema, increasing International Society of Lymphology stage, positively correlates with the number of CD4
+ Th cells in the dermis and subcutaneous tissues of the lymphedematous limb [
14]. In other studies, we showed that transgenic mice lacking Th cells, or inhibition of Th cell responses using neutralizing antibodies or tacrolimus, a calcineurin inhibitor that decreases T cell proliferation by antagonizing IL2, can both prevent the development of lymphedema and treat it once it has developed [
15,
16,
17]. In contrast, depletion of cytotoxic T cells, macrophages, or B-cells had no effect or worsened the phenotype of lymphedema [
15,
16,
18]. More recently, other research groups have also shown that Th cells play a crucial role in the pathophysiology of lymphedema, confirming our previous findings [
19,
20].
We also found that Th2 differentiation is an important regulator of lymphedema development [
14,
21]. Clinical biopsy specimens from patients with unilateral BCRL showed an increased number of Th2 cells infiltrating into the dermis and subcutaneous tissues of lymphedematous tissues compared with normal skin [
14]. Using mouse models, we showed that shortly following lymphatic injury, DCs and Langerhans cells just below the epidermis are activated and migrate to the regional lymph nodes [
16]. There, these antigen-presenting cells promote differentiation of naïve Th cells to a mixed Th1/Th2 phenotype that expresses skin-homing receptors that guide them to the skin distal to the zone of lymphatic injury. Transgenic mice that have impaired Th2 differentiation capability do not develop lymphedema following lymphatic injury [
21]. In contrast, mice with impaired Th1 differentiation capacity develop lymphedema, and the severity of the disease is indistinguishable from wild-type controls. Similarly, treatment of mice with neutralizing antibodies against IL4 or IL13, cytokines necessary for differentiation of naïve Th cells to Th2 phenotype, not only prevented the development of lymphedema in preclinical mouse models but also treated lymphedema once it was established [
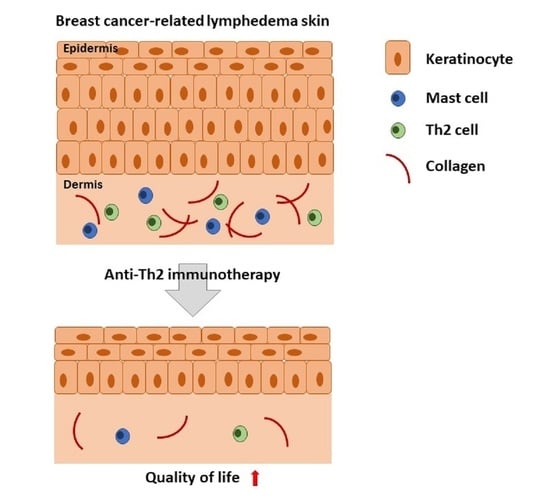
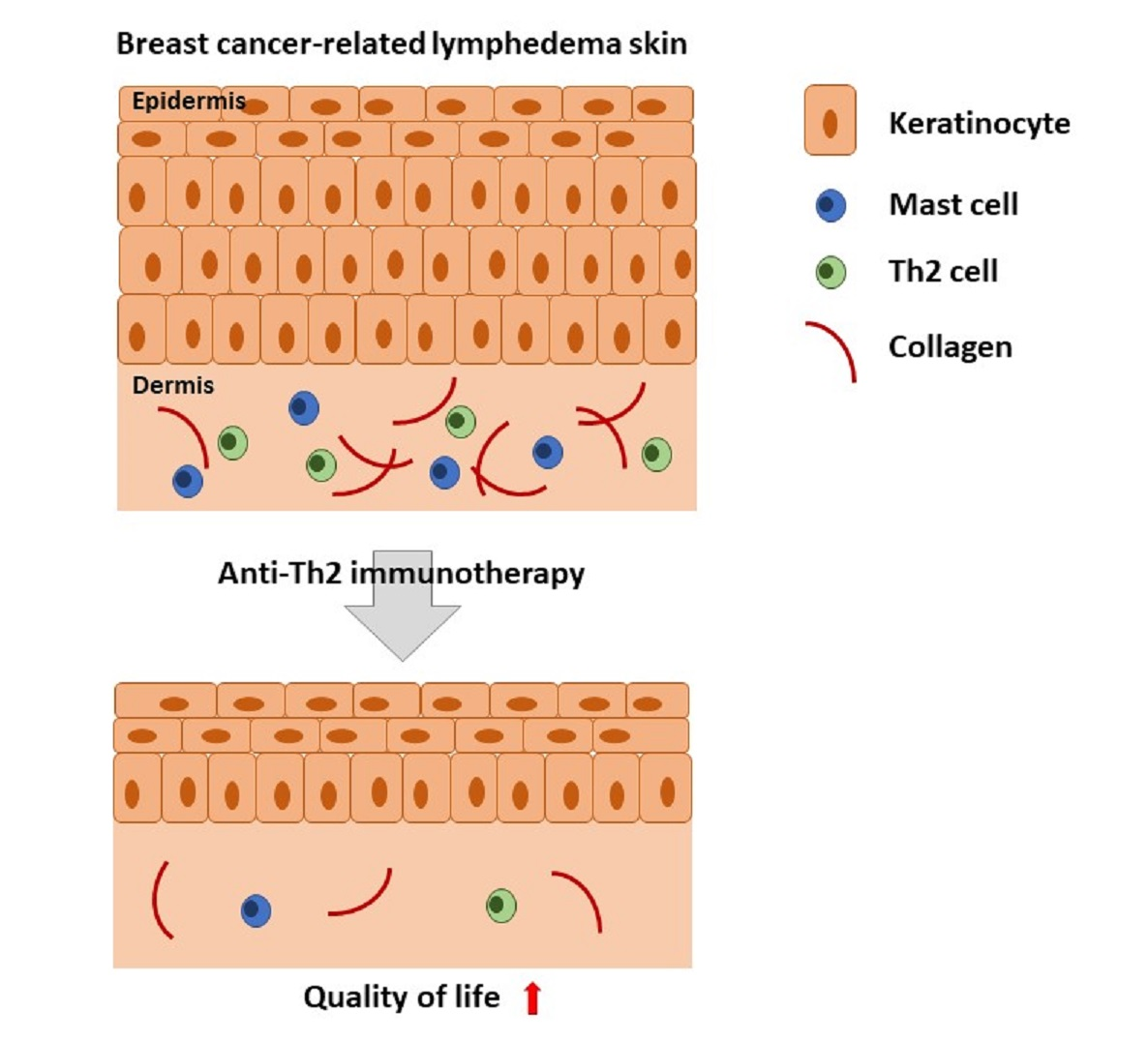
14]. Mechanistically, we found that cytokines derived from Th2 cells (IL4, IL13) increase lymphatic leakiness, increase collagen deposition and fibrosis in the dermis and collecting lymphatics, inhibit lymphangiogenesis, and impair lymphatic pumping [
14,
22]. These findings led us and others to hypothesize that lymphedema is a fibroproliferative disease with the progressive replacement of functional parenchyma (lymphatic vessels) with fibrous tissues [
20]. This hypothesis is supported by the fact that fibroproliferative conditions are common; fibrosis is a preserved end-pathway for chronic inflammation and organ failure in the heart, lung, pancreas, skin, and kidney [
23]. The fibroproliferative hypothesis also explains why lymphedema develops in a delayed fashion following surgery since the fibrotic threshold needed to develop symptoms takes time to happen. Variability in fibrotic responses among patients may also provide a rationale for the clinical observation that the severity of secondary lymphedema is highly variable and difficult to predict. Thus, inhibition of fibrosis with anti-Th2 therapies may be a viable means of clinically preventing or treating lymphedema.
Targeted therapeutics that inhibit immune responses are now commonly used to treat a variety of chronic disorders, such as atopic dermatitis, psoriasis, ankylosing spondylitis, inflammatory bowel disease, asthma, and rheumatoid arthritis. These treatments have significantly reduced treatment costs and improved outcomes by decreasing side effects of traditional anti-inflammatory therapies such as corticosteroids and non-specific immunosuppressants. In most cases, monoclonal antibodies inhibit cytokines or cytokine receptors, thereby blocking the inflammatory pathway responsible for the disease. This approach has also been used for Th2 disorders by blocking the activity of both IL4 and IL13 since these cytokines share a common receptor (IL4-Rα) and have overlapping biologic activity. Dupilumab, a monoclonal antibody that binds the alpha chain of IL4-Rα, is FDA approved for the treatment of adult patients with moderate-severe atopic dermatitis who have failed treatment with topical agents [
24]. This drug has also shown promising results with chronic sinusitis and nasal polyposis [
25] and bullous pemphigoid [
26]. Other uses of IL4 and IL13 antibodies have been developed and used in clinical trials for Th2-mediated diseases, including eosinophilic esophagitis, some forms of asthma, and pulmonary fibrosis. Based on this rationale, the purpose of this study was to assess the safety and efficacy of a combination treatment with monoclonal antibodies that block both IL4 and IL13 (QBX258) for the treatment of patients with BCRL.
4. Discussion
In this pilot study, we utilized an immunotherapy approach to treat secondary lymphedema and found that these treatments are well-tolerated, accrual to a study of this type is feasible, and that patients are highly motivated to participate. Given the nature of this disease and our many exclusion criteria, we were pleased with the accrual of patients to the trial and would have been successful in recruiting our goal number had we not been limited by the drug expiration. Although our patients experienced some adverse events, these issues were mostly self-limited and minor. One patient developed lymphedema-related cellulitis approximately 6 weeks after starting therapy; however, this patient had a history of cellulitis in the past (most recently 6 months before the study). Recurrent cellulitis occurs in about 30% of patients with lymphedema and is a significant cause of morbidity in this patient population. Nevertheless, the patient recovered after intravenous antibiotics.
One patient, who had a history of locally advanced breast cancer, developed pulmonary metastasis after completing drug therapy in our trial. Although causality cannot be ruled out, given the aggressive nature of her underlying disease process this event is unfortunately not unexpected. Indeed, before the start of our trial, we were very concerned about the potential for immunotherapy to increase the risk of cancer recurrence or tumor metastasis since T cell responses play a key role in tumor immune responses [
47,
48]. However, previous clinical and experimental studies suggest that Th2 cytokines promote tumor growth and metastasis and that inhibition of Th2 differentiation may potentiate tumor immune responses [
47,
49,
50]. Breast tumors are infiltrated by Th2 cells that strongly express IL4 and IL13, and these cytokines promote tumor growth by directly interacting with tumor cells, inhibiting DC responses and regulating the expression of cancer cell differentiation markers. Activation of IL4/IL13 signaling pathways increases breast cancer invasion and propensity for lung metastasis [
51]. Importantly, the blockade of Th2 responses increases tumor surveillance by immune cells and inhibits tumor growth and metastasis in various tumor types, including breast cancer [
47,
48,
52,
53,
54]. These findings led some authors to propose that the blockade of Th2 responses may be a viable strategy for breast cancer treatment suggesting that these treatments would also be safe for the treatment of BCRL [
55].
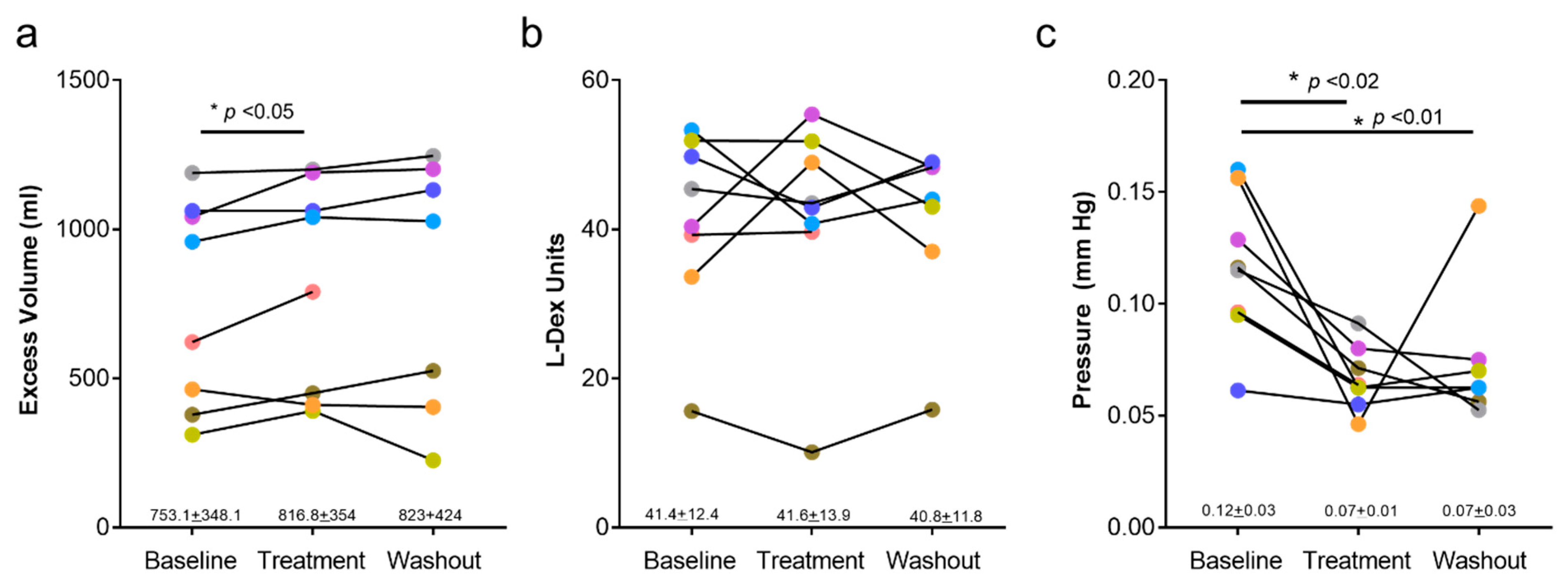
A disappointing finding in our study was that QBX258 treatment was not effective in decreasing arm volumes (in fact, arm volumes were slightly increased after treatment). This result may be a statistical error because we did not reach our accrual goal. It is also possible that this increase in volume was related to avoiding manual lymphatic massage or high compression garments during the study period. It is also possible that our inclusion criteria of a relatively large baseline volume differential (>300 cc) biased our selection towards patients with more advanced lymphedema in whom drug treatment may be less effective or who may require longer treatments to promote reversal of the chronic pathologic changes. Fibroadipose deposition in these patients, such as end-stage changes in other fibrotic disorders, may not be reversible. This hypothesis is supported by the finding that surgical treatments for lymphedema are most effective for patients with early-stage (stage 0 or 1) disease [
56]. Our findings suggest that future trials may be more meaningful if they are geared towards patients with an earlier-stage disease or if more sensitive primary outputs (e.g., patient-reported outcomes, skin tonometry, L-Dex, and histologic examination) are selected.
Other investigators have also reported on the use of anti-inflammatory treatments in patients with lymphedema. For example, Rockson and colleagues used mouse models of lymphedema to show that the molecular profile of the disease is characterized by inflammation, fibrosis, and oxidative stress [
57]. In subsequent preclinical studies, these authors found that treatment with non-steroidal anti-inflammatory medications (ketoprofen) decreases inflammation and improves lymphedema [
13,
57]. These findings led to a clinical trial to test the efficacy of ketoprofen for the treatment of lymphedema. The study design included an initial open-label treatment phase (21 patients) followed by a randomized controlled study in which 34 patients with either primary or secondary lymphedema of the upper or lower extremity were treated with ketoprofen twice daily (16 patients) or placebo (18 patients) for 4 months [
58]. This study, similar to ours, showed that treatment with ketoprofen improved skin histologic examination (decreased thickness and improved histopathology score) and decreased skin infiltration with macrophages and neutrophils. However, similar to the findings of our current study, ketoprofen treatment did not reduce the overall limb volumes or decrease tissue fluid content as assessed by bioimpedance measurements. More recent studies from Rockson and colleagues have shown that the therapeutic benefits of ketoprofen are attributable to the inhibition of leukotriene B
4 (LTB
4) [
59]. Bestatin, an LTB
4 inhibitor, improved histologic findings of lymphedema, decreased inflammation, and enhanced lymphatic function in a mouse model of lymphedema. Interestingly, low concentrations of LTB
4 improved lymphangiogenesis; however, higher concentrations of this molecule, as found in patients with lymphedema, inhibit lymphangiogenesis and lymphatic vessel sprouting. A recent phase 2 clinical trial with Bestatin (ULTRA trial) finished enrollment, and molecular studies of treatment responses are underway (Stanley Rockson, personal communication).
Several recent studies have shown that doxycycline is effective for the treatment of secondary lymphedema caused by filarial infections and that these improvements may be related to the anti-Th2 effects of this drug [
20,
60]. For example, in a clinical trial of 162 patients randomized to treatment with either amoxicillin (control group), doxycycline, or placebo for 6 weeks, found that patients treated with doxycycline had significant reductions in the severity of lymphedema 12 and 24 months after treatment. Nearly 44% of patients treated with doxycycline had decreased lymphedema stage at these time points; in contrast improvements were only noted in 3.2% and 5.6% of the patients treated with amoxicillin or placebo, respectively [
60]. In support of our findings suggesting that Th2 cytokines play a role in the pathophysiology of secondary lymphedema, a more recent report showed that improvements resulting from doxycycline treatment were related to decreased Th2 inflammatory responses in a mouse model of filariasis [
20]. Taken together, these findings suggest that secondary lymphedema resulting from either surgical injury or helminth infection and lymphatic obstruction may share a common pathophysiology and that treatments aimed at this pathway may be effective.
Patients with lymphedema have a substantially decreased quality of life [
61] and, to our knowledge, ours is the first study in which patient-reported outcomes were analyzed using a validated questionnaire following drug treatment. We noted significant improvements in the physical and social but not psychological dimensions of our quality of life measures after treatment with QBX258. These improvements were statistically significant overall, with five out of eight patients reporting improved outcomes. Improvements with drug therapy disappeared, returning to baseline levels in the washout period after the drug was discontinued. Although it is possible that improvements in some patients were simply a placebo effect due to the study design, it is also possible that these results reflect subtle improvements in pathological changes that are not reflected by gross changes such as limb volume measurements. Another possibility is that changes in the psychological dimension are less responsive to treatment due to the chronic nature of the disease process. Our findings are consistent with Toyserkani et al., who recently reported their results on a preliminary study on the use of adipose-derived regenerative cells to treat BCRL in 10 patients [
62]. In this study, women with unilateral stage I or II BCRL with an average excess volume of 300 cc were treated with adipose-derived stem cells injected into the axillary area and evaluated with measurements and quality of life questionnaires (disabilities of the arm, shoulder, and hand [DASH] outcome and Lymphedema Quality of Life [LYMQOL]) 1, 3, and 6 months after treatment. Similar to the findings in our study, Toyserkani et al. found that stem cell treatments did not decrease arm volume or dual energy x-ray absorptiometry (DXA); however, the authors noted significant improvements in physical findings, such as a sensation of heaviness or tension, as well as the overall DASH scores. Interestingly, changes in the psychological aspects of lymphedema, as assessed by LYMQOL, did not improve with stem cell therapy, suggesting that these impairments may be more challenging to treat or may reflect complex psychological issues related to cancer diagnosis and treatment.
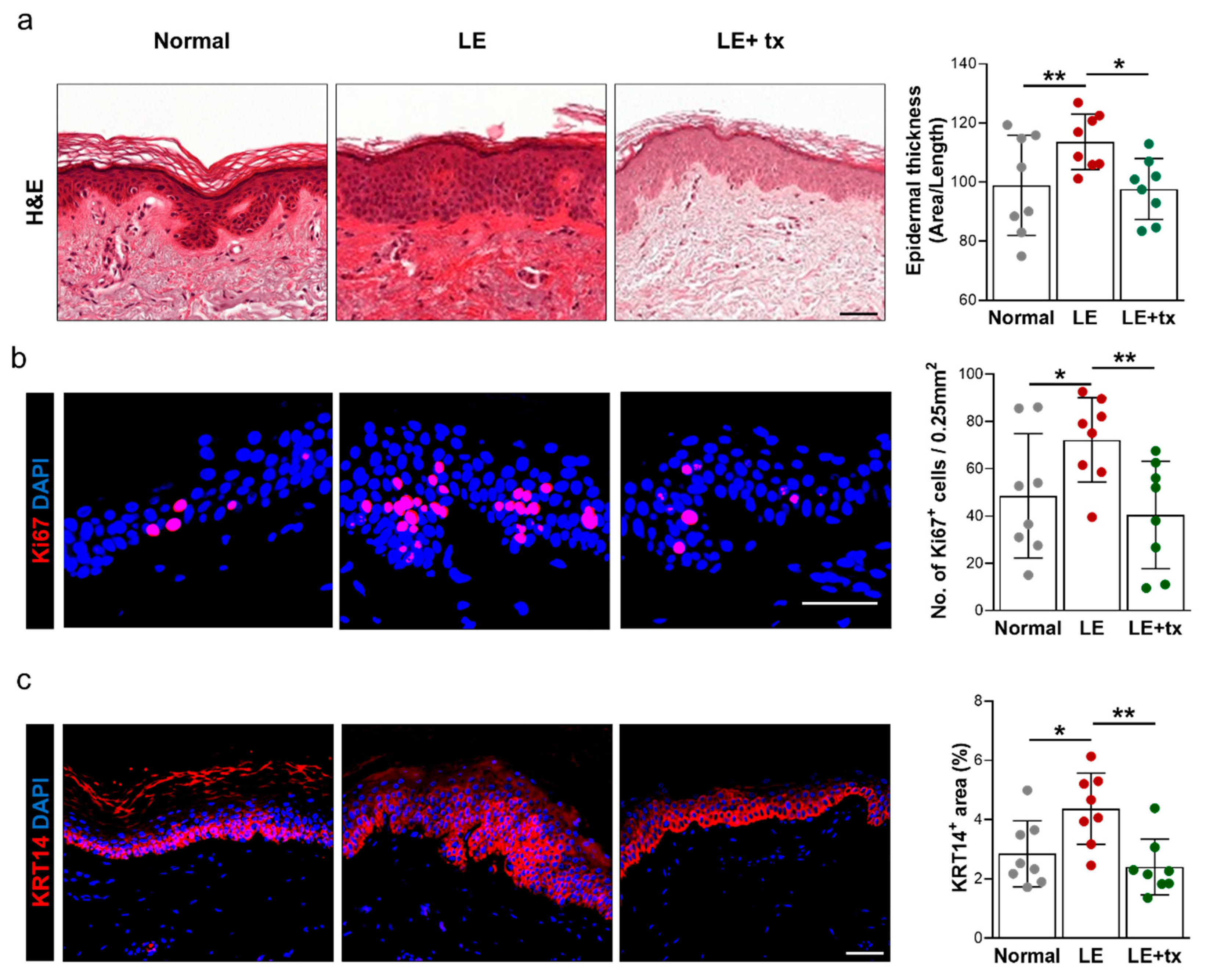
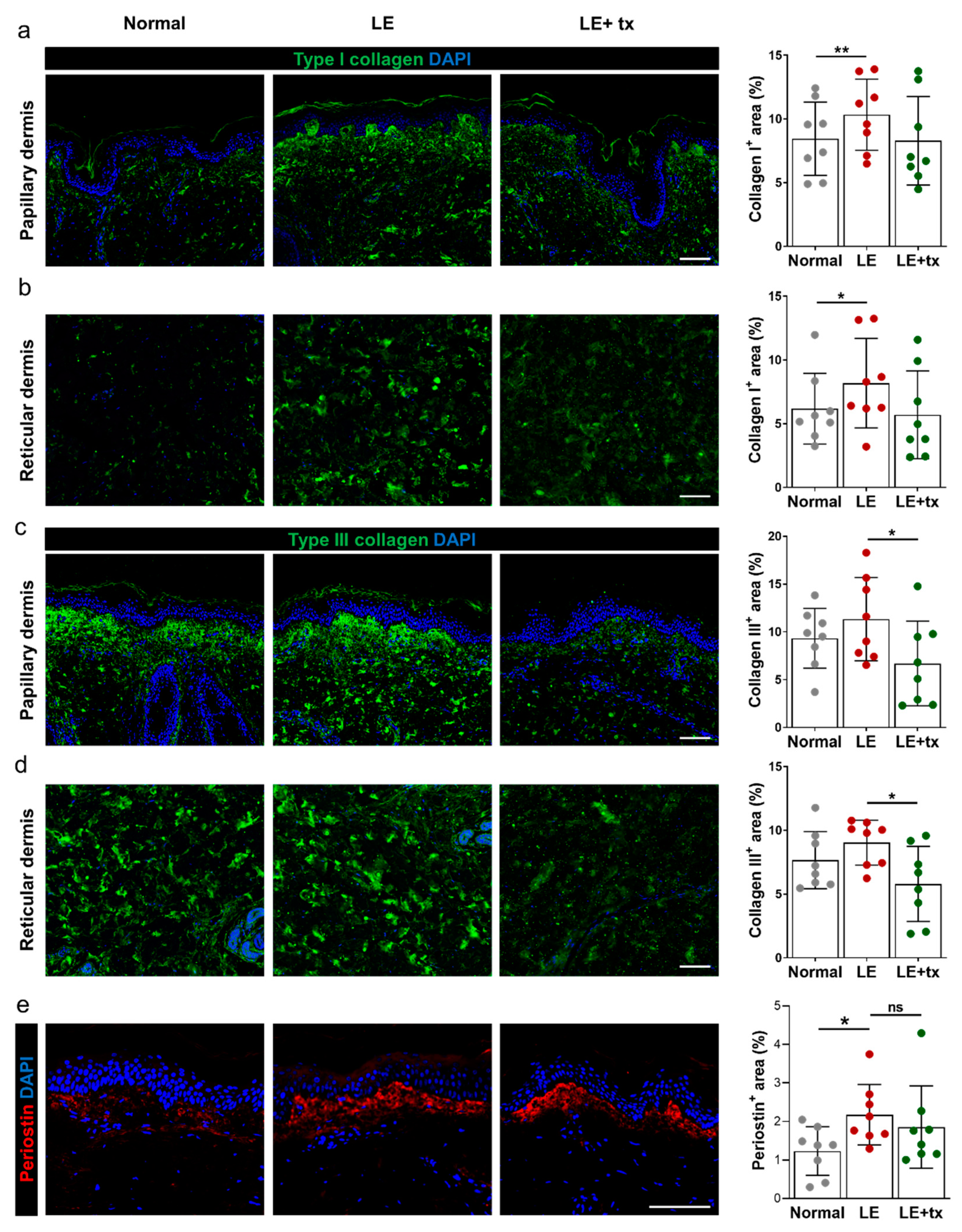
Our hypothesis that treatment with QBX258 results in subtle but significant tissue changes that may be responsible for improvements in quality of life scales and decreased skin fibrosis as reflected by skin tonometry is supported by our histologic analysis. In these studies, we noted significant decreases in hyperkeratosis, epidermal proliferation, type III collagen deposition, and a decrease in the number of infiltrating mast cells in biopsy samples obtained from the lymphedematous arm compared with the normal contralateral limb. Indeed, consistent with our findings with skin tonometry, we found that the thickness of the epidermis in the lymphedematous limb decreased to levels that were equivalent to the normal arm after 4 months of treatment with QBX258. We also noted decreases in the number of CD4
+ cells and type I collagen deposition. However, these differences did not reach statistical significance, possibly because our patient accrual was lower than expected. These findings are supported by Rockson et al., who showed that treatment with ketoprofen improved pathological skin changes in lymphedema [
58]. Our findings are also supported by our previous studies in which we have shown surgical treatment of lymphedema not only improves the symptoms of lymphedema but also improves pathological skin changes [
63].
Interestingly, we found that patients with lymphedema have significantly increased expression of Th2-inducing cytokines (TSLP, IL33, IL25) in the epidermal cells of the lymphedematous limb, and that treatment with QBX258 decreased or normalized these changes. This finding is important and suggests that epidermal cells may play a role in the pathophysiology of lymphedema and may help coordinate or initiate chronic Th2 responses. This hypothesis is supported by previous studies implicating epidermal cell expression of these cytokines in the pathophysiology of other atopic diseases, including atopic dermatitis, asthma, allergic rhinoconjunctivitis, and eosinophilic esophagitis [
43,
44,
45,
46,
64,
65].
TSLP is a member of the IL2 cytokine family and is expressed primarily by epithelial cells in the skin, lungs, and the gut. TSLP expression can be induced by bacterial products, inflammatory cytokines, or injury and is required for antiparasitic responses by regulating Th2 cytokine expression [
66,
67]. In addition, TSLP has been implicated in breast cancer pathogenesis by regulating the DC expression of OX40L, differentiating the Th2 cells, and increasing production of IL13 [
47]. Consistent with our findings in lymphedematous skin, keratinocytes are significant producers of TSLP, and the expression of TSLP increased the skin lesions of patients with atopic dermatitis [
68]. Experimental overexpression of TSLP in keratinocytes or intradermal injections of this cytokine, by acting on DCs and other mechanisms, result in the development of atopic dermatitis in mice, infiltration of Th2 differentiated CD4
+ cells, and systemic Th2 inflammatory responses [
67,
68,
69,
70,
71]. TSLP also acts synergistically with IL1 and TNF to activate mast cells that produce high levels of Th2 cytokines [
66]. Mast cells, in turn, can regulate epithelial TSLP expression in allergic rhinitis [
44]. The role of mast cells in lymphedema pathophysiology remains unknown; however, our findings that mast cell numbers are increased in lymphedematous skin and return to normal levels following QBX258 treatment suggest that these cells may play a role in this disease.
Several clinical trials have targeted TSLP. For example, Tezepelumab is a monoclonal human IgG2 that neutralizes TSLP by interfering with its receptor binding. A phase 2 clinical trial showed that treatment with Tezepelumab decreased the rates of asthma exacerbations in patients with moderate to severe disease over a 1-year period [
72]. This drug also showed improvement in a study of 113 adults with atopic dermatitis over a 12-week period, but this result did not achieve statistical significance due to greater than expected improvements in placebo-treated patients [
73]. Our study’s findings suggest that TSLP may also be a target for lymphedema treatment and that additional studies are warranted.
IL33 is a member of the IL1 family of cytokines and, similar to TSLP, has been implicated in various atopic diseases including atopic dermatitis, eosinophilic esophagitis, and asthma by genome-wide association studies as well as by studies demonstrating increased expression of IL33 in affected tissues [
45,
46,
64,
74,
75,
76]. Levels of IL33 expression correlate with the severity of atopic dermatitis [
77]. IL33 is expressed by epithelial cells of the skin, gut, and lung and acts on naïve CD4
+ cells to promote Th2 differentiation and activation of mast cells and eosinophils [
76,
78]. Consistent with the findings from our study, IL33 is expressed in the nucleus of keratinocytes but is released in pathological conditions [
78,
79]. IL33 is also expressed by activated mast cells [
79], and these cells can modulate IL33 activity by processing the full-length protein [
80].
IL25, similar to IL33 and TSLP, induces Th2-biased responses, promotes the expansion of splenic plasma cells and eosinophils, and increases expression of IL4 and IL13 [
81]. IL25 is thought to amplify atopic inflammatory reactions by increasing the expression of Th2 cytokines such as IL13 and IL4 [
81] and can cause mast cell degranulation [
82]. Our findings suggest that the expression of TSLP, IL33, and IL25 is increased in the epidermis of the lymphedematous skin and that treatment with QBX258 decreases this response. These findings require additional study and suggest that epidermal cells may play a role in the pathology of lymphedema by coordinating or amplifying Th2 responses.


 ,
, 







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}