
Elevated Nitrite/Nitrate Ratio as a Potential Biomarker for the Differential Diagnosis of Pleural Effusions


Abstract
:1. Introduction
2. Materials and Methods
2.1. Chemicals
2.2. Pleural Effusions Collection
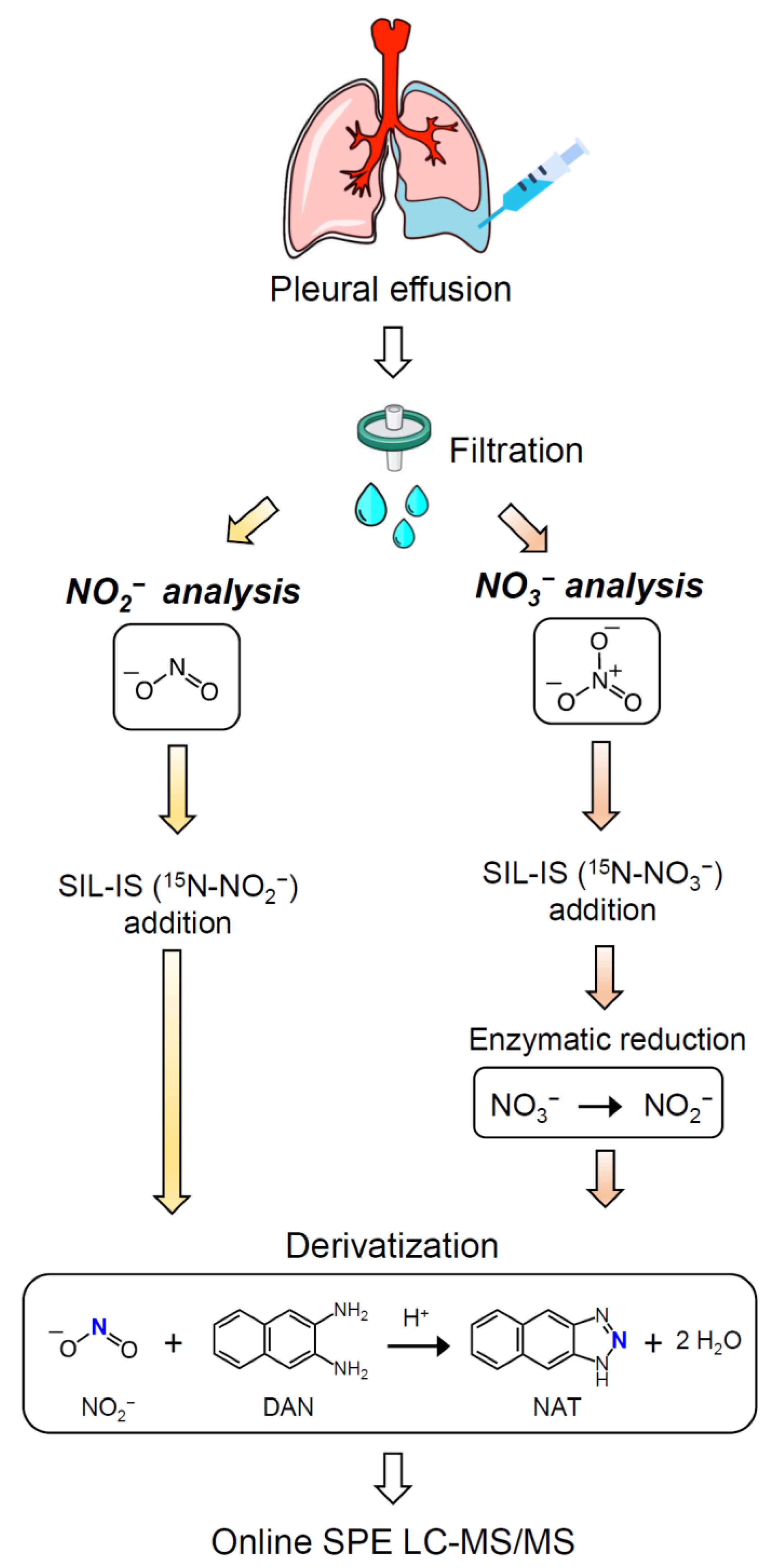
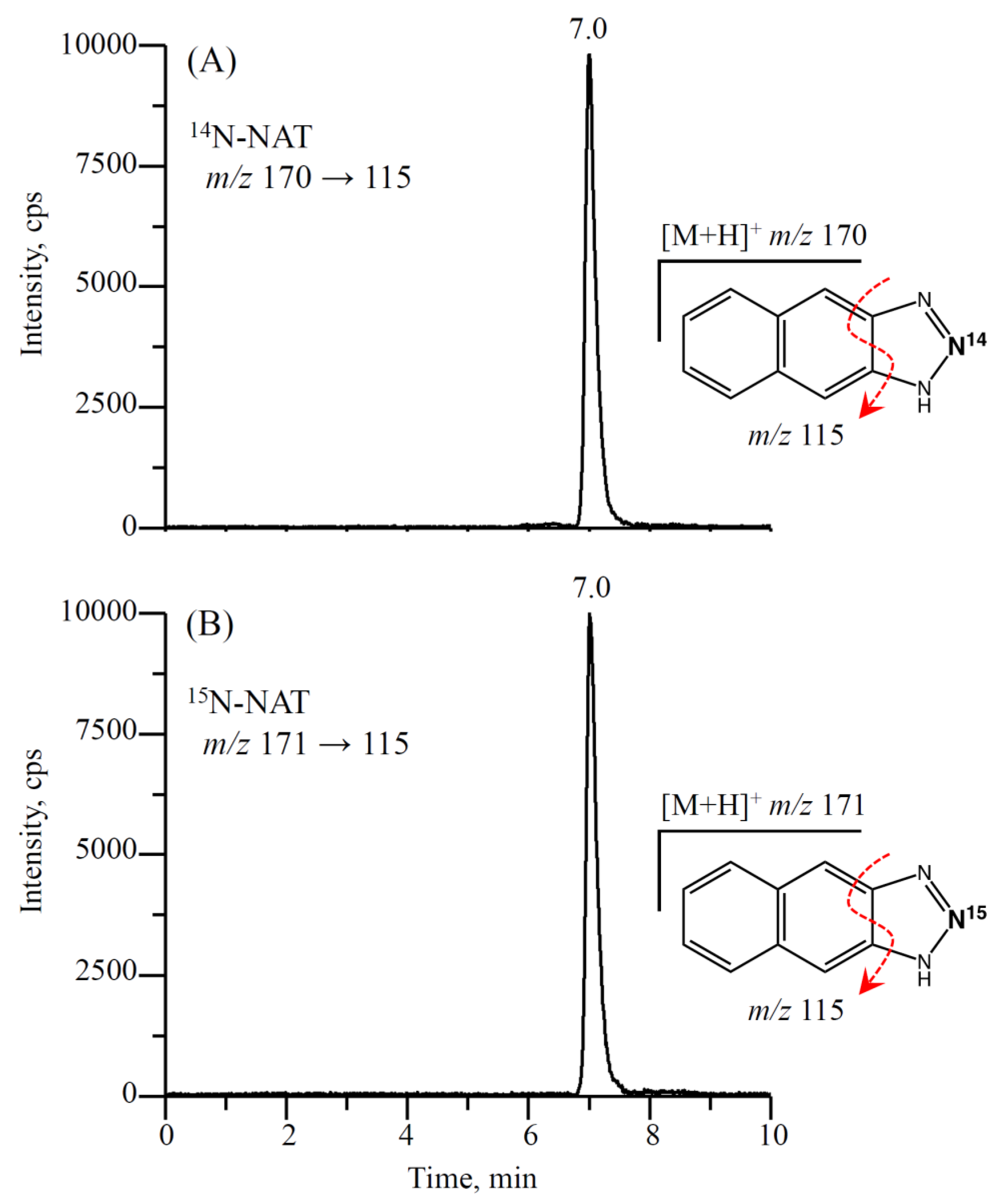
2.3. Analysis of Nitrite/Nitrate in Pleural Effusions Using Isotope-Dilution LC-MS/MS
2.4. Statistical Methods
3. Results
3.1. Etiology of PEs and General Characteristics of Patients
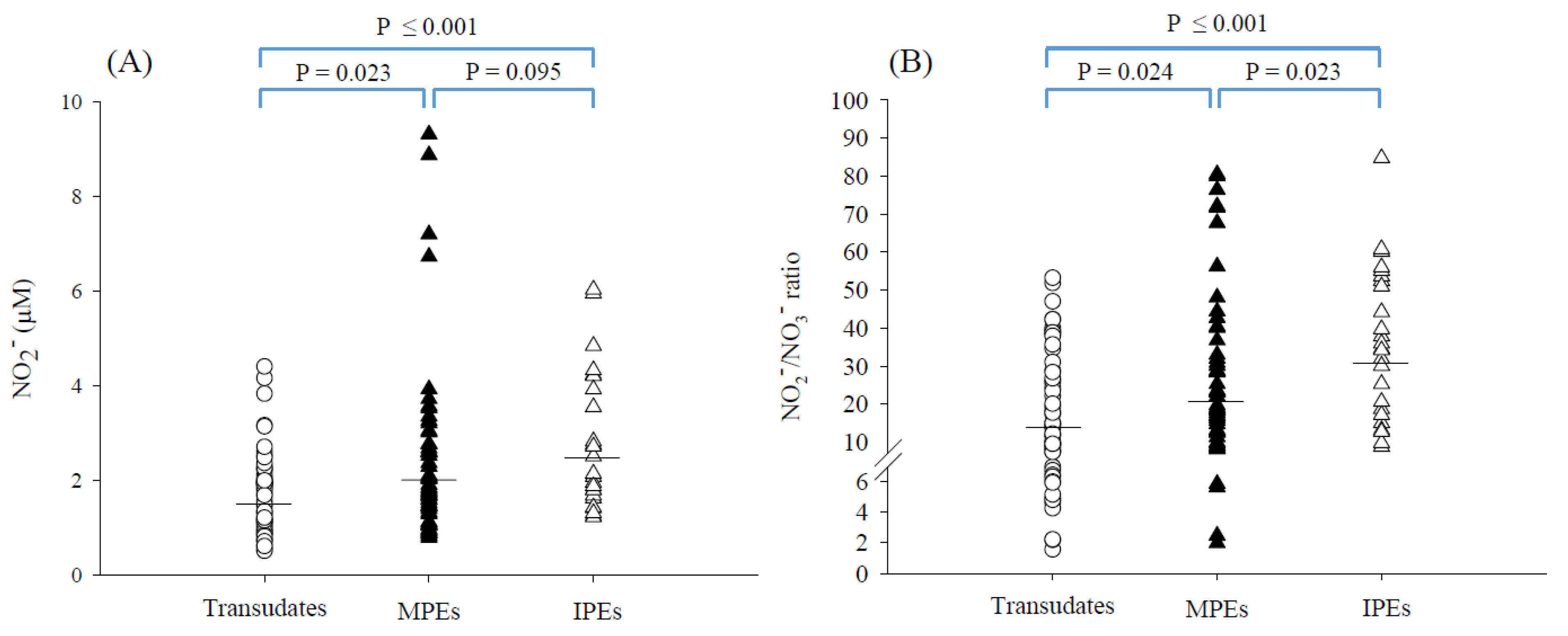
3.2. Nitrite and Nitrate Concentrations in PEs
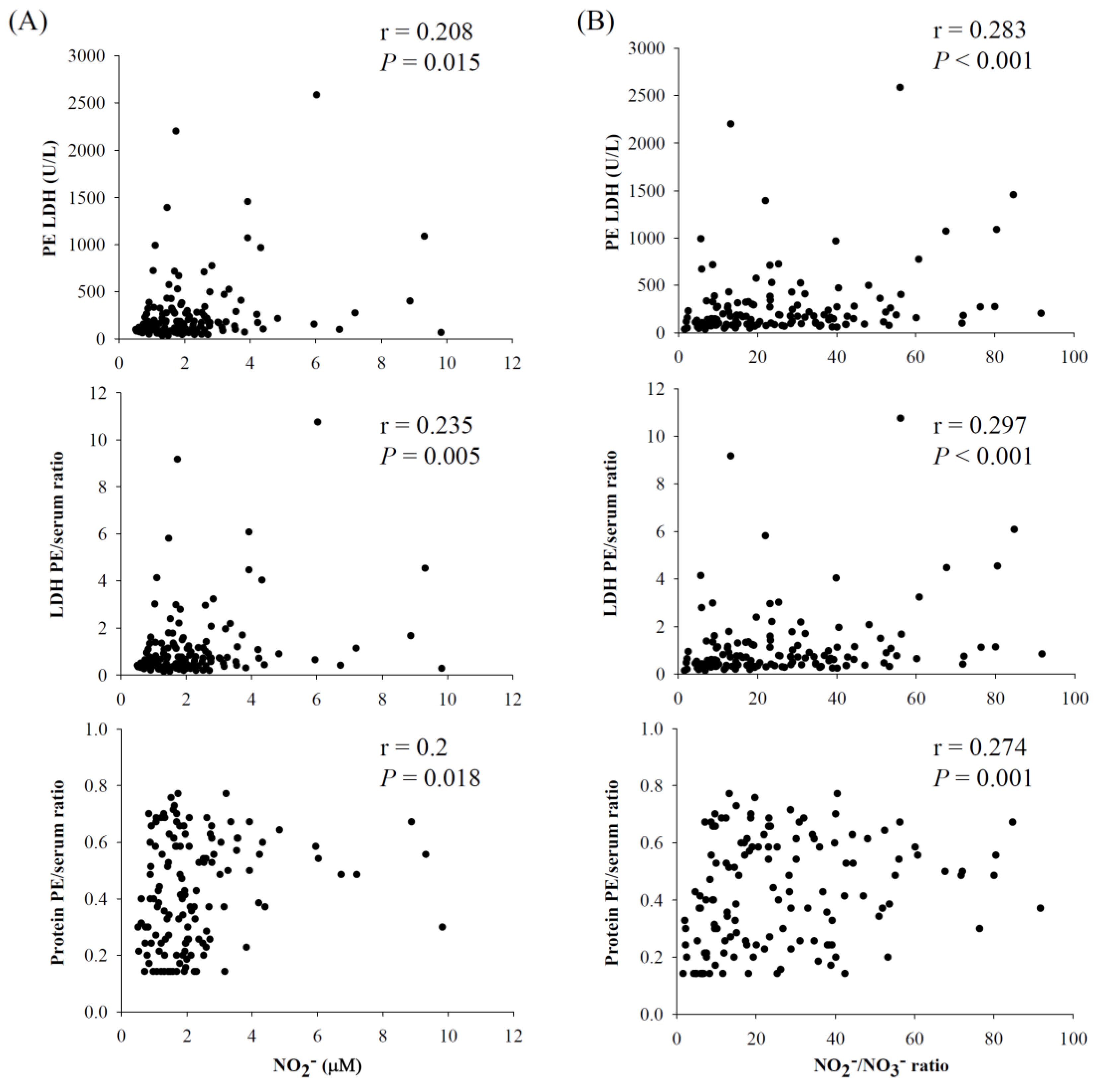
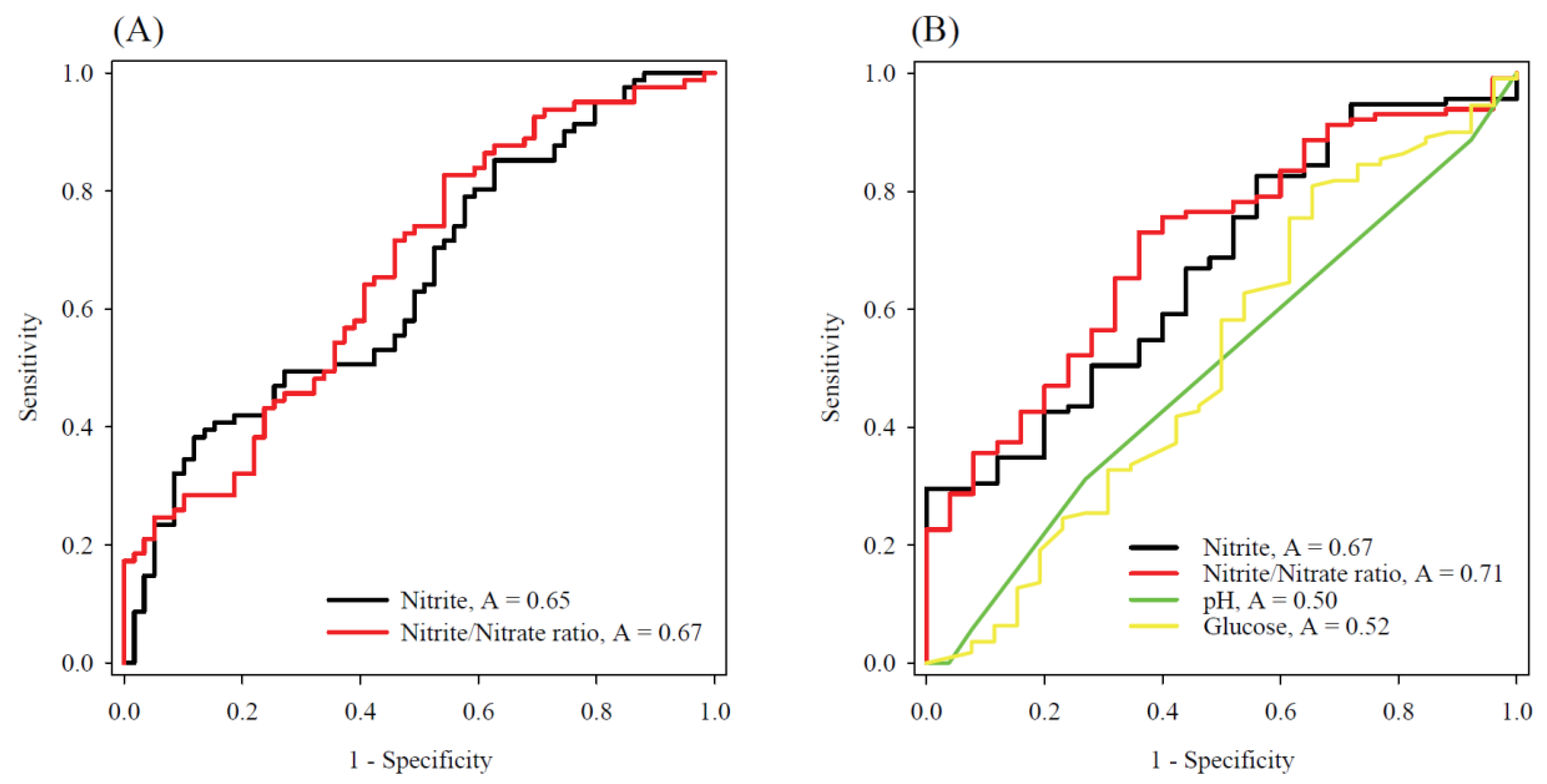
3.3. The Diagnostic Potential of Nitrite and Nitrate Concentrations in the Differentiation of PEs
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Porcel, J.M.; Light, R.W. Pleural Fluid Analysis: Are Light’s criteria still relevant after half a century? Clin. Chest Med. 2021, 42, 599–609. [Google Scholar] [CrossRef] [PubMed]
- Light, R.W. The light criteria: The beginning and why they are useful 40 years later. Clin. Chest Med. 2013, 34, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Porcel, J.M. Pleural fluid biomarkers: Beyond the Light criteria. Clin. Chest Med. 2013, 34, 27–37. [Google Scholar] [CrossRef]
- Maranhao, B.H.F.; da Silva Junior, C.T.; Barillo, J.L.; de Castro, C.L.T.; de Souza, J.B.S.; Silva, P.S.; Stirbulov, R. Diagnostic accuracy with total adenosine deaminase as a biomarker for discriminating pleural transudates and exudates in a population-based cohort study. Dis. Markers 2021, 2021, 6648535. [Google Scholar] [CrossRef]
- Lepine, P.A.; Thomas, R.; Nguyen, S.; Lacasse, Y.; Cheah, H.M.; Creaney, J.; Muruganandan, S.; Martel, S.; Lee, Y.C.G.; Delage, A. Simplified criteria using pleural fluid cholesterol and lactate dehydrogenase to distinguish between exudative and transudative pleural effusions. Respiration 2019, 98, 48–54. [Google Scholar] [CrossRef]
- Porcel, J.M.; Bielsa, S.; Esquerda, A.; Ruiz-Gonzalez, A.; Falguera, M. Pleural fluid C-reactive protein contributes to the diagnosis and assessment of severity of parapneumonic effusions. Eur. J. Intern. Med. 2012, 23, 447–450. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, N.; Ishii, T.; Kita, N.; Kanaji, N.; Nakamura, H.; Nanki, N.; Ueda, Y.; Tojo, Y.; Kadowaki, N.; Bandoh, S. The usefulness of pleural fluid presepsin, C-reactive protein, and procalcitonin in distinguishing different causes of pleural effusions. BMC Pulm. Med. 2018, 18, 176. [Google Scholar] [CrossRef]
- Maskell, N.A.; Batt, S.; Hedley, E.L.; Davies, C.W.; Gillespie, S.H.; Davies, R.J. The bacteriology of pleural infection by genetic and standard methods and its mortality significance. Am. J. Respir. Crit. Care Med. 2006, 174, 817–823. [Google Scholar] [CrossRef] [Green Version]
- Izhakian, S.; Wasser, W.G.; Fox, B.D.; Vainshelboim, B.; Kramer, M.R. The diagnostic value of the pleural fluid C-reactive protein in parapneumonic effusions. Dis. Markers 2016, 2016, 7539780. [Google Scholar] [CrossRef] [Green Version]
- Porcel, J.M.; Light, R.W. Diagnostic approach to pleural effusion in adults. Am. Fam. Physician 2006, 73, 1211–1220. [Google Scholar]
- Korhonen, R.; Lahti, A.; Kankaanranta, H.; Moilanen, E. Nitric oxide production and signaling in inflammation. Curr. Drug Targets Inflamm. Allergy 2005, 4, 471–479. [Google Scholar] [CrossRef] [PubMed]
- Tsikas, D. Methods of quantitative analysis of the nitric oxide metabolites nitrite and nitrate in human biological fluids. Free Radic. Res. 2005, 39, 797–815. [Google Scholar] [CrossRef] [PubMed]
- Lauer, T.; Preik, M.; Rassaf, T.; Strauer, B.E.; Deussen, A.; Feelisch, M.; Kelm, M. Plasma nitrite rather than nitrate reflects regional endothelial nitric oxide synthase activity but lacks intrinsic vasodilator action. Proc. Natl. Acad. Sci. USA 2001, 98, 12814–12819. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahluwalia, A.; Gladwin, M.; Coleman, G.D.; Hord, N.; Howard, G.; Kim-Shapiro, D.B.; Lajous, M.; Larsen, F.J.; Lefer, D.J.; McClure, L.A.; et al. Dietary nitrate and the epidemiology of cardiovascular disease: Report from a national heart, lung, and blood institute workshop. J. Am. Heart Assoc. 2016, 5, e003402. [Google Scholar] [CrossRef]
- Hu, C.W.; Chang, Y.J.; Yen, C.C.; Chen, J.L.; Muthukumaran, R.B.; Chao, M.R. (15)N-labelled nitrite/nitrate tracer analysis by LC-MS/MS: Urinary and fecal excretion of nitrite/nitrate following oral administration to mice. Free Radic. Biol. Med. 2019, 143, 193–202. [Google Scholar] [CrossRef]
- Turgut, T.; Ilhan, N.; Deveci, F.; Akpolat, N.; Erden, E.S.; Muz, M.H. Glutathione and nitrite levels in induced sputum at COPD patients and healthy smokers. J. Thorac. Dis. 2014, 6, 765–771. [Google Scholar]
- Formanek, W.; Inci, D.; Lauener, R.P.; Wildhaber, J.H.; Frey, U.; Hall, G.L. Elevated nitrite in breath condensates of children with respiratory disease. Eur. Respir. J. 2002, 19, 487–491. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Mei, F.; Bai, L.; Zhou, S.; Liu, D.; Yao, L.; Ahluwalia, A.; Ghiladi, R.A.; Su, L.; Shu, T.; et al. Serum nitrite and nitrate: A potential biomarker for post-COVID-19 complications? Free Radic. Biol. Med. 2021, 175, 216–225. [Google Scholar] [CrossRef]
- Bahadoran, Z.; Mirmiran, P.; Jeddi, S.; Carlstrom, M.; Azizi, F.; Ghasemi, A. Circulating markers of nitric oxide homeostasis and cardiometabolic diseases: Insights from population-based studies. Free Radic. Res. 2019, 53, 359–376. [Google Scholar] [CrossRef]
- Ghasemi, A.; Zahediasl, S.; Azizi, F. Reference values for serum nitric oxide metabolites in an adult population. Clin. Biochem. 2010, 43, 89–94. [Google Scholar] [CrossRef]
- Hoshino, T.; Nishima, D.; Enseki, M.; Umehara, N.; Fukasawa, C.; Ishiwada, N. Pediatric parapneumonic effusion/pleural empyema in Japan: A nationwide survey. Pediatr. Infect. Dis. J. 2022, 41, 20–23. [Google Scholar] [CrossRef]
- Forsythe, S.J.; Dolby, J.M.; Webster, A.D.; Cole, J.A. Nitrate- and nitrite-reducing bacteria in the achlorhydric stomach. J. Med. Microbiol. 1988, 25, 253–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, H.; Duncan, C.; Townend, J.; Killham, K.; Smith, L.M.; Johnston, P.; Dykhuizen, R.; Kelly, D.; Golden, M.; Benjamin, N.; et al. Nitrate-reducing bacteria on rat tongues. Appl. Environ. Microbiol. 1997, 63, 924–930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sato-Suzuki, Y.; Washio, J.; Wicaksono, D.P.; Sato, T.; Fukumoto, S.; Takahashi, N. Nitrite-producing oral microbiome in adults and children. Sci. Rep. 2020, 10, 16652. [Google Scholar] [CrossRef] [PubMed]
- Chao, M.R.; Shih, Y.M.; Hsu, Y.W.; Liu, H.H.; Chang, Y.J.; Lin, B.H.; Hu, C.W. Urinary nitrite/nitrate ratio measured by isotope-dilution LC-MS/MS as a tool to screen for urinary tract infections. Free Radic. Biol. Med. 2016, 93, 77–83. [Google Scholar] [CrossRef]
- Light, R.W. Clinical practice. Pleural effusion. N. Engl. J. Med. 2002, 346, 1971–1977. [Google Scholar] [CrossRef]
- Mambatta, A.K.; Jayarajan, J.; Rashme, V.L.; Harini, S.; Menon, S.; Kuppusamy, J. Reliability of dipstick assay in predicting urinary tract infection. J. Family. Med. Prim. Care 2015, 4, 265–268. [Google Scholar] [CrossRef]
- Utine, G.E.; Ozcelik, U.; Yalcin, E.; Dogru, D.; Kiper, N.; Aslan, A.; Kanra, G. Childhood parapneumonic effusions: Biochemical and inflammatory markers. Chest 2005, 128, 1436–1441. [Google Scholar] [CrossRef] [Green Version]
- Giustarini, D.; Dalle-Donne, I.; Colombo, R.; Milzani, A.; Rossi, R. Adaptation of the Griess reaction for detection of nitrite in human plasma. Free Radic. Res. 2004, 38, 1235–1240. [Google Scholar] [CrossRef]
- Sun, J.; Zhang, X.J.; Broderick, M.; Fein, H. Measurement of nitric oxide production in biological systems by using Griess Reaction assay. Sensors 2003, 3, 276–284. [Google Scholar] [CrossRef] [Green Version]
- Lam, C.W.; Law, C.Y. Pleural effusion lipoproteins measured by NMR spectroscopy for diagnosis of exudative pleural effusions: A novel tool for pore-size estimation. J. Proteome Res. 2014, 13, 4104–4112. [Google Scholar] [CrossRef] [PubMed]
- Wahl, S.M.; McCartney-Francis, N.; Chan, J.; Dionne, R.; Ta, L.; Orenstein, J.M. Nitric oxide in experimental joint inflammation. Benefit or detriment? Cells Tissues Organs 2003, 174, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Herrero-Cervera, A.; Soehnlein, O.; Kenne, E. Neutrophils in chronic inflammatory diseases. Cell Mol. Immunol. 2022, 19, 177–191. [Google Scholar] [CrossRef]
- Garg, N.; Syngle, A.; Krishan, P. Nitric Oxide: Link between Inflammation and Endothelial Dysfunction in Rheumatoid Arthritis. Int. J. Angiol. 2017, 26, 165–169. [Google Scholar] [CrossRef] [PubMed]
- Zweier, J.L.; Li, H.; Samouilov, A.; Liu, X. Mechanisms of nitrite reduction to nitric oxide in the heart and vessel wall. Nitric Oxide 2010, 22, 83–90. [Google Scholar] [CrossRef] [Green Version]
- Spack, L.; Havens, P.L.; Griffith, O.W. Measurements of total plasma nitrite and nitrate in pediatric patients with the systemic inflammatory response syndrome. Crit. Care Med. 1997, 25, 1071–1078. [Google Scholar] [CrossRef]
- Linnane, S.J.; Keatings, V.M.; Costello, C.M.; Moynihan, J.B.; O’Connor, C.M.; Fitzgerald, M.X.; McLoughlin, P. Total sputum nitrate plus nitrite is raised during acute pulmonary infection in cystic fibrosis. Am. J. Respir. Crit. Care Med. 1998, 158, 207–212. [Google Scholar] [CrossRef]
- Lin, T.Y.; Hwang, K.P.; Liu, C.C.; Tang, R.B.; Lin, C.Y.; Gilbert, G.L.; Thapa, K.; Monegal, J.S.; Pircon, J.Y.; Van Dyke, M.K.; et al. Etiology of empyema thoracis and parapneumonic pleural effusion in Taiwanese children and adolescents younger than 18 years of age. Pediatr. Infect. Dis. J. 2013, 32, 419–421. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cause | All Patients, n (%) |
|---|---|
| Exudates | 83 (58) |
| Malignant | 56 (39.2) |
| Lung | 34 (23.8) |
| Breast | 11 (7.7) |
| Others | 11 (7.7) |
| Infectious | 27 (18.9) |
| Parapneumonic | 23 (16.1) |
| Empyema | 4 (2.8) |
| Transudates | 60 (42) |
| CHF | 15 (10.5) |
| Cirrhosis | 8 (5.6) |
| Hypoalbuminemia | 33 (23.1) |
| CKD | 4 (2.8) |
| Variables | Exudates (n = 83) | Transudates (n = 60) | p Value |
|---|---|---|---|
| Age, yr | 69 ± 13 (41–92) a | 75 ± 14 (42–98) | 0.004 |
| Sex, male/female, n | 42/41 | 33/27 | |
| BMI, kg/m2 | 23 ± 3.9 (14–34) | 22 ± 4.2 (15–44) | 0.119 |
| Pleural effusions | |||
| pH | 7.5 (7.5–7.6) b | 7.6 (7.5–7.6) | 0.272 |
| LDH, U/L | 313 (264–371) | 85.7 (78.1–94) | ≤0.001 |
| Protein, g/dL | 3.7 (3.5–4.0) | 1.7 (1.6–1.9) | ≤0.001 |
| LDH PE/serum ratio | 1.3 (1.1–1.6) | 0.4 (0.3–0.4) | ≤0.001 |
| Protein PE/serum ratio | 0.5 (0.5–0.6) | 0.3 (0.2–0.3) | ≤0.001 |
| Glucose, mg/dL | 102 (86–120) | 139 (129–150) | 0.022 |
| WBCs, cells/μL | 1082 (824–1421) | 242 (177–332) | <0.001 |
| Lymphocytes,% | 38 (29–50) | 51 (43–59) | 0.998 |
| Neutrophils, % | 8 (6–11) | 7 (5–10) | 0.639 |
| Monocytes, % | 8 (6–9) | 8 (6–10) | 0.390 |
| Nitrite, μM | 2.12 (1.88–2.40) | 1.49 (1.31–1.69) | 0.002 |
| Nitrate, mM | 0.094 (0.082–0.107) | 0.108 (0.088–0.134) | 0.672 |
| Nitrite/nitrate ratio (μM/mM) | 23.3 (19.7–27.6) | 14.0 (11.3–17.4) | ≤0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chao, M.-R.; Chang, Y.-J.; Shih, Y.-M.; Chen, J.-L.; Yen, C.-C.; Hu, C.-W. Elevated Nitrite/Nitrate Ratio as a Potential Biomarker for the Differential Diagnosis of Pleural Effusions. Antioxidants 2022, 11, 1327. https://doi.org/10.3390/antiox11071327
Chao M-R, Chang Y-J, Shih Y-M, Chen J-L, Yen C-C, Hu C-W. Elevated Nitrite/Nitrate Ratio as a Potential Biomarker for the Differential Diagnosis of Pleural Effusions. Antioxidants. 2022; 11(7):1327. https://doi.org/10.3390/antiox11071327
Chicago/Turabian StyleChao, Mu-Rong, Yuan-Jhe Chang, Ying-Ming Shih, Jian-Lian Chen, Cheng-Chieh Yen, and Chiung-Wen Hu. 2022. "Elevated Nitrite/Nitrate Ratio as a Potential Biomarker for the Differential Diagnosis of Pleural Effusions" Antioxidants 11, no. 7: 1327. https://doi.org/10.3390/antiox11071327