
CFD Study of the Effect of the Angle Pattern on Iliac Vein Compression Syndrome
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
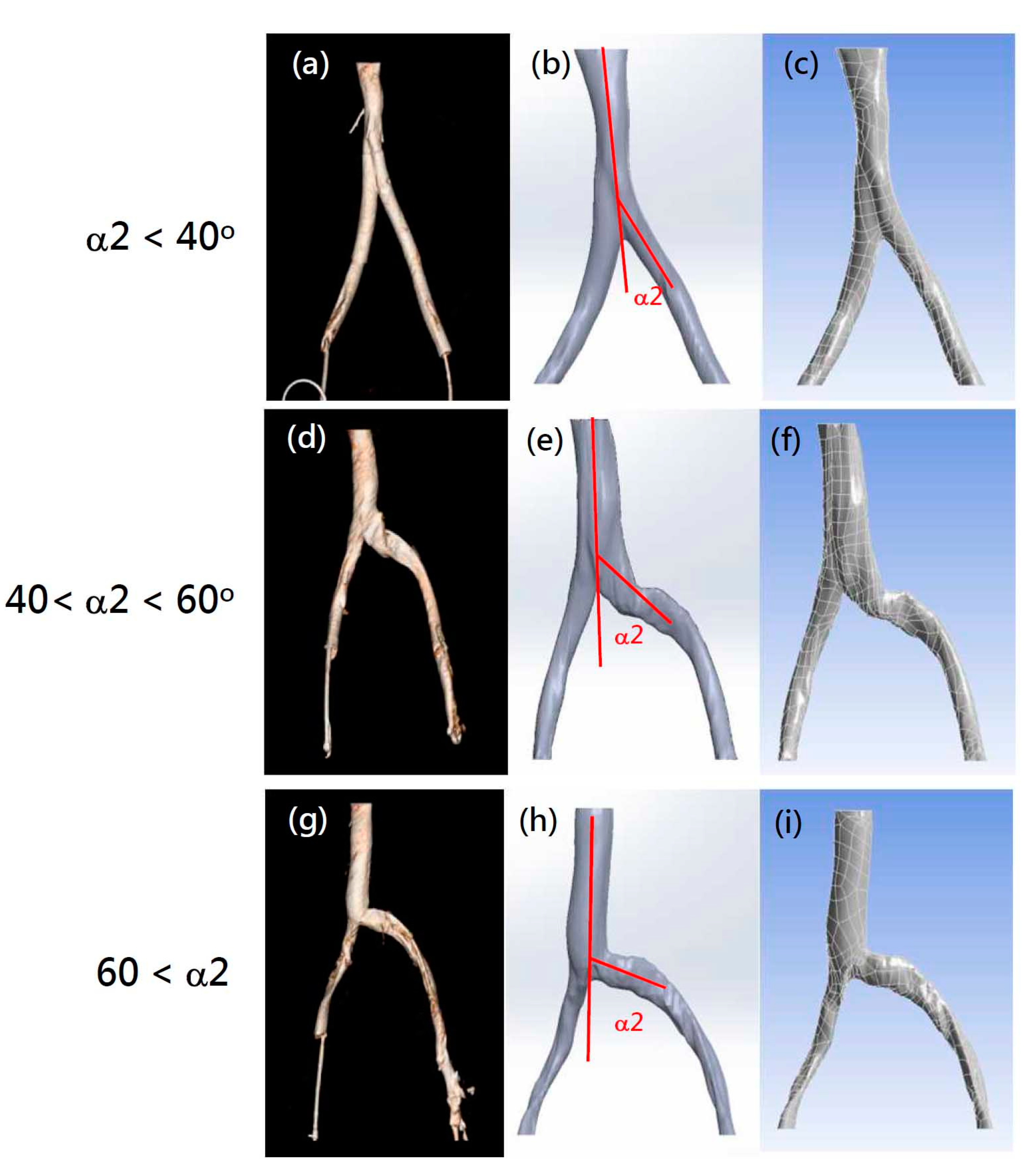
2.1. Patient Selection and Model Creation
2.2. Boundary Conditions and Material Properties
2.3. Mathematical Modeling
2.4. Physical Model Validation
2.5. Problem Definition
3. Results and Discussion
3.1. Material Properties Validation
3.2. CFD Model Selection
3.3. Validating the CFD Model
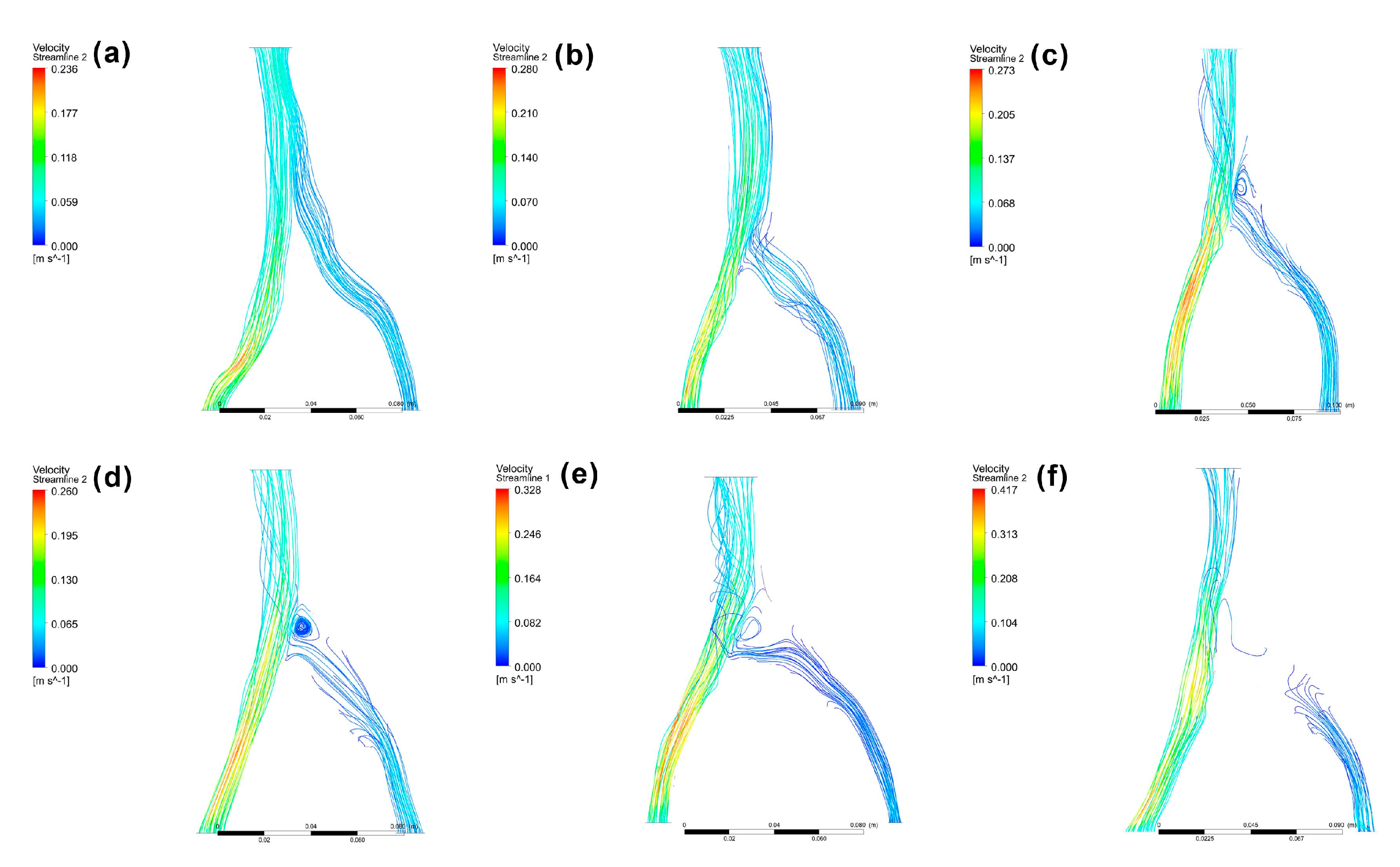
3.4. Patient-Specific CFD Simulation
3.5. Study Limitations
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- May, R.; Thurner, J. The cause of the predominantly sinistral occurrence of thrombosis of the pelvic veins. Angiology 1957, 8, 419–427. [Google Scholar] [CrossRef] [PubMed]
- Fazel, R.; Froehlich, J.B.; Williams, D.M.; Saint, S.; Nallamothu, B.K. Clinical problem-solving. A sinister development—A 35-year-old woman presented to the emergency department with a 2-day history of progressive swelling and pain in her left leg, without antecedent trauma. N. Engl. J. Med. 2007, 357, 53–59. [Google Scholar] [CrossRef]
- Li, J.; Chen, H.; Chen, W.; Zhou, K.; Xu, Z.; Xu, M.; Sun, Z. Novel typing of iliac vein compression in asymptomatic individuals evaluated by contrast enhanced CT. Surg. Radiol. Anat. 2021, 43, 1149–1157. [Google Scholar] [CrossRef] [PubMed]
- Radaideh, Q.; Patel, N.M.; Shammas, N.W. Iliac vein compression: Epidemiology, diagnosis and treatment. Vasc. Health Risk Manag. 2019, 15, 115–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Labropoulos, N.; Borge, M.; Pierce, K.; Pappas, P.J. Criteria for defining significant central vein stenosis with duplex ultrasound. J. Vasc. Surg. 2007, 46, 101–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carr, S.; Chan, K.; Rosenberg, J.; Kuo, W.T.; Kothary, N.; Hovsepian, D.M.; Sze, D.Y.; Hofmann, L.V. Correlation of the diameter of the left common iliac vein with the risk of lower-extremity deep venous thrombosis. J. Vasc. Interv. Radiol. 2012, 23, 1467–1472. [Google Scholar] [CrossRef]
- Iyer, S.; Angle, J.F.; Uflacker, A.; Sharma, A.M. Venous compression syndromes: A review. Curr. Treat. Options Cardio. Med. 2017, 19, 45. [Google Scholar] [CrossRef]
- Góes Junior, A.M.O.; Araújo, R.S.; Furlaneto, I.P.; Vieira, W.B. Compression of left renal vein and left common iliac vein on CT scans: How often are they detected? J. Vasc. Bras. 2020, 19, e20190121. [Google Scholar] [CrossRef]
- Brinegar, K.N.; Sheth, R.A.; Khademhosseini, A.; Bautista, J.; Oklu, R. Iliac vein compression syndrome: Clinical, imaging and pathologic findings. World J. Radiol. 2015, 7, 375–381. [Google Scholar] [CrossRef]
- Cavalcante, L.P.; dos Santos Souza, J.E.; Pereira, R.M.; Bernardes, M.V.; da Silva Amanajas, A.M.; Parisati, M.H.; da Rocha, R.D.; de Araujo, A.O. Iliac vein compression syndrome: Literature review. J. Vasc. Bras. 2015, 14, 78–83. [Google Scholar] [CrossRef]
- Marques, M.A.; Silveira, P.R.M.; von Ristow, A.; Gress, M.; Massière, B.; Vescovi, A.; Filho, J.M.C.; Vieira, R.D. Prevalencia de marcadores de trombofilia em pacientes portadores da sindrome de May-Thurner e trombose de veia iliaca comum esquerda. J. Vasc. Bras. 2010, 9, 229–232. [Google Scholar] [CrossRef] [Green Version]
- Moudgill, N.; Hager, E.; Gonsalves, C.; Larson, R.; Lombardi, J.; DiMuzio, P. May-Thurner syndrome: Case report and review of the literature involving modern endovascular therapy. Vascular 2009, 17, 330–335. [Google Scholar] [CrossRef] [PubMed]
- Nazzal, M.; El-Fedaly, M.; Kazan, V.; Qu, W.; Renno, A.W.; Al-Natour, M.; Abbas, J. Incidence and clinical significance of iliac vein compression. Vascular 2015, 23, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Ou-Yang, L.; Lu, G.M. Underlying anatomy and typing diagnosis of May-Thurner syndrome and clinical significance: An observation based on CT. Spine 2016, 41, E1284–E1291. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, W.; Al Safran, Z.; Hasan, H.; Zeid, W.A. Endovascular management of may-thurner syndrome. Ann. Vasc. Dis. 2012, 5, 217–221. [Google Scholar] [CrossRef] [Green Version]
- Foit, N.A.; Chen, Q.M.; Cook, B.; Hammerberg, E.M. Iliofemoral deep vein thrombosis after tibial plateau fracture fixation related to undiagnosed May-Thurner syndrome: A case report. Patient Saf. Surg. 2013, 7, 12. [Google Scholar] [CrossRef] [Green Version]
- Raju, S.; Neglen, P. High prevalence of nonthrombotic iliac vein lesions in chronic venous disease: A permissive role in pathogenicity. J. Vasc. Surg. 2006, 44, 136–144. [Google Scholar] [CrossRef] [Green Version]
- O’Sullivan, G.J.; Semba, C.P.; Bittner, C.A.; Kee, S.T.; Razavi, M.K.; Sze, D.Y.; Dake, M.D. Endovascular management of iliac vein compression (May-Thurner) syndrome. J. Vasc. Interv. Radiol. 2000, 11, 823–836. [Google Scholar] [CrossRef] [PubMed]
- Menichini, C.; Xu, X.Y. Mathematical modeling of thrombus formation in idealized models of aortic dissection: Initial findings and potential applications. J. Math. Biol. 2016, 73, 1205–1226. [Google Scholar] [CrossRef] [Green Version]
- Song, X.; Zheng, Y.; Song, X.; Wang, X.; Ye, W. An image analysis of the major angles along the pathway of iliac veins involved in endovenous interventions. J. Vasc. Surg. Venous. Lymphat. Disord. 2021, 9, 81–87. [Google Scholar] [CrossRef]
- Verhaeghe, R. Iliac vein compression as anatomical cause of thrombophilia: Cockett’s syndrome revisited. Thromb. Haemost. 1995, 74, 1398–1401. [Google Scholar] [CrossRef] [PubMed]
- Cockett, F.B.; Thomas, L. The iliac compression syndrome. Br. J. Surg. 1965, 52, 816–821. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Gao, N.; Shen, L.; Yang, J.; Zhu, Y.; Li, Z.; Si, Y. Endovascular treatment for symptomatic iliac vein compression syndrome: A prospective consecutive series of 48 patients. Ann. Vasc. Surg. 2014, 28, 695–704. [Google Scholar] [CrossRef] [PubMed]
- Doost, S.N.; Ghista, D.; Su, B.; Zhong, L.; Morsi, Y.S. Heart blood flow simulation: A perspective review. BioMed. Eng. Online 2016, 15, 101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taebi, A. Deep Learning for Computational Hemodynamics: A Brief Review of Recent Advances. Fluids 2022, 7, 197. [Google Scholar] [CrossRef]
- Kamada, H.; Nakamura, M.; Ota, H.; Higuchi, S.; Takase, K. Blood flow analysis with computational fluid dynamics and 4D-flow MRI for vascular diseases. J. Cardiol. 2022, 80, 386–396. [Google Scholar] [CrossRef]
- Zhong, L.; Zhang, J.M.; Su, B.; Tan, R.S.; Allen, J.C.; Kassab, G.S. Application of patient-specific computational fluid dynamics in coronary and intra-cardiac flow simulations: Challenges and opportunities. Front. Physiol. 2018, 9, 742. [Google Scholar] [CrossRef]
- Xu, H.; Piccinelli, M.; Leshnower, B.G.; Lefieux, A.; Taylor, W.R.; Veneziani, A. Coupled morphological-hemodynamic computational analysis of type B aortic dissection: A longitudinal study. Ann. Biomed. Eng. 2018, 46, 927–939. [Google Scholar] [CrossRef]
- Osswald, A.; Karmonik, C.; Anderson, J.R.; Rengier, F.; Karck, M.; Engelke, J.; Kallenbach, K.; Kotelis, D.; Partovi, S.; Böckler, D.; et al. Elevated wall shear stress in aortic type B dissection may relate to retrograde aortic type a dissection: A computational fluid dynamics pilot study. Eur. J. Vasc. Endovasc. Surg. 2017, 54, 324–330. [Google Scholar] [CrossRef] [Green Version]
- Aramburu, J.; Anto’n, R.; Rodrı´guez-Fraile, M.; Sangro, B.; Bilbao, J.I. Computational fluid dynamics modeling of liver radioembolization: A review. Cardiovasc. Intervent. Radiol. 2022, 45, 12–20. [Google Scholar] [CrossRef]
- Wu, T.; Zhu, Q. Advancement in the haemodynamic study of intracranial aneurysms by computational fluid dynamics. Brain Hemorrhages 2021, 2, 71–75. [Google Scholar] [CrossRef]
- Uchiyama, Y.; Fujimura, S.; Takao, H.; Suzuki, T.; Hayakawa, M.; Ishibashi, T.; Karagiozov, K.; Fukudome, K.; Murayama, Y.; Yamamoto, M. Hemodynamic investigation of the effectiveness of a two overlapping flow diverter configuration for cerebral aneurysm treatment. Bioengineering 2021, 8, 143. [Google Scholar] [CrossRef] [PubMed]
- Albadawi, M.; Abuouf, Y.; Elsagheer, S.; Sekiguchi, H.; Ookawara, S.; Ahmed, M. Influence of rigid–elastic artery wall of carotid and coronary stenosis on hemodynamics. Bioengineering 2022, 9, 708. [Google Scholar] [CrossRef] [PubMed]
- Smadi, O.; Abdelkarim, A.; Awad, S.; Almomani, T.D. Hemodynamic performance of dysfunctional prosthetic heart valve with the concomitant presence of subaortic stenosis: In silico study. Bioengineering 2020, 7, 90. [Google Scholar] [CrossRef] [PubMed]
- Yi, H.; Johnson, M.; Bramlage, L.C.; Ludwig, B.; Yang, Z. Effects of pulsatile flow rate and shunt ratio in bifurcated distal arteries on hemodynamic characteristics involved in two patient-specific internal carotid artery sidewall aneurysms: A numerical study. Bioengineering 2022, 9, 326. [Google Scholar] [CrossRef]
- Bonnefous, O.; Pereira, V.M.; Ouared, R.; Brina, O.; Aerts, H.; Hermans, R.; van Nijnatten, F.; Stawiaski, J.; Ruijters, D. Quantification of arterial flow using digital subtraction angiography. Med. Phys. 2012, 39, 6264–6275. [Google Scholar] [CrossRef]
- Lee, H.J.; Hong, J.S.; Lin, C.J.; Kao, Y.H.; Chang, F.C.; Luo, C.B.; Chu, W.F. Automatic flow analysis of digital subtraction angiography using independent component analysis in patients with carotid stenosis. PLoS ONE 2017, 12, e0185330. [Google Scholar] [CrossRef] [Green Version]
- Kabir, A.; Sultana, K.; Uddin, A. Performance of k-ω and k-ε model for blood flow simulation in stenosed artery. J. Bangladesh Math. Soc. 2020, 40, 111–125. [Google Scholar] [CrossRef]
- Metzger, P.B.; Rossi, F.H.; Kambara, A.M.; Izukawa, N.M.; Saleh, M.H.; Pinto, I.M.F.; Amorim, J.E.; Thorpe, P.E. Criteria for detecting significant chronic iliac venous obstructions with duplex ultrasound. J. Vasc. Surg. Venous. Lymphat. Disord. 2016, 4, 18–27. [Google Scholar] [CrossRef]
- Febina, J.; Sikkandar, M.Y.; Sudharsan, N.M. Wall shear stress estimation of thoracic aortic aneurysm using computational fluid dynamics. Comput. Math. Methods Med. 2018, 2018, 7126532. [Google Scholar] [CrossRef] [Green Version]
- Cho, Y.I.; Kensey, K.R. Effects of the non-Newtonian viscosity of blood on flows in a diseased arterial vessel. Part 1: Steady flows. Biorheology 1991, 28, 241–262. [Google Scholar] [CrossRef] [PubMed]
- Song, X.; Wood, H.G.; Day, S.W.; Olsen, D.B. Studies of turbulence models in a computational fluid dynamics model of a blood pump. Artif. Organs 2003, 27, 935–937. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sikkandar, M.Y.; Sudharsan, N.M.; Begum, S.S.; Ng, E.Y.K. Computational fluid dynamics: A technique to solve complex biomedical engineering problems—A review. WSEAS Trans. Biol. Biomed. 2019, 16, 121–137. [Google Scholar]
- Ku, D.N. Blood flow in arteries. Ann. Rev. Fluid Mech. 1997, 29, 399–434. [Google Scholar] [CrossRef]
- Mahalingam, A.; Gawandalkar, U.U.; Kini, G.; Buradi, A.; Araki, T.; Ikeda, N.; Nicolaides, A.; Laird, J.R.; Saba, L.; Suri, J.S. Numerical analysis of the effect of turbulence transition on the hemodynamic parameters in human coronary arteries. Cardiovasc. Diagn. Ther. 2016, 6, 208–220. [Google Scholar] [CrossRef] [Green Version]
- Saqr, K.M.; Tupin, S.; Rashad, S.; Endo, T.; Niizuma, K.; Tominaga, T.; Makoto, O. Physiologic blood flow is turbulent. Sci. Rep. 2020, 10, 15492. [Google Scholar] [CrossRef]
- Sengupta, S.; Zhu, Y.; Hamady, M.; Xu, X.Y. Evaluating the haemodynamic performance of endografts for complex aortic arch repair. Bioengineering 2022, 9, 573. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | |
|---|---|
| Age, years | 58.19 ± 15.45 (21–79) |
| Male | 11 (35.5%) |
| Female | 20 (64.5%) |
| α1, degrees | 34.1 ± 11.9 (18–65) |
| α2, degrees | 48.8 ± 17.7 (25–90) |
| α1 + α2, degrees | 82.9 ± 22.8 (45–130) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, H.-W.; Chen, C.-H.; Fan, Y.-J.; Lin, C.-Y.; Hsu, W.-H.; Su, I.-C.; Lin, C.-L.; Chiang, Y.-C.; Huang, H.-M. CFD Study of the Effect of the Angle Pattern on Iliac Vein Compression Syndrome. Bioengineering 2023, 10, 688. https://doi.org/10.3390/bioengineering10060688
Chen H-W, Chen C-H, Fan Y-J, Lin C-Y, Hsu W-H, Su I-C, Lin C-L, Chiang Y-C, Huang H-M. CFD Study of the Effect of the Angle Pattern on Iliac Vein Compression Syndrome. Bioengineering. 2023; 10(6):688. https://doi.org/10.3390/bioengineering10060688
Chicago/Turabian StyleChen, Hsuan-Wei, Chao-Hsiang Chen, Yu-Jui Fan, Chun-Yu Lin, Wen-Hsien Hsu, I-Chang Su, Chun-Li Lin, Yuan-Ching Chiang, and Haw-Ming Huang. 2023. "CFD Study of the Effect of the Angle Pattern on Iliac Vein Compression Syndrome" Bioengineering 10, no. 6: 688. https://doi.org/10.3390/bioengineering10060688