Healthcare Applications of Artificial Intelligence and Analytics: A Review and Proposed Framework





1
Department of Informatics and Engineering, Université du Québec en Outaouais, 101, rue Saint-Jean-Bosco, Gatineau, QC J8X 3X7, Canada
2
Department of Administrative Sciences, Université du Québec en Outaouais, 101, rue Saint-Jean-Bosco, Gatineau, QC J8X 3X7, Canada
3
Sprott School of Business, Carleton University, 810 Dunton Tower 1125 Colonel By Drive Ottawa, ON K1S 5B6, Canada
4
Telfer School of Management, University of Ottawa, 55 Laurier Avenue East Ottawa, ON K1N 6N5, Canada
*
Author to whom correspondence should be addressed.
Appl. Sci. 2020, 10(18), 6553; https://doi.org/10.3390/app10186553
Submission received: 18 August 2020
/
Revised: 14 September 2020
/
Accepted: 17 September 2020
/
Published: 19 September 2020
(This article belongs to the Special Issue 10th Anniversary of Applied Sciences: Invited Papers in Applied Biosciences and Bioengineering Section)
Abstract
:Healthcare is considered as one of the most promising application areas for artificial intelligence and analytics (AIA) just after the emergence of the latter. AI combined to analytics technologies is increasingly changing medical practice and healthcare in an impressive way using efficient algorithms from various branches of information technology (IT). Indeed, numerous works are published every year in several universities and innovation centers worldwide, but there are concerns about progress in their effective success. There are growing examples of AIA being implemented in healthcare with promising results. This review paper summarizes the past 5 years of healthcare applications of AIA, across different techniques and medical specialties, and discusses the current issues and challenges, related to this revolutionary technology. A total of 24,782 articles were identified. The aim of this paper is to provide the research community with the necessary background to push this field even further and propose a framework that will help integrate diverse AIA technologies around patient needs in various healthcare contexts, especially for chronic care patients, who present the most complex comorbidities and care needs.
1. Introduction
The founding father of artificial intelligence (AI), Alan Turing, has defined this discipline as “the science and engineering of making machines, especially intelligent computer programs” [1]. Programs which enable computers to mimic human cognitive functions are called artificial intelligence systems. The beginning of AI is linked to philosophy, possibilities, demonstrations, fantasies, and imagination [2]. The IA field emerged in response to several simultaneous needs, opportunities, and interests.
AI combined with analytics (AIA) is increasingly adopted in many sectors, including healthcare. Indeed, medicine was one of the most effective use of Analytics and today a promising application area for AI. Research already started in the mid-20th century and applications were developed and proposed to clinicians to assist them in their practice. These applications include clinical decision support system, automated surgery, patient monitoring and assistance, management of healthcare, etc. The current methods used, as we will see in the next sections, are mainly based on knowledge discovery using data and machine learning, ontologies, and semantics, as well as reasoning. In this article, we survey the status of AI in healthcare during the last 5 years. We focus the review on five relevant technologies integrating AIA: data mining; ontologies, semantic reasoning, and ontology-extended clinical guidelines; clinical decision support systems; smart home; medical big data.
The choice of the different aspects of artificial intelligence discussed in our study is not fortuitous. Indeed, we noticed that they have a striking interest in the medical field, especially in recent years. Data mining algorithms are very often used in learning, prediction, and they are also used in imaging, voice processing, and even in all that is emotion and feeling. Ontologies, thanks to their reasoning ability, their usefulness as means of understanding, sharing, reuse, and integration, have gained ground in medicine. Both disciplines are used in clinical decision support systems that are useful in clinical practice to improve the quality of care. They are also used in smart homes to help persons suffering from cognitive deficiencies in their daily living activities. Medical big data is becoming more and more present in the medical field and its use for analytics is unavoidable.
2. Methodology
To perform the literature review, we relied in great part on the PRISMA Statement and flowchart [3]. Our main source was Scopus because it is the largest abstract and indexing database in the world (according to Elsevier) and thus includes a very expanded spectrum of journals. A detailed search of publication of papers about big data in healthcare between 2016 and 2020 was used for review. The review included only English language publications with the search strategy in Table 1. Our strategy of research is composed of seven steps: (1) decompose each subject into concepts; (2) enrich its vocabulary that means for each of the concepts identified, the vocabulary is enriched by listing synonyms or equivalent terms; (3) understand the logical links (AND, OR, NOT) between words, in order to place them correctly; (4) check the particularities of the search tool to be used, if quotes are permitted, for example; (5) formulate the first research request; (6) analyze the results; (7) improve the query. We used the keywords that directly describe the disciplines we were interested in. We chose the appropriate combination operators. Asterisks at the end of the word ‘a’* search for multiple variants of ‘a’ in the database. The code [tiab] restricts the query to search in the title and the abstract of the paper, sometimes using acronyms for specific algorithms, e.g., Support Vector Machine (SVM), K-nearest neighbor (KNN).
As shown in Table 2, our search strategy resulted in the following tally of articles as per five AIA applications. We report here the number of articles at each stage of our review. The criteria for selection at each stage are as follows:
- Found: articles matching our search strategy of AIA applications.
- Relevant: articles relevant as it presents one of the AIA applications we focused on.
- Cited: article cited in our review as it made significant advances complementary to others.
The first column of Table 2 (found) refers to the papers found in Scopus that respond to the key words used in the request search. As the number of articles found is huge, we cannot cite all of them, we cite the most relevant in terms of novelty in artificial intelligence in healthcare.
3. AI Applications
3.1. Data Mining
Data mining is the process of extraction of knowledge and features from data using automatic or semiautomatic methods, it combines machine learning and data science. Indeed, data mining describes, discovers relevant patterns, associations, and knowledge to make predictions, according to pre-established criteria. In healthcare, data mining is becoming increasingly popular and essential. There is large potential for use of data mining in healthcare. These can be grouped as the management of healthcare, evaluation of diagnosis and treatment effectiveness; customer relationship management; detection of fraud and abuse.
Applications of data mining techniques in breast cancer diagnosis, treatment, and prognosis was the subject of a study provided in [3]. Generally, two phases for making the decisions are distinguished in the medical world: differential diagnosis (DD) and final or provisional diagnosis (FD). In the first phase the medical history of the patients, the symptoms of disease, the results of different laboratory tests (blood testing, etc.) are perceived by physicians as the input data. The latter are handled by physicians based on their medical knowledge for disease diagnosis. In the second stage and given the identified disease, first recommendations and treatments would start. Until now, one of the important challenges in cancer treatment is to determine the most common symptoms that can help in cancer diagnosis. There were many research studies conducted to identify the patterns of cancers and create a smart method for diagnosis of tumors in the early stages. The method also suggests the best treatments. To identify kinds of cancers (benign breast tumors from malignant ones), most of physicians undertake surgical biopsy. However, most of them believed that biopsy is a critical task and should be prevented when possible. Consequently, proposing a smart system that can help physicians to determine the type of cancer and avoid surgical biopsy would be helpful for patients as well as for physicians. In [3], the authors attempted to cover research works related to diagnosis of breast cancers, when applying various techniques of data mining along with their results. Most of the reviewed research works (on diagnosis, treatment, or prognosis of breast cancers) are concerned with comparing the accuracy rate of data mining various algorithms or techniques. There is not yet a tool to automatically diagnose or predict breast cancer. Further, there is no research work that applies customized features to offer the best treatments to patients.
In [4] Lashari et al. reviewed and analyzed the current medical data classification practices, advancements, and prospects using data mining. They highlighted the main approaches used to enhance classification accuracy. There is a wide literature which suggests that data mining is very effective for the classification task.
Among the algorithms of data mining used in healthcare applications are the following: decision trees [5,6,7,8,9], neural networks [10,11,12,13,14,15], SVM [16,17,18,19], k-means [20,21,22], logical regression [23], KNN (K-nearest neighbors) [24], and naïve Bayes classifier [25,26,27]. These algorithms can be combined to improve the data analysis process as it is done in [28] where the authors combined random forest, decision trees, neural network, SVM, logistic regression, and KNN algorithms to find out the health and anticipate the mortality risks of patients contaminated with COVID-19. The purpose of the application is to help hospitals to decide on the patient priority order when the system is submerged and avoid delays in dispensing to patients the needed care.
COVID-19 has had a lot of interest from the medical informatics community since its emergence. Deep learning algorithms are widely used as in [29] where they are combined with CT images to screen for COVID-19. The authors proposed a deep learning algorithm framework to extract specific graphical features from CT images and propose a clinical diagnosis in front of the pathogenic test. The ultimate objective is saving critical time for disease control. To estimate and predict mortality caused by COVID-19 in real time, a new methodology is reported in [29]. This methodology consists of the Patient Information Based Algorithm (PIBA), using available data gathered during an epidemic. To evaluate the methodology, the authors used preliminary data from China, the algorithm was successfully applied to estimate the death rate and predict the death numbers in the Korean population. According to the authors the algorithm can be used to estimate the death rate of a new infectious disease in real-time and to predict future deaths. Another interesting work proposed an automatic detection system as a fast alternative diagnosis option to prevent the spread of COVID-19 [30]. The approach consists of using three different convolutional neural network-based models (ResNet50, InceptionV3, and InceptionResNetV2) for the detection of a coronavirus pneumonia infected patient using chest X-ray radiographs. Among the results of this work is that chest X-ray images are a very good tool for the detection of COVID-19.
3.2. Ontologies and Semantic Reasoning
An ontology as defined by Gruber is an explicit specification of a conceptualization [31]. It refers to an engineering artifact made up of a specific vocabulary describing a certain reality using a set of explicit assumptions regarding the intended meaning of the vocabulary words. With the explosion of data, the number of sources, and their heterogeneity, the concept of ontology has become a very important field of research.
Medicine has been one of the preferred fields of experimentation for ontologies due to the tremendous progress in this domain. The interoperability and reusability are two of the main criteria that these ontologies must satisfy. They are designed and shared by the scientific community through four main resources: (i) the OBOFoundry (http://www.obofoundry.org/) whose objective is to develop a family of interoperable ontologies that are both well-formed and scientifically accurate. It holds 175 ontologies (as of May 2020) covering, among others, diseases, diagnosis, treatment, anatomy, etc.; (ii) the BioPortal [32], that aims to create software and support services for the application of ontologies in biomedical science. It holds 1016 (as of May 2020) ontologies and is run by the NIH National Center for Biomedical Ontology; (iii) the Ontology Look-up Service (https://www.ebi.ac.uk/ols/index) that is a repository of biomedical ontologies. It holds 237 (as of September 2019) ontologies and aims to provide means to find, query, and navigate biomedical ontologies and controlled vocabularies; (iv) UMLS (https://www.nlm.nih.gov/research/umls/index.html). The developed ontologies cover diagnosis and treatment of multiple diseases such as diabetes, breast cancer, Alzheimer’s, hypertension, asthma, etc. They also represent drug, cell, phenotype, radiology, anatomy, chemical, infectious diseases, clinical search, psychology, nursing, laboratory, units of measurement, mass spectrometry, epigenetic, biology system, etc. Very recently, COVID-19 was integrated in Infectious Disease Ontology (IDO) that provides all aspects of the infectious disease domain [33].
In [34], the authors devised the role of ontologies in bioresearch in general, either biological or biomedical. They showed interesting results from a functional perspective. The interest of the article resides in the description of different aspects of ontologies in biological and biomedical domains. Four main features are generally present in almost all ontologies, and when combined they play an important role in the success of ontologies: provision of standard identifiers for classes and relations that represent the phenomena within a domain; provision of a vocabulary for a domain; provision of metadata that describes the intended meaning of the classes and relations in ontologies; provision of machine-readable axioms and definitions that enable computational access to some aspects of the meaning of classes and relations. A functional perspective on ontologies in biology and biomedicine is provided by the authors with a special focus on what ontologies can do and describing how they can be used in support of integrative research. They also outlined perspectives for using ontologies in data-driven science, their application in structured data mining and machine learning applications.
According to [35], in the past decade in some east Asian countries, air pollution became a serious threat to public health. In Taiwan, pollution and related illnesses became a serious problem, where sore throat, asthma, bronchitis, sinusitis, laryngitis, etc., are some of the common symptoms and illnesses. An ontology-based herb therapy recommendation web for respiration system health was proposed by the authors. The aim was to sort out the knowledge and build an easy-access web system. The latter provides reliable and comprehensive knowledge of herbs to improve respiration system wellness. The feedback from users confirm the practicality and usefulness of the designed system. The use of herbs in daily diet and as alternative treatments is not new, but it still needs great promotion and education as many people have gone to hospitals to get quick and easy pills to feel better. Promoting this knowledge remains a long and great challenge.
On the other hand Saleha Asad et al. [36] were interested in the use of an ontology to detect drug abuse epidemiology. The authors improved an existing ontology-based system (PREDOSE for PREscription Drug abuse Online Surveillance and Epidemiology) in which the objective was to extract the relevant knowledge from websites and blogs on illicit drug usage. PREDOSE does not cover the brand names and slang terms of drugs, nor the risk factors related to the illicit drugs. It does not provide the information on drugs that are prohibited in different countries. The proposed system aims to compensate for any lack of PREDOSE by providing useful information related to drug addiction and its prohibited information. Thanks to this new approach, users can query the knowledge base for information such as street names or slang terms for drugs. Users can also obtain information on the different company names for a single chemical formulation of a drug, as well as their side effects. Some information is updated and expanded in the approach as the number of classes has increased from 43 to 114. In addition, the model gains efficiency by defining semantic rules.
In [37] the authors used a Semantic-Based Knowledge Management System (SKMS) that supports knowledge acquisition and integrates various approaches to provide a systematic practical platform to knowledge practitioners. The aim of SKMS is to identify roles of healthcare professionals, duties that can be performed according to personnel competencies, and projects that are conducted as a part of tasks to complete defined goals of clinical processes. In this work, the authors proposed an ontology-based approach to investigate implicit knowledge acquisition and information flow issues. SKMS is useful to assist providing the right information to right users as needed in different tasks to carry out activities in processes of healthcare units. This framework supports tacit and explicit knowledge acquisition management. It provides a systematic way to acquire implicit knowledge from subject matter experts or knowledge mentors, model it formally, and transform it into a machine-readable form to develop a health information system (HIS) that provides a variety of health services that can better meet the needs of health care professionals and users. The goal of the ontological-based modelling method is inviting the organization to move towards patient-centered systems, enlarge opportunities, and simplify reuse of existing healthcare practices for new reform initiatives. Using an ontology gives new vision to manage knowledge and provides help to develop HIS with different and new implementation strategies.
The work in [38] focused on the evaluation of the ability of crowdsourcing methods to detect errors in SNOMED CT (Systematized Nomenclature of Medicine Clinical Terms) and to investigate the demanding challenges of upgradable ontology verification. The authors presented a methodology to crowdsource ontology verification that uses micro tasking combined with a Bayesian classifier. The results of the study showed that the crowd can indeed identify errors in SNOMED CT that experts also find, which suggests that the proposed method will likely perform well on similar ontologies. When experts are unavailable, added to limitation of budget, or width of the ontology which makes it difficult to evaluate it manually, we can use the crowd which can be particularly useful. It can address the challenges of scalable ontology verification, completing not only intuitive, common-sense tasks, but also expert-level, knowledge-intensive tasks. According to the results of this study, crowdsourcing may help to solve problems that require considerable biomedical expertise.
The research [39] published in Transcultural Psychiatry is a profound critic of care in American eating disorders treatment. The author gave the example of a patient and developed all the ideas regarding ontology, recognition, and elusiveness of care in the defined context. Clinical management of eating disorders is both central and elusive, both an organizing principle and an ever-receding horizon. The care for people with eating disorders is the clinic’s responsibility, which is meant to work on meeting their medical, social, and psychological needs. The problem is that the resources needed to provide that care are not ultimately held by the clinic itself but are gate kept by managed care companies. Those companies manage care, and they have the ultimate decision on who will receive care or not, they also fix the conditions, and of what that care will consist of. In the managed care framework, the fewer resources one needs, the better a patient one is seen to be, a stance that perilously mirrors eating disorders themselves. The concept of ‘‘care’’ operates across several domains simultaneously, sometimes folding back on itself to produce oblique expressions or even cause harm. Managed care companies reviewed the treatment progress of the patients on a semiweekly basis, assessing the degree to which they were proceeding along expected recovery trajectories. Satisfactory progress is assessed, and the treatment coverage could be terminated at the wish of the companies. A patient can be judged to be chronically manipulative, and could be forced to go out of treatment, either by the termination of insurance benefits or by the clinic asking her to leave. The logic of care in this context thus perpetuates a paradoxical tearing apart of the client’s agency, which in turn makes care an ever-changing, mutable, and elusive goal.
Additionally, many ontologies were developed to diagnose and treat diseases such as diabetes mellitus [40,41,42], liver cancer [43], myocardial infarction [44], dermatosis [45], hypertension [46], Ebola virus infection [47], fibrotic interstitial lung disease [48], breast cancer [49,50], pneumonia [51,52,53], and Alzheimer’s [54]. Some ontologies are for differential diagnosis [55,56,57] and others for drugs [58,59,60].
Finally, one of the key areas of semantic applications in healthcare is Ontology-Extended Clinical Guidelines. OpenClinical.net knowledge sharing project [61] provides a sharable knowledge base for open access and open source repository. Its operationalization is governed by four principles such as supporting community to build, document and share models of clinical expertise, providing open access to the content for clinical and research use, ensuring fairness in recognition of efforts and value created by the users of the tool, and empowering them to disseminate their expert knowledge. The solutions offered by the tool are ontology driven and they help understanding, capturing, and organizing knowledge that concerns medical item management used in hospitals.
3.3. Clinical Decision Support Systems
The medical informatics community is very interested in developing methods and tools to support clinical processes, varying from reminders, recommendations, and messaging systems, to decision support, treatment planning, and clinical workflow services. Clinical decision support systems (CDSS) that aim to help healthcare providers to make better decisions and improve patient care were proposed more than a half-century ago. This help concerns both diagnosis and treatment [62]. According to several studies, if used effectively, this aid could improve the quality, safety, and high performance of health care [63,64,65,66]. The lynchpin of CDSS success is well defined in [67] “The goal of CDSS is to provide the right information, to the right person, in the right format, through the right channel, at the right point in workflow to improve health and health care decisions and outcomes”.
An interesting article [68] discusses the use of fuzzy decision support systems for diabetes diagnosis. The authors presented an ontology-based system and implemented a new semantically interpretable FRBS (Fuzzy Rule-Based Systems) framework to diagnose diabetes. To provide a more intuitive and accurate design, the authors used in their framework multiple aspects of knowledge-fuzzy inference, ontology reasoning, and a fuzzy analytical hierarchy process (FAHP). The proposed system offers numerous unique and essential enhancements to the implementation of an accurate, dynamic, semantically intelligent, and interpretable CDSS. In the fuzzy rules evaluation process the ontology semantic similarity of diabetes complications are considered, as well as symptoms concepts. The proposed system helps physicians and patients to accurately diagnose diabetes mellitus as it was shown in the testing of the framework using a real data set. The authors worked on a hospital in Egypt, they combined the proposed FRBS using JAVA APIs and produced the hierarchical FRBS (H-FRBS). In an actual hospital environment, although all features are required, certain features are more critical than others. For example, diabetes symptoms are more important than lipid profile. Moreover, in some cases, not all features are known for a given patient, and physicians must decide with the available information. The resulting system can make decisions with different combinations of data sources and with different confidence levels. According to the authors the framework is smart and can provide more accurate results than existing studies. Further improvements can be made to extend its functionality as it was built within an open architecture. The system can even be applied to any other medical field in a simple and easy way. Its current limitations are that it does not yet allow full interoperability with the HER (Electronic Health Records) system and does not consider data regarding patients from social media.
The paper [69] presents a type-2 fuzzy ontology-aided recommendation system. The system monitors the patient’s body by recommending diets with specific foods and drugs. The system begins first by extracting the values of patient risk factors. Then, it determines the patient’s health condition via wearable sensors. At last, it delivers recommendations consisting of diabetes-specific prescriptions for a smart medicine box and food for a smart refrigerator. Protégé Web Ontology Language (OWL)-2 tools are used in this ontology, the aim is to deliver decision-making knowledge based on patient information. The recommendation process uses Semantic Web Rule Language (SWRL) rules and fuzzy logic. The performance of the proposed ontology was evaluated after the development of each phase to measure the improvement level. This system can effectively overcome the load of chronic patients on hospitals, help physicians to automatically retrieve patient physiological information for diagnoses, and can assist old patients with chronic diseases for long-term care without continuous visits to physicians.
In the context of the patient’s infectious illness and comorbidities, the authors in [70] proposed an approach to the problem of inflammatory syndrome identification. It consists of implementing a computerized early warning tool for sepsis in which they researched to determine clinical metric performance of a cloud-based computerized sepsis clinical decision support system (CDSS), understand the epidemiology of sepsis, and identify opportunities for quality improvement. The study was conducted in several hospitals in different regions of the United States. According to the authors the cloud-based sepsis CDSS integrated with enterprise EHR systems is an approach toward early recognition of sepsis in a hospital setting.
Middleton et al. undertook a retrospective study over 25 years of use of CDSS since 1990 [71], which was designed to provide clinicians, staff, and patients with knowledge and person-specific information. Those system filters filter information and present it at convenient times, to enhance health and health care. The authors subscribe to the belief that, as a component of a Learning Health System CDSS is essential where a cycle of information is created from data generation, to aggregation, analysis, knowledge creation, knowledge dissemination and use, and ongoing measurement for continuous feedback and refinement. Over time, evolution of the techniques and approaches made it more and more efficient for practitioners and CDSS became fundamental. CDSS is evolving in important ways: increasing in availability of electronic data and knowledge bases for CDSS from industry to support traditional evidence-based medicine. Electronic health records provide data that are being aggregated in efficient ways to support the notion of ‘practice-based’ evidence. They help to support developing new forms of inference for CDSS. Middleton et al. reflected on the number of main dimensions of CDSS which adversely impact the effective implementation and use of CDSS in clinical practice, and certain developments which may accelerate its use. In summary, the authors suggested that the evolution and increased use of CDSS in practice is inevitable given the explosion of biomedical knowledge, and the pressure to improve quality and lower costs in value-based care.
In [72], the interest in developing a CDSS for pediatric abdominal pain in an Emergency Department is related to an important demand for organizing the process. Emergencies are under heavy pressure on a regular basis. The authors were interested in abdominal pain with focus on appendicitis of children. Diagnosis of appendicitis in children is challenging. The CDSS was designed to help guide management of pediatric patients with acute abdominal pain within the Health Care Systems Research Network (HCSRN). The system uses, when available, prior diagnoses, medicines, laboratory, and other clinical data. At intervention sites, “risk for appendicitis” is defined and assigned in exact terms. The system provides targeted recommendations regarding management and a summary that can be pasted into the clinical note. At this stage, the system is ongoing at two large health care systems in the HCSRN which each have histories of successfully developing, implementing, and evaluating CDSS systems. Experience from HCSRN sites was of great importance and helped the study team. Using the collaborative approach to problem solving may have been difficult to achieve with organizations outside of the network. The challenge remains in finding the balance between achieving target enrolment and enrolling the appropriate target population.
Fuzzy sets can be defined from statistical information and rules for constructing CDSSs are, in this case, based on fuzzy logic. In [73], an approach is proposed to make use of statistical information describing dependence between input variables and output classes. The approach is based on possibility theory. The goal was to obtain fuzzy partitions particularly useful for classification purposes and suitable for medical applications. Here we are in the presence of a technical paper in which the authors conducted field studies to calibrate their model. CDSSs are applied to single patients, therefore conclusions are better described by the membership of patient’s characteristics to different classes, which can be encoded by possibility measures. Moreover, DSSs mostly give results in the form of a single, most reliable class.
Selection and implementation of a CDSS for imaging was a subject study proposed in [74]. The tool presented as a procedure is intended to help radiologists ensure that they can understand and contribute to the process of implementing the CDSS for imaging. The efficacy of imaging CDSS was discussed in detail, the authors gave insightful discussion on the legislation and evidence of the system. They also showed number of considerations for selecting a CDSS vendor, tips for configuring CDSS in a fashion consistent with departmental goals, and pointers for implementation and change management. It was shown that number of studies have demonstrated a reduction in imaging utilization growth and improved appropriateness of advanced imaging requests after the implementation of imaging CDSS. The need for new CDSS is driven by different changes in legislation regarding healthcare. The study showed evidence that careful implementation of CDSS can have a significant impact on inappropriate imaging utilization. Careful planning is required when using CDSS, it can become an administrative obstacle to providing high-quality patient care. Radiologists should pay careful attention that CDSS is configured in a way that facilitates lasting, collaborative relationships with referring physicians and highlights the value of the radiologist as a clinical consultant rather than a clinical commodity.
Patient privacy preservation in clinical decision support systems was the focus of [73]. Indeed, the protection of patient privacy when using clinical decision systems became an important subject with the exponentially increasing data used. The authors proposed a new privacy-preserving patient-oriented CDSS. The system helps clinician to complementarily diagnose the risk of patients’ disease by preserving their privacy. The past patients’ historical data are stored in cloud and can be used to train a Bayesian classifier algorithm. Information is preserved without leaking any patient medical data. The algorithm uses training data to classify and compute the disease risk for new patients.
The authors of [75] were interested in how a CDSS can help in using Traumatic Brain Injury (TBI) Prediction Rules. The importance of prediction rules and guidelines lies in their ability to safely impact care. The primary aim of the authors was to determine whether implementing the two age based PECARN TBI (Pediatric Emergency Care Applied Research Network) clinical prediction rules by using a multifaceted intervention, centered around computerized CDSS, would decrease the rate of cranial CT (Computed Tomography) use for children with minor blunt head trauma at very low risk of TBIs, without increasing the rate of missed TBIs. In a second stage the aim of the authors was to determine whether CDSS that provided risk data for TBI for all children with minor blunt head trauma would decrease CT use. According to the authors, the implementation of TBI prediction rules and provision of risks of TBI by using computerized CDSS was associated with modest but variable decreases in rates of CT use for children at very low risk of TBI and for all children with minor blunt head trauma, without increasing the rate of missed injuries. However, decreased CT rates were inconsistent.
The overall goal for the study presented in [76] is to identify decision complexity and its constituents in combination with cognitive strategies to inform the design of health information technology. It was important to provide valuable cognitive support to clinicians. The authors focused on the following research questions:
- What factors are associated with decision-making complexity experienced by ID experts?
- What cognitive strategies do ID experts use to deal with complexity?
Several medical experts were interviewed for the study. A structured documentation process of coding within a systematic examination of individual interviews were included in the procedure, in which the ID experts have a long experience of on average 18.5 years. Out of 10 ID experts, two were female and eight were male. Identification of complexity factors in the procedure needed use of cognitive strategies which can be of help to the ID experts. It was shown from the study that a way to rework the paradigm of evidence-based medicine exists and can enhance the management of complex clinical tasks. It was typically assumed from the practice guidelines of the reviewers that leeway for clinical judgement is allowed as the experienced clinician is assessing the patient. However, clinicians are prompt to accept the rule-based recommendations as the guidelines are incorporated into the clinical decision support systems. ID experts deal with decision complexity using different mechanisms. Some cognitive factors contribute to this decision complexity, in which we can cite:
- overall clinical picture does not match the pattern,
- lack of comprehension of the situation, and
- social and emotional pressures.
There are multiple facets and potentials of sentiments analysis; the authors of [77] managed to describe them in the context of medicine and healthcare for several reasons. Various persons are involved in a treatment process; we can find physicians of different specialties, therapists, and nurses. The importance of identifying personal observations and attitudes of a physician is highly acknowledged as they play a role when appearing in medical records. They permit having a complete view of a patient’s health status, and other healthcare professionals will benefit from it. Observations or experiences in contrast to examinations results, are communicated in an unstructured way in reports and documents. Examination results on the other hand are often reported in a structured manner. That is why it is important to pay attention when extracting opinions from observations or examination results. They are very helpful in assessing clinical data and monitoring health status of patients. Automated decision support is made easier for practitioners. The medical conditions of a patient impact his life even though clinical documents are often written in an objective manner, for this reason sentiment analysis is of importance and helps to determine the impact from those written documents. Sentiment lexicons are usual in approaches that deal with sentiment analysis [78,79,80].
The authors of [77] provide an important basis for recognizing sentiment terms and patterns of sentiment expressions in natural language texts. Existing approaches to sentiment analysis from medical web data are either machine-learning based or rule-based. The authors worked on technical topics in which they expected a similarity to clinical narratives. The aim of their analysis is to examine the language and sentiment expressions in clinical narratives and medical social media. They used thousands of entries from different data sources to perform the experiment. Within a quantitative comparison, they analyzed and compared the word usage of the six text types: (1) nurse letter; (2) discharge summaries; (3) drug reviews; (4) Medblogs; and (5) Slashdot interviews. This analysis could be used for many purposes. Uncertainty, attitudes, and implicit sentiment could be collected and considered in clinical decision-making. Solutions for sentiment analysis lay in the construction of a domain-specific sentiment lexicon and the development of methods that allow sentiment to be judged depending on the context.
The IBM Watson [81] is a CDSS that includes both machine learning and natural language processing modules, and has made promising progress in oncology. In a cancer, 99% of the treatment recommendations made from Watson are like the physician decisions. Moreover, Watson cooperated with Quest Diagnostics to offer the AI Genetic Diagnostic Analysis. Further work needs to be done on standardizing methods for knowledge and data representation, CDSS implementation in clinical care environments, and knowledge exchange.
A final example is the recommender system called DeepSurv [82] uses a neural network to recommend personalized treatments according the patients’ covariates and predict the effect of treatment options on a patient’s risk.
Overall, CDSS technology remains one of the key areas of AIA applications in healthcare. Their degree of advancement is by far the most mature, but still offers opportunities for innovation.
3.4. Smart Homes
A smart home is the residence that uses a set of devices that connect via a network, most commonly a local LAN (Local Area Network) or the internet. These devices include sensors, RFID (Radio Frequency Identification), and other appliances connected to the Internet of Things (IoT) that can be remotely monitored and accessed. It is a new paradigm that aims to provide services that respond to the perceived needs of the users and enhance domestic comfort, convenience, security, and leisure. They play an important role for elderly persons and health care technologies. Smart homes are very seductive and attract a lot of researchers. Indeed, several works tackled human activity recognition in smart homes which plays an important role in people’s daily lives. Successful human activity recognition applications include activity recognition [83,84,85,86,87,88,89,90,91,92], gesture recognition [93,94], home behavior analysis [95,96], and emotion recognition [97,98]. Living assistance is another aspect of research in the smart home context. These systems are used to provide assistance, in particular to people with cognitive deficiencies such as dementia [99]. The authors of [100] reported a new protocol named Ergo to address smart homes for assisted living. The developed protocol has been used in an old home built in 1938 which was converted into a smart home with the use of sensing technologies. It predicts wellness of a resident through the monitoring of different appliances used by him/her and his/her movements.
In [101], the authors were interested in assisting patients with sclerosis disease in a smart home and the authors of [102] studied the influence of expressive speech on automatic speech recognition performances and applied their approach on elderly people assistance.
The authors of [103] propose a system, for smart homes, which combines Internet of Things (IoT) and big data analytics technology with fog and cloud computing. The challenge is related to developing fast solutions that can handle large volumes of unstructured smart home data. Fog computing is of importance as it provides fast near real-time analytics while the abundance of computing and storage resources in the cloud system is used to carry out computationally intensive applications.
An approach by combining knowledge-driven with data-driven reasoning to permit activity models to evolve and adapt automatically based on users’ particularities was proposed in [104]. The reasoning is knowledge-driven in this case and the authors made it able to infer an initial activity model. At upper stage, the model will be trained using data to produce a dynamic activity model that learns users’ varying actions. The results of the study showed that the learned activity model yields significantly higher recognition rates than the initial activity model.
RUDO [105] is a home ambient intelligence system that was designed to help blind people living with sighted people. This system helps blind people through a single user interface that helps by means of work on a computer, writing in Braille on a regular keyboard, etc. RUDO increases their independence of these people and creates conditions that allow them to become fully involved.
We notice that there are many patents about smart homes. The authors of [106] developed a device telemetry circuit to detect electrical anomalies in a plurality of smart home devices. In [107], systems and methods of providing status information in a smart home security detection system to a user are developed. Once the sensor has detected and received identifying information from an electronic device, a controller device determines whether this detected identifying information is from the electronic device of an authorized user and provides an operational status message to the electronic device.
It is important to mention that smart homes are concerned with big data [103]. This is what makes the use of the data mining and machine learning interesting in predicting, detecting, and assisting in smart home contexts.
Smart homes that are becoming more and more popular within the scientific community and end user are facing five barriers [108]: (1) the fit with users’ current and changing lifestyles; (2) the ease with which smart home technologies can be administered; (3) interoperability between systems; (4) reliability; (5) privacy and security. Other barriers in their adoption are high cost, poor usability, inflexibility, and a lack of general user involvement.
Despite the progress within the scientific community on researching innovative solutions for smart homes, their adoption still falls short of end-user needs, prompting search for new strategies.
3.5. Medical Big Data
Big data refers to large and varied sets of information that are growing at a very rapid rate. It is characterized by the 10 V: volume, velocity, variety, veracity, value, validity, variability, virality, and visualization [109]. Medical big data are distinct from big data of other disciplines, and they are also different from traditional clinical epidemiology data. Big data technology is applied on predictive modeling and clinical decision support, research, safety surveillance, disease, and public health. We find medical big data in different circles: in clinical registries, electronic health records, biometric data, administrative claim records, patient reported data, medical imaging, biomarker data, prospective cohort studies, etc. As the sources of data are different, the dimensions of data evolve and become complex as large size, disparate sources, multiple scales, incongruences, incompleteness, and complexity are encountered.
In the literature, most of the published papers concern the usefulness of big data in the medical field, the dangers as well as the perspectives and challenges. Big data shows effectiveness across the entire range of public health disciplines. This ability ranges from “monitoring population health in real-time” to develop “definitive extents and databases on the occurrence of many diseases” [110]. Indeed, the health areas that use of big data include public health [111,112,113], environmental health research [114], epidemiology [112,115,116], infectious disease [110,113,117], sleep science [118], maternal and child health [119,120], safety and occupational health [121,122], healthy food and nutrition [123,124,125], and smart homes [103,126,127]. There is optimism and evidence for big data’s value in public health, both in research and in intervention.
The authors of [117] studied the opportunities for using big data for global infectious disease surveillance. They estimate that the big data will massively improve the granularity and timeliness of available epidemiological information with hybrid systems enhancing traditional surveillance systems, and better prospects for accurate infectious disease models and forecasts.
Data mining is very used in the big data context, not to say that they are very connected. We know that the data mining algorithms are more performant when the volume of data is very large. As an example, the authors in [128] introduce the modern plastic surgeon to machine learning and computational interpretation of big data.
Application of big data analytics in medical domain is promising. Therefore, it is critical to point out some of challenges for big data applications in healthcare [129]: (1) the evidence of practical benefits of big data analytics is scarce; (2) there are many methodological issues, such as data quality, data inconsistency and instability, limitations of observational studies, validation, analytical issues, and legal issues.
Clinical practice needs to integrate big data analytics and take advantage from it. The authors of [130] assume that big data research in health informatics has not yet gained popularity in cardiology, but there is great potential for its value in research and clinical cardiology.
4. Discussion and Framework
The five key AIA applications reviewed were chosen due to their higher extent of application, but there are many more healthcare technologies and application opportunities.
In healthcare, we noticed that AI is very focused on applying data mining algorithms on various problems such as diagnosis and treatment. That allows automated systems to make predictions and recommendations. Indeed, a data mining algorithm is used to learn a model to best predict the decision variable of a new example. It can also make associations between different frequent item sets and generate association rules with a certain confidence degree that can be used in prediction.
Artificial intelligence raises many hopes in the healthcare sector even though its real implementation in the hospital environment and the daily lives of patients remains reluctant. Indeed, development of AI systems in health care is accompanied by ethical issues inherent to their use. Concerns about the protection of privacy, confidentiality, and even intimacy are worrisome. There are also challenges with respect to the free and informed consent of patients.
Despite the great advantages of using big data in healthcare and artificial intelligence since the analysis of large volumes of data leads to better decisions, its use raises a few problems related in particular to security and privacy (often personal data, if not sensitive). These represent threats for smart homes adoption, with its extensive use of big data and data mining. Finally, it is not always possible to explain the reasons that lead AI systems to make recommendations and decisions, even if we know that it is data mining algorithms and ontologies that are used. This leads to considerations about the lack of transparency—the AI black box.
AI applications can improve healthcare quality in hospitals on one hand, and on the other hand they can provide an efficient assistance to patients with difficulties in their daily life even outside of hospitals. AI in healthcare entails reducing medical errors and adverse events. Nevertheless, there is also what is called complacency in automation that threatens safety of AI in healthcare. In case of repeated use, physicians, especially those who are very busy, may accept AI systems guidance and transfer to them the responsibility even to make all decisions. These systems are given more weight than they deserve. Physicians may unconsciously learn to avoid available alternatives when an AI system repeatedly demonstrates that it is consistent with their diagnoses. We must balance the potential for improvement against the risk of negative results.
AI also faces another major challenge in health: its results must be interpretable by humans in a consistent manner. For example, interpretation of imaging tests is a common cause of misdiagnosis especially in the diagnosis of pneumonia. Hence, AI has been applied in the settings of automated chest radiograph interpretation by using machine learning and deep learning algorithms, but many limitations were identified [138].
While our review is by no means exhaustive, their convergence may help us show the many more areas requiring further research, especially providing more ample empirical evidence for extensive field deployment. This requires applying AIA to serve patients within a complex environment, involving a degree of variability that is often overlooked or hard to reproduce in clinical informatics studies.
To help future research, we propose an innovative architecture to integrate intelligent systems to help guide the delivery of primary healthcare. As presented in Figure 1, our framework can help integrate diverse AIA technologies around patient needs in various healthcare contexts, especially for complex cases (e.g., chronic care) who present comorbidities requiring coordination. This means that AIA technologies, features, and applications are linked to health outcomes directly, allowing a better representation of patient concerns in AIA design. A patient’s lifecycle spans within and beyond the healthcare system, allowing to monitor and diagnose health issues at all stages. The information is thereby generated, captured by AIA technology, and translated into intelligent system applications.
To link this health informatics framework to medical evidence, we build upon the Expanded Chronic Care Model (ECCM) from [139], based on [140]. Working within a modern, integrated primary healthcare network through advanced collaborative IT solutions, we focus on leveraging the growing amount of patient-centric Big Data available to care providers. Intelligent systems allow the automated guidance of the patient’s service pathway. Figure 1 presents this three-step cycle, integrating the five AIA technologies reviewed:
- Extraction of optimal rules and trajectories, integration with clinical and administrative decision support systems, and formulation of care pathway guidance (AIA 1-4-5).
- Automatic guidance of care pathways, reusing rules from knowledge base, and ensuring patient autonomy in telehealth (AIA 1-2-3).
- Patient real-time guidance, high-frequency analysis of health needs, and policy development based on rules and evidence (AIA 2-3-4).
Our model emphasizes the use of advanced patient-centric IT using prequalified, evidence-based knowledge repertoires to validate and reuse care pathway rules. In addition, we are seeking to integrate AI tools capable of linking to existing clinical and administrative information systems, while improving processes and rules within care trajectories, to promote continuity of front-line interprofessional care through knowledge sharing.
This framework will be used for an empirical research program, seeking evidence of the potential of this intelligent architecture. We seek to demonstrate the real impact of rules-based knowledge sharing tools in interprofessional primary care. Through a partnership with a large healthcare network, we will measure the quality, safety, and efficiency of care for chronic patients.
5. Conclusions
We reviewed the key current research areas of AI combined with analytics technology (AIA) applied to healthcare and proposed a framework to help integrate them within the complex care pathways of chronic care patients. Our objective was to summarizes the past 5 years of healthcare applications of AIA, across different techniques and medical specialties, and discuss the current issues and challenges, relating this revolutionary technology. The five technologies reviewed were chosen due to their higher extent of application, but there are many more healthcare technologies and application opportunities: data mining; ontologies, semantic reasoning, and ontology-extended clinical guidelines; clinical decision support systems; smart homes; medical big data.
Although AIA promises to entirely transform medical practice, many technical challenges lie ahead, and the real-life implementation is still facing obstacles. Indeed, the lack of collaboration with the medical staff is a major determinant of the success of these research works. There are also social, economic, and legal challenges, requiring further reviews and analyses to integrate AIA properly to the healthcare service reality.
There is a great deal of work on artificial intelligence in medicine, but there is a lack of evaluation by clinicians and using real clinical data. This is due, among others, to the lack of access to this clinical data. In addition, the lack of data for learning with data mining algorithms, and the frequent updating of this data has a big impact on the predictions made by these algorithms. Another important point is that training an algorithm on data containing misdiagnoses, erroneous treatments, or wrong scenarios that have not been reported will also have a negative impact on the performance of the algorithm in their predictions. These various challenges can hardly be addressed in the present conceptual review. We plan in future work to perform a detailed meta-analysis on a specific set of articles to ensure comparability of datasets and explore the relative bias and other factors affecting AIA effectiveness.
As clinical and medical systems grow, there will be an inevitable increase in their clinical use and implementation, which will lead to new issues. AIA aims to improve the quality of care by reducing clinician’s error and decreasing their exhaustion arising from routine clinical activities and tasks. However, it may not reduce physician workload, as clinical guidelines might recommend that examinations be carried out more often for at-risk patients.
Author Contributions
Conceptualization, all authors; methodology, S.A. and S.G.; investigation, S.A.; writing—original draft preparation, S.A. and S.G.; writing—review and editing, S.G., A.R. and G.R.; tables and figures, S.G.; copy editing, S.G.; project administration, S.G.; funding acquisition, S.G., A.R. and G.R. All authors have read and agreed to the published version of the manuscript.
Funding
We acknowledge support by the National Capital Management Research Fund.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Turing, A.M. Computing machinery and intelligence. In Parsing the Turing Test; Springer: Berlin/Heidelberg, Germany, 2009; pp. 23–65. [Google Scholar]
- Buchanan, B.G. A (very) brief history of artificial intelligence. Ai Mag. 2005, 26, 53. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The, P.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lashari, S.A.; Ibrahim, R.; Senan, N.; Taujuddin, N. Application of data mining techniques for medical data classification: A review. In Proceedings of the MATEC Web of Conferences, Warsaw, Poland, 5–7 October 2018; p. 06003. [Google Scholar]
- Lakshmi, B.; Indumathi, T.; Ravi, N. A Study on C. 5 decision tree classification algorithm for risk predictions during pregnancy. Procedia Technol. 2016, 24, 1542–1549. [Google Scholar] [CrossRef] [Green Version]
- Mirza, S.; Mittal, S.; Zaman, M. Decision Support Predictive model for prognosis of diabetes using SMOTE and Decision tree. Int. J. Appl. Eng. Res. 2018, 13, 9277–9282. [Google Scholar]
- Xue, D.; Frisch, A.; He, D. Differential Diagnosis of Heart Disease in Emergency Departments Using Decision Tree and Medical Knowledge. In Heterogeneous Data Management, Polystores, and Analytics for Healthcare; Springer: Berlin/Heidelberg, Germany, 2019; pp. 225–236. [Google Scholar]
- Chaurasia, V.; Pal, S.; Tiwari, B. Chronic kidney disease: A predictive model using decision tree. Int. J. Eng. Res. Technol. 2018, 11, 1781–1794. [Google Scholar]
- AlZu’bi, S.; Shehab, M.; Al-Ayyoub, M.; Jararweh, Y.; Gupta, B. Parallel implementation for 3d medical volume fuzzy segmentation. Pattern Recognit. Lett. 2020, 130, 312–318. [Google Scholar] [CrossRef]
- Abdulaziz Mohsen, A.; Alsurori, M.; Aldobai, B.; Mohsen, G.A. New approach to medical diagnosis using artificial neural network and decision tree algorithm: Application to dental diseases. Int. J. Inf. Eng. Electron. Bus. 2019, 11, 52. [Google Scholar] [CrossRef]
- Le, T.-L.; Huynh, T.-T.; Lin, L.-Y.; Lin, C.-M.; Chao, F. A K-means Interval Type-2 Fuzzy Neural Network for Medical Diagnosis. Int. J. Fuzzy Syst. 2019, 21, 2258–2269. [Google Scholar] [CrossRef]
- Shinde, A.; Kale, S.; Samant, R.; Naik, A.; Ghorpade, S. Heart Disease Prediction System using Multilayered Feed Forward Neural Network and Back Propagation Neural Network. Int. J. Comput. Appl. 2017, 166, 32–36. [Google Scholar]
- Karayılan, T.; Kılıç, Ö. Prediction of heart disease using neural network. In Proceedings of the 2017 International Conference on Computer Science and Engineering (UBMK), Antalya, Turkey, 5–7 October 2017; pp. 719–723. [Google Scholar]
- Sundaram, N.M. An Improved Elman Neural Network Classifier for classification of Medical Data for Diagnosis of Diabetes. Int. J. Eng. Sci. 2018, 16317, 16321. [Google Scholar]
- Rajalingam, B.; Priya, R. Multimodal medical image fusion based on deep learning neural network for clinical treatment analysis. Int. J. Chemtech Res. 2018, 11, 160–176. [Google Scholar]
- Rojas-Domínguez, A.; Padierna, L.C.; Valadez, J.M.C.; Puga-Soberanes, H.J.; Fraire, H.J. Optimal hyper-parameter tuning of SVM classifiers with application to medical diagnosis. IEEE Access 2017, 6, 7164–7176. [Google Scholar] [CrossRef]
- Zhu, H.; Liu, X.; Lu, R.; Li, H. Efficient and privacy-preserving online medical prediagnosis framework using nonlinear SVM. IEEE J. Biomed. Health Inform. 2016, 21, 838–850. [Google Scholar] [CrossRef] [PubMed]
- Zeng, N.; Qiu, H.; Wang, Z.; Liu, W.; Zhang, H.; Li, Y. A new switching-delayed-PSO-based optimized SVM algorithm for diagnosis of Alzheimer’s disease. Neurocomputing 2018, 320, 195–202. [Google Scholar] [CrossRef]
- Vogado, L.H.; Veras, R.M.; Araujo, F.H.; Silva, R.R.; Aires, K.R. Leukemia diagnosis in blood slides using transfer learning in CNNs and SVM for classification. Eng. Appl. Artif. Intell. 2018, 72, 415–422. [Google Scholar] [CrossRef]
- Khanmohammadi, S.; Adibeig, N.; Shanehbandy, S. An improved overlapping k-means clustering method for medical applications. Expert Syst. Appl. 2017, 67, 12–18. [Google Scholar] [CrossRef]
- Shakeel, P.M.; Baskar, S.; Dhulipala, V.S.; Jaber, M.M. Cloud based framework for diagnosis of diabetes mellitus using K-means clustering. Health Inf. Sci. Syst. 2018, 6, 16. [Google Scholar] [CrossRef]
- Gürüler, H. A novel diagnosis system for Parkinson’s disease using complex-valued artificial neural network with k-means clustering feature weighting method. Neural Comput. Appl. 2017, 28, 1657–1666. [Google Scholar] [CrossRef]
- Wu, M.; Krishna, S.; Thornhill, R.E.; Flood, T.A.; McInnes, M.D.; Schieda, N. Transition zone prostate cancer: Logistic regression and machine-learning models of quantitative ADC, shape and texture features are highly accurate for diagnosis. J. Magn. Reson. Imaging 2019, 50, 940–950. [Google Scholar] [CrossRef]
- Enriko, I.K.A.; Suryanegara, M.; Gunawan, D. Heart Disease Diagnosis System with k-Nearest Neighbors Method Using Real Clinical Medical Records. In Proceedings of the 4th International Conference on Frontiers of Educational Technologies, Moscow, Russia, 25–27 June 2018; pp. 127–131. [Google Scholar]
- Khanna, D.; Sharma, A. Kernel-Based Naive Bayes Classifier for Medical Predictions. In Intelligent Engineering Informatics; Springer: Berlin/Heidelberg, Germany, 2018; pp. 91–101. [Google Scholar]
- Shen, Y.; Li, Y.; Zheng, H.-T.; Tang, B.; Yang, M. Enhancing ontology-driven diagnostic reasoning with a symptom-dependency-aware Naïve Bayes classifier. BMC Bioinform. 2019, 20, 330. [Google Scholar] [CrossRef] [Green Version]
- Orphanou, K.; Dagliati, A.; Sacchi, L.; Stassopoulou, A.; Keravnou, E.; Bellazzi, R. Combining naive bayes classifiers with temporal association rules for coronary heart disease diagnosis. In Proceedings of the 2016 IEEE International Conference on Healthcare Informatics (ICHI), Chicago, IL, USA, 4–7 October 2016; pp. 81–92. [Google Scholar]
- Pourhomayoun, M.; Shakibi, M. Predicting mortality risk in patients with COVID-19 using artificial intelligence to help medical decision-making. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Li, J.; Guo, S.; Xie, N.; Yao, L.; Cao, Y.; Day, S.W.; Howard, S.C.; Graff, J.C.; Gu, T. Real-time estimation and prediction of mortality caused by COVID-19 with patient information based algorithm. Sci. Total Environ. 2020, 727, 138394. [Google Scholar] [CrossRef] [PubMed]
- Narin, A.; Kaya, C.; Pamuk, Z. Automatic detection of coronavirus disease (covid-19) using X-ray images and deep convolutional neural networks. arXiv 2020, arXiv:2003.10849. [Google Scholar]
- Gruber, T.R. A translation approach to portable ontology specifications. Knowl. Acquis. 1993, 5, 199–220. [Google Scholar] [CrossRef]
- Rubin, D.L.; Lewis, S.E.; Mungall, C.J.; Misra, S.; Westerfield, M.; Ashburner, M.; Sim, I.; Chute, C.G.; Storey, M.-A.; Smith, B. National center for biomedical ontology: Advancing biomedicine through structured organization of scientific knowledge. Omics A J. Integr. Biol. 2006, 10, 185–198. [Google Scholar] [CrossRef] [Green Version]
- Babcock, S.; Cowell, L.G.; Beverley, J.; Smith, B. The Infectious Disease Ontology in the Age of COVID-19; OSF Preprints; Center for Open Science: Charlottesville, VA, USA, 2020. [Google Scholar]
- Hoehndorf, R.; Schofield, P.N.; Gkoutos, G.V. The role of ontologies in biological and biomedical research: A functional perspective. Brief. Bioinform. 2015, 16, 1069–1080. [Google Scholar] [CrossRef] [Green Version]
- Chien, H.-Y.; Chen, J.-F.; Chen, Y.-Y.; Lin, P.-S.; Chang, Y.-T.; Chen, R.-C. An Ontology-Based Herb Therapy Recommendation for Respiration System. In Proceedings of the 2017 International Conference on Intelligent Information Hiding and Multimedia Signal Processing, Matsue, Japan, 12–15 August 2017; pp. 74–81. [Google Scholar]
- Asad, S.; Saba, T.; Hussain, S.; Ahmed, M.; Akram, S.; Khan, A.; Anjum, A.; Shah, M.A.; Javaid, N. An ontology-based approach for detecting drug abuse epidemiology. J. Med. Imaging Health Inform. 2017, 7, 1324–1337. [Google Scholar] [CrossRef]
- Fareedi, A.A.; Ghazawneh, A. An Ontology Approach for Knowledge Acquisition and Development of Health Information System (HIS). In Proceedings of the 27th International Conference on Information Systems Development, Lund, Sweden, 21–24 August 2018. [Google Scholar]
- Mortensen, J.M.; Minty, E.P.; Januszyk, M.; Sweeney, T.E.; Rector, A.L.; Noy, N.F.; Musen, M.A. Using the wisdom of the crowds to find critical errors in biomedical ontologies: A study of SNOMED CT. J. Am. Med. Inform. Assoc. 2015, 22, 640–648. [Google Scholar] [CrossRef] [Green Version]
- Lester, R.J. Ground zero: Ontology, recognition, and the elusiveness of care in American eating disorders treatment. Transcult. Psychiatry 2018, 55, 516–533. [Google Scholar] [CrossRef] [Green Version]
- El-Sappagh, S.; Ali, F. DDO: A diabetes mellitus diagnosis ontology. In Applied Informatics; Springer: Berlin/Heidelberg, Germany, 2016; p. 5. [Google Scholar]
- El-Sappagh, S.; Kwak, D.; Ali, F.; Kwak, K.-S. DMTO: A realistic ontology for standard diabetes mellitus treatment. J. Biomed. Semant. 2018, 9, 8. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.; Lu, D.; Zhu, M.; Muzammal, M.; Samuel, O.W.; Huang, G.; Li, W.; Wu, H. OMDP: An ontology-based model for diagnosis and treatment of diabetes patients in remote healthcare systems. Int. J. Distrib. Sens. Netw. 2019, 15, 1550147719847112. [Google Scholar] [CrossRef]
- Messaoudi, R.; Jaziri, F.; Mtibaa, A.; Grand-Brochier, M.; Ali, H.M.; Amouri, A.; Fourati, H.; Chabrot, P.; Gargouri, F.; Vacavant, A. Ontology-based approach for liver cancer diagnosis and treatment. J. Digit. Imaging 2019, 32, 116–130. [Google Scholar] [CrossRef] [PubMed]
- Hu, S.; Zuo, H.; Qi, J.; Hu, Y.; Yu, B. Analysis of effects of Schisandra in the treatment of myocardial infarction based on three-mode gene ontology network. Front. Pharmacol. 2019, 10, 232. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Qi, X.; Zhang, J.; Wang, Z. Classical Formula Ontology Construction and Application in the Diagnosis and Treatment of Dermatosis. In Proceedings of the 2018 IEEE/WIC/ACM International Conference on Web Intelligence (WI), Santiago, Chile, 3–6 December 2018; pp. 615–618. [Google Scholar]
- Jie, W.; Yan, P.; Xiaoxiao, R.; Yixuan, Q. An Expert System for Diagnosis and Treatment of Hypertension Based on Ontology. In Proceedings of the International Conference on Bio-Inspired Computing: Theories and Applications, Beijing, China, 2–4 November 2018; pp. 264–274. [Google Scholar]
- Joob, B.; Wiwanitkit, V. Feasibility of using melatonin as a new treatment agent for Ebola virus infection: A gene ontology study. Asian Pac. J. Trop. Biomed. 2016, 2, 179–180. [Google Scholar] [CrossRef] [Green Version]
- Ryerson, C.J.; Walsh, S.L.; Collard, H.R. Reply to Moodley: A Standardized Diagnostic Ontology for Fibrotic Interstitial Lung Disease. Am. J. Respir. Crit. Care Med. 2018, 197, 1366–1367. [Google Scholar] [CrossRef]
- Salem, Y.B.; Idoudi, R.; Ettabaa, K.S.; Hamrouni, K.; Solaiman, B. Ontology based possibilistic reasoning for breast cancer aided diagnosis. In Proceedings of the European, Mediterranean, and Middle Eastern Conference on Information Systems, Coimbra, Potugal, 7–8 September 2017; pp. 353–366. [Google Scholar]
- Ameur, S.T.B.; Cloppet, F.; Wendling, L.; Sellami, D. Ontology based decision system for breast cancer diagnosis. In Proceedings of the Tenth International Conference on Machine Vision (ICMV 2017), Vienna, Austria, 13–15 November 2017; p. 106962. [Google Scholar]
- Azzi, S.; Iglewski, M.; Nabelsi, V. Ontology design for pneumonia diagnostic. In Proceedings of the International Conference on Biomedical and Health Informatics (BHI) 2018 and the IEEE Conference on Body Sensor Networks (BSN), Las Vegas, NV, USA, 4–7 March 2018. [Google Scholar]
- Azzi, S.; Iglewski, M.; Nabelsi, V. Design of a Pneumonia Ontology for Diagnosis Decision Support System. Int. J. Med. Health Sci. 2018. [Google Scholar] [CrossRef]
- Azzi, S.; Iglewski, M.; Nabelsi, V. Competency questions for biomedical ontology reuse. Procedia Comput. Sci. 2019, 160, 362–368. [Google Scholar] [CrossRef]
- Shoaip, N.; Barakat, S.; Elmogy, M. Alzheimer’s Disease Integrated Ontology (ADIO). In Proceedings of the 2019 14th International Conference on Computer Engineering and Systems (ICCES), Cairo, Egypt, 15–16 December 2019; pp. 374–379. [Google Scholar]
- Filice, R.W.; Kahn, C.E. Integrating an ontology of radiology differential diagnosis with ICD-10-cm, RadLex, and SNOMED CT. J. Digit. Imaging 2019, 32, 206–210. [Google Scholar] [CrossRef]
- Gribova, V.; Okun, D.; Petryaeva, M.; Shalfeeva, E.; Tarasov, A. Ontology for Differential Diagnosis of Acute and Chronic Diseases. In Proceedings of the Russian Conference on Artificial Intelligence, Mosco, Russia, 24–27 September 2018; pp. 152–163. [Google Scholar]
- Köhler, S.; Øien, N.C.; Buske, O.J.; Groza, T.; Jacobsen, J.O.; McNamara, C.; Vasilevsky, N.; Carmody, L.C.; Gourdine, J.; Gargano, M. Encoding Clinical Data with the Human Phenotype Ontology for Computational Differential Diagnostics. Curr. Protoc. Hum. Genet. 2019, 103, e92. [Google Scholar] [CrossRef]
- Lin, Y.; Mehta, S.; Küçük-McGinty, H.; Turner, J.P.; Vidovic, D.; Forlin, M.; Koleti, A.; Nguyen, D.-T.; Jensen, L.J.; Guha, R. Drug target ontology to classify and integrate drug discovery data. J. Biomed. Semant. 2017, 8, 50. [Google Scholar] [CrossRef] [Green Version]
- Li, F.; Wang, M.; Pham, H.A.; Xiang, Y.; Tao, C.; Du, J.; Rao, G. Systematic Design of Drug Repurposing-Oriented Alzheimer’s Disease Ontology. In Proceedings of the 2019 IEEE International Conference on Healthcare Informatics (ICHI), Xi’an, China, 10–13 June 2019; pp. 1–5. [Google Scholar]
- Mutowo, P.; Bento, A.P.; Dedman, N.; Gaulton, A.; Hersey, A.; Lomax, J.; Overington, J.P. A drug target slim: Using gene ontology and gene ontology annotations to navigate protein-ligand target space in ChEMBL. J. Biomed. Semant. 2016, 7, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fox, J.; Gutenstein, M.; Khan, O.; South, M.; Thomson, R. OpenClinical. net: A platform for creating and sharing knowledge and promoting best practice in healthcare. Comput. Ind. 2015, 66, 63–72. [Google Scholar] [CrossRef]
- Kawamoto, K.; Del Fiol, G. Clinical decision support systems in healthcare. Health Inform.-E-Book 2016, 170, 203. [Google Scholar]
- Buntin, M.B.; Burke, M.F.; Hoaglin, M.C.; Blumenthal, D. The benefits of health information technology: A review of the recent literature shows predominantly positive results. Health Aff. 2011, 30, 464–471. [Google Scholar] [CrossRef] [PubMed]
- Lyman, J.A.; Cohn, W.F.; Bloomrosen, M.; Detmer, D.E. Clinical decision support: Progress and opportunities. J. Am. Med. Inform. Assoc. 2010, 17, 487–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawamoto, K.; Lobach, D.F. Proposal for fulfilling strategic objectives of the US roadmap for national action on decision support through a service-oriented architecture leveraging HL7 services. J. Am. Med. Inform. Assoc. 2007, 14, 146–155. [Google Scholar] [CrossRef] [Green Version]
- Chaudhry, B.; Wang, J.; Wu, S.; Maglione, M.; Mojica, W.; Roth, E.; Morton, S.C.; Shekelle, P.G. Systematic review: Impact of health information technology on quality, efficiency, and costs of medical care. Ann. Intern. Med. 2006, 144, 742–752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osheroff, J.A.; Teich, J.M.; Middleton, B.; Steen, E.B.; Wright, A.; Detmer, D.E. A roadmap for national action on clinical decision support. J. Am. Med. Inform. Assoc. 2007, 14, 141–145. [Google Scholar] [CrossRef] [Green Version]
- El-Sappagh, S.; Alonso, J.M.; Ali, F.; Ali, A.; Jang, J.-H.; Kwak, K.-S. An ontology-based interpretable fuzzy decision support system for diabetes diagnosis. IEEE Access 2018, 6, 37371–37394. [Google Scholar] [CrossRef]
- Ali, F.; Islam, S.R.; Kwak, D.; Khan, P.; Ullah, N.; Yoo, S.-j.; Kwak, K.S. Type-2 fuzzy ontology–aided recommendation systems for IoT–based healthcare. Comput. Commun. 2018, 119, 138–155. [Google Scholar] [CrossRef]
- Amland, R.C.; Hahn-Cover, K.E. Clinical decision support for early recognition of sepsis. Am. J. Med. Qual. 2016, 31, 103–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Middleton, B.; Sittig, D.; Wright, A. Clinical decision support: A 25 year retrospective and a 25 year vision. Yearb. Med. Inform. 2016, 25, S103–S116. [Google Scholar]
- Ekstrom, H.L.; Kharbanda, E.O.; Ballard, D.W.; Vinson, D.R.; Vazquez-Benitez, G.; Chettipally, U.K.; Dehmer, S.P.; Kunisetty, G.; Sharma, R.; Rauchwerger, A.S. Development of a Clinical Decision Support System for Pediatric Abdominal Pain in Emergency Department Settings Across Two Health Systems Within the HCSRN. EGEMS 2019, 7, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pota, M.; Esposito, M.; De Pietro, G. Fuzzy partitioning for clinical DSSs using statistical information transformed into possibility-based knowledge. Knowl.-Based Syst. 2014, 67, 1–15. [Google Scholar] [CrossRef]
- Jensen, J.D.; Durand, D.J. Partnering with your health system to select and implement clinical decision support for imaging. J. Am. Coll. Radiol. 2017, 14, 262–268. [Google Scholar] [CrossRef]
- Dayan, P.S.; Ballard, D.W.; Tham, E.; Hoffman, J.M.; Swietlik, M.; Deakyne, S.J.; Alessandrini, E.A.; Tzimenatos, L.; Bajaj, L.; Vinson, D.R. Use of traumatic brain injury prediction rules with clinical decision support. Pediatrics 2017, 139, e20162709. [Google Scholar] [CrossRef] [Green Version]
- Islam, R.; Weir, C.R.; Jones, M.; Del Fiol, G.; Samore, M.H. Understanding complex clinical reasoning in infectious diseases for improving clinical decision support design. BMC Med. Inform. Decis. Mak. 2015, 15, 101. [Google Scholar] [CrossRef] [Green Version]
- Denecke, K.; Deng, Y. Sentiment analysis in medical settings: New opportunities and challenges. Artif. Intell. Med. 2015, 64, 17–27. [Google Scholar] [CrossRef]
- Araque, O.; Zhu, G.; Iglesias, C.A. A semantic similarity-based perspective of affect lexicons for sentiment analysis. Knowl.-Based Syst. 2019, 165, 346–359. [Google Scholar] [CrossRef]
- Teng, Z.; Vo, D.-T.; Zhang, Y. Context-sensitive lexicon features for neural sentiment analysis. In Proceedings of the 2016 Conference on Empirical Methods in Natural Language Processing, Austin, TX, USA, 1–5 November 2016; pp. 1629–1638. [Google Scholar]
- Khoo, C.S.; Johnkhan, S.B. Lexicon-based sentiment analysis: Comparative evaluation of six sentiment lexicons. J. Inf. Sci. 2018, 44, 491–511. [Google Scholar] [CrossRef]
- Lohr, S. IBM is counting on its bet on Watson, and paying big money for it. NY Times 2016, 17, 2016. [Google Scholar]
- Katzman, J.L.; Shaham, U.; Cloninger, A.; Bates, J.; Jiang, T.; Kluger, Y. DeepSurv: Personalized treatment recommender system using a Cox proportional hazards deep neural network. BMC Med. Res. Methodol. 2018, 18, 24. [Google Scholar] [CrossRef] [PubMed]
- Ronao, C.A.; Cho, S.-B. Human activity recognition with smartphone sensors using deep learning neural networks. Expert Syst. Appl. 2016, 59, 235–244. [Google Scholar] [CrossRef]
- Ma, M.; Fan, H.; Kitani, K.M. Going deeper into first-person activity recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 1894–1903. [Google Scholar]
- Hassan, M.M.; Uddin, M.Z.; Mohamed, A.; Almogren, A. A robust human activity recognition system using smartphone sensors and deep learning. Future Gener. Comput. Syst. 2018, 81, 307–313. [Google Scholar] [CrossRef]
- Ignatov, A. Real-time human activity recognition from accelerometer data using Convolutional Neural Networks. Appl. Soft Comput. 2018, 62, 915–922. [Google Scholar] [CrossRef]
- Cippitelli, E.; Gasparrini, S.; Gambi, E.; Spinsante, S. A human activity recognition system using skeleton data from RGBD sensors. Comput. Intell. Neurosci. 2016, 2016, 4351435. [Google Scholar] [CrossRef] [Green Version]
- Wang, A.; Chen, G.; Shang, C.; Zhang, M.; Liu, L. Human activity recognition in a smart home environment with stacked denoising autoencoders. In Proceedings of the 2016 International Conference on Web-Age Information Management, Nanchang, China, 3–5 June 2016; pp. 29–40. [Google Scholar]
- Cicirelli, F.; Fortino, G.; Giordano, A.; Guerrieri, A.; Spezzano, G.; Vinci, A. On the design of smart homes: A framework for activity recognition in home environment. J. Med. Syst. 2016, 40, 200. [Google Scholar] [CrossRef]
- Mehr, H.D.; Polat, H.; Cetin, A. Resident activity recognition in smart homes by using artificial neural networks. In Proceedings of the 2016 4th International Istanbul Smart Grid Congress and Fair (ICSG), Istanbul, Turkey, 20–21 April 2016; pp. 1–5. [Google Scholar]
- Fan, X.; Xie, Q.; Li, X.; Huang, H.; Wang, J.; Chen, S.; Xie, C.; Chen, J. Activity recognition as a service for smart home: Ambient assisted living application via sensing home. In Proceedings of the 2017 IEEE International Conference on AI & Mobile Services (AIMS), Honolulu, HI, USA, 15–30 June 2017; pp. 54–61. [Google Scholar]
- Gayathri, K.; Easwarakumar, K.; Elias, S. Activity Recognition and Dementia Care in Smart Home. In Digital India; Springer: Berlin/Heidelberg, Germany, 2018; pp. 33–47. [Google Scholar]
- Zou, H.; Zhou, Y.; Yang, J.; Jiang, H.; Xie, L.; Spanos, C.J. WiFi-enabled device-free gesture recognition for smart home automation. In Proceedings of the 2018 IEEE 14th International Conference on Control and Automation (ICCA), Anchorage, AK, USA, 12–15 June 2018; pp. 476–481. [Google Scholar]
- Singh, G.; Nelson, A.; Lu, S.; Robucci, R.; Patel, C.; Banerjee, N. Event-driven low-power gesture recognition using differential capacitance. IEEE Sens. J. 2016, 16, 4955–4967. [Google Scholar] [CrossRef]
- Kaur, M.; Kaur, G.; Sharma, P.K.; Jolfaei, A.; Singh, D. Binary cuckoo search metaheuristic-based supercomputing framework for human behavior analysis in smart home. J. Supercomput. 2020, 76, 2479–2502. [Google Scholar] [CrossRef]
- Pan, Z.; Pacheco, J.; Hariri, S.; Chen, Y.; Liu, B. Context Aware Anomaly Behavior Analysis for Smart Home Systems. Int. J. Inf. Commun. Eng. 2019, 13, 261–274. [Google Scholar]
- Chen, M.; Yang, J.; Zhu, X.; Wang, X.; Liu, M.; Song, J. Smart home 2.0: Innovative smart home system powered by botanical IoT and emotion detection. Mob. Netw. Appl. 2017, 22, 1159–1169. [Google Scholar] [CrossRef]
- Fu, C. Smart Home Control Method Based on Emotion Recognition and the System Thereof. U.S. Patent No. 10,013,977, 3 July 2018. [Google Scholar]
- Demir, E.; Köseoğlu, E.; Sokullu, R.; Şeker, B. Smart home assistant for ambient assisted living of elderly people with dementia. Procedia Comput. Sci. 2017, 113, 609–614. [Google Scholar] [CrossRef]
- Ghayvat, H.; Liu, J.; Mukhopadhyay, S.C.; Gui, X. Wellness sensor networks: A proposal and implementation for smart home for assisted living. IEEE Sens. J. 2015, 15, 7341–7348. [Google Scholar] [CrossRef]
- Stahl, C.; Laub, P. Maintaining multiple sclerosis patients’ quality of life: A case study on environment control assistance in a smart home. In Proceedings of the 10th International Conference on PErvasive Technologies Related to Assistive Environments, Rhodes, Greece, 21–23 June 2017; pp. 83–86. [Google Scholar]
- Aman, F.; Aubergé, V.; Vacher, M. Influence of expressive speech on ASR performances: Application to elderly assistance in smart home. In Proceedings of the International Conference on Text, Speech, and Dialogue, Brno, Czech Republic, 12–16 September 2016; pp. 522–530. [Google Scholar]
- Yassine, A.; Singh, S.; Hossain, M.S.; Muhammad, G. IoT big data analytics for smart homes with fog and cloud computing. Future Gener. Comput. Syst. 2019, 91, 563–573. [Google Scholar] [CrossRef]
- Sukor, A.S.A.; Zakaria, A.; Rahim, N.A.; Kamarudin, L.M.; Setchi, R.; Nishizaki, H. A hybrid approach of knowledge-driven and data-driven reasoning for activity recognition in smart homes. J. Intell. Fuzzy Syst. 2019, 36, 4177–4188. [Google Scholar] [CrossRef]
- Hudec, M.; Smutny, Z. RUDO: A home ambient intelligence system for blind people. Sensors 2017, 17, 1926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warren, D.A.; Marschalkowski, E. Smart-Home Device Telemetry Circuits for Detecting Electrical Anomalies in a Population of Devices. U.S. Patent No. 10,557,640, 11 February 2020. [Google Scholar]
- Boettcher, J.; Sloo, D.H.; Boyd, J.A.; Le Guen, S. Systems and Methods of Providing Status Information in a Smart Home Security Detection System. U.S. Patent No. 10,593,190, 17 March 2020. [Google Scholar]
- Hargreaves, T.; Wilson, C.; Hauxwell-Baldwin, R. Learning to live in a smart home. Build. Res. Inf. 2018, 46, 127–139. [Google Scholar] [CrossRef] [Green Version]
- Manogaran, G.; Thota, C.; Lopez, D.; Vijayakumar, V.; Abbas, K.M.; Sundarsekar, R. Big data knowledge system in healthcare. In Internet of Things and big Data Technologies for Next Generation Healthcare; Springer: Berlin/Heidelberg, Germany, 2017; pp. 133–157. [Google Scholar]
- Simonsen, L.; Gog, J.R.; Olson, D.; Viboud, C. Infectious disease surveillance in the big data era: Towards faster and locally relevant systems. J. Infect. Dis. 2016, 214, S380–S385. [Google Scholar] [CrossRef] [Green Version]
- Benbow, N.; Kirkpatrick, C.; Gupta, A.; Villamar, J.; Chernyshov, K.; Cramer, N.; Mena, L.; Mayer, R.; Young, S. An Iterative Process of Integrating and Developing Big Data Modeling and Visualization Tools in Collaboration With Public Health Officials; SAGE Publications Ltd.: New York, NY, USA, 2020. [Google Scholar]
- Salerno, J.; Knoppers, B.M.; Lee, L.M.; Hlaing, W.M.; Goodman, K.W. Ethics, big data and computing in epidemiology and public health. Ann. Epidemiol. 2017, 27, 297–301. [Google Scholar] [CrossRef]
- Chae, S.; Kwon, S.; Lee, D. Predicting infectious disease using deep learning and big data. Int. J. Environ. Res. Public Health 2018, 15, 1596. [Google Scholar] [CrossRef] [Green Version]
- Choirat, C.; Braun, D.; Kioumourtzoglou, M.-A. Data Science in Environmental Health Research. Curr. Epidemiol. Rep. 2019, 6, 291–299. [Google Scholar] [CrossRef] [PubMed]
- Ehrenstein, V.; Nielsen, H.; Pedersen, A.B.; Johnsen, S.P.; Pedersen, L. Clinical epidemiology in the era of big data: New opportunities, familiar challenges. Clin. Epidemiol. 2017, 9, 245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brody, J.A.; Morrison, A.C.; Bis, J.C.; O’Connell, J.R.; Brown, M.R.; Huffman, J.E.; Ames, D.C.; Carroll, A.; Conomos, M.P.; Gabriel, S. Analysis commons, a team approach to discovery in a big-data environment for genetic epidemiology. Nat. Genet. 2017, 49, 1560–1563. [Google Scholar] [CrossRef] [PubMed]
- Bansal, S.; Chowell, G.; Simonsen, L.; Vespignani, A.; Viboud, C. Big data for infectious disease surveillance and modeling. J. Infect. Dis. 2016, 214, S375–S379. [Google Scholar] [CrossRef]
- Bragazzi, N.L.; Guglielmi, O.; Garbarino, S. SleepOMICS: How big data can revolutionize sleep science. Int. J. Environ. Res. Public Health 2019, 16, 291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boone-Heinonen, J.; Tillotson, C.; O’Malley, J.; Cottrell, E.; Gaudino, J.; Amofah, A.; Rivo, M.; Brickman, A.; Mayer, K.; McBurnie, M. Characterizing a “big data” cohort of over 200,000 low-income US infants and children for obesity research: The Advance Early Life Cohort. Matern. Child Health J. 2017, 21, 421–431. [Google Scholar] [CrossRef] [Green Version]
- Lamminpää, R.; Gissler, M.; Vehviläinen-Julkunen, K. Utilization of large data sets in maternal health in Finland. J. Perinat. Neonatal Nurs. 2017, 31, 236–243. [Google Scholar] [CrossRef]
- Maugard, C.; Bosson-Rieutort, D.; François, O.; Bonneterre, V. 1154 Big Data and Occupational Health Surveillance: Use of French Medico-Administrative Databases for Hypothesis Generation Regarding Occupational Risks in Agriculture; BMJ Publishing Group Ltd.: London, UK, 2018. [Google Scholar]
- Maugard, C.; Rieutort, D.B.; Ozenfant, D.; François, O.; Bonneterre, V. Big-data and occupational health surveillance: Screening of occupational determinants of health among French agricultural workers, through data mining of medico-administrative databases. Rev. D’épidémiologie Et De St. Publique 2018, 66, S262–S263. [Google Scholar] [CrossRef]
- Phillips, C.A.; Pollock, B.H. Big Data for Nutrition Research in Pediatric Oncology: Current State and Framework for Advancement. Jnci Monogr. 2019, 2019, 127–131. [Google Scholar] [CrossRef]
- McDonald, D.; Glusman, G.; Price, N.D. Personalized nutrition through big data. Nat. Biotechnol. 2016, 34, 152. [Google Scholar] [CrossRef]
- Paul, P.; Aithal, P.; Bhuimali, A. Enhancing Cloud and Big Data Systems for healthy Food and Nutrition Information Systems Practice: A Conceptual Study. Int. J. Sci. Res. Biol. Sci. 2017, 4, 5. [Google Scholar] [CrossRef]
- Al-Ali, A.-R.; Zualkernan, I.A.; Rashid, M.; Gupta, R.; AliKarar, M. A smart home energy management system using IoT and big data analytics approach. IEEE Trans. Consum. Electron. 2017, 63, 426–434. [Google Scholar] [CrossRef]
- Yassine, A.; Singh, S.; Alamri, A. Mining human activity patterns from smart home big data for health care applications. IEEE Access 2017, 5, 13131–13141. [Google Scholar] [CrossRef]
- Kanevsky, J.; Corban, J.; Gaster, R.; Kanevsky, A.; Lin, S.; Gilardino, M. Big data and machine learning in plastic surgery: A new frontier in surgical innovation. Plast. Reconstr. Surg. 2016, 137, 890e–897e. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.H.; Yoon, H.-J. Medical big data: Promise and challenges. Kidney Res. Clin. Pract. 2017, 36, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.; Groeneveld, P.W. Big data, health informatics, and the future of cardiovascular medicine. J. Am. Coll. Cardiol. 2017, 69, 899–902. [Google Scholar] [CrossRef]
- Sanaei, A.; Sepehri, M.M. Quality Improvement through Intensive Care Registries: The Value of Big Data in Clinical Decision Making. Arch. Anesth. Crit. Care 2020. [Google Scholar] [CrossRef]
- Van den Heuvel, L.; Dorsey, R.R.; Prainsack, B.; Post, B.; Stiggelbout, A.M.; Meinders, M.J.; Bloem, B.R. Quadruple Decision Making for Parkinson’s Disease Patients: Combining Expert Opinion, Patient Preferences, Scientific Evidence, and Big Data Approaches to Reach Precision Medicine. J. Parkinson’s Dis. 2020, 10, 223–231. [Google Scholar] [CrossRef] [Green Version]
- Duan, Y.; Edwards, J.S.; Dwivedi, Y.K. Artificial intelligence for decision making in the era of Big Data–evolution, challenges and research agenda. Int. J. Inf. Manag. 2019, 48, 63–71. [Google Scholar] [CrossRef]
- Roosan, D.; Samore, M.; Jones, M.; Livnat, Y.; Clutter, J. Big-data based decision-support systems to improve clinicians’ cognition. In Proceedings of the 2016 IEEE International Conference on Healthcare Informatics (ICHI), Chicago, IL, USA, 4–7 October 2016; pp. 285–288. [Google Scholar]
- Saunders, G.H.; Christensen, J.H.; Gutenberg, J.; Pontoppidan, N.H.; Smith, A.; Spanoudakis, G.; Bamiou, D.-E. Application of Big Data to Support Evidence-Based Public Health Policy Decision-Making for Hearing. Ear Hear. 2020. [Google Scholar] [CrossRef]
- Kumar, Y.; Sood, K.; Kaul, S.; Vasuja, R. Big Data Analytics and Its Benefits in Healthcare. In Big Data Analytics in Healthcare; Springer: Berlin/Heidelberg, Germany, 2020; pp. 3–21. [Google Scholar]
- Price, W.N.; Cohen, I.G. Privacy in the age of medical big data. Nat. Med. 2019, 25, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Kallianos, K.; Mongan, J.; Antani, S.; Henry, T.; Taylor, A.; Abuya, J.; Kohli, M. How far have we come? Artificial intelligence for chest radiograph interpretation. Clin. Radiol. 2019, 74, 338–345. [Google Scholar] [CrossRef] [PubMed]
- Barr, V.; Robinson, S.; Marin-Link, B.; Underhill, L.; Dotts, A.; Ravensdale, D.; Salivaras, S. The expanded chronic care model. Hosp. Q. 2003, 7, 73–82. [Google Scholar] [PubMed] [Green Version]
- Wagner, E.H.; Austin, B.T.; Davis, C.; Hindmarsh, M.; Schaefer, J.; Bonomi, A. Improving Chronic Illness Care: Translating Evidence Into Action. Health Aff. 2001, 20, 64–78. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
Patient-centric framework for healthcare artificial intelligence and analytics (AIA). Source: Inspired by [139], based on [140].


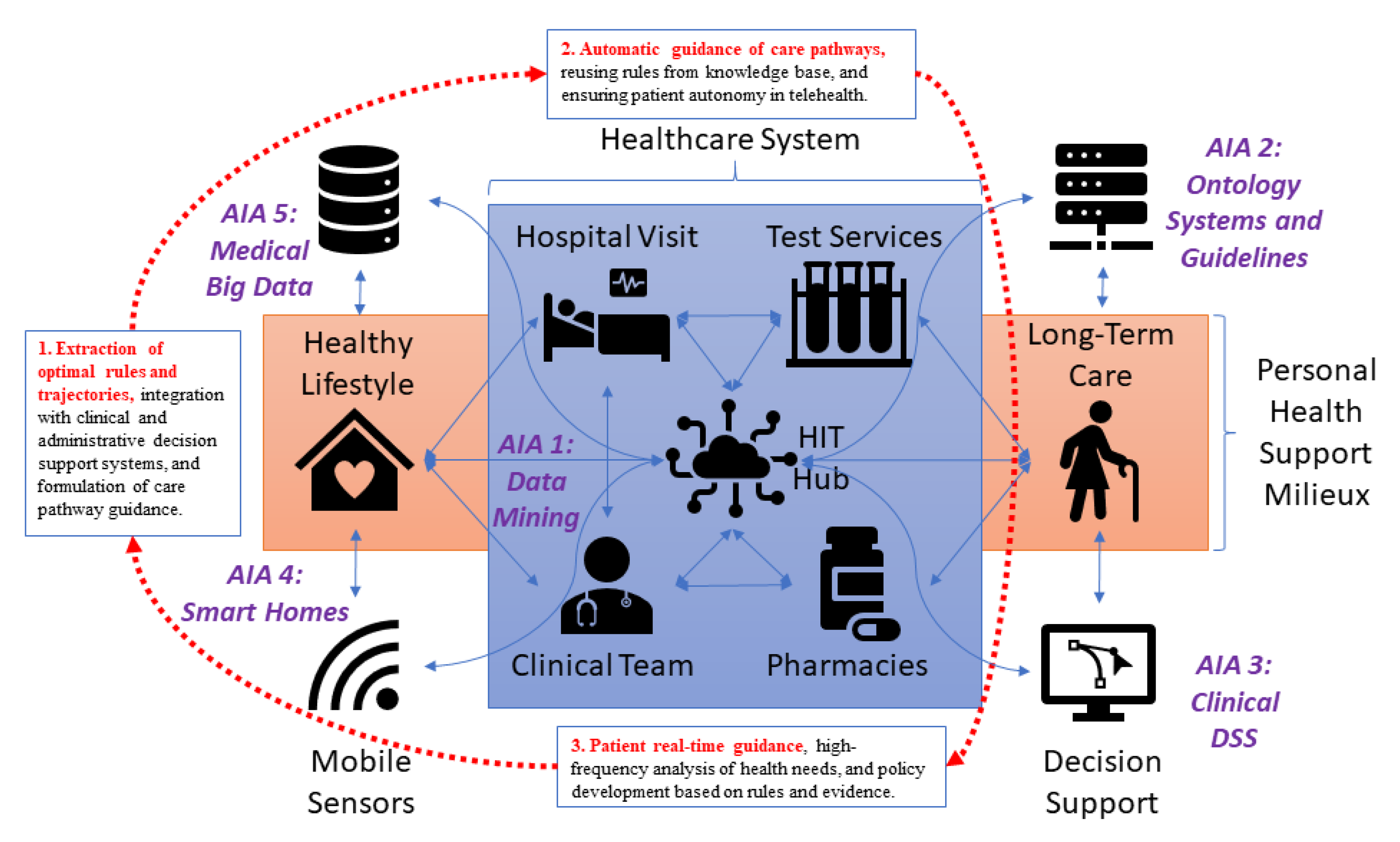{kind=link}
Table 1.
Search strategy.
| Filtering | Search Query |
|---|---|
| Data mining | (“machine learning”[tiab] OR “data mining”[tiab] OR “text mining”[tiab] OR “mining”[tiab] OR “decision tree”[tiab] OR “neural network”[tiab] OR “SVM”[tiab] OR bayes*[tiab] OR “KNN”[tiab] OR “K-means”[tiab]) AND (med*[tiab] OR clinic*[tiab] OR health*[tiab]) |
| Ontologies and semantic reasoning | Ontology AND (med*[tiab] OR clinic*[tiab] OR health*[tiab] OR emergenc*[tiab] OR physician*[tiab] OR psycholog*[tiab] OR pain [tiab] OR therapy [tiab] OR treat*[tiab] OR drug*[tiab] OR disease*[tiab] OR diagnos*[tiab] OR emotion*[tiab]) OR (computerized clinical guideline*[tiab] OR computerized clinical practice guideline*[tiab])) |
| Clinical decision support systems | (monitor*[tiab] OR assist*[tiab] OR recommend*[tiab] OR “decision support”[tiab] OR “decision making”[tiab] OR “computer assisted”[tiab] OR “reminder system”[tiab] OR “support system”[tiab] OR expert system*[tiab]) AND (med*[tiab] OR clinic*[tiab] OR health*[tiab] OR emergenc*[tiab] OR physician*[tiab] OR psycholog*[tiab] OR pain [tiab] OR therapy [tiab] OR treat*[tiab] OR drug*[tiab] OR disease*[tiab] OR diagnos*[tiab] OR emotion*[tiab]) |
| Smart homes | (smart home*[tiab]) AND (activity recognition*[tiab] “expression recognition”[tiab] OR assist*[tiab] OR recogni*[tiab] OR detect*[tiab] OR guid*[tiab] OR algorithm*[tiab] OR “security”[tiab] OR web service*[tiab]OR “system”[tiab] OR “application”[tiab] OR “technology”[tiab] OR “engine”[tiab] OR “framework”[tiab] OR “behaviour analysis”[tiab]) |
| Medical big data | “Big data” [tiab] AND (med*[tiab] OR clinic*[tiab] OR health*[tiab]) |
Table 2.
Systematic review stages.
| AI Applications | Found | Relevant | Cited |
|---|---|---|---|
| Data mining | 5987 | 1052 | 29 |
| Ontologies and semantic reasoning and clinical guidelines | 2912 | 675 | 34 |
| Clinical decision support systems | 3970 | 2198 | 21 |
| Smart homes | 6444 | 2932 | 30 |
| Medical big data | 5469 | 689 | 23 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Azzi, S.; Gagnon, S.; Ramirez, A.; Richards, G. Healthcare Applications of Artificial Intelligence and Analytics: A Review and Proposed Framework. Appl. Sci. 2020, 10, 6553. https://doi.org/10.3390/app10186553
AMA Style
Azzi S, Gagnon S, Ramirez A, Richards G. Healthcare Applications of Artificial Intelligence and Analytics: A Review and Proposed Framework. Applied Sciences. 2020; 10(18):6553. https://doi.org/10.3390/app10186553
Chicago/Turabian StyleAzzi, Sabrina, Stéphane Gagnon, Alex Ramirez, and Gregory Richards. 2020. "Healthcare Applications of Artificial Intelligence and Analytics: A Review and Proposed Framework" Applied Sciences 10, no. 18: 6553. https://doi.org/10.3390/app10186553
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.