
Orthodontic Loads in Teeth after Regenerative Endodontics: A Finite Element Analysis of the Biomechanical Performance of the Periodontal Ligament


Abstract
:1. Introduction
2. Materials and Methods
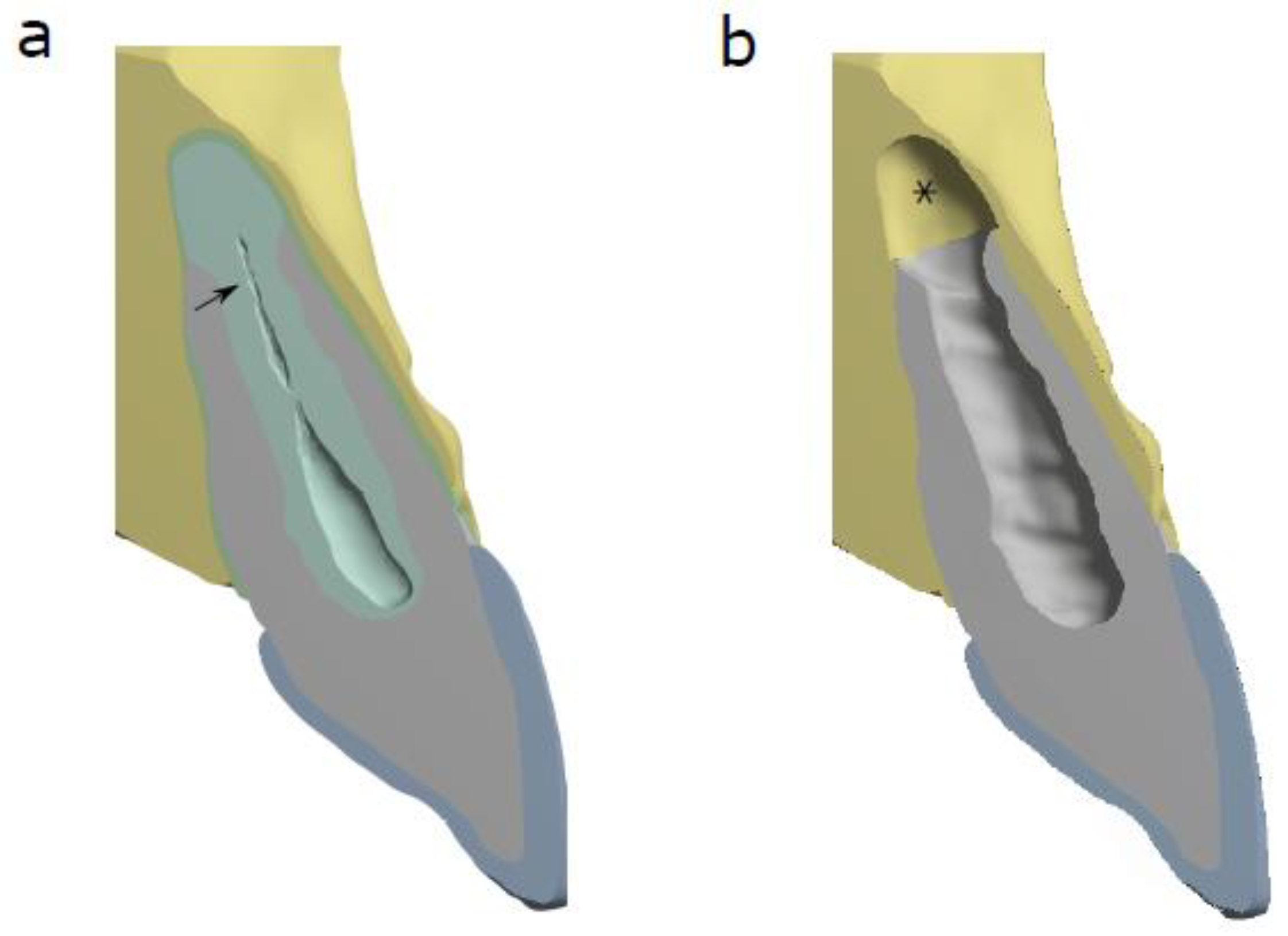
2.1. 3D FEA Models and Tissue Properties
2.2. Loading Scenario
2.3. Analysis of Stress
3. Results
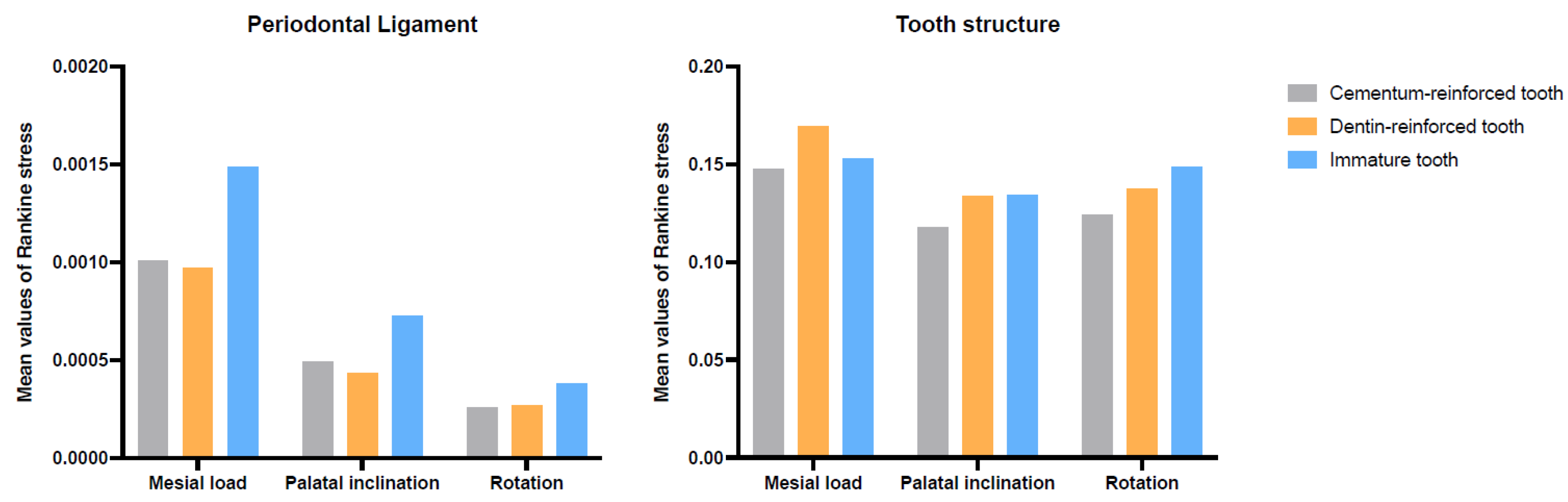
3.1. Mean Stress Values of the Periodontal Ligament and Tooth for Each Scenario
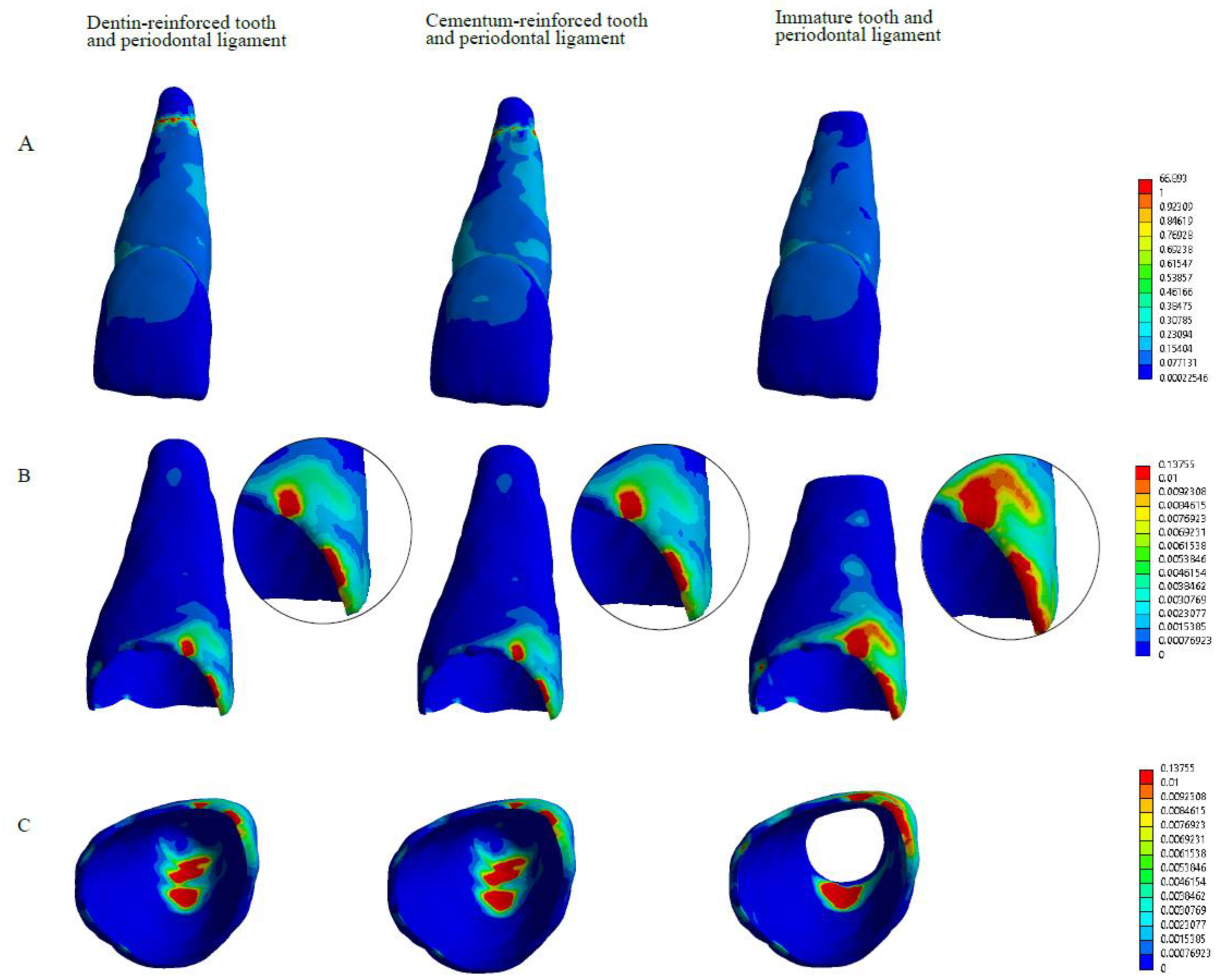
3.2. Distribution of the Stress of the Tooth Structure for Mesial Load
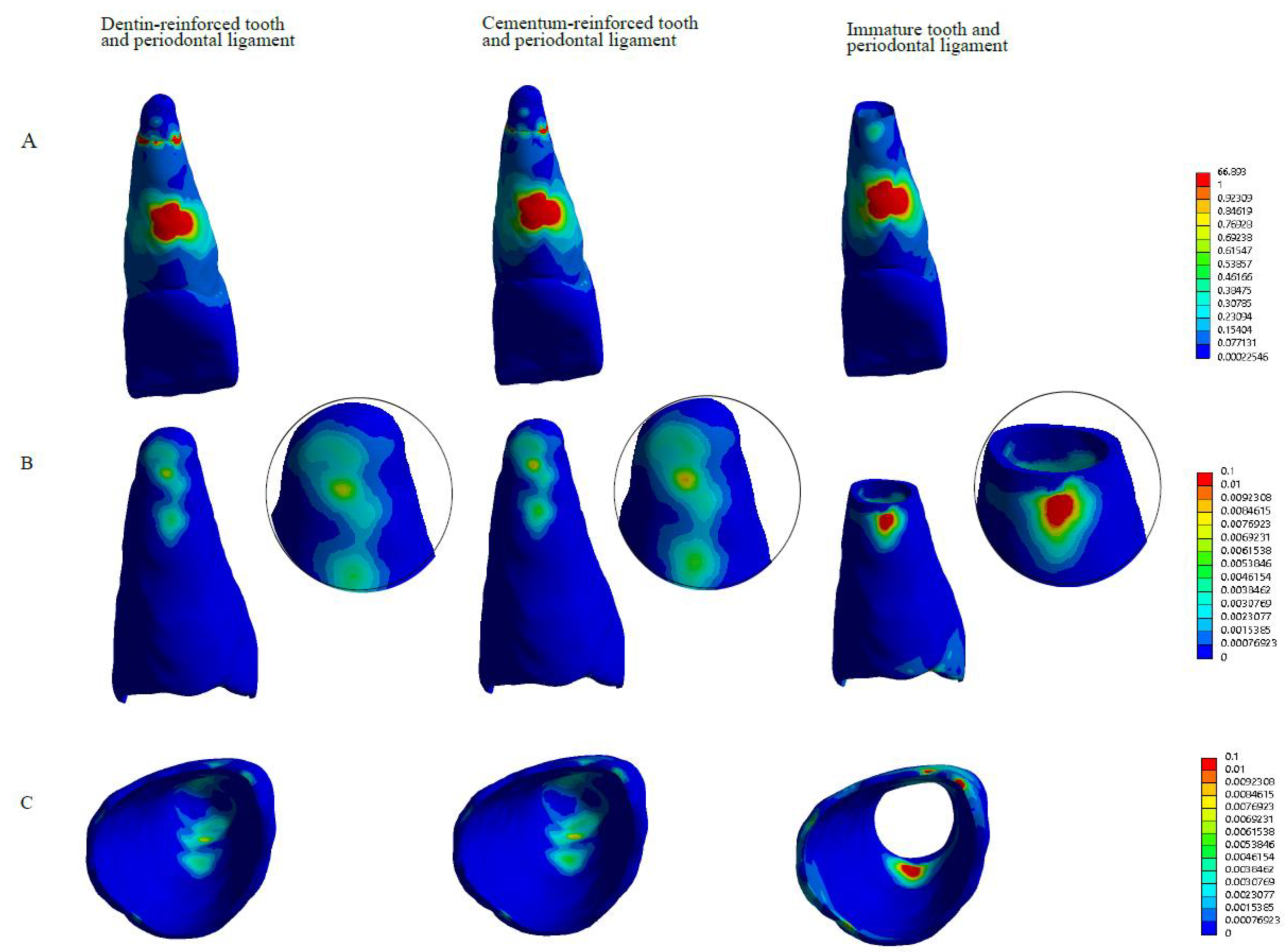
3.3. Distribution of the Stress of the Tooth Structure for Palatal Inclination
3.4. Distribution of the Stress of the Tooth Structure for Rotation Scenario
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Murray, P.E.; Garcia-Godoy, F.; Hargreaves, K.M. Regenerative Endodontics: A Review of Current Status and a Call for Action. J. Endod. 2007, 33, 377–390. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.; Zeng, Q.; Wei, X.; Zhao, W.; Cui, M.; Gu, J.; Lu, J.; Yang, M.; Ling, J. Regenerative Endodontics Versus Apexification in Immature Permanent Teeth with Apical Periodontitis: A Prospective Randomized Controlled Study. J. Endod. 2017, 43, 1821–1827. [Google Scholar] [CrossRef]
- Lovelace, T.W.; Henry, M.A.; Hargreaves, K.M.; Diogenes, A. Evaluation of the delivery of mesenchymal stem cells into the root canal space of necrotic immature teeth after clinical regenerative endodontic procedure. J. Endod. 2011, 37, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Galler, K.M.; D'Souza, R.N.; Federlin, M.; Cavender, A.C.; Hartgerink, J.D.; Hecker, S.; Schmalz, G. Dentin conditioning codetermines cell fate in regenerative endodontics. J. Endod. 2011, 237, 1536–1541. [Google Scholar] [CrossRef]
- Lolato, A.; Bucchi, C.; Taschieri, S.; Kabbaney, A.E.; Fabbro, M.D. Platelet concentrates for revitalization of immature necrotic teeth: A systematic review of the clinical studies. Platelets 2016, 27, 383–392. [Google Scholar] [CrossRef] [PubMed]
- Austah, O.; Joon, R.; Fath, W.M.; Chrepa, V.; Diogenes, A.; Ezeldeen, M.; Couve, E.; Ruparel, N.B. Comprehensive Characterization of 2 Immature Teeth Treated with Regenerative Endodontic Procedures. J. Endod. 2018, 44, 1802–1811. [Google Scholar] [CrossRef]
- Lei, L.; Chen, Y.; Zhou, R.; Huang, X.; Cai, Z. Histologic and Immunohistochemical Findings of a Human Immature Permanent Tooth with Apical Periodontitis after Regenerative Endodontic Treatment. J. Endod. 2015, 41, 1172–1179. [Google Scholar] [CrossRef]
- Nosrat, A.; Kolahdouzan, A.; Hosseini, F.; Mehrizi, E.A.; Verma, P.; Torabinejad, M. Histologic outcomes of uninfected human immature teeth treated with regenerative endodontics: 2 case reports. J. Endod. 2015, 41, 1725–1729. [Google Scholar] [CrossRef]
- Del Fabbro Lolato, A.; Bucchi, C.; Taschieri, S.; Weinstein, R.L. Autologous Platelet Concentrates for Pulp and Dentin Regeneration: A Literature Review of Animal Studies. J. Endod. 2016, 42, 250–257. [Google Scholar] [CrossRef]
- Goldberg, M.; Kulkarni, A.B.; Young, M.; Boskey, A. Dentin: Structure, Composition and Mineralization. Front. Biosci. 2011, 3, 711–735. [Google Scholar] [CrossRef]
- Yamauchi, N.; Nagaoka, H.; Yamauchi, S.; Teixeira, F.B.; Miguez, P.; Yamauchi, M. Immunohistological characterization of newly formed tissues after regenerative procedure in immature dog teeth. J. Endod. 2011, 37, 1636–1641. [Google Scholar] [CrossRef] [PubMed]
- Salmon, C.R.; Tomazela, D.M.; Ruiz, K.G.; Foster, B.L.; Paes Leme, A.F.; Sallum, E.A. Proteomic analysis of human dental cementum and alveolar bone. J. Proteom. 2013, 91, 544–555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ho, S.P.; Yu, B.; Yun, W.; Marshall, G.W.; Ryder, M.I.; Marshall, S.J. Structure, chemical composition and mechanical properties of human and rat cementum and its interface with root dentin. Acta Biomater. 2010, 5, 707–718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bucchi, C.; Marcé-Nogué, J.; Galler, K.M.; Widbiller, M. Biomechanical performance of an immature maxillary central incisor after revitalization: A finite element analysis. Int. Endod. J. 2019, 52, 1508–1518. [Google Scholar] [CrossRef]
- Jonsdottir, S.H.; Giesen, E.B.W.; Maltha, J.C. Biomechanical behaviour of the periodontal ligament of the beagle dog during the first 5 hours of orthodontic force application. Eur. J. Orthod. 2006, 28, 547–552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, L.; Liu, W.; Zhao, J.; Zhang, L.; Liu, W.; Zhao, J.; Jin, F.; Jin, Y. Mechanical stress regulates osteogenic differentiation and RANKL/OPG ratio in periodontal ligament stem cells by the Wnt/beta-catenin pathway. Biochim. Biophys. Acta 2016, 1860, 2211–2219. [Google Scholar] [CrossRef]
- Wise, G.E.; King, G.J. Mechanisms of tooth eruption and orthodontic tooth movement. J. Dent. Res. 2008, 87, 414–434. [Google Scholar] [CrossRef] [Green Version]
- Weltman, B.; Vig, K.W.; Fields, H.W.; Shanker, S.; Kaizar, E.E. Root resorption associated with orthodontic tooth movement: A systematic review. Am. J. Orthod. Dentofac. Orthop. 2010, 137, 462–476. [Google Scholar] [CrossRef] [Green Version]
- Galler, K.M.; Krastl, G.; Simon, S.; Van Gorp, G.; Meschi, N.; Vahedi, B.; Lambrechts, P. European Society of Endodontology position statement: Revitalization procedures. Int. Endod. J. 2016, 49, 717–723. [Google Scholar] [CrossRef]
- Natera, M.; Mukherjee, P.M. Regenerative Endodontic Treatment with Orthodontic Treatment in a Tooth with Dens Evaginatus: A Case Report with a 4-year Follow-up. J. Endod. 2018, 44, 952–955. [Google Scholar] [CrossRef]
- Chaniotis, A. Orthodontic Movement after Regenerative Endodontic Procedure: Case Report and Long-term Observations. J. Endod. 2018, 44, 432–437. [Google Scholar] [CrossRef]
- Cvek, M. Prognosis of luxated non-vital maxillary incisors treated with calcium hydroxide and filled with gutta-percha. A retrospective clinical study. Dent. Traumatol. 1992, 8, 45–55. [Google Scholar] [CrossRef]
- Qian, L.; Todo, M.; Morita, Y.; Matsushita, Y.; Koyano, K. Deformation analysis of the periodontium considering the viscoelasticity of the periodontal ligament. Dent Mater 2009, 25, 1285–1292. [Google Scholar] [CrossRef]
- Doblaré, M.; García, J.M.; Gómez, M.J. Modelling bone tissue fracture and healing: A review. Eng. Fract. Mech. 2004, 71, 1809–1840. [Google Scholar] [CrossRef]
- Pérez-González, A.; Iserte-Vilar, J.L.; González-Lluch, C. Interpreting finite element results for brittle materials in endodontic restorations. Biomed. Eng. Online 2011, 10, 44. [Google Scholar] [CrossRef] [Green Version]
- Walmsley, C.W.; Smits, P.D.; Quayle, M.R.; McCurry, M.R.; Richards, H.S.; Oldfield, C.C.; Wroe, S.; Clausen, P.D.; McHenry, C.R. Why the Long Face? The Mechanics of Mandibular Symphysis Proportions in Crocodiles. PLoS ONE 2013, 8, e53873. [Google Scholar] [CrossRef] [Green Version]
- Alexander, A.; Torabinejad, M.; Vahdati, S.A.; Nosrat, A.; Verma, P.; Grandhi, A.; Shabahang, S. Regenerative Endodontic Treatment in Immature Noninfected Ferret Teeth Using Blood Clot or SynOss Putty as Scaffolds. J. Endod. 2020, 6, 209–215. [Google Scholar] [CrossRef]
- Ciavarella, D.; Tepedino, M.; Gallo, C.; Montaruli, G.; Zhurakivska, K.; Coppola, L.; Troiano, G.; Chimenti, C.; Laurenziello, M.; Lo Russo, L. Post-orthodontic position of lower incisors and gingival recession: A retrospective study. J. Clin. Exp. Dent. 2017, 9, e1425–e1430. [Google Scholar] [CrossRef]
- Rangiani, A.; Jing, Y.; Ren, Y.; Yadav, S.; Taylor, R.; Feng, J.Q. Critical roles of periostin in the process of orthodontic tooth movement. Eur. J. Orthod. 2016, 38, 373–378. [Google Scholar] [CrossRef] [Green Version]
- Brudvik, P.; Rygh, P. Multi-nucleated cells remove the main hyalinized tissue and start resorption of adjacent root surfaces. Eur. J. Orthod. 1994, 16, 265–273. [Google Scholar] [CrossRef]
- Li, Z.; Yu, M.; Jin, S.; Wang, Y.; Luo, R.; Huo, B.; Liu, D.; He, D.; Zhou, Y.; Liu, Y. Stress distribution and collagen remodeling of periodontal ligament during orthodontic tooth movement. Front. Pharmacol. 2019, 10, 1263. [Google Scholar] [CrossRef] [PubMed]
- Shaw, A.M.; Sameshima, G.T.; Vu, H.V. Mechanical stress generated by orthodontic forces on apical root cementum: A finite element model. Orthod. Craniofac. Res. 2004, 7, 98–107. [Google Scholar] [CrossRef] [PubMed]
- Anthrayose, P.; Nawal, R.R.; Yadav, S.; Talwar, S.; Yadav, S. Effect of revascularization and apexification procedures on biomechanical behaviour of immature maxillary central incisor teeth: A three-dimensional finite element analysis study. Clin. Oral Investig. 2021, 25, 6671–6679. [Google Scholar] [CrossRef] [PubMed]
- Zhou, R.; Wang, Y.; Chen, Y.; Chen, S.; Lyu, H.; Cai, Z.; Huang, X. Radiographic, Histologic, and Biomechanical Evaluation of Combined Application of Platelet-rich Fibrin with Blood Clot in Regenerative Endodontics. J. Endod. 2017, 43, 2034–2040. [Google Scholar] [CrossRef] [PubMed]
- Papadopoulou, K.; Hasan, I.; Keilig, L.; Reimann, S.; Eliades, T.; Jäger, A.; Deschner, J.; Bourauel, C. Biomechanical time dependency of the periodontal ligament: A combined experimental and numerical approach. Eur. J. Orthod. 2013, 35, 811–818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toms, S.R.; Eberhardt, A.W. A nonlinear finite element analysis of the periodontal ligament under orthodontic tooth loading. Am. J. Orthod. Dentofac. Orthop. 2003, 123, 657–665. [Google Scholar] [CrossRef]
- Keilig, L.; Drolshagen, M.; Tran, K.L.; Hasan, I.; Reimann, S.; Deschner, J.; Brinkmann, K.; Krause, R.; Favino, M.; Bourauel, C. In vivo measurements and numerical analysis of the biomechanical characteristics of the human periodontal ligament. Ann. Anat. 2016, 206, 80–88. [Google Scholar] [CrossRef]
- Pini, M.; Zysset, P.; Botsis, J.; Contro, R. Tensile and compressive behaviour of the bovine periodontal ligament. J. Biomech. 2004, 37, 111–119. [Google Scholar] [CrossRef]
- Shibata, T.; Botsis, J.; Bergomi, M.; Mellal, A.; Komatsu, K. Mechanical behavior of bovine periodontal ligament under tension-compression cyclic displacements. Eur. J. Oral Sci. 2006, 114, 74–82. [Google Scholar] [CrossRef] [PubMed]
- Martin, G.; Ricucci, D.; Gibbs, J.L.; Lin, L.M. Histological findings of revascularized/revitalized immature permanent molar with apical periodontitis using platelet-rich plasma. J. Endod. 2013, 39, 138–144. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tissue | Young’s Modulus | Poisson Coefficient |
|---|---|---|
| Enamel | 84,100 | 0.31 |
| Dentine | 18,600 | 0.31 |
| Cementum | 8200 | 0.3 |
| Bone | 14,700 | 0.31 |
| C10 | C01 | C20 | C11 | C02 | C30 | C21 | C12 | C03 |
|---|---|---|---|---|---|---|---|---|
| −0.0048 | 0.00505 | 0.008 | 0.0012 | 0 | 0.004 | 0 | 0 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bucchi, C.; Del Fabbro, M.; Marcé-Nogué, J. Orthodontic Loads in Teeth after Regenerative Endodontics: A Finite Element Analysis of the Biomechanical Performance of the Periodontal Ligament. Appl. Sci. 2022, 12, 7063. https://doi.org/10.3390/app12147063
Bucchi C, Del Fabbro M, Marcé-Nogué J. Orthodontic Loads in Teeth after Regenerative Endodontics: A Finite Element Analysis of the Biomechanical Performance of the Periodontal Ligament. Applied Sciences. 2022; 12(14):7063. https://doi.org/10.3390/app12147063
Chicago/Turabian StyleBucchi, Cristina, Massimo Del Fabbro, and Jordi Marcé-Nogué. 2022. "Orthodontic Loads in Teeth after Regenerative Endodontics: A Finite Element Analysis of the Biomechanical Performance of the Periodontal Ligament" Applied Sciences 12, no. 14: 7063. https://doi.org/10.3390/app12147063