
Effect of Polyphenolic Complements on Cognitive Function in the Elderly: A Systematic Review

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Information Sources and Search Terms
2.3. Data Extraction
2.4. Quality Evaluation
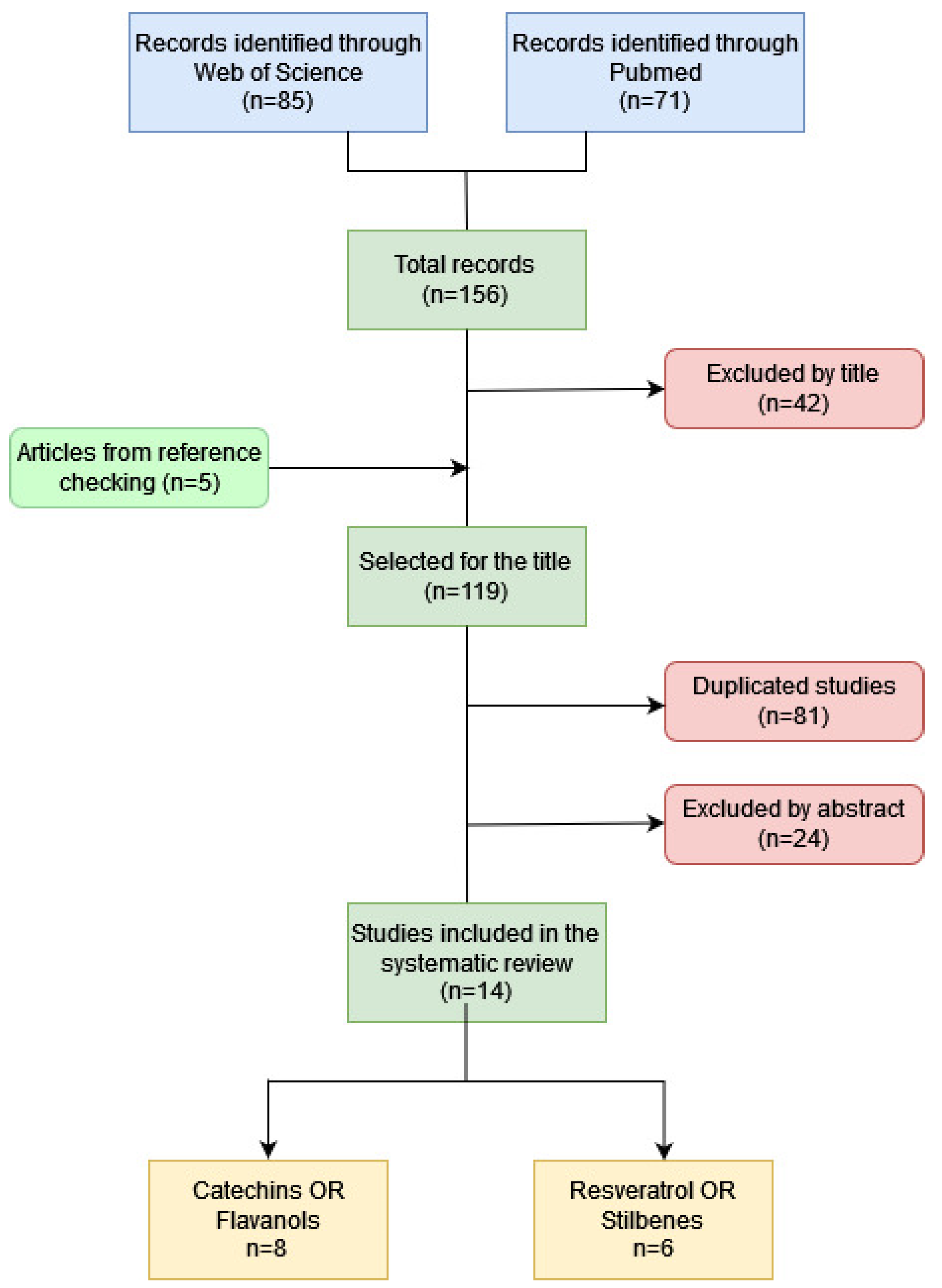
3. Results
3.1. Characteristics of Included Studies
3.2. Effects of the Intervention with Flavanols
3.3. Effects of Intervention with Stilbenes
4. Discussion
4.1. Main Findings
4.2. Strengths and Limitations
4.3. Comparison with Other Reviews
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Alzheimer’s Disease International. Informe Mundial Sobre el Alzheimer 2019: Actitudes Hacia la Demencia; Alzheimer’s Disease International: London, UK, 2019. [Google Scholar]
- Livingston, G.; Sommerlad, A.; Orgeta, V.; Costafreda, S.G.; Huntley, J.; Ames, D.; Ballard, C.; Banerjee, S.; Burns, A.; Cohen-Mansfield, J. Dementia prevention, intervention and care. Lancet 2007, 390, 2673–2734. [Google Scholar] [CrossRef] [Green Version]
- Gustafson, D.R.; Clare Morris, M.; Scarmeas, N.; Shah, R.C.; Sijben, J.; Yaffe, K.; Zhu, X. New perspectives on Alzheimer’s disease and nutrition. J. Alzheim. Dis. 2015, 46, 1111–1127. [Google Scholar] [CrossRef] [PubMed]
- Huhn, S.; Kharabian Masouleh, S.; Stumvoll, M.; Villringer, A.; Witte, A.V. Components of a Mediterranean diet and their impact on cognitive functions in aging. Front. Aging Neurosci. 2015, 7, 132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hill, E.; Goodwill, M.A.; Gorelik, A.; Szoeke, C. Diet and biomarkers of Alzheimer’s disease: A systematic review and meta-analysis. Neurobiol Aging 2018, 76, 45–52. [Google Scholar] [CrossRef]
- Del Rio, D.; Rodriguez-Mateos, A.; Spencer, J.P.; Tognolini, M.; Borges, G.; Crozier, A. Dietary (poly)phenolics in human health: Structures, bioavailability, and evidence of protective effects against chronic diseases. Antioxid. Redox Signal. 2013, 18, 1818–1892. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.; Shim, J.; Lee, C.Y.; Lee, K.W.; Lee, H.J. Cocoa phytochemicals: Recent advances in molecular mechanisms on health. Crit. Rev. Food Sci. Nutr. 2014, 54, 1458–1472. [Google Scholar] [CrossRef]
- Mastroiacovo, D.; Kwik-Uribe, C.; Grassi, D.; Necozione, S.; Raffaele, A.; Pistacchio, L.; Desideri, G. Cocoa flavanol consumption improves cognitive function, blood pressure control, and metabolic profile in elderly subjects: The Cocoa, Cognition, and Aging (CoCoA) Study—A randomized controlled trial. Am. J. Clin. Nutr. 2015, 101, 538–548. [Google Scholar] [CrossRef]
- Desideri, G.; Kwik-Uribe, C.; Grassi, D.; Necozione, S.; Ghiadoni, L.; Mastroiacovo, D.; Ferri, C. Benefits in cognitive function, blood pressure, and insulin resistance through cocoa flavanol consumption in elderly subjects with mild cognitive impairment: The Cocoa, Cognition, and Aging (CoCoA) study. Hypertension 2012, 60, 794–801. [Google Scholar] [CrossRef] [Green Version]
- Anton, S.D.; Ebner, N.; Dzierzewski, J.M.; Zlatar, Z.Z.; Gurka, M.J.; Dotson, V.M.; Manini, T.M. Effects of 90 days of resveratrol supplementation on cognitive function in elders: A pilot study. J. Altern. Complement. Med. 2018, 24, 725–732. [Google Scholar] [CrossRef]
- Evans, H.M.; Howe, P.R.; Wong, R.H. Effects of resveratrol on cognitive performance, mood and cerebrovascular function in post-menopausal women; a 14-week randomised placebo-controlled intervention trial. Nutrients 2017, 9, 27. [Google Scholar] [CrossRef] [Green Version]
- Ide, K.; Yamada, H.; Takuma, N.; Kawasaki, Y.; Harada, S.; Nakase, J.; Sagesaka, Y.M. Effects of green tea consumption on cognitive dysfunction in an elderly population: A randomized placebo-controlled study. Nutr. J. 2016, 15, 49. [Google Scholar] [CrossRef] [Green Version]
- Köbe, T.; Witte, A.V.; Schnelle, A.; Tesky, V.A.; Pantel, J.; Schuchardt, J.P.; Flöel, A. Impact of resveratrol on glucose control, hippocampal structure and connectivity, and memory performance in patients with mild cognitive impairment. Front. Neurosci. 2017, 11, 105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuriyama, S.; Hozaka, A.; Ohmori, K.; Shimazu, T.; Matsui, T.; Ebihara, S.; Awata, S.; Nagatomi, R.; Arai, H.; Tsuji, I. Green tea consumption and cognitive function: A cross-sectional study from the Tsurugaya Project. Am. J. Clin. Nutr. 2006, 83, 355–361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atmaca, N.; Atmaca, H.T.; Kanici, A.; Anteplioglu, T. Protective effect of resveratrol on sodium fluoride-induced oxidative stress, hepatotoxicity and neurotoxicity in rats. Food Chem Toxicol. 2014, 70, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Guo, R.; Li, W.; Liu, B.; Li, S.; Zhang, B.; Xu, Y. Resveratrol protects vascular smooth muscle cells against high glucose-induced oxidative stress and cell proliferation in vitro. Med. Sci. Monit. Basic Res. 2014, 20, 82–92. [Google Scholar] [PubMed] [Green Version]
- Kennedy, D.O. Polyphenols and the human Brain: Plant “secondary metabolite” ecologic roles and endogenous signaling functions drive benefits. Adv. Nutr. Int. Rev. J. 2014, 5, 515–533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sandhu, K.V.; Sherwin, E.; Schellekens, H.; Stanton, C.; Dinan, T.G.; Cryan, J.F. Feeding the microbiota-gut-brain axis: Diet, microbiome, and neuropsychiatry. Transl. Res. J. Lab. Clin. Med. 2017, 179, 223–244. [Google Scholar] [CrossRef] [PubMed]
- Spencer, J.P. Flavonoids and brain health: Multiple effects underpinned by common mechanisms. Genes Nutr. 2009, 4, 243–250. [Google Scholar] [CrossRef] [Green Version]
- Brickman, A.M.; Khan, U.A.; Provenzano, F.A.; Yeung, L.K.; Suzuki, W.; Schroeter, H.; Small, S.A. Enhancing dentate gyrus function with dietary flavanols improves cognition in older adults. Nat. Neurosci. 2014, 17, 1798–1803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krikorian, R.; Boespflug, E.L.; Fleck, D.E.; Stein, A.L.; Wightman, J.D.; Shidler, M.D.; Sadat-Hossieny, S. Concord grape juice supplementation and neurocognitive function in human aging. J. Agric. Food Chem. 2012, 60, 5736–5742. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Torosyan, N.; Silverman, D.H. Examining the impact of grape consumption on bran metabolism and cognitive function in patients with mild decline in cognition: A double-blinded placebo controlled pilot study. Exp. Gerontol. 2017, 87, 121–128. [Google Scholar] [CrossRef]
- Lamport, D.J.; Pal, D.; Moutsiana, C.; Field, D.T.; Williams, C.M.; Spencer, J.P.; Butler, L.T. The effect of flavanol-rich cocoa on cerebral perfusion in healthy older adults during conscious resting state: A placebo controlled, crossover, acute trial. J. Psychopharmacol. 2015, 232, 3227–3234. [Google Scholar] [CrossRef] [Green Version]
- Pase, M.P.; Scholey, A.B.; Pipingas, A.; Kras, M.; Nolidin, K.; Gibbs, A.; Stough, C. Cocoa polyphenols enhance positive mood states but not cognitive performance: A randomized, placebo-controlled trial. J. Psychopharmacol. 2013, 27, 451–458. [Google Scholar] [CrossRef]
- Witte, A.V.; Kerti, L.; Margulies, D.S.; Flöel, A. Effects of resveratrol on memory performance, hippocampal functional connectivity, and glucose metabolism in healthy older adults. J. Neurosci. 2014, 34, 7862–7870. [Google Scholar] [CrossRef] [Green Version]
- Moran, C.; Scotto di Palumbo, A.; Bramham, J.; Moran, A.; Rooney, B.; De Vito, G.; Egan, B. Effects of a six-month multi-ingredient nutrition supplement intervention of omega-3 polyunsaturated fatty acids, vitamin D, resveratrol, and whey protein on cognitive function in older adults: A randomised, double-blind, controlled trial. JPAD J. Prev. Alzheim. 2018, 5, 175–183. [Google Scholar] [CrossRef]
- Wong, R.H.X.; Nealon, R.S.; Scholey, A.; Howe, P.R.C. Low dose resveratrol improves cerebrovascular function in type 2 diabetes mellitus. Nutr. Metab. Cardiovasc. Dis. 2016, 26, 393–399. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Green, S. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. The Cochrane Collaboration. 2011. Available online: www.cochrane-handbook.org (accessed on 3 November 2021).
- Del Bo’, C.; Bernardi, S.; Marino, M.; Porrini, M.; Tucci, M.; Guglielmetti, S.; Cherubini, A.; Carrieri, B.; Kirkup, B.; Kroon, P.; et al. Systematic Review on Polyphenol Intake and Health Outcomes: Is There Sufficient Evidence to Define a Health-Promoting Polyphenol-Rich Dietary Pattern? Nutrients 2019, 11, 1355. [Google Scholar]
- Ammar, A.; Trabelsi, K.; Müller, P.; Bouaziz, B.; Boukhris, O.; Glenn, J.M.; Bott, N.; Driss, T.; Chtourou, H.; Müller, N.; et al. The Effect of (Poly)phenol-Rich Interventions on Cognitive Functions and Neuroprotective Measures in Healthy Aging Adults: A Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 9, 835. [Google Scholar] [CrossRef] [Green Version]
- Cheng, N.; Bell, L.; Lamport, D.J.; Williams, C.M. Dietary Flavonoids and Human Cognition: A Meta-Analysis. Mol. Nutr. Food Res. 2022, 25, e2100976. [Google Scholar] [CrossRef]
- Hernando, S.; Gartziandia, O.; Herran, E.; Pedraz, J.L.; Igartua, M.; Hernandez, R.M. Advances in nanomedicine for the treatment of Alzheimer’s and Parkinson’s diseases. Nanomedicine 2016, 11, 1267–1285. [Google Scholar] [CrossRef]
- Moore, K.; Hughes, C.F.; Ward, M.; Hoey, L.; McNulty, H. Diet, nutrition and the ageing brain: Current evidence and new directions. Proc. Nutr. Soc. 2018, 77, 152–163. [Google Scholar] [CrossRef]
- McGrattan, A.M.; McGuinness, B.; McKinley, M.C.; Kee, F.; Passmore, P.; Woodside, J.V.; McEvoy, C.T. Diet and Inflammation in Cognitive Ageing and Alzheimer’s Disease. Curr. Nutr. Rep. 2019, 8, 53–65. [Google Scholar] [CrossRef] [Green Version]
- Siervo, M.; Shannon, O.M.; Llewellyn, D.J.; Stephan, B.C.; Fontana, L. Mediterranean diet and cognitive function: From methodology to mechanisms of action. Free Radic. Biol. Med. 2021, 176, 105–117. [Google Scholar] [CrossRef]
- Meeusen, R. Exercise, nutrition and the brain. Sports Med. 2014, 44, S47–S56. [Google Scholar] [CrossRef] [Green Version]
- Lamport, D.J.; Williams, C.M. Polyphenols and Cognition In Humans: An Overview of Current Evidence from Recent Systematic Reviews and Meta-Analyses. Brain Plast. 2021, 6, 139–153. [Google Scholar] [CrossRef]


{kind=link}
| Database | Combination | Results | Selection by Title | Duplicates | Selection by Abstract |
|---|---|---|---|---|---|
| Web of Science | (Catechins OR Flavanols) AND (“cognitive impairment” OR “cognitive function” OR “cognitive task” OR “neurodegenerative disease” OR neuroinflammation OR “neurophysicological function”) | 11 | 11 | 0 | 5 |
| (Catechins OR Flavanols) AND (“cognitive impairment” OR “delayed memory” OR “cognitive performance”) | 16 | 16 | 10 | 1 | |
| PubMed | (Catechins OR Flavanols) AND (“cognitive impairment” OR “cognitive function” OR “cognitive task” OR neuroinflammation) | 11 | 10 | 10 | - |
| (Catechins OR Flavanols) AND “neurodegenerative disease” | 0 | 0 | 0 | 0 | |
| (Catechins OR Flavanols) AND “neurophysicological function” | 0 | 0 | 0 | 0 | |
| (Catechins OR Flavanols) AND (“cognitive impairment” OR “delayed memory” OR “cognitive performance”) | 9 | 9 | 9 | - | |
| Web of Science | (Flavonols OR Quercetin OR Quercetine) AND (“cognitive impairment” OR “cognitive function” OR “cognitive task” OR “neurodegenerative disease” OR neuroinflammation OR “neurophysicological function”) | 9 | 7 | 4 | 1 |
| (Flavonols OR Quercetin OR Quercetine) AND (“cognitive impairment” OR “delayed memory” OR “cognitive performance”) | 12 | 10 | 9 | 1 | |
| PubMed | (Flavonols OR Quercetin) AND (“cognitive impairment” OR “cognitive function” OR “cognitive task” OR neuroinflammation) | 5 | 5 | 5 | - |
| (Flavonols OR Quercetin) AND (“neurodegenerative disease” OR “neurophysicological function”) | 0 | 0 | 0 | 0 | |
| (Flavonols OR Quercetin OR Quercetine) AND (“cognitive impairment” OR “delayed memory” OR “cognitive performance”) | 6 | 6 | 6 | - | |
| Web of Science | (Resveratrol OR Stilbenes) AND (“cognitive impairment” OR “cognitive function” OR “cognitive task” OR “neurodegenerative disease” OR neuroinflammation OR “neurophysicological function”) | 18 | 10 | 2 | 4 |
| (Resveratrol OR Stilbenes) AND (“cognitive impairment” OR “delayed memory” OR “cognitive performance”) | 19 | 11 | 8 | 1 | |
| PubMed | (Resveratrol OR Stilbenes) AND (“cognitive impairment” OR “cognitive function” OR “cognitive task” OR neuroinflammation) | 24 | 10 | 9 | 0 |
| (Resveratrol OR Stilbenes) AND (“neurophysicological function”) | 0 | 0 | 0 | 0 | |
| (Resveratrol OR Stilbenes) AND (“neurodegenerative disease”) | 0 | 0 | 0 | 0 | |
| (Resveratrol OR Stilbenes) AND (“cognitive impairment” OR “delayed memory” OR “cognitive performance”) | 16 | 9 | 9 | - | |
| Additional bibliography obtained from the articles | 5 | 0 | 1 |
| Study | Number of Participants | Pathologies of the Participants | Selection Criteria | Follow-Up (Months) |
|---|---|---|---|---|
| Catechins/Flavanols | ||||
| Ide et al. (2016) [12] | 33 (27 at the end) I: 17 (14) C: 16 (13) | Yes -17 Alzheimer’s -15 Insanity -1 Lewy body dementia | -Over 50 years. -Do not consume antioxidant stress supplements (vit E, C, A, and B-carotene). -MMSE (Japanese version) < 28 -No allergy to tea. -Without severe cardiac, respiratory, hepatic, or renal dysfunction or anemia. | 12 |
| 29 women 4 men Mean age: 84.8 y | ||||
| Mastroiacovo et al. (2015) [8] | 90 (86 at the end) -High intake: 30 (29) -Average intake: 30 (29) -Low intake: 30 (28) | No | -No smoking. -Do not consume supplements (vit C and E) and/or medications with antioxidants (statins and glitazones), or drugs that interfere with consciousness (benzodiazepines and antidepressants), or chocolate or cocoa. -MMSE ≥ 27 and geriatric depression scale < 11. -BMI ≤ 30 and no weight change (±10%) in the last 6 months. -No medical conditions (no cardiovascular disease, cerebrovascular event, neurological or thyroid disorders, or inflammatory diseases). | 2 |
| 37 women 53 men Median age: 69.6 y | ||||
| Brickman et al. (2014) [20] | 37 -High intake + exercise: 8 -High intake + no exercise: 11 -Low intake + exercise: 9 -Low intake + no exercise: 9 | No | -Do not consume dietary or herbal supplements. -No treatment with psychotropic drugs or current psychiatric disorder. -No diabetes Dx. -People who do not exercise regularly or do not exceed the American Heart Association standards for average physical fitness. -No contraindication to aerobic exercise. -Not lactose intolerant. | 3 |
| 28 women 9 men Median age: 57.8 y | ||||
| Desideri et al. (2012) [9] | 90 -High intake: 30 -Intermediate: 30 -Low: 30 | Yes -Mild Cognitive Impairment | -Dx mild cognitive impairment according to Petersen criteria. -Do not smoke or take statins. -No Dx obesity (BMI > 30). | 2 |
| No differentiated data for women and men | ||||
| Krikorian et al. (2012) [21] | 21 I: 10 C:11 | Yes -Mild Cognitive Impairment | -Dx mild cognitive impairment. -No Dx or suspected dementia, diabetes, kidney disease, liver disease, serious psychiatric conditions, and substance abuse. | 4 |
| 10 women 11 men Average age men: 76.9 y Median age women: 76 y | ||||
| Lee et al. (2017) [22] | 10 I: 5 C:5 | Yes -Mild Cognitive Impairment | -Cognitive deficit and/or personality change present for at least 6 months but without a diagnosis of Alzheimer’s or other cause of dementia. Not have cognitive dysfunction that decreases the ability to perform daily activities. -No history of thyroid disease. -No auditory or motor deficit that prevents performing the tests. -No treatment for Alzheimer’s or dementia-related medications. -CT/MRI if stroke, tumor, hemorrhage, ictal activity, or hydrocephalus is suspected. | 6 |
| 5 women 5 men Average age 72.2 y | ||||
| Lamport et al. (2015) [23] | 18 High intake: 9/9 Low intake: 9/9 | No | -No chronic drug use. No high alcohol consumption (15 units/week) or illegal substances. -No neurological symptoms, MMSE ≥ 26. -No current or recent disease (obesity, diabetes, cardiovascular disease, hypertension, stroke, gallbladder or gastrointestinal problems). -No language or hearing impairments. -No allergy or sensitivity to chocolate, dairy, nuts, or gluten. | 1 day Crossover study Washout: 1 week |
| 10 women 8 men Average age: 61 y | ||||
| Pase et al. (2013) [24] | 71 -High intake: 24 -Average intake: 25 -Placebo: 22 | No | -No smoking. -Do not consume vitamin supplements, herbal extracts or illicit drugs. -Not being pregnant or breastfeeding. -No heart disease, hypertension, anxiety, depression, psychiatric disorders or epilepsy, or any other health disorder that affects food metabolism, such as kidney, liver, or gastrointestinal disease. | 1 |
| 47 women 24 men | ||||
| Resveratrol/Stilbenes | ||||
| Witte et al. (2014) [25] | 46 I: 23 -C:23 | Yes -Overweight | -Not in treatment with antidepressants. -Do not consume a daily consumption of 50 g of alcohol, nor 10 cigarettes, nor 6 cups of coffee per day or more. -MMSE ≥ 26 points. -No serious medical, neurological, and psychiatric illnesses without treatment. -No Dx diabetes mellitus type 2. -Speak native German. | 6 +1/2 |
| 18 women 28 men Mean age group I: 64.8 y Mean age group C: 63.7 y | ||||
| Anton et al. (2018) [10] | 32 -I (1000 mg): 10 -I (300 mg): 12 -C: 10 | Yes -Overweight or obesity | -No smoking. -Do not consume anabolic drugs or anticholinesterase inhibitors or anticoagulants (the use of aspirin is allowed) or statins. Not on antidepressant treatment. -Not on active treatment for cancer, stroke (<6 months), peripheral vascular disease, coronary artery disease (myocardial infarction < 6 months), stage III or IV congestive heart failure, valvular heart disease, severe anemia, liver or kidney disease, diabetes, severe arthritis, limb fracture ≤ 6 months, or limb amputation. -Do not consume excessive alcohol (>2 drinks/day) or >1 glass of red wine or purple grape juice/week. -Not consuming or having consumed a dietary supplement containing resveratrol, quercetin, grape seed extract, ginko biloba, or P. cuspidatum in the previous 90 days. -No Dx dementia disease, severe psychiatric illness, or Parkinson’s disease. -No deterioration in vision and hearing. -Sedentary (less than 120 min of physical activity of moderate intensity per week). -Self-reported ability to walk one mile. -CES-D ≤ 20. -MMSE > 24 points. -BMI: 25–34.9 kg/m2. -Not a BP > 180/100 mmHg or a resting heart rate > 120 beats per minute. -Not having participated in another clinical trial or intake of an investigational product ≤ 30 days before the exam. -No contraindications for MRI. | 3 |
| Average age: 73.34 y | ||||
| Moran et al. (2018) [26] | 51 (37 at the end) I: 26 (20) C:23 (17) | No | -65 years or older. -Normal cognitive function (MMSE > 24). -Defined as “healthy” (free from disease). -Independent, mobile, and able to complete the test. | 6 |
| 19 women 18 men Average age: 75.14 y | ||||
| Wong et al. (2016) [27] | 36 I (300 mg): 36/36 I (150 mg): 36/36 I (75 mg): 36/36 C: 36/36 | Yes -Diabetes mellitus type 2 | -Do not smoke or use nicotine therapy. -Not being on insulin or warfarin treatment. -No change in pre-existing medication or supplements during the intervention. -Not a modified MMSE (Australian version) <78/100. -No BP > 160/100 mmHg, no BMI > 40 mg/m2. -With the ability to obtain satisfactory images of the MCA bilaterally by TCD. -No serious head injuries. -No Dx of dementia, severe depression, stroke or neurological conditions; nor kidney or liver disease. | 1 dayCross study. Wash: 1 week |
| 10 postmenopausal women 26 men Average age: 68.47 y | ||||
| Evans et al. (2017) [11] | 80 (72 at the end) postmenopausal women I: 37 Q:35 | No | -No smoking. -Not on insulin, warfarin, or hormone replacement therapy in the last six months. -No suspicion of dementia, modified MMSE (Australian version) ≥78 points. -No history of breast or cervical cancer. -No Dx of cardiovascular, renal, hepatic disease, depression or disorders. | 3 + 1/2 |
| Median age: 61.5 y | ||||
| Kobe et al. (2017) [13] | 40 I: 18 c:22 | Yes -Mild Cognitive Impairment (diagnosed according to May criteria 12 months before) | -No MMSE < 24 at initial visit. -No BMI < 18 kg/m2 or >35 kg/m2. -Be right-handed. -Speak German fluently. -No serious untreated medical, neurological, or psychiatric illnesses and brain pathologies identified on MRI. | 6 + 1/2 |
| 21 women 19 men Mean age group I: 65 y Average age group C: 69 y | ||||
| Study | Intervention | Cognitive Variable Measurement Tool and Measurement Frequency (Months) | Results |
|---|---|---|---|
| Catechins/Flavanols | |||
| Ide et al. (2016) [12] | -I: 2 g/day green tea (220.2 mg catechins) -C: placebo | -MMSE (Japanese version) -NPQ-I -Laboratory tests (MDA-LDL, TC, LDL, HDL, TG, FPG, HbA1c) | -The levels of MDA-LDL, a marker of oxidative stress, were significantly lower in the green tea group. -No significant changes in the rest of the analytical parameters. -No significant changes in MMSE-J or NPI-Q scores. |
| (0–3-6–9–12 months) | |||
| Mastroiacovo et al. (2015) [8] | -I: HF drink (993 mg/day flavanol) -I: IF drink (520 mg/day flavanol) -I: LF drink (48 mg/day flavanol) | -MMSE -TMT A and B -VFT -BP -Laboratory tests (glucose, insulin, TC, LDL, HDL, TG, HOMA-IR index, 8-Iso-PGF) | -Lower response time after the HF and IF drinks in the TMT tests. -Improvement in all treatments in the VFT test, but greater improvement after the HF drink. -Lower SBP and improvement in insulin resistance and fluid peroxidation after drinking HF and IF. -No change in MMSE score or DBP. |
| (0–2 months) | |||
| Brickman et al. (2014) [20] | -I: High intake (900 mg cocoa flavanols and 138 mg epicatechin daily) + aerobic exercise (1 h/day 4 days/week) -I: High intake + no aerobic exercise -I: Low intake (10 mg cocoa flavanols and 12 mg epicatechin daily) + aerobic exercise (1 h/day 4 days/week) -I: Low intake (10 mg cocoa flavanols and 12 mg epicatechin daily) + no aerobic exercise | -ModBent test -fMRI | -An intervention with high flavanol content has a significant effect on ModBent performance (independent of exercise). Improvement of 630 ms with respect to those of the intervention with low content. -Changes in the ModBent and changes in the CBV images of the dentate gyrus are correlated. -Exercise has no significant effect on ModBent. |
| (0–3 months) | |||
| Desideri et al. (2012) [9] | -I: High intake (990 mg/day flavanols) -I: Intermediate intake (520 mg/day flavanols) -I: Low intake (45 mg/day flavanols) | -MMSE -TMT A and B -VFT -BP -Laboratory tests (glucose, insulin, TC, LDL, HDL, TG, HOMA-IR index, 8-Iso-PGF) | -Lower response time after high intake drinks (−14.3 s and −29.2 s) and intermediate (−8 s and −22.8 s) in the TMT A and B tests, respectively. -Greater improvement in VFT in subjects with high drink intake (+8 words in 60 s) and medium (+5.1 words), and, to a lesser extent, in low intake (+1.2 words). -Lower insulin resistance in high (−1.6 mU/L) and medium (−0.9 mU/L) intake. -Lower glucose levels in high (−0.6 mmol/L) and medium (−0.5 mmol/L) intake. -BP: High intake (SBP −10 mmHg and DBP −4.8 mmHg), medium (SBP −8.2 mmHg and DBP −3.4 mmHg) and, to a lesser extent, low intake (SBP −1.4 mmHg and DBP −0.9 mmHg). -Total plasma levels of 8-iso-PGF2 decrease in high (−99.8 pg/L) and intermediate (−65.8 pg/L) intake. -No change in MMSE score. -No changes in insulin, total cholesterol, LDL, HDL, and triglycerides. |
| (0–2 months) | |||
| Krikorian et al. (2012) [21] | -I: Grape juice (425 mgl/L anthocyanins and 888 mg/L procyanidins) -C: Placebo * Daily dose by weight (6.3–7.8 mL/kg) | -GDS -RAVLT -CVLT -BP -Laboratory tests (glucose, insulin) -Anthropometric parameters (weight, height) -fMRI | -CVLT without changes, but with a tendency to better performance in the placebo group (13.8 vs. 12.4) but fewer errors (7.16 vs. 5.03) and better ability to distinguish the elements learned in the intervention group. -Greater activation in the regions of the hemisphere (fMRI images) of the patients in the group consuming grape juice, in turn being associated with a vascular benefit. -No changes in analytical or anthropometric parameters. -No changes in the GDS. |
| (0–4 months) | |||
| Lee et al. (2017) [22] | -I: freeze-dried grape powder made from fresh California grapes -C: placebo * 72 g/day, equivalent to 3 standard servings of fresh grapes per day. | -ADAS-Cog -MMSE -HVLT -Benton visual retention test -ROFT Test -Boston Appointments Test -Fluency of FAC letters -Fluency of categories (naming animals) -Stroop test -TMT A and B -WCST -Symbol and digit speed (WAIS-III tasks) -MFQ -HDRS -fMRI | -Improvements in attention/working memory according to the WAIS-III tasks in the intervention group. -Decline in the posterior cingulate and superior posterolateral temporal cortical regions in the placebo group while the intervention group did not observe said decline. -No significant changes in the rest of the tests. |
| (0–6 months) | |||
| Lamport et al. (2015) [23] | -High intake: 494 mg/day flavanols -Low intake: 23 mg/day flavanols | -CBF -fMRI | -Better regional cerebral perfusion in the group that consumed the drink with high flavanol intake (in the anterior cingulate cortex and in the parietal lobe regions). |
| (0–2 h) | |||
| Pase et al. (2013) [24] | -I: High intake (500 mg/day cocoa flavanols) -I: Average intake (250 mg/day cocoa flavanols) -C: Placebo | -CDR -Bond-Lader Visual Analogue Scale | -Greater calm and self-rated satisfaction after receiving 30 days of treatment with high dose of flavanols. -Mood did not change with acute treatment. -Cognitive performance did not vary at any of the measurement times. |
| (0–1 h-2.5 h-4 h-30 days) | |||
| Resveratrol/Stilbenes | |||
| Witte et al. (2014) [25] | -I: 200 mg resveratrol and 320 mg quercetin daily -C: Placebo | -AVLT -PANAS -Freiburger Physical Activity Questionnaire -BP -Laboratory tests (glucose, insulin, TC, LDL, HDL, TG, HbA1c, leptin, BDNF, IGF-1, TNF-, interleukin 6, hs-CRP) -Anthropometric parameters (biomedical impedance, weight, height) -Vascular markers (CMIT)-fMRI | -Better delayed recall and recognition in the subjects of the intervention group. Learning ability significantly improved in both groups, but with a greater difference in the group that ingested resveratrol and quercetin. After the intervention, retention in the subjects was lower. * retention: number of correct words recalled after the fifth trial (maximum 15 words) subtracted from those recalled correctly after the 30 min delay (maximum 15 words). * delayed recall: number of words correctly recalled after the 30 min delay (maximum 15 words). * recognition: number of words correctly recognized minus false positives from a subsequent list of 45 words read aloud that included 15 correct words and 30 new ones (maximum 15). * learning capacity: sum of words correctly recalled during the five immediate learning trials (maximum score: 75 words). -Increased functional connectivity of the hippocampus in the frontal, parietal, and occipital areas. -Decrease in HB1ac (−0.13%) and DBP (−5.2 mmHg), and increase in leptin (+7.5 ng/mL). -No change in physical activity and mood. |
| (0–6+1/2 months) | |||
| Anton et al.(2018) [10] | -I: 1000 mg/day of resveratrol -I: 300 mg/day of resveratrol -C: placebo | -COWA. -Word Digits Forward and Backward and Digit Symbol Substitution Test (WAIS-IV tasks) -Eriksen flanking task- HVLT-R. -Change of tasks -TMT A and B | -Better psychomotor speed in the TMT A test in the intervention group with 1000 mg/day of resveratrol compared with 300 mg/day of resveratrol (−10.59 s) and placebo (−8.79 s). -No significant changes in performance on tests of visual attention, working memory, verbal fluency, and semantic memory between treatment groups. |
| (0–3 months) | |||
| Moran et al. (2018) [26] | -I: multi-ingredient supplement (omega-3 polyunsaturated fatty acids, vitamin D, 150 mg resveratrol and whey protein) -C: placebo | -TMT A and B -RAVLT -TUG -CFQ -Stroop test (CW version) -COWA -Digits of words forwards and backwards (WAIS-III task) | -In the intervention group there was a shorter response time in the Stroop Test both at 3 and 6 months, compared with the placebo group. -No significant changes in the rest of the tests. |
| (0–3-6 months) | |||
| Wong et al.(2016) [27] | -I: 300 mg/day of resveratrol -I: 150 mg/day of resveratrol -I: 75 mg/day of resveratrol -C: placebo | -CVR | -Resveratrol consumption increased CVR in MCA with all 3 doses of resveratrol: mean change from placebo was 13.8 ± 3.5% at intake of 75 mg resveratrol, 8.9 ± 3.5% in the 150 mg resveratrol dose, and 13.7 ± 3.3% in the 300 mg resveratrol dose. -The 75 mg dose was the only effective one in PCA, 13.2 ± 4.5% compared to placebo. |
| (0–45/60 min–90/120 min after treatment). Four separate visits of 7 days were made | |||
| Evans et al. (2017) [11] | -I: 150 mg/day of trans-resveratrol (2 capsules of 75 mg) C: placebo | -TMT A and B -RAVLT -Cambridge Semantic Memory Battery -BP and heart rate -TCD -CVR -Double Scope Task -POMS-V2 -CES-D | -Significant improvements in the immediate RAVLT (+4.5 words), in categorical fluency (+3.2 words), and in the camel and cactus test (+2.8 correct answers). These improvements correlate with a 17% CVR increase. -Mood tended to improve in the intervention group but not significantly. |
| (0–3 + 1/2 months) | |||
| Kobe et al. (2017) [13] | -I: 200 mg of resveratrol and 350 mg of quercetin daily -C: Placebo 1015 mg/day of olive oil | -RAVLT -PANAS -BDI -STAI X1 -Freiburger physical activity questionnaire -Analytical parameters (glucose, insulin, LDL, HDL, HbA1c and hs-CRP) -Anthropometric parameters (BMI and weight) -fMRI | -No significant differences in memory performance between the intervention group and the placebo group. -HbA1c was significantly reduced (−0.15%) after resveratrol intervention. -Hippocampal volume is preserved, and functional connectivity at rest of the hippocampus improves in the intervention group. |
| 0–6 + 1/2 months | |||
| Generation of Random Sequences (Selection Bias) | Allocation Concealment (Selection Bias) | Participant and Staff Blinding (Performance Bias) | Blinding of the Outcome Assessment (Detection Bias) | Incomplete Outcome Data (Attrition Bias) | Selective Reporting (Reporting Bias) | |
|---|---|---|---|---|---|---|
| Ide et al. (2016) | + | ? | ? | ? | + | + |
| Mastroiacovo et al. (2015) | ? | ? | + | ? | + | + |
| Brickman et al. (2014) | ? | ? | − | ? | + | + |
| Desideri et al. (2012) | ? | + | + | + | + | + |
| Krikorian et al. (2012) | ? | ? | + | ? | ? | ? |
| Lamport et al. (2015) | + | + | + | + | ? | ? |
| Witte et al. (2014) | ? | ? | + | ? | + | ? |
| Pase et al. (2013) | + | + | + | + | ? | ? |
| Anton et al. (2018) | + | ? | ? | ? | ? | ? |
| Moran et al. (2018) | + | ? | + | + | + | + |
| Lee et al. (2017) | ? | ? | + | + | + | ? |
| Wong et al. (2016) | ? | + | + | + | + | + |
| Evans et al. (2017) | − | + | + | + | + | + |
| Kobe et al. (2017) | + | + | ? | ? | + | ? |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodrigo-Gonzalo, M.J.; González-Manzano, S.; Mendez-Sánchez, R.; Santos-Buelga, C.; Recio-Rodríguez, J.I. Effect of Polyphenolic Complements on Cognitive Function in the Elderly: A Systematic Review. Antioxidants 2022, 11, 1549. https://doi.org/10.3390/antiox11081549
Rodrigo-Gonzalo MJ, González-Manzano S, Mendez-Sánchez R, Santos-Buelga C, Recio-Rodríguez JI. Effect of Polyphenolic Complements on Cognitive Function in the Elderly: A Systematic Review. Antioxidants. 2022; 11(8):1549. https://doi.org/10.3390/antiox11081549
Chicago/Turabian StyleRodrigo-Gonzalo, María José, Susana González-Manzano, Roberto Mendez-Sánchez, Celestino Santos-Buelga, and Jose Ignacio Recio-Rodríguez. 2022. "Effect of Polyphenolic Complements on Cognitive Function in the Elderly: A Systematic Review" Antioxidants 11, no. 8: 1549. https://doi.org/10.3390/antiox11081549