
Maxillary Sinus Osteoma as a Support for Dental Implant Associated to Sinus Augmentation Procedure: A Case Report and Literature Review

 ,
,  ,
,  and
and
Abstract
:1. Introduction
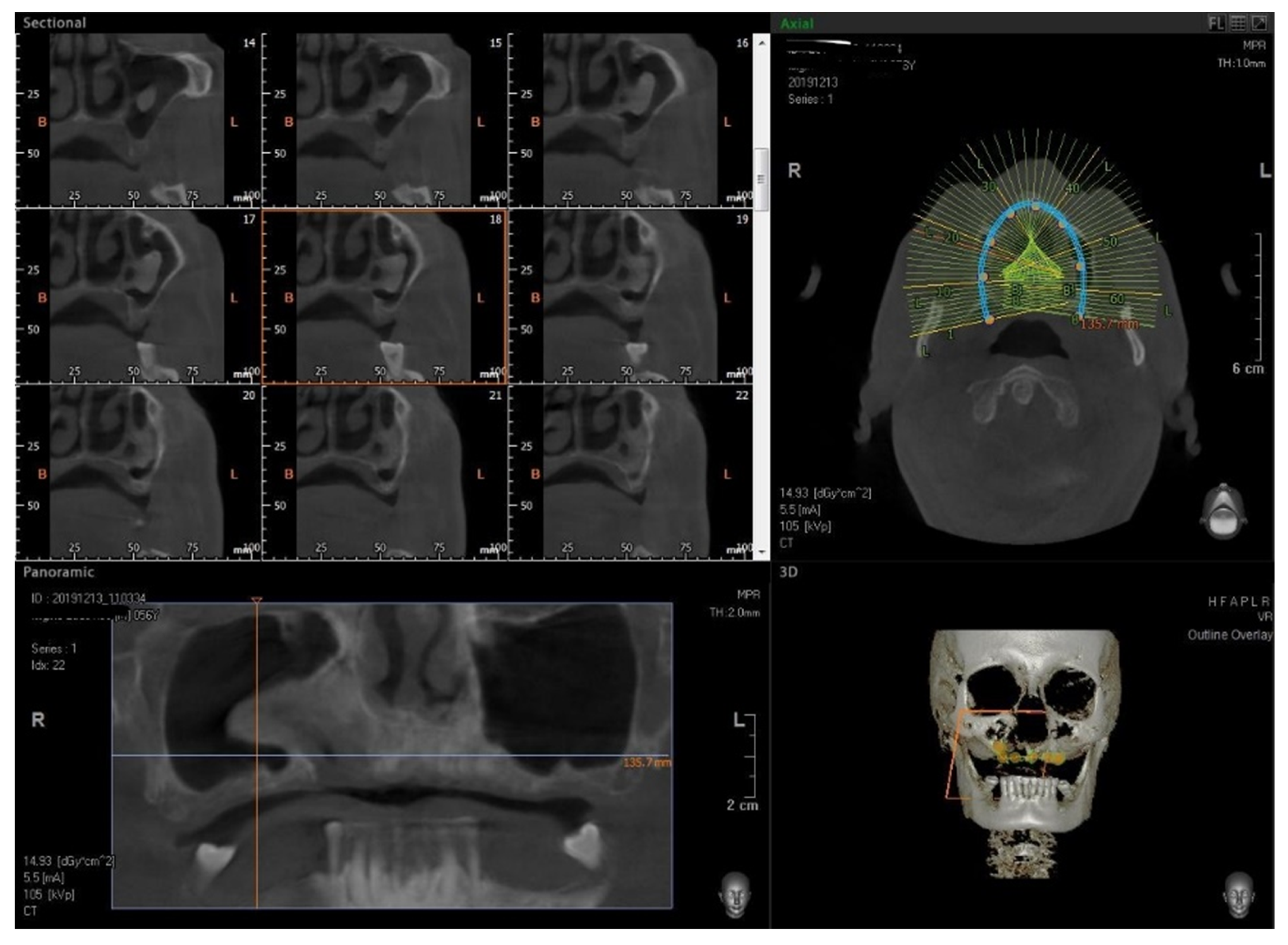
2. Materials and Methods
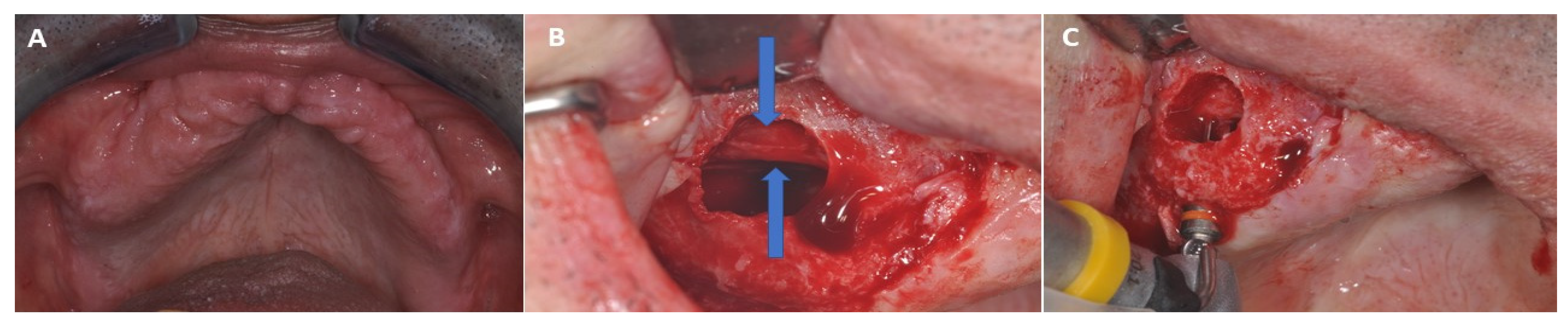
2.1. Surgical Procedure
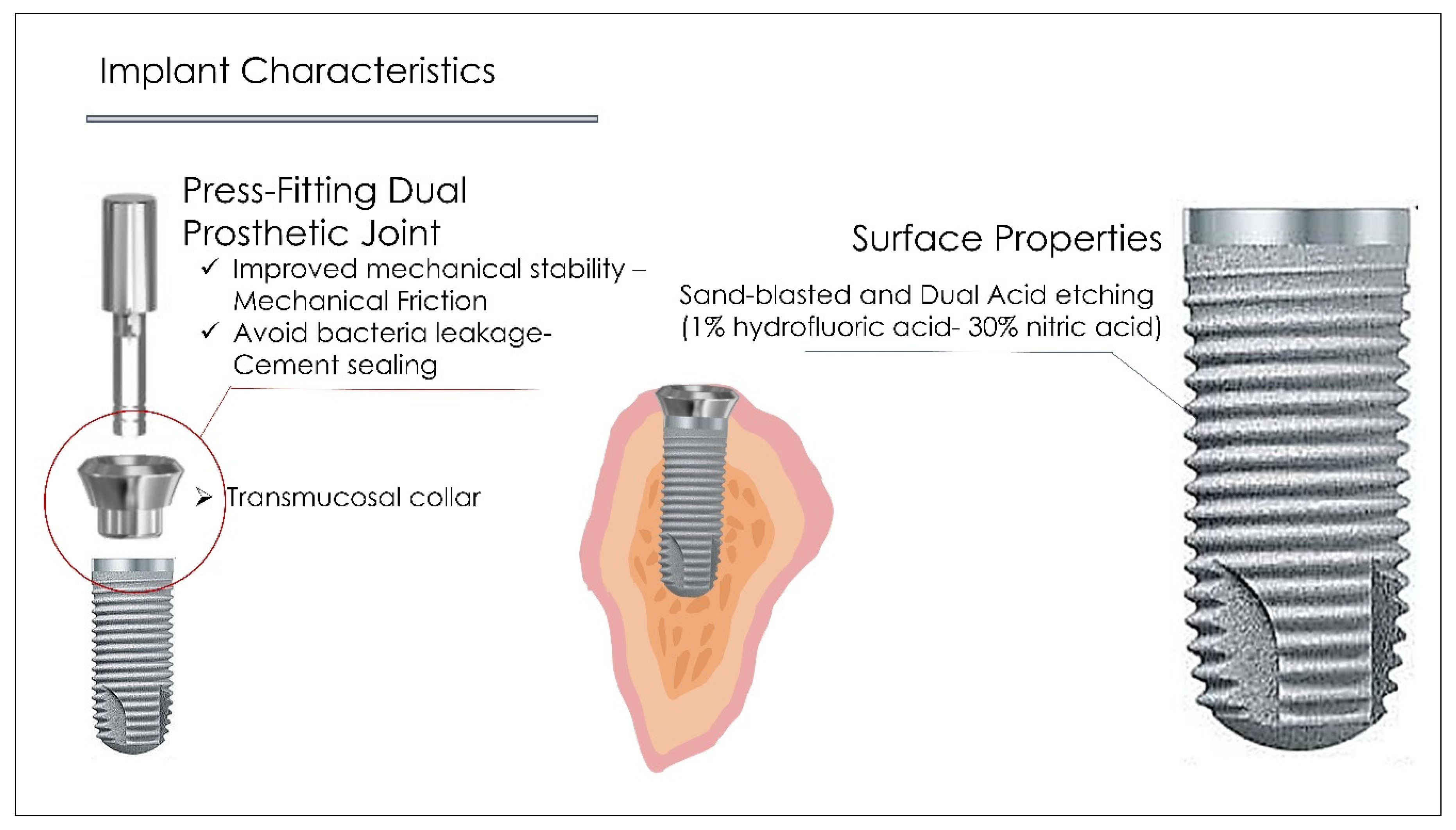
2.2. Dental Implant Characteristics
2.3. Systematic Literature Review
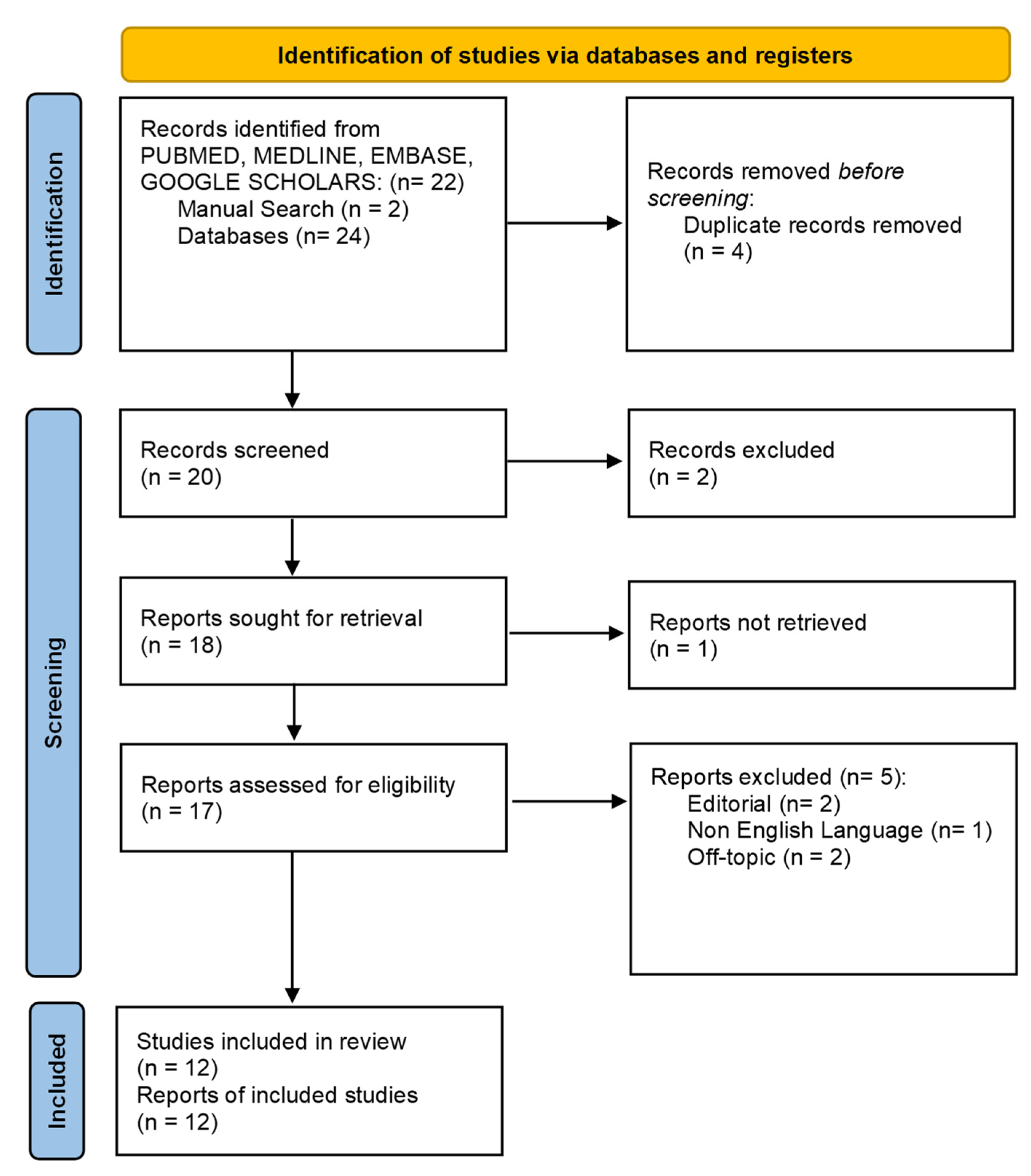
2.3.1. Screening Procedure
2.3.2. Inclusion and Exclusion Criteria
2.3.3. Paper Selection Assessment
2.3.4. Article Assessment
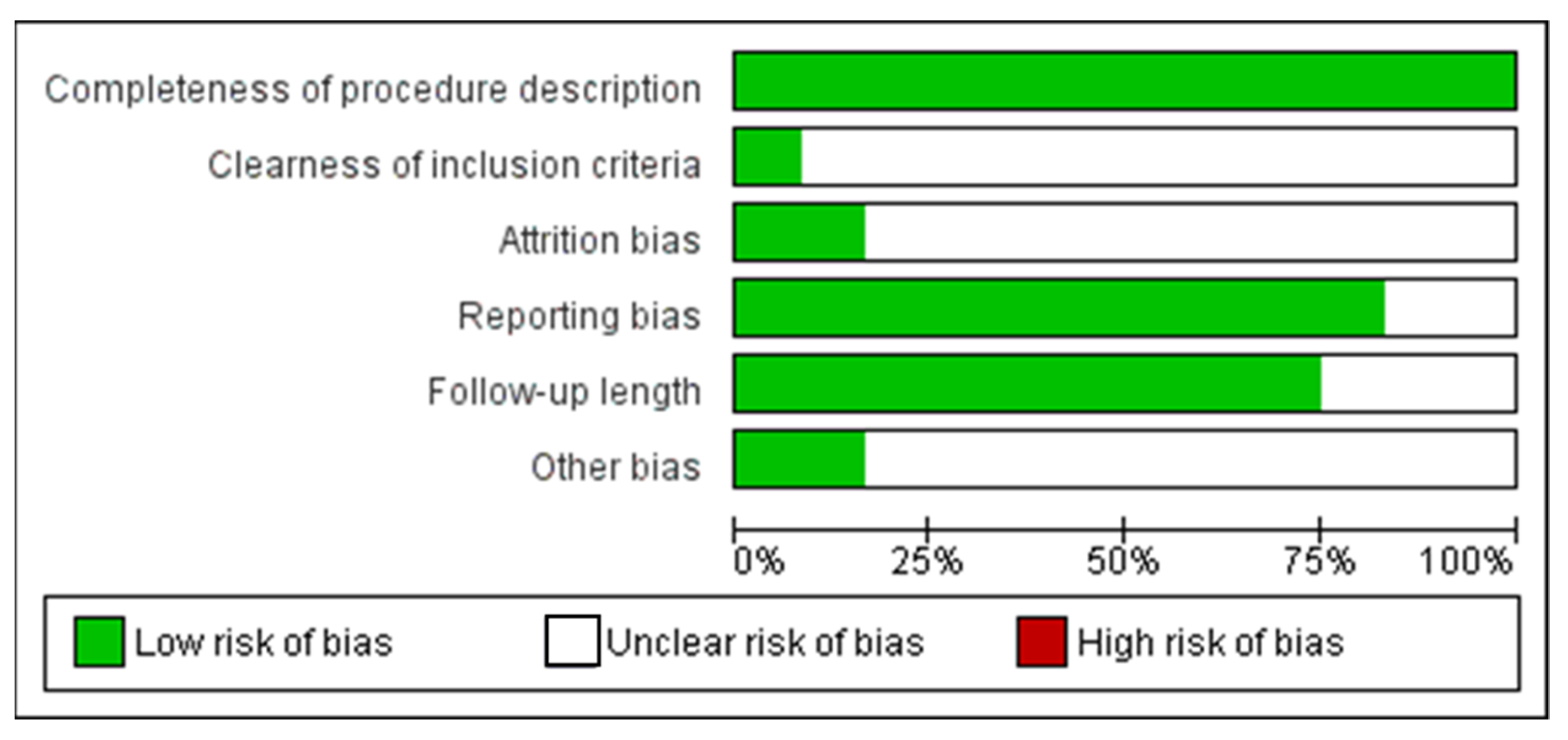
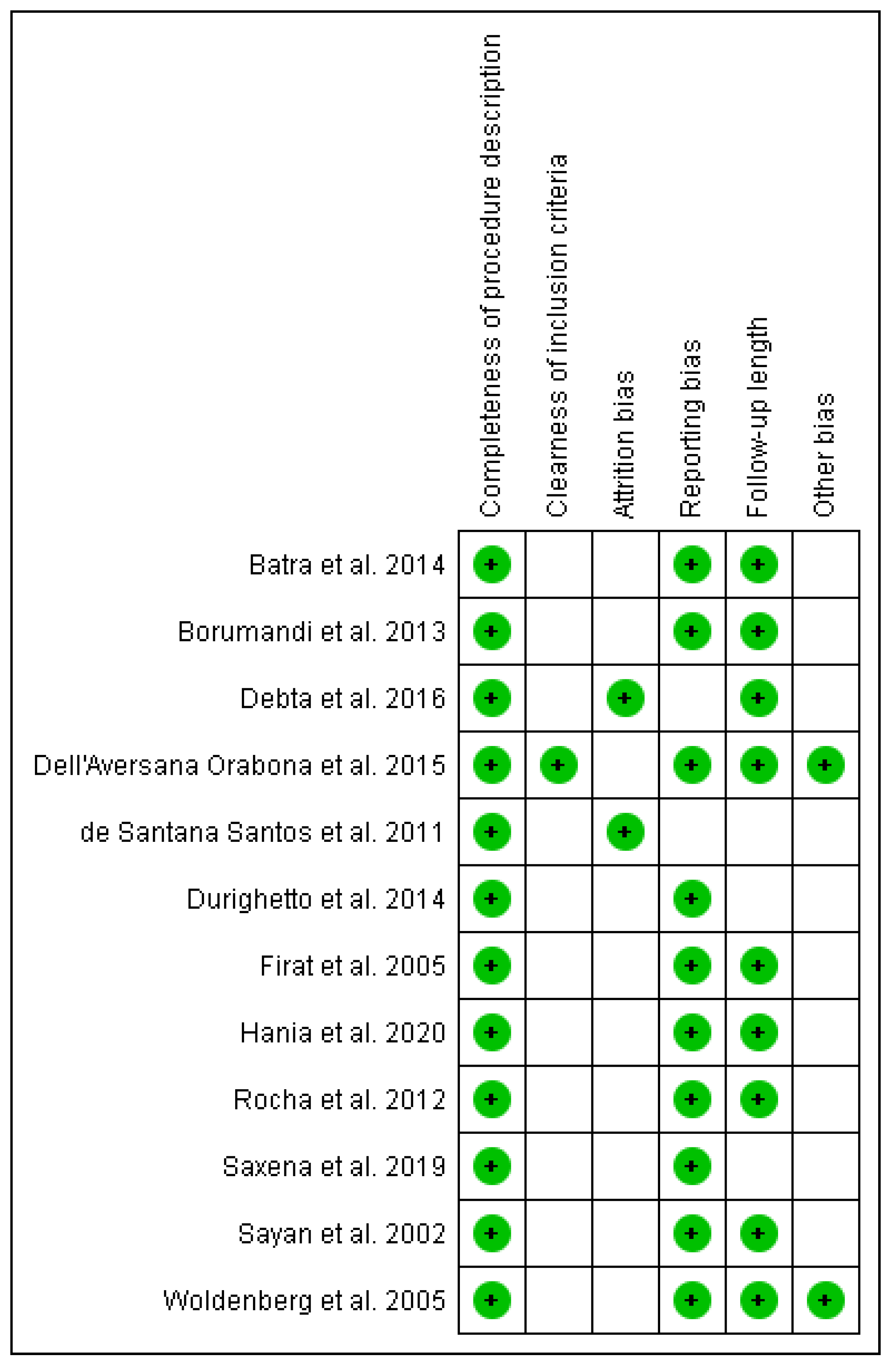
2.3.5. Risk of Bias Measurement
3. Results
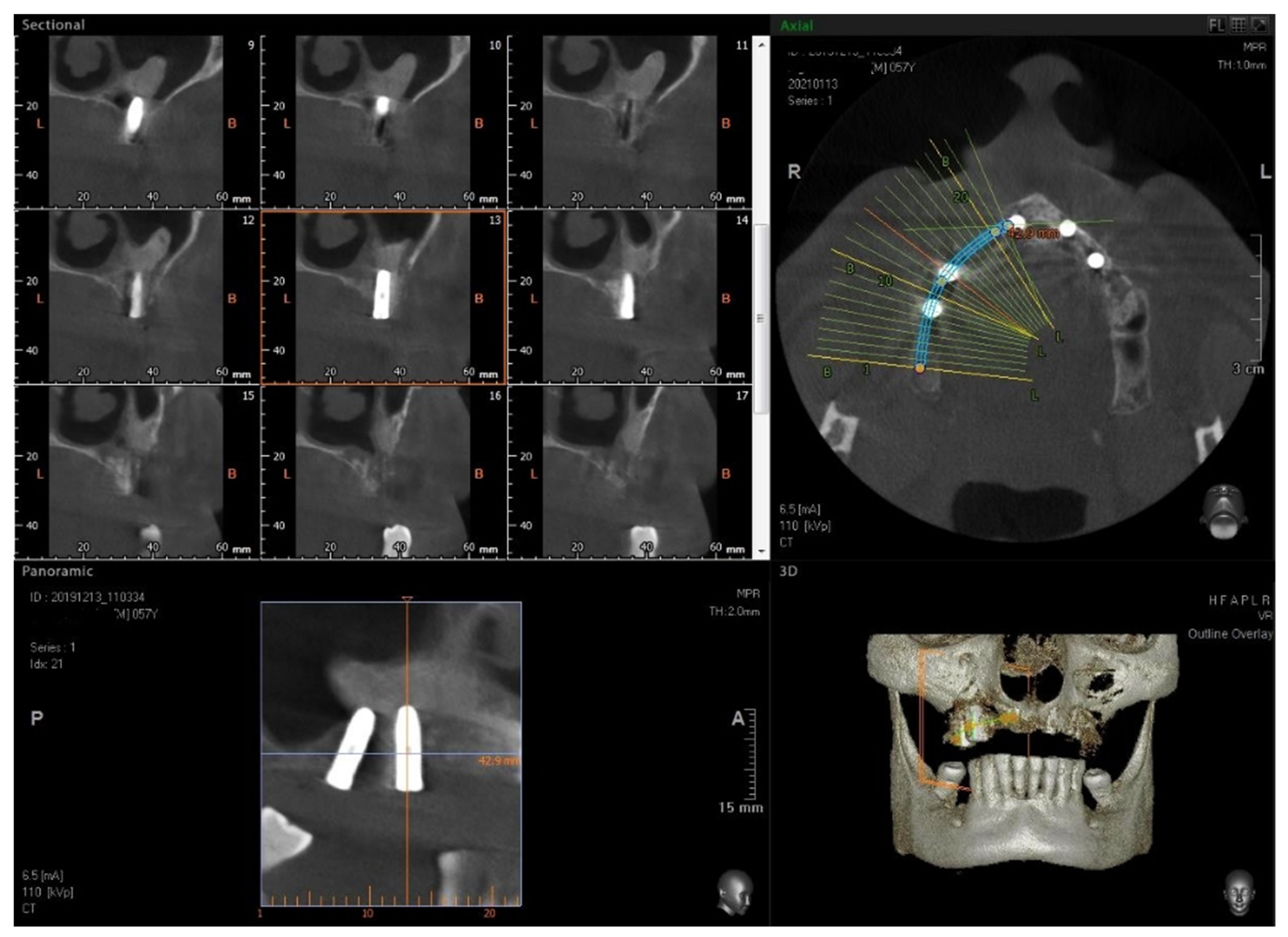
3.1. Surgical Procedure
3.2. Article Selection Process
3.3. Included Articles Characteristics
3.4. Risk of Bias Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Buser, D.; Janner, S.F.; Wittneben, J.-G.; Brägger, U.; Ramseier, C.A.; Salvi, G.E. 10-Year Survival and Success Rates of 511 Titanium Implants with a Sandblasted and Acid-Etched Surface: A Retrospective Study in 303 Partially Edentulous Patients. Clin. Implant. Dent. Relat. Res. 2012, 14, 839–851. [Google Scholar] [CrossRef] [PubMed]
- Albrektsson, T.; Berglundh, T.; Lindhe, J. Osseointegration: Historic Background and Current Concepts. Clin. Periodontol. Implant. Dent. 2003, 4, 809–820. [Google Scholar]
- Mijiritsky, E.; Barone, A.; Cinar, I.C.; Nagy, K.; Shacham, M. 3D Considerations and Outcomes of Immediate Single Implant Insertion and Provisionalization at the Maxillary Esthetic Zone: A Long-Term Retrospective Follow-Up Study of up to 18 Years. J. Clin. Med. 2021, 10, 4138. [Google Scholar] [CrossRef] [PubMed]
- Lorusso, F.; Noumbissi, S.; Francesco, I.; Rapone, B.; Khater, A.G.A.; Scarano, A. Scientific Trends in Clinical Research on Zirconia Dental Implants: A Bibliometric Review. Materials 2020, 13, 5534. [Google Scholar] [CrossRef]
- Albrektsson, T.; Chrcanovic, B.; Östman, P.-O.; Sennerby, L. Initial and Long-Term Crestal Bone Responses to Modern Dental Implants. Periodontology 2000 2017, 73, 41–50. [Google Scholar] [CrossRef]
- Naves, M.M.; Menezes, H.H.M.; Magalhães, D.; Ferreira, J.A.; Ribeiro, S.F.; de Mello, J.D.B.; Costa, H.L. Effect of Macrogeometry on the Surface Topography of Dental Implants. Int. J. Oral Maxillofac. Implants 2015, 30, 789–799. [Google Scholar] [CrossRef] [Green Version]
- Ryu, H.-S.; Namgung, C.; Lee, J.-H.; Lim, Y.-J. The Influence of Thread Geometry on Implant Osseointegration under Immediate Loading: A Literature Review. J. Adv. Prosthodont. 2014, 6, 547–554. [Google Scholar] [CrossRef] [Green Version]
- Velasco, E.; Monsalve-Guil, L.; Jimenez, A.; Ortiz, I.; Moreno-Muñoz, J.; Nuñez-Marquez, E.; Pegueroles, M.; Pérez, R.A.; Gil, F.J. Importance of the Roughness and Residual Stresses of Dental Implants on Fatigue and Osseointegration Behavior. In Vivo Study in Rabbits. J. Oral Implantol. 2016, 42, 469–476. [Google Scholar] [CrossRef]
- Wu-Yuan, C.D.; Eganhouse, K.J.; Keller, J.C.; Walters, K.S. Oral Bacterial Attachment to Titanium Surfaces: A Scanning Electron Microscopy Study. J. Oral Implantol. 1995, 21, 207–213. [Google Scholar]
- Scarano, A.; Piattelli, A.; Polimeni, A.; Di Iorio, D.; Carinci, F. Bacterial Adhesion on Commercially Pure Titanium and Anatase-Coated Titanium Healing Screws: An in Vivo Human Study. J. Periodontol. 2010, 81, 1466–1471. [Google Scholar] [CrossRef]
- Montegrotto Group for the Study of Peri-implant Disease; Canullo, L.; Schlee, M.; Wagner, W.; Covani, U. International Brainstorming Meeting on Etiologic and Risk Factors of Peri-Implantitis, Montegrotto (Padua, Italy), August 2014. Int. J. Oral Maxillofac. Implants 2015, 30, 1093–1104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zandim-Barcelos, D.L.; de Carvalho, G.G.; Sapata, V.M.; Villar, C.C.; Hämmerle, C.; Romito, G.A. Implant-Based Factor as Possible Risk for Peri-Implantitis. Braz. Oral Res. 2019, 33, e067. [Google Scholar] [CrossRef] [PubMed]
- Klotz, A.L.; Fobbe, H.; Rammelsberg, P.; Lorenzo Bermejo, J.; Kappel, S. Survival and Success of Tooth-Implant-Supported and Solely Implant-Supported Double-Crown-Retained Overdentures: A Prospective Study over a Period of up to 11 Years. Clin. Oral Implants Res. 2021, 32, 1425–1432. [Google Scholar] [CrossRef] [PubMed]
- Mavriqi, L.; Lorusso, F.; Conte, R.; Rapone, B.; Scarano, A. Zygomatic Implant Penetration to the Central Portion of Orbit: A Case Report. BMC Ophthalmol 2021, 21, 121. [Google Scholar] [CrossRef] [PubMed]
- Scarano, A.; Barros, R.R.M.; Iezzi, G.; Piattelli, A.; Novaes, A.B. Acellular Dermal Matrix Graft for Gingival Augmentation: A Preliminary Clinical, Histologic, and Ultrastructural Evaluation. J. Periodontol. 2009, 80, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Borges, F.L.; Dias, R.O.; Piattelli, A.; Onuma, T.; Gouveia Cardoso, L.A.; Salomão, M.; Scarano, A.; Ayub, E.; Shibli, J.A. Simultaneous Sinus Membrane Elevation and Dental Implant Placement without Bone Graft: A 6-Month Follow-up Study. J. Periodontol. 2011, 82, 403–412. [Google Scholar] [CrossRef] [PubMed]
- Bhalla, N.; Dym, H. Update on Maxillary Sinus Augmentation. Dent. Clin. N. Am. 2021, 65, 197–210. [Google Scholar] [CrossRef] [PubMed]
- Scarano, A.; Sinjari, B.; Murmura, G.; Lorusso, F. Neurosensory Disturbance of the Inferior Alveolar Nerve After 3025 Implant Placements. Implant Dent. 2017, 26, 735–743. [Google Scholar] [CrossRef] [PubMed]
- Schlund, M.; Meeus, J.; Politis, C.; Ferri, J. Management of Sinus Graft Infection-a Systematic Review. Int. J. Oral Maxillofac. Surg. 2022, 51, 690–698. [Google Scholar] [CrossRef] [PubMed]
- Minetti, E.; Celko, M.; Contessi, M.; Carini, F.; Gambardella, U.; Giacometti, E.; Santillana, J.; Beca Campoy, T.; Schmitz, J.H.; Libertucci, M.; et al. Implants Survival Rate in Regenerated Sites with Innovative Graft Biomaterials: 1 Year Follow-Up. Materials 2021, 14, 5292. [Google Scholar] [CrossRef] [PubMed]
- Inchingolo, F.; Dipalma, G.; Paduanelli, G.; De Oliveira, L.A.; Inchingolo, A.M.; Georgakopoulos, P.I.; Inchingolo, A.D.; Malcangi, G.; Athanasiou, E.; Fotopoulou, E.; et al. Computer-Based Quantification of an Atraumatic Sinus Augmentation Technique Using CBCT. J. Biol. Regul. Homeost. Agents 2019, 33, 31–39. [Google Scholar] [PubMed]
- Pjetursson, B.E.; Tan, W.C.; Zwahlen, M.; Lang, N.P. A Systematic Review of the Success of Sinus Floor Elevation and Survival of Implants Inserted in Combination with Sinus Floor Elevation. J. Clin. Periodontol. 2008, 35, 216–240. [Google Scholar] [CrossRef] [PubMed]
- Spinato, S.; Bernardello, F.; Galindo-Moreno, P.; Zaffe, D. Maxillary Sinus Augmentation by Crestal Access: A Retrospective Study on Cavity Size and Outcome Correlation. Clin. Oral Implants Res. 2015, 26, 1375–1382. [Google Scholar] [CrossRef] [PubMed]
- Stacchi, C.; Lombardi, T.; Ottonelli, R.; Berton, F.; Perinetti, G.; Traini, T. New Bone Formation after Transcrestal Sinus Floor Elevation Was Influenced by Sinus Cavity Dimensions: A Prospective Histologic and Histomorphometric Study. Clin. Oral Implants Res. 2018, 29, 465–479. [Google Scholar] [CrossRef] [PubMed]
- Scarano, A.; Degidi, M.; Iezzi, G.; Pecora, G.; Piattelli, M.; Orsini, G.; Caputi, S.; Perrotti, V.; Mangano, C.; Piattelli, A. Maxillary Sinus Augmentation With Different Biomaterials: A Comparative Histologic and Histomorphometric Study in Man. Implant Dent. 2006, 15, 197–207. [Google Scholar] [CrossRef] [PubMed]
- Vinci, R.; Teté, G.; Lucchetti, F.R.; Capparé, P.; Gherlone, E.F. Implant Survival Rate in Calvarial Bone Grafts: A Retrospective Clinical Study with 10 Year Follow-Up. Clin. Implant. Dent. Relat. Res. 2019, 21, 662–668. [Google Scholar] [CrossRef] [PubMed]
- Trimarchi, M.; Giordano Resti, A.; Vinciguerra, A.; Danè, G.; Bussi, M. Dacryocystorhinostomy: Evolution of Endoscopic Techniques after 498 Cases. Eur. J. Ophthalmol. 2020, 30, 998–1003. [Google Scholar] [CrossRef] [PubMed]
- Yacoub, M.-R.; Trimarchi, M.; Cremona, G.; Dal Farra, S.; Ramirez, G.A.; Canti, V.; Della Torre, E.; Baldini, M.; Pignatti, P.; Bussi, M.; et al. Are Atopy and Eosinophilic Bronchial Inflammation Associated with Relapsing Forms of Chronic Rhinosinusitis with Nasal Polyps? Clin. Mol. Allergy 2015, 13, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carini, F.; Longoni, S.; Simone, M.; Monai, D.; Saggese, V.; Porcaro, G. Central Osteoma of the Maxilla: Implant Rehabilitation with Immediate Loading in Fresh Extraction Socket. Ann. Stomatol. 2014, 5, 10. [Google Scholar]
- Nah, K.-S. Osteomas of the Craniofacial Region. Imaging Sci. Dent. 2011, 41, 107–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Association, W.M. World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. JAMA 2013, 310, 2191–2194. [Google Scholar]
- Agha, R.A.; Franchi, T.; Sohrabi, C.; Mathew, G.; Kerwan, A.; SCARE Group. The SCARE 2020 Guideline: Updating Consensus Surgical CAse REport (SCARE) Guidelines. Int. J. Surg. 2020, 84, 226–230. [Google Scholar] [CrossRef] [PubMed]
- Scarano, A.; Lorusso, F.; Arcangelo, M.; D’Arcangelo, C.; Celletti, R.; de Oliveira, P.S. Lateral Sinus Floor Elevation Performed with Trapezoidal and Modified Triangular Flap Designs: A Randomized Pilot Study of Post-Operative Pain Using Thermal Infrared Imaging. Int. J. Environ. Res. Public Health 2018, 15, 1277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Assenza, B.; Scarano, A.; Petrone, G.; Iezzi, G.; Thams, U.; San Roman, F.; Piattelli, A. Crestal Bone Remodeling in Loaded and Unloaded Implants and the Microgap: A Histologic Study. Implant Dent. 2003, 12, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Assenza, B.; Tripodi, D.; Scarano, A.; Perrotti, V.; Piattelli, A.; Iezzi, G.; D’Ercole, S. Bacterial Leakage in Implants with Different Implant-Abutment Connections: An in Vitro Study. J. Periodontol. 2012, 83, 491–497. [Google Scholar] [CrossRef] [PubMed]
- Scarano, A.; Assenza, B.; Inchingolo, F.; Mastrangelo, F.; Lorusso, F. New Implant Design with Midcrestal and Apical Wing Thread for Increased Implant Stability in Single Postextraction Maxillary Implant. Case Rep. Dent. 2019, 2019, 9529248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hania, M.; Sharif, M.O. Maxillary Sinus Osteoma: A Case Report and Literature Review. J. Orthod. 2020, 47, 240–244. [Google Scholar] [CrossRef] [PubMed]
- Saxena, S.; Ashwin, V.G.; Rajinikanth, D. A Sizeable Solitary Pedunculated Peripheral Osteoma of the Hard Palate: A Case Report. Indian J. Otolaryngol. Head Neck Surg. 2019, 71, 813–815. [Google Scholar] [CrossRef] [PubMed]
- Debta, P.; Debta, F.M.; Bussari, S.; Acharya, S.S.; Jeergal, V.A. Cancellous Osteoma of Maxilla: A Rare Case Report. J. Int. Soc. Prev. Community Dent. 2016, 6, 261–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Santana Santos, T.; Frota, R.; Martins-Filho, P.R.S.; Melo, A.R.; de Souza Andrade, E.S.; de Oliveira e Silva, E.D.; Avelar, R.L. Central Osteoma of the Maxilla with Involvement of Paranasal Sinus. J. Craniofac. Surg. 2011, 22, 589–591. [Google Scholar] [CrossRef] [PubMed]
- Durighetto, A.F.; de Moraes Ramos, F.M.; da Rocha, M.A.; da Cruz Perez, D.E. Peripheral Osteoma of the Maxilla: Report of a Case. Dentomaxillofac. Radiol. 2007, 36, 308–310. [Google Scholar] [CrossRef] [PubMed]
- Batra, N.; Batra, R.; Singh, G.; Gaur, A. Peripheral Osteoma of Maxilla: A Case Report. Natl. J. Maxillofac. Surg. 2014, 5, 240–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rocha, J.F.; Gonçales, A.G.B.; da Silva Sampieri, M.B.; da Silva, A.A.; Matsumoto, M.A.; Gonçales, E.S. Peripheral Osteoma of the Maxillary Sinus: A Case Report. Oral Maxillofac. Surg. 2012, 16, 315–319. [Google Scholar] [CrossRef] [PubMed]
- Firat, D.; Sirin, Y.; Bilgic, B.; Ozyuvaci, H. Large Central Osteoma of the Maxillary Antrum. Dentomaxillofac. Radiol. 2005, 34, 322–325. [Google Scholar] [CrossRef]
- Borumandi, F.; Lukas, H.; Yousefi, B.; Gaggl, A. Maxillary Sinus Osteoma: From Incidental Finding to Surgical Management. J. Oral Maxillofac. Pathol. 2013, 17, 318. [Google Scholar] [CrossRef] [Green Version]
- Dell’Aversana Orabona, G.; Salzano, G.; Iaconetta, G.; Piombino, P.; Ponzo, L.; Santella, A.; Astarita, F.; Solari, D.; Salzano, F.A.; Califano, L. Facial Osteomas: Fourteen Cases and a Review of Literature. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 1796–1802. [Google Scholar]
- Woldenberg, Y.; Nash, M.; Bodner, L. Peripheral Osteoma of the Maxillofacial Region. Diagnosis and Management: A Study of 14 Cases. Med. Oral Patol. Oral Cir. Bucal. 2005, 10 (Suppl. 2), E139–E142. [Google Scholar]
- Sayan, N.B.; Uçok, C.; Karasu, H.A.; Günhan, O. Peripheral Osteoma of the Oral and Maxillofacial Region: A Study of 35 New Cases. J. Oral Maxillofac. Surg. 2002, 60, 1299–1301. [Google Scholar] [CrossRef]
- Saratziotis, A.; Emanuelli, E. Osteoma of the Medial Wall of the Maxillary Sinus: A Primary Cause of Nasolacrimal Duct Obstruction and Review of the Literature. Case Rep. Otolaryngol. 2014, 2014, 348459. [Google Scholar] [CrossRef]
- Bhatt, G.; Gupta, S.; Ghosh, S.; Mohanty, S.; Kumar, P. Central Osteoma of Maxilla Associated with an Impacted Tooth: Report of a Rare Case with Literature Review. Head Neck Pathol. 2019, 13, 554–561. [Google Scholar] [CrossRef]
- Dalambiras, S.; Boutsioukis, C.; Tilaveridis, I. Peripheral Osteoma of the Maxilla: Report of an Unusual Case. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2005, 100, e19–e24. [Google Scholar] [CrossRef] [PubMed]
- Antohi, C.; Haba, D.; Caba, L.; Ciofu, M.L.; Drug, V.-L.; Bărboi, O.-B.; Dobrovăț, B.I.; Pânzaru, M.-C.; Gorduza, N.C.; Lupu, V.V.; et al. Novel Mutation in APC Gene Associated with Multiple Osteomas in a Family and Review of Genotype-Phenotype Correlations of Extracolonic Manifestations in Gardner Syndrome. Diagnostics 2021, 11, 1560. [Google Scholar] [CrossRef] [PubMed]
- Chan, H.-L.; Wang, H.-L. Sinus Pathology and Anatomy in Relation to Complications in Lateral Window Sinus Augmentation. Implant Dent. 2011, 20, 406–412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.J.; Lee, K.H.; Park, S.Y.; Kim, H.K. One-Stage Reconstruction for Midfacial Defect after Radical Tumor Resection. Clin. Exp. Otorhinolaryngol. 2012, 5, 53–56. [Google Scholar] [CrossRef]
- Adwani, D.; Bhattacharya, A.; Arora, R.S.; Soni, R.; Adwani, N. Resection and Reconstruction of Maxillary Class IIIc Defect in a Case of Adenoid Cystic Carcinoma: Cost-Sensitive Technique without Microvascular Grafts. Case Rep. Dent. 2013, 2013, 865010. [Google Scholar] [CrossRef]
- Mlouka, M.; Tlili, M.; Hamrouni, A.; Selmi, R.; Khanfir, F.; Khalfi, M.S.; Ben Amor, F. Lateral Maxillary Sinus Floor Elevation in the Presence of a Sinus Osteoma: A Case Report. Clin. Case Rep. 2021, 9, e04124. [Google Scholar] [CrossRef]
- Torkzaban, P.; Ziaei, N.; Tootiaee, B.; Khoshhal, M.; Vafaee, F.; Panahandeh, N. Effect of Implant-Abutment Connection Type on Stress Distribution in Peri-Implant Bone and Abutment Micromovement: A Three-Dimensional Finite Element Analysis. J. Long-Term Eff. Med. Implants 2019, 29, 113–124. [Google Scholar] [CrossRef]
- Goellner, M.; Schmitt, J.; Karl, M.; Wichmann, M.; Holst, S. The Effect of Axial and Oblique Loading on the Micromovement of Dental Implants. Int. J. Oral Maxillofac. Implants 2011, 26, 257–264. [Google Scholar]
- Olsson, M.; Urde, G.; Andersen, J.B.; Sennerby, L. Early Loading of Maxillary Fixed Cross-Arch Dental Prostheses Supported by Six or Eight Oxidized Titanium Implants: Results after 1 Year of Loading, Case Series. Clin. Implant Dent. Relat. Res. 2003, 5, 81–87. [Google Scholar] [CrossRef]
- Piattelli, A.; Scarano, A.; Piattelli, M.; Podda, G. Implant Periapical Lesions: Clinical, Histologic, and Histochemical Aspects. A Case Report. Int. J. Periodontics Restor. Dent. 1998, 18, 181–187. [Google Scholar]
- Scarano, A.; Di Domizio, P.; Petrone, G.; Iezzi, G.; Piattelli, A. Implant Periapical Lesion: A Clinical and Histologic Case Report. J. Oral Implantol. 2000, 26, 109–113. [Google Scholar] [CrossRef]
- Albrektsson, T.; Canullo, L.; Cochran, D.; De Bruyn, H. “Peri-Implantitis”: A Complication of a Foreign Body or a Man-Made “Disease”. Facts and Fiction: Peri-Implantitis: Facts and Fiction. Clin. Implant. Dent. Relat. Res. 2016, 18, 840–849. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Population\Patients | Intervention | Comparison | Outcomes |
|---|---|---|---|
| Patient group of interest? | What is the main intervention you wish to consider? | Is there an alternative intervention to compare? | What is the clinical outcome? |
| Subjects affected by maxillary sinus osteoma. | The intervention was total/partial lesion removal and rehabilitation procedure. | The comparison was performed with conservative and non-surgical approaches. | The complete/partial lesion removal did not produce a recurrence of the lesion. |
| Search Strategies | |
|---|---|
| Keywords | keyword search: ((maxilla *) AND (antrum OR Sinus) AND (central OR peripheral OR extraskeletal) AND Osteoma) |
| Databases | PubMed/Medline, EMBASE, Cochrane electronic databases |
| Author | Journal | Study Design | Age | Etiology | Position | Lesion (s) Size | Treatment Protocol | Post Operative Events | Recurrency | Subject (s) | Type | Study Findings |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Hania et al. [37] | J Orthod. | Case report | 15 years | Premature extraction of maxillary deciduous canines | Maxillary antrum | - | Lesion Removal/osteoplasty | Uneventful | - | One (1) male | peripheral osteoma | Trauma/dental extraction and osteoma correlation |
| Saxena et al. [38] | Indian J Otolaryngol Head Neck Surg | Case report | 38 years | - | Hard palate | 5 × 4 × 2 cm | Lesion Removal/osteoplasty | Uneventful | - | One (1) male | peripheral osteoma | Lesions usually managed conservatively; excepts symptomatic cases. |
| Debta et al. [39] | J Int Soc Prev Community Dent | Case report | 37 years | Posterior Maxilla/Antrum | 3 × 1.5 cm | Lesion Removal/osteoplasty | Uneventful | One (1) female | peripheral osteoma | The lesion removal is the elective treatment; the recurrence rate is very low. | ||
| de Santana Santos et al. [40] | J Craniofac Surg | Case report | 44 years | - | Maxillary antrum | - | Lesion Removal/osteoplasty | Uneventful | One (1) male | Central Osteoma | The traumatic factor could induce an endosteal osteoblasts activity and the development of central osteoma. | |
| Durighetto et al. [41] | Dentomaxillofac Radiol | Case report | 42 years | - | Maxillary alveolar process, maxillary sinus, | 3 cm diameter | Lesion Removal/osteoplasty | Small area of ulceration | One (1) male | peripheral osteoma | no recurrence of the lesion after 6 years | |
| Woldenberg et al. [47] | Med Oral Patol Oral CirBucal | Case series | range 13 to 79 years | Not determined | 9 cases Body mandible 3 Temporal Bone 1 Maxilla 1 Maxillary antrum | range 1.0 cm to 4.0 cm | Lesion Removal/osteoplasty | deformity, mucosal ulcer, limitation of ATM movement, sensitivity, and headache | - | Eight (8) Female; Six (6) male | peripheral osteoma | Mandibular osteomas may be a genetic marker for the development of colorectal carcinoma |
| Sayan et al. [48] | J Oral Maxillofac Surg | Retrospective study | range 14 to 58 years | Not determined | (a) frontal bone (28.57%), (b) mandible(22.85%) (c) maxilla (14.28%) | - | Lesion Removal/osteoplasty | - | Twenty-three (23) males, Twelve (12) females | peripheral osteoma | The complete surgical removal at the base where it unites with the cortical bone is necessary | |
| Batra et al. [42] | Natl J Maxillofac Surg | Case report | 32 years | - | Maxillary alveolar process, maxillary sinus, infraorbital rim, right piriform | 6.3 × 6.3 × 6.5 cm | Lesion Removal/osteoplasty | no sensory deficit and the involved teeth were not devitalized | One (1) female | peripheral osteoma | Some lesions likely to present as true neoplasm of bone; other lesions may be the alteration of bone as a response to trauma or infection | |
| Rocha et al. [43] | Oral Maxillofac Surg | Case report | 18 years | Not determined | Maxillary sinus | 3 cm diameter | Lesion Removal/osteoplasty | - | One (1) female | peripheral osteoma | Osteomas most frequently occur in the frontal and ethmoid sinuses, and are rare in the maxillary sinus | |
| Firat et al. [44] | Dentomaxillofac Radiol | Case report | 15 years | Not determined | Maxillary sinus | - | Lesion Removal/osteoplasty | Impacted teeth | - | One (1) male | peripheral osteoma | New research efforts must be made to enlighten particularly the unknown aetiology of osteoma formation |
| Borumandi et al. [45] | J Oral Maxillofac Pathol | Case report | 39 years | Not determined | Maxillary sinus | 2 cm diameter | Lesion Removal/osteoplasty | One (1) male | peripheral osteoma | The midface osteomas appear frequently in the frontoethmoidal sinuses | ||
| Dell’Aversana Orabona et al. [46] | Eur Rev Med Pharmacol | Case series | range 24–61 years | Not determined | (a) 3 cases mandibular angle (b) 7 subjects anterior body (c) 4 patients alveolar processes (d) 2 Maxillary lesions | range 1.0 to 3.8 cm | Lesion Removal/osteoplasty | (a) Nine patients out of the eleven (81.8%) facial swelling (b) 1 subject dysesthesia of the trigeminal nerve (7.14%) (c) 4 cases uneventful | - | Six (6) male; eight (8) female | peripheral osteoma | Craniofacial osteomas are more frequent in the mandible, with no predilection for any specific age range |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scarano, A.; Tartaglia, G.; Rapone, B.; Inchingolo, F.; Lorusso, F. Maxillary Sinus Osteoma as a Support for Dental Implant Associated to Sinus Augmentation Procedure: A Case Report and Literature Review. Appl. Sci. 2022, 12, 5435. https://doi.org/10.3390/app12115435
Scarano A, Tartaglia G, Rapone B, Inchingolo F, Lorusso F. Maxillary Sinus Osteoma as a Support for Dental Implant Associated to Sinus Augmentation Procedure: A Case Report and Literature Review. Applied Sciences. 2022; 12(11):5435. https://doi.org/10.3390/app12115435
Chicago/Turabian StyleScarano, Antonio, Gianluca Tartaglia, Biagio Rapone, Francesco Inchingolo, and Felice Lorusso. 2022. "Maxillary Sinus Osteoma as a Support for Dental Implant Associated to Sinus Augmentation Procedure: A Case Report and Literature Review" Applied Sciences 12, no. 11: 5435. https://doi.org/10.3390/app12115435