A Smart Terrain Identification Technique Based on Electromyography, Ground Reaction Force, and Machine Learning for Lower Limb Rehabilitation


Abstract
:1. Introduction
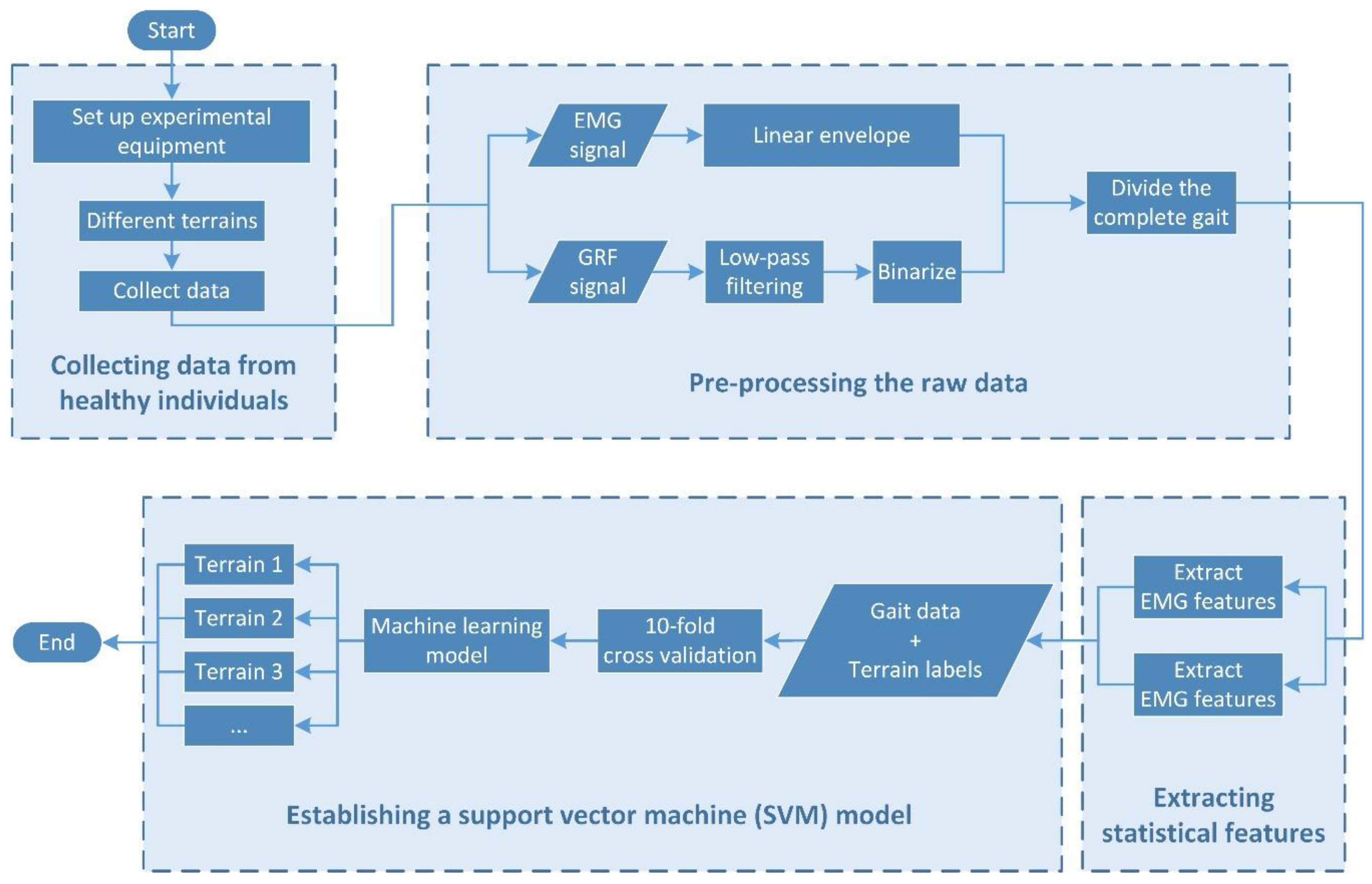
2. Methodology
- Collecting data from healthy individuals;
- Pre-processing the raw data;
- Extracting the statistical features;
- Establishing an SVM model.
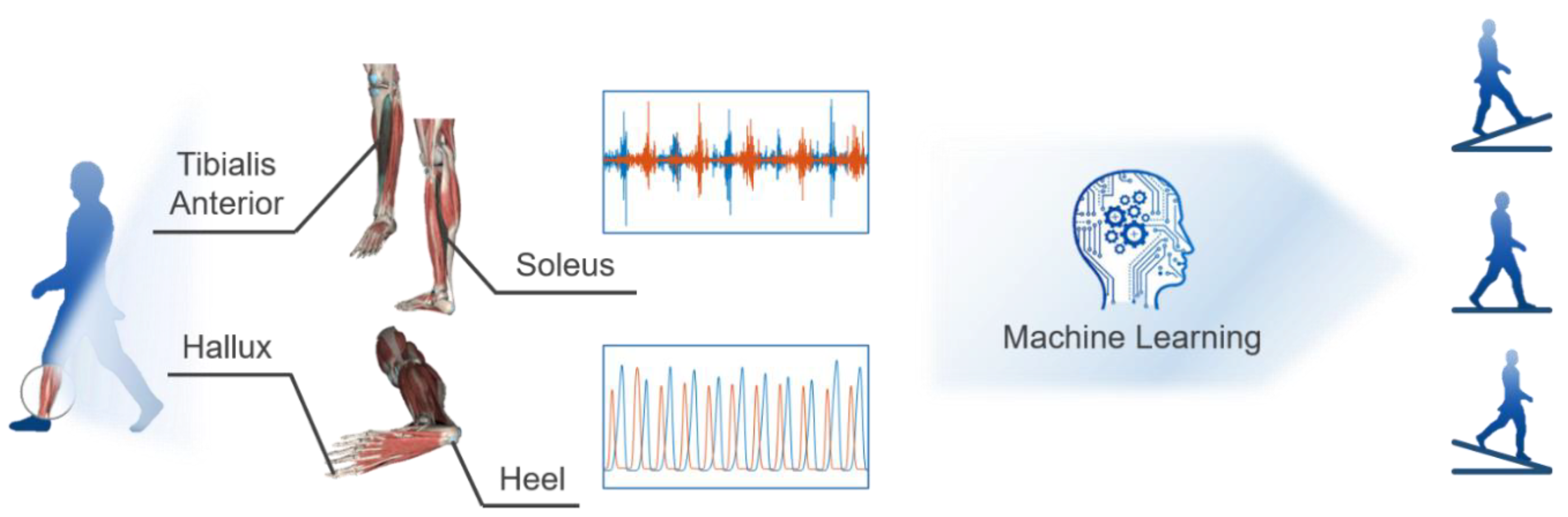
2.1. Experiment Setup
2.2. Data Pre-Processing
2.3. Feature Extraction
- Force and time features extracted from the GRF curve. Such features reflect the variation and relationship of the two GRF measures during a stride or between two consecutive strides and they are depicted in Figure 4a.
- Time-domain features extracted from the filtered EMG data, including the mean absolute value (MAV), standard deviation (STD), root mean square (RMS), and waveform length (WL), which are broadly used features, such as in [28,49]. Such features reflect the overall activation level of the muscle in a stride.
- Muscle force features extracted from the EMG and LE, including the TA peak, TA 80, SL peak, SL 25. Such features reflect the muscle force level at a particular timing of a stride and they are depicted in Figure 4b.
2.4. Establishment of SVM Model
2.5. Evaluation of the Selected Features and the SVM Model
3. Results and Discussion
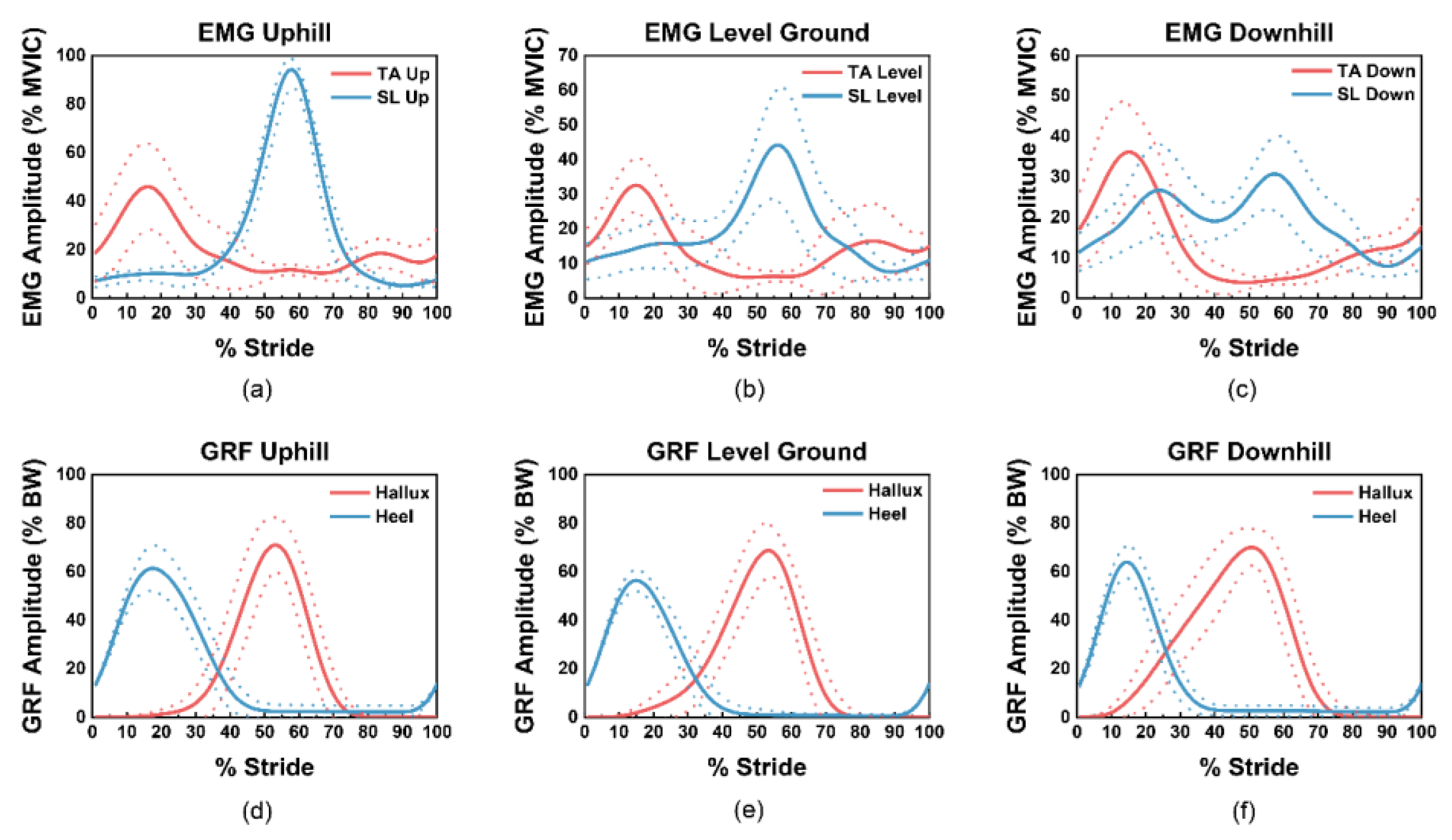
- The profile of the EMG, LE and GRF curves;
- The comparison and explanation of the differences between the extracted features in the different terrains;
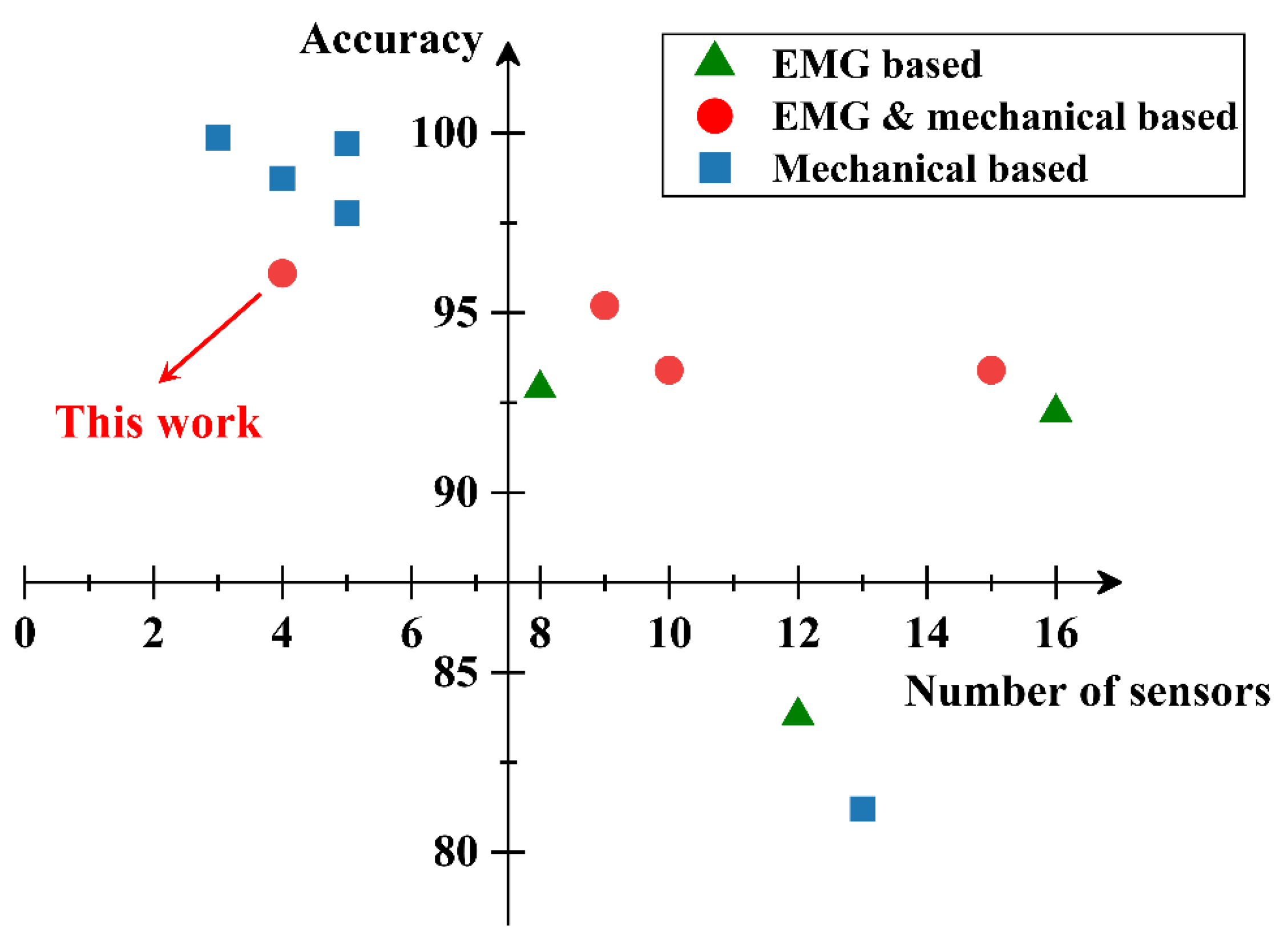
- The classification performance of the SVM model and the discussion on sensor fusion.
3.1. EMG and GRF Profiles
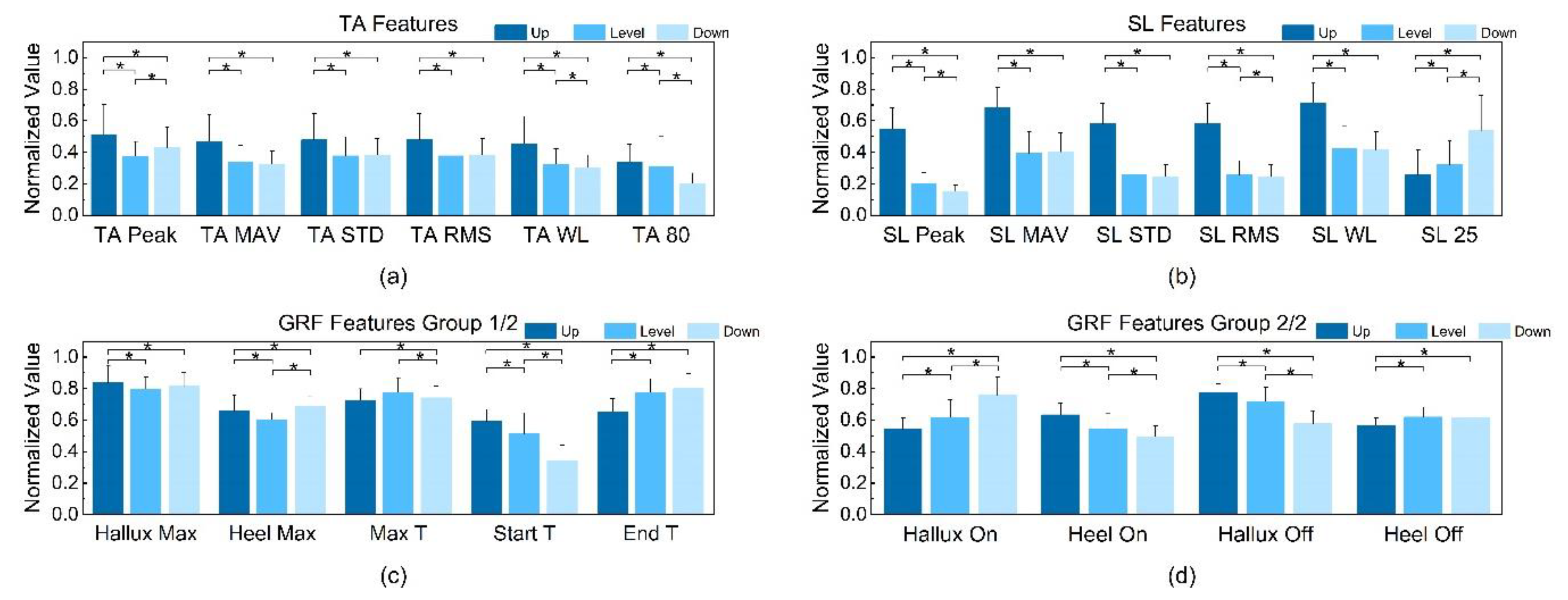
3.2. Statistical Features in Different Terrains
3.2.1. TA EMG
3.2.2. SL EMG
3.2.3. Ground Reaction Force
3.3. Training Performance of SVM and Comparison between the EMG and GRF Features
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Yan, T.F.; Cempini, M.; Oddo, C.M.; Vitiello, N. Review of assistive strategies in powered lower-limb orthoses and exoskeletons. Robot. Auton. Syst. 2015, 64, 120–136. [Google Scholar] [CrossRef]
- Mekki, M.; Delgado, A.D.; Fry, A.; Putrino, D.; Huang, V. Robotic Rehabilitation and Spinal Cord Injury: A Narrative Review. Neurotherapeutics 2018, 15, 604–617. [Google Scholar] [CrossRef] [Green Version]
- Meng, W.; Liu, Q.; Zhou, Z.D.; Ai, Q.S.; Sheng, B.; Xie, S.Q. Recent development of mechanisms and control strategies for robot-assisted lower limb rehabilitation. Mechatronics 2015, 31, 132–145. [Google Scholar] [CrossRef]
- Chen, B.; Zi, B.; Wang, Z.Y.; Qin, L.; Liao, W.H. Knee exoskeletons for gait rehabilitation and human performance augmentation: A state-of-the-art. Mech. Mach. Theory 2019, 134, 499–511. [Google Scholar] [CrossRef]
- Shultz, A.H.; Lawson, B.E.; Goldfarb, M. Variable Cadence Walking and Ground Adaptive Standing with a Powered Ankle Prosthesis. IEEE Trans. Neural Syst. Rehabil. Eng. 2016, 24, 495–505. [Google Scholar] [CrossRef]
- Esquenazi, A.; Talaty, M.; Packel, A.; Saulino, M. The ReWalk Powered Exoskeleton to Restore Ambulatory Function to Individuals with Thoracic-Level Motor-Complete Spinal Cord Injury. Am. J. Phys. Med. Rehabil. 2012, 91, 911–921. [Google Scholar] [CrossRef] [Green Version]
- Kawamoto, H.; Lee, S.; Kanbe, S.; Sankai, Y. Power assist method for HAL-3 using EMG-based feedback controller. In Proceedings of the SMC’03 Conference Proceedings. 2003 IEEE International Conference on Systems, Man and Cybernetics. Conference Theme—System Security and Assurance (Cat. No.03CH37483), Washington, DC, USA, 8 October 2003; pp. 1648–1653. [Google Scholar]
- Yano, H.; Tamefusa, S.; Tanaka, N.; Saitou, H.; Iwata, H. Gait rehabilitation system for stair climbing and descending. In Proceedings of the 2010 IEEE Haptics Symposium, Waltham, MA, USA, 25–26 March 2010; pp. 393–400. [Google Scholar]
- Bisio, I.; Delfino, A.; Lavagetto, F.; Sciarrone, A. Enabling IoT for in-home rehabilitation: Accelerometer signals classification methods for activity and movement recognition. IEEE Internet Things J. 2016, 4, 135–146. [Google Scholar] [CrossRef]
- Horak, F.; King, L.; Mancini, M. Role of body-worn movement monitor technology for balance and gait rehabilitation. Phys. Ther. 2015, 95, 461–470. [Google Scholar] [CrossRef] [Green Version]
- Bianchi, V.; Bassoli, M.; Lombardo, G.; Fornacciari, P.; Mordonini, M.; De Munari, I. IoT Wearable Sensor and Deep Learning: An Integrated Approach for Personalized Human Activity Recognition in a Smart Home Environment. IEEE Internet Things J. 2019, 6, 8553–8562. [Google Scholar] [CrossRef]
- Kańtoch, E. Human activity recognition for physical rehabilitation using wearable sensors fusion and artificial neural networks. In Proceedings of the 2017 Computing in Cardiology (CinC), Rennes, France, 24–27 September 2017; pp. 1–4. [Google Scholar]
- Shi, D.; Zhang, W.; Zhang, W.; Ding, X. A Review on Lower Limb Rehabilitation Exoskeleton Robots. Chin. J. Mech. Eng. 2019, 32, 74. [Google Scholar] [CrossRef] [Green Version]
- Banala, S.K.; Kim, S.H.; Agrawal, S.K.; Scholz, J.P. Robot assisted gait training with active leg exoskeleton (ALEX). IEEE Trans. Neural Syst. Rehabil. Eng. 2008, 17, 2–8. [Google Scholar] [CrossRef]
- Taati, B.; Wang, R.; Huq, R.; Snoek, J.; Mihailidis, A. Vision-based posture assessment to detect and categorize compensation during robotic rehabilitation therapy. In Proceedings of the 2012 4th IEEE RAS & EMBS International Conference on Biomedical Robotics and Biomechatronics (BioRob), Rome, Italy, 24–27 June 2012; pp. 1607–1613. [Google Scholar]
- Marchal-Crespo, L.; Riener, R. Robot-assisted gait training. In Rehabilitation Robotics; Academic Press: London, UK, 2018; pp. 227–240. [Google Scholar]
- Yuan, K.B.; Wang, Q.N.; Wang, L. Fuzzy-Logic-Based Terrain Identification with Multisensor Fusion for Transtibial Amputees. IEEE-Asme Trans. Mech. 2015, 20, 618–630. [Google Scholar] [CrossRef]
- Gupta, R.; Agarwal, R. Electromyographic Signal-Driven Continuous Locomotion Mode Identification Module Design for Lower Limb Prosthesis Control. Arab. J. Sci. Eng. 2018, 43, 7817–7835. [Google Scholar] [CrossRef]
- Long, Y.; Du, Z.-J.; Wang, W.-D.; Zhao, G.-Y.; Xu, G.-Q.; He, L.; Mao, X.-W.; Dong, W. PSO-SVM-based online locomotion mode identification for rehabilitation robotic exoskeletons. Sensors 2016, 16, 1408. [Google Scholar] [CrossRef] [Green Version]
- Kyeong, S.; Shin, W.; Yang, M.; Heo, U.; Feng, J.-R.; Kim, J. Recognition of walking environments and gait period by surface electromyography. Front. Inf. Technol. Electron. Eng. 2019, 20, 342–352. [Google Scholar] [CrossRef]
- Joshi, D.; Hahn, M.E. Terrain and Direction Classification of Locomotion Transitions Using Neuromuscular and Mechanical Input. Ann. Biomed. Eng. 2016, 44, 1275–1284. [Google Scholar] [CrossRef]
- Afzal, T.; Iqbal, K.; White, G.; Wright, A.B. A method for locomotion mode identification using muscle synergies. IEEE Trans. Neural Syst. Rehabil. Eng. 2016, 25, 608–617. [Google Scholar] [CrossRef]
- Huo, W.G.; Mohammed, S.; Amirat, Y.; Kong, K. Active Impedance Control of a Lower Limb Exoskeleton to Assist Sit-to-Stand Movement. In Proceedings of the 2016 IEEE International Conference on Robotics and Automation, Stockholm, Sweden, 16–21 May 2016; Okamura, A., Menciassi, A., Ude, A., Burschka, D., Lee, D., Arrichiello, F., Liu, H., Moon, H., Neira, J., Sycara, K., Eds.; IEEE: New York, NY, USA, 2016; pp. 3530–3536. [Google Scholar]
- Lim, D.H.; Kim, W.S.; Kim, H.J.; Han, C.S. Development of real-time gait phase detection system for a lower extremity exoskeleton robot. Int. J. Precis. Eng. Manuf. 2017, 18, 681–687. [Google Scholar] [CrossRef]
- Peternel, L.; Noda, T.; Petric, T.; Ude, A.; Morimoto, J.; Babic, J. Adaptive Control of Exoskeleton Robots for Periodic Assistive Behaviours Based on EMG Feedback Minimisation. PLoS ONE 2016, 11, 26. [Google Scholar] [CrossRef] [Green Version]
- Young, A.J.; Ferris, D.P. State of the Art and Future Directions for Lower Limb Robotic Exoskeletons. IEEE Trans. Neural Syst. Rehabil. Eng. 2017, 25, 171–182. [Google Scholar] [CrossRef]
- Young, A.J.; Simon, A.M.; Hargrove, L.J. A Training Method for Locomotion Mode Prediction Using Powered Lower Limb Prostheses. IEEE Trans. Neural Syst. Rehabil. Eng. 2014, 22, 671–677. [Google Scholar] [CrossRef]
- Jin, D.; Yang, J.; Zhang, R.; Wang, R.; Zhang, J. Terrain identification for prosthetic knees based on electromyographic signal features. Tsinghua Sci. Technol. 2006, 11, 74–79. [Google Scholar] [CrossRef]
- Shultz, A.H.; Goldfarb, M. A Unified Controller for Walking on Even and Uneven Terrain with a Powered Ankle Prosthesis. IEEE Trans. Neural Syst. Rehabil. Eng. 2018, 26, 788–797. [Google Scholar] [CrossRef]
- Kang, I.; Kunapuli, P.; Hsu, H.; Young, A.J. Electromyography (EMG) Signal Contributions in Speed and Slope Estimation Using Robotic Exoskeletons. In Proceedings of the 2019 IEEE 16th International Conference on Rehabilitation Robotics (ICORR), Toronto, ON, Canada, 24–28 June 2019; pp. 548–553. [Google Scholar]
- Ming, L.; Fan, Z.; Helen, H.H. An Adaptive Classification Strategy for Reliable Locomotion Mode Recognition. Sensors 2017, 17, 2020. [Google Scholar] [CrossRef] [Green Version]
- Huang, H.; Zhang, F.; Hargrove, L.J.; Dou, Z.; Rogers, D.R.; Englehart, K.B. Continuous locomotion-mode identification for prosthetic legs based on neuromuscular–mechanical fusion. IEEE Trans. Biomed. Eng. 2011, 58, 2867–2875. [Google Scholar] [CrossRef] [Green Version]
- Huang, H.; Kuiken, T.A.; Lipschutz, R.D. A strategy for identifying locomotion modes using surface electromyography. IEEE Trans. Biomed. Eng. 2008, 56, 65–73. [Google Scholar] [CrossRef] [Green Version]
- Chen, B.; Zheng, E.; Wang, Q. A locomotion intent prediction system based on multi-sensor fusion. Sensors 2014, 14, 12349–12369. [Google Scholar] [CrossRef] [Green Version]
- Martinez-Hernandez, U.; Mahmood, I.; Dehghani-Sanij, A.A. Simultaneous Bayesian recognition of locomotion and gait phases with wearable sensors. IEEE Sens. J. 2017, 18, 1282–1290. [Google Scholar] [CrossRef] [Green Version]
- Gui, K.; Liu, H.; Zhang, D. A Practical and Adaptive Method to Achieve EMG-Based Torque Estimation for a Robotic Exoskeleton. IEEE/ASME Trans. Mech. 2019, 24, 483–494. [Google Scholar] [CrossRef]
- Hong, Y.W.; King, Y.; Yeo, W.; Ting, C.; Chuah, Y.; Lee, J.; Chok, E.-T. Lower extremity exoskeleton: Review and challenges surrounding the technology and its role in rehabilitation of lower limbs. Aust. J. Basic Appl. Sci. 2013, 7, 520–524. [Google Scholar]
- Chen, B.J.; Wang, Q.N.; Wang, L. Adaptive Slope Walking with a Robotic Transtibial Prosthesis Based on Volitional EMG Control. IEEE-Asme Trans. Mech. 2015, 20, 2146–2157. [Google Scholar] [CrossRef]
- Winter, D.A.; Yack, H.J. EMG profiles during normal human walking: Stride-to-stride and inter-subject variability. Electroencephalogr. Clin. Neurophysiol. 1987, 67, 402–411. [Google Scholar] [CrossRef]
- Nazmi, N.; Rahman, M.A.A.; Yamamoto, S.I.; Ahmad, S.A. Walking gait event detection based on electromyography signals using artificial neural network. Biomed. Signal Process. Control 2019, 47, 334–343. [Google Scholar] [CrossRef]
- Day, S. Important Factors in Surface EMG Measurement; Bortec Biomedical Ltd Publishers: Calgary, AB, Canada, 2002; pp. 1–17. [Google Scholar]
- Hermens, H.J.; Freriks, B.; Merletti, R.; Stegeman, D.; Blok, J.; Rau, G.; Disselhorst-Klug, C.; Hägg, G. European recommendations for surface electromyography. Roessingh Res. Dev. 1999, 8, 13–54. [Google Scholar]
- Nazmi, N.; Rahman, M.A.A.; Ariff, M.H.M.; Ahmad, S.A. Generalization of ANN Model in Classifying Stance and Swing Phases of Gait using EMG Signals. In Proceedings of the 2018 Ieee-Embs Conference on Biomedical Engineering and Sciences, Sarawak, Malaysia, 3–6 December 2018; pp. 461–466. [Google Scholar]
- Murley, G.S.; Menz, H.B.; Landorf, K.B. Electromyographic patterns of tibialis posterior and related muscles when walking at different speeds. Gait Posture 2014, 39, 1080–1085. [Google Scholar] [CrossRef]
- Ma, L.; Yang, Y.; Chen, N.; Song, R.; Li, L. Effect of different terrains on onset timing, duration and amplitude of tibialis anterior activation. Biomed. Signal Process. Control 2015, 19, 115–121. [Google Scholar] [CrossRef]
- Komi, P.V.; Tesch, P. EMG frequency spectrum, muscle structure, and fatigue during dynamic contractions in man. Eur. J. Appl. Physiol. Occup. Physiol. 1979, 42, 41–50. [Google Scholar] [CrossRef]
- Larsson, B.; Månsson, B.; Karlberg, C.; Syvertsson, P.; Elert, J.; Gerdle, B. Reproducibility of surface EMG variables and peak torque during three sets of ten dynamic contractions. J. Electromyogr. Kinesiol. 1999, 9, 351–357. [Google Scholar] [CrossRef]
- Wang, J.; Tang, L.; Bronlund, J.E. Surface EMG signal amplification and filtering. Int. J. Comput. Appl. 2013, 82, 15–22. [Google Scholar] [CrossRef]
- Chowdhury, R.H.; Reaz, M.B.I.; Ali, M.A.B.; Bakar, A.A.A.; Chellappan, K.; Chang, T.G. Surface Electromyography Signal Processing and Classification Techniques. Sensors 2013, 13, 12431–12466. [Google Scholar] [CrossRef]
- Barzilay, O.; Wolf, A. A fast implementation for EMG signal linear envelope computation. J. Electromyogr. Kinesiol. 2011, 21, 678–682. [Google Scholar] [CrossRef] [PubMed]
- Dutta, A.; Khattar, B.; Banerjee, A. Nonlinear Analysis of Electromyogram Following Neuromuscular Electrical Stimulation-Assisted Gait Training in Stroke Survivors. In Converging Clinical and Engineering Research on Neurorehabilitation; Springer: Berlin, Germany, 2013; pp. 53–57. [Google Scholar]
- Barsakcioglu, D.Y.; Farina, D. A real-time surface emg decomposition system for non-invasive human-machine interfaces. In Proceedings of the 2018 IEEE Biomedical Circuits and Systems Conference (BioCAS), Cleveland, OH, USA, 17–19 October 2018; pp. 1–4. [Google Scholar]
- Burden, A. How should we normalize electromyograms obtained from healthy participants? What we have learned from over 25 years of research. J. Electromyogr. Kinesiol. 2010, 20, 1023–1035. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.F.; Winter, D. Electromyographic amplitude normalization methods: Improving their sensitivity as diagnostic tools in gait analysis. Arch. Phys. Med. Rehabil. 1984, 65, 517–521. [Google Scholar] [PubMed]
- Yang, J.F.; Winter, D.A. Electromyography reliability in maximal and submaximal isometric contractions. Arch. Phys. Med. Rehabil. 1983, 64, 417–420. [Google Scholar]
- David, A.W. The Biomechanics and Motor Control of Human Gait; University of Waterloo Press: Waterloo, ON, Canada, 1988. [Google Scholar]
- Tabard-Fougère, A.; Rose-Dulcina, K.; Pittet, V.; Dayer, R.; Vuillerme, N.; Armand, S. EMG normalization method based on grade 3 of manual muscle testing: Within-and between-day reliability of normalization tasks and application to gait analysis. Gait Posture 2018, 60, 6–12. [Google Scholar] [CrossRef]
- Colacino, F.M.; Emiliano, R.; Mace, B.R. Subject-specific musculoskeletal parameters of wrist flexors and extensors estimated by an EMG-driven musculoskeletal model. Med. Eng. Phys. 2012, 34, 531–540. [Google Scholar] [CrossRef] [Green Version]
- Buongiorno, D.; Barone, F.; Solazzi, M.; Bevilacqua, V.; Frisoli, A. A linear optimization procedure for an emg-driven neuromusculoskeletal model parameters adjusting: Validation through a myoelectric exoskeleton control. In Proceedings of the International Conference on Human Haptic Sensing and Touch Enabled Computer Applications, London, UK, 4–7 July 2016; pp. 218–227. [Google Scholar]
- Kim, S.; Nussbaum, M.A.; Esfahani, M.I.M.; Alemi, M.M.; Alabdulkarim, S.; Rashedi, E. Assessing the influence of a passive, upper extremity exoskeletal vest for tasks requiring arm elevation: Part I–“Expected” effects on discomfort, shoulder muscle activity, and work task performance. Appl. Ergon. 2018, 70, 315–322. [Google Scholar] [CrossRef]
- Wannop, J.W.; Worobets, J.T.; Stefanyshyn, D.J. Normalization of ground reaction forces, joint moments, and free moments in human locomotion. J. Appl. Biomech. 2012, 28, 665–676. [Google Scholar] [CrossRef]
- Tao, W.; Liu, T.; Zheng, R.; Feng, H. Gait Analysis Using Wearable Sensors. Sensors 2012, 12, 2255–2283. [Google Scholar] [CrossRef]
- Jung, J.Y.; Heo, W.; Yang, H.; Park, H. A Neural Network-Based Gait Phase Classification Method Using Sensors Equipped on Lower Limb Exoskeleton Robots. Sensors 2015, 15, 27738–27759. [Google Scholar] [CrossRef]
- Subasi, A. Classification of EMG signals using PSO optimized SVM for diagnosis of neuromuscular disorders. Comput. Boil. Med. 2013, 43, 576–586. [Google Scholar] [CrossRef] [PubMed]
- Tavakoli, M.; Benussi, C.; Lopes, P.A.; Osorio, L.B.; de Almeida, A.T. Robust hand gesture recognition with a double channel surface EMG wearable armband and SVM classifier. Biomed. Signal Process. Control 2018, 46, 121–130. [Google Scholar] [CrossRef]
- Ziegier, J.; Gattringer, H.; Mueller, A. Classification of gait phases based on bilateral emg data using support vector machines. In Proceedings of the 2018 7th IEEE International Conference on Biomedical Robotics and Biomechatronics (Biorob), Enschede, The Netherlands, 26–29 August 2018; pp. 978–983. [Google Scholar]
- Xi, X.; Tang, M.; Luo, Z. Feature-level fusion of surface electromyography for activity monitoring. Sensors 2018, 18, 614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savur, C.; Sahin, F. Real-time american sign language recognition system using surface emg signal. In Proceedings of the 2015 IEEE 14th International Conference on Machine Learning and Applications (ICMLA), Miami, FL, USA, 9–11 December 2015; pp. 497–502. [Google Scholar]
- Alkan, A.; Günay, M. Identification of EMG signals using discriminant analysis and SVM classifier. Expert Syst. Appl. 2012, 39, 44–47. [Google Scholar] [CrossRef]
- Kruskal, W.H.; Wallis, W.A. Use of ranks in one-criterion variance analysis. J. Am. Stat. Assoc. 1952, 47, 583–621. [Google Scholar] [CrossRef]
- Chan, Y.; Walmsley, R.P. Learning and understanding the Kruskal-Wallis one-way analysis-of-variance-by-ranks test for differences among three or more independent groups. Phys. Ther. 1997, 77, 1755–1761. [Google Scholar] [CrossRef]
- Figueiredo, J.; Moreno, J.C.; Santos, C.P. Assistive locomotion strategies for active lower limb devices. In Proceedings of the 2017 IEEE 5th Portuguese Meeting on Bioengineering (ENBENG), Coimbra, Portugal, 16–18 February 2017; pp. 1–4. [Google Scholar]
- Arsenault, A.; Winter, D.; Marteniuk, R. Is there a ‘normal’ profile of EMG activity in gait? Med. Biol. Eng. Comput. 1986, 24, 337–343. [Google Scholar] [CrossRef]
- Vernillo, G.; Giandolini, M.; Edwards, W.B.; Morin, J.-B.; Samozino, P.; Horvais, N.; Millet, G.Y. Biomechanics and physiology of uphill and downhill running. Sports Med. 2017, 47, 615–629. [Google Scholar] [CrossRef]
- Alexander, N.; Schwameder, H. Effect of sloped walking on lower limb muscle forces. Gait Posture 2016, 47, 62–67. [Google Scholar] [CrossRef]
- Lay, A.N.; Hass, C.J.; Nichols, T.R.; Gregor, R.J. The effects of sloped surfaces on locomotion: An electromyographic analysis. J. Biomech. 2007, 40, 1276–1285. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Height/cm | Weight/kg | Age |
|---|---|---|
| 175.70 ± 6.63 | 66.20 ± 9.19 | 20.80 ± 1.40 |
| Relevant Work | Ramp Angle |
|---|---|
| [22] | 4.78 degree |
| [27] | 10 degree |
| [31] | 10 degree |
| [19] | 12 degree |
| [35] | 8.5 degree |
| This work | 5.2 degree |
| Symbol | The Meaning of the Features |
|---|---|
| GRF-Based | |
| Hallux Max | The max value of hallux GRF |
| Heel Max | The max value of heel GRF |
| Max T | The time interval between the two peaks |
| Hallux ON | The duration of Hallux GRF above the threshold |
| Heel ON | The duration of Heel GRF above the threshold |
| Hallux OFF | The duration of Hallux GRF below the threshold |
| Heel OFF | The duration of Heel GRF below the threshold |
| Start T | The time interval between Hallux ON and Heel ON |
| End T | The time interval between Hallux OFF and Heel OFF |
| EMG-Based | |
| TA Peak | The peak value of the TA linear envelope |
| TA MAV | |
| TA STD | |
| TA RMS | |
| TA WL | WL of TA EMG; , where Δxi = xi − xi−1 |
| TA 80 | The value of the TA linear envelope at 80% gait |
| SL Peak | The peak value of the SL linear envelope |
| SL MAV | MAV of the SL EMG, |
| SL STD | STD of the SL EMG; |
| SL RMS | RMS of the SL EMG; |
| SL WL | WL of SL EMG; , where Δxi = xi − xi−1 |
| SL 25 | The value of the SL linear envelope at 25% gait |
| Actual Value | Positive | Negative | |
|---|---|---|---|
| Prediction | |||
| Positive | TP | FP | |
| Negative | FN | TN | |
| GRF | EMG | GRF + EMG | ||
| Accuracy ± SD | 80.96% ± 6.17% | 89.93% ± 3.63% | 96.76% ± 1.57% | |
| SEN ± SD | Uphill | 83.44% ± 5.47% | 95.00% ± 3.28% | 98.59% ± 1.15% |
| Level ground | 78.68% ± 7.36% | 88.49% ± 4.62% | 96.87% ± 1.62% | |
| Downhill | 80.99% ± 10.25% | 86.04% ± 6.97% | 94.59% ± 3.24% | |
| SPE ± SD | Uphill | 78.84% ± 7.34% | 86.31% ± 4.76% | 95.77% ± 1.79% |
| Level ground | 84.07% ± 5.44% | 92.46% ± 2.90% | 97.99% ± 0.99% | |
| Downhill | 80.35% ± 5.94% | 91.23% ± 3.73% | 96.64% ± 2.19% | |
| Prediction | Uphill | Level | Downhill | |
|---|---|---|---|---|
| Actual Terrains | ||||
| Uphill | 98.59% ± 1.15% | 1.41% ± 1.15% | 0% ± 0% | |
| Level | 0.86% ± 1.54% | 96.87% ± 1.62% | 2.27% ± 1.52% | |
| Downhill | 0.35% ± 0.73% | 5.06% ± 3.25% | 94.59% ± 3.24% | |
| [20] | [21] | [22] | [32] | This Work | |
|---|---|---|---|---|---|
| Input | Interaction force, 4 EMG 1, 4 GRF 2 Position sensor | 7 EMG 2 Accelerometers | 12 EMG | 9 EMG 6 GRF | 2 EMG 2 GRF |
| Methodology | BLDA | SVM and LDA | Muscle Synergies | SVM and LDA | SVM |
| Overall Accuracy | 96.1% | 67.1% (only EMG) 95.2% (only Accelerometers) | 83.8% | 97.7% | 96.8% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gao, S.; Wang, Y.; Fang, C.; Xu, L. A Smart Terrain Identification Technique Based on Electromyography, Ground Reaction Force, and Machine Learning for Lower Limb Rehabilitation. Appl. Sci. 2020, 10, 2638. https://doi.org/10.3390/app10082638
Gao S, Wang Y, Fang C, Xu L. A Smart Terrain Identification Technique Based on Electromyography, Ground Reaction Force, and Machine Learning for Lower Limb Rehabilitation. Applied Sciences. 2020; 10(8):2638. https://doi.org/10.3390/app10082638
Chicago/Turabian StyleGao, Shuo, Yixuan Wang, Chaoming Fang, and Lijun Xu. 2020. "A Smart Terrain Identification Technique Based on Electromyography, Ground Reaction Force, and Machine Learning for Lower Limb Rehabilitation" Applied Sciences 10, no. 8: 2638. https://doi.org/10.3390/app10082638