
Does the Behavior of Pediatric Patients towards Dental Treatment Influence the Pattern of Adjacent (Sound, Decayed, and Filled) Proximal Surfaces in Primary Molars?

 , , ,
, , ,
Abstract
:1. Introduction
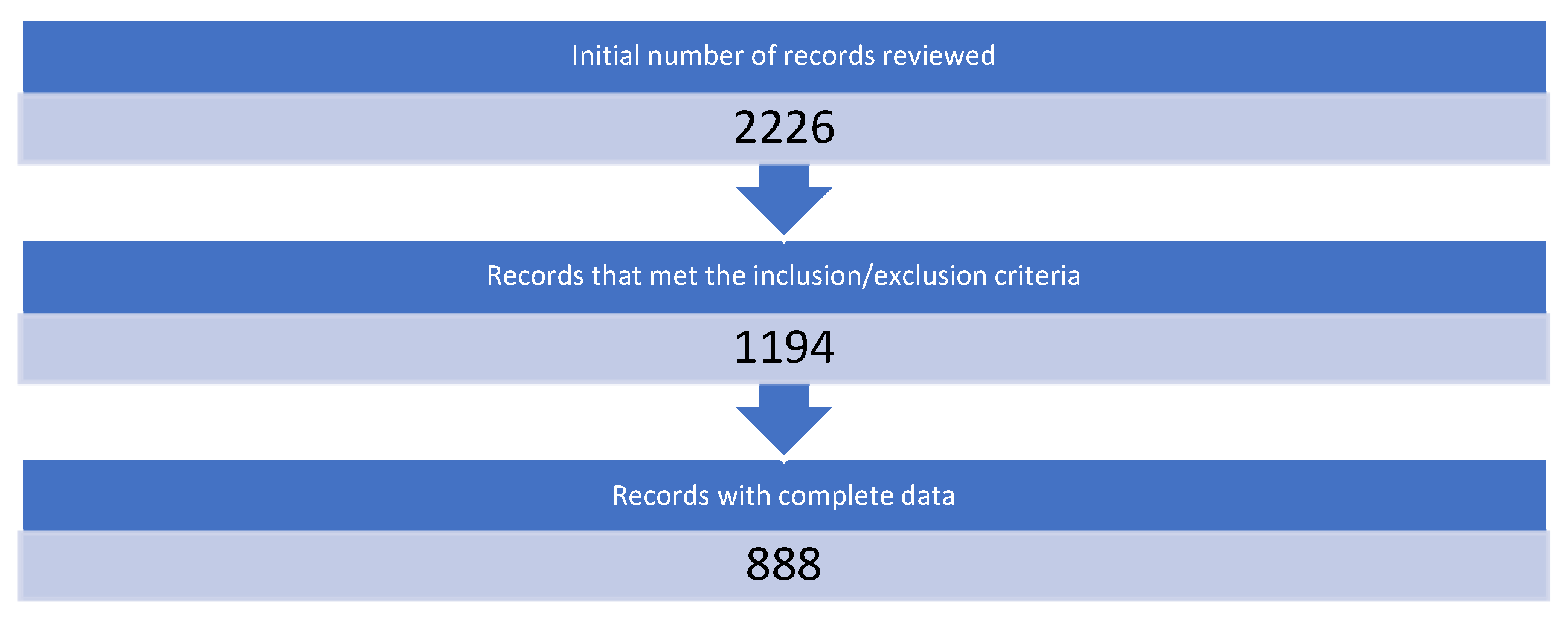
2. Materials and Methods
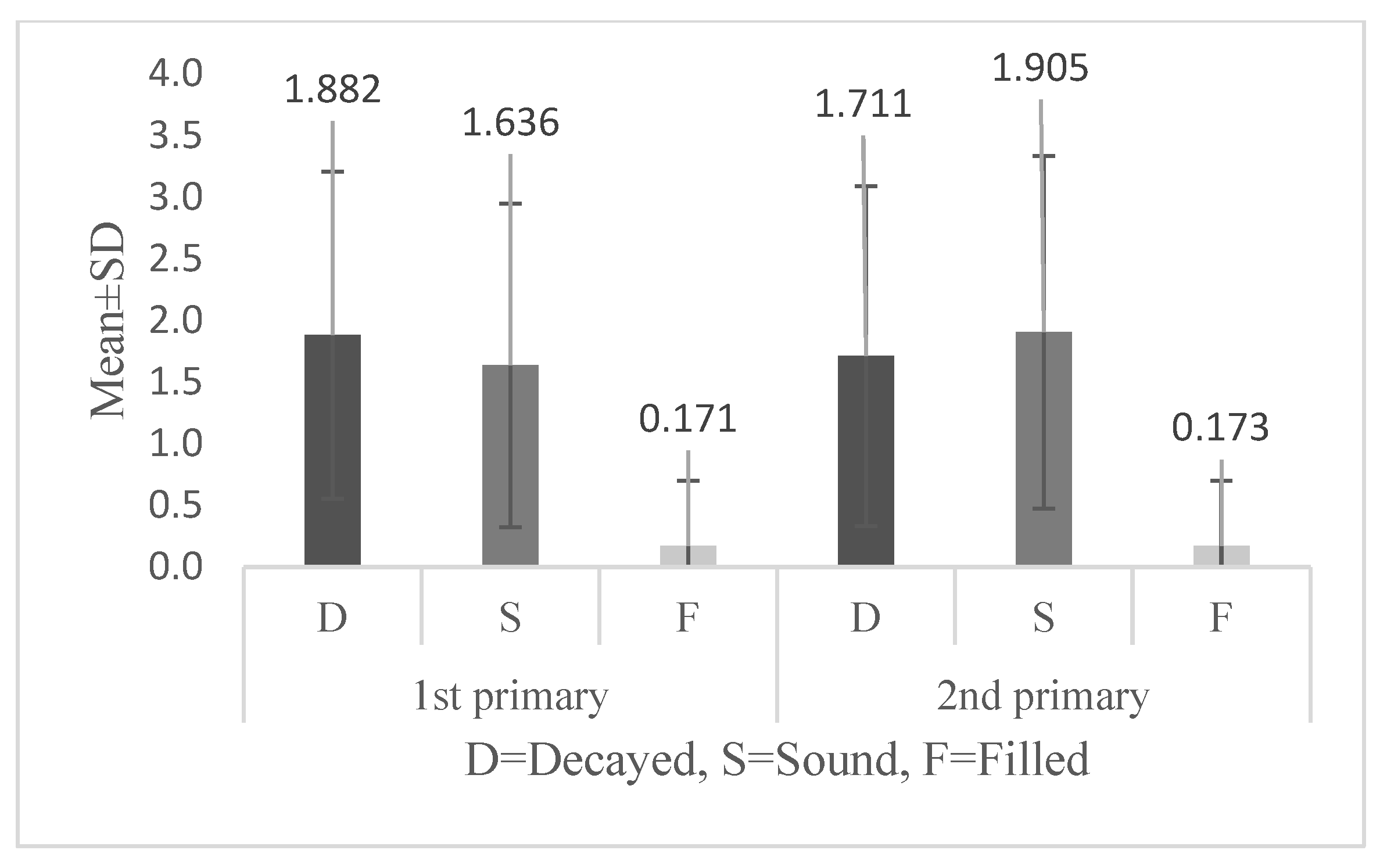
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Al-Meedani, L.A.; Al-Dlaigan, Y.H. Prevalence of dental caries and associated social risk factors among preschool children in Riyadh, Saudi Arabia. Pak. J. Med. Sci. Q. 2016, 32, 452. [Google Scholar] [CrossRef] [PubMed]
- Kathmandu, R.Y. The burden of restorative dental treatment for children in Third World countries. Int. Dent. J. 2002, 52, 1–9. [Google Scholar]
- Pitts, N.B.; Zero, D.T.; Marsh, P.D.; Ekstrand, K.; Weintraub, J.A.; Ramos-Gomez, F.; Tagami, J.; Twetman, S.; Tsakos, G.; Ismail, A. Dental Caries. Nat. Rev. Dis. Primers 2017, 3, 17030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farsi, N.; Merdad, L.; Mirdad, S. Caries Risk Assessment in Preschool Children in Saudi Arabia. Oral Heal. Prev Dent 2013, 11, 271–280. [Google Scholar]
- Farooqi, F.A.; Khabeer, A.; Moheet, I.; Khan, S.Q.; Farooq, I. Prevalence of dental caries in primary and permanent teeth and its relation with tooth brushing habits among schoolchildren in Eastern Saudi Arabia. Saudi Med, J. 2015, 36, 737–742. [Google Scholar] [CrossRef]
- Al-Ansari, A.A. Prevalence, severity, and secular trends of dental caries among various saudi populations: A literature review. Saudi, J. Med. Med. Sci. 2014, 2, 142. [Google Scholar] [CrossRef]
- Khan, N.B.; Al-Ghannam, N.A.; Al-Shammery, A.R.; Wyne, A.H. Caries in primary school children: Prevalence, severity and pattern in Al-Ahsa, Saudi Arabia. Saudi Dent. J. 2001, 13, 71–74. [Google Scholar]
- Al-Wazzan, K.A. Dental caries prevalence in 6–7 year-old schoolchildren in Riyadh region: A comparative study with the 1987–Oral Health Survey of Saudi Arabia Phase, I. Saudi Dent. J. 2004, 16, 54–61. [Google Scholar]
- Salwa, A.; Al, S. Dental caries prevalence among 12–14 year-old schoolchildren in Riyadh: A 14 year follow-up study of the oral health survey of Saudi Arabia phase, I. Saudi Dent. J. 2006, 18, 2–7. [Google Scholar]
- Amin, T.T.; Al-Abad, B.M. Oral hygiene practices, dental knowledge, dietary habits and their relation to caries among male primary school children in Al Hassa, Saudi Arabia. Int. J. Dent. Hyg. 2008, 6, 361–370. [Google Scholar] [CrossRef]
- Al Agili, D.E.; Niazy, H.A.; Pass, M.A. Prevalence and socioeconomic determinants of dental sealant use among schoolchildren in Saudi Arabia. East. Mediterr. Health J. 2012, 18, 1209–1216. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Saudi Arabia; Virajsilp, V.; Thearmontree, A.; Aryatawong, S.; Paiboonwarachat, D. Comparison of proximal caries detection in primary teeth between laser fluorescence and bitewing radiography. Pediatr. Dent. 2005, 27, 493–499. Available online: https://www.moh.gov.sa/en/Ministry/Projects/tooth-decay/Pages/default.aspx (accessed on 30 September 2021).
- Shimada, Y.; Burrow, M.F.; Araki, K.; Zhou, Y.; Hosaka, K.; Sadr, A.; Yoshiyama, M.; Miyazaki, T.; Sumi, Y.; Tagami, J. 3D imaging of proximal caries in posterior teeth using optical coherence tomography. Sci. Rep. 2020, 10, 15754. [Google Scholar] [CrossRef]
- Kamburoğlu, K.; Kolsuz, E.; Murat, S.; Yüksel, S.; Özen, T. Proximal caries detection accuracy using intraoral bitewing radiography, extraoral bitewing radiography and panoramic radiography. DMFR 2012, 41, 450–459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skudutyte-Rysstad, R.; Tveit, A.B.; Espelid, I.; Kopperud, S.E. Posterior composites and new caries on adjacent surfaces-any association? Longitudinal study with a split-mouth design. BMC Oral Health 2016, 16, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Afroughi, S.; Faghihzadeh, S.; Khaledi, M.; Ghandehari Motlagh, M. Effects of adjacent teeth on caries status of a deciduous tooth in 3–5 years-old children. Armaghane Danesh 2010, 15, 253–261. [Google Scholar]
- Yang, C.; Zou, H.; Zou, J. Analysis on dental uncooperative behaviors of the first-visit children in clinic. West China J. Stomatol. 2011, 29, 501–504. [Google Scholar]
- Ibrahim Masoud, B.D. Prevalence and distribution of caries in the primary dentition in a cosmopolitan Saudi population. Saudi Dent. J. 1995, 7, 23–28. [Google Scholar]
- Lee, C.Y.; Ting, C.C.; Wu, J.H.; Lee, K.T.; Chen, H.S.; Chang, Y.Y. Dental visiting behaviours among primary schoolchildren: Application of the health belief model. Int. J. Dent. Hyg. 2018, 16, e88–e95. [Google Scholar] [CrossRef]
- Buldur, B. Behavior management in pediatric dentistry: An overview and interpretation. Pesqui. Bras. Odontopediatr. Clin. Integr. 2019, 19, 4649. [Google Scholar] [CrossRef]
- Narayan, V.; Samuel, S. Appropriateness of various behavior rating scales used in pediatric dentistry: A Review. J. Glob. Oral Health 2020, 2, 112–117. [Google Scholar] [CrossRef] [Green Version]
- Lakhani, B.; Indushekar, K.R.; Garg, S.; Singh, N.; Tomer, E. Behavior assessment using frankl rating scale and identification of personality in pediatric dental operatory. J. Child Adolesc. Behav. 2017, 5, 1–5. [Google Scholar] [CrossRef]
- Elfrink, M.E.C.; Veerkamp, J.S.J.; Kalsbeek, H. Caries pattern in primary molars in Dutch 5-year-old children. Eur. Arch. Paediatr. Dent. 2006, 7, 236–240. [Google Scholar] [CrossRef]
- Gomez, S.S.; Emilson, C.-G.; Corvalan, G.C.; Quiroz, M. Efficacy of sealing the mesial surfaces of first permanent molars with respect to the status of the distal surfaces of the second primary molars in children at high caries-risk. Eur. Arch. Paediatr. Dent. 2013, 15, 65–73. [Google Scholar] [CrossRef]
- Academy of Pediatric Dentistry. Behavior guidance for the pediatric dental patient. In The Reference Manual of Pediatric Dentistry; American Academy of Pediatric Dentistry: Chicago, IL, USA, 2021; pp. 306–324. [Google Scholar]
- Panda, S.; Quadri, M.; Hadi, I.H.; Jably, R.M.; Hamzi, A.M.; Jafer, M.A. Does Dental Fear in Children Predict Untreated Dental Caries? An Analytical Cross-Sectional Study. Children 2021, 8, 382. [Google Scholar] [CrossRef] [PubMed]
- Alsadat, F.A.; El-Housseiny, A.A.; Alamoudi, N.M.; Elderwi, D.A.; Ainosa, A.M.; Dardeer, F.M. Dental fear in primary school children and its relation to dental caries. Niger. J. Clin. Pract. 2018, 21, 1454–1460. [Google Scholar] [PubMed]
- Dicker, R.C.; Coronado, F.; Koo, D.; Parrish, R.G. Principles of Epidemiology in Public Health Practice, An Introduction to Applied Epidemiology and Biostatistics, 3rd ed.; Department of Health and Human Services, Centers for Disease Control and Prevention (CDC), Office of Workforce and Career Development: Atlanta, GA, USA, 2006. [Google Scholar]
- Schroth, R.J.; Quiñonez, C.; Shwart, L.; Wagar, B. Brandon WagarTreating Early Childhood Caries Under General Anesthesia: A National Review of Canadian Data. J. Can. Dent. Assoc. 2016, 82, g20. [Google Scholar]
- Lee, J.Y.; Vann, W.F.; Roberts, M.W. A cost analysis of treating pediatric dental patients using general anesthesia versus conscious sedation. Pediatr. Dent. 2000, 22, 27–32. [Google Scholar]
- Bedard, A.D.; Gamble, J. Early childhood caries: Recurrence after comprehensive dental treatment under general anaesthesia. Eur. Arch. Paediatr. Dent. 2010, 11, 269–273. [Google Scholar]
- Patini, R.; Staderini, E.; Cantiani, M.; Camodeca, A.; Guglielmi, F.; Gallenzi, P. Dental anaesthesia for children–effects of a computer-controlled delivery system on pain and heart rate: A andomized clinical trial. Br. J. Oral Maxillofac. Surg. 2018, 56, 744–749. [Google Scholar] [CrossRef]
- Ashley, P.F.; Chaudhary, M.; Lourenço-Matharu, L. Sedation of children undergoing dental treatment. Cochrane Database Syst. Rev. 2018, 2018, CD003877. [Google Scholar] [CrossRef] [Green Version]
- American Academy of Pediatric Dentistry. Guideline on caries-risk assessment and management for infants, children, and adolescents. Pediatr. Dent. 2013, 35, E157–E164. [Google Scholar]
- Tickotsky, N.; Petel, R.; Araki, R.; Moskovitz, M. Caries Progression Rate in Primary Teeth: A Retrospective Study. J. Clin. Pediatr. Dent. 2017, 41, 358–361. [Google Scholar] [CrossRef] [PubMed]
- Reisine, S.T.; Psoter, W. Socioeconomic Status and Selected Behavioral Determinants as Risk Factors for Dental Caries. J. Dent. Educ. 2001, 65, 1009–1016. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| n (%) | |
|---|---|
| Gender n = 1194 Male Female | 634 (53.1) 560 (46.9) |
| Nationality n = 1194 Saudi Non-Saudi | 942 (78.9) 252 (21.1) |
| Medical History n = 1194 Healthy Non-healthy | 1087 (91.0) 107 (9.0) |
| Patient Behavior n = 888 Cooperative Non-cooperative | 710 (80.0) 178 (20.0) |
| Mean ± SD | |
| Age (years) n = 1194 | 7.51 ± 2.0 |
| 2nd Primary M Decay | 2nd Primary M Sound | 2nd Primary M Filled | |
|---|---|---|---|
| 1st Primary D Decay | 0.61 (p < 0.001) * | −0.44 (p < 0.001) | −0.19 (p < 0.001) |
| 1st Primary D Sound | −0.5 (p < 0.001) | 0.66 (p < 0.001) * | −0.14 (p < 0.001) |
| 1st Primary D Filled | −0.14 (p < 0.001) | −0.14 (p < 0.001) | 0.60 (p < 0.001) * |
| Variables Reference group | Univariate Regression Coefficient (95% CI) | Multivariate Regression Coefficient (95% CI) | |
|---|---|---|---|
| 2nd Primary Mesial Decay | |||
| Models for decayed surface adjacent to decayed | 1st Primary Distal Decay | 0.61 (0.59–0.68) * | 0.61 (0.58–0.69) * |
| Gender (female) | 0.00 (−0.15–0.16) | 0.02 (−0.08–0.21) | |
| Age | −0.04 (−0.07–0.01) | 0.06 (0.01–0.08) * | |
| Nationality (Saudi) | 0.05 (−0.35–0.03) | −0.02 (−0.25–0.11) | |
| Medical History (healthy) | −0.04 (−0.48–0.07) | −0.05 (−0.53–0.00) | |
| Patient Cooperation (non-cooperative) | 0.09 (0.07–0.52) * | 0.1 (0.16–0.53) * | |
| 2nd Primary Mesial Sound | |||
| Models for sound surface adjacent to sound | 1st Primary Distal Sound | 0.62 (0.62–0.72) * | 0.60 (0.61–0.72)* |
| Gender (female) | 0.00 (−0.16–0.17) | −0.02 (−0.20–0.09) | |
| Age | −0.07 (−0.9–−0.01) * | −0.05 (−0.08–0.00) | |
| Nationality (Saudi) | 0.03 (−0.9–0.31) | 0.02 (−0.1–0.27) | |
| Medical History (healthy) | 0.07 (0.05–0.62) * | −0.04 (−0.47–0.07) | |
| Patient Cooperation (non-cooperative) | −0.07 (−0.48–−0.02) * | −0.09 (−0.52–−0.15) * | |
| 2nd Primary Mesial Filled | |||
| Models for filled surface adjacent to filled | 1st Primary Distal Filled | 0.61 (−0.05–0.10) | 0.61 (0.55–0.66) * |
| Gender (female) | 0.001 (−0.06–0.06) | 0.00 (−0.06–0.06) | |
| Age | 0.03 (−0.01–0.02) | 0.01 (−0.01–0.02) | |
| Nationality (Saudi) | 0.01 (−0.06–0.09) | 0.00 (−0.06–0.07) | |
| Medical History (healthy) | 0.00 (−0.10–0.11) | 0.02 (−0.07–0.14) | |
| Patient Cooperation (non-cooperative) | 0.01 (−0.08–0.11) | 0.01 (−0.05–0.09) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bakhurji, E.; Alagil, J.; Almulhim, H.; Alfuhaid, R.; Alqanas, S.; Al-Khalifa, K.S. Does the Behavior of Pediatric Patients towards Dental Treatment Influence the Pattern of Adjacent (Sound, Decayed, and Filled) Proximal Surfaces in Primary Molars? Appl. Sci. 2022, 12, 1910. https://doi.org/10.3390/app12041910
Bakhurji E, Alagil J, Almulhim H, Alfuhaid R, Alqanas S, Al-Khalifa KS. Does the Behavior of Pediatric Patients towards Dental Treatment Influence the Pattern of Adjacent (Sound, Decayed, and Filled) Proximal Surfaces in Primary Molars? Applied Sciences. 2022; 12(4):1910. https://doi.org/10.3390/app12041910
Chicago/Turabian StyleBakhurji, Eman, Jumana Alagil, Hussah Almulhim, Raghad Alfuhaid, Sarah Alqanas, and Khalifa S. Al-Khalifa. 2022. "Does the Behavior of Pediatric Patients towards Dental Treatment Influence the Pattern of Adjacent (Sound, Decayed, and Filled) Proximal Surfaces in Primary Molars?" Applied Sciences 12, no. 4: 1910. https://doi.org/10.3390/app12041910