Vision-Assisted Interactive Human-in-the-Loop Distal Upper Limb Rehabilitation Robot and its Clinical Usability Test

 , , and
, , and
Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
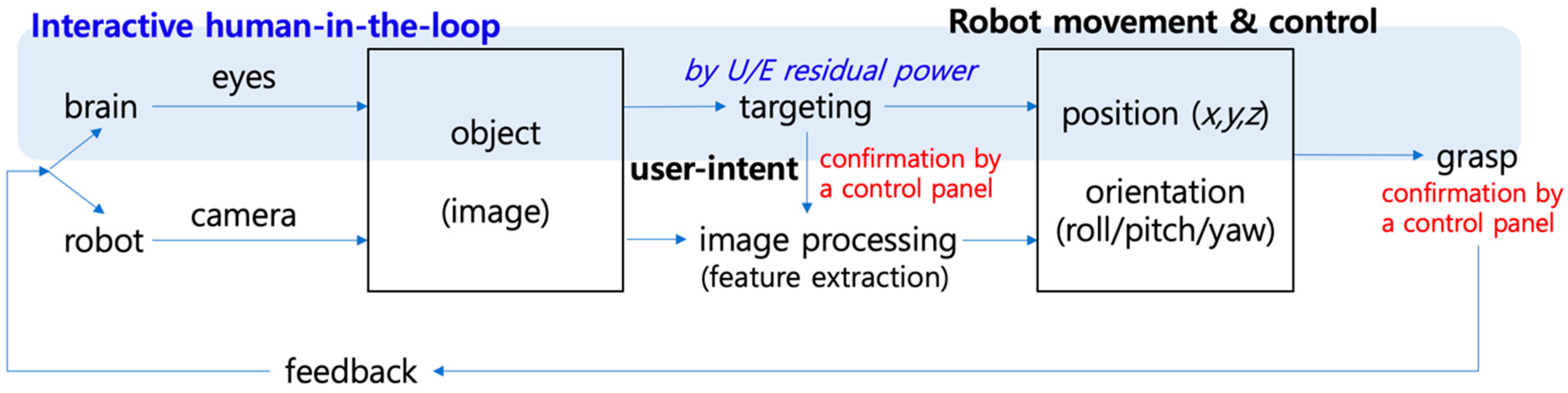
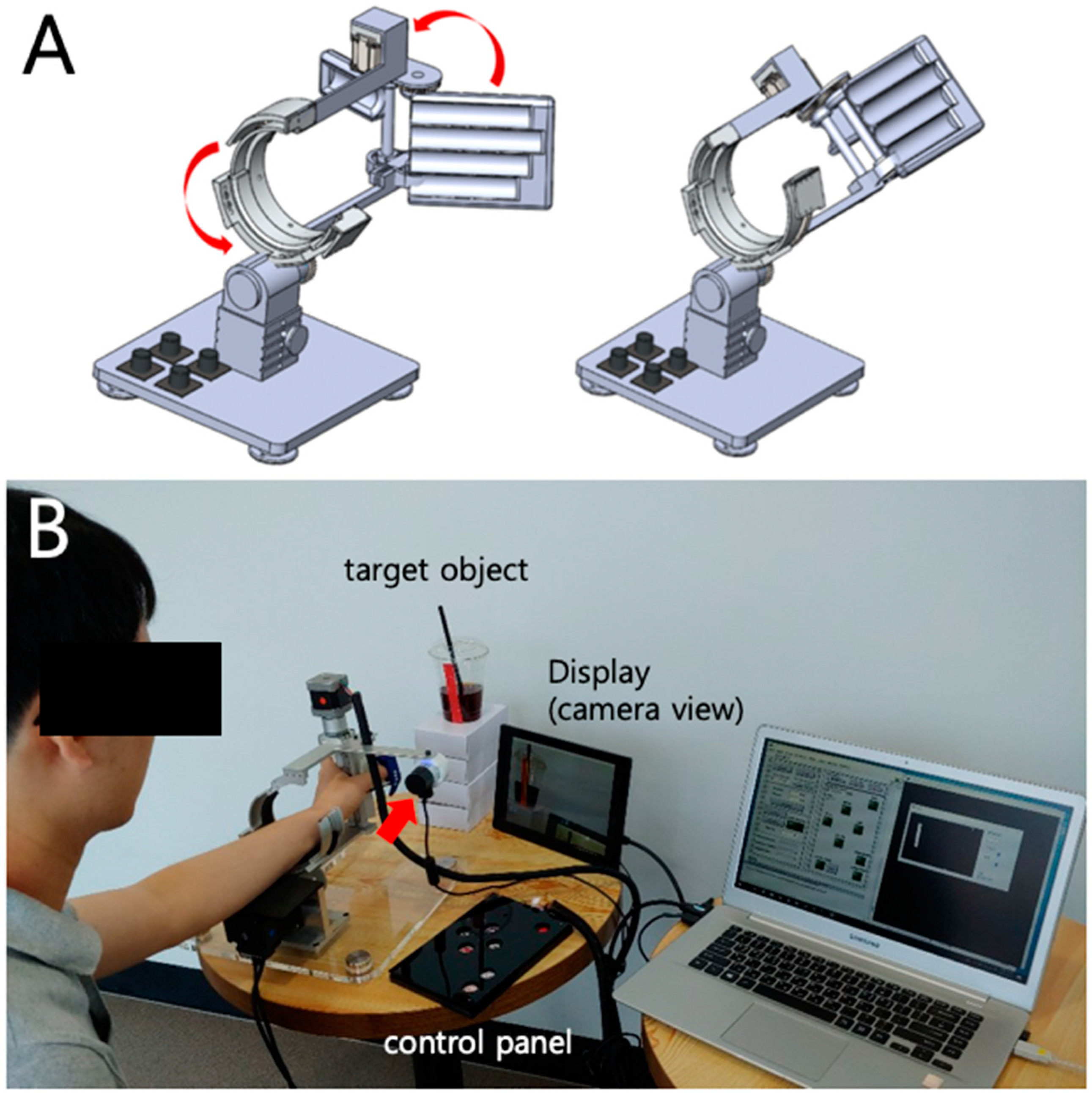
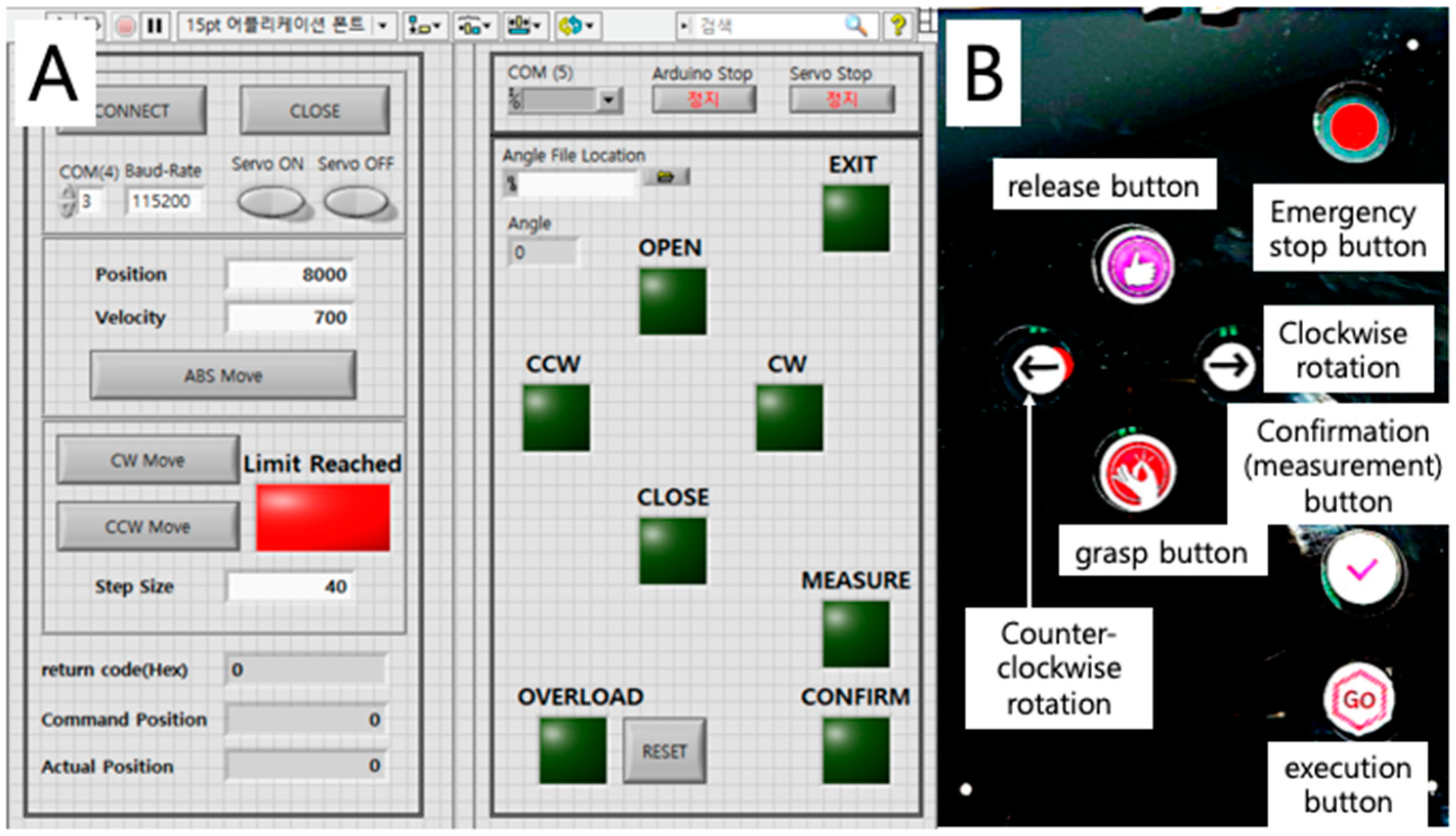
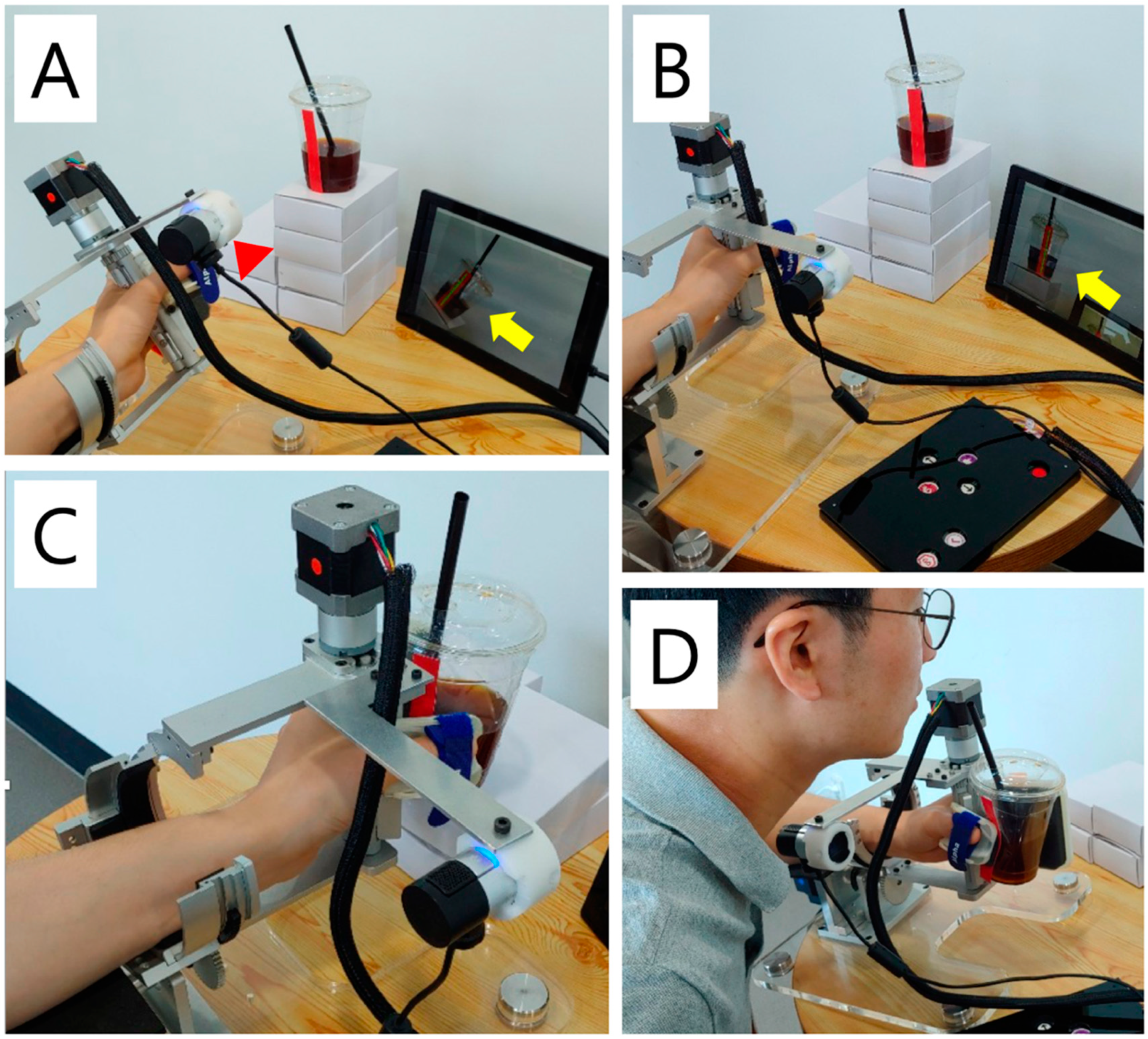
2.1. Development of a Vision-Assisted Distal Upper Limb Rehabilitation Robot
2.1.1. Design of a Two-Axis Distal Upper Limb Rehabilitation Robot
2.1.2. Assembly of the Robot
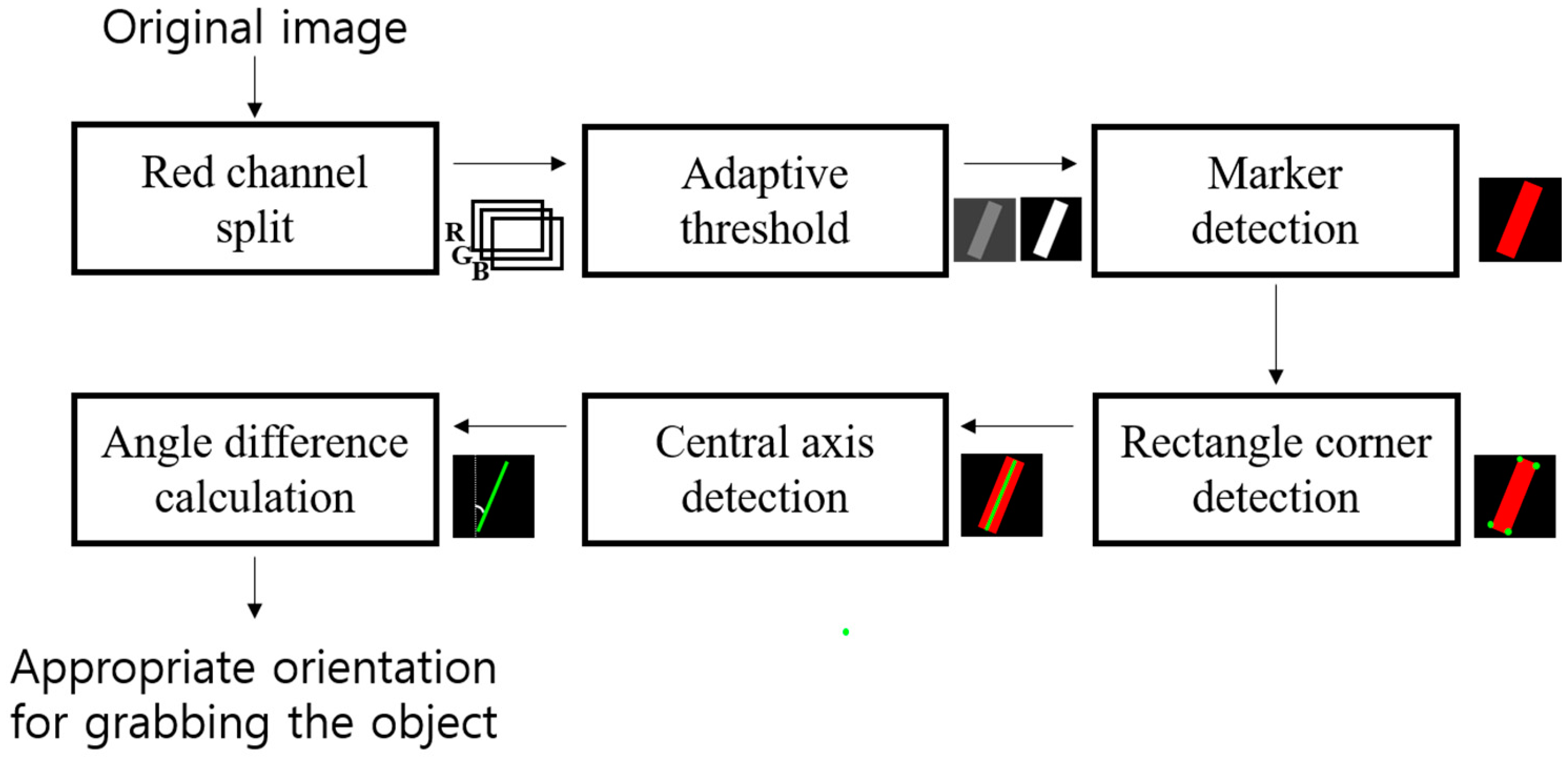
2.1.3. Image-Processing Algorithm for Recognizing User-intent
2.2. Preliminary Usability Test
2.2.1. Participants
2.2.2. Procedure
2.2.3. Statistical Analysis
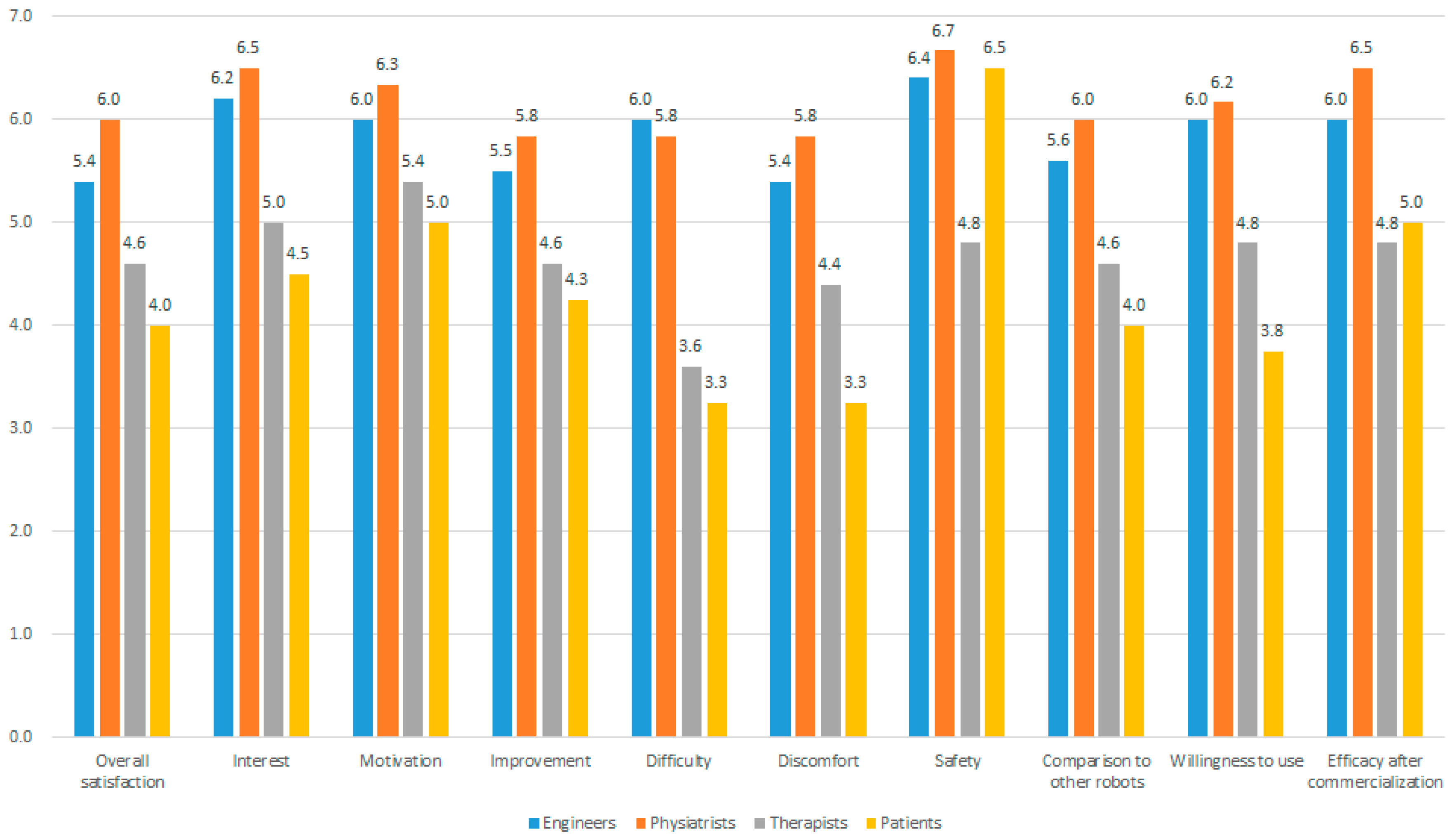
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Declaration
Conflicts of Interest
References
- Carolei, A.; Sacco, S.; De Santis, F.; Marini, C. Epidemiology of stroke. Clin. Exp. Hypertens. 2002, 24, 479–483. [Google Scholar] [CrossRef] [PubMed]
- Mehrholz, J.; Pohl, M.; Platz, T.; Kugler, J.; Elsner, B. Electromechanical and robot-assisted arm training for improving activities of daily living, arm function, and arm muscle strength after stroke. Cochrane Database Syst. Rev. 2012, 6. [Google Scholar] [CrossRef]
- Huang, V.S.; Krakauer, J.W. Robotic neurorehabilitation: A computational motor learning perspective. J. Neuroeng. Rehabil. 2009, 6, 5. [Google Scholar] [CrossRef] [PubMed]
- Mazzoleni, S.; Duret, C.; Grosmaire, A.G.; Battini, E. Combining Upper Limb Robotic Rehabilitation with Other Therapeutic Approaches after Stroke: Current Status, Rationale, and Challenges. Biomed. Res. Int. 2017, 2017, 8905637. [Google Scholar] [CrossRef] [PubMed]
- Colombo, R.; Pisano, F.; Mazzone, A.; Delconte, C.; Micera, S.; Carrozza, M.C.; Dario, P.; Minuco, G. Design strategies to improve patient motivation during robot-aided rehabilitation. J. Neuroeng. Rehabil. 2007, 4, 3. [Google Scholar] [CrossRef]
- Novak, D.; Nagle, A.; Keller, U.; Riener, R. Increasing motivation in robot-aided arm rehabilitation with competitive and cooperative gameplay. J. Neuroeng. Rehabil. 2014, 11, 64. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.H.; Kim, M.Y.; Lee, J.Y.; Jeon, Y.J.; Kim, S.; Lee, S.; Seo, B.; Choi, Y. Effects of virtual reality-based rehabilitation on distal upper extremity function and health-related quality of life: A single-blinded, randomized controlled trial. J. Neuroeng. Rehabil. 2016, 13, 17. [Google Scholar] [CrossRef]
- Gassert, R.; Dietz, V. Rehabilitation robots for the treatment of sensorimotor deficits: A neurophysiological perspective. J. Neuroeng. Rehabil. 2018, 15, 46. [Google Scholar] [CrossRef]
- Stroppa, F.; Loconsole, C.; Marcheschi, S.; Mastronicola, N.; Frisoli, A. An Improved Adaptive Robotic Assistance Methodology for Upper-Limb Rehabilitation. In Haptics: Science, Technology, and Applications; EuroHaptics. Lecture Notes in Computer Science; Springer: Cham, Switzerland, 2018; pp. 513–525. [Google Scholar]
- Steinisch, M.; Tana, M.G.; Comani, S. A post-stroke rehabilitation system integrating robotics, VR and high-resolution EEG imaging. IEEE Trans. Neural Syst. Rehabil. Eng. 2013, 21, 849–859. [Google Scholar] [CrossRef]
- Buongiorno, D.; Sotgiu, E.; Leonardis, D.; Marcheschi, S.; Solazzi, M.; Frisolo, A. WRES: A novel 3DoF WRist ExoSkeleton with tendon-driven differential transmission for neuro-rehabilitation and teleoperation. IEEE Robot. Autom. Lett. 2018, 3, 2152–2159. [Google Scholar] [CrossRef]
- Sarac, M.; Solazzi, M.; Sotgiu, E.; Bergamasco, M.; Frisoli, A. Design and kinematic optimization of a novel underactuated robotic hand exoskeleton. Meccanica 2017, 52, 749–761. [Google Scholar] [CrossRef]
- Villafane, J.H.; Taveggia, G.; Galeri, S.; Bissolotti, L.; Mulle, C.; Imperio, G.; Valdes, K.; Borboni, A.; Negrini, S. Efficacy of Short-Term Robot-Assisted Rehabilitation in Patients with Hand Paralysis After Stroke: A Randomized Clinical Trial. Hand 2018, 13, 95–102. [Google Scholar] [CrossRef] [PubMed]
- In, H.; Cho, K.J.; Kim, K.; Lee, B. Jointless structure and under-actuation mechanism for compact hand exoskeleton. In Proceedings of the 2011 IEEE International Conference on Rehabilitation Robotics, Zurich, Switzerland, 29 June–1 July 2011. [Google Scholar]
- Bertani, R.; Melegari, C.; De Cola, M.C.; Bramanti, A.; Bramanti, P.; Calabro, R.S. Effects of robot-assisted upper limb rehabilitation in stroke patients: A systematic review with meta-analysis. Neurol. Sci. 2017, 38, 1561–1569. [Google Scholar] [CrossRef] [PubMed]
- Lo, H.S.; Xie, S.Q. Exoskeleton robots for upper-limb rehabilitation: State of the art and future prospects. Med. Eng. Phys. 2012, 34, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Mazzoleni, S.; Sale, P.; Tiboni, M.; Franceschini, M.; Carrozza, M.C.; Posteraro, F. Upper limb robot-assisted therapy in chronic and subacute stroke patients: A kinematic analysis. Converg. Clin. Eng. Res. Neurorehabilit. 2013, 92, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Klamroth-Marganska, V.; Blanco, J.; Campen, K.; Curt, A.; Dietz, V.; Ettlin, T.; Felder, M.; Fellinghauer, B.; Guidali, M.; Kollmar, A.; et al. Three-dimensional, task-specific robot therapy of the arm after stroke: A multicentre, parallel-group randomised trial. Lancet Neurol. 2014, 13, 159–166. [Google Scholar] [CrossRef]
- Ho, N.S.; Tong, K.Y.; Hu, X.L.; Fung, K.L.; Wei, X.J.; Rong, W.; Susanto, E.A. An EMG-driven exoskeleton hand robotic training device on chronic stroke subjects: Task training system for stroke rehabilitation. In Proceedings of the IEEE International Conference on Rehabilitation Robotics, Zurich, Switzerland, 29 June–1 July 2011; pp. 1–5. [Google Scholar] [CrossRef]
- Krabben, T.; Prange, G.B.; Molier, B.I.; Stienen, A.H.; Jannink, M.J.; Buurke, J.H.; Rietman, J.S. Influence of gravity compensation training on synergistic movement patterns of the upper extremity after stroke, a pilot study. J. Neuroeng. Rehabil. 2012, 9, 44. [Google Scholar] [CrossRef] [PubMed]
- Masiero, S.; Armani, M.; Ferlini, G.; Rosati, G.; Rossi, A. Randomized trial of a robotic assistive device for the upper extremity during early inpatient stroke rehabilitation. Neurorehabil. Neural Repair 2014, 28, 377–386. [Google Scholar] [CrossRef]
- Krakauer, J.W. Arm function after stroke: From physiology to recovery. Semin. Neurol. 2005, 25, 384–395. [Google Scholar] [CrossRef] [PubMed]
- Jarrasse, N.; Proietti, T.; Crocher, V.; Robertson, J.; Sahbani, A.; Morel, G.; Roby-Brami, A. Robotic exoskeletons: A perspective for the rehabilitation of arm coordination in stroke patients. Front. Hum. Neurosci. 2014, 8, 947. [Google Scholar] [CrossRef]
- Collinger, J.L.; Wodlinger, B.; Downey, J.E.; Wang, W.; Tyler-Kabara, E.C.; Weber, D.J.; McMorland, A.J.; Velliste, M.; Boninger, M.L.; Schwartz, A.B. High-performance neuroprosthetic control by an individual with tetraplegia. Lancet 2013, 381, 557–564. [Google Scholar] [CrossRef] [Green Version]
- Kwak, N.S.; Muller, K.R.; Lee, S.W. A lower limb exoskeleton control system based on steady state visual evoked potentials. J. Neural. Eng. 2015, 12, 056009. [Google Scholar] [CrossRef]
- Kim, Y.J.; Park, S.W.; Yeom, H.G.; Bang, M.S.; Kim, J.S.; Chung, C.K.; Kim, S. A study on a robot arm driven by three-dimensional trajectories predicted from non-invasive neural signals. Biomed. Eng. Online 2015, 14, 81. [Google Scholar] [CrossRef] [Green Version]
- Downey, J.E.; Weiss, J.M.; Muelling, K.; Venkatraman, A.; Valois, J.S.; Hebert, M.; Bagnell, J.A.; Schwartz, A.B.; Collinger, J.L. Blending of brain-machine interface and vision-guided autonomous robotics improves neuroprosthetic arm performance during grasping. J. Neuroeng. Rehabil. 2016, 13, 28. [Google Scholar] [CrossRef] [Green Version]
- Bang, M.S.; Kim, S.; Nam, H.S.; Kim, Y.J.; Oh, B.M.; Beom, J.; Seo, H.G.; Leigh, J.H.; Koh, S.; Park, S.W. Upper Limb Rehabilitation Robot Module and Upper Limb Rehabilitation System for Precision Control by Image Processing. Korean Patent 1018316020000, 19 February 2018. [Google Scholar]
- Nam, H.S.; Lee, W.H.; Seo, H.G.; Kim, Y.J.; Bang, M.S.; Kim, S. Inertial measurement unit based upper extremity motion characterization for action research arm test and activities of daily living. Sensors 2019, 19, 1782. [Google Scholar] [CrossRef]
- Kang, B.B.; Choi, H.; Lee, H.; Cho, K.J. Exo-Glove Poly II: A Polymer-Based Soft Wearable Robot for the Hand with a Tendon-Driven Actuation System. Soft Robot 2018. [Google Scholar] [CrossRef] [PubMed]
- Sale, P.; Mazzoleni, S.; Lombardi, V.; Galafate, D.; Massimiani, M.P.; Posteraro, F.; Damiani, C.; Franceschini, M. Recovery of hand function with robot-assisted therapy in acute stroke patients: A randomized-controlled trial. Int. J. Rehabil. Res. 2014, 37, 236–242. [Google Scholar] [CrossRef] [PubMed]
- Crinion, J.T.; Leff, A.P. Recovery and treatment of aphasia after stroke: Functional imaging studies. Curr. Opin. Neurol. 2007, 20, 667–673. [Google Scholar] [CrossRef] [PubMed]
- Rao, D.; Le, Q.V.; Phoka, T.; Quigley, M.; Sudsang, A.; Ng, A.Y. Grasping novel objects with depth segmentation. In Proceedings of the Intelligent Robots and Systems, Taipei, Taiwan, 18–22 Octember 2010; pp. 2578–2585. [Google Scholar]
- Zhao, X.; Dou, L.; Su, Z.; Liu, N. Study of the navigation method for a snake robot based on the kinematics model with MEMS IMU. Sensors 2018, 18, 879. [Google Scholar] [CrossRef] [PubMed]
- Coad, M.M.; Blumenschein, L.H.; Cutler, S.; Reyna Zepeda, J.A.; Naclerio, N.D.; El-Hussieny, H.; Mehmood, U.; Ryu, J.H.; Hawkes, E.W.; Okamura, A.M. Vine robots: Design, teleoperation, and deployment for navigation and exploration. arXiv 2019, arXiv:1903.00069. [Google Scholar]
- Bishop, P.A.; Herron, R.L. Use and Misuse of the Likert Item Responses and Other Ordinal Measures. Int. J. Exerc. Sci. 2015, 8, 297. [Google Scholar]
- Zrenner, C.; Belardinelli, P.; Muller-Dahlhaus, F.; Ziemann, U. Closed-loop neuroscience and non-invasive brain stimulation: A tale of two loops. Front. Cell. Neurosci. 2016, 10, 92. [Google Scholar] [CrossRef]
- Alia, C.; Spalletti, C.; Lai, S.; Panarese, A.; Lamola, G.; Bertolucci, F.; Vallone, F.; Di Garbo, A.; Chisari, C.; Micera, S.; et al. Neuroplastic changes following brain ischemia and their contribution to stroke recovery: Novel approaches in neurorehabilitation. Front. Cell. Neurosci. 2017, 11, 76. [Google Scholar] [CrossRef]
- Pei, Y.C.; Chen, J.L.; Wong, A.M.K.; Tseng, K.C. An evaluation of the design and usability of a novel robotic bilateral arm rehabilitation device for patients with stroke. Front. Neurorobot. 2017, 11, 36. [Google Scholar] [CrossRef]
- Yang, J.; Xie, H.; Shi, J. A novel motion-coupling design for a jointless tendon-driven finger exoskeleton for rehabilitation. Mech. Mach. Theory 2016, 99, 83–102. [Google Scholar] [CrossRef]
- Almassri, A.M.; Wan Hasan, W.Z.; Ahmad, S.A.; Ishak, A.J.; Ghazali, A.M.; Talib, D.N.; Wada, C. Pressure sensor: State of the art, design, and application for robotic hand. J. Sens. 2015, 2015, 12. [Google Scholar] [CrossRef]
- He, Y.; Eguren, D.; Luu, T.P.; Contreras-Vidal, J.L. Risk management and regulations for lower limb medical exoskeletons: A review. Med. Devices 2017, 10, 89. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Raised Issue | Potential Solution |
|---|---|
| - Need for feedback at the end of range while grasping to avoid over-actuation. | - Insertion of pressure sensors for tactile feedback. |
| - Contour and fitting of the hand part needs improvement. | - Individualized manufacture of the hand part with three-dimensional printers. |
| - It would be better if active assistive exercise function was included. | - Insertion of force sensors to recognize active movements of the patients. |
| - Switch pad should be more simple and easier to use and control, especially when considering elderly patients. | - Object recognition and consequent robot movement could be automatized using image-based machine learning algorithm. |
| - The size of the robot needs to be reduced and redundant cables should be minimized. | - Design modification necessary when developing final prototype for mass production and also medical device approval process. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nam, H.S.; Hong, N.; Cho, M.; Lee, C.; Seo, H.G.; Kim, S. Vision-Assisted Interactive Human-in-the-Loop Distal Upper Limb Rehabilitation Robot and its Clinical Usability Test. Appl. Sci. 2019, 9, 3106. https://doi.org/10.3390/app9153106
Nam HS, Hong N, Cho M, Lee C, Seo HG, Kim S. Vision-Assisted Interactive Human-in-the-Loop Distal Upper Limb Rehabilitation Robot and its Clinical Usability Test. Applied Sciences. 2019; 9(15):3106. https://doi.org/10.3390/app9153106
Chicago/Turabian StyleNam, Hyung Seok, Nhayoung Hong, Minwoo Cho, Chiwon Lee, Han Gil Seo, and Sungwan Kim. 2019. "Vision-Assisted Interactive Human-in-the-Loop Distal Upper Limb Rehabilitation Robot and its Clinical Usability Test" Applied Sciences 9, no. 15: 3106. https://doi.org/10.3390/app9153106