
Oxidative Status in Adult Anorexia Nervosa Patients and Healthy Controls—Results from a Cross-Sectional Pilot Study

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Blood Sampling
2.3. Oxidative Stress Biomarkers
2.4. Psychological and Dietary Scales
2.5. Statistical Analyses
3. Results
3.1. Group Characteristics
3.2. Psychological Evaluation and Questionnaires
3.3. Oxidative Stress Biomarkers
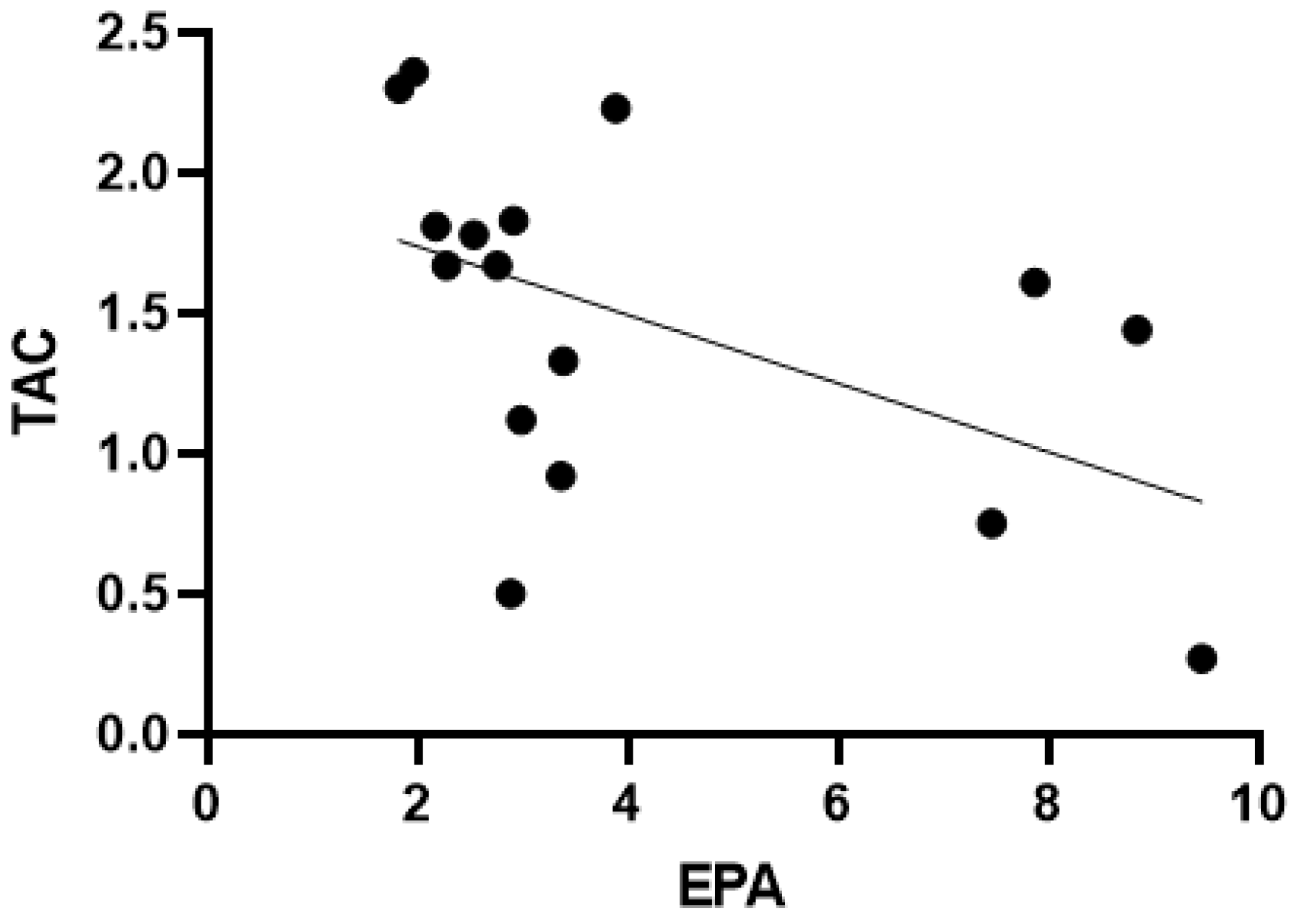
3.4. Correlations
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Herpertz, S.; Fichter, M.; Herpertz-Dahlmann, B.; Hilbert, A.; Tuschen-Caffier, B.; Vocks, S.; Zeeck, A. S3-Leitlinie Diagnostik Und Behandlung Der Essstörungen; Springer: Berlin/Heidelberg, Germany, 2011. [Google Scholar]
- Löwe, B.; Zipfel, S.; Buchholz, C.; Dupont, Y.; Reas, D.; Herzog, W. Long-term outcome of anorexia nervosa in a prospective 21-year follow-up study. Psychol. Med. 2001, 31, 881–890. [Google Scholar] [CrossRef] [Green Version]
- Gibson, D.; Workman, C.; Mehler, P.S. Medical complications of anorexia nervosa and bulimia nervosa. Psychiatr. Clin. 2019, 42, 263–274. [Google Scholar] [CrossRef] [PubMed]
- Heilbronn, L.K.; Milner, K.-L.; Kriketos, A.; Russell, J.; Campbell, L.V. Metabolic dysfunction in anorexia nervosa. Obes. Res. Clin. Pract. 2007, 1, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Zenger, F.; Russmann, S.; Junker, E.; Wüthrich, C.; Bui, M.; Lauterburg, B. Decreased glutathione in patients with anorexia nervosa. Risk factor for toxic liver injury? Eur. J. Clin. Nutr. 2004, 58, 238–243. [Google Scholar] [CrossRef]
- Lackner, S.; Mörkl, S.; Müller, W.; Fürhapter-Rieger, A.; Oberascher, A.; Lehofer, M.; Bieberger, C.; Wonisch, W.; Amouzadeh-Ghadikolai, O.; Moser, M. Novel approaches for the assessment of relative body weight and body fat in diagnosis and treatment of anorexia nervosa: A cross-sectional study. Clin. Nutr. 2019, 38, 2913–2921. [Google Scholar] [CrossRef] [Green Version]
- Berg, D.; Youdim, M.B.; Riederer, P. Redox imbalance. Cell Tissue Res. 2004, 318, 201–213. [Google Scholar] [CrossRef]
- Valko, M.; Leibfritz, D.; Moncol, J.; Cronin, M.T.; Mazur, M.; Telser, J. Free radicals and antioxidants in normal physiological functions and human disease. Int. J. Biochem. Cell Biol. 2007, 39, 44–84. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Vadodaria, K.C.; Lenkei, Z.; Kato, T.; Gage, F.H.; Marchetto, M.C.; Santos, R. Mitochondria, metabolism, and redox mechanisms in psychiatric disorders. Antioxid. Redox Signal. 2019, 31, 275–317. [Google Scholar] [CrossRef] [PubMed]
- Leonard, B.E. Inflammation as the cause of the metabolic syndrome in depression. Mod. Trends Pharm. 2013, 28, 117–126. [Google Scholar] [CrossRef]
- Zelzer, S.; Tatzber, F.; Herrmann, M.; Wonisch, W.; Rinnerhofer, S.; Kundi, M.; Obermayer-Pietsch, B.; Niedrist, T.; Cvirn, G.; Wultsch, G.; et al. Work Intensity, Low-Grade Inflammation, and Oxidative Status: A Comparison between Office and Slaughterhouse Workers. Oxidative Med. Cell. Longev. 2018, 2018, 2737563. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winklhofer-Roob, B.M.; Faustmann, G.; Roob, J.M. Low-density lipoprotein oxidation biomarkers in human health and disease and effects of bioactive compounds. Free. Radic. Biol. Med. 2017, 111, 38–86. [Google Scholar] [CrossRef] [PubMed]
- Breusing, N.; Grune, T.; Andrisic, L.; Atalay, M.; Bartosz, G.; Biasi, F.; Borovic, S.; Bravo, L.; Casals, I.; Casillas, R. An inter-laboratory validation of methods of lipid peroxidation measurement in UVA-treated human plasma samples. Free. Radic. Res. 2010, 44, 1203–1215. [Google Scholar] [CrossRef] [PubMed]
- Górska, P.; Górna, I.; Przysławski, J. Mediterranean diet and oxidative stress. Nutr. Food Sci. 2020, 51, 1–9. [Google Scholar] [CrossRef]
- Mazzocchi, A.; Leone, L.; Agostoni, C.; Pali-Schöll, I. The Secrets of the Mediterranean Diet. Does [Only] Olive Oil Matter? Nutrients 2019, 11, 2941. [Google Scholar] [CrossRef] [Green Version]
- Lindschinger, M.; Tatzber, F.; Schimetta, W.; Schmid, I.; Lindschinger, B.; Cvirn, G.; Stanger, O.; Lamont, E.; Wonisch, W. A randomized pilot trial to evaluate the bioavailability of natural versus synthetic vitamin B complexes in healthy humans and their effects on homocysteine, oxidative stress and antioxidant levels. Oxidative Med. Cell. Longev. 2019, 2019, 6082613. [Google Scholar] [CrossRef] [Green Version]
- Resch, U.; Helsel, G.; Tatzber, F.; Sinzinger, H. Antioxidant status in thyroid dysfunction. Clin. Chem. Lab. Med. 2002, 40, 1132–1134. [Google Scholar] [CrossRef]
- Tatzber, F.; Griebenow, S.; Wonisch, W.; Winkler, R. Dual method for the determination of peroxidase activity and total peroxides-iodide leads to a significant increase of peroxidase activity in human sera. Anal. Biochem. 2003, 316, 147–153. [Google Scholar] [CrossRef]
- Charach, G.; Rabinovich, A.; Argov, O.; Weintraub, M.; Charach, L.; Ayzenberg, O.; George, J. Anti-oxidized low-density lipoprotein antibodies in chronic heart failure. World J. Cardiol. 2012, 4, 302. [Google Scholar] [CrossRef]
- Randrianarisoa, E.; Lehn-Stefan, A.; Wang, X.; Hoene, M.; Peter, A.; Heinzmann, S.S.; Zhao, X.; Königsrainer, I.; Königsrainer, A.; Balletshofer, B.; et al. Relationship of Serum Trimethylamine N-Oxide (TMAO) Levels with early Atherosclerosis in Humans. Sci Rep. 2016, 6, 26745. [Google Scholar] [CrossRef] [Green Version]
- Wonisch, W.; Falk, A.; Sundl, I.; Winklhofer-Roob, B.M.; Lindschinger, M. Oxidative stress increases continuously with BMI and age with unfavourable profiles in males. Aging Male 2012, 15, 159–165. [Google Scholar] [CrossRef]
- Tatzber, F.; Wonisch, W.; Lackner, S.; Lindschinger, M.; Pursch, W.; Resch, U.; Trummer, C.; Murkovic, M.; Zelzer, S.; Holasek, S. A Micromethod for Polyphenol High-Throughput Screening Saves 90 Percent Reagents and Sample Volume. Antioxidants 2020, 9, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Enko, D.; Zelzer, S.; Baranyi, A.; Herrmann, M.; Meinitzer, A. Determination of Trimethylamine-N-oxide by a Simple Isocratic High-Throughput Liquid-Chromatography Tandem Mass-Spectrometry Method. Clin. Lab. 2020, 66. [Google Scholar] [CrossRef]
- Hilbert, A.; Tuschen-Caffier, B.; Ohms, M. Eating disorder examination: Deutschsprachige Version des strukturierten Essstörungsinterviews. Diagnostica 2004, 50, 98–106. [Google Scholar] [CrossRef]
- Yu, J.; Lu, M.; Tian, L.; Lu, W.; Meng, F.; Chen, C.; Tang, T.; He, L.; Yao, Y. Prevalence of disordered eating attitudes among university students in wuhu, china. Nutr. Hosp. 2015, 32, 1753. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatric Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An inventory for measuring depression. Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamilton, M. A rating scale for depression. J. Neurol Neurosurg Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean diet and survival in a Greek population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef] [Green Version]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Xu, D.; Zhao, W.; Song, J.; Yin, L.; Wang, K.; Wei, L.; Xu, Y.; Li, H.; Min, B.; Tang, N. The Relationship of Large-Artery Atherothrombotic Stroke with Plasma Trimethylamine N-Oxide Level and Blood Lipid-Related Indices: A Cross-Sectional Comparative Study. BioMed Res. Int. 2021, 2021, 5549796. [Google Scholar] [CrossRef]
- Oliveras-Lopez, M.J.; Ruiz-Prieto, I.; Bolanos-Rios, P.; De la Cerda, F.; Martin, F.; Jauregui-Lobera, I. Antioxidant activity and nutritional status in anorexia nervosa: Effects of weight recovery. Nutrients 2015, 7, 2193–2204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kovalčíková, A.G.; Tichá, Ľ.; Šebeková, K.; Celec, P.; Čagalová, A.; Sogutlu, F.; Podracká, Ľ. Oxidative status in plasma, urine and saliva of girls with anorexia nervosa and healthy controls: A cross-sectional study. J. Eat. Disord. 2021, 9, 54. [Google Scholar] [CrossRef]
- Lackner, S.; Meier-Allard, N.; Mörkl, S.; Müller, W.; Fürhapter-Rieger, A.; Mangge, H.; Zelzer, S.; Holasek, S. Hypercarotenemia in Anorexia Nervosa Patients May Influence Weight Balance: Results of a Clinical Cross-Sectional Cohort Study. Front. Psychiatry 2021, 12, 758300. [Google Scholar] [CrossRef]
- Prohan, M.; Amani, R.; Nematpour, S.; Jomehzadeh, N.; Haghighizadeh, M.H. Total antioxidant capacity of diet and serum, dietary antioxidant vitamins intake, and serum hs-CRP levels in relation to depression scales in university male students. Redox Rep. 2014, 19, 133–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cumurcu, B.E.; Ozyurt, H.; Etikan, I.; Demir, S.; Karlidag, R. Total antioxidant capacity and total oxidant status in patients with major depression: Impact of antidepressant treatment. Psychiatry Clin. Neurosci. 2009, 63, 640–644. [Google Scholar] [CrossRef] [PubMed]
- Pilch, W.; Wyrostek, J.; Piotrowska, A.; Czerwińska-Ledwig, O.; Zuziak, R.; Sadowska-Krępa, E.; Maciejczyk, M.; Żychowska, M. Blood pro-oxidant/antioxidant balance in young men with class II obesity after 20 sessions of whole body cryostimulation: A preliminary study. Redox. Rep. 2021, 26, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Pilch, W.; Tota, Ł.; Piotrowska, A.; Śliwicka, E.; Czerwińska-Ledwig, O.; Zuziak, R.; Pilaczyńska-Szcześniak, Ł. Effects of Nordic Walking on Oxidant and Antioxidant Status: Levels of Calcidiol and Proinflammatory Cytokines in Middle-Aged Women. Oxidative Med. Cell. Longev. 2018, 2018, 6468234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rowicka, G.; Dylag, H.; Ambroszkiewicz, J.; Riahi, A.; Weker, H.; Chelchowska, M. Total Oxidant and Antioxidant Status in Prepubertal Children with Obesity. Oxid. Med. Cell Longev. 2017, 2017, 5621989. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mörkl, S.; Lackner, S.; Müller, W.; Gorkiewicz, G.; Kashofer, K.; Oberascher, A.; Painold, A.; Holl, A.; Holzer, P.; Meinitzer, A.; et al. Gut microbiota and body composition in anorexia nervosa inpatients in comparison to athletes, overweight, obese, and normal weight controls. Int. J. Eat. Disord. 2017, 50, 1421–1431. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, Z.M.; Phillipou, A.; Castle, D.J.; Eikelis, N.; Lambert, E.A. Arterial stiffness in underweight and weight-restored anorexia nervosa. Psychophysiology 2021, 58, e13913. [Google Scholar] [CrossRef] [PubMed]
- Tonhajzerova, I.; Mestanikova, A.; Jurko, A., Jr.; Grendar, M.; Langer, P.; Ondrejka, I.; Jurko, T.; Hrtanek, I.; Cesnekova, D.; Mestanik, M. Arterial stiffness and haemodynamic regulation in adolescent anorexia nervosa versus obesity. Appl. Physiol. Nutr. Metab. 2020, 45, 81–90. [Google Scholar] [CrossRef]
- Cinelli, G.; Criscuolo, M.; Bifone, C.; Chianello, I.; Castiglioni, M.C.; De Lorenzo, A.; Di Renzo, L.; Tozzi, A.E.; Vicari, S.; Zanna, V. Food Addiction in a Group of Italian Adolescents Diagnosed for Eating Disorder. Nutrients 2020, 12, 1524. [Google Scholar] [CrossRef]
- Fazeli, P.K.; Lawson, E.A.; Faje, A.T.; Eddy, K.T.; Lee, H.; Fiedorek, F.T.; Breggia, A.; Gaal, I.M.; DeSanti, R.; Klibanski, A. Treatment with a Ghrelin Agonist in Outpatient Women with Anorexia Nervosa: A Randomized Clinical Trial. J. Clin. Psychiatry 2018, 79, 7823. [Google Scholar] [CrossRef]
- Treasure, J.; Duarte, T.A.; Schmidt, U. Eating disorders. Lancet 2020, 395, 899–911. [Google Scholar] [CrossRef]
- Ribaudo, G.; Bortoli, M.; Pavan, C.; Zagotto, G.; Orian, L. Antioxidant Potential of Psychotropic Drugs: From Clinical Evidence to In Vitro and In Vivo Assessment and toward a New Challenge for in Silico Molecular Design. Antioxidants 2020, 9, 714. [Google Scholar] [CrossRef] [PubMed]
- Marvanova, M.; Gramith, K. Role of antidepressants in the treatment of adults with anorexia nervosa. Ment. Health Clin. 2018, 8, 127–137. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| AN M (SD)/M (Min; Max; IQR) | HC M (SD)/M (Min; Max; IQR) | p-Value | |
|---|---|---|---|
| Height [m] | 1.64 (0.06) | 1.68 (0.07) | 0.007 |
| Weight [kg] | 37.03 (6.78) | 64.32 (12.79) | <0.001 |
| BMI [kg/m2] | 13.71 (1.97) | 22.23 (3.37) | <0.001 |
| Age [years] | 23 (18; 54; 20–30) | 26 (22.00; 27; 25–30.75) | 0.136 |
| Name of Questionnaire | AN M (SD)/M (Min; Max; IQR) | HC M (SD)/M (Min; Max; IQR) | p-Value |
|---|---|---|---|
| EDEQ shape concern | 4.03 (1.43) | 0.69 (0.66) | <0.001 |
| EDEQ total | 3.1 (0.76; 5.7; 1.54–4.47) | 0.37 (0; 57; 0.23–0.71) | <0.001 |
| EDEQ restraint | 3.4 (0; 6; 0.25–4.95) | 0.3 (0; 22; 0–0.85) | <0.001 |
| EDEQ eating concern | 4 (0; 5.2; 1.3–4.4) | 0 (0; 1.2; 0–0.2) | <0.001 |
| EDEQ weight concern | 2.7 (1.6; 6; 2.2–4) | 2 (0; 2.2; 0–1) | <0.001 |
| EAT-26 | 26 (6; 51; 18.75–36.75) | 2 (0; 8; 0–5.5) | <0.001 |
| MDS | 7 (2; 11; 3.75–9) | 8 (5; 12; 7–9) | 0.266 |
| HAMD | 18 (4; 31; 11–18) | 1 (0; 8; 0–1) | <0.001 |
| BDI | 25.5 (1; 44; 13.5–33.5) | 1 (0; 17; 0–1) | 0.001 |
| Ox Stress Parameters | AN M (SD)/M (Min; Max; IQR) | HC M (SD)/M (Min; Max; IQR) | p-Value |
|---|---|---|---|
| TAC [mmol/L] | 1.47 (0.62) | 1.91 (0.56) | 0.036 |
| Ppm [mmol/L] | 7.79 (0.52) | 7.7 (0.34) | 0.476 |
| TOC [µmol/L] | 138 (23; 355; 96–171) | 144 (85; 573; 131–204.5) | 0.427 |
| oLAb [mU/mL] | 513 (185; 6000; 185–2729.5) | 513 (185; 6000; 366.5–1811.5) | 0.408 |
| EPA [U/L] | 2.98 (1.82; 10.42; 2.40–7.67) | 3.07 (1.11; 12.92; 2.55–7.53) | 0.547 |
| TMAO [µmol/L] | 2.16 (1.01) | 2.14 (1.05) | 0.949 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wagner-Skacel, J.; Haidacher, F.; Wiener, M.; Pahsini, K.; Marinschek, S.; Lahousen, T.; Wonisch, W.; Bengesser, S.; Butler, M.I.; Lackner, S.; et al. Oxidative Status in Adult Anorexia Nervosa Patients and Healthy Controls—Results from a Cross-Sectional Pilot Study. Antioxidants 2022, 11, 842. https://doi.org/10.3390/antiox11050842
Wagner-Skacel J, Haidacher F, Wiener M, Pahsini K, Marinschek S, Lahousen T, Wonisch W, Bengesser S, Butler MI, Lackner S, et al. Oxidative Status in Adult Anorexia Nervosa Patients and Healthy Controls—Results from a Cross-Sectional Pilot Study. Antioxidants. 2022; 11(5):842. https://doi.org/10.3390/antiox11050842
Chicago/Turabian StyleWagner-Skacel, Jolana, Fiona Haidacher, Markus Wiener, Karoline Pahsini, Sabine Marinschek, Theresa Lahousen, Willibald Wonisch, Susanne Bengesser, Mary I. Butler, Sonja Lackner, and et al. 2022. "Oxidative Status in Adult Anorexia Nervosa Patients and Healthy Controls—Results from a Cross-Sectional Pilot Study" Antioxidants 11, no. 5: 842. https://doi.org/10.3390/antiox11050842