
Auditory Processing Disorder Test Battery in European Portuguese—Development and Normative Data for Pediatric Population

 , , and
, , and 
Abstract
:1. Introduction
Paper Structure
2. Methods
2.1. Selection of Tests for the Battery
2.2. Development of the BAPA-PE Battery
2.2.1. SSW for European Portuguese (SSW-EP)
2.2.2. Filtered Speech (FS)
2.2.3. Speech in Noise (SIN)
2.2.4. Detection of Interval in Noise (DIN)
2.2.5. Frequency Pattern (FP)
2.2.6. Duration Pattern (DP)
2.3. Application to Normal Hearing Group
Analyses
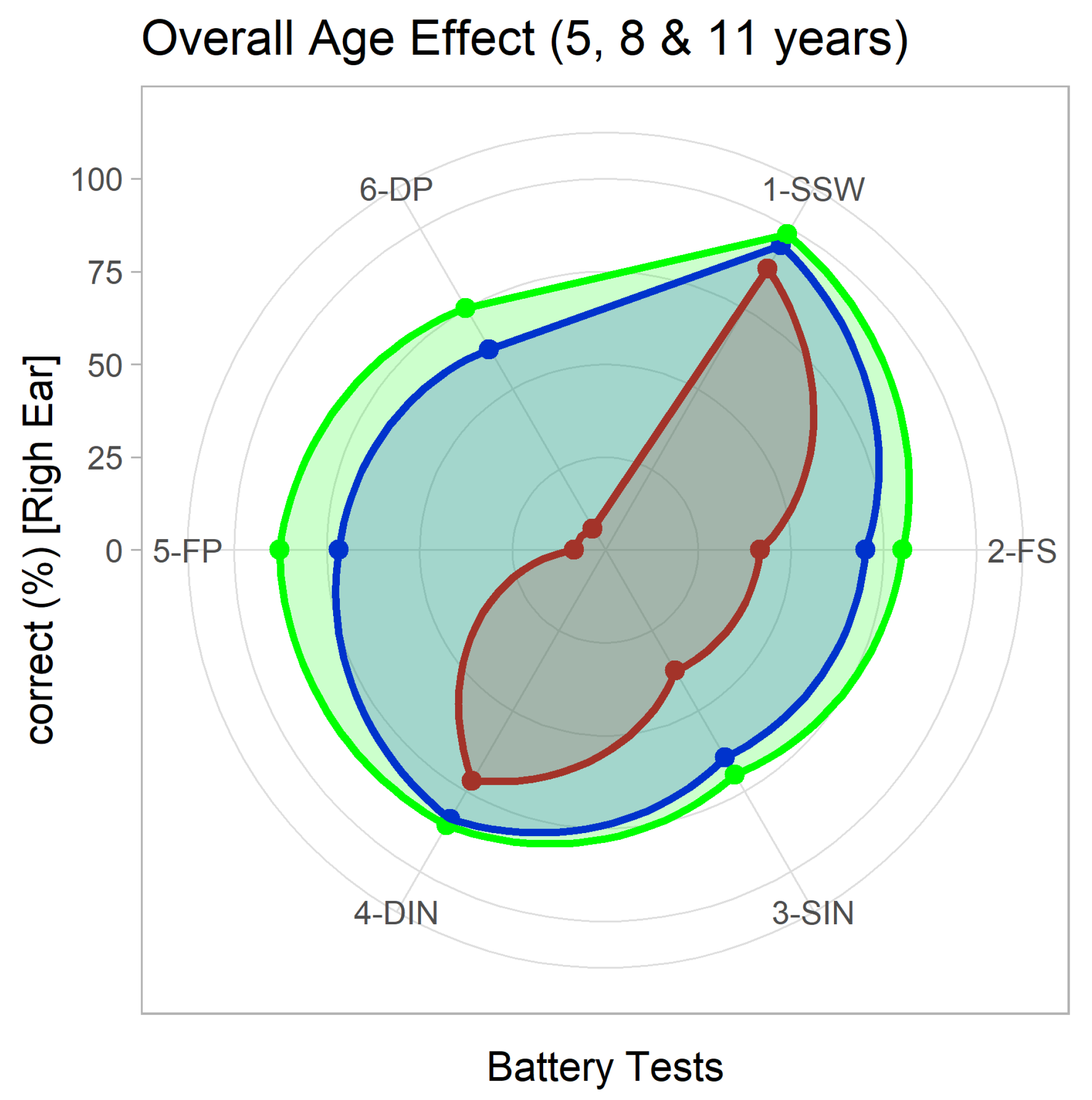
3. Results
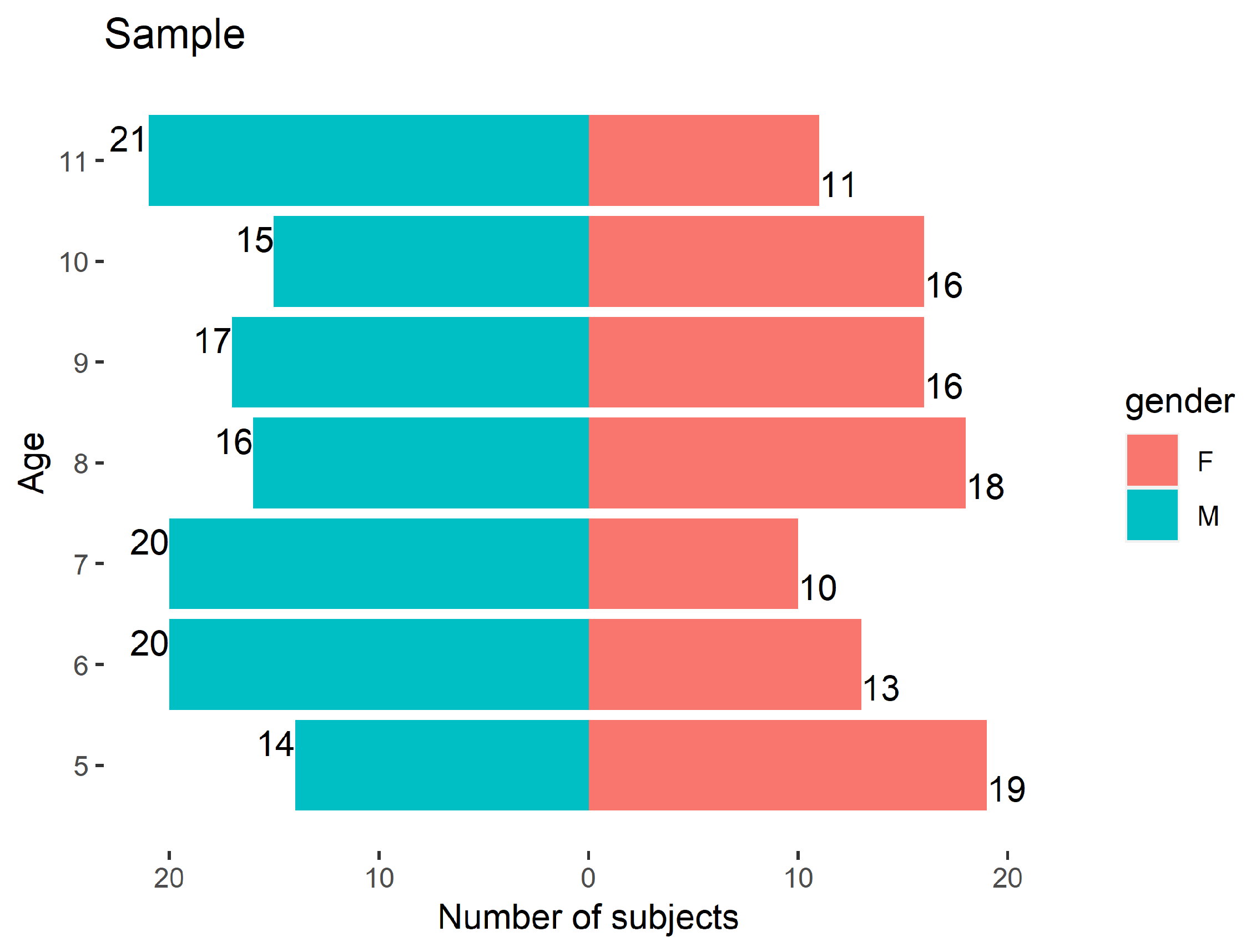
3.1. General Characterization
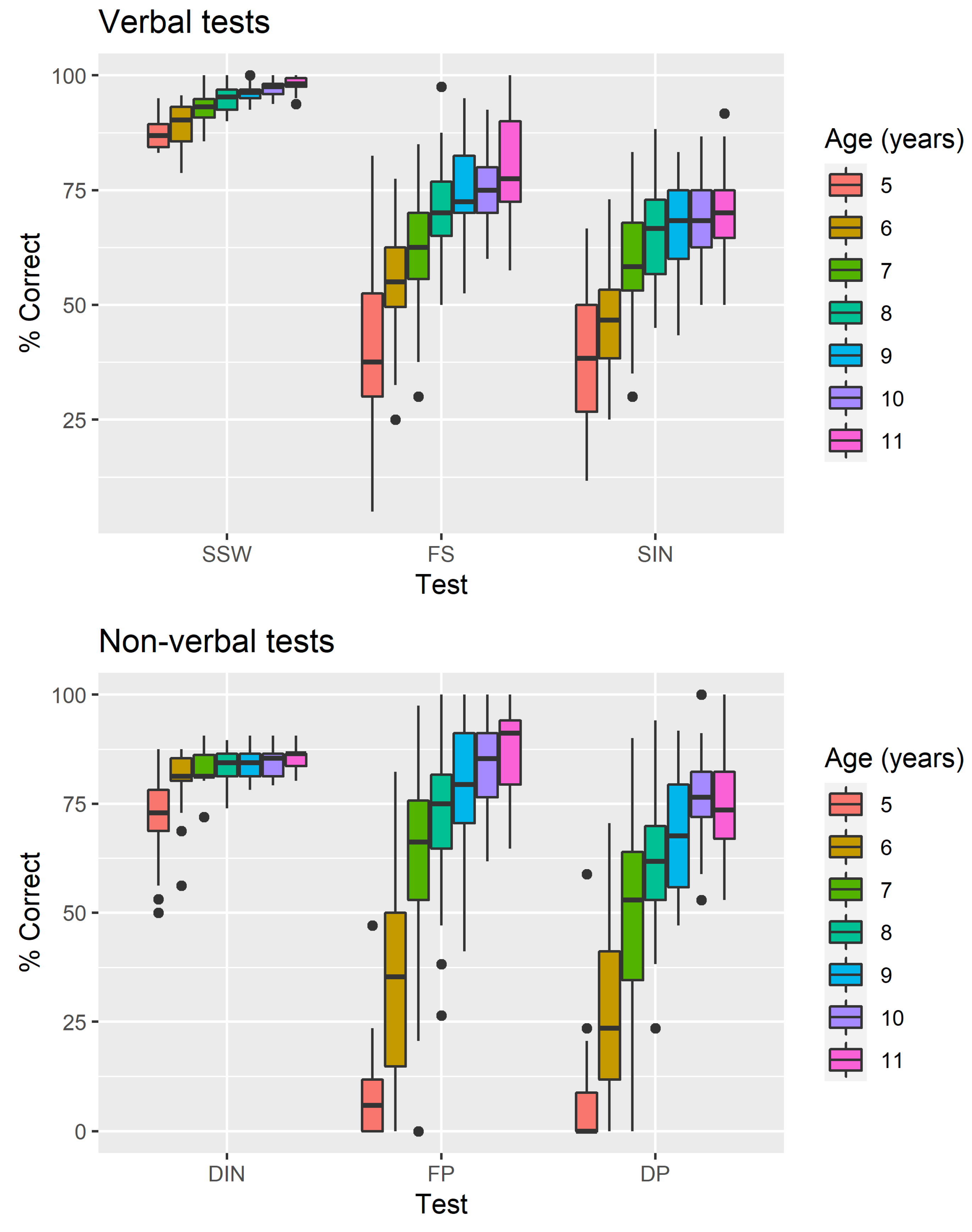
3.2. Results for Individual Tests
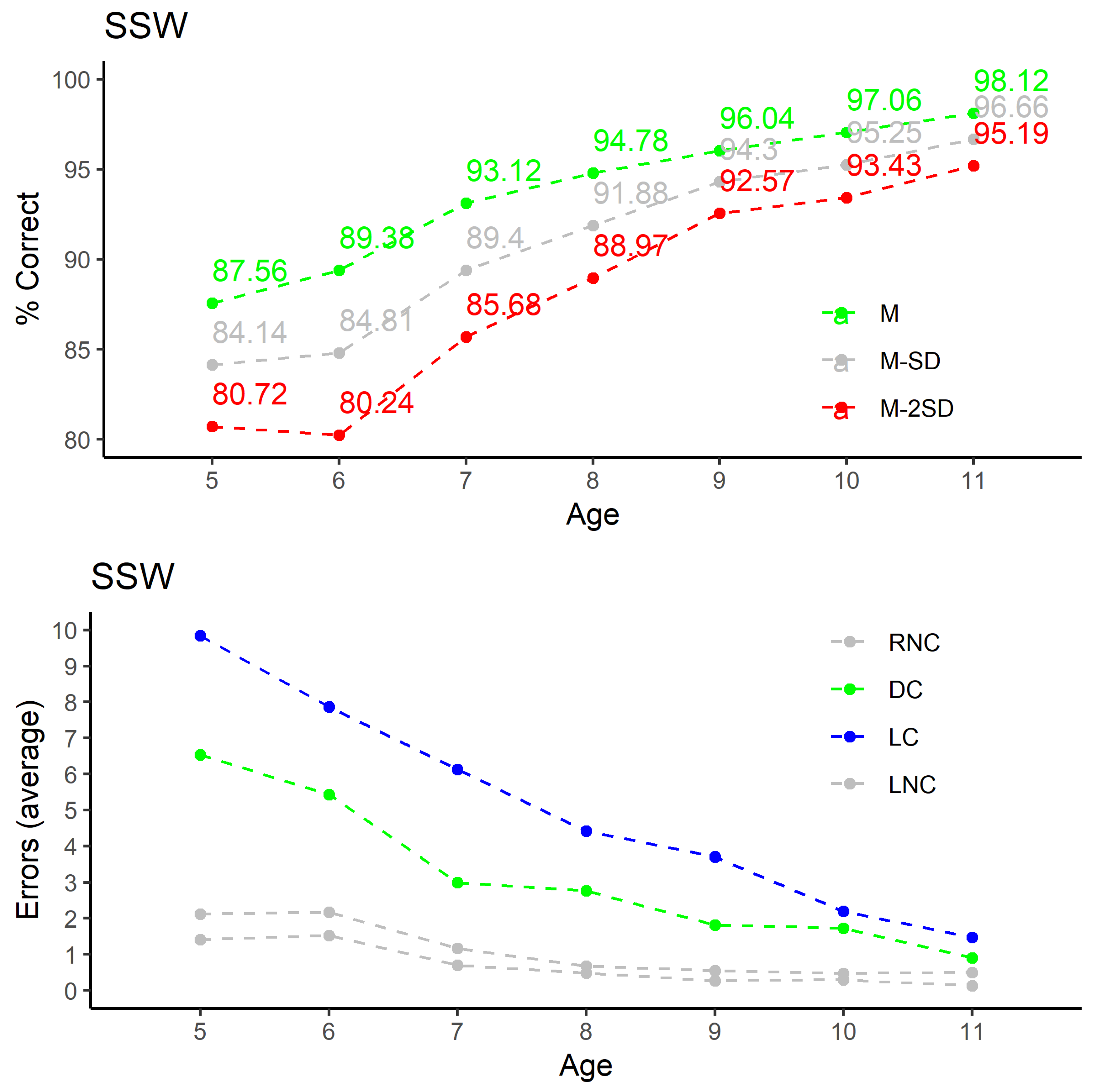
3.2.1. SSW for European Portuguese
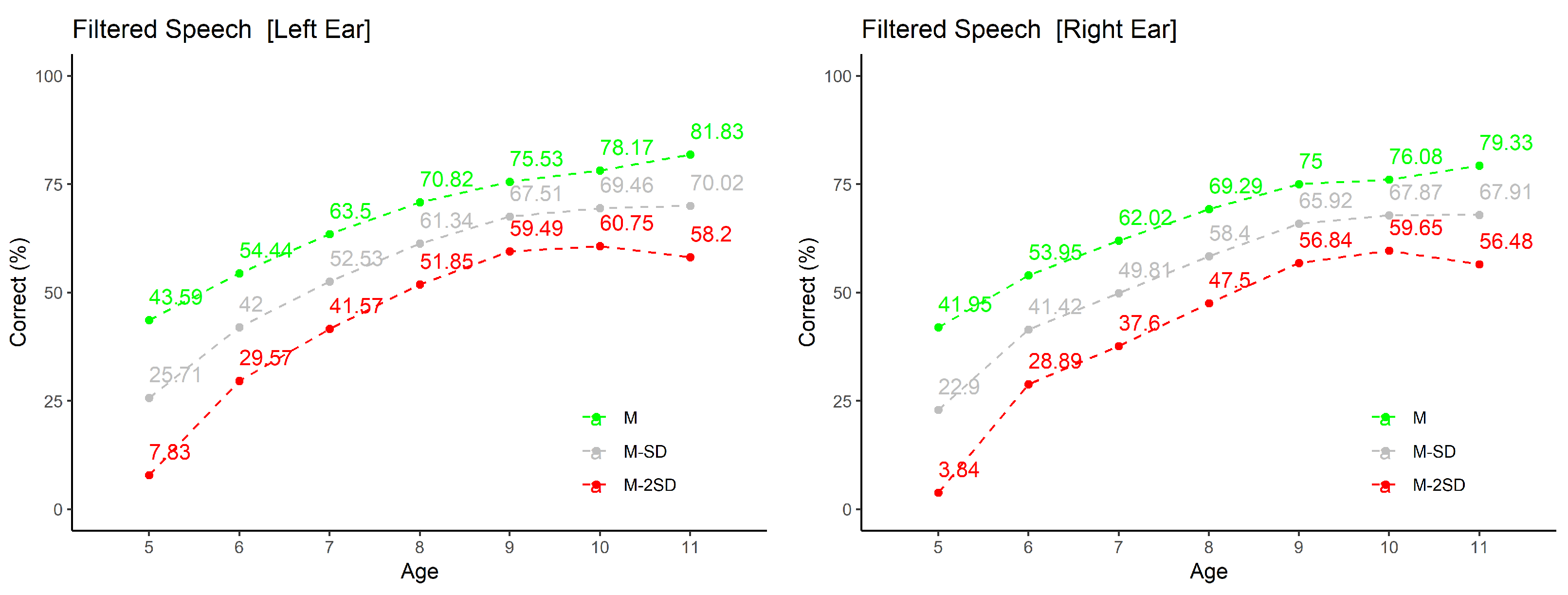
3.2.2. Filtered Speech
3.2.3. Speech in Noise
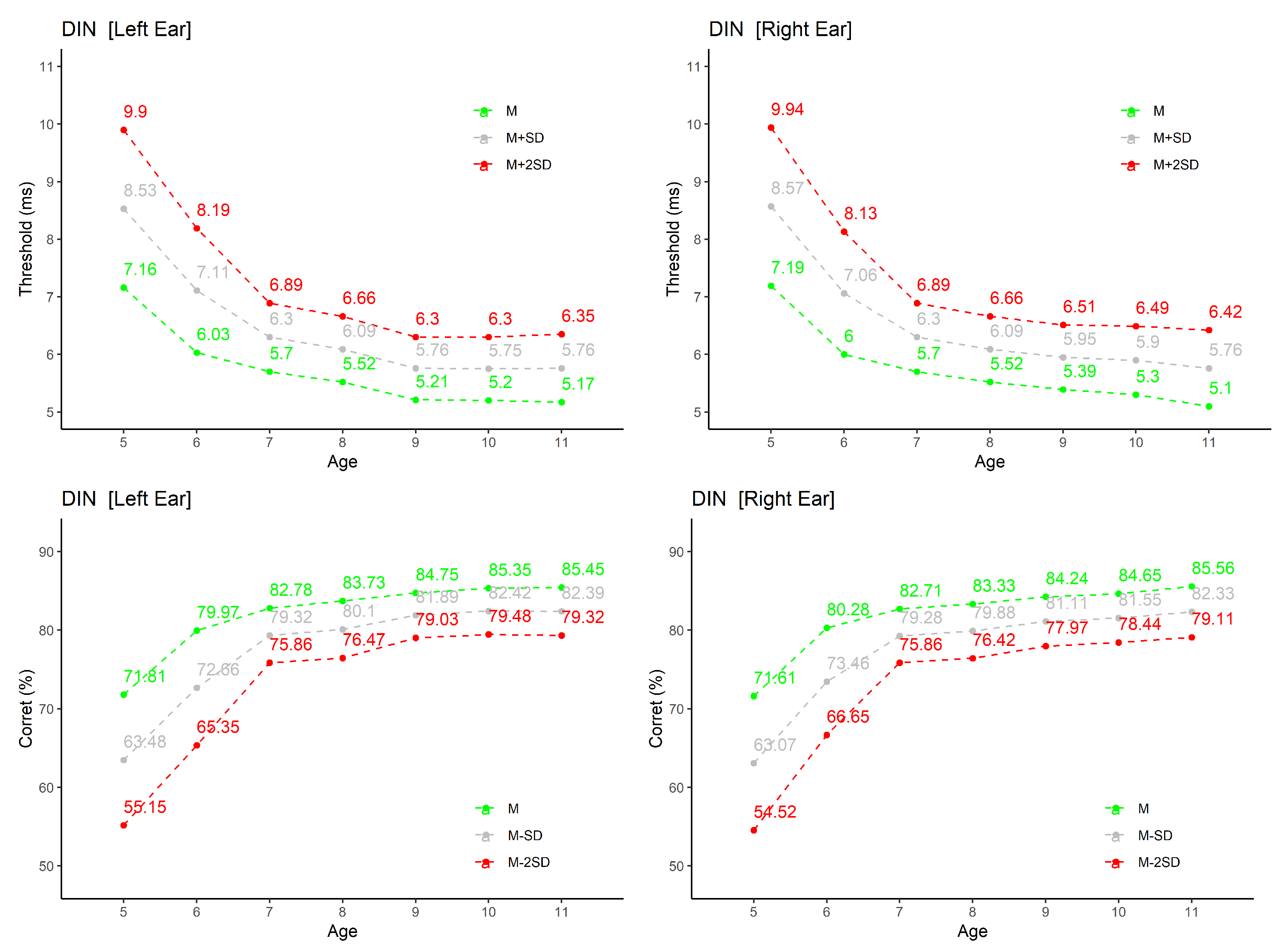
3.2.4. Detection of Interval in Noise
3.2.5. Frequency Pattern
3.2.6. Duration Pattern
4. Discussion
4.1. SSW for European Portuguese
4.2. Filtered Speech
4.3. Speech in Noise
4.4. Detection of Interval in Noise
4.5. Frequency Pattern
4.6. Duration Pattern
5. Conclusions
Future Work
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Keith, W.; Purdy, S.; Baily, M.; Kay, F. New Zealand Guidelines on Auditory Processing Disorder; New Zealand Audiological Society: Auckland, New Zealand, 2019. [Google Scholar]
- American Speech-Language-Hearing Association (ASHA). Central Auditory Processing Disorders; ASHA: Rockville, MD, USA, 2005. [Google Scholar]
- Iliadou, V.V.; Ptok, M.; Grech, H.; Pedersen, E.R.; Brechmann, A.; Deggouj, N.; Kiese-Himmel, C.; Śliwińska-Kowalska, M.; Nickisch, A.; Demanez, L.; et al. A European perspective on auditory processing disorder-current knowledge and future research focus. Front. Neurol. 2017, 8, 622. [Google Scholar] [CrossRef] [Green Version]
- Katz, J. The use of staggered spondaic words for assessing the integrity of the central auditory nervous-system. J. Audit. Res. 1962, 2, 327–337. [Google Scholar]
- Martins, J.H. Avaliação do Processamento Auditivo Central e Dificuldades de Aprendizagem. Ph.D. Thesis, University of Lisbon, Lisbon, Portugal, 2017. [Google Scholar]
- Keith, R.W. Development and standardization of SCAN-A: Test of auditory processing disorders in adolescents and adults. J. Am. Acad. Audiol. 1995, 6, 286. [Google Scholar] [PubMed]
- Keith, R.W. Development and standardization of SCAN-C test for auditory processing disorders in children. J. Am. Acad. Audiol. 2000, 11, 438–445. [Google Scholar] [PubMed]
- Domitz, D.M.; Schow, R.L. A New CAPD Battery—Multiple Auditory Processing Assessment. Am. J. Audiol. 2000, 9, 101–111. [Google Scholar] [CrossRef] [Green Version]
- Musiek, F.E.; Chermak, G.D. Three commonly asked questions about central auditory processing disorders: Assessment. Am. J. Audiol. 1994, 3, 23–27. [Google Scholar] [CrossRef] [PubMed]
- Task Force on Central Auditory Processing Consensus Development. Central auditory processing: Current status of research and implications for clinical practice. Am. J. Audiol. 1996, 5, 41–52. [Google Scholar] [CrossRef]
- Neijenhuis, K.; Snik, A.; Priester, G.; van Kordenoordt, S.; van den Broek, P. Age effects and normative data on a Dutch test battery for auditory processing disorders. Int. J. Audiol. 2002, 41, 334–346. [Google Scholar] [CrossRef] [PubMed]
- Yathiraj, A.; Maggu, A.R. Validation of the Screening Test for Auditory Processing (STAP) on school-aged children. Int. J. Pediatr. Otorhinolaryngol. 2014, 78, 479–488. [Google Scholar] [CrossRef] [PubMed]
- Mattsson, T.S.; Follestad, T.; Andersson, S.; Lind, O.; Øygarden, J.; Nordgård, S. Normative data for diagnosing auditory processing disorder in Norwegian children aged 7–12 years. Int. J. Audiol. 2018, 57, 10–20. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, E.R.; Dahl-Hansen, B.; Christensen-Dalsgaard, J.; Brandt, C. Implementation and evaluation of a Danish test battery for auditory processing disorder in children. Int. J. Audiol. 2017, 56, 538–549. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Audiology (AAA). American Academy of Audiology Clinical Practice Guidelines: Diagnosis, Treatment and Management of Children and Adults with Central Auditory Processing Disorder; AAA: Reston, VA, USA, 2010. [Google Scholar]
- Moore, D.R.; Cowan, J.A.; Riley, A.; Edmondson-Jones, A.M.; Ferguson, M.A. Development of auditory processing in 6-to 11-yr-old children. Ear Hear. 2011, 32, 269–285. [Google Scholar] [CrossRef] [PubMed]
- Canadian Interorganizational Steering Group for Speech-Language Pathology and Audiology. Canadian Guidelines on Auditory Processing Disorder in Children and Adults: Assessment and Intervention; CISG: Peterborough, ON, Canada, 2012. [Google Scholar]
- Whitelaw, G.M. Assessment and management of auditory processing disorders in children. In Pediatric Audiology: Diagnosis, Technology, and Management; Thieme Medical Publishers, Inc.: New York, NY, USA, 2008; pp. 145–155. [Google Scholar]
- Lucker, J. Auditory processing abilities in children: When to test? Audiol. Today 2015, 27, 24–31. [Google Scholar]
- Shapiro, Z. Don’t Wait to Diagnose Auditory Processing Disorder: A pediatric audiologist disagrees with the general philosophy of waiting until a child turns 7 to evaluate for auditory processing disorder. ASHA Lead. 2016, 21, 34–35. [Google Scholar] [CrossRef]
- Fonseca, V. Dificuldades de Aprendizagem; Artes Médicas: Porto Alegre, Brazil, 1995. [Google Scholar]
- British Society of Audiology (BSA). Position Statement and Practice Guidance Auditory Processing Disorder (APD); British Society of Audiology: West Lothian, UK, 2018. [Google Scholar]
- Ferre, J.M. Auditory dysfunction beyond the 8th nerve: Understanding central auditory processing disorders. Perspect. Hear. Hear. Disord. Res. Diagn. 2015, 19, 4–11. [Google Scholar] [CrossRef] [Green Version]
- Alves, M. Habilidades Auditivas e Linguagem em Crianças com Implante Coclear. Master’s Thesis, Mestrado em Ciências da Fala e da Audição, Universidade de Aveiro, Aveiro, Portugal, 2010. [Google Scholar]
- Martins, J.H. Testes de Avaliação do Processamento Auditivo Central: SSW em Português Europeu [Central Auditory Processing Evaluation Tests: SSW for European Portuguese]. Master’s Thesis, Mestrado em Ciências da Fala e da Audição, Universidade de Aveiro, Aveiro, Portugal, 2007. [Google Scholar]
- MATLAB; The MathWorks Inc.: Natick, MA, USA, 2007.
- Alves, M.; Teixeira, A.; Bastos, C.; Martins, J.H.; Ribeiro, C. Habilidades Auditivas e Linguagem em Crianças com Implante Coclear [Auditory Abilities and Language in Children with Cochlear Implant]. In Cadernos de Otorrinolaringologia; 2013; Available online: http://cadernosorl.com/artigos/15/6.pdf (accessed on 14 September 2021).
- Pinheiro, M.L. Tests of central auditory function in children with learning disabilities. In Central Auditory Dysfunction; Keith, R., Ed.; Grune & Stratton: New York, NY, USA, 1977; pp. 223–256. [Google Scholar]
- Baran, J.A. Test battery considerations. In Handbook of (Central) Auditory Processing Disorder; Musiek, F., Ed.; Plural Publishing: San Diego, CA, USA, 2007. [Google Scholar]
- Martins, J.H.; Teixeira, A. Bateria de Avaliação do Processamento Auditivo para o Português Europeu (BAPA-PE); WIDEX: Lisbon, Portugal, 2018. [Google Scholar]
- Wiley, M.; Wiley, J.F. Advanced R Statistical Programming and Data Models; Apress: Berkeley, CA, USA, 2019. [Google Scholar]
- Bellis, T. Assessment and Management of Central Auditory Processing Disorders in the Educational Setting: From Science to Practice; Delmar Learning: Clifton Park, NY, USA, 2003. [Google Scholar]
- Mangabeira-Albernaz, P.L. Logoaudiometria. In Processamento Auditivo Central: Manual de Avaliação; Pereira, L.D., Schochat, E., Eds.; Lovise: São Paulo, Brazil, 1997; pp. 37–42. [Google Scholar]
- Shinn, J.B.; Chermak, G.D.; Musiek, F.E. GIN (Gaps-In-Noise) performance in the pediatric population. J. Am. Acad. Audiol. 2009, 20, 229–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Musiek, F.E.; Baran, J.A. The Auditory System: Anatomy, Physiology, and Clinical Correlates; Pearson Education, Inc.: London, UK, 2006. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Battery | Ref | Information |
|---|---|---|
| SCAN-A: Test of Auditory Processing Disorders in Adolescents and Adults | [6] | Can be seen as an early example of a battery. Six tests: two filtered words (FW), two auditory figure-ground (AFG), a competing words (CW), and a competing sentences (CS). |
| SCAN-C: Test for Auditory Processing Disorders in Children-Revised | [7] | The improvements to the initial test included new test instructions to make them easier for young children, stimuli presented on a compact disc, revision of the Competing Words subtest, and the addition of a Competing Sentences subtest. Normative data were obtained on 650 children age 5 years to 11 years, 11 months old and published in 2000. |
| MAPA: Multiple Auditory Processing Assessment | [8] | Developed based on Musiek and Chermak [9] and ASHA recommendations [10] and published in 2000. Includes four commonly used tests, selected and recorded for use in assessing school children. The tests were administered to a sample of 81 third grade children along with the SCAN. Four separate factors emerged from the four MAPA tests: monaural separation/closure, auditory pattern/temporal ordering, binaural integration, and binaural separation. |
| Dutch battery | [11] | Originally developed to diagnose auditory processing disorders (APDs) in adults. Consists of eight tests: words-in noise, filtered speech, binaural fusion, dichotic digits, frequency and duration patterns, backward masking, categorical perception and digit span. Descriptive statistics were computed in 2002 on data obtained from 75 children from primary school (age 9–12 years) and 30 adolescents from secondary school (age 14–16 years) with normal hearing and intelligence. Age effects were present in most tests. |
| STAP: Screening Test for Auditory Processing | [12] | Contains four subsections: speech-in-noise, dichotic consonant vowel, gap detection and auditory memory. It was administered to 500 school-going children in the age range of 8–13 years (141 children at-risk on the Screening Checklist for Auditory Processing). |
| Norwegian Battery | [13] | Consists of Filtered Words, Competing Words, Dichotic Digits, Gaps In Noise, Duration and Frequency Pattern, Binaural Masking Level Difference, and HIST Speech in Noise test. A total of 268 normal hearing children aged 7–12 years participated in the study. Results, published in 2018, revealed no differences between genders. The children showed improving performance by age on all tests, except for the Gaps In Noise and Binaural Masking Level Difference. |
| Danish Auditory Processing Disorders (APD) battery | [14] | Published in 2017. Consists of four behavioral tests: the filtered words (FW) test, the dichotic digits (DD) test, the gap detection (GD) test, and the binaural masking level difference (BMLD) test. Evaluated on 158 children (75 boys and 83 girls, aged 6–16 years) with no known history of auditory problems to obtain normative values. |
| Test | Normality Criterion |
|---|---|
| Tonal audiogram | 20 dB HL at 125, 250, 500, 1000, 2000, 4000, 8000 Hz . |
| Bilateral tympanogram | Type A curve, ipsi and contralateral acoustic reflexes present within the normal range. (Acoustic admittance peak 0.35 to 1.25, mm H2O—between −50 to + 50 daPa.) |
| Otoacoustic emissions | Present within the normal range (DPOAE—F1 65 dB SPL, f2 50 dB SPL, SNR at 4/5, f2 frequencies 3dB higher than 2 standard deviations above the mean noise). |
| Analysis | Sec. | GLM Model |
|---|---|---|
| All Monaural | Section 3.1 | correct Test + Gender + Age + Ear + Region + Laterality + (1| Subject) |
| SSW (global) | Section 3.1 | correct Gender + Age + Region + Laterality + (1| Subject) |
| SSW | Section 3.2.1 | correct Age + Ear + Competition + (1| Subject) |
| FS | Section 3.2.2 | correct Age + Ear + (1| Subject) |
| SIN | Section 3.2.3 | correct Age + Ear + (1| Subject) |
| DIN | Section 3.2.4 | threshold Age + Ear + (1| Subject) |
| correct Age + Ear + (1| Subject) | ||
| FP | Section 3.2.5 | correct Age + Ear + numSegments + (1|Subject) |
| DP | Section 3.2.6 | correct Age + Ear + numSegments + (1|Subject) |
| Age | Bellis (2003) | Left | Right |
|---|---|---|---|
| 7 | 62 | 64 | 62 |
| 8 | 70 | 71 | 69 |
| 9 | 68 | 76 | 75 |
| 10 | 72 | 78 | 76 |
| 11 | 75 | 81 | 79 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martins, J.H.; Alves, M.; Andrade, S.; Falé, I.; Teixeira, A. Auditory Processing Disorder Test Battery in European Portuguese—Development and Normative Data for Pediatric Population. Audiol. Res. 2021, 11, 474-490. https://doi.org/10.3390/audiolres11030044
Martins JH, Alves M, Andrade S, Falé I, Teixeira A. Auditory Processing Disorder Test Battery in European Portuguese—Development and Normative Data for Pediatric Population. Audiology Research. 2021; 11(3):474-490. https://doi.org/10.3390/audiolres11030044
Chicago/Turabian StyleMartins, Jorge Humberto, Marisa Alves, Susana Andrade, Isabel Falé, and António Teixeira. 2021. "Auditory Processing Disorder Test Battery in European Portuguese—Development and Normative Data for Pediatric Population" Audiology Research 11, no. 3: 474-490. https://doi.org/10.3390/audiolres11030044