
Nitrotyrosine, Nitrated Lipoproteins, and Cardiovascular Dysfunction in Patients with Type 2 Diabetes: What Do We Know and What Remains to Be Explained?




Abstract
:1. Introduction
1.1. Cardiovascular Disease in Patients Living with Diabetes Mellitus
1.2. Lipid Disorders in the Course of Diabetes Mellitus
1.3. Modified Lipoproteins in Atherogenesis
1.4. Oxidative Stress
1.5. The Purpose of This Paper
2. Nitrotyrosine, Diabetes, and Cardiovascular Disease
2.1. Cellular and Molecular Mechanisms
2.2. Association between Nitrotyrosine and Selected Risk Factors of CVD
2.3. Significance of Nitrotyrosine Measurements in Diagnosis of CVD and Prognosis
3. Nitrated Lipoproteins and Diabetes Mellitus
4. Nitrated Lipoproteins and Cardiovascular Disease
5. Factors Influencing Blood Concentration of Nitrated Lipoproteins
6. Conclusions and Directions for Future Research
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| ABCA1 | ATP-binding cassette transporter A1 |
| apoA-I | apolipoprotein A-I |
| apoB | apolipoprotein B |
| CABG | coronary artery bypass grafting |
| CETP | cholesteryl ester transfer protein |
| CHD | coronary heart disease |
| CIMT | carotid intima–media thickness |
| CKD | chronic kidney disease |
| COPD | chronic obstructive pulmonary disease |
| COX-2 | cyclooxygenase-2 |
| CVD | cardiovascular disease |
| DM | diabetes mellitus |
| ESRD | end-stage renal disease |
| FFA | free fatty acid |
| FMD | flow-mediated dilation |
| FoxO1 | transcription factor forkhead box O1 |
| Foxa2 | transcription factor forkhead box A2 |
| HDL | high-density lipoprotein |
| HDL-C | high-density lipoprotein cholesterol |
| HIV | human immunodeficiency virus |
| ICVD | ischemic cerebrovascular disease |
| IR | insulin resistance |
| LDL | low-density lipoprotein |
| LDL-C | low-density lipoprotein cholesterol |
| MPO | myeloperoxidase |
| MS | metabolic syndrome |
| MTP | microsomal triglyceride transfer protein |
| NO | nitric oxide |
| NT-apoA–I | nitrated apolipoprotein A–I |
| NT-apoB | nitrated apolipoprotein B |
| NT-HDL | nitrated high-density lipoprotein |
| NT-LDL | nitrated low-density lipoprotein |
| NT-Tyr | nitrotyrosine |
| OS | oxidative stress |
| oxLDL | oxidized LDL particle |
| PAD | peripheral arterial disease |
| PON-1 | paraoxonase-1 |
| PPARβ | peroxisome proliferator-activated receptor β |
| PTP-1B | protein-tyrosine phosphatase-1B |
| PWV | pulse-wave velocity |
| ROS | reactive oxygen species |
| RNS | reactive nitrogen species |
| sdLDL | small dense low-density lipoprotein |
| SREBP1c | sterol regulatory element-binding protein 1c |
| TG | triglycerides |
| T1DM | type 1 diabetes mellitus |
| T2DM | type 2 diabetes mellitus |
| VLDL | very low-density lipoprotein |
| VRI | vascular reactivity index |
| VSAP | vasospastic angina pectoris |
References
- Lovic, D.; Piperidou, A.; Zografou, I.; Grassos, H.; Pittaras, A.; Manolis, A. The growing epidemic of diabetes mellitus. Curr. Vasc. Pharmacol. 2020, 18, 104–109. [Google Scholar] [CrossRef]
- Fan, W. Epidemiology in diabetes mellitus and cardiovascular disease. Cardiovasc. Endocrinol. 2017, 6, 8–16. [Google Scholar] [CrossRef]
- Mahtta, D.; Khalid, U.; Misra, A.; Samad, Z.; Nasir, K.; Virani, S.S. Premature atherosclerotic cardiovascular disease: What have we learned recently? Curr. Atheroscler. Rep. 2020, 22, 44. [Google Scholar] [CrossRef]
- Jakubiak, G.K.; Pawlas, N.; Cieślar, G.; Stanek, A. Chronic lower extremity ischemia and its association with the frailty syndrome in patients with diabetes. Int. J. Environ. Res. Public Health 2020, 17, 9339. [Google Scholar] [CrossRef]
- Jakubiak, G.K.; Pawlas, N.; Cieślar, G.; Stanek, A. Pathogenesis and clinical significance of in-stent restenosis in patients with diabetes. Int. J. Environ. Res. Public Health 2021, 18, 11970. [Google Scholar] [CrossRef]
- Norata, G.D.; Pirillo, A.; Catapano, A.L. Modified HDL: Biological and physiopathological consequences. Nutr. Metab. Cardiovasc. Dis. 2006, 16, 371–386. [Google Scholar] [CrossRef]
- Summerhill, V.I.; Grechko, A.V.; Yet, S.F.; Sobenin, I.A.; Orekhov, A.N. The atherogenic role of circulating modified lipids in atherosclerosis. Int. J. Mol. Sci. 2019, 20, 3561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Obama, T.; Itabe, H. Neutrophils as a novel target of modified low-density lipoproteins and an accelerator of cardiovascular diseases. Int. J. Mol. Sci. 2020, 21, 8312. [Google Scholar] [CrossRef]
- Warraich, H.J.; Rana, J.S. Dyslipidemia in diabetes mellitus and cardiovascular disease. Cardiovasc. Endocrinol. 2017, 6, 27–32. [Google Scholar] [CrossRef]
- Bahiru, E.; Hsiao, R.; Phillipson, D.; Watson, K.E. Mechanisms and treatment of dyslipidemia in diabetes. Curr. Cardiol. Rep. 2021, 23, 26. [Google Scholar] [CrossRef]
- Taskinen, M.R.; Borén, J. New insights into the pathophysiology of dyslipidemia in type 2 diabetes. Atherosclerosis 2015, 239, 483–495. [Google Scholar] [CrossRef] [PubMed]
- Zozulińska, D. Atherogenic dyslipidaemia in type 2 diabetes. Kardiol. Pol. 2006, 64, S567–S571. [Google Scholar] [PubMed]
- Sivan, E.; Boden, G. Free fatty acids, insulin resistance, and pregnancy. Curr. Diab. Rep. 2003, 3, 319–322. [Google Scholar] [CrossRef]
- Chirieac, D.V.; Chirieac, L.R.; Corsetti, J.P.; Cianci, J.; Sparks, C.E.; Sparks, J.D. Glucose-stimulated insulin secretion suppresses hepatic triglyceride-rich lipoprotein and apoB production. Am. J. Physiol. Endocrinol. Metab. 2000, 279, E1003–E1011. [Google Scholar] [CrossRef]
- Chirieac, D.V.; Cianci, J.; Collins, H.L.; Sparks, J.D.; Sparks, C.E. Insulin suppression of VLDL apo B secretion is not mediated by the LDL receptor. Biochem. Biophys. Res. Commun. 2002, 297, 134–137. [Google Scholar] [CrossRef]
- Chirieac, D.V.; Collins, H.L.; Cianci, J.; Sparks, J.D.; Sparks, C.E. Altered triglyceride-rich lipoprotein production in Zucker diabetic fatty rats. Am. J. Physiol. Endocrinol. Metab. 2004, 287, E42–E49. [Google Scholar] [CrossRef] [Green Version]
- Taghibiglou, C.; Rashid-Kolvear, F.; Van Iderstine, S.C.; Le-Tien, H.; Fantus, I.G.; Lewis, G.F.; Adeli, K. Hepatic very low density lipoprotein-ApoB overproduction is associated with attenuated hepatic insulin signaling and overexpression of protein-tyrosine phosphatase 1B in a fructose-fed hamster model of insulin resistance. J. Biol. Chem. 2002, 277, 793–803. [Google Scholar] [CrossRef] [Green Version]
- Kuriyama, H.; Yamashita, S.; Shimomura, I.; Funahashi, T.; Ishigami, M.; Aragane, K.; Miyaoka, K.; Nakamura, T.; Takemura, K.; Man, Z.; et al. Enhanced expression of hepatic acyl-coenzyme A synthetase and microsomal triglyceride transfer protein messenger RNAs in the obese and hypertriglyceridemic rat with visceral fat accumulation. Hepatology 1998, 27, 557–562. [Google Scholar] [CrossRef]
- Lin, M.C.; Gordon, D.; Wetterau, J.R. Microsomal triglyceride transfer protein (MTP) regulation in HepG2 cells: Insulin negatively regulates MTP gene expression. J. Lipid Res. 1995, 36, 1073–1081. [Google Scholar] [CrossRef]
- Au, W.S.; Kung, H.F.; Lin, M.C. Regulation of microsomal triglyceride transfer protein gene by insulin in HepG2 cells: Roles of MAPKerk and MAPKp38. Diabetes 2003, 52, 1073–1080. [Google Scholar] [CrossRef] [Green Version]
- Kamagate, A.; Qu, S.; Perdomo, G.; Su, D.; Kim, D.H.; Slusher, S.; Meseck, M.; Dong, H.H. FoxO1 mediates insulin-dependent regulation of hepatic VLDL production in mice. J. Clin. Investig. 2008, 118, 2347–2364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koo, S.H.; Montminy, M. Fatty acids and insulin resistance: A perfect storm. Mol. Cell. 2006, 21, 449–450. [Google Scholar] [CrossRef] [PubMed]
- Lorey, M.B.; Öörni, K.; Kovanen, P.T. Modified lipoproteins induce arterial wall inflammation during atherogenesis. Front. Cardiovasc. Med. 2022, 9, 841545. [Google Scholar] [CrossRef] [PubMed]
- Younis, N.; Soran, H.; Sharma, R.; Charlton-Menys, K.; Durrington, P. Lipoprotein glycation in atherogenesis. Clin. Lipidol. 2009, 4, 781–790. [Google Scholar] [CrossRef]
- Poznyak, A.V.; Nikiforov, N.G.; Markin, A.M.; Kashirskikh, D.A.; Myasoedova, V.A.; Gerasimova, E.V.; Orekhov, A.N. Overview of oxLDL and its impact on cardiovascular health: Focus on atherosclerosis. Front. Pharmacol. 2021, 11, 613780. [Google Scholar] [CrossRef]
- El Hadri, K.; Smith, R.; Duplus, E.; El Amri, C. Inflammation, oxidative stress, senescence in atherosclerosis: Thioredoxine-1 as an emerging therapeutic target. Int. J. Mol. Sci. 2021, 23, 77. [Google Scholar] [CrossRef]
- Yaribeygi, H.; Atkin, S.L.; Sahebkar, A. A review of the molecular mechanisms of hyperglycemia-induced free radical generation leading to oxidative stress. J. Cell. Physiol. 2019, 234, 1300–1312. [Google Scholar] [CrossRef]
- Tramutola, A.; Lanzillotta, C.; Perluigi, M.; Butterfield, D.A. Oxidative stress, protein modification and alzheimer disease. Brain Res. Bull. 2017, 133, 88–96. [Google Scholar] [CrossRef]
- Kulbacka, J.; Saczko, J.; Chwiłkowska, A. Stres oksydacyjny w procesach uszkodzenia komórek. Pol. Merk. Lek. 2009, 27, 44–47. [Google Scholar]
- Teleanu, R.I.; Chircov, C.; Grumezescu, A.M.; Volceanov, A.; Teleanu, D.M. Antioxidant therapies for neuroprotection–a review. J. Clin. Med. 2019, 8, 1659. [Google Scholar] [CrossRef] [Green Version]
- Truong, V.L.; Jeong, W.S. Cellular defensive mechanisms of tea polyphenols: Structure-activity relationship. Int. J. Mol. Sci. 2021, 22, 9109. [Google Scholar] [CrossRef] [PubMed]
- Parker, H.; Winterbourn, C.C. Reactive oxidants and myeloperoxidase and their involvement in neutrophil extracellular traps. Front. Immunol. 2013, 3, 424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cervantes Gracia, K.; Llanas-Cornejo, D.; Husi, H. CVD and oxidative stress. J. Clin. Med. 2017, 6, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liguori, I.; Russo, G.; Curcio, F.; Bulli, G.; Aran, L.; Della-Morte, D.; Gargiulo, G.; Testa, G.; Cacciatore, F.; Bonaduce, D.; et al. Oxidative stress, aging, and diseases. Clin. Interv. Aging 2018, 13, 757–772. [Google Scholar] [CrossRef] [Green Version]
- Stanek, A.; Cholewka, A.; Wielkoszyński, T.; Romuk, E.; Sieroń, A. Decreased oxidative stress in male patients with active phase ankylosing spondylitis who underwent whole-body cryotherapy in closed cryochamber. Oxid. Med. Cell. Longev. 2018, 2018, 7365490. [Google Scholar] [CrossRef]
- Stanek, A.; Brożyna-Tkaczyk, K.; Myśliński, W. Oxidative stress markers among obstructive sleep apnea patients. Oxid. Med. Cell. Longev. 2021, 2021, 9681595. [Google Scholar] [CrossRef]
- Jakubiak, G.K.; Osadnik, K.; Lejawa, M.; Kasperczyk, S.; Osadnik, T.; Pawlas, N. Oxidative stress in association with metabolic health and obesity in young adults. Oxid. Med. Cell. Longev. 2021, 2021, 9987352. [Google Scholar] [CrossRef]
- Jakubiak, G.K.; Osadnik, K.; Lejawa, M.; Osadnik, T.; Goławski, M.; Lewandowski, P.; Pawlas, N. “Obesity and insulin resistance” is the component of the metabolic syndrome most strongly associated with oxidative stress. Antioxidants 2022, 11, 79. [Google Scholar] [CrossRef]
- Maiuolo, J.; Gliozzi, M.; Carresi, C.; Musolino, V.; Oppedisano, F.; Scarano, F.; Nucera, S.; Scicchitano, M.; Bosco, F.; Macri, R.; et al. Nutraceuticals and cancer: Potential for natural polyphenols. Nutrients 2021, 13, 3834. [Google Scholar] [CrossRef]
- Schiffers, C.; Reynaert, N.L.; Wouters, E.F.M.; van der Vliet, A. Redox dysregulation in aging and COPD: Role of NOX enzymes and implications for antioxidant strategies. Antioxidants 2021, 10, 1799. [Google Scholar] [CrossRef]
- Rasaei, N.; Asbaghi, O.; Samadi, M.; Setayesh, L.; Bagheri, R.; Gholami, F.; Soveid, N.; Casazza, K.; Wong, A.; Suzuki, K.; et al. Effect of green tea supplementation on antioxidant status in adults: A systematic review and meta-analysis of randomized clinical trials. Antioxidants 2021, 10, 1731. [Google Scholar] [CrossRef] [PubMed]
- Pacher, P.; Szabó, C. Role of peroxynitrite in the pathogenesis of cardiovascular complications of diabetes. Curr. Opin. Pharmacol. 2006, 6, 136–141. [Google Scholar] [CrossRef] [PubMed]
- Stankova, T.R.; Delcheva, G.T.; Maneva, A.I.; Vladeva, S.V. Serum levels of carbamylated LDL, nitrotyrosine and soluble lectin-like oxidized low-density lipoprotein receptor-1 in poorly controlled type 2 diabetes mellitus. Folia Med. 2019, 61, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Bo, S.; Gambino, R.; Guidi, S.; Silli, B.; Gentile, L.; Cassader, M.; Pagano, G.F. Plasma nitrotyrosine levels, antioxidant vitamins and hyperglycaemia. Diabet. Med. 2005, 22, 1185–1189. [Google Scholar] [CrossRef] [PubMed]
- Segre, C.A.; Hueb, W.; Garcia, R.M.; Rezende, P.C.; Favarato, D.; Strunz, C.M.; Sprandel Mda, C.; Roggério, A.; Carvalho, A.L.; Maranhão, R.C.; et al. Troponin in diabetic patients with and without chronic coronary artery disease. BMC Cardiovasc. Disord. 2015, 15, 72. [Google Scholar] [CrossRef] [Green Version]
- Korkmaz-Icöz, S.; Kocer, C.; Sayour, A.A.; Kraft, P.; Benker, M.I.; Abulizi, S.; Georgevici, A.I.; Brlecic, P.; Radovits, T.; Loganathan, S.; et al. The sodium-glucose cotransporter-2 inhibitor canagliflozin alleviates endothelial dysfunction following in vitro vascular ischemia/reperfusion injury in rats. Int. J. Mol. Sci. 2021, 22, 7774. [Google Scholar] [CrossRef]
- Wu, N.; Shen, H.; Liu, H.; Wang, Y.; Bai, Y.; Han, P. Acute blood glucose fluctuation enhances rat aorta endothelial cell apoptosis, oxidative stress and pro-inflammatory cytokine expression in vivo. Cardiovasc. Diabetol. 2016, 15, 109. [Google Scholar] [CrossRef] [Green Version]
- Zanetti, M.; Gortan Cappellari, G.; Barbetta, D.; Semolic, A.; Barazzoni, R. Omega 3 polyunsaturated fatty acids improve endothelial dysfunction in chronic renal failure: Role of eNOS activation and of oxidative stress. Nutrients 2017, 9, 895. [Google Scholar] [CrossRef] [Green Version]
- Ceriello, A.; Esposito, K.; La Sala, L.; Pujadas, G.; De Nigris, V.; Testa, R.; Bucciarelli, L.; Rondinelli, M.; Genovese, S. The protective effect of the Mediterranean diet on endothelial resistance to GLP-1 in type 2 diabetes: A preliminary report. Cardiovasc. Diabetol. 2014, 13, 140. [Google Scholar] [CrossRef] [PubMed]
- Chikopela, T.; Goma, F.; Kaluba, L.; Mutale, W.; Guure, C.; Heimburger, D.C.; Koethe, J.R. Arterial stiffness is associated with oxidative stress and endothelial activation among persons with treated HIV in Zambia. South. Afr. J. HIV Med. 2021, 22, 1298. [Google Scholar] [CrossRef]
- Beckmann, J.S.; Ye, Y.Z.; Anderson, P.G.; Chen, J.; Accavitti, M.A.; Tarpey, M.M.; White, C.R. Extensive nitration of protein tyrosines in human atherosclerosis detected by immunohistochemistry. Biol. Chem. Hoppe Seyler 1994, 375, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Guilgen, G.; Werneck, M.L.; de Noronha, L.; Martins, A.P.; Varela, A.M.; Nakao, L.S.; Pecoits-Filho, R. Increased calcification and protein nitration in arteries of chronic kidney disease patients. Blood Purif. 2011, 32, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Luksha, N.; Luksha, L.; Carrero, J.J.; Hammarqvist, F.; Stenvinkel, P.; Kublickiene, K. Impaired resistance artery function in patients with end-stage renal disease. Clin. Sci. 2011, 120, 525–536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paier, A.; Agewall, S.; Kublickiene, K. Expression of heat shock proteins and nitrotyrosine in small arteries from patients with coronary heart disease. Heart Vessel. 2009, 24, 260–266. [Google Scholar] [CrossRef]
- Sardu, C.; D’Onofrio, N.; Torella, M.; Portoghese, M.; Mureddu, S.; Loreni, F.; Ferraraccio, F.; Panarese, I.; Trotta, M.C.; Gatta, G.; et al. Metformin therapy effects on the expression of sodium-glucose cotransporter 2, leptin, and SIRT6 levels in pericoronary fat excised from pre-diabetic patients with acute myocardial infarction. Biomedicines 2021, 9, 904. [Google Scholar] [CrossRef]
- Monami, M.; Candido, R.; Pintaudi, B.; Targher, G.; Mannucci, E.; SID-AMD joint panel for Italian guidelines on treatment of type 2 diabetes. Effect of metformin on all-cause mortality and major adverse cardiovascular events: An updated meta-analysis of randomized controlled trials. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 699–704. [Google Scholar] [CrossRef]
- Zhang, K.; Yang, W.; Dai, H.; Deng, Z. Cardiovascular risk following metformin treatment in patients with type 2 diabetes mellitus: Results from meta-analysis. Diabetes Res. Clin. Pract. 2020, 160, 108001. [Google Scholar] [CrossRef]
- Li, T.; Providencia, R.; Mu, N.; Yin, Y.; Chen, M.; Wang, Y.; Liu, M.; Yu, L.; Gu, C.; Ma, H. Association of metformin monotherapy or combined therapy with cardiovascular risks in patients with type 2 diabetes mellitus. Cardiovasc. Diabetol. 2021, 20, 30. [Google Scholar] [CrossRef]
- Chen, Y.; Li, H.; Ye, Z.; Găman, M.A.; Tan, S.C.; Zhu, F. The effect of metformin on carotid intima-media thickness (CIMT): A systematic review and meta-analysis of randomized clinical trials. Eur. J. Pharmacol. 2020, 886, 173458. [Google Scholar] [CrossRef]
- Kolijn, D.; Pabel, S.; Tian, Y.; Lódi, M.; Herwig, M.; Carrizzo, A.; Zhazykbayeva, S.; Kovács, Á.; Fülöp, G.Á.; Falcão-Pires, I.; et al. Empagliflozin improves endothelial and cardiomyocyte function in human heart failure with preserved ejection fraction via reduced pro-inflammatory-oxidative pathways and protein kinase Gα oxidation. Cardiovasc. Res. 2021, 117, 495–507. [Google Scholar] [CrossRef]
- Zhou, Y.; Wang, H.; Man, F.; Guo, Z.; Xu, J.; Yan, W.; Li, J.; Pan, Q.; Wang, W. Sitagliptin protects cardiac function by reducing nitroxidative stress and promoting autophagy in Zucker diabetic fatty (ZDF) rats. Cardiovasc. Drugs Ther. 2018, 32, 541–552. [Google Scholar] [CrossRef] [PubMed]
- Mayyas, F.; Alzoubi, K.H.; Bonyan, R. The role of spironolactone on myocardial oxidative stress in rat model of streptozotocin-induced diabetes. Cardiovasc. Ther. 2017, 35, e12242. [Google Scholar] [CrossRef] [PubMed]
- Helmstädter, J.; Keppeler, K.; Aust, F.; Küster, L.; Frenis, K.; Filippou, K.; Vujacic-Mirski, K.; Tsohataridis, S.; Kalinovic, S.; Kröller-Schön, S.; et al. GLP-1 analog liraglutide improves vascular function in polymicrobial sepsis by reduction of oxidative stress and inflammation. Antioxidants 2021, 10, 1175. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Wang, Y.; Zhang, J.; Potter, B.J.; Sowers, J.R.; Zhang, C. Bariatric surgery reduces visceral adipose inflammation and improves endothelial function in type 2 diabetic mice. Arterioscler. Thromb. Vasc. Biol. 2011, 31, 2063–2069. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.L.; Wei, J.R. 3-nitrotyrosine, a biomarker for cardiomyocyte apoptosis induced by diabetic cardiomyopathy in a rat model. Mol. Med. Rep. 2013, 8, 989–994. [Google Scholar] [CrossRef] [Green Version]
- Wang, F.; Yuan, Q.; Chen, F.; Pang, J.; Pan, C.; Xu, F.; Chen, Y. Fundamental mechanisms of the cell death caused by nitrosative stress. Front. Cell Dev. Biol. 2021, 9, 742483. [Google Scholar] [CrossRef]
- Ott, C.; Tomasina, F.; Campolo, N.; Bartesaghi, S.; Mastrogiovanni, M.; Leyva, A.; Batthyány, C.; Meinl, W.; Grune, T.; Radi, R. Decreased proteasomal cleavage at nitrotyrosine sites in proteins and peptides. Redox Biol. 2021, 46, 102106. [Google Scholar] [CrossRef]
- Yang, C.; Xue, L.; Wu, Y.; Li, S.; Zhou, S.; Yang, J.; Jiang, C.; Ran, J.; Jiang, Q. PPARβ down-regulation is involved in high glucose-induced endothelial injury via acceleration of nitrative stress. Microvasc. Res. 2022, 139, 104272. [Google Scholar] [CrossRef]
- Quintela, A.M.; Jiménez, R.; Gómez-Guzmán, M.; Zarzuelo, M.J.; Galindo, P.; Sánchez, M.; Vargas, F.; Cogolludo, A.; Tamargo, J.; Pérez-Vizcaíno, F.; et al. Activation of peroxisome proliferator-activated receptor-β/-δ (PPARβ/δ) prevents endothelial dysfunction in type 1 diabetic rats. Free Radic. Biol. Med. 2012, 53, 730–741. [Google Scholar] [CrossRef]
- Mihm, M.J.; Jing, L.; Bauer, J.A. Nitrotyrosine causes selective vascular endothelial dysfunction and DNA damage. J. Cardiovasc. Pharmacol. 2000, 36, 182–187. [Google Scholar] [CrossRef]
- Mu, H.; Wang, X.; Lin, P.; Yao, Q.; Chen, C. Nitrotyrosine promotes human aortic smooth muscle cell migration through oxidative stress and ERK1/2 activation. Biochim. Biophys. Acta 2008, 1783, 1576–1584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pialoux, V.; Poulin, M.J.; Hemmelgarn, B.R.; Muruve, D.A.; Chirico, E.N.; Faes, C.; Sola, D.Y.; Ahmed, S.B. Cyclooxygenase-2 inhibition limits angiotensin II-induced DNA oxidation and protein nitration in humans. Front. Physiol. 2017, 8, 138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daugherty, A.; Cassis, L. Angiotensin II-mediated development of vascular diseases. Trends Cardiovasc. Med. 2004, 14, 117–120. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Z.J.; Vapaatalo, H.; Mervaala, E. Angiotensin II and vascular inflammation. Med. Sci Monit. 2005, 11, RA194–RA205. [Google Scholar] [PubMed]
- Szumska, M.; Wielkoszyński, T.; Tyrpień, K. 3-nitrotyrosine determination as nitrosative stress marker and health attitudes of medical students considering exposure to environmental tobacco smoke. Przegl. Lek. 2012, 69, 798–802. [Google Scholar] [PubMed]
- Wielkoszyński, T.; Zalejska-Fiolka, J.; Strzelczyk, J.K.; Owczarek, A.J.; Cholewka, A.; Kokoszczyk, K.; Stanek, A. 5α,6α-epoxyphytosterols and 5α,6α-epoxycholesterol increase nitrosative stress and inflammatory cytokine production in rats on low-cholesterol diet. Oxid. Med. Cell. Longev. 2020, 2020, 4751803. [Google Scholar] [CrossRef] [PubMed]
- Adams, T.; Wan, E.; Wei, Y.; Wahab, R.; Castagna, F.; Wang, G.; Emin, M.; Russo, C.; Homma, S.; Le Jemtel, T.H.; et al. Secondhand smoking is associated with vascular inflammation. Chest 2015, 148, 112–119. [Google Scholar] [CrossRef] [Green Version]
- Jin, H.; Webb-Robertson, B.J.; Peterson, E.S.; Tan, R.; Bigelow, D.J.; Scholand, M.B.; Hoidal, J.R.; Pounds, J.G.; Zangar, R.C. Smoking, COPD, and 3-nitrotyrosine levels of plasma proteins. Environ. Health Perspect. 2011, 119, 1314–1320. [Google Scholar] [CrossRef] [Green Version]
- Choromańska, B.; Myśliwiec, P.; Dadan, J.; Maleckas, A.; Zalewska, A.; Maciejczyk, M. Effects of age and gender on the redox homeostasis of morbidly obese people. Free Radic. Biol. Med. 2021, 175, 108–120. [Google Scholar] [CrossRef]
- Fenster, C.P.; Darley-Usmar, V.M.; Landar, A.L.; Gower, B.A.; Weinsier, R.L.; Hunter, G.R.; Patel, R.P. Weight loss and race modulate nitric oxide metabolism in overweight women. Free Radic. Biol. Med. 2004, 37, 695–702. [Google Scholar] [CrossRef]
- Fuentes-Venado, C.E.; Terán-Pérez, G.; Espinosa-Hernández, V.M.; Martínez-Herrera, E.; Segura-Uribe, J.J.; Mercadillo, R.E.; Pinto-Almazán, R.; Guerra-Araiza, C. Nutritional status influences oxidative stress and insulin resistance in preschool children. Metab. Syndr. Relat. Disord. 2021, 19, 513–523. [Google Scholar] [CrossRef] [PubMed]
- Choromańska, B.; Myśliwiec, P.; Łuba, M.; Wojskowicz, P.; Myśliwiec, H.; Choromańska, K.; Dadan, J.; Żendzian-Piotrowska, M.; Zalewska, A.; Maciejczyk, M. Bariatric surgery normalizes protein glycoxidation and nitrosative stress in morbidly obese patients. Antioxidants 2020, 9, 1087. [Google Scholar] [CrossRef] [PubMed]
- Pennathur, S.; Jaiswal, M.; Vivekanandan-Giri, A.; White, E.A.; Ang, L.; Raffel, D.M.; Rubenfire, M.; Pop-Busui, R. Structured lifestyle intervention in patients with the metabolic syndrome mitigates oxidative stress but fails to improve measures of cardiovascular autonomic neuropathy. J. Diabetes Complicat. 2017, 31, 1437–1443. [Google Scholar] [CrossRef]
- Jialal, I.; Devaraj, S.; Adams-Huet, B.; Chen, X.; Kaur, H. Increased cellular and circulating biomarkers of oxidative stress in nascent metabolic syndrome. J. Clin. Endocrinol. Metab. 2012, 97, E1844–E1850. [Google Scholar] [CrossRef] [Green Version]
- Macut, D.; Simic, T.; Lissounov, A.; Pljesa-Ercegovac, M.; Bozic, I.; Djukic, T.; Bjekic-Macut, J.; Matic, M.; Petakov, M.; Suvakov, S.; et al. Insulin resistance in non-obese women with polycystic ovary syndrome: Relation to byproducts of oxidative stress. Exp. Clin. Endocrinol. Diabetes 2011, 119, 451–455. [Google Scholar] [CrossRef] [PubMed]
- Ceriello, A.; Assaloni, R.; Da Ros, R.; Maier, A.; Quagliaro, L.; Piconi, L.; Esposito, K.; Giugliano, D. Effect of irbesartan on nitrotyrosine generation in non-hypertensive diabetic patients. Diabetologia 2004, 47, 1535–1540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charkiewicz, A.E.; Garley, M.; Ratajczak-Wrona, W.; Nowak, K.; Jabłońska, E.; Maślach, D.; Omeljaniuk, W.J. Profile of new vascular damage biomarkers in middle-aged men with arterial hypertension. Adv. Med. Sci. 2021, 66, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Shishehbor, M.H.; Aviles, R.J.; Brennan, M.L.; Fu, X.; Goormastic, M.; Pearce, G.L.; Gokce, N.; Keaney, J.F., Jr.; Penn, M.S.; Sprecher, D.L.; et al. Association of nitrotyrosine levels with cardiovascular disease and modulation by statin therapy. JAMA 2003, 289, 1675–1680. [Google Scholar] [CrossRef] [Green Version]
- Pirro, M.; Schillaci, G.; Mannarino, M.R.; Savarese, G.; Vaudo, G.; Siepi, D.; Paltriccia, R.; Mannarino, E. Effects of rosuvastatin on 3-nitrotyrosine and aortic stiffness in hypercholesterolemia. Nutr. Metab. Cardiovasc. Dis. 2007, 17, 436–441. [Google Scholar] [CrossRef]
- Ferlazzo, N.; Currò, M.; Isola, G.; Maggio, S.; Bertuccio, M.P.; Trovato-Salinaro, A.; Matarese, G.; Alibrandi, A.; Caccamo, D.; Ientile, R. Changes in the biomarkers of oxidative/nitrosative stress and endothelial dysfunction are associated with cardiovascular risk in periodontitis patients. Curr. Issues Mol. Biol. 2021, 43, 704–715. [Google Scholar] [CrossRef]
- Quidim, A.V.L.; Bruno, T.; Leocádio, P.C.L.; Santos, I.S.; Alvarez-Leite, J.I.; Dos Reis Menta, P.L.; Lotufo, P.A.; Benseñor, I.M.; Goulart, A.C. The prognostic value of nitrotyrosine levels in coronary heart disease: Long-term evaluation in the Acute Coronary Syndrome Registry Strategy (ERICO study). Clin. Biochem. 2019, 66, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Heslop, C.L.; Frohlich, J.J.; Hill, J.S. Myeloperoxidase and C-reactive protein have combined utility for long-term prediction of cardiovascular mortality after coronary angiography. J. Am. Coll. Cardiol. 2010, 55, 1102–1109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanabe, K.; Kawai, Y.; Kitayama, M.; Akao, H.; Ishida, R.; Motoyama, A.; Wakasa, M.; Saito, R.; Aoki, H.; Fujibayashi, K.; et al. Increased levels of the oxidative stress marker, nitrotyrosine in patients with provocation test-induced coronary vasospasm. J. Cardiol. 2014, 64, 86–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elfatih, A.; Anderson, N.R.; Mansoor, S.; Ahmed, S.; Horton, R.; Holland, M.R.; Gama, R. Plasma nitrotyrosine in reversible myocardial ischaemia. J. Clin. Pathol. 2005, 58, 95–96. [Google Scholar] [CrossRef] [Green Version]
- Zhu, L.; Li, S.; Liu, W.; Chen, J.; Yu, Q.; Zhang, Z.; Li, Y.; Liu, J.; Chen, X. Real time detection of 3-nitrotyrosine using smartphone-based electrochemiluminescence. Biosens. Bioelectron. 2021, 187, 113284. [Google Scholar] [CrossRef]
- Rebolledo, O.R.; Actis Dato, S.M. Postprandial hyperglycemia and hyperlipidemia-generated glycoxidative stress: Its contribution to the pathogenesis of diabetes complications. Eur. Rev. Med. Pharmacol. Sci. 2005, 9, 191–208. [Google Scholar]
- Bakillah, A.; Tedla, F.; Ayoub, I.; John, D.; Norin, A.J.; Hussain, M.M.; Brown, C. Plasma nitration of high-density and low-density lipoproteins in chronic kidney Disease Patients Receiving Kidney Transplants. Mediat. Inflamm. 2015, 2015, 352356. [Google Scholar] [CrossRef] [Green Version]
- Peng, L.; Li, X.; Li, Y.; Zhao, W.; Nie, S.; Yu, H.; Qi, Y.; Qin, Y.; Zhang, H. Increased concentrations of myeloperoxidase in serum and serum extracellular vesicles are associated with type 2 diabetes mellitus. Clin. Chim. Acta. 2021, 522, 70–76. [Google Scholar] [CrossRef]
- Moldoveanu, E.; Tanaseanu, C.; Tanaseanu, S.; Kosaka, T.; Manea, G.; Marta, D.S.; Popescu, L.M. Plasma markers of endothelial dysfunction in type 2 diabetics. Eur. J. Intern. Med. 2006, 17, 38–42. [Google Scholar] [CrossRef]
- Wiersma, J.J.; Meuwese, M.C.; van Miert, J.N.; Kastelein, A.; Tijssen, J.G.; Piek, J.J.; Trip, M.D. Diabetes mellitus type 2 is associated with higher levels of myeloperoxidase. Med. Sci. Monit. 2008, 14, CR406–CR410. [Google Scholar]
- Rovira-Llopis, S.; Rocha, M.; Falcon, R.; de Pablo, C.; Alvarez, A.; Jover, A.; Hernandez-Mijares, A.; Victor, V.M. Is myeloperoxidase a key component in the ROS-induced vascular damage related to nephropathy in type 2 diabetes? Antioxid. Redox. Signal. 2013, 19, 1452–1458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qaddoumi, M.G.; Alanbaei, M.; Hammad, M.M.; Al Khairi, I.; Cherian, P.; Channanath, A.; Thanaraj, T.A.; Al-Mulla, F.; Abu-Farha, M.; Abubaker, J. Investigating the role of myeloperoxidase and angiopoietin-like protein 6 in obesity and diabetes. Sci. Rep. 2020, 10, 6170. [Google Scholar] [CrossRef] [Green Version]
- Schindhelm, R.K.; Alssema, M.; Diamant, M.; Teerlink, T.; Dekker, J.M.; Kok, A.; Kostense, P.J.; Nijpels, G.; Heine, R.J.; Scheffer, P.G. Comparison of two consecutive fat-rich and carbohydrate-rich meals on postprandial myeloperoxidase response in women with and without type 2 diabetes mellitus. Metabolism 2008, 57, 262–267. [Google Scholar] [CrossRef]
- Hermo, R.; Mier, C.; Mazzotta, M.; Tsuji, M.; Kimura, S.; Gugliucci, A. Circulating levels of nitrated apolipoprotein A-I are increased in type 2 diabetic patients. Clin. Chem. Lab. Med. 2005, 43, 601–606. [Google Scholar] [CrossRef] [PubMed]
- Gugliucci, A.; Hermo, R.; Tsuji, M.; Kimura, S. Lower serum paraoxonase-1 activity in type 2 diabetic patients correlates with nitrated apolipoprotein A-I levels. Clin. Chim. Acta 2006, 368, 201–202. [Google Scholar] [CrossRef] [PubMed]
- Shokri, Y.; Variji, A.; Nosrati, M.; Khonakdar-Tarsi, A.; Kianmehr, A.; Kashi, Z.; Bahar, A.; Bagheri, A.; Mahrooz, A. Importance of paraoxonase 1 (PON1) as an antioxidant and antiatherogenic enzyme in the cardiovascular complications of type 2 diabetes: Genotypic and phenotypic evaluation. Diabetes Res. Clin. Pract. 2020, 161, 108067. [Google Scholar] [CrossRef]
- Chen, X.; Bakillah, A.; Zhou, L.; Pan, X.; Hoepfner, F.; Jacob, M.; Jiang, X.C.; Lazar, J.; Schlitt, A.; Hussain, M.M. Nitrated apolipoprotein AI/apolipoprotein AI ratio is increased in diabetic patients with coronary artery disease. Atherosclerosis 2016, 245, 12–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, N.; Xie, S.; Li, J.; Tian, R.; Peng, Y.Y. Myeloperoxidase-mediated oxidation targets serum apolipoprotein A-I in diabetic patients and represents a potential mechanism leading to impaired anti-apoptotic activity of high density lipoprotein. Clin. Chim. Acta 2015, 441, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Shao, B.; Pennathur, S.; Heinecke, J.W. Myeloperoxidase targets apolipoprotein A-I, the major high density lipoprotein protein, for site-specific oxidation in human atherosclerotic lesions. J. Biol. Chem. 2012, 287, 6375–6386. [Google Scholar] [CrossRef] [Green Version]
- Zheng, L.; Settle, M.; Brubaker, G.; Schmitt, D.; Hazen, S.L.; Smith, J.D.; Kinter, M. Localization of nitration and chlorination sites on apolipoprotein A-I catalyzed by myeloperoxidase in human atheroma and associated oxidative impairment in ABCA1-dependent cholesterol efflux from macrophages. J. Biol. Chem. 2005, 280, 38–47. [Google Scholar] [CrossRef] [Green Version]
- DiDonato, J.A.; Aulak, K.; Huang, Y.; Wagner, M.; Gerstenecker, G.; Topbas, C.; Gogonea, V.; DiDonato, A.J.; Tang, W.H.W.; Mehl, R.A.; et al. Site-specific nitration of apolipoprotein A-I at tyrosine 166 is both abundant within human atherosclerotic plaque and dysfunctional. J. Biol. Chem. 2014, 289, 10276–10292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shao, B.; Heinecke, J.W. Impact of HDL oxidation by the myeloperoxidase system on sterol efflux by the ABCA1 pathway. J. Proteom. 2011, 74, 2289–2299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panasenko, O.M.; Briviba, K.; Klotz, L.O.; Sies, H. Oxidative modification and nitration of human low-density lipoproteins by the reaction of hypochlorous acid with nitrite. Arch. Biochem. Biophys. 1997, 343, 254–259. [Google Scholar] [CrossRef] [PubMed]
- Adedayo, A.; Eluwole, A.; Tedla, F.; Kremer, A.; Mastrogiovanni, N.; Khan, M.; Rosenberg, C.; Dreizen, P.; La Rosa, J.; Salciccioli, L.; et al. Association between nitrated lipoproteins and vascular function in type 2 diabetes. Front. Biosci. (Landmark Ed.) 2021, 26, 644–663. [Google Scholar] [CrossRef] [PubMed]
- Mathew, A.V.; Li, L.; Byun, J.; Guo, Y.; Michailidis, G.; Jaiswal, M.; Chen, Y.E.; Pop-Busui, R.; Pennathur, S. Therapeutic lifestyle changes improve HDL function by inhibiting myeloperoxidase-mediated oxidation in patients with metabolic syndrome. Diabetes Care 2018, 41, 2431–2437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mayyas, F.; Baydoun, D.; Ibdah, R.; Ibrahim, K. Atorvastatin reduces plasma inflammatory and oxidant biomarkers in patients with risk of atherosclerotic cardiovascular disease. J. Cardiovasc. Pharmacol. Ther. 2018, 23, 216–225. [Google Scholar] [CrossRef]
- Sexton, T.R.; Wallace, E.L.; Macaulay, T.E.; Charnigo, R.J.; Evangelista, V.; Campbell, C.L.; Bailey, A.L.; Smyth, S.S. The effect of rosuvastatin on thromboinflammation in the setting of acute coronary syndrome. J. Thromb. Thrombolysis 2015, 39, 186–195. [Google Scholar] [CrossRef] [Green Version]
- Ndrepepa, G.; Braun, S.; Schömig, A.; Kastrati, A. Impact of therapy with statins, beta-blockers and angiotensin-converting enzyme inhibitors on plasma myeloperoxidase in patients with coronary artery disease. Clin. Res. Cardiol. 2011, 100, 327–333. [Google Scholar] [CrossRef]
- Khou, V.; De La Mata, N.L.; Kelly, P.J.; Masson, P.; O’Lone, E.; Morton, R.L.; Webster, A.C. Epidemiology of cardiovascular death in kidney failure: An Australian and New Zealand cohort study using data linkage. Nephrology 2022, 27, 430–440, online ahead of print. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| In a study on rats, it was shown that hyperinsulinemia induced by intravenous glucose administration inhibited the hepatic secretion of VLDL molecules (the reduction in TG secretion was 30% and the reduction in apolipoprotein B (apoB) secretion was 66%) [14]. |
| In a study performed on hepatocytes derived from mice, the suppressive effect of insulin on VLDL secretion was not dependent on LDL-receptor function [15]. |
| In Zucker diabetic fatty rats, increased TG production over the course of hyperinsulinemia was shown to be related to the increased expression of sterol regulatory element-binding protein 1c (SREBP-1c), whereas increased apoB production involved posttranscriptional processes [16]. |
| In an IR model of fructose-fed hamsters, the activity of phosphatidylinositol 3-kinase was shown to be significantly reduced, as well as the activity of protein-tyrosine phosphatase-1B (PTP-1B) being significantly higher, in the hepatocytes of these animals. Interestingly, the increase in PTP-1B was associated with the marked suppression of a cysteine protease (ER-60) playing a role in intracellular apoB degradation [17]. |
| The activity of microsomal triglyceride transfer protein (MTP) was shown to be significantly increased in an animal model of T2DM [18] and in studies performed on hepatocytes [19,20]. The MAPK pathway was shown to participate in the insulin-mediated inhibition of MTP synthesis [20]. Moreover, increased transcription factor forkhead box O1 (FoxO1) and decreased transcription factor forkhead box A2 (Foxa2) activity may participate in the regulation of VLDL excretion mediated by insulin [21,22]. |
| 3-nitrotyrosine overexpression has been shown to be associated with endothelial dysfunction [46,47,48,49,50]. |
| The 3-nitrotyrosine content in the arterial wall is higher in patients with worse cardiovascular system conditions [51,52,53,54]. |
| Certain drugs used in the treatment of diabetes mellitus and CVDs can reduce the expression of 3-nitrotyrosine [55,60,61,62,63,65]. |
| Most of the studies cited indicate that the expression of 3-nitrotyrosine generally tends to increase with the presence of cardiovascular risk factors such as age, obesity, smoking, consumption of highly processed foods, and the presence of features of metabolic syndrome [75,76,77,78,79,80,81,82,83,84,85,86]. |
| There are currently no unambiguous data that would allow the use of the determination of the level of 3-nitrotyrosine in the diagnosis of CVDs and in the assessment of prognosis [87,88,89,90,91,92,93,94]. |
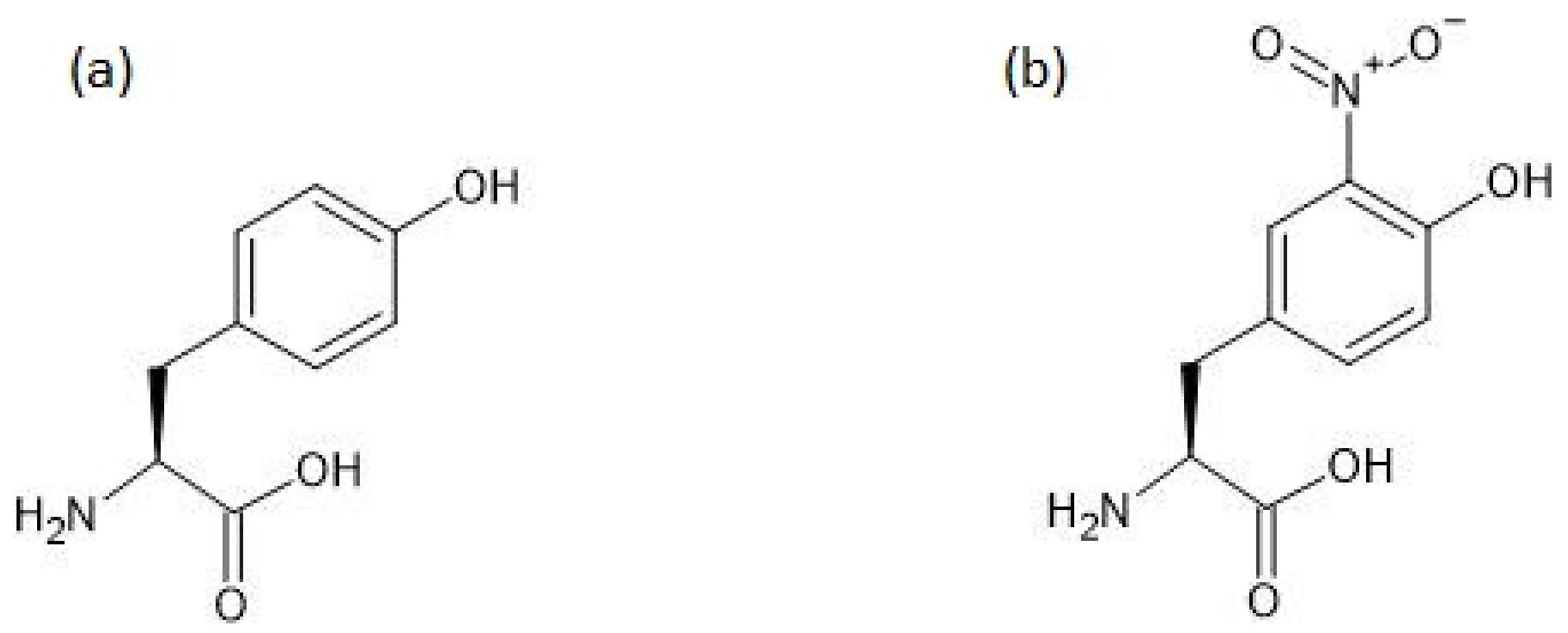
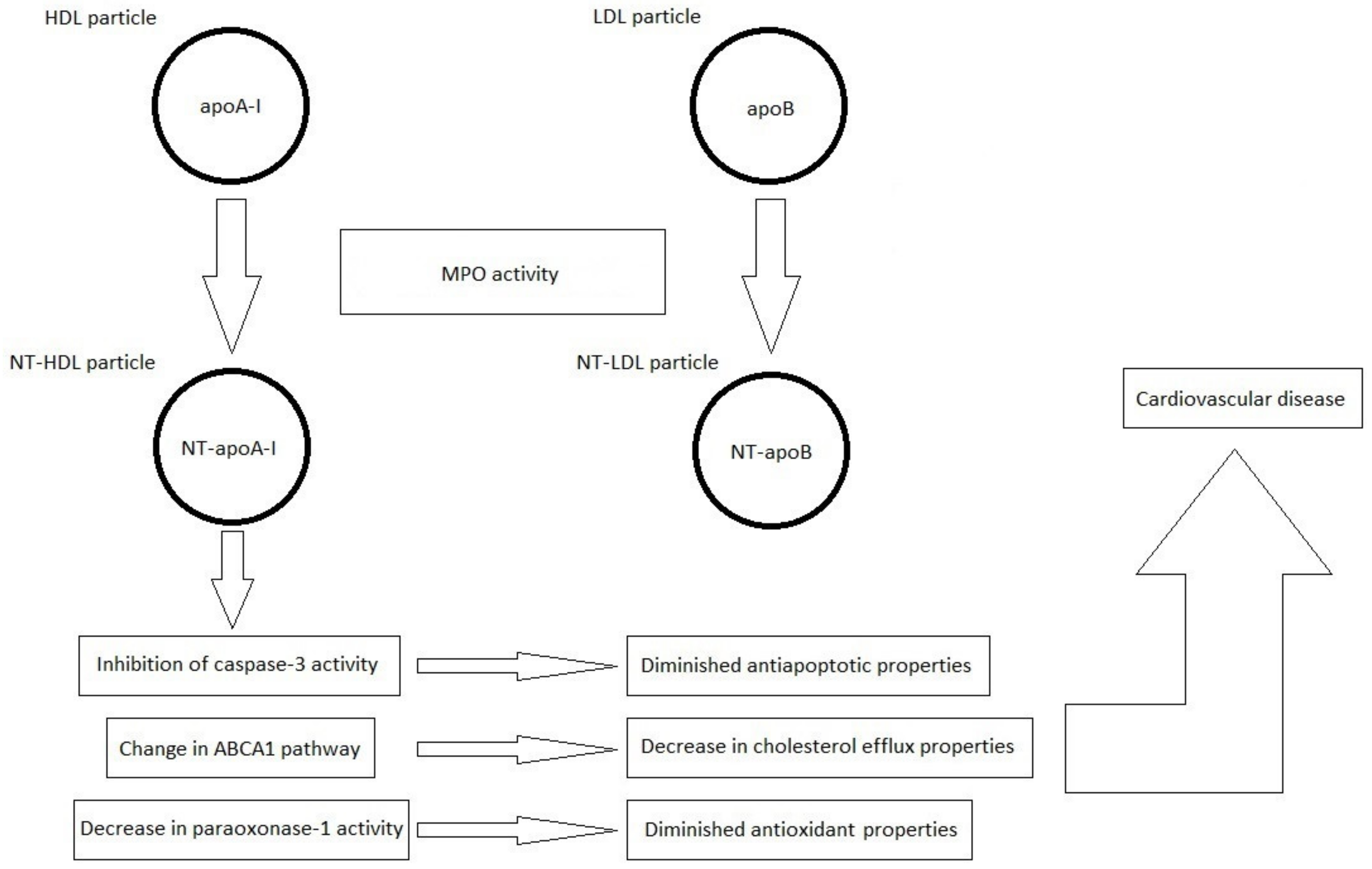
| The nitrated lipoproteins NT-HDL and NT-LDL result from the nitration of tyrosyl residues in the polypeptide chain of apoA-I and apoB, respectively [97]. |
| Lipoprotein nitration is influenced by the catalytic activity of myeloperoxidase, which is suspected to be increased in patients with DM, although this is not unambiguous [98,99,100,101,102,103]. |
| Currently, more information on nitrated HDL particles than on nitrated LDL particles is available in the literature. |
| The nitration of HDL molecules is associated with a decreased activity of paraoxonase-1 and caspase-3 [105,108], and also influences the transport of cholesterol via ABCA1 [112]. |
| The mechanisms mentioned above are associated with a reduction in the antioxidant and antiapoptotic properties of HDL particles and a reduction in the ability to transport cholesterol. Therefore, nitrated HDL particles have weaker antiatherogenic properties than native HDL particles [105,108,112]. |
| Research Question |
|---|
| Is there a relationship between the concentration of nitrated lipoproteins and parameters of glycemic control in patients with diabetes? |
| Is there a relationship between the concentration of nitrated lipoproteins and the systemic parameters of oxidative stress in patients with diabetes? |
| Is there a relationship between the concentration of nitrated lipoproteins and the characteristics of myocardial systolic and/or diastolic dysfunction in patients with diabetes? |
| Is there a relationship between the concentration of nitrated lipoproteins and the characteristics of subclinical dysfunction of the cardiovascular system measured with parameters such as flow-mediated dilation, intima–media thickness, pulse-wave velocity, ankle-brachial index, and toe-brachial index in patients with diabetes? |
| Is there a relationship between the concentration of nitrated lipoproteins and anthropometric parameters (body mass index, waist circumference, waist–hip ratio, and body composition analysis results) in patients with diabetes? |
| Can the concentration of nitrated lipoproteins be a useful marker of the risk of developing CVD and the risk of cardiovascular events in a prospective observation, and is the concentration of nitrated lipoproteins in this range a parameter independent of the concentration of nitrotyrosine and myeloperoxidase activity? |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jakubiak, G.K.; Cieślar, G.; Stanek, A. Nitrotyrosine, Nitrated Lipoproteins, and Cardiovascular Dysfunction in Patients with Type 2 Diabetes: What Do We Know and What Remains to Be Explained? Antioxidants 2022, 11, 856. https://doi.org/10.3390/antiox11050856
Jakubiak GK, Cieślar G, Stanek A. Nitrotyrosine, Nitrated Lipoproteins, and Cardiovascular Dysfunction in Patients with Type 2 Diabetes: What Do We Know and What Remains to Be Explained? Antioxidants. 2022; 11(5):856. https://doi.org/10.3390/antiox11050856
Chicago/Turabian StyleJakubiak, Grzegorz K., Grzegorz Cieślar, and Agata Stanek. 2022. "Nitrotyrosine, Nitrated Lipoproteins, and Cardiovascular Dysfunction in Patients with Type 2 Diabetes: What Do We Know and What Remains to Be Explained?" Antioxidants 11, no. 5: 856. https://doi.org/10.3390/antiox11050856