
3D Printing in Surgical Planning and Intra-Operative Assistance: A Case Report on Cervical Deformity Correction Surgery
 , , , ,
, , , ,
Abstract
:1. Introduction
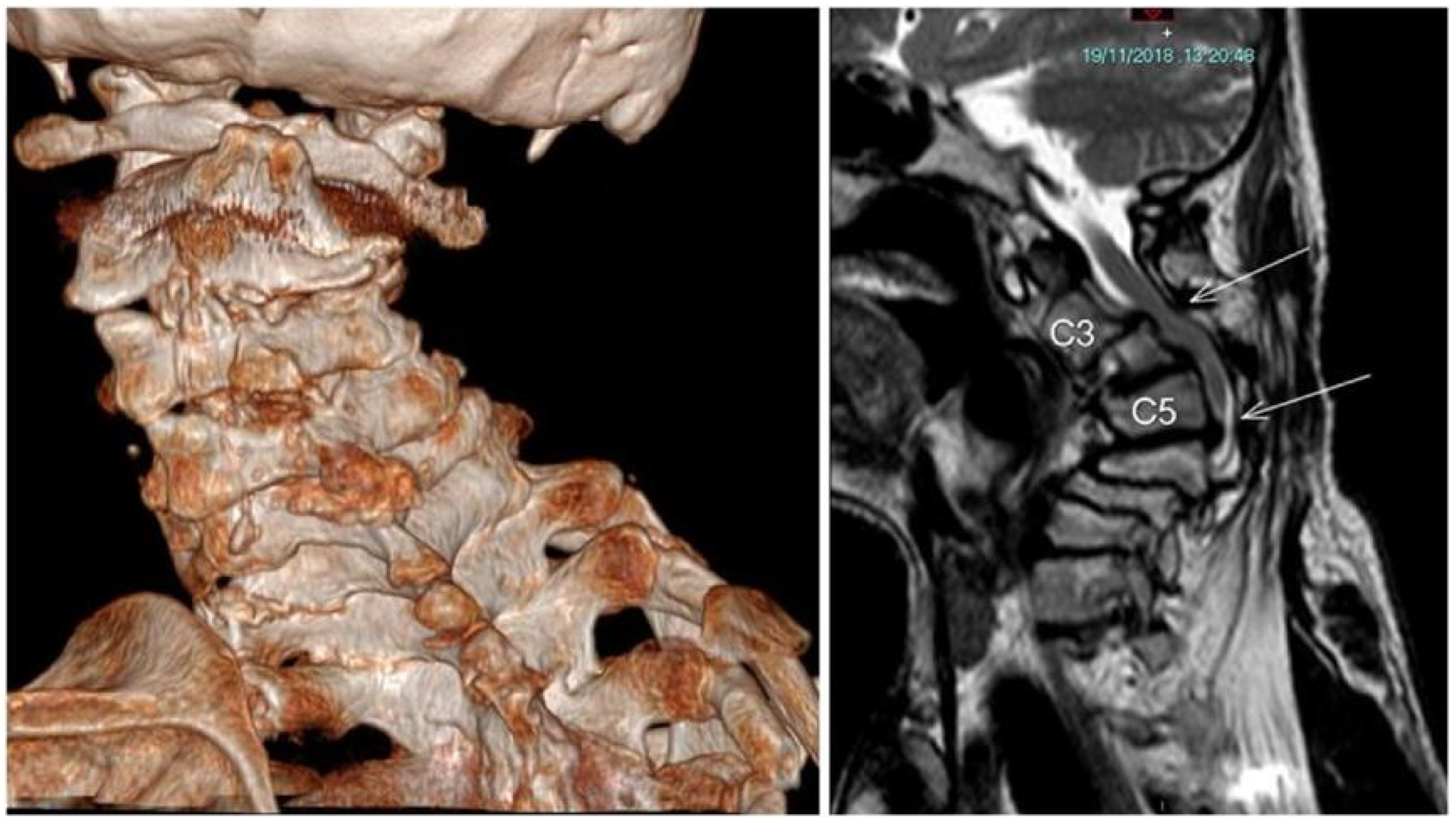
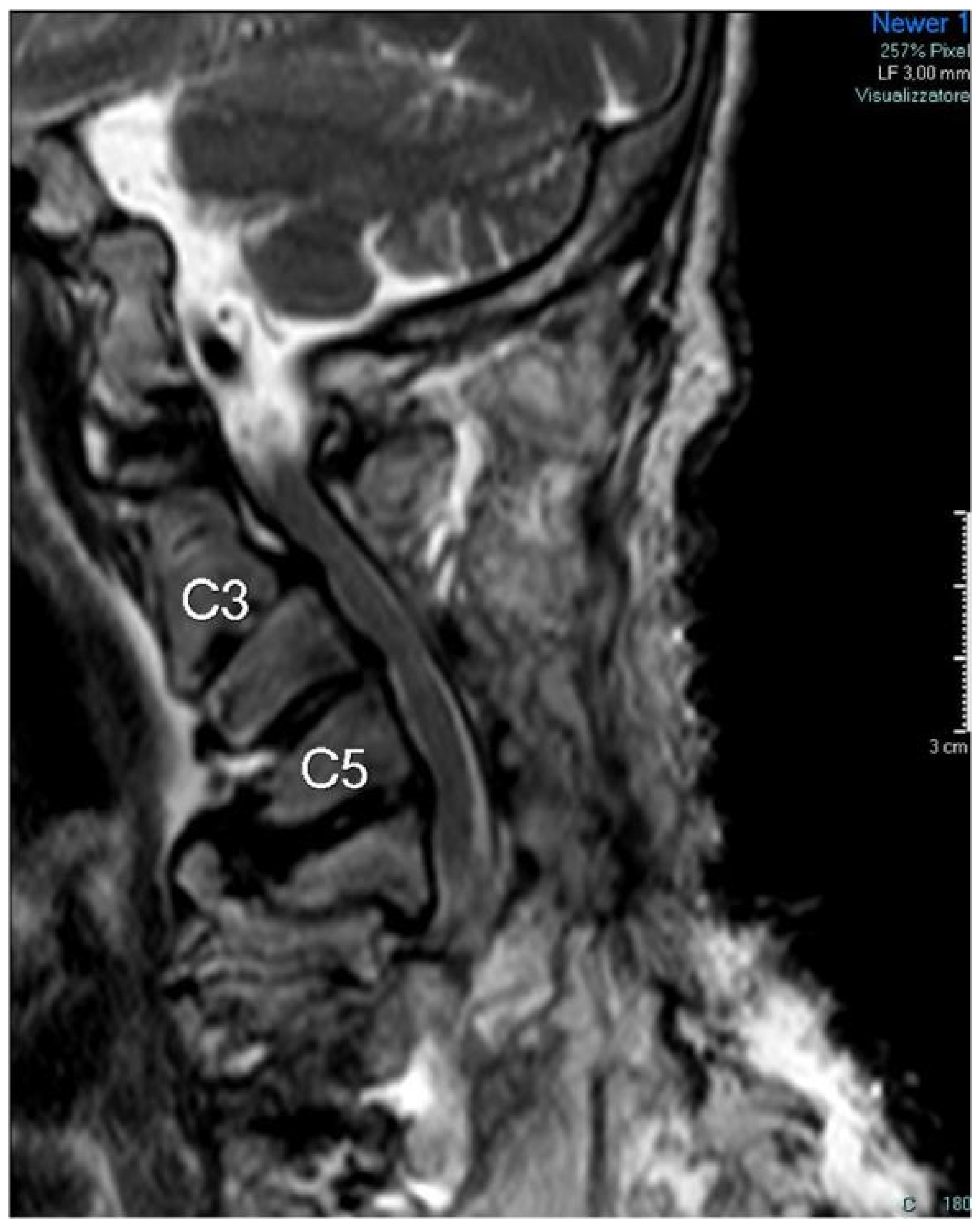
2. Case Description
Patient Details
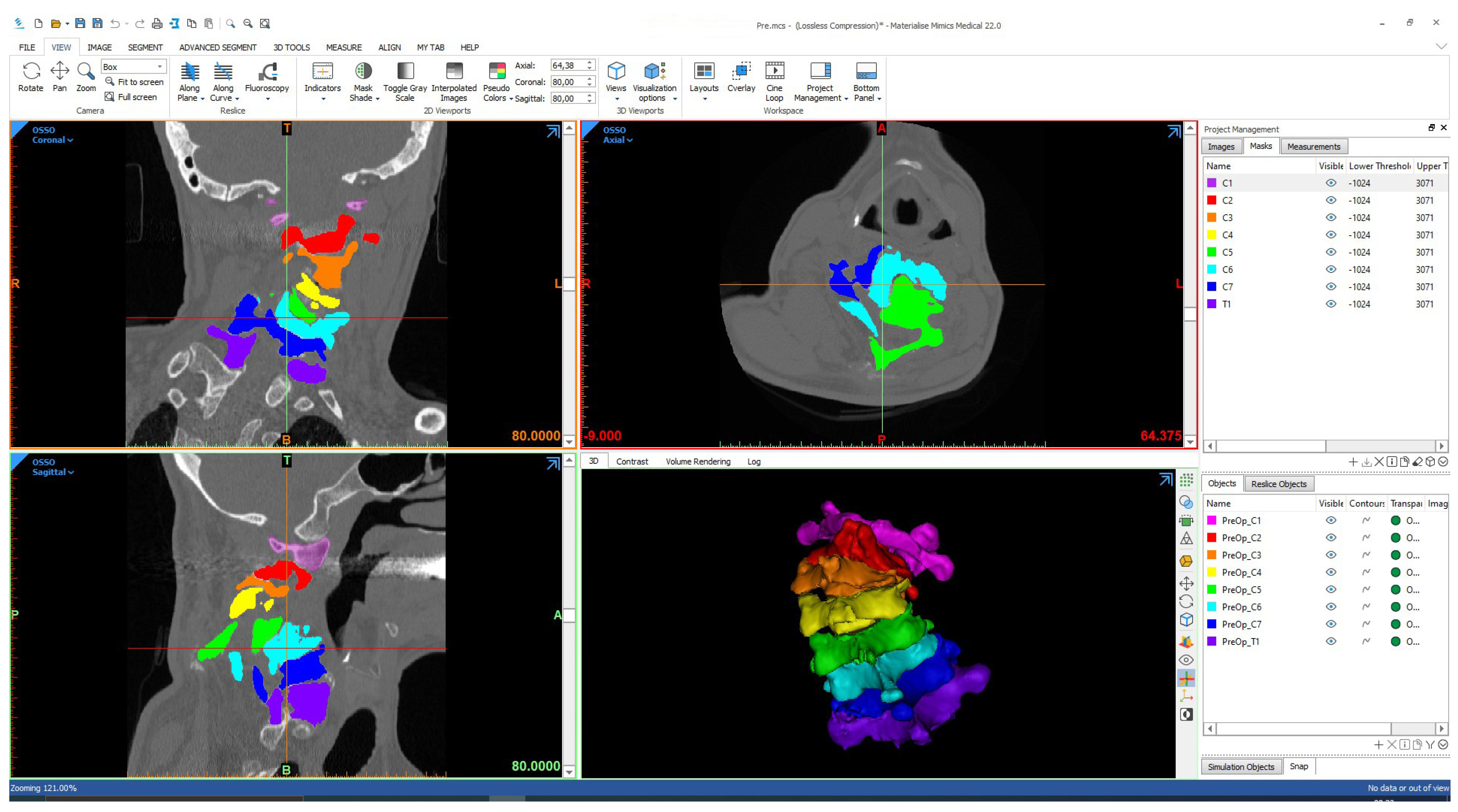
3. 3D Modelling, Printing, and Surgical Planning
4. Surgical Procedure
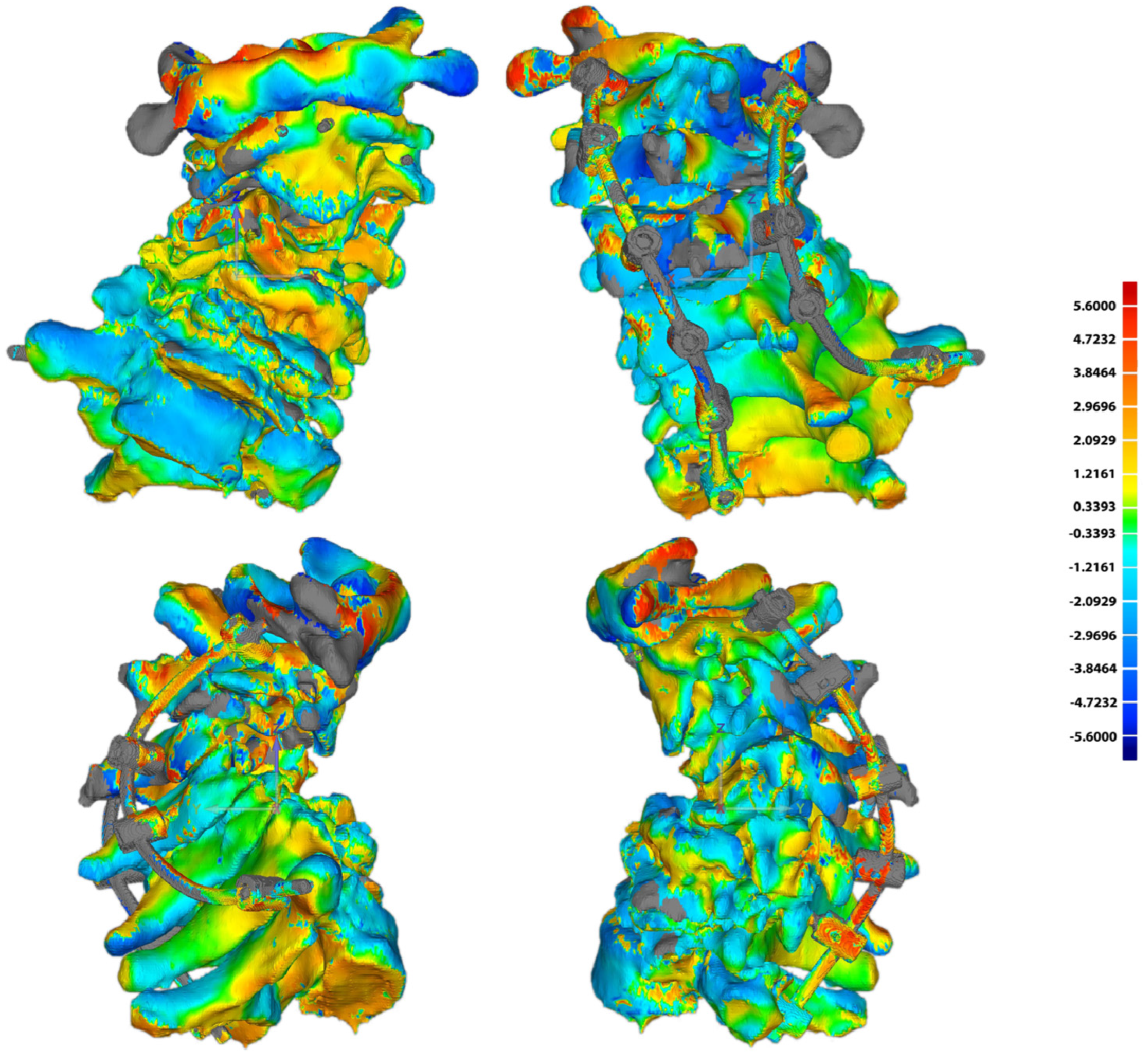
5. Follow-Up Control
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Scheer, J.K.; Tang, J.A.; Smith, J.S.; Acosta, F.L., Jr.; Protopsaltis, T.S.; Blondel, B.; Bess, S.; Shaffrey, C.I.; Deviren, V.; Lafage, V.; et al. International Spine Study G (2013) Cervical spine alignment, sagittal deformity, and clinical implications: A review. J. Neurosurg. Spine 2013, 19, 141–159. [Google Scholar] [CrossRef] [Green Version]
- Dru, A.B.; Lockney, D.T.; Vaziri, S.; Decker, M.; Polifka, A.J.; Fox, W.C.; Hoh, D.J. Cervical Spine Deformity Correction Techniques. Neurospine 2019, 16, 470–482. [Google Scholar] [CrossRef] [Green Version]
- Sharan, A.D.; Krystal, J.D.; Singla, A.; Nassr, A.; Kang, J.D.; Riew, K.D. Advances in the understanding of cervical spine deformity. Instr. Course Lect. 2015, 64, 417–426. [Google Scholar]
- Yeom, J.S.; Buchowski, J.M.; Kim, H.J.; Chang, B.S.; Lee, C.K.; Riew, K.D. Risk of vertebral artery injury: Comparison between C1-C2 transarticular and C2 pedicle screws. Spine J. 2013, 13, 775–785. [Google Scholar] [CrossRef]
- Guo, F.; Dai, J.; Zhang, J.; Ma, Y.; Zhu, G.; Shen, J.; Niu, G. Individualized 3D printing navigation template for pedicle screw fixation in upper cervical spine. PLoS ONE 2017, 12, e0171509. [Google Scholar] [CrossRef] [Green Version]
- Rahmathulla, G.; Nottmeier, E.W.; Pirris, S.M.; Deen, H.G.; Pichelmann, M.A. Intraoperative image-guided spinal navigation: Technical pitfalls and their avoidance. Neurosurg. Focus 2014, 36, E3. [Google Scholar] [CrossRef] [Green Version]
- Durastanti, G.; Leardini, A.; Siegler, S.; Durante, S.; Bazzocchi, A.; Belvedere, C. Comparison of cartilage and bone morphological models of the ankle joint derived from different medical imaging technologies. Quant. Imaging Med. Surg. 2019, 9, 1368–1382. [Google Scholar] [CrossRef]
- Matsiushevich, K.; Belvedere, C.; Leardini, A.; Durante, S. Quantitative comparison of freeware software for bone mesh from DICOM files. J. Biomech. 2019, 84, 247–251. [Google Scholar] [CrossRef]
- Belvedere, C.; Ortolani, M.; Marcelli, E.; Bortolani, B.; Matsiushevich, K.; Durante, S.; Cercenelli, L.; Leardini, A. Comparison of Bone Segmentation Software over Different Anatomical Parts. Appl. Sci. 2022, 12, 6097. [Google Scholar] [CrossRef]
- Fidanza, A.; Perinetti, T.; Logroscino, G.; Saracco, M. 3D Printing Applications in Orthopaedic Surgery: Clinical Experience and Opportunities. Appl. Sci. 2022, 12, 3245. [Google Scholar] [CrossRef]
- Salazar, D.; Huff, T.J.; Cramer, J.; Wong, L.; Linke, G.; Zuniga, J. Use of a three-dimensional printed anatomical model for tumor management in a pediatric patient. SAGE Open Med. Case Rep. 2020, 8, 2050313X2092760. [Google Scholar] [CrossRef]
- Belvedere, C.; Siegler, S.; Fortunato, A.; Caravaggi, P.; Liverani, E.; Durante, S.; Ensini, A.; Konow, T.; Leardini, A. New comprehensive procedure for custom-made total ankle replacements: Medical imaging, joint modeling, prosthesis design, and 3D printing. J. Orthop. Res. 2019, 37, 760–768. [Google Scholar] [CrossRef]
- Chen, P.C.; Chang, C.C.; Chen, H.T.; Lin, C.Y.; Ho, T.Y.; Chen, Y.J.; Tsai, C.H.; Tsou, H.K.; Lin, C.S.; Chen, Y.W.; et al. The Accuracy of 3D Printing Assistance in the Spinal Deformity Surgery. Biomed. Res. Int. 2019, 2019, 7196528. [Google Scholar] [CrossRef] [Green Version]
- Baskaran, V.; Strkalj, G.; Strkalj, M.; Di Ieva, A. Current Applications and Future Perspectives of the Use of 3D Printing in Anatomical Training and Neurosurgery. Front. Neuroanat. 2016, 10, 69. [Google Scholar] [CrossRef] [Green Version]
- Anderson, P.A. Clinical Applications of 3D Printing. Spine 2017, 42 (Suppl. S7), S30–S31. [Google Scholar] [CrossRef]
- Garg, B.; Mehta, N. Current status of 3D printing in spine surgery. J. Clin. Orthop. Trauma 2018, 9, 218–225. [Google Scholar] [CrossRef]
- Siegler, S.; Konow, T.; Belvedere, C.; Ensini, A.; Kulkarni, R.; Leardini, A. Analysis of surface-to-surface distance mapping during three-dimensional motion at the ankle and subtalar joints. J. Biomech. 2018, 76, 204–211. [Google Scholar] [CrossRef]
- Grood, E.S.; Suntay, W.J. A joint coordinate system for the clinical description of three-dimensional motions: Application to the knee. J. Biomech. Eng. 1983, 105, 136–144. [Google Scholar] [CrossRef]
- Ferrari, A.; Benedetti, M.G.; Pavan, E.; Frigo, C.; Bettinelli, D.; Rabuffetti, M.; Crenna, P.; Leardini, A. Quantitative comparison of five current protocols in gait analysis. Gait Posture 2008, 28, 207–216. [Google Scholar] [CrossRef]
- Parr, W.C.H.; Burnard, J.L.; Wilson, P.J.; Mobbs, R.J. 3D printed anatomical (bio)models in spine surgery: Clinical benefits and value to health care providers. J. Spine Surg. 2019, 5, 549–560. [Google Scholar] [CrossRef]
- Courvoisier, A.; Cebrian, A.; Simon, J.; Désauté, P.; Aubert, B.; Amabile, C.; Thiébaut, L. Virtual Scoliosis Surgery Using a 3D-Printed Model Based on Biplanar Radiographs. Bioengineering 2022, 9, 469. [Google Scholar] [CrossRef]
- Coote, J.D.; Nguyen, T.; Tholen, K.; Stewart, C.; Verter, E.; McGee, J.; Celestre, P.; Sarkar, K. Three-Dimensional Printed Patient Models for Complex Pediatric Spinal Surgery. Ochsner J. 2019, 19, 49–53. [Google Scholar] [CrossRef] [Green Version]
- Leary, O.P.; Crozier, J.; Liu, D.D.; Niu, T.; Pertsch, N.J.; Camara-Quintana, J.Q.; Svokos, K.A.; Syed, S.; Telfeian, A.E.; Oyelese, A.A.; et al. Three-Dimensional Printed Anatomic Modeling for Surgical Planning and Real-Time Operative Guidance in Complex Primary Spinal Column Tumors: Single-Center Experience and Case Series. World Neurosurg. 2021, 145, e116–e126. [Google Scholar] [CrossRef]
- Hoang, D.; Perrault, D.; Stevanovic, M.; Ghiassi, A. Surgical applications of three-dimensional printing: A review of the current literature & how to get started. Ann. Transl. Med. 2016, 4, 456. [Google Scholar] [CrossRef] [Green Version]
- Senkoylu, A.; Daldal, I.; Cetinkaya, M. 3D printing and spine surgery. J. Orthop. Surg. 2020, 28, 230949902092708. [Google Scholar] [CrossRef]
- Punyaratabandhu, T.; Liacouras, P.C.; Pairojboriboon, S. Using 3D models in orthopedic oncology: Presenting personalized advantages in surgical planning and intraoperative outcomes. 3D Print. Med. 2018, 4, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Morgan, C.; Khatri, C.; Hanna, S.A.; Ashrafian, H.; Sarraf, K.M. Use of three-dimensional printing in preoperative planning in orthopaedic trauma surgery: A systematic review and meta-analysis. World J. Orthop. 2019, 11, 57–67. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PRE | Planes | C7 | C6 | C5 | C4 | C3 | C2 | C1 |
| SAGITTAL | 14.3 | 14.2 | 14.3 | −10.1 | −48.5 | −59.2 | −2.7 | |
| FRONTAL | −0.2 | 1.8 | −0.8 | −9.5 | −28.3 | −28.8 | −39.2 | |
| TRANSVERSE | −6.4 | 1.4 | 1.7 | −8.0 | 0.1 | 28.4 | −17.6 | |
| POS | Planes | C7 | C6 | C5 | C4 | C3 | C2 | C1 |
| SAGITTAL | 10.8 | 6.8 | 7.7 | −19.1 | −46.8 | −53.0 | −1.4 | |
| FRONTAL | −0.5 | 1.9 | −0.6 | −7.3 | −15.9 | −18.4 | −31.4 | |
| TRANSVERSE | −7.3 | 0.8 | 1.5 | −0.3 | 0.5 | 23.3 | −7.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Belvedere, C.; Ortolani, M.; Leardini, A.; Cappuccio, M.; Amendola, L.; De Iure, F. 3D Printing in Surgical Planning and Intra-Operative Assistance: A Case Report on Cervical Deformity Correction Surgery. Appl. Sci. 2022, 12, 11564. https://doi.org/10.3390/app122211564
Belvedere C, Ortolani M, Leardini A, Cappuccio M, Amendola L, De Iure F. 3D Printing in Surgical Planning and Intra-Operative Assistance: A Case Report on Cervical Deformity Correction Surgery. Applied Sciences. 2022; 12(22):11564. https://doi.org/10.3390/app122211564
Chicago/Turabian StyleBelvedere, Claudio, Maurizio Ortolani, Alberto Leardini, Michele Cappuccio, Luca Amendola, and Federico De Iure. 2022. "3D Printing in Surgical Planning and Intra-Operative Assistance: A Case Report on Cervical Deformity Correction Surgery" Applied Sciences 12, no. 22: 11564. https://doi.org/10.3390/app122211564