Clinical Role of Newly Developed ALBI and mALBI Grades for Treatment of Hepatocellular Carcinoma


1
Gastroenterology Center, Ehime Prefectural Central Hospital, Kasuga-cho 83, Ehime 790-0024, Japan
2
Department of Nursing, Gifu Kyoritsu University, Gifu 503-8550, Japan
*
Author to whom correspondence should be addressed.
Appl. Sci. 2020, 10(20), 7178; https://doi.org/10.3390/app10207178
Submission received: 2 September 2020
/
Revised: 12 October 2020
/
Accepted: 13 October 2020
/
Published: 15 October 2020
(This article belongs to the Special Issue Treatment Strategies for Hepatocellular Carcinoma)
Abstract
:Hepatocellular carcinoma (HCC) is a leading cause of death worldwide. The selection of therapeutic modalities and the prognosis of affected patients are well known to be dependent not only on the tumor burden but also on the hepatic reserve function. Antiviral treatments for chronic hepatitis related to a viral infection and an increase in cases of nonviral HCC associated with the aging of society have resulted in dramatic changes regarding the characteristics of HCC patients. With recent developments in therapeutic modalities for HCC, a more detailed assessment of hepatic function has become an important need. Studies in which the relationship of albumin-bilirubin (ALBI) grade with the prognosis of HCC patients was investigated were reviewed in order to evaluate the usefulness of newly developed ALBI and modified ALBI (mALBI) grades for HCC treatment, as those scoring methods are considered helpful for predicting the prognosis and selecting therapeutic modalities based on the expected prognosis.
1. Introduction
Hepatocellular carcinoma (HCC) is a leading cause of death worldwide [1,2]. In addition to liver transplantation, surgical resection, radiofrequency ablation (RFA), transarterial catheter chemoembolization (TACE), and tyrosine kinase inhibitors (TKIs) have been developed as standard treatments for each stage. It is well known that the prognosis of HCC patients is dependent not only on tumor burden but also hepatic reserve function [3,4,5].
The present review is conducted to focus on the useful predictive value of a newly developed assessment tool of hepatic function for prognosis with each modality for the treatment of patients with HCC.
1.1. Child–Pugh Classification as a Traditional Assessment Tool for Hepatic Function and Rapid Changes of Clinical Environment
Traditionally, the Child–Pugh classification has been used worldwide for a long period as a standard assessment tool for hepatic reserve function [6] because it is easy for clinicians to remember and calculate (Table 1).
The evidence-based clinical practice guideline for HCC of the Japan Society of Hepatology (JSH) [7] and Barcelona Clinic liver cancer staging system (BCLC) staging [8] therapeutic strategies for all HCC stages, and the subclassification for BCLC-B (intermediate) stage HCC for treatment guidance (Bolondi’s criteria [9] and Kindai criteria [10]) use Child–Pugh score/classification as an assessment method to evaluate the pretreatment hepatic reserve. In addition, clinical trends of HCC cases have shown dynamic changes. For example, the ability to treat the hepatic function of HCC patients affected by a hepatitis B virus (HBV) or hepatitis C virus (HCV) infection has shown improvement, because of the development of effective antiviral treatments (nucleotide analog for HBV, interferon therapy and direct acting antiviral agents for HCV). Moreover, there is an increasing number of HCC patients without HBV or HCV, which has become an important issue in association with the aging of society, as those often demonstrate good hepatic function [11,12]. As a result, in Japan, the percentage of HCC patients with Child–Pugh class A has increased from 52.1% in the 1990s to 84.8% in the late 2010s [13]. Moreover, some weak points of the Child–Pugh classification have been pointed out, including subjective factors (ascites, encephalopathy), interrelated factors (serum albumin level, ascites), semi-quantitative characteristics, and a lack of statistical evidence (Table 1).
1.2. A Development of New Assessment Tool for Hepatic Function: ALBI Grade
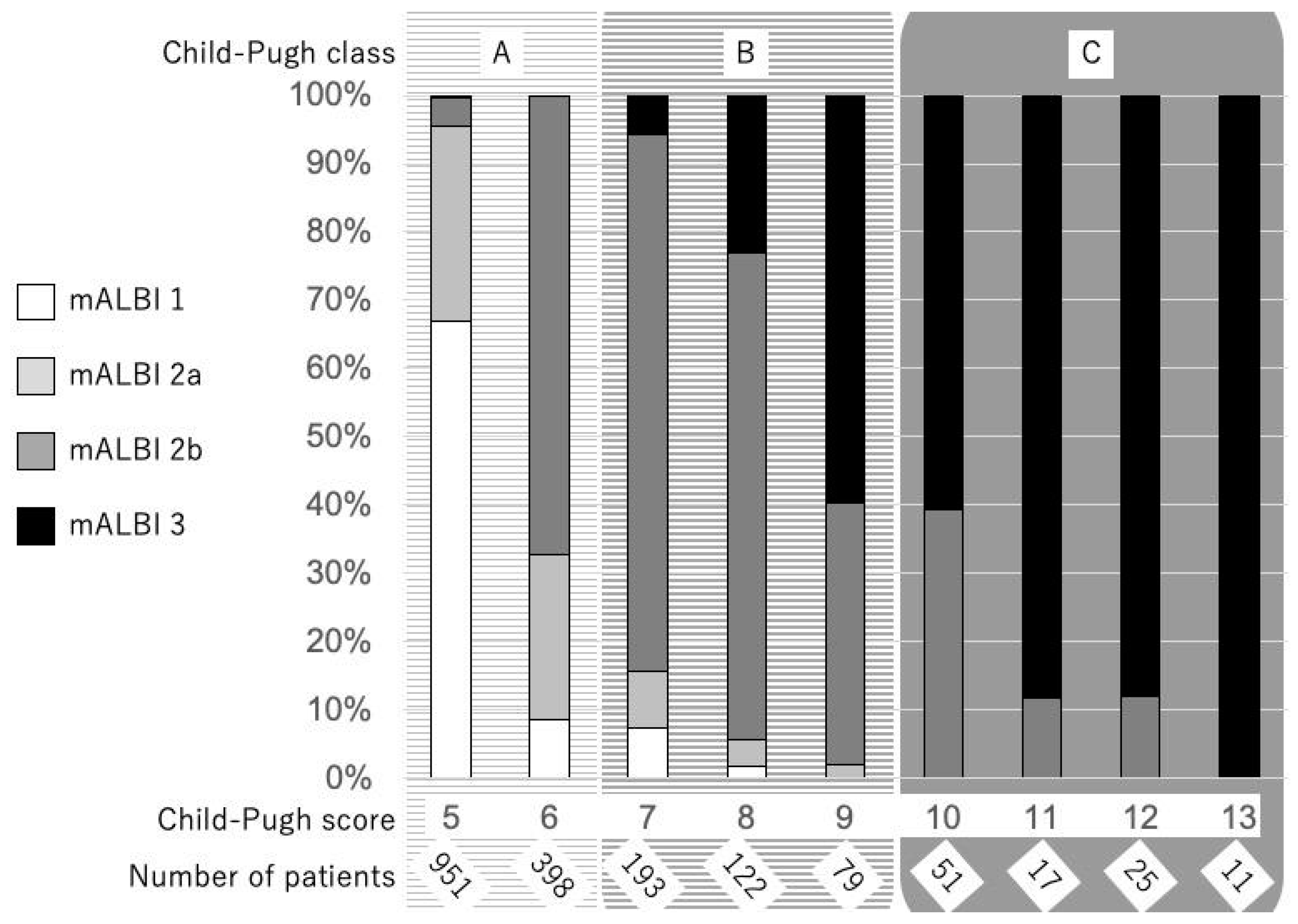
As noted above, the need for an objective and more detailed assessment tool, especially for patients with good hepatic function, has become an urgent issue. Recently, a simple and objective method for the evaluation of hepatic reserve function using only albumin and total-bilirubin measurements, termed albumin-bilirubin (ALBI) grade based on a formula (log10 bilirubin (µmol/L) × 0.66) + (albumin (g/L) × −0.085], has been proposed, with the values ≤−2.60, >−2.60 to ≤−1.39, and >−1.39 used to denote grades 1, 2, and 3, respectively [14]. Calculating only with two objective factors (bilirubin and albumin) is one of advantages because they are very common serum data and the frequency of a lack of data is low, especially in retrospective analyses. Following its development, it has been confirmed that ALBI grade can be used as an alternative assessment to the Child–Pugh classification, both in the evidence based clinical practice guideline for HCC of JSH (n = 3495) [15] and in the BCLC staging, with a weighted kappa value (which is a statistic for measuring the interevaluator reliability of qualitative items) of 0.917 noted with a multicenter cohort (n = 3696) [16]. As a result, ALBI grade has become recognized as a useful assessment tool for hepatic reserve function worldwide. However, a weak point of this grading system that has been pointed out is that grade 2 covers a wide range, similar to class B in the Child–Pugh classification. On the other hand, as opposed to the Child–Pugh score, which is a nominal variable, ALBI scoring has a great advantage as a continuous variable. To provide a more detailed assessment of hepatic reserve function, a modified ALBI (mALBI) grade has been proposed, with four grades including subgrades 2a and 2b, divided by the use of an ALBI score of −2.27 as the cutoff value for an indocyanine green retention rate at 15 min (ICG-R15) at 30% [17], because the ALBI score has been shown to have a correlation with ICG-R15 (r = 0.616, p < 0.001) [18]. The distribution of mALBI grades in comparison with Child–Pugh scores is shown in Figure 1 (1850 naïve HCC patients treated at Ehime Prefectural Central Hospital from 2000 to 2019). We consider that both ALBI and mALBI grades should be used for the assessment of hepatic function in patients, not only with early stage but also with intermediate and advanced stage HCC BCLC-B and -C, as they provide an opportunity to assess changes of hepatic function in detail during a clinical course (Figure 1).
2. ALBI Grade Related to Treatment Modalities
2.1. CURATIVE Treatments
2.1.1. Liver Transplantation
Tai reported that the age of the recipient and donor, and an ALBI score ≥−1.28 and grade 3 were independent factors related to post-transplant survival (each p < 0.01), whereas the Model for End-Stage Liver Disease (MELD) score was not [19]. In another report, ALBI grade 2 (HR = 1.827, p < 0.001) and grade 3 (HR 2.589, p < 0.001) were shown to be independent risk factors of poor survival in patients with HCC within the Milan criteria (single tumor less than 5 cm in size or no more than three tumors, all less than 3 cm in diameter) [20] and treated with liver transplantation [21], while an ALBI-based prognostic model with a total range of 0 to 6 points was derived based on the sum of five variables; 1 point each for age ≥65 years, alpha-fetoprotein (AFP) >100 ng/mL, presence of ascites, performance status 1 to 4, and ALBI grade 2, with 2 points for ALBI grade 3 [21]. Kormberg et al. reported that post-transplant recurrence rates for patients classified as ALBI grade 1, 2, and 3 were 10.5%, 15.9%, and 68.2%, respectively (p < 0.01) [22]. In addition, the ALBI grade might have a good value for predicting post-transplant complications. Zhang et al. noted that patients with grade 3 had a higher risk of bacterial pneumonia and early allograft dysfunction as compared to those with grade 1 (p = 0.029 and p = 0.038, respectively) or grade 2 (p = 0.006 and p = 0.007, respectively), and that the ALBI grade had a better predictive value for 30-day mortality as compared to Child–Pugh and MELD [area under the receiver operating characteristic curve (AUC): 0.702 (95% CI: 0.644–0.756), 0.669 (95% CI: 0.580–0.697), and 0.540 (95% CI: 0.580–0.697), respectively] [23].
2.1.2. Surgical Resection
In surgical resection cases, the ALBI grade had the best results with the Akaike information criterion (AIC) [24] (an index for evaluating the goodness of a statistical model widely used for statistical inference) for predicting overall survival (OS) in a comparison of 12 different hepatic reserve function models [25]. Even when analyzing hepatic reserve function in Child–Pugh class A patients with solitary HCC within the Milan criteria [20], the preoperative ALBI score was shown to have a prognostic predictive value (HR (95% CI)1.026–1.800, p = 0.033) (the one-, two-, and five-year OS rates: ALBI 1 vs. ALBI 2 = 94.53%, 88.40%, and 68.42%, vs. 92.08%, 82.42%, and 56.07%) [26]. The importance of the postoperative ALBI grade has also been reported for predicting long-term outcome after curative surgical resection [27] as well as for predicting posthepatectomy liver failure (PHLF) [28,29]. The AUC of the ALBI score for predicting PHLF was better than those of others (ALBI score vs. Child–Pugh score vs. MELD vs. ICG R15 = 0.745 vs. 0.665 vs. 0.649 vs. 0.668) [29]. Ye et al. noted the usefulness of the △ALBI score [postoperative (day 1) ALBI score – preoperative (last test before operation) ALBI score] (≤0.71 vs. >0.71) for OS and RFS (HR 0.507, p = 0.018, and HR 0.622, p = 0.004, respectively) as well as the postoperative ALBI grade (2 vs. 3) (HR 0.545, p = 0.014, and HR 0.659, p = 0.008, respectively) [30].
2.1.3. RFA
In addition to RFA cases, the ALBI grade has been reported to be a useful assessment tool for predicting prognosis. Chen found that ALBI grade 2 or 3 was an independent risk factor associated with poor RFS (HR 1.825, p = 0.001) as well as OS (HR 2.191, p = 0.005) in 271 patients with BCLC-0 [31]. In addition, Oh et al. reported that the five-year OS rate of patients with ALBI grade 1 was better than that of those with ALBI grade 2 (88.5% vs. 73.8%, p < 0.001) and showed the ALBI grade to be an independent factor associated with OS (HR 2.32, p = 0.002) [32]. In another study, Ho et al. stated that the ALBI grade may serve as an objective and feasible surrogate for prognostic prediction in HCC patients undergoing RFA, based on the results of comparisons of prognostic performance among 10 liver function models, in which the AIC of ALBI was superior to that of the others [33]. In addition to these studies, the therapeutic effect of RFA on prognosis was unexpectedly small in HCC patients with ALBI grade 3, because the prognosis of patients with ALBI grade 3 (n = 27) was worse that of those with ALBI grade 1 or 2 (n = 232) (median survival 2.7 vs. 4.8 years, p = 0.0168) [34].
Recently, a randomized controlled trial was designed to prospectively compare the efficacy of resection and RFA as the first approach for primary HCC, but it found no significant difference in OS between them [35]. However, Chong et al. reported that surgical resection offered superior OS and disease-free survival (DFS) results as compared to RFA in an ALBI grade 1 cohort after propensity score matching (p = 0.0002 and p < 0.0001 respectively), while there were no significant differences for those between surgical resection and RFA in the ALBI grade 2 cohort (p = 0.7119 and p = 0.3266, respectively) [36]. From the viewpoint of the hepatic reserve function (ALBI grade vs. Child–Pugh classification), it is necessary to conduct further investigations on the strategy for the selection of a curative therapeutic modality.
2.2. Palliative Treatment
2.2.1. TACE
TACE is recognized worldwide as a standard treatment for BCLC-B HCC, while a few reports have also noted that the ALBI grade is associated with OS in HCC patients treated with TACE. Khalid et al. found that only the ALBI grade showed a statistically significant association with OS (HR 3.06, p = 0.038) [37], and Izumoto et al. noted that ALBI grade 2 was a significant prognostic factor for worse OS in a study of 192 BCLC-B HCC patients with good hepatic function (Child–Pugh score ≤ 7) (HR 1.548, p = 0.048) [38]. The results of the OPTIMIS trial highlighted the negative influence of TACE on hepatic function as well as the importance of judging TACE failure in clinical practice [39]. In addition, with recent advancements in TKI treatment, the concept of the TACE refractory status [40] and switching to TKI therapy have been recognized as important for improving prognosis. Another report noted that the ALBI grade demonstrated a higher rate of deterioration of hepatic reserve function (grade 1 to 2: 18.4% to 21.4%/1 TACE) than the Child–Pugh classification (class A to B: 8.6% to 13.8%/1 TACE) during a clinical course that included repeated TACE procedures in 212 BCLC-B HCC patients with Child–Pugh class A [41]. Mohammed et al. also reported the usefulness of the ALBI score as a statistically significant prognostic factor for acute chronic liver failure at 90 days after TACE (OR 3.99, p = 0.002) [42]. Thus, as compared to the Child–Pugh classification, the ALBI grade might also play a greater role in the assessment of hepatic reserve function for TACE used to treat unresectable HCC.
Bolondi’s criteria [9] and Kindai criteria [10] had been proposed as a subclassification for BCLC-B with the Child–Pugh score in order to help judge the possible effectiveness of switching therapy. However, recently, Lee et al. proposed an ALBI-based model for the prediction of OS after TACE in BCLC-B cases [43], while a new subgrouping for BCLC-B (intermediate stage) HCC [Modified Intermediate stage of liver CANcer (MICAN) criteria] [44], in which the ALBI grade was used instead of the Child–Pugh score, has been proposed. More recently, the Asia-Pacific Primary Liver Cancer Expert (APPLE) group presented a consensus statement and proposed “TACE-unsuitable” criteria using mALBI [45]. Child–Pugh class A is not always a necessary and sufficient condition for TKI treatment in unresectable HCC, and a detailed assessment with ALBI and mALBI grades has begun to play an increasingly important clinical role in the treatment strategy for unresectable HCC.
2.2.2. ALBI and mALBI Grading for TKI Treatments
As of July 2020, multiple TKI drugs (sorafenib, regorafenib, lenvatinib, ramucirumab, cabozantinib) have become available worldwide. In an analysis of advanced HCC patients treated with sorafenib as part of a phase III study, ALBI grade 1 (p = 0.001) was associated with better progression-free survival [46]. Tada et al. reported that OS differed significantly between ALBI grades 1 and 2 (HR 1.44, p = 0.011) among patients with a Child–Pugh score of 5 and treated with sorafenib [47]. In another study, a Cox regression analysis of 415 advanced HCC patients classified as Child–Pugh A who underwent sorafenib treatment, baseline ALBI grade 2 (p < 0.001) and ALBI grade increased during treatment (p < 0.001) and were strongly associated with mortality [48]. The ALBI grade is thought to be an independent predictor of survival [46,48,49,50]. In 2017, regorafenib became available as a second-line therapy for patients who experienced sorafenib failure [51]. Along with the introduction of regorafenib, the ALBI grade has been found to be important. Not all u-HCC patients treated with sorafenib meet the RESORCE trial criteria [51] at the time of sorafenib failure, and thus the frequency of those indicated for regorafenib has been reported to range from only 30.6% to 44.2% after confirmation by radiological findings to have PD with sorafenib therapy [52,53,54,55,56]. Takada et al. showed that, at the time of the radiological progressive disease, the factors that met the RESORCE study inclusion criteria were not only the baseline ALBI score (−2.33; OR 2.5, p = 0.01) but also the degree of change in liver function after four weeks of sorafenib treatment (<0.255; OR4.9, p < 0.001) [57]. Furthermore, Yukimoto et al. demonstrated that an ALBI score of −2.53 at the time of introduction of sorafenib was useful as a cutoff value for predicting the eligibility for regorafenib after sorafenib failure [56], as did a report by Moriguchi et al. [58].
In 2018, lenvatinib was introduced as a new first-line treatment [59]. Its usefulness in clinical practice not only as a first-line but also as a second-line or later treatment option has also been reported in Japan [60,61], and this is an important clinical issue, as many patients do not meet the RESORCE criteria because of sorafenib intolerability. It has been reported that mALBI grades 2b or 3 (score > −2.27) were the only significant prognostic factors for the survival of patients undergoing lenvatinib treatment (HR 4.632, p = 0.004) [62]. Another study showed that sequential treatment with TKIs including lenvatinib had an impact in prolonging OS and that the total duration of administration of all TKIs demonstrated a good correlation with overall survival (r = 0.946, p < 0.001) [63]. In that report as well, OS with a TKI sequential treatment including treatment for u-HCC was good (n = 84) (median survival 46.4 months), and mALBI grades 2b or 3 (score > −2.27) at the time of introduction of the first-line TKI were also the only prognostic factors (HR 2.319, p = 0.034). Fuchigami et al. reported similar results in which patients with mALBI grade 1 and 2a (score ≤ −2.27) showed better prognosis for lenvatinib treatment (HR 0.16, p = 0.006) [64], as did Kaneko et al. for all patients treated with TKI therapy (median survival: mALBI grade 1:2a:2b and 3 = 20.1:16.3:9.8 months; p = 0.0003) [65]. Moreover, another study indicated that the predictive value for OS of mALBI was superior to that of the Child–Pugh score (AIC: 592.3 vs. 599.7) (c-index: 0.655 vs. 0.597) and non-mALBI grade 1/2a at the start of treatment and that there was a significant risk factor for a decline to Child–Pugh class B during therapy (HR 2.552, p < 0.001) when using lenvatinib treatment as a first-line drug [66]. Based on the findings noted above, the minimum condition for introducing TKI treatment is thought to be mALBI grade 2a (score ≤ −2.27), and ALBI scoring is considered to be a very useful assessment tool when considering indications for TKI treatment (Table 2).
3. Others
3.1. Combination Use of ALBI with Another Clinical Indicator
Some reports have proposed a combination use with ALBI and other tools for the prediction of a prognosis. One introduced an ALBI-based model for HCC beyond Milan criteria (ALBI-HOME) with six parameters (ALBI grade 2, grade 3, serum AFP, total tumor volume, ascites, performance status 0/1) [67], while others noted the predictive ability for OS and DFS of the combination of the ALBI grade and FIB-4 index for HCC patients within the Milan criteria treated with resection, [68] and RFS for all HCC patients treated with resection curatively [69]. In addition, the prognostic usefulness of a nomogram integrating preoperative ALBI and serum γ-glutamyl transpeptidase (GGT) for postoperative OS and DFS, [70] as well as an ALBI-TAE model with three factors (beyond up-to-11 criteria, AFP >200 ng/mL, ALBI grades 2 or 3) in patients receiving TACE for BCLC-B stage HCC [43] have also been reported.
3.2. ALBI and mALBI Grading as Part of Total Staging Scoring System and Treatment Algorithms
The Japan integrated staging score (JIS) [4,5], which is simply calculated using only the TNM stage of the Liver Cancer Study Group of Japan (LCSGJ) [71] and Child–Pugh classification, has been proposed as an easy total stage scoring system. Recently, the ALBI-TNM score (ALBI-T), calculated with the TNM of LCSGJ and the ALBI grade instead of the Child–Pugh classification, has been developed as a modified JIS [17,18,72,73]. Another method, the Modified Cancer of the Liver Italian Program (CLIP) score with the ALBI grade, has also been reported [74,75,76]. It was noted that when the ALBI grade was used instead of the Child–Pugh classification with the evidence-based clinical practice guidelines for HCC of the LCSGJ (n = 3495), there was only a small difference with regard to the therapeutic selection and the AIC of ALBI-T was better than that of JIS (21989.4 vs. 22075.1) [18]. In a multicenter analysis (n = 6649), the AIC of mALBI-T, calculated with the mALBI grade and TNM of LCSGJ, was superior to that calculated with ALBI-T and JIS (45327.1 vs. 45467.7 and 45555.8) [17]. Elsharawy et al. reported that the AUCs for predicting prognosis of ALBI-T and mALBI-T were better than the other tools (e.g., Child–Pugh classification, BCLC stage, ALBI grade, ALBI-based BCLC) as a validation study (n = 1910) [77]. Thus, the development of not only ALBI but also mALBI grading is thought to provide matching tools for contemporary clinical practice for the treatment of HCC cases (Table 3).
4. Limitations of ALBI Grade
Although the ALBI score provides a good index for predicting complications following adult-to-adult living donor liver transplantation and has been shown to have a predictive ability similar to that of the Child–Pugh classification and MELD score [23], the weak points of the ALBI grade with regard to the prognostic predictive power of the decompensated cirrhosis status (especially with ascites) and ruptured HCC must be kept in mind. Many clinicians have a consensus that HCC patients with uncontrollable ascites are not eligible for aggressive treatments, except for liver transplantation. In a comparison of ALBI grade and MELD in patients undergoing transjugular intrahepatic portosystemic shunt (TIPS) creation due to portal hypertension complications (variceal bleeding 55%, ascites 35%, others 10%), Khabbaz et al. reported that only MELD was associated with a transplant-free survival [78], while it was also a better predictor of both 30-day and overall survival as compared to the ALBI grade (c-index: 0.74 vs. 0.64 and 0.63 vs. 0.59, respectively) [79], while Kim et al. reported that the MELD-Na score could effectively identify hepatic function and prognosis in HCC patients with ascites when compared with ALBI, Child–Pugh and MELD scores [80]. Additionally, Wu et al. demonstrated that the Child–Pugh score could predict OS of patients with a ruptured HCC treated both with and without resection (all p < 0.0001), whereas the ALBI grade could not [81]. Needless to say, it is necessary to pay attention to the interpretation of the results in any assessment methods for hepatic reserve function in constitutional jaundice patients with an elevated bilirubin level including Gilbert’s syndrome.
5. Conclusions
ALBI and mALBI grades are worthy of clinical application for patients receiving treatments for HCC. With regards to predicting prognosis in those patients receiving curative as well as palliative treatments for u-HCC, a more detailed assessment of hepatic function provided by ALBI and mALBI grades can be used effectively in clinical situations. In the near future, the establishment of an HCC treatment algorithm using ALBI/mALBI grades is anticipated.
Author Contributions
A.H. and T.K. conceived this review article and participated in its design and coordination. A.H. and T.K. drafted the text. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Mak, L.-Y.; Cruz-Ramón, V.; Chinchilla-López, P.; Torres, H.A.; LoConte, N.K.; Rice, J.P.; Foxhall, L.E.; Sturgis, E.M.; Merrill, J.K.; Bailey, H.H.; et al. Global Epidemiology, Prevention, and Management of Hepatocellular Carcinoma. Am. Soc. Clin. Oncol. Educ. Book 2018, 38, 262–279. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.D.; Hainaut, P.; Gores, G.J.; Amadou, A.; Plymoth, A.; Roberts, L.R. A global view of hepatocellular carcinoma: Trends, risk, prevention and management. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 589–604. [Google Scholar] [CrossRef] [PubMed]
- Okuda, K.; Ohtsuki, T.; Obata, H.; Tomimatsu, M.; Okazaki, N.; Hasegawa, H.; Nakajima, Y.; Ohnishi, K. Natural history of hepatocellular carcinoma and prognosis in relation to treatment. Study of 850 patients. Cancer 1985, 56, 918–928. [Google Scholar] [CrossRef]
- Kudo, M.; Chung, H.; Osaki, Y. Prognostic staging system for hepatocellular carcinoma (CLIP score): Its value and limitations, and a proposal for a new staging system, the Japan Integrated Staging Score (JIS score). J. Gastroenterol. 2003, 38, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Kudo, M.; Chung, H.; Haji, S.; Osaki, Y.; Oka, H.; Seki, T.; Kasugai, H.; Sasaki, Y.; Matsunaga, T. Validation of a new prognostic staging system for hepatocellular carcinoma: The JIS score compared with the CLIP score. Hepatol. (Baltimore, Md.) 2004, 40, 1396–1405. [Google Scholar] [CrossRef] [PubMed]
- Pugh, R.N.H.; Murray-Lyon, I.M.; Dawson, J.L.; Pietroni, M.C.; Williams, R. Transection of the oesophagus for bleeding oesophageal varices. BJS 1973, 60, 646–649. [Google Scholar] [CrossRef]
- Kokudo, N.; Hasegawa, K.; Akahane, M.; Igaki, H.; Izumi, N.; Ichida, T.; Uemoto, S.; Kaneko, S.; Kawasaki, S.; Ku, Y.; et al. Evidence-based Clinical Practice Guidelines for Hepatocellular Carcinoma: The Japan Society of Hepatology 2013 update (3rd JSH-HCC Guidelines). Hepatol. Res. 2015, 45. [Google Scholar] [CrossRef]
- Forner, A.; Reig, M.; Bruix, J. Hepatocellular carcinoma. Lancet 2018, 391, 1301–1314. [Google Scholar] [CrossRef]
- Burroughs, A.; Dufour, J.-F.; Galle, P.R.; Mazzaferro, V.; Piscaglia, F.; Raoul, J.L.; Sangro, B.; Bolondi, L. Heterogeneity of Patients with Intermediate (BCLC B) Hepatocellular Carcinoma: Proposal for a Subclassification to Facilitate Treatment Decisions. Semin. Liver Dis. 2013, 32, 348–359. [Google Scholar] [CrossRef]
- Kudo, M.; Arizumi, T.; Ueshima, K.; Sakurai, T.; Kitano, M.; Nishida, N. Subclassification of BCLC B Stage Hepatocellular Carcinoma and Treatment Strategies: Proposal of Modified Bolondi’s Subclassification (Kinki Criteria). Dig. Dis. 2015, 33, 751–758. [Google Scholar] [CrossRef]
- Hiraoka, A.; Ochi, M.; Matsuda, R.; Aibiki, T.; Okudaira, T.; Kawamura, T.; Yamago, H.; Nakahara, H.; Suga, Y.; Azemoto, N.; et al. Ultrasonography screening for hepatocellular carcinoma in Japanese patients with diabetes mellitus. J. Diabetes 2015, 8, 640–646. [Google Scholar] [CrossRef] [PubMed]
- Tateishi, R.; Uchino, K.; Fujiwara, N.; Takehara, T.; Okanoue, T.; Seike, M.; Yoshiji, H.; Yatsuhashi, H.; Shimizu, M.; Torimura, T.; et al. A nationwide survey on non-B, non-C hepatocellular carcinoma in Japan: 2011–2015 update. J. Gastroenterol. 2018, 54, 367–376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumada, T.; Toyoda, H.; Tada, T.; Yasuda, S.; Tanaka, J. Changes in Background Liver Function in Patients with Hepatocellular Carcinoma over 30 Years: Comparison of Child-Pugh Classification and Albumin Bilirubin Grade. Liver Cancer 2020, 1–11. [Google Scholar] [CrossRef]
- Johnson, P.J.; Berhane, S.; Kagebayashi, C.; Satomura, S.; Teng, M.; Reeves, H.L.; O’Beirne, J.; Fox, R.; Skowronska, A.; Palmer, D.; et al. Assessment of Liver Function in Patients With Hepatocellular Carcinoma: A New Evidence-Based Approach—The ALBI Grade. J. Clin. Oncol. 2015, 33, 550–558. [Google Scholar] [CrossRef] [PubMed]
- Hiraoka, A.; Kumada, T.; Kudo, M.; Hirooka, M.; Tsuji, K.; Itobayashi, E.; Kariyama, K.; Ishikawa, T.; Tajiri, K.; Ochi, H.; et al. Albumin-Bilirubin (ALBI) Grade as Part of the Evidence-Based Clinical Practice Guideline for HCC of the Japan Society of Hepatology: A Comparison with the Liver Damage and Child-Pugh Classifications. Liver Cancer 2017, 6, 204–215. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.W.H.; Kumada, T.; Toyoda, H.; Tada, T.; Chong, C.C.N.; Mo, F.K.F.; Yeo, W.; Johnson, P.J.; Lai, P.B.S.; To, K.-F.; et al. Integration of albumin-bilirubin (ALBI) score into Barcelona Clinic Liver Cancer (BCLC) system for hepatocellular carcinoma. J. Gastroenterol. Hepatol. 2016, 31, 1300–1306. [Google Scholar] [CrossRef]
- Hiraoka, A.; Kumada, T.; Tsuji, K.; Takaguchi, K.; Itobayashi, E.; Kariyama, K.; Ochi, H.; Tajiri, K.; Hirooka, M.; Shimada, N.; et al. Validation of Modified ALBI Grade for More Detailed Assessment of Hepatic Function in Hepatocellular Carcinoma Patients: A Multicenter Analysis. Liver Cancer 2018, 8, 121–129. [Google Scholar] [CrossRef] [PubMed]
- Hiraoka, A.; Michitaka, K.; Kumada, T.; Izumi, N.; Kadoya, M.; Kokudo, N.; Kubo, S.; Matsuyama, Y.; Nakashima, O.; Sakamoto, M.; et al. Validation and Potential of Albumin-Bilirubin Grade and Prognostication in a Nationwide Survey of 46,681 Hepatocellular Carcinoma Patients in Japan: The Need for a More Detailed Evaluation of Hepatic Function. Liver Cancer 2017, 6, 325–336. [Google Scholar] [CrossRef]
- Tai, K.; Kuramitsu, K.; Kido, M.; Tanaka, M.; Komatsu, S.; Awazu, M.; Gon, H.; So, S.; Tsugawa, D.; Mukubo, H.; et al. Impact of Albumin-Bilirubin Score on Short- and Long-Term Survival After Living-Donor Liver Transplantation: A Retrospective Study. Transplant. Proc. 2020, 52, 910–919. [Google Scholar] [CrossRef]
- Mazzaferro, V.; Regalia, E.; Doci, R.; Andreola, S.; Pulvirenti, A.; Bozzetti, F.; Montalto, F.; Ammatuna, M.; Morabito, A.; Gennari, L. Liver Transplantation for the Treatment of Small Hepatocellular Carcinomas in Patients with Cirrhosis. N. Engl. J. Med. 1996, 334, 693–700. [Google Scholar] [CrossRef] [PubMed]
- Ho, S.-Y.; Liu, P.-H.; Hsu, C.-Y.; Hsia, C.-Y.; Su, C.-W.; Huang, Y.-H.; Lei, H.-J.; He, Y.-J.; Hou, M.-C.; Huo, T.-I. An Albumin-Bilirubin (ALBI) Grade–based Prognostic Model For Patients With Hepatocellular Carcinoma Within Milan Criteria. Am. J. Clin. Oncol. 2019, 42, 698–704. [Google Scholar] [CrossRef] [PubMed]
- Kornberg, A.; Witt, U.; Schernhammer, M.; Kornberg, J.; Müller, K.; Friess, H.; Thrum, K. The role of preoperative albumin-bilirubin grade for oncological risk stratification in liver transplant patients with hepatocellular carcinoma. J. Surg. Oncol. 2019, 120, 1126–1136. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Liu, C.; Tan, Y.; Tan, L.; Jiang, L.; Yang, J.; Yang, J.; Yan, L.; Wen, T. Albumin-Bilirubin Score for Predicting Post-Transplant Complications Following Adult-to-Adult Living Donor Liver Transplantation. Ann. Transplant. 2018, 23, 639–646. [Google Scholar] [CrossRef] [PubMed]
- Akaike, H. Information theory as an extension of the maximum likelihood principle. In Proceedings of the 2nd International Symposium on Information Theory; Petrov, B.N., Caski, F., Eds.; Springer: New York, NY, USA, 1973; pp. 267–281. [Google Scholar]
- Ho, S.-Y.; Liu, P.-H.; Hsu, C.-Y.; Hsia, C.-Y.; Su, C.-W.; Lee, Y.-H.; Huang, Y.-H.; Lee, F.-Y.; Hou, M.-C.; Huo, T.-I. Comparison of twelve liver functional reserve models for outcome prediction in patients with hepatocellular carcinoma undergoing surgical resection. Sci. Rep. 2018, 8, 4773. [Google Scholar] [CrossRef] [PubMed]
- Dong, Z.-R.; Zou, J.; Sun, D.; Shi, G.-M.; Ke, A.-W.; Cai, J.-B.; Sun, H.-C.; Qiu, S.-J.; Li, T.; Zhou, J.; et al. Preoperative Albumin-Bilirubin Score for Postoperative Solitary Hepatocellular Carcinoma within the Milan Criteria and Child-Pugh A Cirrhosis. J. Cancer 2017, 8, 3862–3867. [Google Scholar] [CrossRef] [Green Version]
- Amisaki, M.; Uchinaka, E.; Morimoto, M.; Tokuyasu, N.; Sakamoto, T.; Honjo, S.; Saito, H.; Fujiwara, Y. Post-operative albumin-bilirubin grade predicts long-term outcomes among Child–Pugh grade A patients with hepatocellular carcinoma after curative resection. Hepatobiliary Pancreat. Dis. Int. 2018, 17, 502–509. [Google Scholar] [CrossRef]
- Zhang, Z.-Q.; Xiong, L.; Zhou, J.-J.; Miao, X.-Y.; Li, Q.-L.; Wen, Y.; Zou, H. Ability of the ALBI grade to predict posthepatectomy liver failure and long-term survival after liver resection for different BCLC stages of HCC. World J. Surg. Oncol. 2018, 16, 208. [Google Scholar] [CrossRef]
- Zou, H.; Yang, X.; Li, Q.-L.; Zhou, Q.-X.; Xiong, L.; Wen, Y. A Comparative Study of Albumin-Bilirubin Score with Child-Pugh Score, Model for End-Stage Liver Disease Score and Indocyanine Green R15 in Predicting Posthepatectomy Liver Failure for Hepatocellular Carcinoma Patients. Dig. Dis. 2018, 36, 236–243. [Google Scholar] [CrossRef]
- Ye, L.; Liang, R.; Zhang, J.; Chen, C.; Chen, X.; Zhang, Y.; Wang, G.; Yang, Y.; Chen, G. Postoperative albumin-bilirubin grade and albumin-bilirubin change predict the outcomes of hepatocellular carcinoma after hepatectomy. Ann. Transl. Med. 2019, 7, 367. [Google Scholar] [CrossRef]
- Chen, P.-C.; Chiu, N.-C.; Su, C.-W.; Huang, Y.-H.; Hou, M.-C.; Lin, H.-C.; Wu, J.-C. Albumin-bilirubin grade may determine the outcomes of patients with very early stage hepatocellular carcinoma after radiofrequency ablation therapy. J. Chin. Med. Assoc. 2019, 82, 2–10. [Google Scholar] [CrossRef]
- Oh, I.S.; Sinn, D.H.; Kang, T.W.; Lee, M.W.; Kang, W.; Gwak, G.-Y.; Paik, Y.-H.; Choi, M.S.; Lee, J.H.; Koh, K.C.; et al. Liver Function Assessment Using Albumin–Bilirubin Grade for Patients with Very Early-Stage Hepatocellular Carcinoma Treated with Radiofrequency Ablation. Dig. Dis. Sci. 2017, 62, 3235–3242. [Google Scholar] [CrossRef] [PubMed]
- Ho, S.-Y.; Liu, P.-H.; Hsu, C.-Y.; Chiou, Y.-Y.; Su, C.-W.; Lee, Y.-H.; Huang, Y.-H.; Lee, F.-Y.; Hou, M.-C.; Huo, T.-I. Prognostic Performance of Ten Liver Function Models in Patients with Hepatocellular Carcinoma Undergoing Radiofrequency Ablation. Sci. Rep. 2018, 8, 843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hiraoka, A.; Kumada, T.; Hirooka, M.; Tsuji, K.; Itobayashi, E.; Kariyama, K.; Ishikawa, T.; Tajiri, K.; Ochi, H.; Tada, T.; et al. A better method for assessment of hepatic function in hepatocellular carcinoma patients treated with radiofrequency ablation: Usefulness of albumin-bilirubin grade. Hepatol. Res. 2017, 48, E61–E67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Izumi, N.; Hasegawa, K.; Nishioka, Y.; Takayama, T.; Yamanaka, N.; Kudo, M.; Shimada, M.; Inomata, M.; Kaneko, S.; Baba, H.; et al. A multicenter randomized controlled trial to evaluate the efficacy of surgery vs. radiofrequency ablation for small hepatocellular carcinoma (SURF trial). J. Clin. Oncol. 2019, 37, 4002. [Google Scholar] [CrossRef]
- Chong, C.C.-N.; Chan, A.W.-H.; Wong, J.; Chu, C.-M.; Chan, S.L.; Lee, K.-F.; Yu, S.C.-H.; To, K.F.; Johnson, P.; Lai, P.B. Albumin-bilirubin grade predicts the outcomes of liver resection versus radiofrequency ablation for very early/early stage of hepatocellular carcinoma. Surgeon 2018, 16, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Khalid, M.A.; Achakzai, I.K.; Hanif, F.M.; Ahmed, S.; Majid, Z.; Luck, N.H. To determine the prognostic value of the albumin-bilirubin grade (ALBI) in patients underwent transarterial chemoembolization for unresectable hepatocellular carcinoma. Gastroenterol. Hepatol. Bed Bench 2019, 12, 110–115. [Google Scholar] [PubMed]
- Izumoto, H.; Hiraoka, A.; Ishimaru, Y.; Murakami, T.; Kitahata, S.; Ueki, H.; Aibiki, T.; Okudaira, T.; Miyamoto, Y.; Yamago, H.; et al. Validation of Newly Proposed Time to Transarterial Chemoembolization Progression in Intermediate-Stage Hepatocellular Carcinoma Cases. Oncology 2017, 93, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Peck-Radosavljevic, M.; Kudo, M.; Raoul, J.-L.; Lee, H.C.; Decaens, T.; Heo, J.; Lin, S.-M.; Shan, H.; Yang, Y.; Bayh, I.; et al. Outcomes of patients (pts) with hepatocellular carcinoma (HCC) treated with transarterial chemoembolization (TACE): Global OPTIMIS final analysis. J. Clin. Oncol. 2018, 36, 4018. [Google Scholar] [CrossRef]
- Kudo, M.; Matsui, O.; Izumi, N.; Iijima, H.; Kadoya, M.; Imai, Y.; Okusaka, T.; Miyayama, S.; Tsuchiya, K.; Ueshima, K.; et al. JSH Consensus-Based Clinical Practice Guidelines for the Management of Hepatocellular Carcinoma: 2014 Update by the Liver Cancer Study Group of Japan. Liver Cancer 2014, 3, 458–468. [Google Scholar] [CrossRef]
- Hiraoka, A.; Kumada, T.; Kudo, M.; Hirooka, M.; Koizumi, Y.; Hiasa, Y.; Tajiri, K.; Toyoda, H.; Tada, T.; Ochi, H.; et al. Hepatic Function during Repeated TACE Procedures and Prognosis after Introducing Sorafenib in Patients with Unresectable Hepatocellular Carcinoma: Multicenter Analysis. Dig. Dis. 2017, 35, 602–610. [Google Scholar] [CrossRef]
- Mohammed, M.A.A.; Khalaf, M.; Liang, T.; Wang, D.S.; Lungren, M.P.; Rosenberg, J.; Kothary, N. Albumin-Bilirubin Score: An Accurate Predictor of Hepatic Decompensation in High-Risk Patients Undergoing Transarterial Chemoembolization for Hepatocellular Carcinoma. J. Vasc. Interv. Radiol. 2018, 29, 1527–1534. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.; Hung, Y.; Liu, C.; Lee, R.; Su, C.-W.; Huo, T.-I.; Li, C.; Chao, Y.; Lin, H.; Hou, M.; et al. A new ALBI-based model to predict survival after transarterial chemoembolization for BCLC stage B hepatocellular carcinoma. Liver Int. 2019, 39, 1704–1712. [Google Scholar] [CrossRef] [PubMed]
- Hiraoka, A.; Kumada, T.; Nouso, K.; Tsuji, K.; Itobayashi, E.; Hirooka, M.; Kariyama, K.; Ishikawa, T.; Tada, T.; Toyoda, H.; et al. Proposed New Sub-Grouping for Intermediate-Stage Hepatocellular Carcinoma Using Albumin-Bilirubin Grade. Oncology 2016, 91, 153–161. [Google Scholar] [CrossRef] [PubMed]
- Kudo, M.; Han, K.-H.; Ye, S.-L.; Zhou, J.; Huang, Y.-H.; Lin, S.-M.; Wang, C.-K.; Ikeda, M.; Chan, S.L.; Choo, S.P.; et al. A Changing Paradigm for the Treatment of Intermediate-Stage Hepatocellular Carcinoma: Asia-Pacific Primary Liver Cancer Expert Consensus Statements. Liver Cancer 2020, 9, 245–260. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Rahman, O. Impact of baseline characteristics on outcomes of advanced HCC patients treated with sorafenib: A secondary analysis of a phase III study. J. Cancer Res. Clin. Oncol. 2018, 144, 901–908. [Google Scholar] [CrossRef] [PubMed]
- Tada, T.; Kumada, T.; Toyoda, H.; Tsuji, K.; Hiraoka, A.; Michitaka, K.; Deguchi, A.; Ishikawa, T.; Imai, M.; Ochi, H.; et al. Impact of albumin–bilirubin grade on survival in patients with hepatocellular carcinoma who received sorafenib: An analysis using time-dependent receiver operating characteristic. J. Gastroenterol. Hepatol. 2019, 34, 1066–1073. [Google Scholar] [CrossRef] [PubMed]
- Kuo, Y.-H.; Wang, J.-H.; Hung, C.-H.; Rau, K.-M.; Wu, I.-P.; Chen, C.-H.; Kee, K.-M.; Hu, T.-H.; Lu, S.-N. Albumin-Bilirubin grade predicts prognosis of HCC patients with sorafenib use. J. Gastroenterol. Hepatol. 2017, 32, 1975–1981. [Google Scholar] [CrossRef] [PubMed]
- Ogasawara, S.; Chiba, T.; Ooka, Y.; Suzuki, E.; Kanogawa, N.; Saito, T.; Motoyama, T.; Tawada, A.; Kanai, F.; Yokosuka, O. Liver function assessment according to the Albumin–Bilirubin (ALBI) grade in sorafenib-treated patients with advanced hepatocellular carcinoma. Investig. New Drugs 2015, 33, 1257–1262. [Google Scholar] [CrossRef]
- Nguyen, T.T.H.; Nguyen, V.H.; Nguyen, T.L.; Le, V.Q. Role of Baseline Albumin-Bilirubin Grade on Predict Overall Survival Among Sorafenib-Treated Patients with Hepatocellular Carcinoma in Vietnam. Cancer Control. 2019, 26, 1073274819865269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruix, J.; Qin, S.; Merle, P.; Granito, A.; Huang, Y.-H.; Bodoky, G.; Pracht, M.; Yokosuka, O.; Rosmorduc, O.; Breder, V.; et al. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2017, 389, 56–66. [Google Scholar] [CrossRef] [Green Version]
- Ogasawara, S.; Chiba, T.; Ooka, Y.; Suzuki, E.; Maeda, T.; Yokoyama, M.; Wakamatsu, T.; Inoue, M.; Saito, T.; Kobayashi, K.; et al. Characteristics of patients with sorafenib-treated advanced hepatocellular carcinoma eligible for second-line treatment. Investig. New Drugs 2017, 36, 332–339. [Google Scholar] [CrossRef] [PubMed]
- Terashima, T.; Yamashita, T.; Sunagozaka, H.; Arai, K.; Kawaguchi, K.; Kitamura, K.; Yamashita, T.; Sakai, Y.; Mizukoshi, E.; Honda, M.; et al. Analysis of the liver functional reserve of patients with advanced hepatocellular carcinoma undergoing sorafenib treatment: Prospects for regorafenib therapy. Hepatol. Res. 2018, 48, 956–966. [Google Scholar] [CrossRef] [PubMed]
- Kuzuya, T.; Ishigami, M.; Ishizu, Y.; Honda, T.; Hayashi, K.; Ishikawa, T.; Nakano, I.; Hirooka, Y.; Goto, H. Prognostic Factors Associated with Postprogression Survival in Advanced Hepatocellular Carcinoma Patients Treated with Sorafenib Not Eligible for Second-Line Regorafenib Treatment. Oncology 2018, 95, 91–99. [Google Scholar] [CrossRef] [PubMed]
- Uchikawa, S.; Kawaoka, T.; Aikata, H.; Kodama, K.; Nishida, Y.; Inagaki, Y.; Hatooka, M.; Morio, K.; Nakahara, T.; Murakami, E.; et al. Clinical outcomes of sorafenib treatment failure for advanced hepatocellular carcinoma and candidates for regorafenib treatment in real-world practice. Hepatol. Res. 2018, 48, 814–820. [Google Scholar] [CrossRef] [PubMed]
- Yukimoto, A.; Hirooka, M.; Hiraoka, A.; Michitaka, K.; Ochi, H.; Joko, K.; Imai, Y.; Watanabe, T.; Koizumi, Y.; Yoshida, O.; et al. Using ALBI score at the start of sorafenib treatment to predict regorafenib treatment candidates in patients with hepatocellular carcinoma. Jpn. J. Clin. Oncol. 2018, 49, 42–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takada, H.; Kurosaki, M.; Tsuchiya, K.; Komiyama, Y.; Itakura, J.; Takahashi, Y.; Nakanishi, H.; Yasui, Y.; Tamaki, N.; Maeyashiki, C.; et al. Baseline and Early Predictors of Good Patient Candidates for Second-Line after Sorafenib Treatment in Unresectable Hepatocellular Carcinoma. Cancers 2019, 11, 1256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moriguchi, M.; Aramaki, T.; Sato, R.; Iwai, K.; Tsuchiya, S.; Asakura, K.; Takahashi, A.; Seko, Y.; Umemura, A.; Ymaguchi, K.; et al. Intrahepatic Tumor Burden as a Novel Factor Influencing the Introduction of Second-line Chemotherapy for Hepatocellular Carcinoma. Anticancer. Res. 2020, 40, 3953–3960. [Google Scholar] [CrossRef] [PubMed]
- Kudo, M.; Finn, R.S.; Qin, S.; Han, K.-H.; Ikeda, K.; Piscaglia, F.; Baron, A.; Park, J.-W.; Han, G.; Jassem, J.; et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: A randomised phase 3 non-inferiority trial. Lancet 2018, 391, 1163–1173. [Google Scholar] [CrossRef] [Green Version]
- Hiraoka, A.; Kumada, T.; Kariyama, K.; Takaguchi, K.; Itobayashi, E.; Shimada, N.; Tajiri, K.; Tsuji, K.; Ishikawa, T.; Ochi, H.; et al. Therapeutic potential of lenvatinib for unresectable hepatocellular carcinoma in clinical practice: Multicenter analysis. Hepatol. Res. 2018, 49, 111–117. [Google Scholar] [CrossRef] [Green Version]
- Hiraoka, A.; Kumada, T.; Kariyama, K.; Takaguchi, K.; Atsukawa, M.; Itobayashi, E.; Tsuji, K.; Tajiri, K.; Hirooka, M.; Shimada, N.; et al. Clinical features of lenvatinib for unresectable hepatocellular carcinoma in real-world conditions: Multicenter analysis. Cancer Med. 2018, 8, 137–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hiraoka, A.; Kumada, T.; Atsukawa, M.; Hirooka, M.; Tsuji, K.; Ishikawa, T.; Takaguchi, K.; Kariyama, K.; Itobayashi, E.; Tajiri, K.; et al. Prognostic factor of lenvatinib for unresectable hepatocellular carcinoma in real-world conditions-Multicenter analysis. Cancer Med. 2019, 8, 3719–3728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hiraoka, A.; Kumada, T.; Atsukawa, M.; Hirooka, M.; Tsuji, K.; Ishikawa, T.; Takaguchi, K.; Kariyama, K.; Itobayashi, E.; Tajiri, K.; et al. Important Clinical Factors in Sequential Therapy Including Lenvatinib against Unresectable Hepatocellular Carcinoma. Oncology 2019, 97, 277–285. [Google Scholar] [CrossRef] [PubMed]
- Fuchigami, A.; Imai, Y.; Uchida, Y.; Uchiya, H.; Fujii, Y.; Nakazawa, M.; Ando, S.; Sugawara, K.; Nakayama, N.; Tomiya, T.; et al. Therapeutic efficacy of lenvatinib for patients with unresectable hepatocellular carcinoma based on the middle-term outcome. PLoS ONE 2020, 15, e0231427. [Google Scholar] [CrossRef] [PubMed]
- Kaneko, S.; Tsuchiya, K.; Yasui, Y.; Inada, K.; Kirino, S.; Yamashita, K.; Osawa, L.; Hayakawa, Y.; Sekiguchi, S.; Higuchi, M.; et al. Strategy for advanced hepatocellular carcinoma based on liver function and portal vein tumor thrombosis. Hepatol. Res. 2020. [Google Scholar] [CrossRef]
- Hiraoka, A.; Kumada, T.; Fukunishi, S.; Atsukawa, M.; Hirooka, M.; Tsuji, K.; Ishikawa, T.; Takaguchi, K.; Kariyama, K.; Itobayashi, E.; et al. Post-Progression Treatment Eligibility of Unresectable Hepatocellular Carcinoma Patients Treated with Lenvatinib. Liver Cancer 2019, 9, 73–83. [Google Scholar] [CrossRef] [PubMed]
- Ho, S.-Y.; Liu, P.-H.; Hsu, C.-Y.; Hsia, C.-Y.; Huang, Y.-H.; Su, C.-W.; Lei, H.-J.; Lee, R.-C.; Hou, M.-C.; Huo, T.-I. A New Prognostic Model Based on Albumin–Bilirubin Grade for Hepatocellular Carcinoma Beyond the Milan Criteria. Dig. Dis. Sci. 2019, 65, 658–667. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Luo, Y.; Li, C.; Liu, J.; Xiang, H.; Wen, T. The combination of the preoperative albumin-bilirubin grade and the fibrosis-4 index predicts the prognosis of patients with hepatocellular carcinoma after liver resection. Biosci. Trends 2019, 13, 351–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liao, R.; Li, D.-W.; Du, C.-Y.; Li, M. Combined Preoperative ALBI and FIB-4 Is Associated with Recurrence of Hepatocellular Carcinoma After Curative Hepatectomy. J. Gastrointest. Surg. 2018, 22, 1679–1687. [Google Scholar] [CrossRef]
- Zhang, C.-H.; Ni, X.-C.; Chen, B.-Y.; Qiu, S.-J.; Zhu, Y.-M.; Luo, M. Combined preoperative albumin-bilirubin (ALBI) and serum γ-glutamyl transpeptidase (GGT) predicts the outcome of hepatocellular carcinoma patients following hepatic resection. J. Cancer 2019, 10, 4836–4845. [Google Scholar] [CrossRef]
- Liver Cancer study Group of Japan the general rules for the clinical and pathological study of primary liver cancer. Surg. Today 1989, 19, 98–129. [CrossRef]
- Hiraoka, A.; Kumada, T.; Michitaka, K.; Toyoda, H.; Tada, T.; Ueki, H.; Kaneto, M.; Aibiki, T.; Okudaira, T.; Kawakami, T.; et al. Usefulness of albumin-bilirubin grade for evaluation of prognosis of 2584 Japanese patients with hepatocellular carcinoma. J. Gastroenterol. Hepatol. 2016, 31, 1031–1036. [Google Scholar] [CrossRef] [PubMed]
- Sonohara, F.; Yamada, S.; Tanaka, N.; Suenaga, M.; Takami, H.; Hayashi, M.; Niwa, Y.; Sugimoto, H.; Hattori, N.; Kanda, M.; et al. Perioperative and prognostic implication of albumin-bilirubin-TNM score in Child-Pugh class A hepatocellular carcinoma. Ann. Gastroenterol. Surg. 2018, 3, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Shao, Y.-Y.; Liu, T.-H.; Lee, Y.-H.; Hsu, C.-H.; Cheng, A.-L. Modified CLIP with objective liver reserve assessment retains prognosis prediction for patients with advanced hepatocellular carcinoma. J. Gastroenterol. Hepatol. 2016, 31, 1336–1341. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.W.H.; Chong, C.C.N.; Mo, F.K.F.; Wong, J.; Yeo, W.; Johnson, P.J.; Yu, S.; Lai, P.B.S.; To, K.-F.; Chan, S.L. Incorporating albumin-bilirubin grade into the cancer of the liver Italian program system for hepatocellular carcinoma. J. Gastroenterol. Hepatol. 2017, 32, 221–228. [Google Scholar] [CrossRef]
- Cai, X.-R.; Chen, Z.-H.; Liu, M.-M.; Lin, J.-X.; Zhang, X.-P.; Chen, J.; Lin, Q.; Ma, X.-K.; Wen, J.-Y.; Xie, S.-D.; et al. Modified CLIP score with the albumin-bilirubin grade retains prognostic value in HBV-related hepatocellular carcinoma patients treated with trans-catheter arterial chemoembolization therapy. J. Cancer 2018, 9, 2380–2388. [Google Scholar] [CrossRef] [Green Version]
- Elshaarawy, O.; Alkhatib, A.; ElHelbawy, M.; Gomaa, A.; Allam, N.; Alsebaey, A.; Rewisha, E.; Waked, I. Validation of modified albumin-bilirubin-TNM score as a prognostic model to evaluate patients with hepatocellular carcinoma. World J. Hepatol. 2019, 11, 542–552. [Google Scholar] [CrossRef] [PubMed]
- Khabbaz, R.C.; Lokken, R.P.; Chen, Y.-F.; Lipnik, A.J.; Bui, J.T.; Ray, C.E.; Gaba, R.C. Albumin–Bilirubin and Platelet–Albumin–Bilirubin Grades Do Not Predict Survival After Transjugular Intrahepatic Portosystemic Shunt Creation. Cardiovasc. Interv. Radiol. 2018, 41, 1029–1034. [Google Scholar] [CrossRef]
- Ronald, J.; Wang, Q.; Choi, S.; Suhocki, P.; Hall, M.; Smith, T.; Kim, C. Albumin-bilirubin grade versus MELD score for predicting survival after transjugular intrahepatic portosystemic shunt (TIPS) creation. Diagn. Interv. Imaging 2018, 99, 163–168. [Google Scholar] [CrossRef]
- Kim, K.M.; Shim, S.G.; Sinn, D.H.; Song, J.E.; Kim, B.S.; Kim, H.G. Child-Pugh, MELD, MELD-Na, and ALBI scores: Which liver function models best predicts prognosis for HCC patient with ascites? Scand. J. Gastroenterol. 2020, 55, 951–957. [Google Scholar] [CrossRef]
- Wu, J.-J.; Zhang, Z.-G.; Zhu, P.; Mba’Nbo-Koumpa, A.-A.; Zhang, B.; Chen, X.-P.; Shu, C.; Zhang, W.-G.; Feng, R.-J.; Li, G.-X. Comparative liver function models for ruptured hepatocellular carcinoma: A 10-year single center experience. Asian J. Surg. 2019, 42, 874–882. [Google Scholar] [CrossRef]
Figure 1.
Distribution of mALBI grades with the Child–Pugh score in 1850 HCC patients treated at Ehime Prefectural Central Hospital from 2000 to 2019.
Figure 1.
Distribution of mALBI grades with the Child–Pugh score in 1850 HCC patients treated at Ehime Prefectural Central Hospital from 2000 to 2019.


{kind=link}
Table 1.
Comparisons of the Child–Pugh classification with ALBI and mALBI grades.
| Child-Pugh Classification | ALBI/mALBI Grades | |
|---|---|---|
| Total Bilirubin | score 1: <2.0 mg/dL, score 2: 2.0–3.0 mg/dL, score 3: >3.0 mg/dL | Used (µmol/L) |
| Albumin | score 1: >3.5 g/dL, score 2: 2.8–3.5 g/dL, score 3: <2.8 g/dL | Used (g/L) |
| Prothrombin time | score 1: >70%, score 2: 40–70%, score 3: <40% | No use |
| Ascites | score 1: none, score 2: mild/controlled, score 3: moderate/refractory | No use |
| Encephalopathy | score 1: none, score 2: minimal, score 3: advanced | No use |
| Calculation for score | Sum up all scores and baseline score 5 | log10 bilirubin (µmol/L) × 0.66) + (albumin (g/L) × –0.085 |
| Classification | A 5–6 score, B 7–9 score, C 10–15 score | ALBI grade 1: ≤−2.60, grade 2: >−2.60 to ≤−1.39, grade 3 >−1.39.mALBI grade 2a: >−2.60 to ≤−2.27. grade 2b: >−2.27 to ≤−1.39. |
ALBI grade: albumin-bilirubin grade; mALBI grade: modified ALBI grade.
Table 2.
Overall survival in association with the ALBI grade for each therapeutic modality.
| Author | Area | No. of Patients | Child-Pugh A/B/C (%) | Co-Factors | Results | ||
|---|---|---|---|---|---|---|---|
| Liver transplantation | |||||||
| Tai [19] | Japan | 81 | NA | OS | ALBI 3 vs. MELD ≥ 16 = HR 3.26 (p = 0.004) vs. 2.22 (p = 0.079) | ||
| Kormberg [22] | Germany | 123 | 42.3/57.7/0 | Recurrence-free survival | AFP >100 ng/mL: HR 4.99, p < 0.001, ALBI 3: HR 3.52, p = 0.002 | ||
| Zang [23] | China | 272 | 22.8/51.5/25.7 | OS and complications | AUC for ALBI vs. MELD vs. Child–Pugh for predicting 30-day mortality: 0.702 vs. 0.669 vs. 0.540. AUC for ALBI vs. MELD vs. Child–Pugh for predicting postoperative bacterial pneumonia: 0.765 vs. 0.690 vs. 0.716. AUC for ALBI vs. MELD vs. Child–Pugh for predicting early allograft dysfunction: 0.659 vs. 0.621 vs. 0.630 | ||
| Surgical resection | |||||||
| Ho [25] | Taiwan | 645 | 93.8/6.2/0 | OS | AIC of ALBI vs. Child-Pugh vs. MELD: 3999.7 vs. 4013.0 vs. 4013.6 | ||
| Dong [26] | China | 654 solitary HCC | 100/0/0 | OS and recurrence | Five-year OS: ALBI 1 vs. 2 = 68.4% vs. 56.1%, p = 0.001. Five-year recurrence: ALBI 1 vs. 2 = 45.3% vs. 57.3%, p = 0.002 | ||
| Amisaki [27] | Japan | 136 | 100/0/0 | OS, RFS | Postoperative ALBI | OS: ALBI 3; HR 3.192, p = 0.035, RFS: ALBI 3; HR 2.397, p = 0.024, | |
| Zhang [28] | China | 338 | 91.1/8.9/0 | PHLF | AUC: ALBI vs. Child–Pugh class vs. MELD = 0.790 vs. 0.656 vs. 0.669 | ||
| Zou [29] | China | 473 | 90.3/9.7/0 | PHLF | AUC: Child–Pugh score vs. MELD vs. ICG-R15 vs. ALBI score = 0.665 vs. 0.649 vs. 0.668 vs. 0.745 | ||
| Ye [30] | China | 300 | 94.3/5.7/0 | OS and RFS | △ALBI score (>0.71 vs. ≤0.71) | Five-year OS and RFS: Low vs. high group = 84.2% and 46.9% vs. 59.7% vs. 29.3%, all p < 0.001 | |
| RFA | |||||||
| Chen [31] | Taiwan | 271 with BCLC stage 0 | NA | OS and RFS | OS: ALBI 2 or 3: HR 2.191, p = 0.005, RFS: HR 1.825, p = 0.001 | ||
| Oh [32] | Korea | 368 with BCLC stage 0 | 100/0/0 | OS | ALBI 2 (HR 2.32, p = 0.002) | ||
| Ho [33] | Taiwan | 499 | OS | AIC: ALBI vs. Child–Pugh vs. MELD = 3068.2 vs. 3097.3 vs. 3094.9 | |||
| Hiraoka [34] | Japan | 1101 with tumor (<3 cm, ≤3 tumors) | 76.5/23.5/0 | OS | AIC: ALBI vs. Child–Pugh = 5990.7 vs. 6015.4 | ||
| TACE | |||||||
| Khalid [37] | Pakistan | 71 | 46.5/49.3/4.2 | OS | ALBI score (HR 3.06, p = 0.0380) (Child-Pugh: HR 0.64, p = 0.09) | ||
| Izumoto [38] | Japan | 192 with BCLC-B stage | 84.4/15.6/0 | OS | ALBI grade 2 (HR 1.548, p = 0.048), AFP >100 ng/mL) (HR 1.540, p = 0.033), and TTTP (HR 2.157, p < 0.001) (Child–Pugh B did not remain) | ||
| Mohammed [42] | USA | 123 | 0/68/32 | Acute chronic liver failure 90 days after TACE | OR 3.99, p = 0.002, AUC 0.69 (ALBI score −1.39, sensitivity/specificity = 1.0/0.38) | ||
| TKIs | |||||||
| Abdel-Rahman [46] | Sorafenib arm of NCT00699374 | 544 | 100/0/0 | OS (sorafenib) | ALBI 2: HR 1.531, p < 0.001 ALBI 3: HR 1.570, p = 0.047 | ||
| Tada [47] | Japan | 567 | 76.7/22.8/0.5 | OS (sorafenib) | ALBI score had higher predictive power for OS from 1 to 800 days than Child–Pugh score using time-dependent ROC analysis | ||
| Kuo [48] | Taiwan | 260 | 100/0/0 | OS (sorafenib) | ALBI 2: HR 2.35, p < 0.001 | ||
| Hiraoka [62] | Japan | 152 | 90.1/9.9/0 | OS (lenvatinib) | mALBI grade | Prognostic factor for death in Cox hazard multiple analysis: mALBI 2b or 3 (HR 4.632, p = 0.004) [Child–Pugh score (7 or more) did not remain] (HR 2.543, p = 0.085) |
NA: not applicable; OS: overall survival; ALBI grade: albumin-bilirubin grade; MELD: model for end-stage liver disease; HR: hazard ratio; AFP: alpha-fetoprotein; AUC: area under the curve; RFS: recurrence-free survival; HCC: hepatocellular carcinoma; PHLF: posthepatectomy liver failure; ICG-R15: indocyanine green retention rate at 15 min; △ALBI score: postoperative ALBI score (postoperative day 1)—ALBI score (last test before operation); RFA: radiofrequency ablation; BCLC: Barcelona Clinic liver cancer staging; TACE: transcatheter arterial chemoembolization; TKIs: tyrosine kinase inhibitors; TTTP: time to TACE progression; ROC: receiver operating characteristic; mALBI grade: modified ALBI grade.
Table 3.
Total scoring staging systems using ALBI and mALBI grading.
| Authors | Area | No. of Patients | Results for Predicting OS | |
|---|---|---|---|---|
| Modified CLIP with ALBI grade | Shao [74] | Taiwan | 142 | AIC and c-index: ALBI-CLIP vs. CLIP = 995.0 vs. 1001.1, and 0.724 vs. 0.703, respectively |
| Modified CLIP with ALBI grade | Chan [75] | China | 1973 | AIC and c-index: ALBI-CLIP vs. CLIP = 15493.5 vs. 15534.3, and 0.789 vs. 0.785, respectively |
| Modified CLIP with ALBI grade | Cai [76] | China | 389 HBV-related patients treated with TACE | AIC: ALBI-CLIP vs. CLIP = 2620.2 vs. 2620.5, AUCs for one- and two-year survival: ALBI-CLIP vs. CLIP = 0.697 and 0.618 vs. 0.687 and 0.612, respectively |
| ALBI-T | Hiraoka [72] | Japan | 2584 | MST of score 0, 1, 2, 3, 4, and 5 of ALBI-T vs. JIS: 137.7, 83.2, 53.4, 27.4, 5.0, and 1.4 vs. 97.6, 74.9, 39.7, 15.0, 4.0, and 1.0 months |
| ALBI-T | Sonohara [73] | Japan | 235 treated with surgical resection (all Child-Pugh A) | ALBI-T 3, 4, 5 vs. 0, 1, 2: HR 1.94, p = 0.004 |
| mALBI-T | Hiraoka [17] | Japan | 6649 | AIC and c-index: mALBI-T vs. ALBI-T vs. JIS = 45,327.1 vs. 45,467.7 vs. 45,555.8 and 0.755 vs. 0.744 vs. 0.739, respectively |
ALBI grade: albumin-bilirubin grade; mALBI grade: modified ALBI grade; AIC: Akaike information criterion; CLIP: Cancer of the Liver Italian Program; AUC: area under the curve; HBV: hepatitis B virus; TACE: transcatheter arterial chemoembolization; MST: median survival time; ALBI-T: ALBI-TNM of LCSGJ; mALBI-T: mALBI-TNM stage of LCSGJ.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Hiraoka, A.; Kumada, T. Clinical Role of Newly Developed ALBI and mALBI Grades for Treatment of Hepatocellular Carcinoma. Appl. Sci. 2020, 10, 7178. https://doi.org/10.3390/app10207178
AMA Style
Hiraoka A, Kumada T. Clinical Role of Newly Developed ALBI and mALBI Grades for Treatment of Hepatocellular Carcinoma. Applied Sciences. 2020; 10(20):7178. https://doi.org/10.3390/app10207178
Chicago/Turabian StyleHiraoka, Atsushi, and Takashi Kumada. 2020. "Clinical Role of Newly Developed ALBI and mALBI Grades for Treatment of Hepatocellular Carcinoma" Applied Sciences 10, no. 20: 7178. https://doi.org/10.3390/app10207178
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.