
Sarcopenia Worsening One Month after Transarterial Radioembolization Predicts Progressive Disease in Patients with Advanced Hepatocellular Carcinoma

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
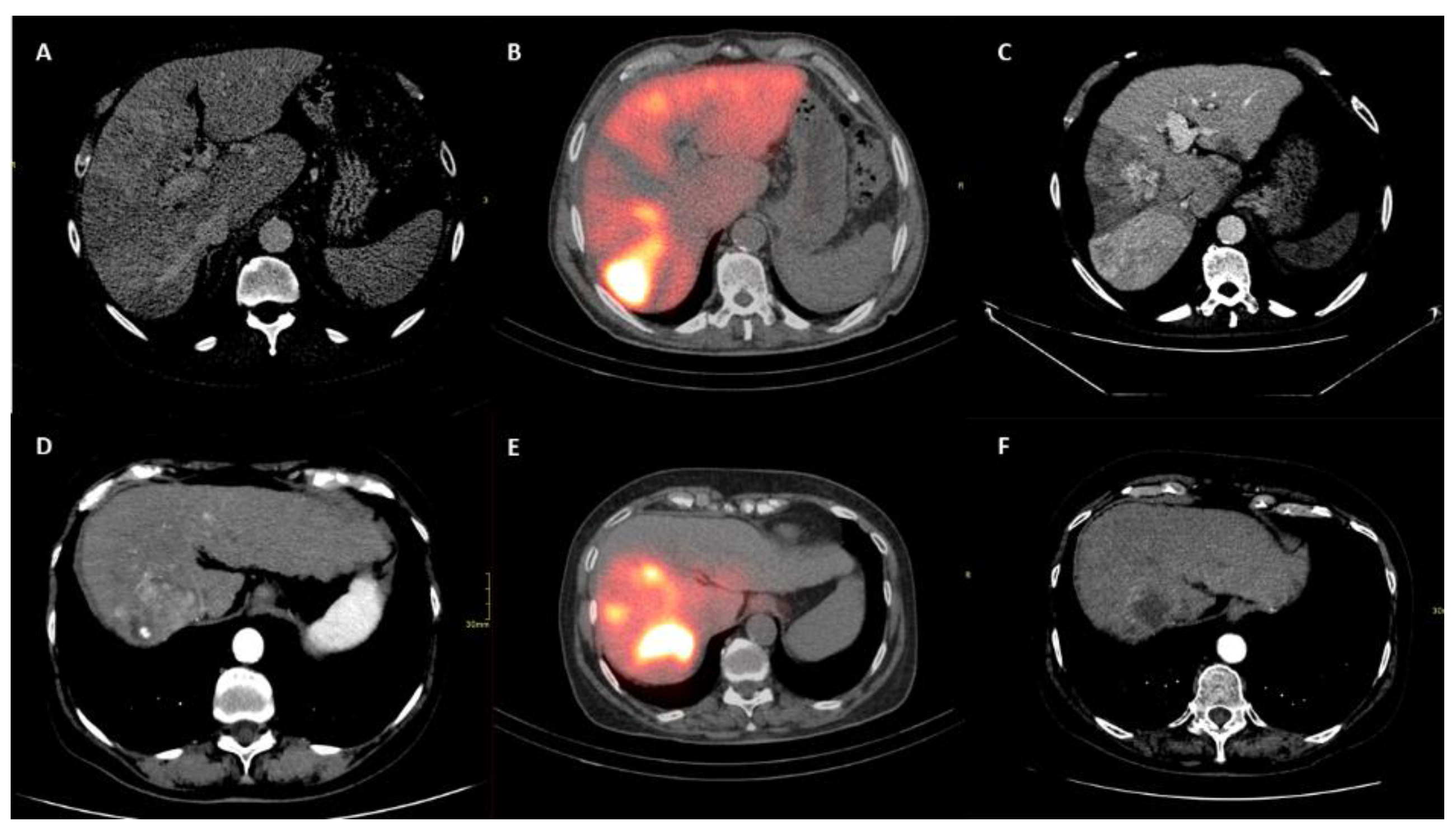
2.2. TARE Treatment and Its Efficacy Assessment
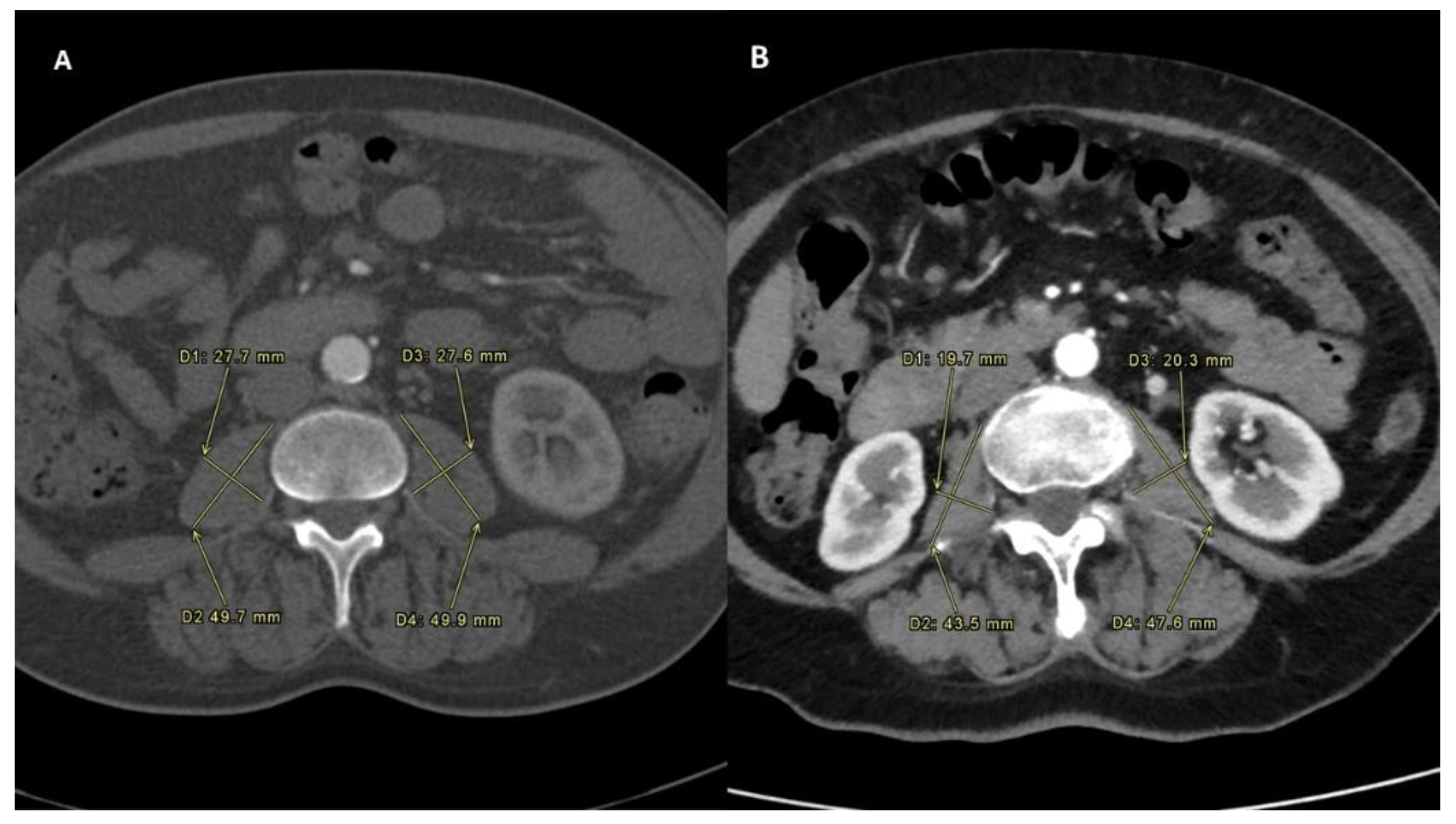
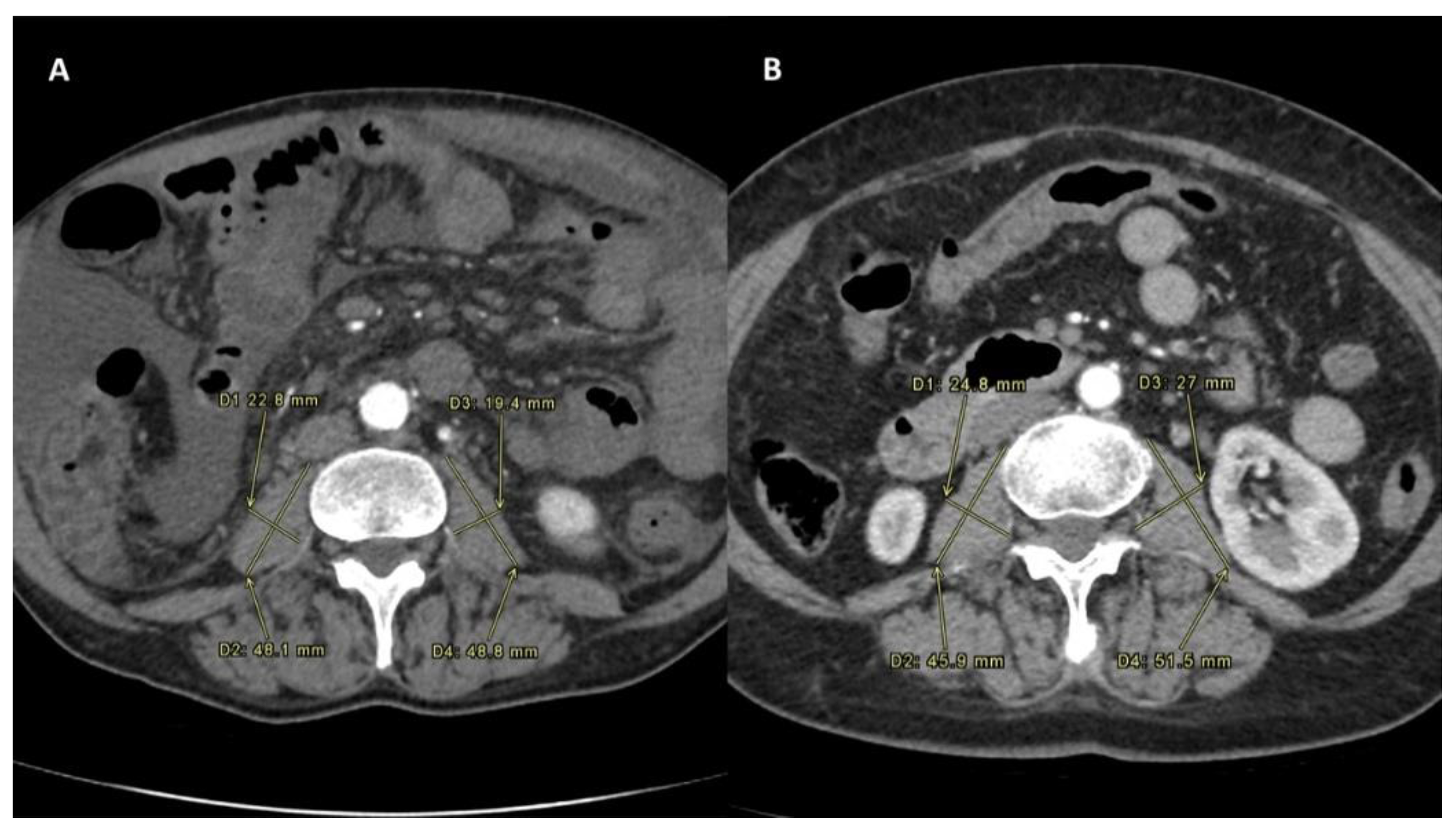
2.3. Definition of Sarcopenia Measurement
2.4. Statistical Analysis
3. Results
3.1. Risk Factors for Progressive Disease
3.2. Diagnostic Ability of the Sarcopenia Measurement
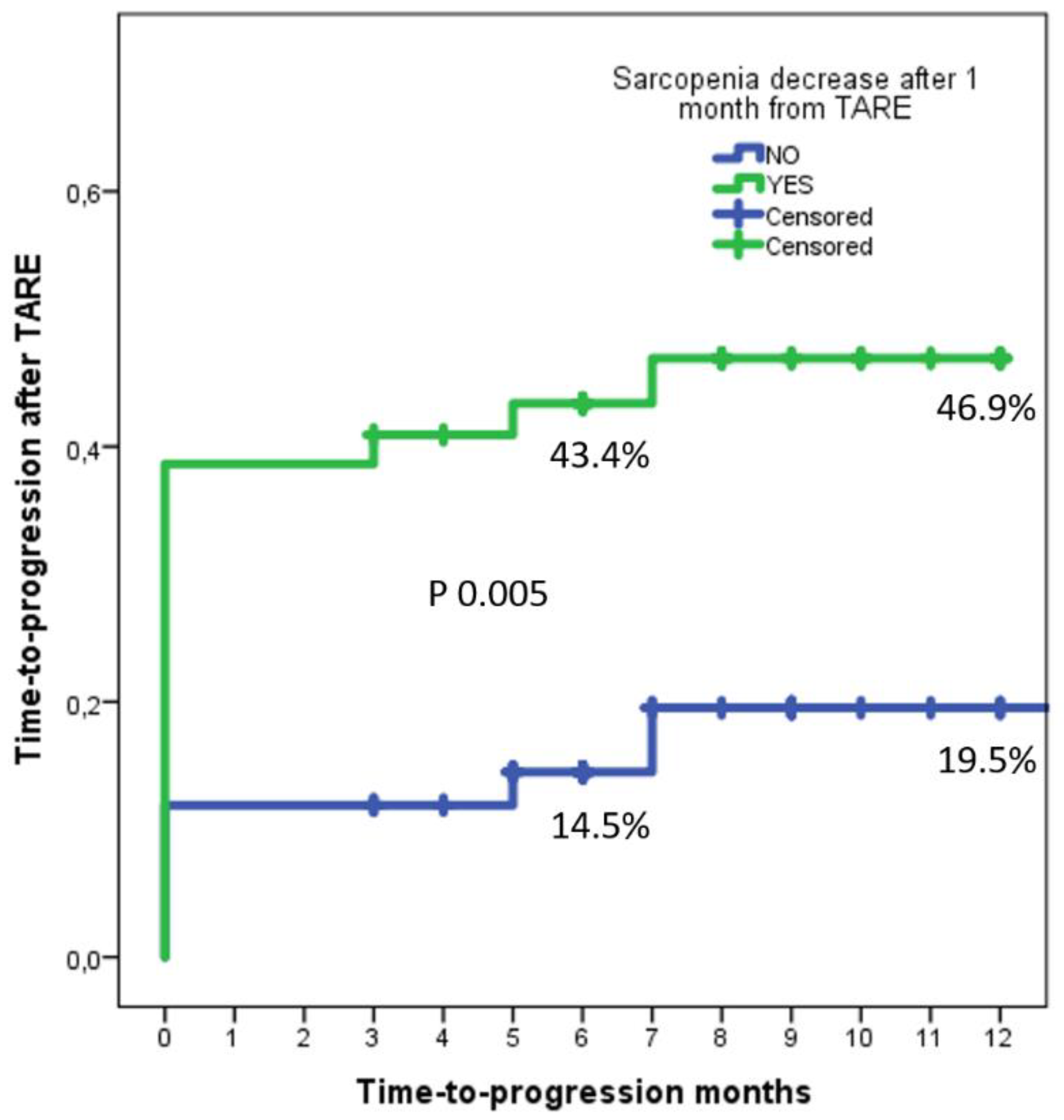
3.3. Time-to-Progress Rates
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sullivan, K.M.; Kenerson, H.L.; Pillarisetty, V.G.; Riehle, K.J.; Yeung, R.S. Precision oncology in liver cancer. Ann. Transl. Med. 2018, 6, e285. [Google Scholar] [CrossRef]
- Manzini, G.; Henne-Bruns, D.; Porzsolt, F.; Kremer, M. Is there a standard for surgical therapy of hepatocellular carci-noma in healthy and cirrhotic liver? A comparison of eight guidelines. BMJ Open Gastroenterol. 2017, 4, e000129. [Google Scholar] [CrossRef]
- Llovet, J.M.; Brú, C.; Bruix, J. Prognosis of Hepatocellular Carcinoma: The BCLC Staging Classification. Semin. Liver Dis. 1999, 19, 329–338. [Google Scholar] [CrossRef]
- Merle, P.; Camus, P.; Abergel, A.; Pageaux, G.P.; Masliah, C.; Bronowicki, J.P.; Zarski, J.P.; Pelletier, G.; Bouattour, M.; Farloux, L.; et al. Safety and efficacy of intra-arterial hepatic chemotherapy with doxorubicin-loaded nanoparticles in hepatocellular carcinoma. ESMO Open 2017, 2, e000238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adcock, C.S.; Florez, E.; Zand, K.A.; Patel, A.; Howard, C.M.; Fatemi, A. Assessment of Treatment Response Following Yttrium-90 Transarterial Radioembolization of Liver Malignancies. Cureus 2018, 10, e2895. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fielding, R.A.; Vellas, B.; Evans, W.J.; Bhasin, S.; Morley, J.E.; Newman, A.B.; van Kan, G.A.; Andrieu, S.; Bauer, J.; Breuille, D.; et al. Sarcopenia: An Undiagnosed Condition in Older Adults. Current Consensus Definition: Prevalence, Etiology, and Consequences. International Working Group on Sarcopenia. J. Am. Med. Dir. Assoc. 2011, 12, 249–256. [Google Scholar] [CrossRef] [Green Version]
- Chang, K.V.; Chen, J.D.; Wu, W.T.; Huang, K.C.; Hsu, C.T.; Han, D.S. Association between loss of skeletal muscle mass and mortality and tumor recurrence in hepatocellular carcinoma: A systematic review and meta-analysis. Liver Cancer 2018, 7, 90–103. [Google Scholar] [CrossRef] [PubMed]
- Takada, H.; Kurosaki, M.; Nakanishi, H.; Takahashi, Y.; Itakura, J.; Tsuchiya, K.; Yasui, Y.; Tamaki, N.; Takaura, K.; Komiyama, Y.; et al. Impact of pre-sarcopenia in sorafenib treatment for advanced hepatocellular carcinoma. PLoS ONE 2018, 13, e0198812. [Google Scholar] [CrossRef] [PubMed]
- Yamashima, M.; Miyaaki, H.; Honda, T.; Shibata, H.; Miuma, S.; Taura, N.; Nakao, K. Significance of psoas muscle thickness as an indicator of muscle atrophy in patients with hepatocellular carcinoma treated with sorafenib. Mol. Clin. Oncol. 2017, 7, 449–453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujita, M.; Takahashi, A.; Hayashi, M.; Okai, K.; Abe, K.; Ohira, H. Skeletal muscle volume loss during transarterial chemoembolization predicts poor prognosis in patients with hepatocellular carcinoma. Hepatol. Res. 2019, 49, 778–786. [Google Scholar] [CrossRef]
- Vasques, J.; Guerreiro, C.S.; Sousa, J.; Pinto, M.; Cortez-Pinto, H. Nutritional support in cirrhotic patients with sarcopenia. Clin. Nutr. ESPEN 2019, 33, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Cheng, T.-Y.; Lee, P.-C.; Chen, Y.-T.; Chao, Y.; Hou, M.-C.; Huang, Y.-H. Pre-sarcopenia determines post-progression outcomes in advanced hepatocellular carcinoma after sorafenib failure. Sci. Rep. 2020, 10, 18375. [Google Scholar] [CrossRef] [PubMed]
- Lencioni, R.; Llovet, J.M. Modified RECIST (mRECIST) Assessment for Hepatocellular Carcinoma. Semin. Liver Dis. 2010, 30, 52–60. [Google Scholar] [CrossRef] [Green Version]
- Loosen, S.H.; Schulze-Hagen, M.; Bruners, P.; Tacke, F.; Trautwein, C.; Kuhl, C.; Luedde, T.; Roderburg, C. Sarcopenia Is a Negative Prognostic Factor in Patients Undergoing Transarterial Chemoembolization (TACE) for Hepatic Malignancies. Cancers 2019, 11, 1503. [Google Scholar] [CrossRef] [Green Version]
- Ahmadzadehfar, H.; Duan, H.; Haug, A.; Walrand, S.; Hoffmann, M. The role of SPECT/CT in radioembolization of liver tumours. Eur. J. Nucl. Med. Mol. Imaging 2014, 41 (Suppl. 1), 115–124. [Google Scholar] [CrossRef]
- Richetta, E.; Pasquino, M.; Poli, M.; Cutaia, C.; Valero, C.; Tabone, M.; Paradisi, B.P.; Pacilio, M.; Pellerito, R.E.; Stasi, M. PET-CT post therapy dosimetry in radioembolization with resin 90Y microspheres: Comparison with pre-treatment SPECT-CT 99mTc-MAA results. Phys. Med. 2019, 64, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Brustia, R.; Savier, E.; Scatton, O. Physical exercise in cirrhotic patients: Towards prehabilitation on waiting list for liver transplantation. A systematic review and meta-analysis. Clin. Res. Hepatol. Gastroenterol. 2018, 42, 205–215. [Google Scholar] [CrossRef]
- Dunne, R.F.; Loh, K.P.; Williams, G.R.; Jatoi, A.; Mustian, K.M.; Mohile, S.G. Cachexia and Sarcopenia in Older Adults with Cancer: A Comprehensive Review. Cancers 2019, 11, 1861. [Google Scholar] [CrossRef] [Green Version]
- Bischoff, S.C.; Bernal, W.; Dasarathy, S.; Merli, M.; Plank, L.D.; Schütz, T.; Plauth, M. ESPEN practical guideline: Clinical nutrition in liver disease. Clin. Nutr. 2020, 39, 3533–3562. [Google Scholar] [CrossRef] [PubMed]
- Lattanzi, B.; Giusto, M.; Albanese, C.; Mennini, G.; D’Ambrosio, D.; Farcomeni, A.; Corradini, S.G.; Rossi, M.; Merli, M. The Effect of 12 Weeks of β-Hydroxy-β-Methyl-Butyrate Supplementation after Liver Transplantation: A Pilot Randomized Controlled Study. Nutrients 2019, 11, 2259. [Google Scholar] [CrossRef] [Green Version]
- Lai, Q.; Magistri, P.; Lionetti, R.; Avolio, A.W.; Lenci, I.; Giannelli, V.; Pecchi, A.; Ferri, F.; Marrone, G.; Angelico, M.; et al. Sarco-Model: A score to predict the dropout risk in the perspective of organ allocation in patients awiting liver transplantation. Liver Int. 2021, 41, 1629–1640. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | No-Sarcopenia Group (n = 42) | Sarcopenia Group (n = 44) | p |
|---|---|---|---|
| Median (IQR) or n (%) | |||
| Age (year)s | 64 (59–66) | 64 (58–71) | 0.45 |
| Male sex | 33 (78.6) | 32 (72.7) | 0.62 |
| Height (cm) | 176 (170–180) | 173 (165–180) | 0.17 |
| Ascites (any grade) Moderate | 16 (38.1) 7 (16.7) | 15 (34.1) 2 (4.5) | 0.82 0.09 |
| Diameter target lesion (mm) | 54 (37–77) | 44 (31–79) | 0.51 |
| Number of nodules | 3 (2–4) | 3 (2–4) | 0.48 |
| Bilobar involvement | 26 (61.9) | 28 (63.6) | 1.00 |
| Liver involved >50% | 12 (28.6) | 9 (20.5) | 0.46 |
| Macrovascular invasion | 23 (54.8) | 24 (54.5) | 1.00 |
| Nodal metastases | 10 (23.8) | 8 (18.2) | 0.60 |
| Bilobar TARE treatment | 25 (59.5) | 23 (52.3) | 0.52 |
| PIVKA measure (AU/mL) at TARE | 200 (93–455) | 168 (44–450) | 0.91 |
| AFP measure (ng/mL) at TARE | 69 (20.244) | 58 (21–205) | 0.87 |
| PMI (mm/m2) at TARE Male sex Female sex | 10.2 (8.6–11.4) 10.0 (8.6–11.6) 11.0 (8.7–11.3) | 11.3 (9.5–12.1) 11.6 (10.1–12.3) 10.2 (8.7–11.5) | 0.04 0.01 0.86 |
| PMI (mm/m2) at 1 month Male sex Female sex | 10.7 (9.2–11.5) 10.6 (9.1–11.6) 11.1 (8.8–11.4) | 10.7 (9.1–11.5) 11.0 (9.9–11.9) 9.3 (8.2–10.6) | 0.70 0.21 0.28 |
| Delta PMI after 1 month Male sex Female sex | 0.1 (0.0–0.3) 0.2 (0.0–0.3) 0.0 (0.0–0.2) | −0.4 (−0.5–−0.2) −0.3 (−0.5–−0.2) −0.4 (−0.8–−0.1) | <0.0001 <0.0001 <0.0001 |
| PMI (mm/m2) at 3 months Male sex Female sex | 10.1 (9.3–11.6) 10.0 (9.1–11.6) 11.0 (8.4–11.6) | 10.4 (8.7–11.4) 10.8 (9.3–11.9) 8.9 (7.5–10.8) | 0.97 0.31 0.19 |
| Delta PMI after 3 months Male sex Female sex | 0.1 (−0.3–0.4) 0.1 (−0.3–0.4) 0.0 (−0.5–0.4) | −0.6 (−1.1–−0.3) −0.6 (−1.1–−0.1) −0.8 (−1.2–−0.5) | <0.0001 0.001 0.003 |
| Decrease PMI after 3 months Male sex Female sex | 14 (33.3) 10 (30.3) 4 (44.4) | 37 (84.1) 25 (78.1) 12 (100.0) | <0.0001 <0.0001 0.006 |
| mRECIST CR | 10 (23.8) | 7 (15.9) | 0.42 |
| mRECIST PR | 18 (42.9) | 13 (29.5) | 0.26 |
| mRECIST SD | 9 (21.4) | 7 (15.9) | 0.59 |
| mRECIST PD | 5 (11.9) | 17 (38.6) | 0.006 |
| Extrahepatic PD | 4 (9.5) | 11 (25.0) | 0.09 |
| Intra + extrahepatic PD | 2 (4.8) | 8 (18.2) | 0.09 |
| PD (intra- and/or extrahepatic) | 7 (16.7) | 20 (45.5) | 0.005 |
| Variable | Beta | SE | Wald | HR | 95%CI | p | |
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| PMI decrease 1-month after TARE | 1.18 | 0.45 | 6.90 | 3.25 | 1.35 | 7.81 | 0.009 |
| Number of nodules | 0.25 | 0.19 | 1.74 | 1.29 | 0.89 | 1.87 | 0.19 |
| Macrovascular invasion | 0.50 | 0.46 | 1.16 | 1.65 | 0.66 | 4.08 | 0.28 |
| Nodal invasion | 0.46 | 0.47 | 0.97 | 1.59 | 0.64 | 3.96 | 0.32 |
| Diameter of the target lesion | 0.002 | 0.01 | 0.10 | 1.00 | 0.99 | 1.02 | 0.76 |
| Variable | AUC | SE | 95%CI | p | |
|---|---|---|---|---|---|
| Lower | Upper | ||||
| PMI at TARE | 0.59 | 0.07 | 0.46 | 0.72 | 0.19 |
| PMI after 1 month | 0.65 | 0.06 | 0.53 | 0.77 | 0.03 |
| Delta-PMI TARE—1 month | 0.70 | 0.06 | 0.58 | 0.82 | 0.003 |
| PMI after 3 months | 0.73 | 0.06 | 0.63 | 0.84 | 0.001 |
| Delta-PMI TARE—3 months | 0.81 | 0.06 | 0.70 | 0.92 | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vallati, G.E.; Trobiani, C.; Teodoli, L.; Lai, Q.; Cappelli, F.; Ungania, S.; Catalano, C.; Lucatelli, P. Sarcopenia Worsening One Month after Transarterial Radioembolization Predicts Progressive Disease in Patients with Advanced Hepatocellular Carcinoma. Biology 2021, 10, 728. https://doi.org/10.3390/biology10080728
Vallati GE, Trobiani C, Teodoli L, Lai Q, Cappelli F, Ungania S, Catalano C, Lucatelli P. Sarcopenia Worsening One Month after Transarterial Radioembolization Predicts Progressive Disease in Patients with Advanced Hepatocellular Carcinoma. Biology. 2021; 10(8):728. https://doi.org/10.3390/biology10080728
Chicago/Turabian StyleVallati, Giulio Eugenio, Claudio Trobiani, Leonardo Teodoli, Quirino Lai, Federico Cappelli, Sara Ungania, Carlo Catalano, and Pierleone Lucatelli. 2021. "Sarcopenia Worsening One Month after Transarterial Radioembolization Predicts Progressive Disease in Patients with Advanced Hepatocellular Carcinoma" Biology 10, no. 8: 728. https://doi.org/10.3390/biology10080728