
Effects of Radial Extracorporeal Shock Wave Therapy in Reducing Pain in Patients with Temporomandibular Disorders: A Pilot Randomized Controlled Trial

 , ,
, ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Intervention
2.3. Outcome Measures
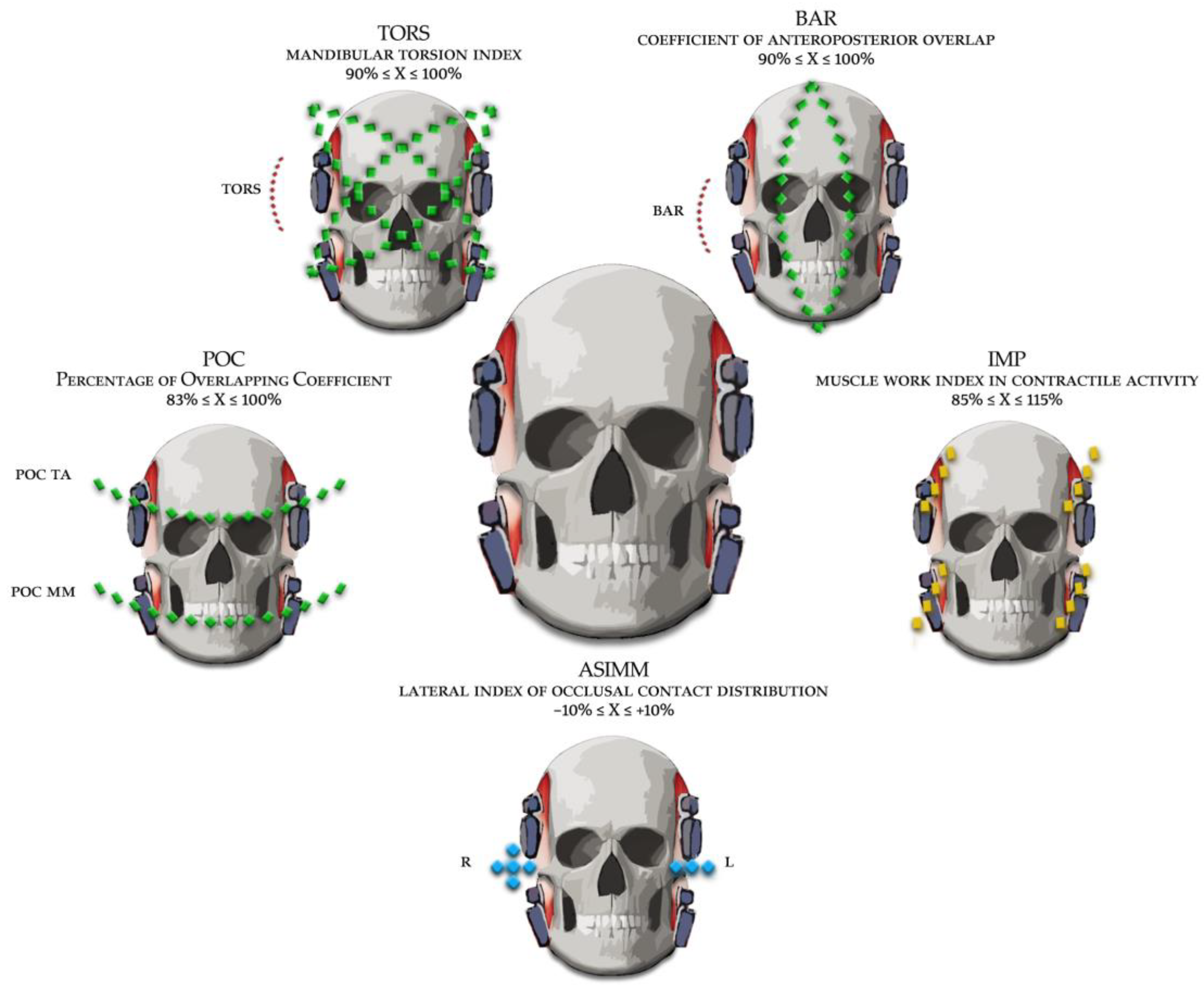
- POC (Percentage of Overlapping Coefficient), a symmetry index computed between the right and left temporalis (POC AT), and the right and left masseter muscles (POC MM). In details, the POC calculates the symmetry of activation between the right and left temporalis, and between the right and left masseter. The POC measure, expressed as percent, is the difference between the normalized (MVC) sEMG signal of the muscle considered. A normality range between 83% and 100% indicates a good symmetry.
- BAR: Occlusal centre of gravity (anterior/posterior), obtained by calculating the ratio between the activities of the pair of temporalis muscles and the pair of masseter muscles. When the temporalis muscles are predominant with respect to the masseters, the occlusal centre of gravity is anterior; conversely, when there is a predominance of the masseter muscles, the occlusal centre of gravity is placed in the posterior sectors of the mouth.
- TORS: Mandibular Torsion Index. It measures the horizontal mandibular torsion during occlusion. It is obtained by comparing the torque of the crossed muscle pairs: comparison between the torque of the right temporalis and the left masseter and between left temporalis and the right masseter.
- ASIM: Asymmetry index. It compares the activity of the right muscles (right AT and right MM) with the activity of the left muscles (left AT and left MM). A positive value indicates greater activation of the right side, conversely a negative value indicates greater activation of the left side. The normal condition varies between −10 and 10.
- IMP: Impact of total standardized muscle activity. The under the curve area of right and left AT and MM over time (5 s MVC). Reference value are between 85 and 115%.

2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Okeson, J.P. Orthodontic Therapy and Temporomandibular Disorders: Should the Orthodontist Even Care? Temporomandibular Disord. Orofac. Pain Separating Controv. Consens. 2009, 9, 15–30. [Google Scholar]
- Schiffman, E.; Ohrbach, R.; Truelove, E.; Look, J.; Anderson, G.; Goulet, J.-P.; List, T.; Svensson, P.; Gonzalez, Y.; Lobbezoo, F.; et al. Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: Recommendations of the International RDC/TMD Consortium Network* and Orofacial Pain Special Interest Group. J. Oral Facial Pain Headache 2014, 28, 6–27. [Google Scholar] [CrossRef] [PubMed]
- Skeie, M.S.; Frid, P.; Mustafa, M.; Aßmus, J.; Rosén, A. DC/TMD examiner protocol: Longitudinal evaluation on interexaminer reliability. Pain Res. Manag. 2018, 2018, 7474608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dubner, R.; Ohrbach, R.; Dworkin, S.F. The Evolution of TMD Diagnosis: Past, Present, Future. Proc. J. Dent. Res. 2016, 95, 1093–1101. [Google Scholar]
- Ahmad, M.; Hollender, L.; Anderson, Q.; Kartha, K.; Ohrbach, R.; Truelove, E.L.; John, M.T.; Schiffman, E.L. Research diagnostic criteria for temporomandibular disorders (RDC/TMD): Development of image analysis criteria and examiner reliability for image analysis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2009, 107, 844–860. [Google Scholar] [CrossRef] [Green Version]
- Wieckiewicz, M.; Smardz, J.; Martynowicz, H.; Wojakowska, A.; Mazur, G.; Winocur, E. Distribution of temporomandibular disorders among sleep bruxers and non-bruxers—A polysomnographic study. J. Oral Rehabil. 2020, 47, 820–826. [Google Scholar] [CrossRef]
- Manfredini, D.; Guarda-Nardini, L.; Winocur, E.; Piccotti, F.; Ahlberg, J.; Lobbezoo, F. Research diagnostic criteria for temporomandibular disorders: A systematic review of axis i epidemiologic findings. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2011, 112, 453–462. [Google Scholar] [CrossRef]
- Dubner, R.; Slade, G.D.; Ohrbach, R.; Greenspan, J.D.; Fillingim, R.B.; Bair, E.; Sanders, A.E.; Diatchenko, L.; Meloto, C.B.; Smith, S.; et al. Painful Temporomandibular Disorder: Decade of Discovery from OPPERA Studies. J. Dent. Res. 2016, 95, 1084–1092. [Google Scholar] [CrossRef] [Green Version]
- Diraçoglu, D.; Yildirim, N.K.; Saral, I.; Özkan, M.; Karan, A.; Özkan, S.; Aksoy, C. Temporomandibular dysfunction and risk factors for anxiety and depression. J. Back Musculoskelet. Rehabil. 2016, 29, 487–491. [Google Scholar] [CrossRef]
- Heft, M.W. Prevalence of TMJ Signs and Symptoms in the Elderly. Gerodontology 1984, 3, 125–130. [Google Scholar] [CrossRef]
- Kaimal, S.; Ahmad, M.; Kang, W.; Nixdorf, D.; Schiffman, E.L. Diagnostic accuracy of panoramic radiography and mri for detecting signs of tmj degenerative joint disease. Gen. Dent. 2018, 66, 34–40. [Google Scholar] [PubMed]
- Orhan, K.; Driesen, L.; Shujaat, S.; Jacobs, R.; Chai, X. Development and Validation of a Magnetic Resonance Imaging-Based Machine Learning Model for TMJ Pathologies. BioMed Res. Int. 2021, 2021, 6656773. [Google Scholar] [CrossRef] [PubMed]
- Montinaro, F.; Nucci, L.; d’Apuzzo, F.; Perillo, L.; Chiarenza, M.C.; Grassia, V. Oral nonsteroidal anti-inflammatory drugs as treatment of joint and muscle pain in temporomandibular disorders: A systematic review. CRANIO 2022, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Ferrillo, M.; Ammendolia, A.; Paduano, S.; Calafiore, D.; Marotta, N.; Migliario, M.; Fortunato, L.; Giudice, A.; Michelotti, A.; de Sire, A. Efficacy of rehabilitation on reducing pain in muscle-related temporomandibular disorders: A systematic review and meta-analysis of randomized controlled trials. J. Back Musculoskelet. Rehabil. 2022, 18, 1–16. [Google Scholar] [CrossRef]
- Singh, H.; Sunil, M.K.; Kumar, R.; Singla, N.; Dua, N.; Garud, S.R. Evaluation of TENS therapy and Placebo drug therapy in the management of TMJ pain disorders: A comparative study. J. Indian Acad. Oral Med. Radiol. 2014, 26, 139–144. [Google Scholar] [CrossRef]
- Madani, A.S.; Ahrari, F.; Nasiri, F.; Abtahi, M.; Tunér, J. Low-level laser therapy for management of TMJ osteoarthritis. Cranio-J. Craniomandib. Pract. 2014, 32, 38–44. [Google Scholar] [CrossRef]
- Deregibus, A.; Ferrillo, M.; Piancino, M.G.; Domini, M.C.; de Sire, A.; Castroflorio, T. Are occlusal splints effective in reducing myofascial pain in patients with muscle-related temporomandibular disorders? A randomized-controlled trial. Turk. J. Phys. Med. Rehabil. 2021, 67, 32–40. [Google Scholar] [CrossRef]
- Minervini, G.; Nucci, L.; Lanza, A.; Femiano, F.; Contaldo, M.; Grassia, V. Temporomandibular disc displacement with reduction treated with anterior repositioning splint: A 2-year clinical and magnetic resonance imaging (MRI) follow-up. J. Biol. Regul. Homeost. Agents 2020, 34, 151–160. [Google Scholar] [PubMed]
- Zhou, H.; Xue, Y.; Liu, P. Application of auriculotemporal nerve block and dextrose prolotherapy in exercise therapy of TMJ closed lock in adolescents and young adults. Head Face Med. 2021, 17, 11. [Google Scholar] [CrossRef]
- de Sire, A.; Marotta, N.; Ferrillo, M.; Agostini, F.; Sconza, C.; Lippi, L.; Respizzi, S.; Giudice, A.; Invernizzi, M.; Ammendolia, A. Oxygen-Ozone Therapy for Reducing Pro-Inflammatory Cytokines Serum Levels in Musculoskeletal and Temporomandibular Disorders: A Comprehensive Review. Int. J. Mol. Sci. 2022, 23, 2528. [Google Scholar] [CrossRef]
- Yan, Z.B.; Wan, Y.D.; Xiao, C.Q.; Li, Y.Q.; Zhang, Y.Y.; An, Y.; Xiong, X. Craniofacial Morphology of Orthodontic Patients with and without Temporomandibular Disorders: A Cross-Sectional Study. Pain Res. Manag. 2022, 2022, 9344028. [Google Scholar] [CrossRef] [PubMed]
- Bizzarro, M.; Generali, C.; Maietta, S.; Martorelli, M.; Ferrillo, M.; Flores-Mir, C.; Perillo, L. Association between 3D palatal morphology and upper arch dimensions in buccally displaced maxillary canines early in mixed dentition. Eur. J. Orthod. 2018, 40, 592–596. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Wu, J. Treatment of temporomandibular joint disorders by ultrashort wave and extracorporeal shock wave: A comparative study. Med. Sci. Monit. 2020, 26, e923461. [Google Scholar] [CrossRef] [PubMed]
- Marinaro, C.; Costantino, C.; D’esposito, O.; Barletta, M.; Indino, A.; de Scorpio, G.; Ammendolia, A. Synergic use of botulinum toxin injection and radial extracorporeal shockwave therapy in multiple sclerosis spasticity. Acta Biomed. 2021, 92, e2021076. [Google Scholar] [CrossRef]
- Ammendolia, A.; Marotta, N.; Demeco, A.; Marinaro, C.; Moggio, L.; Barletta, M.; Costantino, C. Effectiveness of radial shockwave therapy in calcific and non-calcific tendinopathy of the shoulder: A systematic review and meta-analysis. Muscles. Ligaments Tendons J. 2020, 10, 40–47. [Google Scholar] [CrossRef] [Green Version]
- Mattyasovszky, S.G.; Langendorf, E.K.; Ritz, U.; Schmitz, C.; Schmidtmann, I.; Nowak, T.E.; Wagner, D.; Hofmann, A.; Rommens, P.M.; Drees, P. Exposure to radial extracorporeal shock waves modulates viability and gene expression of human skeletal muscle cells: A controlled in vitro study. J. Orthop. Surg. Res. 2018, 13, 75. [Google Scholar] [CrossRef] [Green Version]
- de Sire, A.; Marotta, N.; Agostini, F.; Drago Ferrante, V.; Demeco, A.; Ferrillo, M.; Inzitari, M.T.; Pellegrino, R.; Russo, I.; Ozyemisci Taskiran, O.; et al. A Telerehabilitation Approach to Chronic Facial Paralysis in the COVID-19 Pandemic Scenario: What Role for Electromyography Assessment? J. Pers. Med. 2022, 12, 497. [Google Scholar] [CrossRef]
- Hugger, A.; Hugger, S.; Schindler, H.J. Surface electromyography of the masticatory muscles for application in dental practice. Current evidence and future developments. Int. J. Comput. Dent. 2008, 11, 81–106. [Google Scholar]
- Tecco, S.; Tetè, S.; D’Attilio, M.; Perillo, L.; Festa, F. Surface electromyographic patterns of masticatory, neck, and trunk muscles in temporomandibular joint dysfunction patients undergoing anterior repositioning splint therapy. Eur. J. Orthod. 2008, 30, 592–597. [Google Scholar] [CrossRef] [Green Version]
- De FelÍcio, C.M.; Sidequersky, F.V.; Tartaglia, G.M.; Sforza, C. Electromyographic standardized indices in healthy Brazilian young adults and data reproducibility. J. Oral Rehabil. 2009, 36, 577–583. [Google Scholar] [CrossRef]
- Ferrario, V.F.; Sforza, C.; Colombo, A.; Ciusa, V. An electromyographic investigation of masticatory muscles symmetry in normo-occlusion subjects. J. Oral Rehabil. 2000, 27, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Ferrario, V.F.; Tartaglia, G.M.; Galletta, A.; Grassi, G.P.; Sforza, C. The influence of occlusion on jaw and neck muscle activity: A surface EMG study in healthy young adults. J. Oral Rehabil. 2006, 33, 341–348. [Google Scholar] [CrossRef]
- Tartaglia, G.M.; Antonio Moreira Rodrigues da Silva, M.; Bottini, S.; Sforza, C.; Ferrario, V.F. Masticatory muscle activity during maximum voluntary clench in different research diagnostic criteria for temporomandibular disorders (RDC/TMD) groups. Man. Ther. 2008, 13, 434–440. [Google Scholar] [CrossRef] [PubMed]
- Widmalm, S.E.; Lee, Y.S.; McKay, D.C. Clinical use of qualitative electromyography in the evaluation of jaw muscle function: A practitioner’s guide. Cranio 2007, 25, 63–73. [Google Scholar] [CrossRef]
- Dworkin, S.F. Research diagnostic criteria for temporomandibular disorders: Current status & future relevance. J. Oral Rehabil. 2010, 37, 734–743. [Google Scholar] [CrossRef]
- Cuschieri, S. The CONSORT statement. Saudi J. Anaesth. 2019, 13, S27–S30. [Google Scholar] [CrossRef]
- Tecco, S.; Mummolo, S.; Marchetti, E.; Tetè, S.; Campanella, V.; Gatto, R.; Gallusi, G.; Tagliabue, A.; Marzo, G. SEMG activity of masticatory, neck, and trunk muscles during the treatment of scoliosis with functional braces. A longitudinal controlled study. J. Electromyogr. Kinesiol. 2011, 21, 885–892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tecco, S.; Baldini, A.; Mummolo, S.; Marchetti, E.; Giuca, M.R.; Marzo, G.; Gherlone, E.F. Frenulectomy of the tongue and the influence of rehabilitation exercises on the sEMG activity of masticatory muscles. J. Electromyogr. Kinesiol. 2015, 25, 619–628. [Google Scholar] [CrossRef]
- Di Giacomo, P.; Ferrato, G.; Serritella, E.; Polimeni, A.; Di Paolo, C. Muscular pattern in patients with temporomandibular joint disc displacement with reduction: An electromyographical assessment. Clin. Ter. 2020, 171, e414–e420. [Google Scholar] [CrossRef]
- Sacco, I.C.N.; Gomes, A.A.; Otuzi, M.E.; Pripas, D.; Onodera, A.N. A method for better positioning bipolar electrodes for lower limb EMG recordings during dynamic contractions. J. Neurosci. Methods 2009, 180, 133–137. [Google Scholar] [CrossRef]
- Demeco, A.; Marotta, N.; Moggio, L.; Pino, I.; Marinaro, C.; Barletta, M.; Petraroli, A.; Palumbo, A.; Ammendolia, A. Quantitative analysis of movements in facial nerve palsy with surface electromyography and kinematic analysis. J. Electromyogr. Kinesiol. 2021, 56, 102485. [Google Scholar] [CrossRef] [PubMed]
- Hermens, H.J.; Freriks, B.; Disselhorst-Klug, C.; Rau, G. Development of recommendations for SEMG sensors and sensor placement procedures. J. Electromyogr. Kinesiol. 2000, 10, 361–374. [Google Scholar] [CrossRef]
- de Sire, A.; Marotta, N.; Demeco, A.; Moggio, L.; Paola, P.; Marotta, M.; Iona, T.; Invernizzi, M.; Leigheb, M.; Ammendolia, A. Electromyographic assessment of anterior cruciate ligament injury risk in male tennis players: Which role for visual input? A proof-of-concept study. Diagnostics 2021, 11, 997. [Google Scholar] [CrossRef] [PubMed]
- Ferrario, V.F.; Sforza, C.; Tartaglia, G.M.; Dellavia, C. Immediate effect of a stabilization splint on masticatory muscle activity in temporomandibular disorder patients. J. Oral Rehabil. 2002, 29, 810–815. [Google Scholar] [CrossRef] [PubMed]
- Fuentes, A.D.; Sforza, C.; Miralles, R.; Ferreira, C.L.; Mapelli, A.; Lodetti, G.; Martin, C. Assessment of electromyographic activity in patients with temporomandibular disorders and natural mediotrusive occlusal contact during chewing and tooth grinding. Cranio-J. Craniomandib. Pract. 2017, 35, 152–161. [Google Scholar] [CrossRef]
- Tecco, S.; Cattoni, F.; Darvizeh, A.; Bosco, F.; Sanci, V.; Nota, A.; Gastaldi, G.; Felice Gherlone, E. Evaluation of masticatory muscle function using digital versus traditional techniques for mockup fabrication: A controlled prospective study. Appl. Sci. 2020, 10, 6013. [Google Scholar] [CrossRef]
- Fleckenstein, J.; Zaps, D.; Rüger, L.J.; Lehmeyer, L.; Freiberg, F.; Lang, P.M.; Irnich, D. Discrepancy between prevalence and perceived effectiveness of treatment methods in myofascial pain syndrome: Results of a cross-sectional, nationwide survey. BMC Musculoskelet. Disord. 2010, 11, 32. [Google Scholar] [CrossRef] [Green Version]
- Denneny, D.; Frawley, H.C.; Petersen, K.; McLoughlin, R.; Brook, S.; Hassan, S.; Williams, A.C. Trigger Point Manual Therapy for the Treatment of Chronic Noncancer Pain in Adults: A Systematic Review and Meta-analysis. Arch. Phys. Med. Rehabil. 2019, 100, 562–577. [Google Scholar] [CrossRef]
- Shah, J.P.; Phillips, T.M.; Danoff, J.V.; Gerber, L.H. An in vivo microanalytical technique for measuring the local biochemical milieu of human skeletal muscle. J. Appl. Physiol. 2005, 99, 1977–1984. [Google Scholar] [CrossRef] [Green Version]
- Lopez-Martos, R.; Gonzalez-Perez, L.M.; Ruiz-Canela-Mendez, P.; Urresti-Lopez, F.J.; Gutierrez-Perez, J.L.; Infante-Cossio, P. Randomized, double-blind study comparing percutaneous electrolysis and dry needling for the management of temporomandibular myofascial pain. Med. Oral Patol. Oral y Cir. Bucal 2018, 23, e454–e462. [Google Scholar] [CrossRef]
- Fernández-Carnero, J.; La Touche, R.; Ortega-Santiago, R.; Galan-del-Rio, F.; Pesquera, J.; Ge, H.Y.; Fernández-de-Las-Peñas, C. Short-term effects of dry needling of active myofascial trigger points in the masseter muscle in patients with temporomandibular disorders. Br. Dent. J. 2010, 209, 597. [Google Scholar] [CrossRef]
- Dymarek, R.; Halski, T.; Ptaszkowski, K.; Slupska, L.; Rosinczuk, J.; Taradaj, J. Extracorporeal shock wave therapy as an adjunct wound treatment: A systematic review of the literature. Ostomy Wound Manag. 2014, 60, 26–39. [Google Scholar]
- Contaldo, C.; Högger, D.C.; Khorrami Borozadi, M.; Stotz, M.; Platz, U.; Forster, N.; Lindenblatt, N.; Giovanoli, P. Radial pressure waves mediate apoptosis and functional angiogenesis during wound repair in ApoE deficient mice. Microvasc. Res. 2012, 84, 24–33. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.J.; Wang, F.S.; Yang, K.D.; Weng, L.H.; Hsu, C.C.; Huang, C.S.; Yang, L.C. Shock wave therapy induces neovascularization at the tendon-bone junction. A study in rabbits. J. Orthop. Res. 2003, 21, 984–989. [Google Scholar] [CrossRef]
- Wang, C.J.; Sun, Y.C.; Wong, T.; Hsu, S.L.; Chou, W.Y.; Chang, H.W. Extracorporeal shockwave therapy shows time-dependent chondroprotective effects in osteoarthritis of the knee in rats. J. Surg. Res. 2012, 178, 196–205. [Google Scholar] [CrossRef] [PubMed]
- Walewicz, K.; Taradaj, J.; Rajfur, K.; Ptaszkowski, K.; Kuszewski, M.T.; Sopel, M.; Dymarek, R. The effectiveness of radial extracorporeal shock wave therapy in patients with chronic low back pain: A prospective, randomized, single-blinded pilot study. Clin. Interv. Aging 2019, 14, 1859–1869. [Google Scholar] [CrossRef] [Green Version]
- Damian, M.; Zalpour, C. Trigger point treatment with radial shock waves in musicians with nonspecific shoulder-neck pain: Data from a special physio outpatient clinic for musicians. Med. Probl. Perform. Art. 2011, 26, 211–217. [Google Scholar] [CrossRef]
- Kesikburun, S.; Uran Şan, A.; Kesikburun, B.; Aras, B.; Yaşar, E.; Tan, A.K. Comparison of Ultrasound-Guided Prolotherapy Versus Extracorporeal Shock Wave Therapy in the Treatment of Chronic Plantar Fasciitis: A Randomized Clinical Trial. J. Foot Ankle Surg. 2021, 61, 48–52. [Google Scholar] [CrossRef]
- Manzotti, A.; Viganoni, C.; Lauritano, D.; Bernasconi, S.; Paparo, A.; Risso, R.; Nanussi, A. Evaluation of the stomatognathic system before and after osteopathic manipulative treatment in 120 healthy people by using surface electromyography. Int. J. Environ. Res. Public Health 2020, 17, 3250. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Group A (n = 8) | Group B (n = 7) | |
|---|---|---|
| Sociodemographic characteristics | ||
| Age, years | 28.50 ± 8.85 | 30.71 ± 8.98 |
| Gender, male n (%) | 2 (25.00%) | 1 (14.29%) |
| Clinical characteristics | ||
| Additional diagnosis n (%) | ||
| Migraine | 2 (25.00%) | 2 (28.57%) |
| Chronic tension-type headache | 1 (12.50%) | - |
| Between-Group Differences | ||||||
|---|---|---|---|---|---|---|
| Outcome | Group A (rESWT) | Group B (sham rESWT) | p value | RBC | 95%CI | |
| T0 VAS R | 4.71 ± 2.56 | 3.75 ± 1.71 | 0.631 | 0.21 | [−0.48, 0.74] | |
| T0 VAS L | 4.86 ± 1.57 | 3.75 ± 1.71 | 0.384 | −0.36 | [−0.81, 0.35] | |
| T1 VAS R | 1.72 ± 1.89 | 2.75 ± 1.71 | 0.040 * | −0.46 | [−0.85, 0.23] | |
| T1 VAS L | 1.29 ± 1.11 | 2.50 ± 1.29 | 0.033 * | −0.64 | [−0.91, −0.02] | |
| T2 VAS R | 1.71 ± 1.90 | 2.75 ± 1.71 | 0.292 | 0.43 | [−0.28, 0.83] | |
| T2 VAS L | 1.29 ± 1.11 | 2.50 ± 1.29 | 0.182 | −0.54 | [−0.87, 0.14] | |
| T3 VAS R | 1.00 ± 1.83 | 2.50 ± 1.29 | 0.031 * | −0.61 | [−0.89, 0.04] | |
| T3 VAS L | 0.86 ± 1.86 | 2.50 ± 1.29 | 0.032 * | −0.68 | [−0.92, −0.09] | |
| Intra-Group Differences | ||||||
| Group A (real rESWT plus physical therapy) | p value | MD | SE | |||
| T0 VAS R | 4.71 ± 2.56 | T1 VAS R | 1.71 ± 1.89 | 0.020 * | 3.00 | 0.59 |
| T1 VAS R | 1.71 ± 1.89 | T2 VAS R | 1.14 ± 1.46 | 0.452 | 0.57 | 0.85 |
| T2 VAS R | 1.71 ± 1.90 | T3 VAS R | 1.00 ± 1.83 | 0.064 | 0.71 | 0.92 |
| T0 VAS L | 4.86 ± 1.57 | T1 VAS L | 1.29 ± 1.11 | 0.021 * | 3.57 | 0.88 |
| T1 VAS L | 1.29 ± 1.11 | T2 VAS L | 1.29 ± 2.63 | 0.732 | 0.00 | 1.23 |
| T2 VAS L | 1.29 ± 1.11 | T3 VAS L | 0.86 ± 1.86 | 0.603 | 0.43 | 0.89 |
| Group B (sham rESWT plus physical therapy) | p value | MD | SE | |||
| T0 VAS R | 3.75 ± 1.71 | T1 VAS R | 2.75 ± 1.71 | 0.155 | 1.00 | 0.56 |
| T1 VAS R | 2.75 ± 1.71 | T2 VAS R | 2.25 ± 0.96 | 0.501 | 0.5 | 0.51 |
| T2 VAS R | 2.75 ± 1.71 | T3 VAS R | 2.50 ± 1.29 | 0.653 | 0.25 | 0.66 |
| T0 VAS L | 3.75 ± 1.71 | T1 VAS L | 2.50 ± 1.29 | 0.094 | 1.25 | 0.26 |
| T1 VAS L | 2.50 ± 1.29 | T2 VAS L | 2.25 ± 0.96 | 0.689 | 0.25 | 0.29 |
| T2 VAS L | 2.50 ± 1.29 | T3 VAS L | 2.50 ± 1.29 | 0.732 | 0.01 | 0.43 |
| Group A (rESWT) | Group B (Sham rESWT) | p Value | |
|---|---|---|---|
| POC TA T0 | 80.7 ± 8.1 | 81.1 ± 10.5 | 0.651 |
| POC TA T1 | 82.0 ± 9.8 | 78.6 ± 12.0 | 0.073 |
| POC TA T2 | 79.7 ± 14.8 | 75.1 ± 19.4 | 0.061 |
| POC TA T3 | 87.0 ± 2.0 | 84.3 ± 2.8 | 0.084 |
| POC MM T0 | 81.2 ± 10.2 | 80.9 ± 7.7 | 0.672 |
| POC MM T1 | 85.9 ± 8.9 | 81.3 ± 6.4 | 0.041 * |
| POC MM T2 | 84.8 ± 5.2 | 82.3 ± 3.6 | 0.331 |
| POC MM T3 | 84.2 ± 6.1 | 81.7 ± 6.8 | 0.103 |
| BAR T0 | 75.2 ± 19.8 | 73.7 ± 10.8 | 0.094 |
| BAR T1 | 80.5 ± 10.7 | 75.9 ± 11.9 | 0.066 |
| BAR T2 | 81.0 ± 11.7 | 63.9 ± 14.8 | 0.032 * |
| BAR T3 | 84.4 ± 4.9 | 67.5 ± 22.8 | 0.041 * |
| TORS T0 | 86.5 ± 5.5 | 89.9 ± 0.7 | 0.095 |
| TORS T1 | 87.8 ± 3.6 | 89.2 ± 2.8 | 0.238 |
| TORS T2 | 86.8 ± 7.2 | 84.4 ± 8.9 | 0.145 |
| TORS T3 | 89.4 ± 3.0 | 88.6 ± 3.0 | 0.621 |
| IMP T0 | 71.9 ± 28.9 | 87.2 ± 21.5 | 0.025 * |
| IMP T1 | 68.2 ± 20.2 | 80.3 ± 21.4 | 0.031 * |
| IMP T2 | 84.0 ± 19.0 | 74.5 ± 12.8 | 0.047 * |
| IMP T3 | 86.9 ± 14.0 | 77.9 ± 13.0 | 0.062 |
| ASIM T0 | −1.98 ± 13.9 | 8.72 ± 14.4 | 0.022 * |
| ASIM T1 | 2.35 ± 13.0 | 10.0 ± 15.4 | 0.021 * |
| ASIM T2 | 0.19 ± 8.1 | 4.96 ± 11.0 | 0.566 |
| ASIM T3 | 2.19 ± 9.5 | 7.16 ± 9.4 | 0.431 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marotta, N.; Ferrillo, M.; Demeco, A.; Drago Ferrante, V.; Inzitari, M.T.; Pellegrino, R.; Pino, I.; Russo, I.; de Sire, A.; Ammendolia, A. Effects of Radial Extracorporeal Shock Wave Therapy in Reducing Pain in Patients with Temporomandibular Disorders: A Pilot Randomized Controlled Trial. Appl. Sci. 2022, 12, 3821. https://doi.org/10.3390/app12083821
Marotta N, Ferrillo M, Demeco A, Drago Ferrante V, Inzitari MT, Pellegrino R, Pino I, Russo I, de Sire A, Ammendolia A. Effects of Radial Extracorporeal Shock Wave Therapy in Reducing Pain in Patients with Temporomandibular Disorders: A Pilot Randomized Controlled Trial. Applied Sciences. 2022; 12(8):3821. https://doi.org/10.3390/app12083821
Chicago/Turabian StyleMarotta, Nicola, Martina Ferrillo, Andrea Demeco, Vera Drago Ferrante, Maria Teresa Inzitari, Raffaello Pellegrino, Ilaria Pino, Ilaria Russo, Alessandro de Sire, and Antonio Ammendolia. 2022. "Effects of Radial Extracorporeal Shock Wave Therapy in Reducing Pain in Patients with Temporomandibular Disorders: A Pilot Randomized Controlled Trial" Applied Sciences 12, no. 8: 3821. https://doi.org/10.3390/app12083821