Effect of Whole-Body Vibration on the Functional Responses of the Patients with Knee Osteoarthritis by the Electromyographic Profile of the Vastus Lateralis Muscles during the Five-Repetition Chair Stand Test: A Randomized Crossover Trial

 ,
,  ,
,  , ,
, ,  , , , ,
, , , ,  ,
,  ,
,  add
Show full author list
add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Sample Size
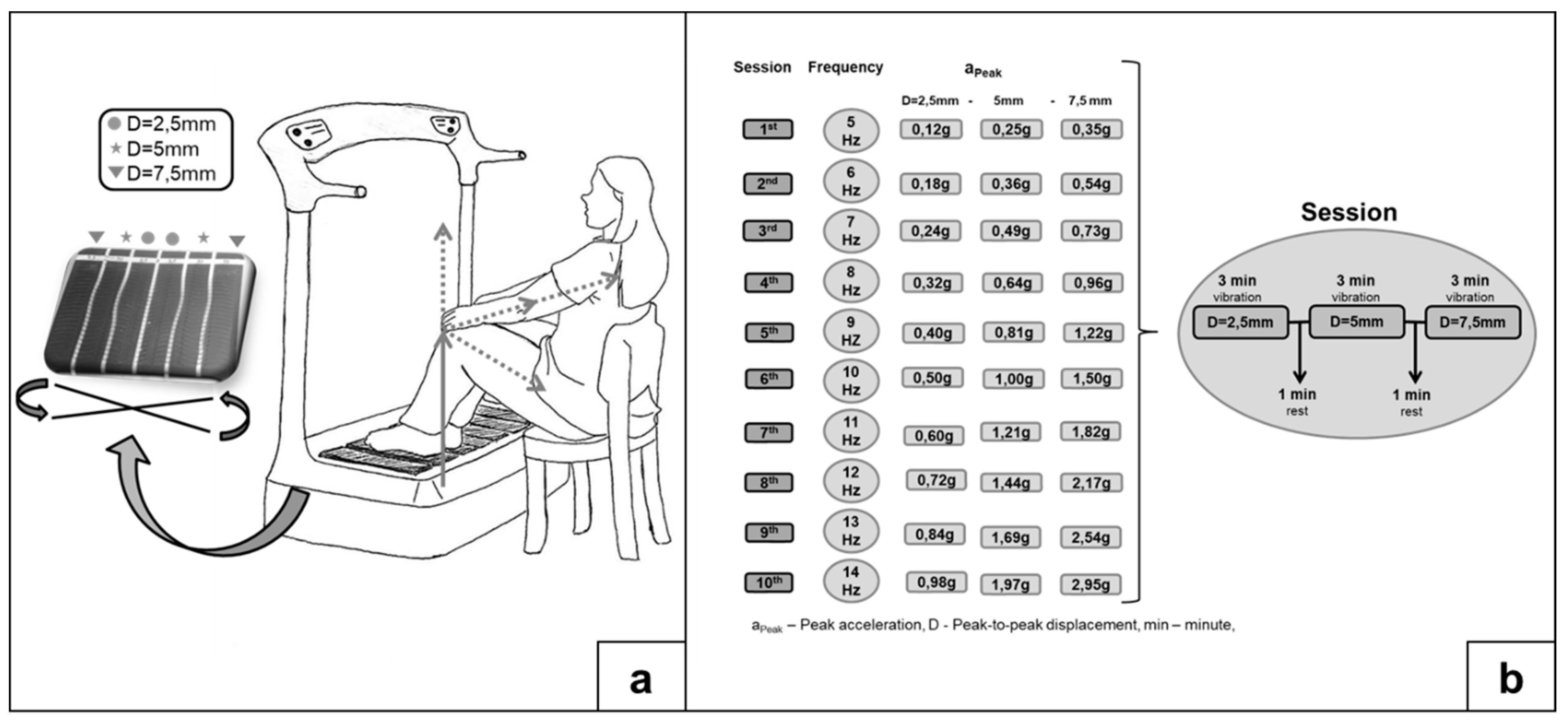
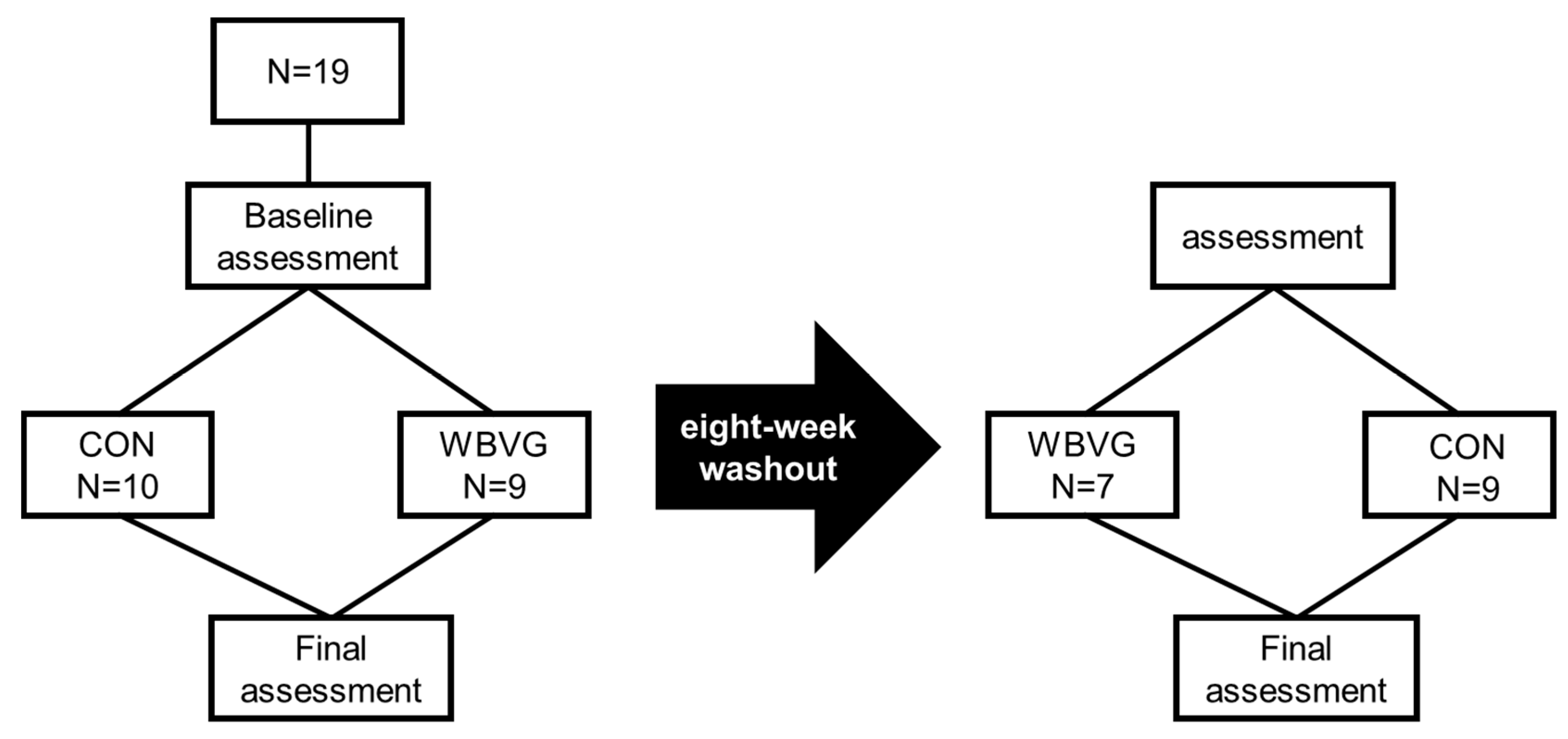
2.3. Interventions and Groups
2.4. Physical Performance Measures
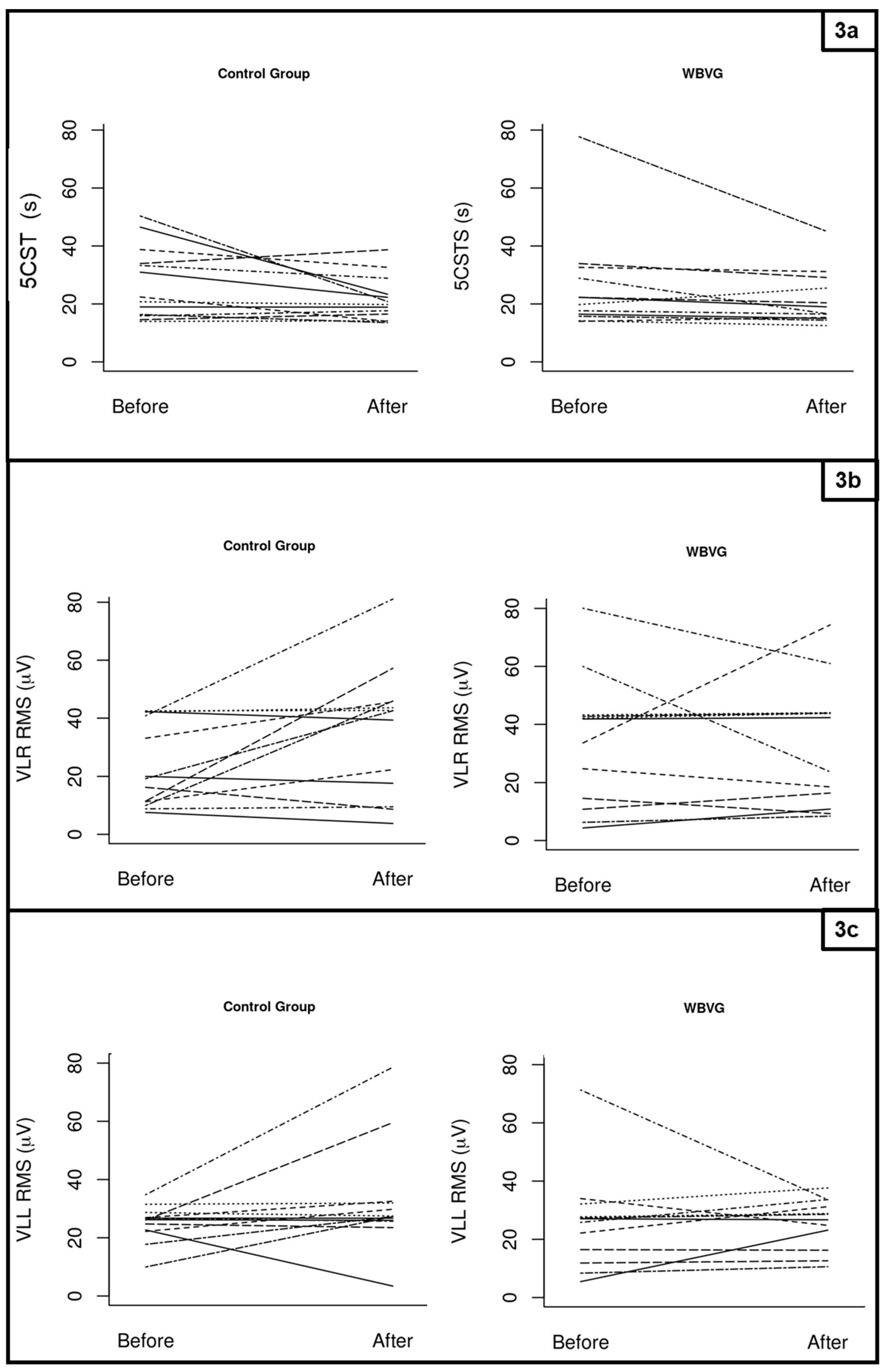
2.4.1. Five-Repetition Chair Stand Test
2.4.2. Measurement and Surface Electromyography Instrumentation
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Cross, M.; Smith, E.; Hoy, D.; Nolte, S.; Ackerman, I.; Fransen, M.; Bridgett, L.; Williams, S.; Guillemin, F.; Hill, C.L.; et al. The global burden of hip and knee osteoarthritis: Estimates from the Global Burden of Disease 2010 study. Ann. Rheum. Dis. 2014, 73, 1323–1330. [Google Scholar] [CrossRef]
- Xu, Q.; Chen, B.; Wang, Y.; Wang, X.; Han, D.; Ding, D.; Zheng, Y.; Cao, Y.; Zhan, H.; Zhou, Y. The Effectiveness of Manual Therapy for Relieving Pain, Stiffness, and Dysfunction in Knee Osteoarthritis: A Systematic Review and Meta-Analysis. Pain Physician 2017, 20, 229–243. [Google Scholar] [CrossRef] [Green Version]
- Kolasinski, S.L.; Neogi, T.; Hochberg, M.C.; Oatis, C.; Guyatt, G.; Block, J.; Callahan, L.; Copenhaver, C.; Dodge, C.; Felson, D.; et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis Rheumatol. 2020, 72, 220–233. [Google Scholar] [CrossRef]
- Holla, J.F.M.; van der Leeden, M.; Heymans, M.W.; Roorda, L.D.; Bierma-Zeinstra, S.M.A.; Boers, M.; Lems, W.F.; Steultjens, M.P.; Dekker, J. Three trajectories of activity limitations in early symptomatic knee osteoarthritis: A 5-year follow-up study. Ann. Rheum. Dis. 2014, 73, 1369–1375. [Google Scholar] [CrossRef] [Green Version]
- Lai, Z.; Wang, X.; Lee, S.; Hou, X.; Wang, L. Effects of whole body vibration exercise on neuromuscular function for individuals with knee osteoarthritis: Study protocol for a randomized controlled trial. Trials 2017, 18, 437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, L. The Role of Proprioceptive Deficits, Ligamentous Laxity, and Malalignment in Development and Progression of Knee Osteoarthritis. J. Rheumatol. 2004, 70, 87–92. [Google Scholar]
- Mills, K.; Hunt, M.A.; Leigh, R.; Ferber, R. A systematic review and meta-analysis of lower limb neuromuscular alterations associated with knee osteoarthritis during level walking. Clin. Biomech. 2013, 28, 713–724. [Google Scholar] [CrossRef] [PubMed]
- Bigham, H.J.; Flaxman, T.E.; Smith, A.J.J.; Benoit, D.L. Neuromuscular adaptations in older males and females with knee osteoarthritis during weight-bearing force control. Knee 2018, 25, 40–50. [Google Scholar] [CrossRef]
- Vigotsky, A.D.; Halperin, I.; Lehman, G.J.; Trajano, G.S.; Vieira, T.M. Interpreting signal amplitudes in surface electromyography studies in sport and rehabilitation sciences. Front. Physiol. 2018, 8, 985. [Google Scholar] [CrossRef] [Green Version]
- Hislop, A.C.; Collins, N.J.; Tucker, K.; Deasy, M.; Semciw, A.I. Does adding hip exercises to quadriceps exercises result in superior outcomes in pain, function and quality of life for people with knee osteoarthritis? A systematic review and meta-analysis. Br. J. Sports Med. 2019, 54, 263–271. [Google Scholar] [CrossRef]
- Clausen, B.; Holsgaard-Larsen, A.; Roos, E.M. An 8-Week Neuromuscular Exercise Program for Patients With Mild to Moderate Knee Osteoarthritis: A Case Series Drawn From a Registered Clinical Trial. J. Athl. Train. 2017, 52, 592–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bokaeian, H.R.; Bakhtiary, A.H.; Mirmohammadkhani, M.; Moghimi, J. The effect of adding whole body vibration training to strengthening training in the treatment of knee osteoarthritis: A randomized clinical trial. J. Bodyw. Mov. Ther. 2016, 20, 334–340. [Google Scholar] [CrossRef] [PubMed]
- Neto, S.B.S.; Marconi, E.M.; Kutter, C.R.; Frederico, E.H.F.F.; de Paiva, P.D.C.; Meyer, P.F.; Chang, S.; Sá-Caputo, D.; Bernardo-Filho, M. Beneficial effects of whole body mechanical vibration alone or combined with auriculotherapy in the pain and in flexion of knee of individuals with knee osteoarthritis. Acupunct. Electrother. Res. 2017, 42, 185–201. [Google Scholar] [CrossRef]
- Moreira-Marconi, E.; Sa-Caputo, D.C.; Dionello, C.F.; Guedes-Aguiar, E.O.; Sousa-Goncalves, C.R.; Morel, D.S.; Paineiras-Domingos, L.L.; Stark, C.; Unger, M.; Bernardo-Filho, M. Whole-body vibration exercise is well tolerated in patients with duchenne muscular dystrophy: A systematic review. African J. Tradit. Complement. Altern. Med. 2017, 14, 2–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferreira, R.; Duarte, J.; Gonçalves, R. Non-pharmacological and non-surgical interventions to manage patients with knee osteoarthritis: An umbrella review. Acta Reumalol. Port 2018, 43, 182–200. [Google Scholar]
- Liphardt, A.M.; Mündermann, A.; Koo, S.; Bäcker, N.; Andriacchi, T.P.; Zange, J.; Mester, J.; Heer, M. Vibration training intervention to maintain cartilage thickness and serum concentrations of cartilage oligometric matrix protein (COMP) during immobilization. Osteoarthr. Cartil. 2009, 17, 1598–1603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rittweger, J. Vibration as an exercise modality: How it may work, and what its potential might be. Eur. J. Appl. Physiol. 2010, 108, 877–904. [Google Scholar] [CrossRef]
- Musumeci, G.; Loreto, C.; Leonardi, R.; Castorina, S.; Giunta, S.; Carnazza, M.L.; Maria Trovato, M.; Pichler, K.; Weinberg, A.M. The effects of physical activity on apoptosis and lubricin expression in articular cartilage in rats with glucocorticoid-induced osteoporosis. J. Bone Miner. Metabo. 2013, 31, 274–284. [Google Scholar] [CrossRef]
- Guglielmino, C.; Musumeci, G. Early Elbow Osteoarthritis in Competitive Enduro Motorcyclist. Scand. J. Med. Sci. Sports 2020. [Google Scholar] [CrossRef]
- Cardinale, M.; Pope, M. The effects of whole body vibration on humans: Dangerous or advantageous? Acta Physiol. Hung. 2003, 90, 195–206. [Google Scholar] [CrossRef]
- Wang, P.; Yang, L.; Liu, C.; Wei, X.; Yang, X.; Zhou, Y.; Jiang, H.; Lei, Z.; Reinhardt, J.D.; He, C. Effects of Whole Body Vibration Exercise associated with Quadriceps Resistance Exercise on functioning and quality of life in patients with knee osteoarthritis: A randomized controlled trial. Clin. Rehabil. 2016, 30, 1074–1087. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.-Q.; Huang, L.-Y.; Liu, Y.; Li, J.-X.; Wu, X.; Li, H.-P.; Wang, L. Effects of tai chi program on neuromuscular function for patients with knee osteoarthritis: Study protocol for a randomized controlled trial. Trials 2013, 14, 375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, X.; Wang, P.; Liu, C.; He, C.; Reinhardt, J.D. The effect of whole body vibration on balance, gait performance and mobility in people with stroke: A systematic review and meta-analysis. Clin. Rehabil. 2015, 29, 627–638. [Google Scholar] [CrossRef] [PubMed]
- Moreira-Marconi, E.; Dionello, C.F.; Morel, D.S.; Sá-Caputo, D.C.; Souza-Gonçalves, C.R.; Paineiras-Domingos, L.L.; Guedes-Aguiar, E.O.; Marin, P.J.; del Cruz, B.P.; Bernardo-Filho, M. Could whole body vibration exercises influence the risk factors for fractures in women with osteoporosis? Osteoporos. Sarcopenia 2016, 2, 214–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dionello, C.F.; Sá-Caputo, D.; Pereira, H.V.F.S.; Sousa-Gonçalves, C.R.; Maiworm, A.I.; Morel, D.S.; Moreira-Marconi, E.; Paineiras-Domingos, L.L.; Bemben, D.; Bernardo-Filho, M. Effects of whole body vibration exercises on bone mineral density of women with postmenopausal osteoporosis without medications: Novel findings and literature review. J. Musculoskelet. Neuronal Interact. 2016, 16, 193–203. [Google Scholar]
- Paineiras-Domingos, L.L.; Sá-Caputo, D.D.C.D.; Moreira-Marconi, E.; Morel, D.S.; da Fontoura Dionello, C.; Sousa-Gonçalves, C.R.; Frederico, É.H.F.F.; Marín, P.J.; Tamini, S.; Sartorio, A.; et al. Can whole body vibration exercises affect growth hormone concentration? A systematic review. Growth Factors 2017, 35, 189–200. [Google Scholar] [CrossRef]
- Sá-Caputo, D.A.C.; Ronikeili-Costa, P.; Carvalho-Lima, R.P.; Bernardo, L.C.; Bravo-Monteiro, M.O.; Costa, R.; de Moraes-Silva, J.; Paiva, D.N.; Machado, C.B.; Mantilla-Giehl, P.; et al. Whole Body Vibration Exercises and the Improvement of the Flexibility in Patient with Metabolic Syndrome. Rehabil. Res. Pract. 2014, 2014, 628518. [Google Scholar] [CrossRef] [Green Version]
- Kütter, C.R.; Moreira-Marconi, E.; Teixeira-Silva, Y.; Moura-Fernandes, M.C.; de Meirelles, A.G.; José dos Santos Pereira, M.; Chang, S.; Bachur, J.A.; Paineiras-Domingos, L.L.; Taiar, R.; et al. Effects of the whole-body vibration and auriculotherapy on the functionality of knee osteoarthritis individuals. Appl. Sci. 2019, 9, 5194. [Google Scholar] [CrossRef] [Green Version]
- Moura-Fernandes, M.C.; Moreira-Marconi, E.; Gonçalves de Meirelles, A.; Paula Ferreira de Oliveira, A.; Silva, A.R.; Felipe Ferreira de Souza, L.; Lírio Pereira da Silva, A.; dos Santos-Fernandes, C.; Bessa Monteiro de Oliveira, B.; Antonio de Souza Gama, M.; et al. Effect of the Combined Intervention with Passive Whole-Body Vibration and Auriculotherapy on the Quality of Life of Individuals with Knee Osteoarthritis Assessed by the WHOQOL-Bref: A Multi-Arm Clinical Trial. Appl. Sci. 2020, 10, 1956. [Google Scholar] [CrossRef] [Green Version]
- Davidson, B.S.; Judd, D.L.; Thomas, A.C.; Mizner, R.L.; Eckhoff, D.G.; Stevens-Lapsley, J.E. Muscle activation and coactivation during five-time-sit-to-stand movement in patients undergoing total knee arthroplasty. J. Electromyogr. Kinesiol. 2013, 23, 1485–1493. [Google Scholar] [CrossRef]
- Ahlback, S. Osteoarthrosis of the knee. A radiographic investigation. Acta Radiol. 1968, 277, 7–72. [Google Scholar]
- Miot, H.A. Tamanho da amostra em estudos clínicos e experimentais. J. Vasc. Bras. 2011, 10, 275–278. [Google Scholar] [CrossRef] [Green Version]
- Rodrigues Da Silva, J.M.; De Rezende, M.U.; Spada, T.C.; Da Silva Francisco, L.; Sabine De Farias, F.E.; Clemente Da Silva, C.A.; Cernigoy, C.H.D.A.; Greve, J.M.D.A.; Ciolac, E.G. Educational program promoting regular physical exercise improves functional capacity and daily living physical activity in subjects with knee osteoarthritis. BMC Musculoskelet. Disord. 2017, 18, 546. [Google Scholar] [CrossRef] [PubMed]
- Dwan, K.; Li, T.; Altman, D.G.; Elbourne, D. CONSORT 2010 statement: Extension to randomised crossover trials. BMJ 2019, 366, l4378. [Google Scholar] [CrossRef] [Green Version]
- Hiroshige, K.; Mahbub, M.H.; Harada, N. Effects of whole-body vibration on postural balance and proprioception in healthy young and elderly subjects: A randomized cross-over study. J. Sports Med. Phys. Fitness 2014, 54, 216–224. [Google Scholar]
- Furness, T.; Bate, N.; Welsh, L.; Naughton, G.; Lorenzen, C. Efficacy of a whole-body vibration intervention to effect exercise tolerance and functional performance of the lower limbs of people with chronic obstructive pulmonary disease. BMC Pulm. Med. 2012, 12, 71. [Google Scholar] [CrossRef] [Green Version]
- Hermens, H.J.; Freriks, B.; Disselhorst-Klug, C.; Rau, G. Development of recommendations for SEMG sensors and sensor placement procedures. J. Electromyogr. Kinesiol. 2000, 10, 361–374. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2018; ISBN 3-900051-07-0. [Google Scholar]
- Hothorn, T.; Hornik, K.; Van de Wiel, M.; Zeileis, A. Implementing a Class of Permutation Tests: The coin Package. J. Stat. Softw. 2008, 28, 1–23. [Google Scholar] [CrossRef]
- Fransen, M.; Mcconnell, S.; Harmer, A.R.; Van Der Esch, M.; Simic, M.; Bennell, K.L. Exercise for osteoarthritis of the knee: A Cochrane systematic review. Br. J. Sports Med. 2015, 49, 1554–1557. [Google Scholar] [CrossRef]
- Salmon, J.R.; Roper, J.A.; Tillman, M.D. Does Acute Whole-Body Vibration Training Improve the Physical Performance of People with Knee Osteoarthritis? J. Strength Cond. Res. 2012, 26, 2983–2989. [Google Scholar] [CrossRef] [Green Version]
- Avelar, N.C.P.; Simão, A.P.; Tossige-Gomes, R.; Neves, C.D.C.; Rocha-Vieira, E.; Coimbra, C.C.; Lacerda, A.C.R. The Effect of Adding Whole-Body Vibration to Squat Training on the Functional Performance and Self-Report of Disease Status in Elderly Patients with Knee Osteoarthritis: A Randomized, Controlled Clinical Study. J. Altern. Complement. Med. 2011, 17, 1149–1155. [Google Scholar] [CrossRef] [PubMed]
- Trans, T.; Aaboe, J.; Henriksen, M.; Christensen, R.; Bliddal, H.; Lund, H. Effect of whole body vibration exercise on muscle strength and proprioception in females with knee osteoarthritis. Knee 2009, 16, 256–261. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Yang, X.; Yang, Y.; Yang, L.; Zhou, Y.; Liu, C.; Reinhardt, J.D.; He, C. Effects of whole body vibration on pain, stiffness and physical functions in patients with knee osteoarthritis: A systematic review and meta-analysis. Clin. Rehabil. 2015, 29, 939–951. [Google Scholar] [CrossRef] [PubMed]
- Avelar, N.C.P.; Ribeiro, V.G.C.; Mezêncio, B.; Fonseca, S.F.; Tossige-Gomes, R.; da Costa, S.J.; Szmuchrowski, L.; Gripp, F.; Coimbra, C.C.; Lacerda, A.C.R. Influence of the knee flexion on muscle activation and transmissibility during whole body vibration. J. Electromyogr. Kinesiol. 2013, 23, 844–850. [Google Scholar] [CrossRef]
- Abbasi, E.; Kahrizi, S.; Razi, M.; Faghihzadeh, S. The effect of whole-body vibration training on the lower extremity muscles ’ electromyographic activities in patients with knee osteoarthritis. Med. J. Islam. Repub. Iran 2017, 31, 107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benedetti, M.G.M.G.; Boccia, G.; Cavazzuti, L.; Magnani, E.; Mariani, E.; Rainoldi, A.; Casale, R. Localized muscle vibration reverses quadriceps muscle hypotrophy and improves physical function: A clinical and electrophysiological study. Int. J. Rehabil. Res. 2017, 40, 339–346. [Google Scholar] [CrossRef]
- Bosco, C.; Colli, R.; Introini, E.; Cardinale, M.; Tsarpela, O.; Madella, A.; Tihanyi, J.; Viru, A. Adaptive responses of human skeletal muscle to vibration exposure. Clin. Physiol. 1999, 19, 183–187. [Google Scholar] [CrossRef]
- Cardinale, M.; Lim, J. Electromyography activity of vastus lateralis muscle during whole-body vibrations of different frequencies. J. Strength Cond. Res. 2003, 17, 621–624. [Google Scholar]
- Pollock, R.D.; Woledge, R.C.; Martin, F.C.; Newham, D.J. Effects of whole body vibration on motor unit recruitment and threshold. J. Appl. Physiol. 2012, 112, 388–395. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variables | CON (n = 10) | WBVG (n = 9) | p-Value |
|---|---|---|---|
| Age (years) | 66.89 (8.55) | 64.1 (8.50) | 0.4862 |
| Stature (m) | 1.592 (0.08) | 1.568 (0.07) | 0.4878 |
| Body mass (kg) | 84.91 (14.7) | 85.21 (16.28) | 0.9671 |
| Body mass index (kg.m−2) | 33.73 (6.92) | 34.98 (8.69) | 0.9438 |
| Mean | Range | Standard Deviation | Coefficient of Variation | Standard Error | Minimum | 1st Quartile | Median | 3rd Quartile | Maximum | p-Value | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 5CST (s) | CON (n = 19) | Before | 27.43 | 36.37 | 12.41 | 0.45 | 3.44 | 13.97 | 16.35 | 22.41 | 33.94 | 50.34 | 0.060 |
| After | 21.63 | 25.12 | 7.63 | 0.35 | 2.11 | 13.57 | 16.50 | 19.78 | 23.34 | 38.69 | |||
| WBVG (n = 16) | Before | 27.29 | 63.69 | 17.21 | 0.63 | 4.77 | 14.00 | 16.47 | 22.28 | 32.63 | 77.69 | 0.018 & | |
| After | 21.72 | 32.57 | 9.49 | 0.43 | 2.73 | 12.53 | 15.25 | 17.82 | 26.38 | 45.10 | |||
| VLR RMS (μV) | CON (n = 19) | Before | 23.49 | 34.96 | 14.38 | 0.61 | 3.99 | 7.57 | 11.30 | 19.22 | 40.84 | 42.53 | 0.352 |
| After | 35.36 | 77.33 | 22.05 | 0.62 | 6.11 | 3.76 | 17.63 | 42.54 | 45.6 | 81.09 | |||
| WBVG (n = 16) | Before | 32.85 | 75.73 | 22.07 | 0.67 | 6.12 | 4.34 | 14.56 | 33.67 | 42.73 | 80.07 | 0.599 | |
| After | 33.03 | 65.88 | 21.65 | 0.65 | 6.25 | 8.43 | 15.00 | 33.01 | 43.91 | 74.31 | |||
| VLL RMS (μV) | CON (n = 19) | Before | 24.99 | 24.83 | 6.16 | 0.24 | 1.71 | 9.96 | 22.68 | 26.21 | 26.93 | 34.79 | 0.095 |
| After | 32.28 | 75.20 | 18.24 | 0.56 | 5.06 | 3.39 | 25.97 | 27.29 | 31.93 | 78.59 | |||
| WBVG (n = 16) | Before | 24.77 | 65.82 | 16.73 | 0.67 | 4.64 | 5.47 | 12.45 | 25.82 | 27.72 | 71.29 | 0.454 | |
| After | 25.64 | 27.05 | 8.60 | 0.33 | 2.48 | 10.59 | 21.42 | 27.64 | 31.81 | 37.64 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moreira-Marconi, E.; Teixeira-Silva, Y.; Meirelles, A.G.d.; Moura-Fernandes, M.C.; Lopes-Souza, P.; Reis-Silva, A.; Marchon, R.M.; Guedes-Aguiar, E.d.O.; Paineiras-Domingos, L.L.; de Sá-Caputo, D.d.C.; et al. Effect of Whole-Body Vibration on the Functional Responses of the Patients with Knee Osteoarthritis by the Electromyographic Profile of the Vastus Lateralis Muscles during the Five-Repetition Chair Stand Test: A Randomized Crossover Trial. Appl. Sci. 2020, 10, 4302. https://doi.org/10.3390/app10124302
Moreira-Marconi E, Teixeira-Silva Y, Meirelles AGd, Moura-Fernandes MC, Lopes-Souza P, Reis-Silva A, Marchon RM, Guedes-Aguiar EdO, Paineiras-Domingos LL, de Sá-Caputo DdC, et al. Effect of Whole-Body Vibration on the Functional Responses of the Patients with Knee Osteoarthritis by the Electromyographic Profile of the Vastus Lateralis Muscles during the Five-Repetition Chair Stand Test: A Randomized Crossover Trial. Applied Sciences. 2020; 10(12):4302. https://doi.org/10.3390/app10124302
Chicago/Turabian StyleMoreira-Marconi, Eloá, Ygor Teixeira-Silva, Alexandre Gonçalves de Meirelles, Marcia Cristina Moura-Fernandes, Patrícia Lopes-Souza, Aline Reis-Silva, Renata Marques Marchon, Eliane de Oliveira Guedes-Aguiar, Laisa Liane Paineiras-Domingos, Danúbia da Cunha de Sá-Caputo, and et al. 2020. "Effect of Whole-Body Vibration on the Functional Responses of the Patients with Knee Osteoarthritis by the Electromyographic Profile of the Vastus Lateralis Muscles during the Five-Repetition Chair Stand Test: A Randomized Crossover Trial" Applied Sciences 10, no. 12: 4302. https://doi.org/10.3390/app10124302