
Unusual Clinical Experience in BRAF Exon 15 p.K601E-Mutated Lung Cancer: A Case Report and Brief Review of the Literature

 ,
,  , ,
, ,  ,
,  and
and 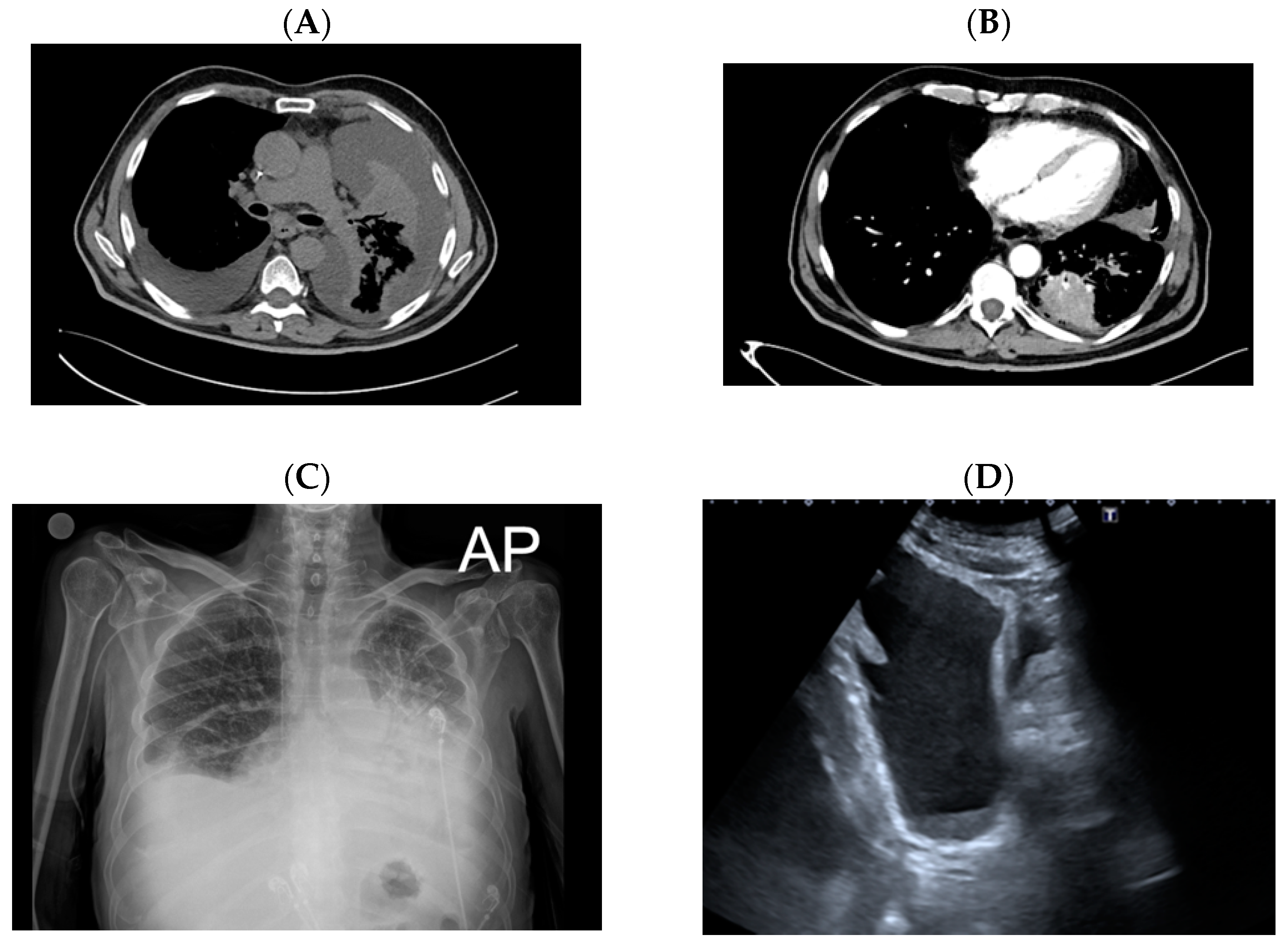{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
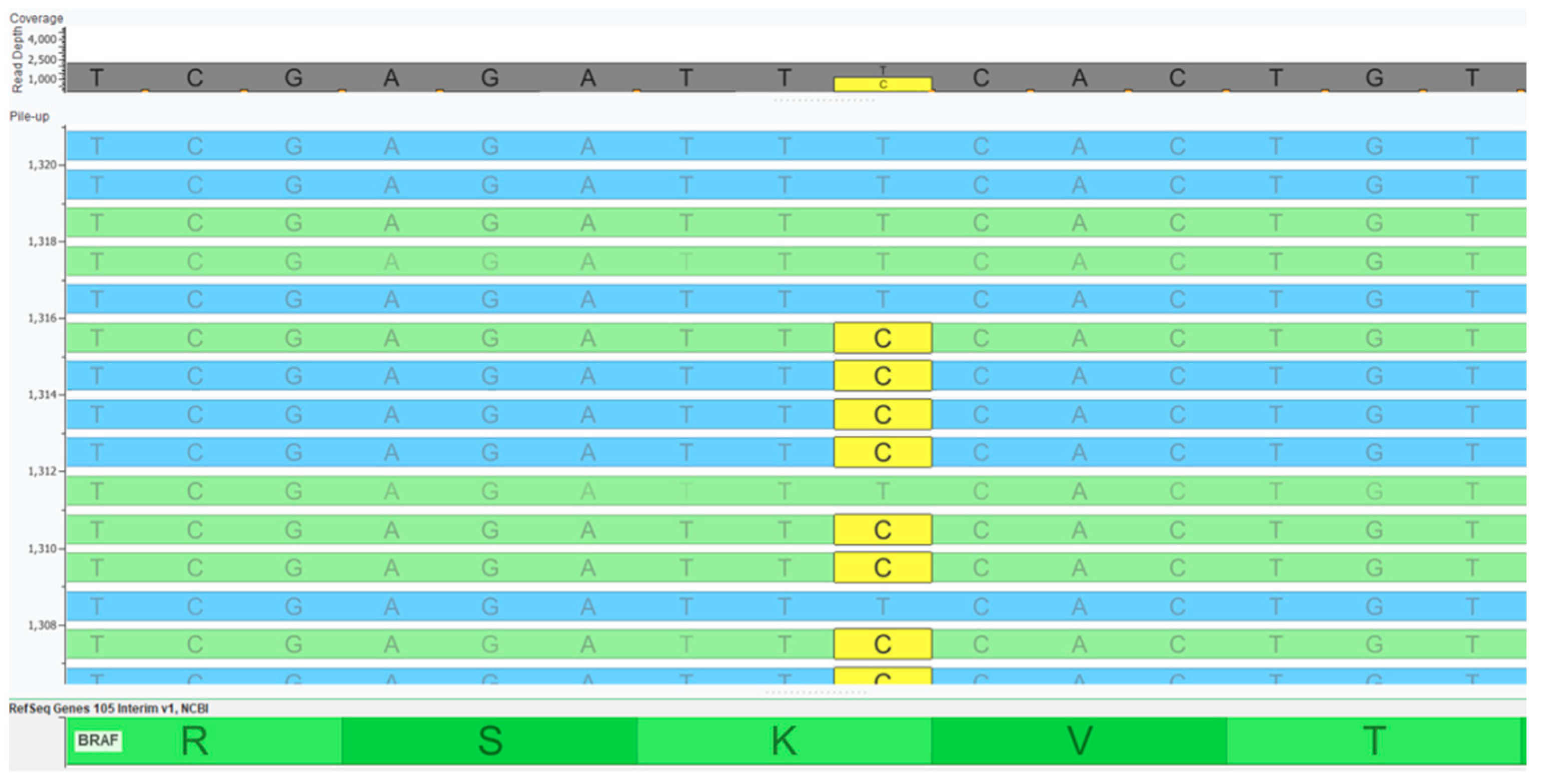
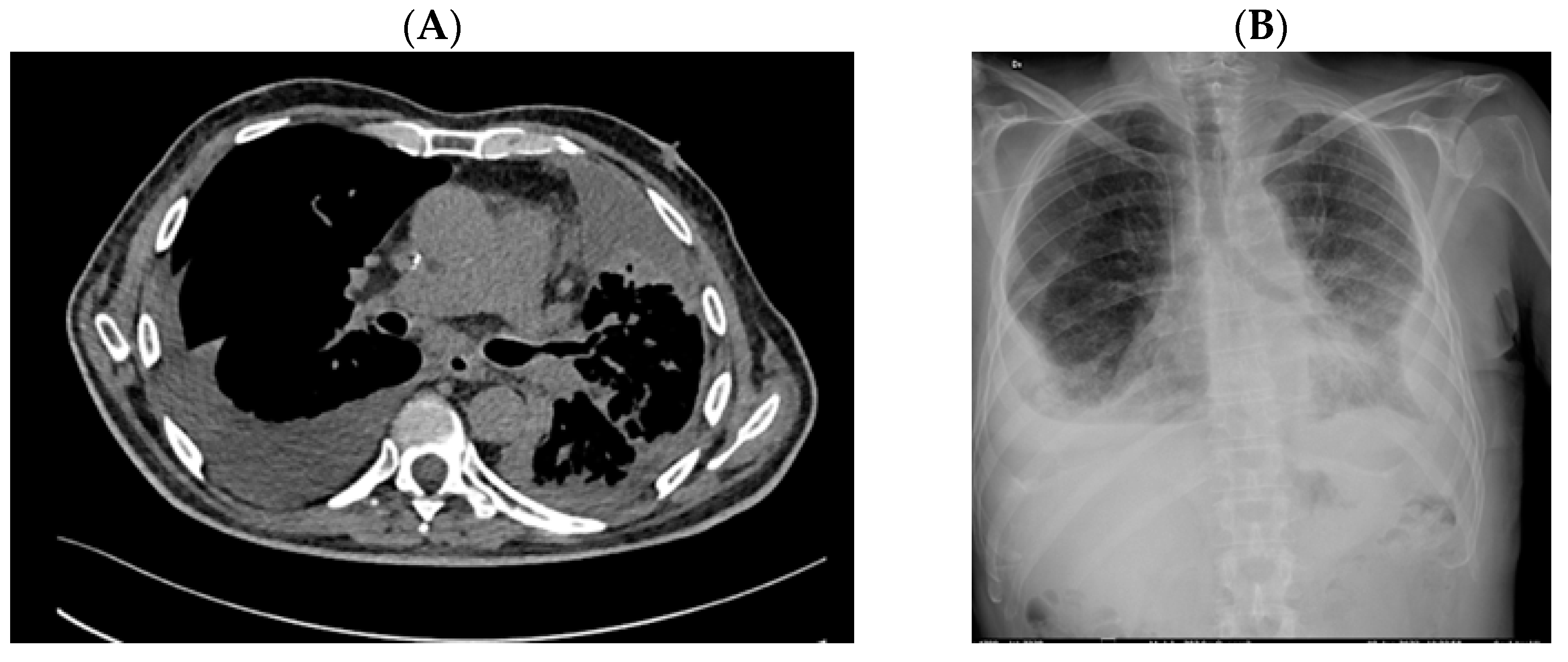
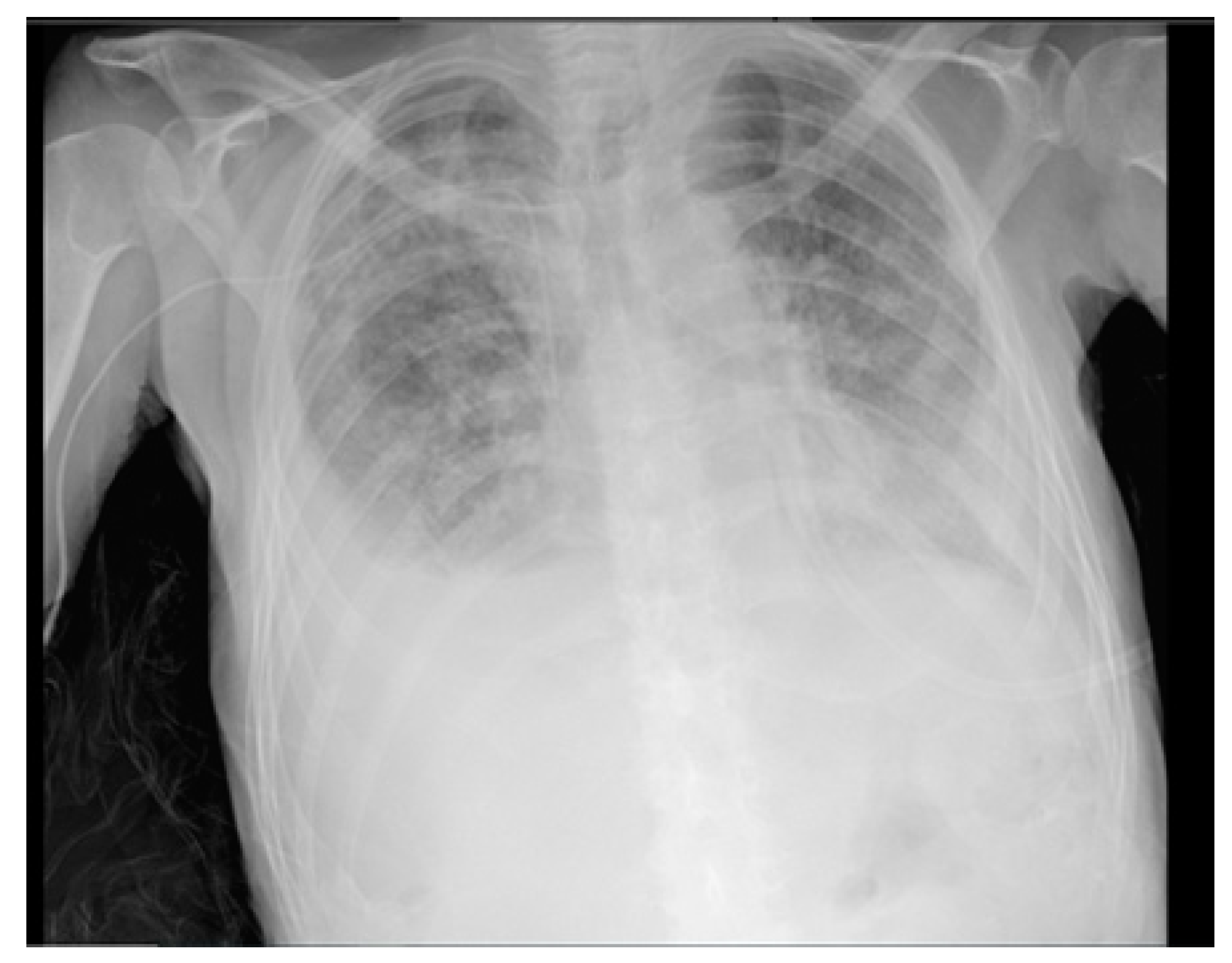
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Huang, R.S.P.; Severson, E.; Haberberger, J.; Duncan, D.L.; Hemmerich, A.; Edgerly, C.; Ferguson, N.L.; Frampton, G.; Owens, C.; Williams, E.; et al. Landscape of Biomarkers in Non-small Cell Lung Cancer Using Comprehensive Genomic Profiling and PD-L1 Immunohistochemistry. Pathol. Oncol. Res. 2021, 27, 592997. [Google Scholar] [CrossRef]
- Leonetti, A.; Facchinetti, F.; Rossi, G.; Minari, R.; Conti, A.; Friboulet, L.; Tiseo, M.; Planchard, D. BRAF in Non-Small Cell Lung Cancer (NSCLC): Pickaxing Another Brick in the Wall. Cancer Treat. Rev. 2018, 66, 82–94. [Google Scholar] [CrossRef]
- Nguyen-Ngoc, T.; Bouchaab, H.; Adjei, A.A.; Peters, S. BRAF Alterations as Therapeutic Targets in Non-Small-Cell Lung Cancer. J. Thorac. Oncol. 2015, 10, 1396–1403. [Google Scholar] [CrossRef] [Green Version]
- Ross, J.S.; Wang, K.; Chmielecki, J.; Gay, L.; Johnson, A.; Chudnovsky, J.; Yelensky, R.; Lipson, D.; Ali, S.M.; Elvin, J.A.; et al. The Distribution of BRAF Gene Fusions in Solid Tumors and Response to Targeted Therapy. Int. J. Cancer. 2016, 138, 881–890. [Google Scholar] [CrossRef] [Green Version]
- Davies, H.; Bignell, G.R.; Cox, C.; Stephens, P.; Edkins, S.; Clegg, S.; Teague, J.; Woffendin, H.; Garnett, M.J.; Bottomley, W.; et al. Mutations of the BRAF Gene in Human Cancer. Nature 2002, 417, 949–954. [Google Scholar] [CrossRef]
- Dankner, M.; Rose, A.A.N.; Rajkumar, S.; Siegel, P.M.; Watson, I.R. Classifying BRAF Alterations in Cancer: New Rational Therapeutic Strategies for Actionable Mutations. Oncogene 2018, 37, 3183–3199. [Google Scholar] [CrossRef]
- Yao, Z.; Torres, N.M.; Tao, A.; Gao, Y.; Luo, L.; Li, Q.; de Stanchina, E.; Abdel-Wahab, O.; Solit, D.B.; Poulikakos, P.I.; et al. BRAF Mutants Evade ERK-Dependent Feedback by Different Mechanisms That Determine Their Sensitivity to Pharmacologic Inhibition. Cancer Cell 2015, 28, 370–383. [Google Scholar] [CrossRef] [Green Version]
- Foster, S.A.; Whalen, D.M.; Özen, A.; Wongchenko, M.J.; Yin, J.; Yen, I.; Schaefer, G.; Mayfield, J.D.; Chmielecki, J.; Stephens, P.J.; et al. Activation Mechanism of Oncogenic Deletion Mutations in BRAF, EGFR, and HER2. Cancer Cell 2016, 29, 477–493. [Google Scholar] [CrossRef] [Green Version]
- Zehir, A.; Benayed, R.; Shah, R.H.; Syed, A.; Middha, S.; Kim, H.R.; Srinivasan, P.; Gao, J.; Chakravarty, D.; Devlin, S.M.; et al. Mutational Landscape of Metastatic Cancer revealed from Prospective Clinical Sequencing of 10,000 Patients. Nat. Med. 2017, 23, 703–713. [Google Scholar] [CrossRef]
- Saalfeld, F.C.; Wenzel, C.; Aust, D.E.; Wermke, M. Targeted therapy in BRAF p.K601E–driven NSCLC: Case report and literature review. JCO Precis. Oncol. 2020, 4, 1163–1166. [Google Scholar]
- Mu, Y.; Yang, K.; Hao, X.; Wang, Y.; Wang, L.; Liu, Y.; Lin, L.; Li, J.; Xing, P. Clinical Characteristics and Treatment Outcomes of 65 Patients With BRAF-Mutated Non-small Cell Lung Cancer. Front. Oncol. 2020, 10, 603. [Google Scholar] [CrossRef]
- Marchetti, A.; Felicioni, L.; Malatesta, S.; Sciarrotta, M.G.; Guetti, L.; Chella, A.; Viola, P.; Pullara, C.; Mucilli, F.; Buttitta, F. Clinical features and outcome of patients with non-small-cell lung cancer harboring BRAF mutations. J. Clin. Oncol. 2011, 29, 3574–3579. [Google Scholar] [CrossRef]
- Litvak, A.M.; Paik, P.K.; Woo, K.M.; Sima, C.S.; Hellmann, M.D.; Arcila, M.E.; Ladanyi, M.; Rudin, C.M.; Kris, M.G.; Riely, G.J. Clinical characteristics and course of 63 patients with BRAF mutant lung cancers. J. Thorac. Oncol. 2014, 9, 1669–1674. [Google Scholar] [CrossRef] [Green Version]
- Mazieres, J.; Drilon, A.; Lusque, A.B.; Mhanna, L.; Cortot, A.; Mezquita, L.; Thai, A.A.; Mascaux, C.; Couraud, S.; Veillon, R.; et al. Immune checkpoint inhibitors for patients with advanced lung cancer and oncogenic driver alterations: Results from the immunotarget registry. Ann. Oncol. 2019, 30, 1321–1328. [Google Scholar] [CrossRef]
- Iaccarino, A.; Pisapia, P.; De Felice, M.; Pepe, F.; Gragnano, G.; De Luca, C.; Ianniello, G.; Malapelle, U. Concomitant Rare KRAS and BRAF Mutations in Lung Adenocarcinoma: A Case Report. J. Mol. Pathol. 2020, 1, 36–42. [Google Scholar] [CrossRef]
- Salimian, K.J.; Fazeli, R.; Zheng, G.; Ettinger, D.; Maleki, Z. V600E BRAF versus Non-V600E BRAF Mutated Lung Adenocarcinomas: Cytomorphology, Histology, Coexistence of Other Driver Mutations and Patient Characteristics. Acta Cytol. 2018, 62, 79–84. [Google Scholar]
- Kim, D.W.; Haydu, L.E.; Joon, A.Y.; Bassett, R.L., Jr.; Siroy, A.E.; Tetzlaff, M.T.; Routbort, M.J.; Amaria, R.N.; Wargo, J.A.; McQuade, J.L.; et al. Clinicopathological features and clinical outcomes associated with TP53 and BRAFNon-V600 mutations in cutaneous melanoma patients. Cancer 2017, 123, 1372–1381. [Google Scholar]
- Moiseyenko, F.V.; Egorenkov, V.V.; Kramchaninov, M.M.; Artemieva, E.V.; Aleksakhina, S.N.; Holmatov, M.M.; Moiseyenko, V.M.; Imyanitov, E.N. Lack of response to vemurafenib in melanoma carrying BRAF K601E mutation. Case Rep. Oncol. 2019, 12, 339–343. [Google Scholar]
- Su, P.L.; Lin, C.Y.; Chen, Y.L.; Chen, W.L.; Lin, C.-C.; Su, W.-C. Durable response to combined dabrafenib and trametinib in a patient with BRAF K601E mutation-positive lung adenocarcinoma: A case report. JTO Clin. Res. Rep. 2021, 2, 100202. [Google Scholar]
- Rogiers, A.; Thomas, D.; Vander Borght, S.; van den Oord, J.J.; Bechter, O.; Dewaele, M.; Rambow, F.; Marine, J.C.; Wolter, P. Dabrafenib plus trametinib in BRAF K601E-mutant melanoma. Br. J. Dermatol. 2019, 180, 421–422. [Google Scholar]
- Gautschi, O.; Bluthgen, M.V.; Smit, E.F.; Wolf, J.; Früh, M.; Peters, S.; Schuler, M.; Zalcman, G.; Milia, J.; Mazieres, J. Targeted therapy for patients with BRAF-mutant lung cancer: Results from the European EURAF cohort. J. Thorac. Oncol. 2015, 10, 1451–1457. [Google Scholar] [CrossRef]
- Yang, C.-Y.; Lin, M.-W.; Chang, Y.-L.; Wu, C.-T.; Yang, P.-C. Programmed Cell DeathLigand 1 Expression in Surgically Resected Stage I Pulmonary Adenocarcinoma and its Correlation with Driver Mutations and Clinical Outcomes. Eur. J. Cancer 2014, 50, 1361–1369. [Google Scholar] [CrossRef]
- Tseng, J.S.; Yang, T.Y.; Wu, C.Y.; Ku, W.H.; Chen, K.C.; Hsu, K.H.; Huang, Y.-H.; Su, K.-Y.; Yu, S.-L.; Cheng, G.-C. Characteristics and Predictive Value of PD-L1 Status in Real-World Non-Small Cell Lung Cancer Patients. J. Immunother. 2018, 41, 292–299. [Google Scholar] [CrossRef]
- Guisier, F.; Dubos-Arvis, C.; Viñas, F.; Doubre, H.; Ricordel, C.; Ropert, S.; Janicot, H.; Bernardi, M.; Fournel, P.; Lamy, R.; et al. Efficacy and Safety of Anti-PD-1 Immunotherapy in Patients with Advanced NSCLC With BRAF, HER2, or MET Mutations or RET Translocation: GFPC 01-2018. J. Thorac. Oncol. 2020, 15, 628–636. [Google Scholar] [CrossRef]
- Niu, X.; Sun, Y.; Planchard, D.; Chiu, L.; Bai, J.; Ai, X.; Lu, S. Durable Response to the Combination of Atezolizumab with Platinum-Based Chemotherapy in an Untreated Non-Smoking Lung Adenocarcinoma Patient With BRAF V600E Mutation: A Case Report. Front. Oncol. 2021, 11, 634920. [Google Scholar] [CrossRef]
- Hanane, K.; Salma, B.; Khadija, B.; Ibrahim, E.; Saber, B.; Hind, M.; Hassan, E. Peritoneal carcinomatosis, an unusual and only site of metastasis from lung adenocarcinoma. Pan Afr. Med. J. 2016, 23, 60. [Google Scholar] [CrossRef]
- Tani, T.; Nakachi, I.; Ikemura, S.; Nukaga, S.; Ohgino, K.; Kuroda, A.; Terai, H.; Masuzawa, K.; Shinozaki, T.; Ishioka, K.; et al. Clinical Characteristics and Therapeutic Outcomes of Metastatic Peritoneal Carcinomatosis in Non-Small-Cell Lung Cancer. Cancer Manag. Res. 2021, 13, 7497–7503. [Google Scholar] [CrossRef]
- Abbate, M.I.; Cortinovis, D.L.; Tiseo, M.; Vavalà, T.; Cerea, G.; Toschi, L.; Canova, S.; Colonese, F.; Bidoli, P. Peritoneal carcinomatosis in non-small-cell lung cancer: Retrospective multicentric analysis and literature review. Future Oncol. 2019, 15, 989–994. [Google Scholar] [CrossRef]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Felice, M.; Pisapia, P.; Pepe, F.; De Luca, C.; Iaccarino, A.; Malapelle, U.; Troncone, G.; Ianniello, G.P. Unusual Clinical Experience in BRAF Exon 15 p.K601E-Mutated Lung Cancer: A Case Report and Brief Review of the Literature. Appl. Sci. 2022, 12, 7552. https://doi.org/10.3390/app12157552
De Felice M, Pisapia P, Pepe F, De Luca C, Iaccarino A, Malapelle U, Troncone G, Ianniello GP. Unusual Clinical Experience in BRAF Exon 15 p.K601E-Mutated Lung Cancer: A Case Report and Brief Review of the Literature. Applied Sciences. 2022; 12(15):7552. https://doi.org/10.3390/app12157552
Chicago/Turabian StyleDe Felice, Marco, Pasquale Pisapia, Francesco Pepe, Caterina De Luca, Antonino Iaccarino, Umberto Malapelle, Giancarlo Troncone, and Giovanni Pietro Ianniello. 2022. "Unusual Clinical Experience in BRAF Exon 15 p.K601E-Mutated Lung Cancer: A Case Report and Brief Review of the Literature" Applied Sciences 12, no. 15: 7552. https://doi.org/10.3390/app12157552