
Effect of Over-The-Counter Tooth-Whitening Products on Enamel Surface Roughness and Microhardness
by
 , and
, and
Abdullah AlShehri
1,*, 
Mohammad H. AlRefeai
2,
Faisal AlZamil
3,
Nawaf AlOtaibi
3 and
Yara AlKinani
4 1
Conservative Dental Department, College of Dentistry, Prince Sattam bin Abdulaziz University, Al-Kharj 11942, Saudi Arabia
2
Department of Restorative Dentistry, Division of Operative Dentistry, College of Dentistry, King Saud University, Riyadh 11451, Saudi Arabia
3
College of Dentistry, Prince Sattam bin Abdulaziz University, Al-Kharj 11942, Saudi Arabia
4
College of Dentistry, Riyadh Elm University, Riyadh 13244, Saudi Arabia
*
Author to whom correspondence should be addressed.
Appl. Sci. 2022, 12(14), 6930; https://doi.org/10.3390/app12146930
Submission received: 2 June 2022
/
Revised: 6 July 2022
/
Accepted: 7 July 2022
/
Published: 8 July 2022
Abstract
:Background: To evaluate the efficacy of new over-the-counter tooth-whitening products on enamel surface roughness and microhardness. Methods: A total of 120 enamel specimens were prepared and randomly allocated into six groups. Group A was treated with 10% carbamide peroxide; Group B was immersed in distilled water; Group C was treated with hydrated silica, sodium hexametaphosphate toothpaste; Group D was treated with sodium bicarbonate; Group E was treated with 0.25% citric acid; and Group F was treated with hydrated silica, charcoal powder. Results: A, B, and D demonstrated decreased Ra, whereas Groups C, E, and F showed an increased Ra after whitening. The changes in Ra from T0 to T1 in each group was statistically significant (p < 0.001) except for Group B (p = 0.85). The groups showed decreased KHN after whitening, except for specimens in Group B (distilled water). The KHN from T0 to T1 decreased significantly for groups A, C, E, and F (p = 0.001). Significant difference was observed at T1 (p < 0.0001). Conclusion: Within the limitations of this study, it could be demonstrated that surface roughness and enamel microhardness changes were influenced by the type, composition, and exposure time of the whitening product.
1. Introduction
Over the past decade, there is an upward trend among the general public to enhance the dentofacial esthetics. This has been warranted by an increased number of patients seeking esthetic dental procedures such as orthodontic treatment and tooth whitening [1,2]. People have placed high value on tooth color, and previous studies have suggested that many of them are dissatisfied and want them to be improved [2,3]. Furthermore, people judge a person’s social competence, intellectual prowess, psychosocial adjustment, and life satisfaction more favorably when their teeth are white [3]. Therefore, tooth whitening has become one of the most frequently sought-after dental treatment in recent years [4]. Subsequently, it has renewed the dental profession’s interest in esthetic dental treatment due to an individual’s desire for whiter and brighter teeth.
Currently, four tooth-whitening modalities are available: professionally applied (in-office), dentist-supervised (at-home), nonsupervised consumer-purchased/over-the-counter (OTC), and do-it-yourself tooth whitening (DOY). However, tooth whitening depends on several factors such as the method of application, pH of the whitening agents, fluctuation of irradiation, length of photoactivation, tooth size, and the selective absorption of the wavelength of the irradiation complex procedure [5,6]. With the increase in demand for over-the-counter (OTC) products, manufacturers have developed whitening products in the form of rinses, chewing gums, gels, toothpaste, strips, paint-on films, and whitening pens. These products are readily available in the market without prescription, and are also easy to use [7]. The lack of data and ease of access to these products is concerning, as they may harm customers’ dentition. Over-the-counter products are vulnerable to mishandling, overuse, and abuse due to their ‘do-it-yourself’ nature [8]. Citric acid is considered as one of the natural products for tooth whitening and many of the tooth-whitening products contain citric acid in low concentrations to avoid enamel erosion [9,10].
Although the availability of OTC whitening products has increased their popularity, their adverse effects and safety remain a concern due to the possibility of damaging dental tissues [11,12,13]. In addition, it is worth mentioning that the Food and Drug Administration (FDA) does not regulate the use of all tooth-whitening OTC products, and these products do also require the American Dental Association (ADA) seal of acceptance indicating that they are safe and effective when used as directed [14,15]. Tooth-whitening products usually contain carbamide peroxide (CP) or hydrogen peroxide (H2O2) in different concentrations (CP-10–20%, H2O2-30–35%) [12]. The active bleaching agent, on the other hand, is H2O2, and its ionization releases free oxygen ions, which cause oxidation of discolored organic pigments in dental hard tissues, resulting in tooth whitening [3].
There is inconsistency in the literature when reporting the adverse effects of tooth-whitening agents (10–35%) in terms of enamel surface morphology alterations and microhardness changes. Several studies have demonstrated that whitening agents negatively affected the enamel surface morphology and microhardness [16,17,18,19,20,21,22,23,24,25,26,27], whereas a few studies using the same concentration of whitening agents showed no such adverse effects [28,29,30,31]. Previous studies on the effect of in-office or at-home bleaching agents on enamel surface changes are abundant and generally satisfying [16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31]. In contrast, evidence on the effects of over-the-counter whitening products on enamel surface morphology alterations and microhardness is lacking. According to the current knowledge of the authors, there is a lack of information on the effect of newly introduced and readily available OTC tooth-whitening products such as instant Dark Stains teeth-whitening kits and toothpaste and whitening pens on enamel surface morphology alterations and microhardness.
Therefore, the aim of this in vitro study was to investigate and compare the effects of newly introduced OTC tooth-whitening products to a dentist-supervised at-home tooth-whitening protocol in terms of enamel microhardness and surface roughness. The null hypothesis was that there is no significant difference in the surface roughness and microhardness between OTC tooth-whitening products and dentist-supervised at-home whitening products.
2. Materials and Methods
2.1. Specimen Preparation
Ethical approval was obtained from the deanship of scientific research at Prince Sattam Bin Abdulalziz University, Al-Kharj, Saudi Arabia (PSAU2021013). Sixty sound human molars free of enamel defects, caries, and heavy stains were collected and stored until use. The crown of each tooth was sectioned longitudinally in a mesiodistal direction to create a 2 mm-thick sample. The sectioning was accomplished using a diamond saw attached to a low-speed IsoMet 1000 precision cutting machine (Buehler, Lake Bluff, IL, USA). The roots of all the teeth were separated from the crown and the obtained crown samples were cleaned and individually embedded in a 6 mm-thick PVC molds using clear self-cure acrylic orthodontic resin (Techno Sin Standard Kit, Protechno, Girona, Spain). The exposed outer enamel surfaces were polished using silicon carbide abrasive paper (grit sizes 400, 600, 1200, and 2400) accustomed to an automated polisher (Rotopol-V, Struers, Cleveland, OH, USA). All the polished samples were then stored in distilled water until microhardness and roughness measurement.
2.2. Tooth-Whitening Treatment
Group A: This group served as positive control. Teeth were whitened with 10% carbamide peroxide (Opalescence, Ultradent, UT, USA) gel placed in a custom-made suck-down tray. The surface treatment time was 8 h/day for 10 days.
Group B: The samples were immersed in 100 mL of distilled water for 10 days.
Group C: The samples were exposed to simulated tooth brushing in a simulating device (ZM 3, SD Mechatronik GMBH, Feldkirchen-Westerham, Germany). The device contained 12 separate slots to attach toothbrushes and perform brushing of 12 samples at a time. The samples were positioned inside the containers and fixed using putty (3M™ Express™ Standard Putty Kit, North Ryde, New South Wales, Australia). Next, soft and straight-bristled toothbrushes (TARA Toothbrush Company LLC, Dammam, Saudi Arabia) were attached to the brush slots. The simulator container was loaded with slurry of distilled water and iWhite instant Dark Stains dentifrice (Sylphar, Deurle, Belgium) at a ratio of 2:1 by weight. Tooth brushing was accomplished with onward and backward action under a load of 200 g, stroke rate of 160/min, and movement length of 38 mm to cover the whole sample surface. The total brushing time was five minutes and 900 strokes, mimicking 60 days of brushing. The total brushing time was computed based on earlier research [32,33], which affirms that with a twice-daily brushing practice, the maximum contact time for each tooth surface per day is 5 s.
Group D: The samples were whitened with a tooth-whitening pen (Active Wow, Tallahassee, FL, USA). The pen was moved up and down to disseminate the gel onto the sample surface and then the sample was allowed to dry for one minute, followed by rinsing under tap water after 20 min. The whitening process was performed for two days.
Group E: The samples were treated with 0.25% citric acid for one hour.
Group F: The samples were whitened with iWhite instant Dark Stains whitening kit (Sylphar, Deurle, Belgium) containing a prefabricated tray. The samples were exposed to the whitening agent in a prefabricated tray for 20 min a day for 5 days.
All the samples were stored in distilled water in an incubator at 37 °C for the duration of the experimental study. In this study, the use of distilled water instead of artificial salvia was agreed upon to solely evaluate the effect of each tooth-whitening product and minimize variables that could affect the outcome of this study.
2.3. Surface Roughness (Ra) Analysis
The Ra of the prepared samples was analyzed using a noncontact profilometer (Bruker Contour GT-K, Tucson, AZ, USA). The profilometer is equipped with a 3D optical microscope with a nanolens atomic force microscopy (AFM) module, which uses a vision 64 (Bruker, Tucson, AZ, USA) to control the device settings and high-resolution graphical output of the scanned sample surface. The sample was placed on the fully automated turret and scanned at a rate of 1× using vertical white-light interferometry with Gaussian regression filter, 1 mm × 1 mm field of view, and broad daylight source [34,35]. Each tooth sample was scanned at three different areas and the Ra values were averaged in µm for that specific sample.
2.4. Microhardness Measurement
Microhardness of the samples was evaluated using a hardness tester (INNOVATEST, Borgharenweg, Maastricht, The Netherlands) equipped with a Knoops pyramid diamond indenter tip. The enamel samples were positioned perpendicular to the long axis of the indenter and were impressed with a load of 300 g for 10 s. The indentations were performed on the even enamel surface for measurement accuracy [36]. Three indents were performed for sample surfaces at different locations with a minimum spacing of twice the indent diagonal. The indentation load and time was invariable for all samples. The measurements were converted into Knoop Hardness Number (KHN) by the software accustomed to the device using Equation (1) as below:
where F is the indentation load (in g) and d is the diagonal of the indentation (in µm).
HK = 14.229 (F/d2)
Microhardness and surface roughness measurements were repeated for all the samples in each group to obtain the final or after whitening readings (T1). (Table 1).
2.5. Statistical Analysis
Data were coded and entered using statistical package for the social sciences (SPSS) software (version 22, IBM SPSS Inc., Chicago, IL, USA) for data analysis. Kolmogorov–Smirnov test demonstrated nonuniform distribution of the data, and hence nonparametric test was applied. Quantitative variables were summarized by median as measures of central tendency and range as measures of dispersion (min–max). The Wilcoxon test was used to evaluate the difference between the measurements within the groups and Kruskal–Wallis test was used to compare the difference between the groups. The Mann–Whitney test was used for pairwise comparison between two independent groups to determine any significant difference (α = 0.05)
3. Results
3.1. Surface Roughness (Ra)
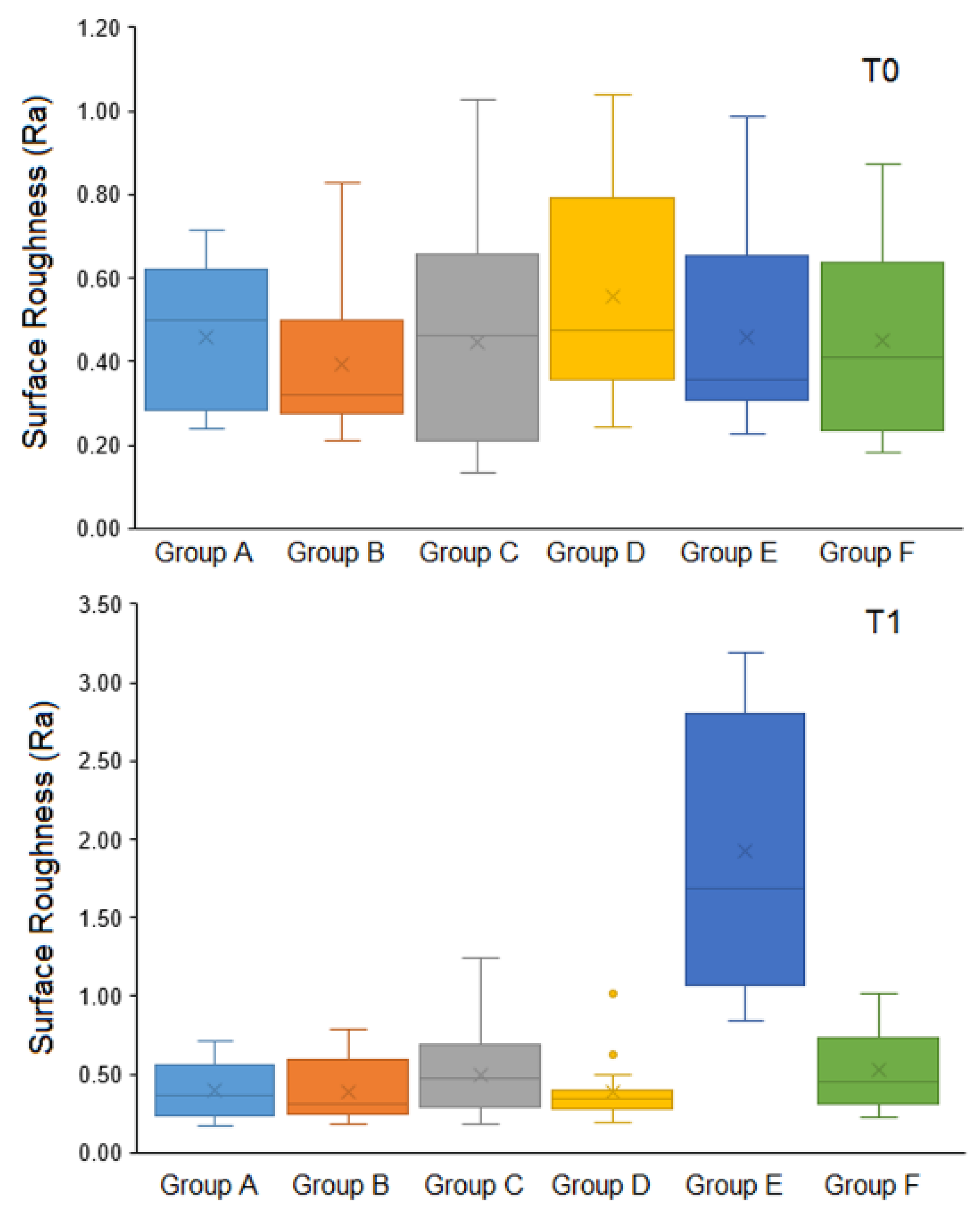
Figure 1 box plots present the median surface roughness (Ra) of the study groups at baseline (T0) and after whitening (T1). Three of the study groups (A, B, and D) demonstrated decreased Ra, whereas groups C, E, and F showed increased Ra after whitening. Group B and E specimens demonstrated the lowest (0.31, 0.19–0.79) and highest Ra (1.69, 0.84–3.19), respectively, after whitening. Among the groups whitened with OTC products, iWhite Dark Stains whitening kit (Group D) specimens demonstrated the lowest Ra (0.35, 0.19–1.01) and iWhite Dark Stains toothpaste (Group C) specimens demonstrated the highest Ra (0.48, 0.19–1.24) at T1. Group A specimens whitened with professionally supervised carbamide peroxide whitening product demonstrated Ra values of 0.36 (0.17–0.71).
Table 2 presents the significant difference in median Ra within and between the groups at T0 and T1 measurement intervals. When comparing Ra from T0 to T1 within each group separately, a statistically significant difference was demonstrated among the study groups (p < 0.001) except for Group B (p = 0.85).
The comparison of Ra showed a non-significant difference between the groups at T0 (H = 3.79, p = 0.579). In contrast, there was a statistically significant difference in Ra between groups at T1 (H = 38.7, p < 0.0001) (Kruskal–Wallis test). Pairwise comparison using the Mann–Whitney test demonstrated a significant difference between Group E and the remaining study groups (p < 0.0001).
3.2. Microhardness (KHN)
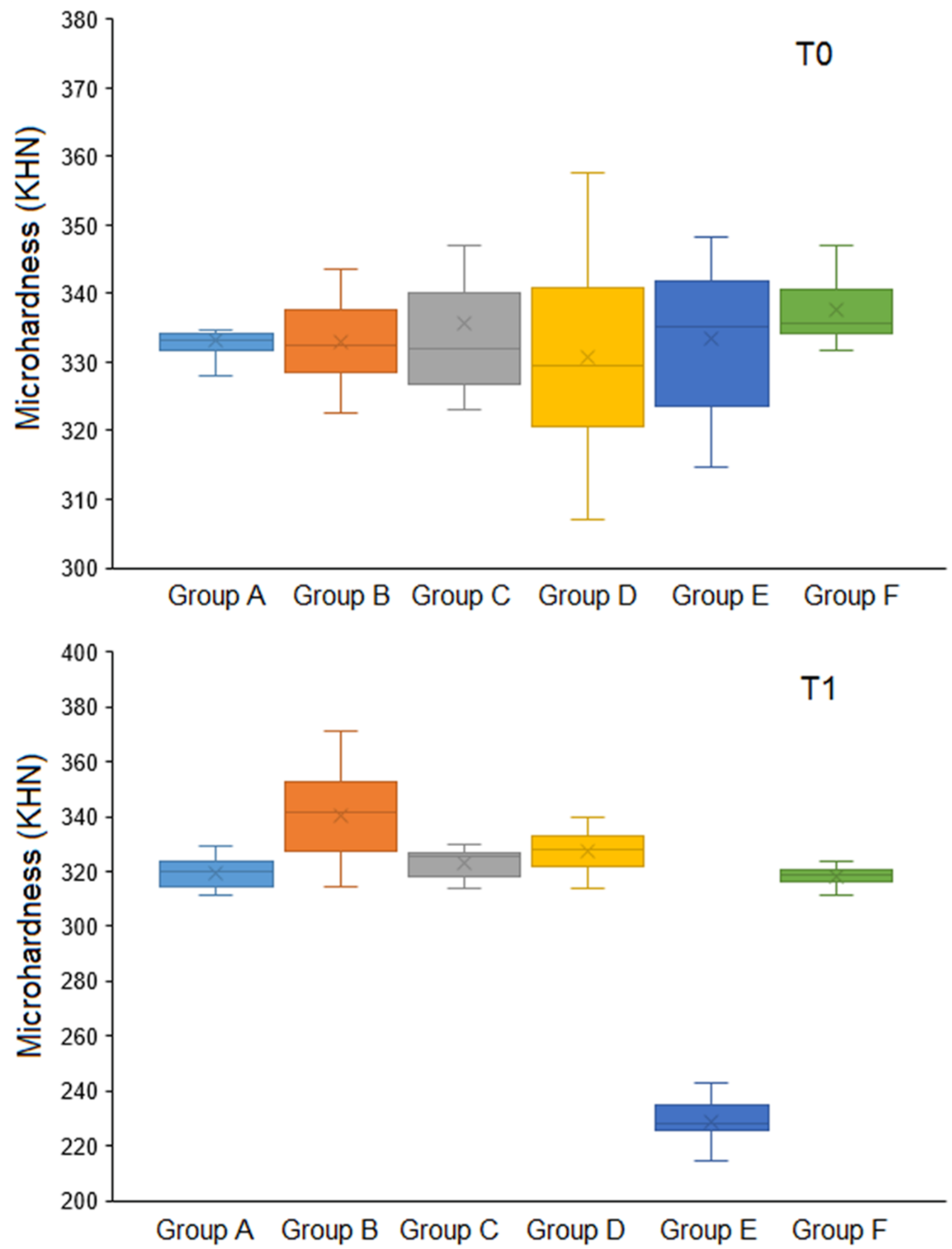
Figure 2 box plots present the median Knoop hardness (KHN) of the study groups at baseline (T0) and after whitening (T1). The study groups showed decreased KHN after whitening, except for specimens immersed in Group B (distilled water), which showed an increased KHN (341.5, 314.7–371.2). The lowest KHN was observed for Group E specimens (227.9, 202.3–272.3). Among the groups whitened with OTC products, iWhite Dark Stains Whitening Kit (Group D) specimens demonstrated the highest KHN (328, 314–340) and whitening pen (Group F) specimens demonstrated the lowest KHN (318.8, 311.4–323.7).
Table 3 presents the significant difference in median KHN within the groups and between the groups at T0 and T1 measurement intervals. The comparison of KHN within the groups from T0 to T1 revealed a significant decrease in the hardness for Groups A, C, E, and F (p = 0.001). Group B specimens showed increased KNH from T0 to T1; however, the difference was not statistically significant (p = 0.112). Similarly, group D specimens demonstrated a nonsignificant decrease in KHN from T0 to T1 (p = 0.29).
The comparison of KHN showed no significant difference between the groups at T0 (H = 8.449, p = 0.133). However, the Kruskal–Wallis test demonstrated significant difference in KHN between the groups at T1 (H = 55.83, p < 0.0001). Hence, pairwise comparison was performed between the groups using the Mann–Whitney test, which showed significant difference in KHN between Group E vs. [Group A (p = 0.012), Group B (p < 0.0001), Group C (p < 0.0001), Group D (p < 0.0001), and Group F (p = 0.032)]; Group F vs. Group B (p = 0.005) and Group A vs. Group B (p < 0.013).
4. Discussion
Different tooth-whitening techniques and products have become popular with both the dental professionals and the public. However, chemical intervention has been found to be the most effective approach in altering both extrinsic and intrinsic tooth stain and discoloration [37]. Bleaching vital teeth entails direct contact of a highly oxidizing whitening agents with the enamel surface for an extended period of time that varies depending on the product used, raising concerns about potential enamel damage [38]. In the current study, dentist-supervised at-home whitening with a 10% carbamide peroxide, which is considered the gold standard for whitening treatment [39,40,41,42], and three new OTC whitening products with no existing literature were tested and compared with regard to surface roughness and enamel microhardness. There was a significant change in surface roughness and Knoop hardness from pre- to post-bleaching among the study groups. Based on the outcome, the null hypothesis was rejected.
The physical and mechanical properties of enamel are affected by changes in enamel morphology and microstructure caused by tooth whitening [43]. The reaction between peroxide and organic molecules on the surface or in the subsurface of the enamel could cause morphological changes in the enamel. When teeth are exposed to peroxide, an initial process of enamel demineralization occurs, resulting in the loss of calcium in the teeth [44]. Apart from the dentist-supervised carbamide peroxide group and the OTC groups, the enamel specimens in this study were also exposed to citric acid and distilled water to better understand the effect of these whitening agents on the enamel surface.
The Ra outcome showed no statistically significant difference between groups before whitening. In contrast, there was a highly statistically significant difference between the groups after whitening. Previous studies have reported an increase in enamel surface roughness following bleaching [45,46,47,48]. Surprisingly, the control Group A and the whitening pen group among the OTC groups in this study showed significantly decreased Ra after whitening. Additionally, there was a statistically significant difference in median roughness from pre- to post-whitening among the groups, except for the distilled water group, which showed no statistically significant difference before and after the treatment. Therefore, the outcomes of the present study are in partial agreement with previous studies that demonstrated changes of negligible quantity or no significant changes in enamel surface roughness following bleaching [49,50,51,52].
The differences in the results across different studies could be attributed to the study design, composition of the bleaching materials, relationship established between concentration of the bleaching agent and duration of use, and also the bleaching agent diffusion capacity and pH [53]. The active ingredients in the whitening products used in this study are varied. Group A contains 10% carbamide peroxide, equivalent to 3.62% H2O2; iWhite instant Dark Stains whitening kit and iWhite instant Dark Stains toothpaste are activated by hydrated silica, sodium hexametaphosphate, and charcoal powder; and the whitening pen is activated by sodium bicarbonate and organic coconut charcoal. However, in recent years it has been well-established that polishing, fluoride application, and remineralizing solutions can significantly reduce the roughness of bleached enamel [47].
Surface hardness measurement is a reasonably easy way of determining the mechanical property of enamel and dentin to withstand plastic deformation from a reference sample, and it is strongly related to mineral component loss or gain [22]. The enamel microhardness measurement results showed no statistically significant difference between groups before experimental treatment. On the other hand, there was a highly statistically significant decrease in KHN between groups after whitening, except for the Active Wow whitening pen group, where the decrease was negligible and nonsignificant. The distilled water group showed an increased hardness, which was nonsignificant.
The contact time of bleaching agent with enamel, the active ingredients of bleaching gels and their concentration, pH, activators, and thickeners are related to the decrease in hardness [46,47]. In addition to affecting the bleaching efficiency, the pH of the whitening agent can also alter the morphology of the enamel surface and the hardness of teeth [46]. The pH of the vast majority of bleaching products on the market is neutral or slightly acidic. Nonetheless, the medium becomes acidic over time following application [54], which causes hardness reduction. Based on the outcome of this study, all whitening agents demonstrated reduced enamel hardness following whitening, which is in agreement with previous studies [38,46,48,55,56,57]. The concentration of citric acid for effective whitening is reported to be at 5% [9]. In the current study, only 0.25% of the citric acid was used for whitening, but still there was highly significant decrease in hardness compared to other groups (335.4 to 227.9 KHN). This study is in disagreement with previous studies that reported no changes in hardness following bleaching [21,28]. Exposing teeth to saliva after bleaching, on the other hand, promotes remineralization and stabilization of enamel hardness [58]. This was further confirmed in a review that used microhardness testing for structural enamel defects after whitening found that those studies that used human saliva and fluoride to closely simulate an intraoral environment and a post-treatment evaluation phase had a lower risk of enamel microhardness reduction than the others [20].
In the present study, 2 mm-thick enamel specimens were used to determine the whitening products’ effect on enamel microhardness and surface roughness. One of the important factors contributing to the effectiveness of whitening products on the tooth surface is the enamel and dentine thickness. Randomized clinical investigations have found that tooth sensitivity after bleaching treatments is only present in the anterior teeth, with the severity of this side effect being directly correlated with the thickness of the enamel and dentin [59,60]. The diffusion of chemicals generated by bleaching gels through enamel and dentin may also be influenced by variations in the thickness of enamel and dentin. The degree of pulp damage can vary as a result of these variations. As a result, the combination of these factors may cause sensitivity following tooth whitening [59].
According to a review of the literature by Haywood [61], bleaching-induced tooth sensitivity typically affects the smaller teeth, namely the mandibular incisors and maxillary laterals. In contrast to premolars, incisors have thinner enamel and dentine layers, which may facilitate the rapid flow of whitening agents to the pulp and leave less time for the production and release of enzymes that protect against damage from whitening agents [62]. In a recent study by Públio et al. [63], the authors demonstrated that the presence of at least 0.5 mm enamel reduced the bleaching effectiveness (higher ΔE) at all measured intervals for both carbamide peroxide and hydrogen peroxide bleaching gels. Furthermore, the thickness of dentin can negatively interfere with color changes of enamel. D’Arce et al. showed that 35% hydrogen peroxide with calcium showed lower bleaching on the enamel surface in 3.5 mm-thickness samples compared to 2 mm [64].
Concerns were raised about the damaging potential of the tooth-whitening agent on the tooth surface and subsurface; the incorporation of fluoride, casein phosphopeptide-stabilized amorphous calcium phosphate nanocomplexes (CPP-ACP), and other remineralization agents aided in the prevention of such outcome. The use of fluoride in conjunction, before, or after the tooth-whitening treatment is beneficial. Fluoride application promotes remineralization and inhibits demineralization of the tooth hard tissues by resisting acid attacks. Fluoride interacts with the mineral portion of the tooth and produces fluorohydroxyapatite mineral, in which it results in a stronger enamel crystal network that is more resistant to acid dissolution caused by demineralization [55]. CPP-ACP is a complex rich of calcium and phosphate, derived from milk, which can aid in the remineralization and inhibit demineralization of the tooth when applied topically or systemically [65]. Recently the introduction of the biomimetic effect of nanohydroxyapatite was effective in reducing tooth surface hypomineralization due to its complete integration within the enamel structure [66].
Future studies directed towards evaluating the whitening effects of the OTC products and the determination of pH would be helpful to better understand the effectiveness of these products. Despite following the manufacturers’ recommendation for the application of the whitening products and testing in accordance with ISO guidelines, the study has a few limitations. Firstly, the samples in between the whitening process were stored in distilled water but not in artificial saliva, which could have promoted remineralization and thereby demonstrated a different outcome. Secondly, the results could have been different in the intraoral environment, which is greatly influenced by enamel structure, salivary composition, and dietary habits. Thus, relating the outcome of this study to clinical conditions should be carried out with extreme consideration.
5. Conclusions
Within the limitations of this study, it could be demonstrated that surface roughness and enamel microhardness changes were influenced by the type, composition, and exposure time of the whitening product. Among the OTC products, the Active Wow whitening pen demonstrated better outcome compared to other OTC products and dentist-supervised 10% carbamide peroxide whitening agent.
Further investigation is needed for the colorimetric and remineralization evaluation of the OTC products used in this study.
Author Contributions
Conceptualization, A.A. and M.H.A.; methodology, F.A., N.A. and Y.A.; investigation, A.A. and M.H.A.; data curation, F.A., N.A. and Y.A.; writing—original draft preparation, F.A., N.A. and Y.A.; writing—review & editing, A.A. and M.H.A.; visualization, A.A.; supervision, A.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
An ethical approval was obtained from the deanship of scientific research at Prince Sattam Bin Abdulalziz University, Al-Kharj, Saudi Arabia (PSAU2021013).
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Shamel, M.; Al-Ankily, M.M.; Bakr, M.M. Influence of different types of whitening tooth pastes on the tooth color, enamel surface roughness and enamel morphology of human teeth. F1000Research 2019, 8, 1764. [Google Scholar] [CrossRef]
- Xiao, J.; Zhou, X.D.; Zhu, W.C.; Zhang, B.; Li, J.Y.; Xu, X. The prevalence of tooth discolouration and the self-satisfaction with tooth colour in a Chinese urban population. J. Oral Rehabil. 2007, 34, 351–360. [Google Scholar] [CrossRef]
- Cvikl, B.; Lussi, A.; Moritz, A.; Flury, S. Enamel Surface Changes After Exposure to Bleaching Gels Containing Carbamide Peroxide or Hydrogen Peroxide. Oper. Dent. 2016, 41, E39–E47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pascolutti, M.; de Oliveira, D. A Radical-Free Approach to Teeth Whitening. Dent. J. 2021, 9, 148. [Google Scholar] [CrossRef] [PubMed]
- Domínguez, A.; García, J.A.; Costela, A.; Gómez, C. Influence of the Light Source and Bleaching Gel on the Efficacy of the Tooth Whitening Process. Photomed. Laser Surg. 2011, 29, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Minoux, M.; Serfaty, R. Vital tooth bleaching: Biologic adverse effects—A review. Quintessence Int. 2008, 39, 645–659. [Google Scholar] [PubMed]
- Naidu, A.S.; Bennani, V.; Brunton, J.M.A.P.; Brunton, P. Over-the-Counter Tooth Whitening Agents: A Review of Literature. Braz. Dent. J. 2020, 31, 221–235. [Google Scholar] [CrossRef]
- Kwon, S.; Meharry, M.; Oyoyo, U.; Li, Y. Efficacy of Do-It-Yourself Whitening as Compared to Conventional Tooth Whitening Modalities: An In Vitro Study. Oper. Dent. 2015, 40, E21–E27. [Google Scholar] [CrossRef] [Green Version]
- Barbuzan-Caragyov, A.; Hajaj, T.; Cojocariu, A.; Christa, S.; Sinescu, C. Efficiency of Natural Ingredients in Teeth Whitening. Dent. Mater. 2022, 38, e6–e7. [Google Scholar] [CrossRef]
- Pratiwi, F.; Tinata, J.K.; Prakasa, A.W.; Istiqomah; Hartini, E.; Isworo, S. Citric acid compounds of tangerines peel extract (Citrus reticulata) as potential materials teeth whitening. J. Phys. Conf. Ser. 2017, 824, 012071. [Google Scholar] [CrossRef]
- Karadas, M.; Duymus, Z.Y. In Vitro Evaluation of the Efficacy of Different Over-The-Counter Products on Tooth Whitening. Braz. Dent. J. 2015, 26, 373–377. [Google Scholar] [CrossRef] [Green Version]
- Li, Y. Safety Controversies in Tooth Bleaching. Dent. Clin. N. Am. 2011, 55, 255–263. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Greenwall, L. Safety issues of tooth whitening using peroxide-based materials. Br. Dent. J. 2013, 215, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Alqahtani, M.Q. Tooth-bleaching procedures and their controversial effects: A literature review. Saudi Dent. J. 2014, 26, 33–46. [Google Scholar] [CrossRef] [Green Version]
- American Dental Association. ADA Current Policies, Adopted 1954–2020. 2021. Available online: https://www.ada.org/-/media/project/ada-organization/ada/ada-org/files/about/current-policies-and-historical-publications/current_policies.pdf (accessed on 22 January 2022).
- Attin, T.; Schmidlin, P.R.; Wegehaupt, F.; Wiegand, A. Influence of study design on the impact of bleaching agents on dental enamel microhardness: A review. Dent. Mater. 2009, 25, 143–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azrak, B.; Callaway, A.; Kurth, P.; Willershausen, B. Influence of Bleaching Agents on Surface Roughness of Sound or Eroded Dental Enamel Specimens. J. Esthet. Restor. Dent. 2010, 22, 391–399. [Google Scholar] [CrossRef] [PubMed]
- Basting, R.T.; Rodrigues, A.L., Jr.; Serra, M.C. The effect of 10% carbamide peroxide, carbopol and/or glycerin on enamel and dentin microhardness. Oper. Dent. 2006, 30, 608–616. [Google Scholar]
- Götz, H.; Duschner, H.; White, D.J.; Klukowska, M.A. Effects of elevated hydrogen peroxide ‘strip’ bleaching on surface and subsurface enamel including subsurface histomorphology, micro-chemical composition and fluorescence changes. J. Dent. 2007, 35, 457–466. [Google Scholar] [CrossRef]
- Joiner, A. Review of the effects of peroxide on enamel and dentine properties. J. Dent. 2007, 35, 889–896. [Google Scholar] [CrossRef]
- Kwon, S.R.; Kurti, S.R.; Oyoyo, U.; Li, Y. Effect of various tooth whitening modalities on microhardness, surface roughness and surface morphology of the enamel. Odontology 2015, 103, 274–279. [Google Scholar] [CrossRef]
- Kwon, S.R.; Wang, J.; Oyoyo, U.; Li, Y. Evaluation of bleaching efficacy and erosion potential of four different over-the-counter bleaching products. Am. J. Dent. 2013, 26, 356–360. [Google Scholar]
- Mondelli, R.F.; Azevedo, J.F.; Francisconi, P.A.; Ishikiriama, S.K.; Mondelli, J. Wear and surface roughness of bovine enamel submitted to bleaching. Eur. J. Esthet. Dent. 2009, 4, 396–403. [Google Scholar]
- Potočnik, I.; Kosec, L.; Gašperšič, D. Effect of 10% Carbamide Peroxide Bleaching Gel on Enamel Microhardness, Microstructure, and Mineral Content. J. Endod. 2000, 26, 203–206. [Google Scholar] [CrossRef]
- Scherer, W.; Penugonda, B.; Styner, D.; Georgescu, M. At-home vital bleaching: Effects on stained enamel and dentin. Pract. Periodontics Aesthet. Dent. 1992, 4, 11–15. [Google Scholar]
- Sun, L.; Liang, S.; Sa, Y.; Wang, Z.; Ma, X.; Jiang, T.; Wang, Y. Surface alteration of human tooth enamel subjected to acidic and neutral 30% hydrogen peroxide. J. Dent. 2011, 39, 686–692. [Google Scholar] [CrossRef]
- Yeh, S.T.; Su, Y.; Lu, Y.C.; Lee, S.Y. Surface changes and acid dissolution of enamel after carbamide peroxide bleach treatment. Oper. Dent. 2005, 30, 507–515. [Google Scholar]
- Mielczarek, A.; Klukowska, M.; Ganowicz, M.; Kwiatkowska, A.; Kwaśny, M. The effect of strip, tray and office peroxide bleaching systems on enamel surfaces in vitro. Dent. Mater. 2008, 24, 1495–1500. [Google Scholar] [CrossRef]
- Polydorou, O.; Hellwig, E.; Hahn, P. The Efficacy of Three Different In-office Bleaching Systems and Their Effect on Enamel Microhardness. Oper. Dent. 2008, 33, 579–586. [Google Scholar] [CrossRef]
- Sulieman, M.; Addy, M.; Macdonald, E.; Rees, J. A safety study in vitro for the effects of an in-office bleaching system on the integrity of enamel and dentine. J. Dent. 2004, 32, 581–590. [Google Scholar] [CrossRef]
- Wang, X.; Mihailova, B.; Klocke, A.; Fittschen, U.E.A.; Heidrich, S.; Hill, M.; Stosch, R.; Güttler, B.; Broekaert, J.A.C.; Bismayer, U. Side effects of a non-peroxide-based home bleaching agent on dental enamel. J. Biomed. Mater. Res. Part A 2009, 88A, 195–204. [Google Scholar] [CrossRef]
- Bizhang, M.; Schmidt, I.; Chun, Y.-H.P.; Arnold, W.H.; Zimmer, S. Toothbrush abrasivity in a long-term simulation on human dentin depends on brushing mode and bristle arrangement. PLoS ONE 2017, 12, e0172060. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.-H.; Kim, S.-H.; Han, J.-S.; Yeo, I.-S.L.; Yoon, H.-I. Optical and Surface Properties of Monolithic Zirconia after Simulated Toothbrushing. Materials 2019, 12, 1158. [Google Scholar] [CrossRef] [Green Version]
- Aldosari, L.I.; Alshadidi, A.A.; Porwal, A.; Al Ahmari, N.M.; Al Moaleem, M.M.; Suhluli, A.M.; Shariff, M.; Shami, A.O. Surface roughness and color measurements of glazed or polished hybrid, feldspathic, and Zirconia CAD/CAM restorative materials after hot and cold coffee immersion. BMC Oral Health 2021, 21, 422. [Google Scholar] [CrossRef]
- Durgesh, B.H.; Alaqeel, S.; Ajwa, N.A.I.K.; Hadhari, M.; Alsadon, O.; Matinlinna, J. Experimental silane primer and grit-blasting distance in orthodontic bonding of zirconia surfaces. Ceram. Silik. 2020, 469–477. [Google Scholar] [CrossRef]
- Chuenarrom, C.; Benjakul, P.; Daosodsai, P. Effect of indentation load and time on knoop and vickers microhardness tests for enamel and dentin. Mater. Res. 2009, 12, 473–476. [Google Scholar] [CrossRef]
- Lee, S.S.; Kwon, S.R.; Ward, M.; Jenkins, W.; Souza, S.; Li, Y. A 3 months clinical evaluation comparing two professional bleaching systems of 25% and 40% hydrogen peroxide and extended treatment outcome using a power versus a manual toothbrush. J. Esthet. Restor. Dent. 2019, 31, 124–131. [Google Scholar] [CrossRef]
- Goyal, K.; Saha, S.G.; Bhardwaj, A.; Saha, M.K.; Bhapkar, K.; Paradkar, S. A comparative evaluation of the effect of three different concentrations of in-office bleaching agents on microhardness and surface roughness of enamel—An in vitro study. Dent. Res. J. 2021, 18, 49. [Google Scholar] [CrossRef]
- Auschill, T.M.; Hellwig, E.; Schmidale, S.; Sculean, A.; Arweiler, N.B. Efficacy, side-effects and patients’ acceptance of different bleaching techniques (OTC, in-office, at-home). Oper. Dent. 2005, 30, 156–163. [Google Scholar] [CrossRef]
- Browning, W.D.; Chan, D.C.; Myers, M.L.; Brackett, W.; Brackett, M.; Pashley, D.H. Comparison of Traditional and Low Sensitivity Whiteners. Oper. Dent. 2008, 33, 379–385. [Google Scholar] [CrossRef] [Green Version]
- Haywood, V.B. Frequently asked questions about bleaching. Compend. Contin. Educ. Dent. 2003, 24, 324–338. [Google Scholar]
- Zekonis, R.; Matis, B.A.; Cochran, M.A.; Al Shetri, S.E.; Eckert, G.J.; Carlson, T.J. Clinical evaluation of in-office and at-home bleaching treatments. Oper. Dent. 2003, 28, 114–121. [Google Scholar]
- Wongpraparatana, I.; Matangkasombut, O.; Thanyasrisung, P.; Panich, M. Effect of Vital Tooth Bleaching on Surface Roughness and Streptococcal Biofilm Formation on Direct Tooth-Colored Restorative Materials. Oper. Dent. 2018, 43, 51–59. [Google Scholar] [CrossRef]
- Wijetunga, C.L.; Otsuki, M.; Abdou, A.; Luong, M.N.; Qi, F.; Tagami, J. The effect of in-office bleaching materials with different pH on the surface topography of bovine enamel. Dent. Mater. J. 2021, 40, 1345–1351. [Google Scholar] [CrossRef]
- De Araújo, L.S.N.; dos Santos, P.H.; Anchieta, R.B.; Catelan, A.F.; Briso, A.L.F.; Zaze, A.C.S.F.; Sundfeld, R.H. Mineral loss and color change of enamel after bleaching and staining solutions combination. J. Biomed. Opt. 2013, 18, 108004. [Google Scholar] [CrossRef]
- Eskelsen, E.; Catelan, A.; Hernades, N.M.A.P.; Soares, L.E.S.; Cavalcanti, A.N.; Aguiar, F.H.B.; Liporoni, P.C.S. Physicochemical changes in enamel submitted to pH cycling and bleaching treatment. Clin. Cosmet. Investig. Dent. 2018, 10, 281–286. [Google Scholar] [CrossRef] [Green Version]
- Pimenta-Dutra, A.-C.; Albuquerque, R.-D.C.; Morgan, L.-F.S.-A.; Pereira, G.-M.; Nunes, E.; Horta, M.-C.; Silveira, F.-F. Effect of bleaching agents on enamel surface of bovine teeth: A SEM study. J. Clin. Exp. Dent. 2017, 9, e46–e50. [Google Scholar] [CrossRef]
- Sasaki, R.T.; Catelan, A.; Bertoldo Edos, S.; Venâncio, P.C.; Groppo, F.C.; Ambrosano, G.M.; Marchi, G.M.; Lima, D.A.; Aguiar, F.H. Effect of 7.5% hydrogen peroxide containing remineralizing agents on hardness, color change, roughness and micromorphology of human enamel. Am. J. Dent. 2015, 28, 261–267. [Google Scholar]
- Farawati, F.A.; Hsu, S.-M.; O’Neill, E.; Neal, D.; Clark, A.; Esquivel-Upshaw, J. Effect of carbamide peroxide bleaching on enamel characteristics and susceptibility to further discoloration. J. Prosthet. Dent. 2019, 121, 340–346. [Google Scholar] [CrossRef]
- Gümüştaş, B.; Gürbüz, Ö.; Begum, G.E. Effects of Bleaching Agents, Neutral Fluoride Gels, and Surface Sealants on Enamel Surface Roughness. J. Oper. Dent. Endod. 2017, 2, 74–78. [Google Scholar] [CrossRef]
- Nam, S.-H.; Ok, S.-M.; Kim, G.-C. Tooth bleaching with low-temperature plasma lowers surface roughness and Streptococcus mutans adhesion. Int. Endod. J. 2018, 51, 479–488. [Google Scholar] [CrossRef]
- Sa, Y.; Sun, L.; Wang, Z.; Ma, X.; Liang, S.; Xing, W.; Jiang, T.; Wang, Y. Effects of Two In-Office Bleaching Agents with Different pH on the Structure of Human Enamel: An In Situ and In Vitro Study. Oper. Dent. 2013, 38, 100–110. [Google Scholar] [CrossRef] [Green Version]
- De Carvalho, A.-C.; De Souza, T.-F.; Liporoni, P.-C.; Pizi, E.-C.; Matuda, L.-S.A.; Catelan, A. Effect of bleaching agents on hardness, surface roughness and color parameters of dental enamel. J. Clin. Exp. Dent. 2020, 12, e670–e675. [Google Scholar] [CrossRef]
- Grazioli, G.; Valente, L.L.; Isolan, C.P.; Pinheiro, H.A.; Duarte, C.G.; Münchow, E.A. Bleaching and enamel surface interactions resulting from the use of highly-concentrated bleaching gels. Arch. Oral Biol. 2018, 87, 157–162. [Google Scholar] [CrossRef]
- Fukuyama, M.; Kawamoto, C.; Saikaew, P.; Matsuda, Y.; Carvalho, R.M.; Selimovic, D.; Sano, H. Effect of topical fluoride application on enamel after in-office bleaching, as evaluated using a novel hardness tester and a transverse microradiography method. Eur. J. Oral Sci. 2017, 125, 471–478. [Google Scholar] [CrossRef]
- Furlan, I.S.; Bridi, E.C.; Amaral, F.; França, F.M.G.; Turssi, C.P.; Basting, R.T. Effect of high- or low-concentration bleaching agents containing calcium and/or fluoride on enamel microhardness. Gen. Dent. 2017, 65, 66–70. [Google Scholar]
- Pinto, C.F.; De Oliveira, R.; Cavalli, V.; Giannini, M. Peroxide bleaching agent effects on enamel surface microhardness, roughness and morphology. Braz. Oral Res. 2004, 18, 306–311. [Google Scholar] [CrossRef]
- Polydorou, O.; Scheitza, S.; Spraul, M.; Vach, K.; Hellwig, E. The effect of long-term use of tooth bleaching products on the human enamel surface. Odontology 2018, 106, 64–72. [Google Scholar] [CrossRef]
- de Almeida, L.C.; Costa, C.A.; Riehl, H.; dos Santos, P.H.; Sundfeld, R.H.; Briso, A.L. Occurrence of sensitivity during at-home and in-office tooth bleaching therapies with or without use of light sources. Acta Odontol. Latinoam. 2012, 25, 3–8. [Google Scholar]
- Duque, C.D.O.; Soares, D.; Basso, F.; Hebling, J.; de Souza Costa, C.D.S. Influence of enamel/dentin thickness on the toxic and esthetic effects of experimental in-office bleaching protocols. Clin. Oral Investig. 2017, 21, 2509–2520. [Google Scholar] [CrossRef] [Green Version]
- Haywood, V.B. Treating sensitivity during tooth whitening. Compend. Contin. Educ. Dent. 2015, 26 (Suppl. 3), 11–20. [Google Scholar]
- Costa, C.A.D.S.; Riehl, H.; Kina, J.F.; Sacono, N.T.; Hebling, J. Human pulp responses to in-office tooth bleaching. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2010, 109, e59–e64. [Google Scholar] [CrossRef] [PubMed]
- Públio, J.D.C.; D’Arce, M.B.F.; Catelan, A.; Ambrosano, G.M.B.; Aguiar, F.H.B.; Lovadino, J.R.; Lima, D.A.N.L. Influence of Enamel Thickness on Bleaching Efficacy: An In-Depth Color Analysis. Open Dent. J. 2016, 10, 438–445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Arce, M.B.F.; Lima, D.A.N.L.; Aguiar, F.; Bertoldo, C.E.S.; Ambrosano, G.M.B.; Lovadino, J.R. Effectiveness of dental bleaching in depth after using different bleaching agents. J. Clin. Exp. Dent. 2013, 5, e100–e107. [Google Scholar] [CrossRef]
- Cochrane, N.; Reynolds, E. Calcium Phosphopeptides—Mechanisms of Action and Evidence for Clinical Efficacy. Adv. Dent. Res. 2012, 24, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Scribante, A.; Farahani, M.R.D.; Marino, G.; Matera, C.; y Baena, R.R.; Lanteri, V.; Butera, A. Biomimetic Effect of Nano-Hydroxyapatite in Demineralized Enamel before Orthodontic Bonding of Brackets and Attachments: Visual, Adhesion Strength, and Hardness in In Vitro Tests. BioMed Res. Int. 2020, 2020, 6747498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Figure 1.
Box plots of surface roughness (Ra) of the study groups at different measurement intervals. Group A—Opalescence™ PF; Group B—distilled water; Group C—iWhite Dark Stains Toothpaste; Group D—24 K white charcoal teeth-whitening pen; Group E—0.
Figure 1.
Box plots of surface roughness (Ra) of the study groups at different measurement intervals. Group A—Opalescence™ PF; Group B—distilled water; Group C—iWhite Dark Stains Toothpaste; Group D—24 K white charcoal teeth-whitening pen; Group E—0.

Figure 2.
Box plots of Knoop hardness (KHN) of the study groups at different measurement intervals. Group A—Opalescence™ PF; Group B—distilled water; Group C—iWhite Dark Stains Toothpaste; Group D—24 K white charcoal teeth-whitening pen; Group E—0.25% Citric.
Figure 2.
Box plots of Knoop hardness (KHN) of the study groups at different measurement intervals. Group A—Opalescence™ PF; Group B—distilled water; Group C—iWhite Dark Stains Toothpaste; Group D—24 K white charcoal teeth-whitening pen; Group E—0.25% Citric.


{kind=link}
{kind=link}
Table 1.
Materials and group coding used in the study.
| Group Code/ Materials/Manufacturer | Composition | Delivery Method/ Duration of Use |
|---|---|---|
| Group A/ Opalescence™ PF/ Ultradent, South Jordan, UT, USA | 10% carbamide peroxide, 0.5% potassium nitrate, and 0.11% fluoride ions (1000 ppm) | Custom-made trays/ Eight hours per day for 10 days |
| Group B | Distilled water | Immersed in 100 mL of distilled water |
| Group C/ iWhite Dark Stains Toothpaste/ Sylphar, Deurle, Belgium | Hydrated Silica, Sodium Hexametaphosphate. Mannitol, Chondrus Crispus Powder, Charcoal Powder, Sodium Fluoride, Sodium Saccharin. | Toothbrush/ Two brushing cycles per day for 60 days |
| Group D/ 24 K White Charcoal Teeth-Whitening Pen/ Active Wow, Tallahassee, FL, USA | Sodium Bicarbonate, Carbomer, Polysorbate 20, Sodium Hydroxide, Potassium Sorbate, Organic Coconut Charcoal. | Whitening pen/One application per day for two days |
| Group E | 0.25% Citric acid | Manual treatment for one hour |
| Group F/ iWhite Dark Stains Whitening Kit/ Sylphar, Deurle, Belgium | Hydrated Silica, Sodium Hexametaphosphate. Mannitol, Chondrus Crispus Powder, Charcoal Powder. | Ready-to-use trays/ 20 min per day for 5 days |
Table 2.
Comparison of surface roughness (Ra) of within and between the study groups, at baseline and after treatment.
Table 2.
Comparison of surface roughness (Ra) of within and between the study groups, at baseline and after treatment.
| Groups | T0 (Ra) | T1 (Ra) | Test of Significance (p) |
|---|---|---|---|
| Group A | 0.5 (0.24–0.72) a | 0.36 (0.17–0.71) a | z = −2.13, p = 0.032 * |
| Group B | 0.32 (0.21–0.83) a | 0.31 (0.19–0.79) a | z = − 0.18, p = 0.85 |
| Group C | 0.46 (0.13–1.03) a | 0.48 (0.19–1.24) a | z = −3.30, p = 0.001 * |
| Group D | 0.47 (0.24–1.04) a | 0.35 (0.19–1.01) a | z = −3.40, p = 0.001 * |
| Group E | 0.36 (0.22–0.99) a | 1.69 (0.84–3.19) b | z = − 3.35, p = 0.001 * |
| Group F | 0.41 (0.18–0.87) a | 0.45 (0.23– 1.02) a | z = −3.41, p = 0.001 * |
| H = 3.79, p = 0.579 | H = 38.7, p < 0.0001 * |
Z; Wilcoxon test; * statistically significant; Different lower case within a column indicates significant difference between the groups (p < 0.0001, pairwise comparison using Mann–Whitney test); H; Kruskal–Wallis test; Group A—Opalescence™ PF; Group B—distilled water; Group C—iWhite Dark Stains Toothpaste; Group D—24 K white charcoal teeth-whitening pen; Group E—0.25% citric acid; Group F—iWhite Dark Stains Whitening Kit.
Table 3.
Comparison of Knoop hardness (KHN) within and between the study groups.
| T0 | T1 | Test of Significance (p) | |
|---|---|---|---|
| Group A | 333.2 (323.7–346.5) a | 320 (311.1–329.1) a | z = −3.41, p = 0.001 * |
| Group B | 332.5 (322.7–343.5) a | 341.5 (314.7–371.2) b | z = −1.59, p = 0.112 |
| Group C | 331.9 (323.2–372.6) a | 325.5 (314–330.1) a,b | z = −3.23, p = 0.001 * |
| Group D | 329.5 (307.1–357.7) a | 328 (314–340) a,b | z = −1.05, p = 0.29 |
| Group E | 335.4 (330.5–340.4) a | 227.9 (202.3–272.3) c | z = − 3.41, p = 0.001 * |
| Group F | 335.7 (331.6–347) a | 318.8 (311.4–323.7) a,d | z = − 3.41, p = 0.001 * |
| H = 8.449, p = 0.133 | H = 55.83, p < 0.0001* |
Z; Wilcoxon test; * statistically significant; different lower case within a column indicates significant difference between the groups (p < 0.0001, pairwise comparison using Mann–Whitney test); H; Kruskal–Wallis test; Group A—Opalescence™ PF; Group B—distilled water; Group C—iWhite Dark Stains Toothpaste; Group D—24 K white charcoal teeth-whitening pen; Group E—0.25% citric acid; Group F—iWhite Dark Stains Whitening Kit.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
AlShehri, A.; AlRefeai, M.H.; AlZamil, F.; AlOtaibi, N.; AlKinani, Y. Effect of Over-The-Counter Tooth-Whitening Products on Enamel Surface Roughness and Microhardness. Appl. Sci. 2022, 12, 6930. https://doi.org/10.3390/app12146930
AMA Style
AlShehri A, AlRefeai MH, AlZamil F, AlOtaibi N, AlKinani Y. Effect of Over-The-Counter Tooth-Whitening Products on Enamel Surface Roughness and Microhardness. Applied Sciences. 2022; 12(14):6930. https://doi.org/10.3390/app12146930
Chicago/Turabian StyleAlShehri, Abdullah, Mohammad H. AlRefeai, Faisal AlZamil, Nawaf AlOtaibi, and Yara AlKinani. 2022. "Effect of Over-The-Counter Tooth-Whitening Products on Enamel Surface Roughness and Microhardness" Applied Sciences 12, no. 14: 6930. https://doi.org/10.3390/app12146930
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.