
Assessment of Fit on Ten Screw-Retained FrameworksRealized through Digital Full-Arch Implant Impression

 ,
,
Abstract
:1. Introduction
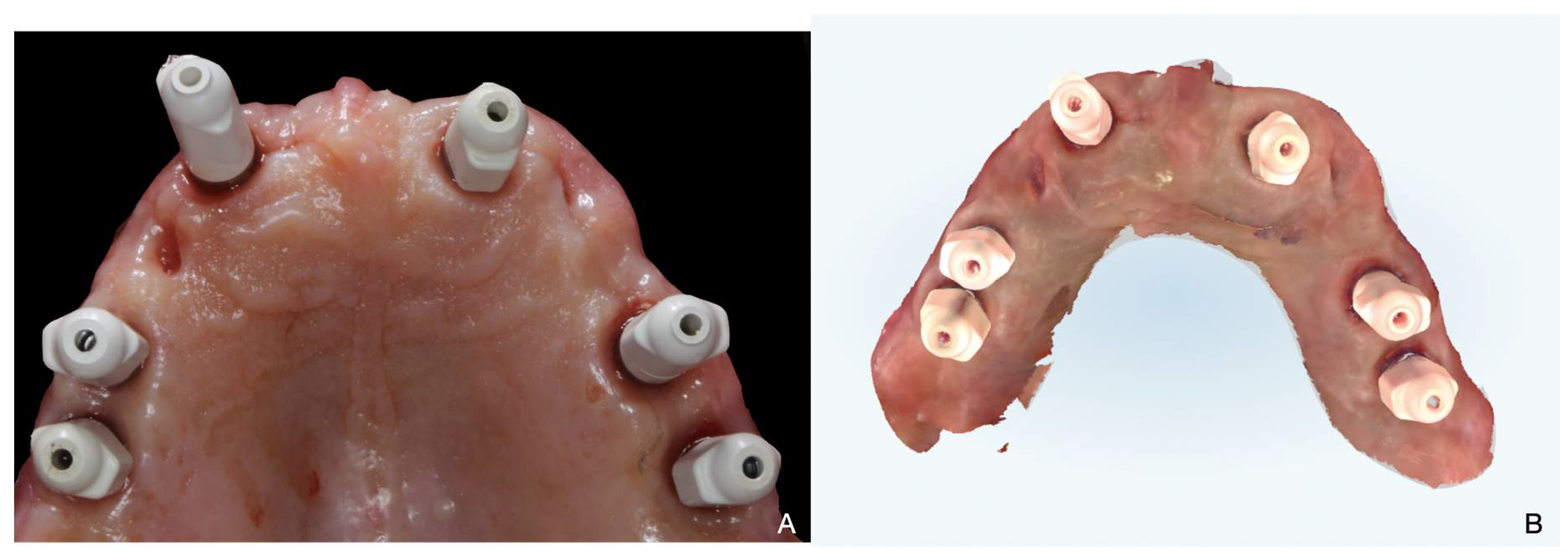
2. Materials and Methods
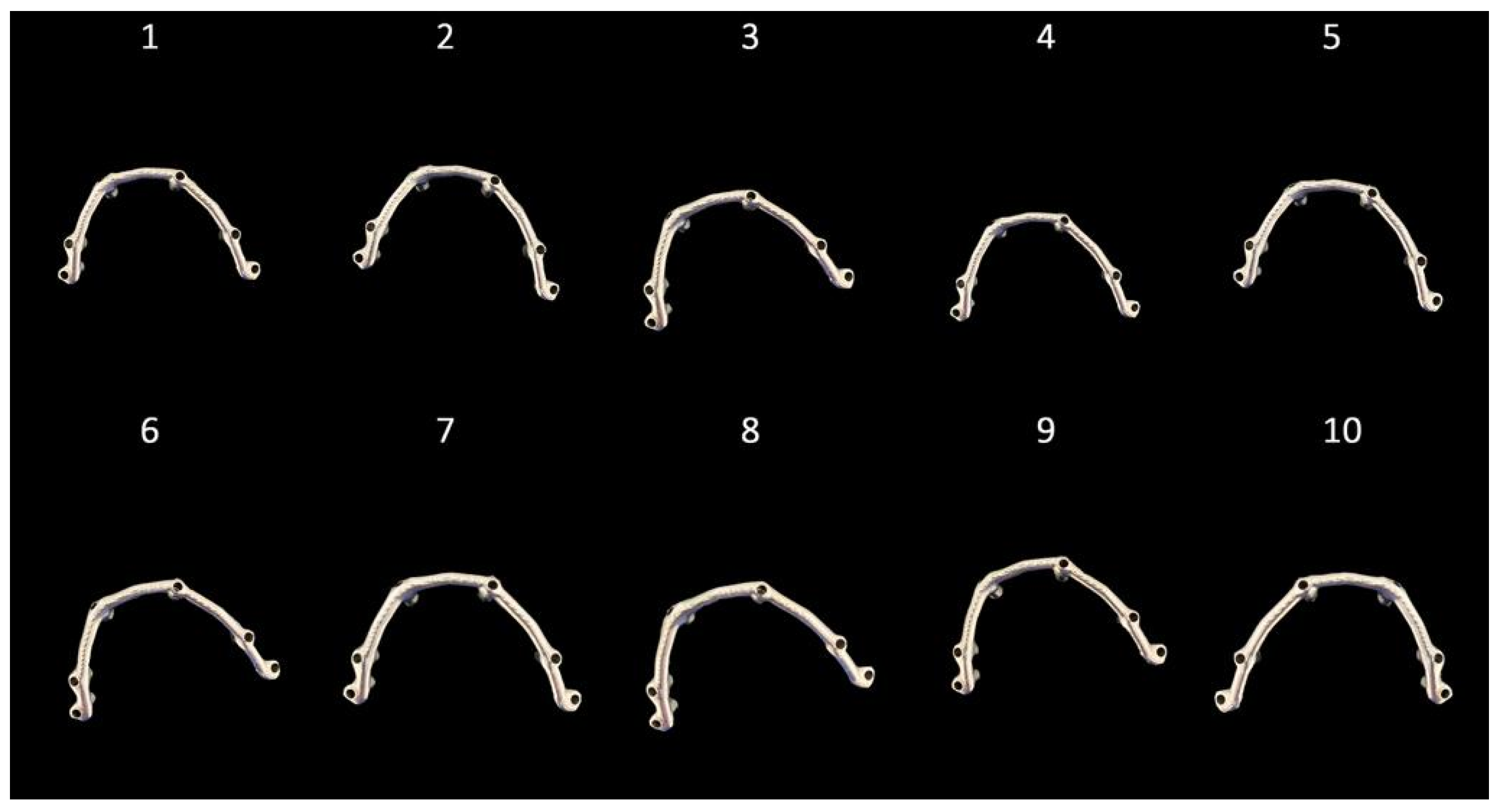
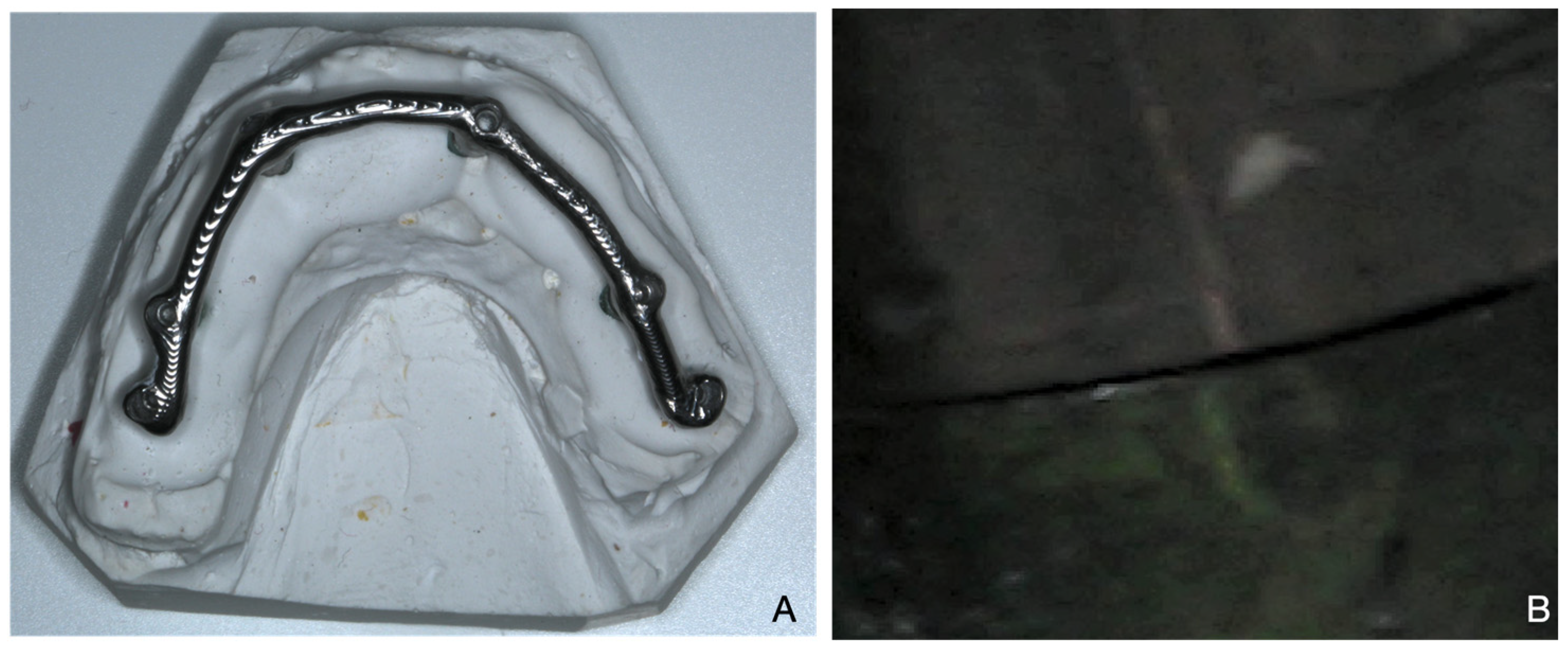
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chochlidakis, K.M.; Papaspyridakos, P.; Geminiani, A.; Chen, C.J.; Feng, I.J.; Ercoli, C. Digital versus conventional impressions for fixed prosthodontics: A systematic review and meta-analysis. J. Prosthet. Dent. 2016, 116, 184–190. [Google Scholar] [CrossRef]
- Granata, S.; Giberti, L.; Vigolo, P.; Stellini, E.; Di Fiore, A. Incorporating a facial scanner into the digital workflow: A dental technique. J. Prosthet. Dent. 2020, 123, 781–785. [Google Scholar] [CrossRef]
- Di Fiore, A.; Vigolo, P.; Graiff, L.; Stellini, E. Digital vs Conventional Workflow for Screw-Retained Single-Implant Crowns: A Comparison of Key Considerations. Int. J. Prosthodont. 2018, 31, 577–579. [Google Scholar] [CrossRef]
- Malaguti, G.; Rossi, R.; Marziali, B.; Esposito, A.; Bruno, G.; Dariol, C.; Di Fiore, A. In vitro evaluation of prosthodontic impression on natural dentition: A comparison between traditional and digital techniques. Oral. Implantol. (Rome) 2017, 14, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Di Fiore, A.; Monaco, C.; Brunello, G.; Granata, S.; Stellini, E.; Yilmaz, B. Automatic Digital Design of the Occlusal Anatomy of Monolithic Zirconia Crowns Compared to Dental Technicians’ Digital Waxing: A Controlled Clinical Trial. J. Prosthodont. 2021, 30, 104–110. [Google Scholar] [CrossRef]
- Ceruso, F.M.; Barnaba, P.; Mazzoleni, S.; Ottria, L.; Gargari, M.; Zuccon, A.; Bruno, G.; Di Fiore, A. Implant-abutment connections on single crowns: A systematic review. Oral. Implantol. (Rome) 2017, 10, 349–353. [Google Scholar] [CrossRef] [PubMed]
- Di Fiore, A.; Meneghello, R.; Graiff, L.; Savio, G.; Vigolo, P.; Monaco, C.; Stellini, E. Full arch digital scanning systems performances for implant-supported fixed dental prostheses: A comparative study of 8 intraoral scanners. J. Prosthodont. Res. 2019, 63, 396–403. [Google Scholar] [CrossRef] [PubMed]
- Mangano, F.G.; Admakin, O.; Bonacina, M.; Lerner, H.; Rutkunas, V.; Mangano, C. Trueness of 12 intraoral scanners in the full-arch implant impression: A comparative in vitro study. BMC Oral. Health 2020, 20, 263. [Google Scholar] [CrossRef] [PubMed]
- Bilmenoglu, C.; Cilingir, A.; Geckili, O.; Bilhan, H.; Bilgin, T. In vitro comparison of trueness of 10 intraoral scanners for implant-supported complete-arch fixed dental prostheses. J. Prosthet. Dent. 2020, 124, 755–760. [Google Scholar] [CrossRef]
- Çakmak, G.; Yilmaz, H.; Treviño, A.; Kökat, A.M.; Yilmaz, B. The effect of scanner type and scan body position on the accuracy of complete-arch digital implant scans. Clin. Implant. Dent. Relat. Res. 2020, 22, 533–541. [Google Scholar] [CrossRef]
- Mizumoto, R.M.; Yilmaz, B.; McGlumphy, E.A., Jr.; Seidt, J.; Johnston, W.M. Accuracy of different digital scanning techniques and scan bodies for complete-arch implant-supported prostheses. J. Prosthet. Dent. 2020, 123, 96–104. [Google Scholar] [CrossRef] [Green Version]
- Mizumoto, R.M.; Alp, G.; Özcan, M.; Yilmaz, B. The effect of scanning the palate and scan body position on the accuracy of complete-arch implant scans. Clin. Implant. Dent. Relat. Res. 2019, 21, 987–994. [Google Scholar] [CrossRef] [PubMed]
- Mennito, A.S.; Evans, Z.P.; Nash, J.; Bocklet, C.; Lauer, K.A.; Bacro, T.; Cayouette, M.; Ludlow, M.; Renne, W.G. Evaluation of the trueness and precision of complete arch digital impressions on a human maxilla using seven different intraoral digital impression systems and a laboratory scanner. J. Esthet. Restor. Dent. 2019, 31, 369–377. [Google Scholar] [CrossRef] [PubMed]
- Monaco, C.; Arena, A.; Pallotti, G.; di Fiore, A.; Scheda, L. Digital bar prototype technique for full-arch rehabilitation on implants. J. Am. Dent. Assoc. 2019, 150, 549–555. [Google Scholar] [CrossRef] [PubMed]
- Di Fiore, A.; Meneghello, R.; Savio, G.; Sivolella, S.; Katsoulis, J.; Stellini, E. In Vitro Implant Impression Accuracy Using a New Photopolymerizing SDR Splinting Material. Clin. Implant. Dent. Relat. Res. 2015, 17 (Suppl. S2), e721–e729. [Google Scholar] [CrossRef] [PubMed]
- Adell, R.; Eriksson, B.; Lekholm, U.; Brånemark, P.; Jemt, T. Long-term follow-up study of osseointegrated implants in the treatment of totally edentulous jaws. Int. J. Oral. Maxillofac. Implants 1990, 5, 347–359. [Google Scholar]
- Jemt, T. Failures and complications in 391 consecutively inserted fixed prostheses supported by Brånemark implant in the edentulous jaw: A study of treatment from the time of prostheses placement to the first annual check-up. Int. J. Oral. Maxillofac. Implants 1991, 6, 270–276. [Google Scholar]
- Gherlone, E.; Capparé, P.; Vinci, R.; Ferrini, F.; Gastaldi, G.; Crespi, R. Conventional Versus Digital Impressions for “All-on-Four” Restorations. Int. J. Oral. Maxillofac. Implants 2016, 31, 324–330. [Google Scholar] [CrossRef]
- Cappare, P.; Sannino, G.; Minoli, M.; Montemezzi, P.; Ferrini, F. Conventional versus Digital Impressions for Full Arch Screw-Retained Maxillary Rehabilitations: A Randomized Clinical Trial. Int. J. Environ. Res. Public. Health 2019, 16, 829. [Google Scholar] [CrossRef] [Green Version]
- Chochlidakis, K.; Papaspyridakos, P.; Tsigarida, A.; Romeo, D.; Chen, Y.W.; Natto, Z.; Ercoli, C. Digital Versus Conventional Full-Arch Implant Impressions: A Prospective Study on 16 Edentulous Maxillae. J. Prosthodont. 2020, 29, 281–286. [Google Scholar] [CrossRef]
- Abduo, J.; Bennani, V.; Waddell, N.; Lyons, K.; Swain, M. Assessing the fit of implant fixed prostheses: A critical review. Int. J. Oral. Maxillofac. Implants 2010, 25, 506–515. [Google Scholar] [PubMed]
- Jemt, T. In vivo measurements of precision of fit involving implant supported prostheses in the edentulous jaw. Int. J. Oral. Maxillofac. Implants 1996, 11, 151–158. [Google Scholar] [PubMed]
- Kan, J.Y.; Rungcharassaeng, K.; Bohsali, K.; Goodacre, C.J.; Lang, B.R. Clinical methods for evaluating implant framework fit. J. Prosthet. Dent. 1999, 81, 7–13. [Google Scholar] [CrossRef]
- Pesce, P.; Pera, F.; Setti, P.; Menini, M. Precision and Accuracy of a Digital Impression Scanner in Full-Arch Implant Rehabilitation. Int. J. Prosthodont. 2018, 31, 171–175. [Google Scholar] [CrossRef] [PubMed]
- Yanase, R.; Binon, P.; Jemt, T.; Gulbransen, H.; Parel, S. How do you test a cast framework fit for a full-arch fixed implant supported prosthesis? Int. J. Oral. Maxillofac. Implants 1994, 9, 469–474. [Google Scholar]
- Di Fiore, A.; De Francesco, M.; Monaco, C.; Stocco, E.; Vigolo, P.; Stellini, E. Comparison of accuracy of single crowns generated from digital and conventional impressions: An in vivo controlled trial. J. Osseointegr. 2019, 11, 107–112. [Google Scholar]
- Ferrini, F.; Sannino, G.; Chiola, C.; Capparé, P.; Gastaldi, G.; Gherlone, E.F. Influence of Intra-Oral Scanner (I.O.S.) on The Marginal Accuracy of CAD/CAM Single Crowns. Int. J. Environ. Res. Public. Health 2019, 16, 544. [Google Scholar] [CrossRef] [Green Version]
- Menini, M.; Setti, P.; Pera, F.; Pera, P.; Pesce, P. Accuracy of multi-unit implant impression: Traditional techniques versus a digital procedure. Clin. Oral. Investig. 2018, 22, 1253–1262. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Framework | Implant 1 (μm) | Implant 2 (μm) | Implant 3 (μm) | Implant 4 (μm) | Implant 5 (μm) | Implant 6 (μm) | Mean (μm) | SD |
|---|---|---|---|---|---|---|---|---|
| 1 | 35 | 33 | 44 | 45 | 38 | 33 | 38 | 5 |
| 2 | 43 | 39 | 46 | 51 | 44 | 41 | 44 | 4 |
| 3 | 35 | 33 | 42 | 45 | 36 | 38 | 38 | 5 |
| 4 | 38 | 35 | 36 | 33 | 33 | 35 | 35 | 2 |
| 5 | 40 | 39 | 48 | 44 | 38 | 37 | 41 | 4 |
| 6 | 28 | 31 | 39 | 41 | 33 | 30 | 34 | 5 |
| 7 | 30 | 32 | 39 | 51 | 37 | 33 | 37 | 8 |
| 8 | 31 | 31 | 44 | 41 | 29 | 30 | 34 | 6 |
| 9 | 32 | 34 | 41 | 40 | 37 | 36 | 37 | 3 |
| 10 | 44 | 38 | 40 | 53 | 43 | 45 | 44 | 5 |
| Mean | 35 | 34 | 42 | 45 | 37 | 36 | ||
| SD | 5 | 3 | 4 | 6 | 4 | 5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Francesco, M.; Stellini, E.; Granata, S.; Mazzoleni, S.; Ludovichetti, F.S.; Monaco, C.; Di Fiore, A. Assessment of Fit on Ten Screw-Retained FrameworksRealized through Digital Full-Arch Implant Impression. Appl. Sci. 2021, 11, 5617. https://doi.org/10.3390/app11125617
De Francesco M, Stellini E, Granata S, Mazzoleni S, Ludovichetti FS, Monaco C, Di Fiore A. Assessment of Fit on Ten Screw-Retained FrameworksRealized through Digital Full-Arch Implant Impression. Applied Sciences. 2021; 11(12):5617. https://doi.org/10.3390/app11125617
Chicago/Turabian StyleDe Francesco, Maurizio, Edoardo Stellini, Stefano Granata, Sergio Mazzoleni, Francesco Saverio Ludovichetti, Carlo Monaco, and Adolfo Di Fiore. 2021. "Assessment of Fit on Ten Screw-Retained FrameworksRealized through Digital Full-Arch Implant Impression" Applied Sciences 11, no. 12: 5617. https://doi.org/10.3390/app11125617