Cone Beam CT Imaging of the Paranasal Region with a Multipurpose X-ray System—Image Quality and Radiation Exposure

Abstract
:1. Introduction
2. Materials and Methods
2.1. Image Acquisition
2.2. Image Quality Assessment
2.3. Estimation of Radiation Exposure
3. Results
3.1. First Cadaver Head Scan
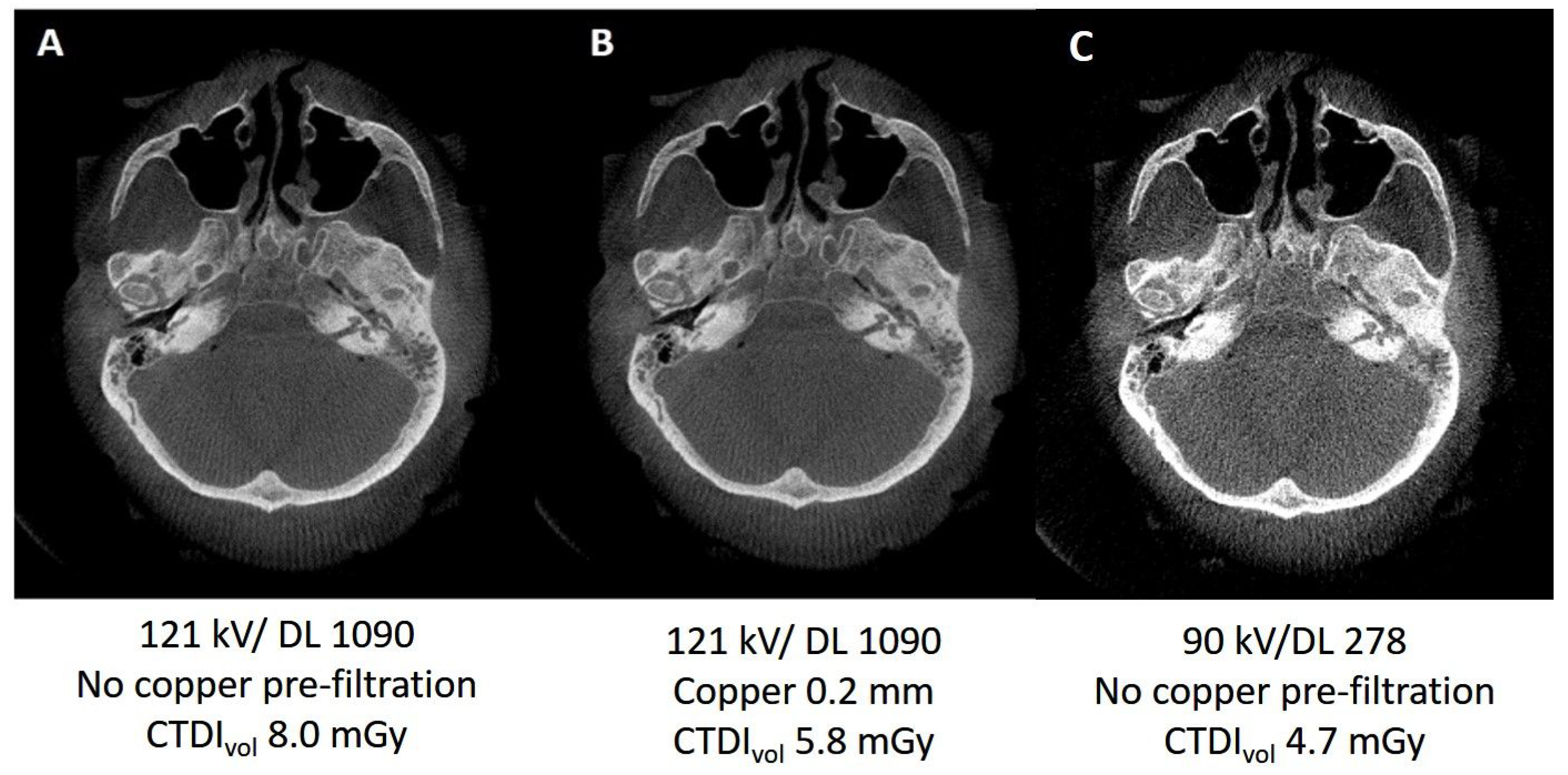
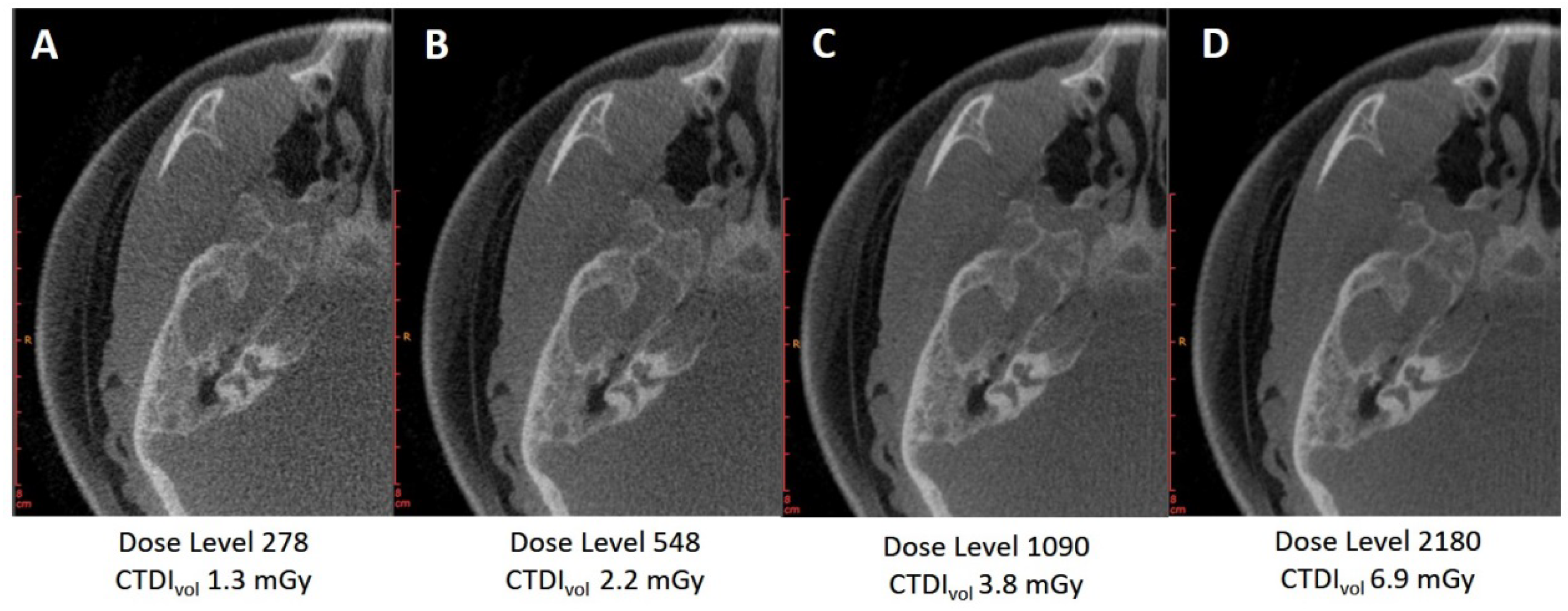
3.1.1. Variation of Tube Voltage
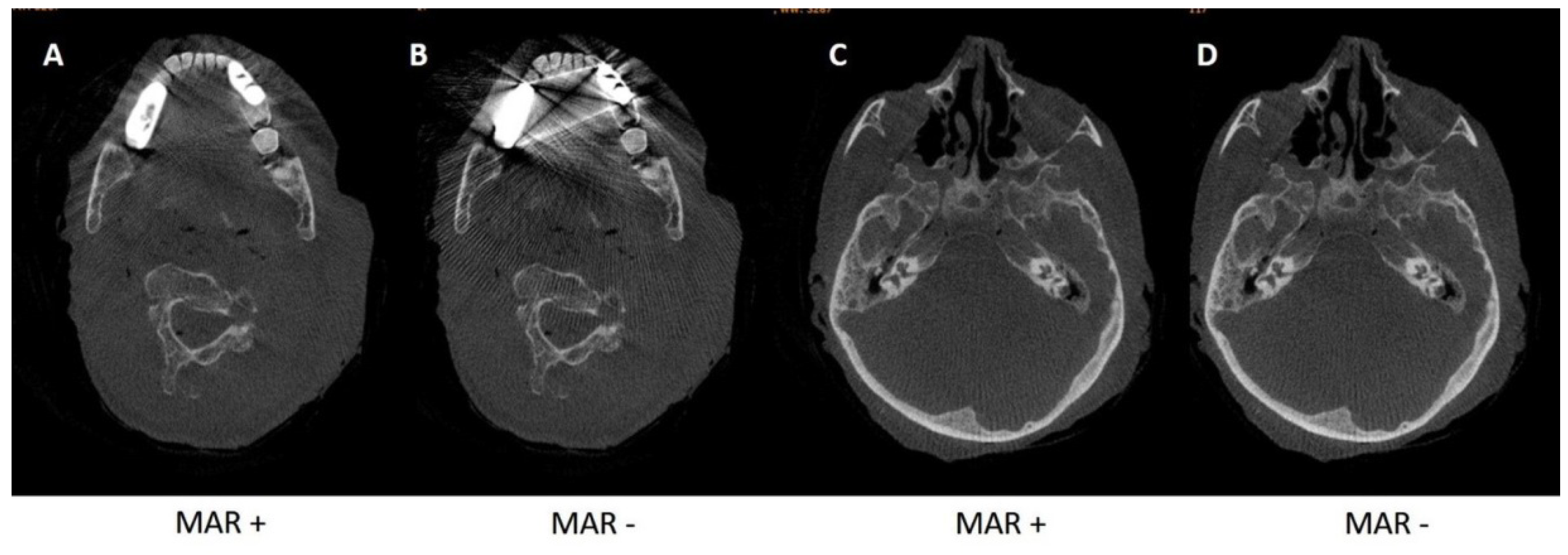
3.1.2. Metal Artifact Reduction Algorithm
3.1.3. Kernels
3.2. Results for Cadaver Heads 2–4
3.2.1. Pre-Filtration with 0.2 vs. 0.3 mm Copper Filter
3.2.2. Pre-Filtration with 0.4 mm Tin Filter
3.3. Statistical Evaluation: Preoperative Imaging vs. Imaging of Sinusitis
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Disclaimer
References
- Blackwell, D.L.; Lucas, J.W.; Clarke, T.C. Summary health statistics for U.S. adults: National health interview survey, 2012. Vital Health Stat. 2014, 10, 1–161. [Google Scholar]
- Rosenfeld, R.M.; Andes, D.; Bhattacharyya, N.; Cheung, D.; Eisenberg, S.; Ganiats, T.G.; Gelzer, A.; Hamilos, D.; Haydon, R.C., III; Hudgins, P.A.; et al. Clinical practice guideline: Adult sinusitis. Otolaryngol. Head Neck Surg. 2007, 137, S1–S31. [Google Scholar] [CrossRef] [PubMed]
- Anon, J.B.; Jacobs, M.R.; Poole, M.D. Antimicrobial treatment guidelines for acute bacterial rhinosinusitis. Otolaryngol. Head Neck Surg. 2004, 130, 1–45. [Google Scholar] [PubMed]
- Duvoisin, B.; Landry, M.; Chapuis, L.; Krayenbuhl, M.; Schnyder, P. Low-dose CT and inflammatory disease of the paranasal sinuses. Neuroradiology 1991, 33, 403–406. [Google Scholar] [CrossRef] [PubMed]
- Tack, D.; Widelec, J.; De Maertelaer, V.; Bailly, J.M.; Delcour, C.; Gevenois, P.A. Comparison between low-dose and standard-dose multidetector CT in patients with suspected chronic sinusitis. Am. J. Roentgenol. 2003, 181, 939–944. [Google Scholar] [CrossRef] [PubMed]
- Abul-Kasim, K.; Strombeck, A.; Sahlstrand-Johnson, P. Low-dose computed tomography of the paranasal sinuses: Radiation doses and reliability analysis. Am. J. Otolaryngol. 2011, 32, 47–51. [Google Scholar] [CrossRef]
- Hoang, J.K.; Eastwood, J.D.; Tebbit, C.L.; Glastonbury, C.M. Multiplanar sinus CT: A systematic approach to imaging before functional endoscopic sinus surgery. Am. J. Roentgenol. 2010, 194, W527–W536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cashman, E.C.; Macmahon, P.J.; Smyth, D. Computed tomography scans of paranasal sinuses before functional endoscopic sinus surgery. World J. Radiol. 2011, 3, 199–204. [Google Scholar] [CrossRef]
- Ide, C.; Trigaux, J.P.; Eloy, P. Chronic sinusitis: The role of imaging. Acta Otorhinolaryngol. Belg. 1997, 51, 247–258. [Google Scholar]
- Konen, E.; Faibel, M.; Kleinbaum, Y.; Wolf, M.; Lusky, A.; Hoffman, C.; Eyal, A.; Tadmor, R. The value of the occipitomental (Waters’) view in diagnosis of sinusitis: A comparative study with computed tomography. Clin. Radiol. 2000, 55, 856–860. [Google Scholar] [CrossRef]
- Lell, M.M.; May, M.S.; Brand, M.; Eller, A.; Buder, T.; Hofmann, E.; Uder, M.; Wuest, W. Imaging the Parasinus Region with a Third-Generation Dual-Source CT and the Effect of Tin Filtration on Image Quality and Radiation Dose. Am. J. Neuroradiol. 2015, 36, 1225–1230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wuest, W.; May, M.; Saake, M.; Brand, M.; Uder, M.; Lell, M. Low-Dose CT of the Paranasal Sinuses: Minimizing X-Ray Exposure with Spectral Shaping. Eur. Radiol. 2016, 26, 4155–4161. [Google Scholar] [CrossRef] [PubMed]
- Miracle, A.C.; Mukherji, S.K. Conebeam CT of the head and neck, part 2: Clinical applications. Am. J. Neuroradiol. 2009, 30, 1285–1292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miracle, A.C.; Mukherji, S.K. Conebeam CT of the head and neck, part 1: Physical principles. Am. J. Neuroradiol. 2009, 30, 1088–1095. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dammann, F.; Bootz, F.; Cohnen, M.; Hassfeld, S.; Tatagiba, M.; Kosling, S. Diagnostic imaging modalities in head and neck disease. Dtsch. Arztebl. Int. 2014, 111, 417–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zoumalan, R.A.; Lebowitz, R.A.; Wang, E.; Yung, K.; Babb, J.S.; Jacobs, J.B. Flat panel cone beam computed tomography of the sinuses. Otolaryngol. Head Neck Surg. 2009, 140, 841–844. [Google Scholar] [CrossRef]
- Casselman, J.W.; Gieraerts, K.; Volders, D.; Delanote, J.; Mermuys, K.; De Foer, B.; Swennen, G. Cone beam CT: Non-dental applications. Jbr-Btr 2013, 96, 333–353. [Google Scholar] [CrossRef] [Green Version]
- Benz, R.M.; Garcia, M.A.; Amsler, F.; Voigt, J.; Fieselmann, A.; Falkowski, A.L.; Stieltjes, B.; Hirschmann, A. Initial evaluation of image performance of a 3-D X-ray system: Phantom-based comparison of 3-D tomography with conventional computed tomography. J. Med. Imaging 2018, 5, 015502. [Google Scholar] [CrossRef]
- Feldkamp, L.A.; Davis, L.C.; Kress, J.W. Practical cone-beam algorithm. J. Opt. Soc. Am. 1984, 1, 612–619. [Google Scholar] [CrossRef] [Green Version]
- Meyer, E.; Raupach, R.; Lell, M.; Schmidt, B.; Kachelriess, M. Frequency split metal artifact reduction (FSMAR) in computed tomography. Med. Phys. 2012, 39, 1904–1916. [Google Scholar] [CrossRef]
- Schegerer, A.A.; Loose, R.; Heuser, L.; Brix, G. Diagnostic reference levels for diagnostic and interventional X-ray procedures in Germany: Update and handling—Answer to the comments of members of the chest radiology workshop of the German Roentgen Society. Rofo 2020, 192, 83. [Google Scholar] [CrossRef] [PubMed]
- Benz, R.M.; Harder, D.; Amsler, F.; Voigt, J.; Fieselmann, A.; Falkowski, A.L.; Stieltjes, B.; Hirschmann, A. Initial Assessment of a Prototype 3D Cone-Beam Computed Tomography System for Imaging of the Lumbar Spine, Evaluating Human Cadaveric Specimens in the Upright Position. Investig. Radiol. 2018, 53, 714–719. [Google Scholar] [CrossRef] [PubMed]
- International Electrotechnical Commission. Medical Electrical Equipment—Part 2-44, Special Requirements for the Safety of X-Ray Equipment for Computed Tomography; IEC Central Office: Geneva, Switzerland, 2004. [Google Scholar]
- Deak, P.D.; Smal, Y.; Kalender, W.A. Multisection CT protocols: Sex- and age-specific conversion factors used to determine effective dose from dose-length product. Radiology 2010, 257, 158–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nemtoi, A.; Czink, C.; Haba, D.; Gahleitner, A. Cone beam CT: A current overview of devices. Dentomaxillofac. Radiol. 2013, 42, 20120443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nardi, C.; Borri, C.; Regini, F.; Calistri, L.; Castellani, A.; Lorini, C.; Colagrande, S. Metal and motion artifacts by cone beam computed tomography (CBCT) in dental and maxillofacial study. Radiol. Med. 2015, 120, 618–626. [Google Scholar] [CrossRef] [PubMed]
- Ludlow, J.B.; Timothy, R.; Walker, C.; Hunter, R.; Benavides, E.; Samuelson, D.B.; Scheske, M.J. Effective dose of dental CBCT-a meta analysis of published data and additional data for nine CBCT units. Dentomaxillofac. Radiol. 2015, 44, 20140197. [Google Scholar] [CrossRef] [Green Version]
- Nardi, C.; Salerno, S.; Molteni, R.; Occhipinti, M.; Grazzini, G.; Norberti, N.; Cordopatri, C.; Colagrande, S. Radiation dose in non-dental cone beam CT applications: A systematic review. Radiol. Med. 2018, 123, 765–777. [Google Scholar] [CrossRef] [Green Version]
- Fakhran, S.; Alhilali, L.; Sreedher, G.; Dohatcu, A.C.; Lee, S.; Ferguson, B.; Branstetter, B.F., IV. Comparison of simulated cone beam computed tomography to conventional helical computed tomography for imaging of rhinosinusitis. Laryngoscope 2014, 124, 2002–2006. [Google Scholar] [CrossRef]
- Pulickal, G.G.; Navaratnam, A.V.; Nguyen, T.; Dragan, A.D.; Dziedzic, M.; Lingam, R.K. Imaging Sinonasal disease with MRI: Providing insight over and above CT. Eur. J. Radiol. 2018, 102, 157–168. [Google Scholar] [CrossRef]
- Luckow, M.; Deyhle, H.; Beckmann, F.; Dagassan-Berndt, D.; Muller, B. Tilting the jaw to improve the image quality or to reduce the dose in cone-beam computed tomography. Eur. J. Radiol. 2011, 80, e389–e393. [Google Scholar] [CrossRef]
- Spin-Neto, R.; Costa, C.; Salgado, D.M.; Zambrana, N.R.; Gotfredsen, E.; Wenzel, A. Patient movement characteristics and the impact on CBCT image quality and interpretability. Dentomaxillofac. Radiol. 2018, 47, 20170216. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Scan Protocol at 121 kV | Minimum Score of Each Reader | Overall Minimum Score | Average DAP (cGycm2) | Mean CTDIvol (mGy) | ||||
|---|---|---|---|---|---|---|---|---|
| DL (nGy) | Pre-Filtration | Skull 1 | Skull 2 | Skull 3 | Skull 4 | |||
| 278 | 0.2 mm Cu | 2 | 2 | 2 | 2 | 2 | 13.1 | 2.4 |
| 278 | 0.3 mm Cu | 2 | 2 | 2 | 2 | 12.6 | 1.7 | |
| 548 | 0.2 mm Cu | 2 | 2/3 * | 2 | 2/3 * | 2 | 23.9 | 3.2 |
| 548 | 0.3 mm Cu | 2/3 * | 2 | 2/3 * | 2 | 21.0 | 2.8 | |
| 1090 | 0.2 mm Cu | 3 | 3 | 3 | 3/4 * | 3 | 46.5 | 5.2 |
| 1090 | 0.3 mm Cu | 3 | 3 | 3/4 * | 3 | 40.5 | 4.7 | |
| 2180 | 0.2 mm Cu | 3 | 4 | 3/4 * | 4 | 3 | 122.0 | 8.1 |
| 2180 | 0.3 mm Cu | 4 | 3/4 * | 4 | 3 | 153.9 | 5.6 | |
| 278 | 0.4 mm Sn | 1 | 1 | 1 | 1 | 49.3 | 1.3 | |
| 548 | 0.4 mm Sn | 1 | 1 | 1 | 1 | 88.0 | 1.9 | |
| 1090 | 0.4 mm Sn | 1 | 1 | 1/2 * | 1 | 214.0 | 3.2 | |
| 2180 | 0.4 mm Sn | 1 | 1/2 * | 2 | 1 | 400.4 | 5.7 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ohlmeyer, S.; Saake, M.; Buder, T.; May, M.; Uder, M.; Wuest, W. Cone Beam CT Imaging of the Paranasal Region with a Multipurpose X-ray System—Image Quality and Radiation Exposure. Appl. Sci. 2020, 10, 5876. https://doi.org/10.3390/app10175876
Ohlmeyer S, Saake M, Buder T, May M, Uder M, Wuest W. Cone Beam CT Imaging of the Paranasal Region with a Multipurpose X-ray System—Image Quality and Radiation Exposure. Applied Sciences. 2020; 10(17):5876. https://doi.org/10.3390/app10175876
Chicago/Turabian StyleOhlmeyer, Sabine, Marc Saake, Thomas Buder, Matthias May, Michael Uder, and Wolfgang Wuest. 2020. "Cone Beam CT Imaging of the Paranasal Region with a Multipurpose X-ray System—Image Quality and Radiation Exposure" Applied Sciences 10, no. 17: 5876. https://doi.org/10.3390/app10175876