
Outpatient Oral Neuropathic Pain Management with Photobiomodulation Therapy: A Prospective Analgesic Pharmacotherapy-Paralleled Feasibility Trial

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.1.1. Patient Cohort
2.1.2. Population (P), Intervention (I), Comparison (C), and Outcome (O)—PICO
- P:
- Adult aged ≥ 18-year-old diagnosed with NP, as a result of pnBMS and OINI (V3), according to ICHD Beta 3 [9].
- I:
- λ810 nm laser-PBM or pharmacological treatment modality.
- C:
- Pharmacotherapy versus laser-PBM.
- O:
- Patient-self-reported pain, physical and psychological functionality, QoL, any reported adverse effects and treatment compliance.
2.1.3. Overall Inclusion and Exclusion Criteria for Both Groups (PBM and MED)
Inclusion Criteria
- Subjects of both genders aged ≥ 18 years old with ongoing NP diagnosed according to the ICHD Beta 3 [9].
- Subjects who were diagnosed with oral iatrogenic neuropathy (OIN) (inferior alveolar nerve or lingual or mental nerve after any dental interventions (mandibular third molar surgery or dental implant intervention).
- Subjects who were diagnosed with pnBMS according to the ICHD Beta 3 BMS (idiopathic without clinical or laboratory test abnormalities) [9].
- Subjects with symptom duration ≥ 3 months with normal appearance of intraoral mucosa.
- Subjects with no physiological or systematic conditions, contributing to the pain.
- Subjects who had never had phototherapy prior to study enrolment.
- Subjects volunteering to enrol to either: MED or PBM group based on their wish.
- Subjects willing to participate in the study from the recruitment process to the end of the protocol.
- Subjects with controlled systematic diseases with American Society of Anaesthesiologists (ASA) Classification I, II.
Exclusion Criteria
- Elicited pain or without pain
- Subjects with symptoms’ duration < 3 months.
- Subjects who have BMS due to other underlining conditions [secondary BMS: BMS by local factors (lfBMS), BMS by systemic factors (sfBMS)].
- Subjects on medications and whose symptoms were improving.
- Pregnant and lactating women.
- Subjects with intraoral mucosal lesions/conditions.
- Subject with the following neuropathic orofacial pain: Trigeminal neuralgia, glossopharyngeal neuralgia, temporomandibular joint dysfunction syndrome, migraine, odonatological and head and neck origin.
- Subjects with systematic diseases/or on medications induce NP.
- Subjects with neurological disorders or autoimmune disorders.
- Subjects with parafunctional habits and intra-oral trauma.
- Subjects with hyposalivation related to Sjogren syndrome (unstimulated saliva production ≤ 0.1 millilitres/minute) or any predisposing factors not related to BMS.
- Subjects who were smokers or had stopped smoking < 6 months prior to enrolling in the study.
2.1.4. Specific Inclusion Criteria for PBM Group
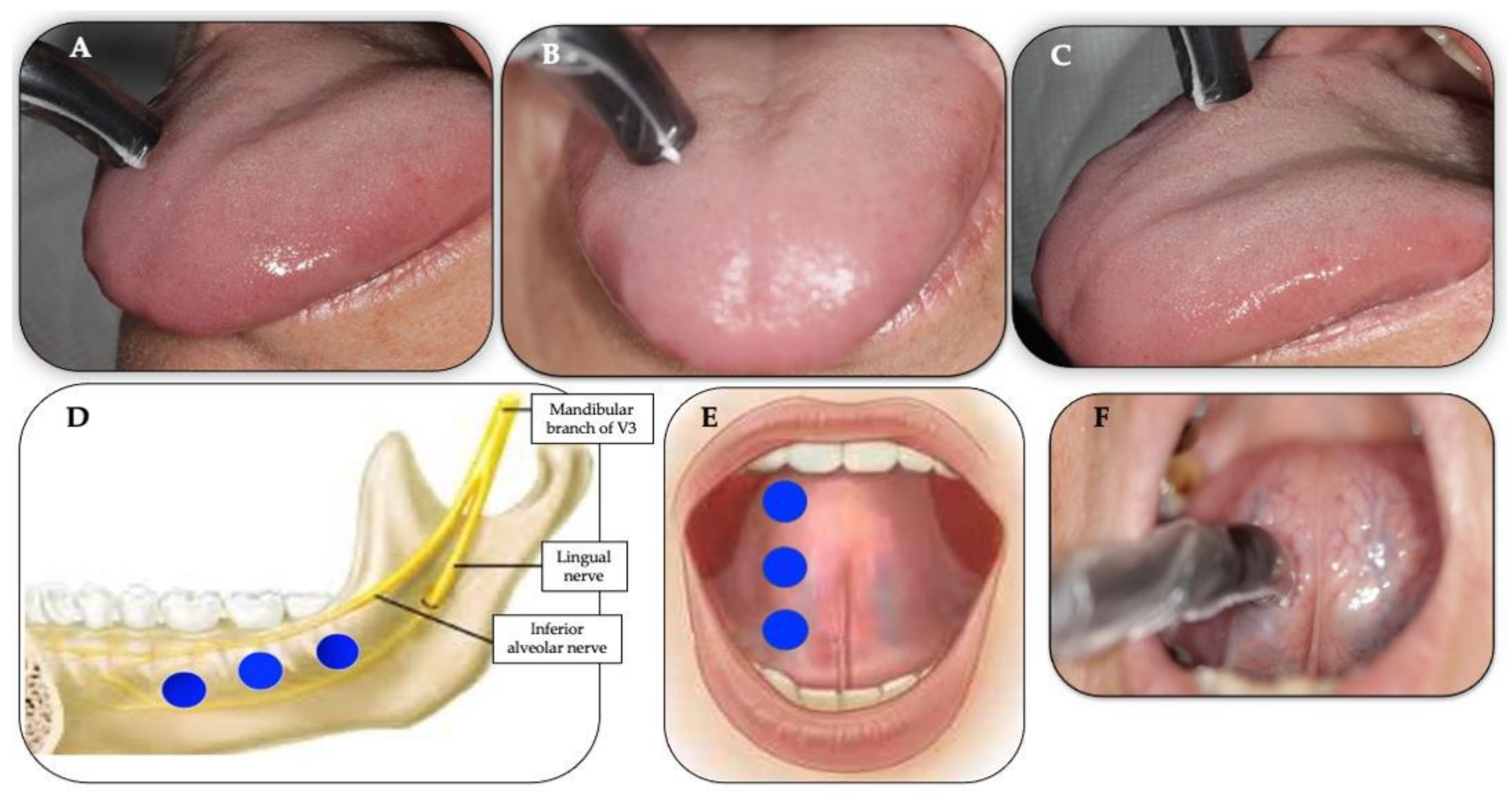
2.1.5. Treatment Protocols
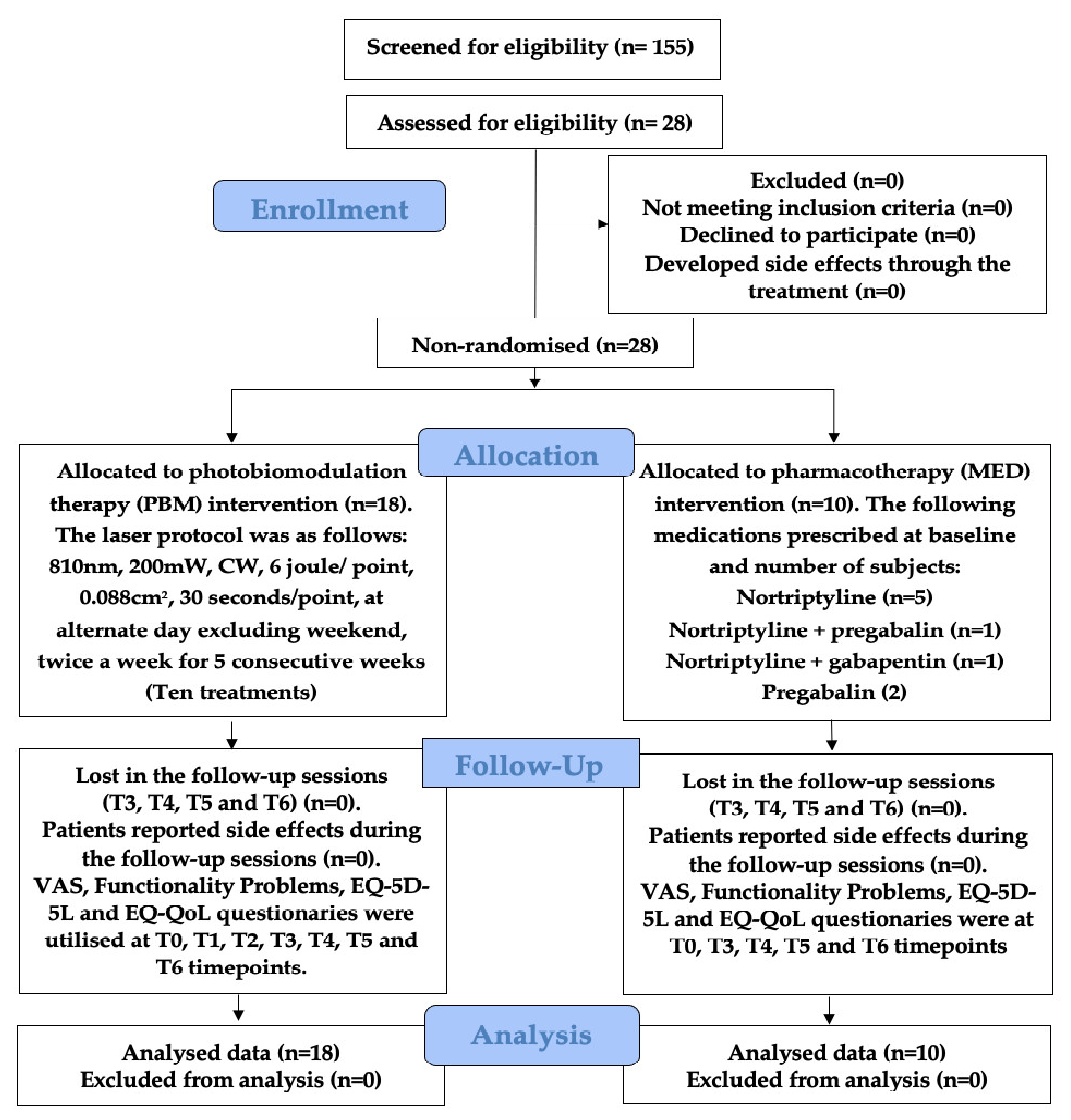
PBM Group Protocol
MED Group Protocol
2.2. Measures and Tools Used to Evaluate Outcome Variables
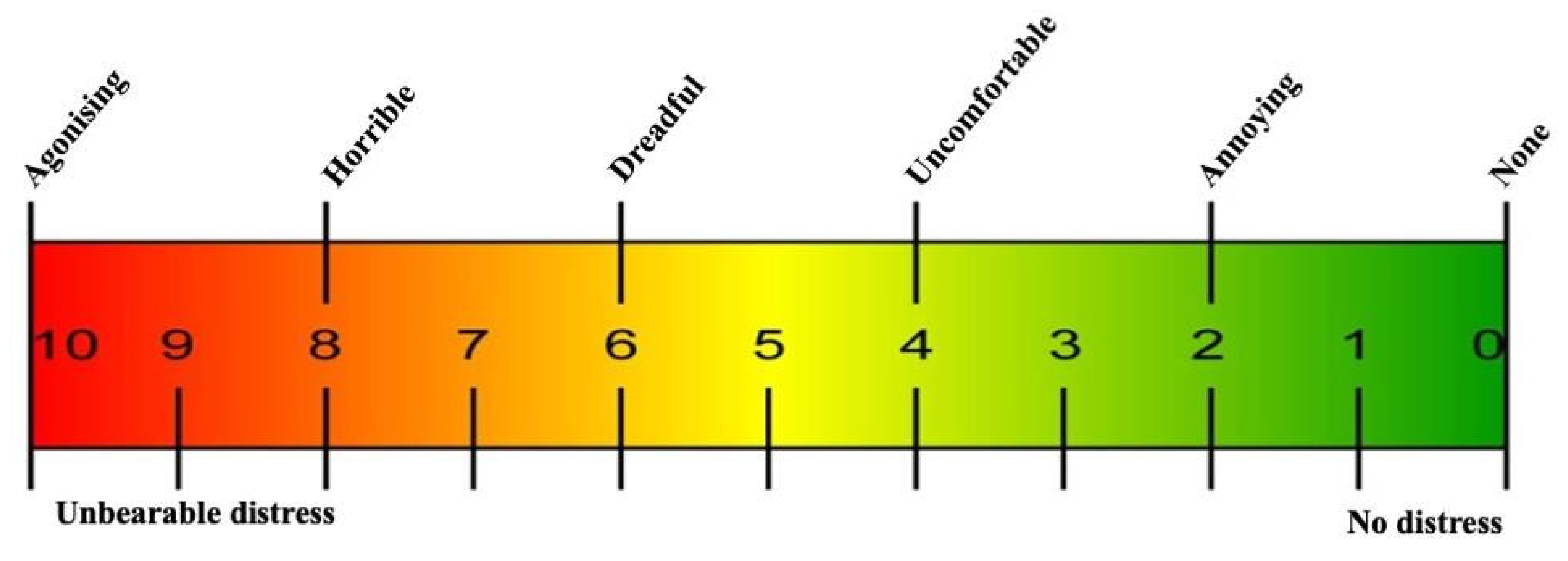
2.2.1. Pain Intensity Assessment
2.2.2. Functionality Problems Questionnaire and Scoring
2.2.3. Psychological Assessment Tool and Overall QoL
2.3. Data Analyses and Statistics
3. Results
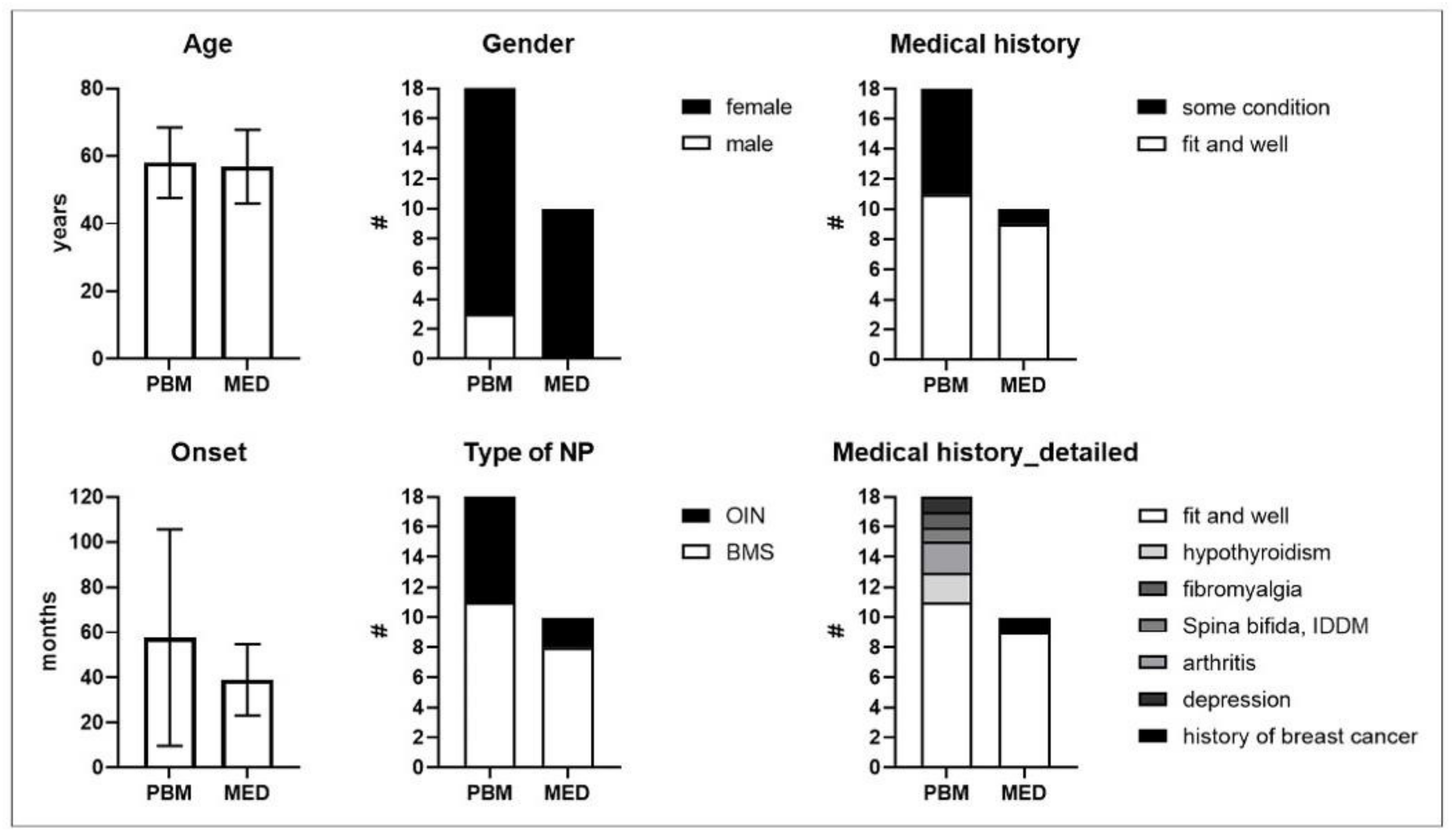
3.1. Trial Study Populations, Demographics and Baseline Characteristics
3.2. Patients’ Acceptance of Treatments
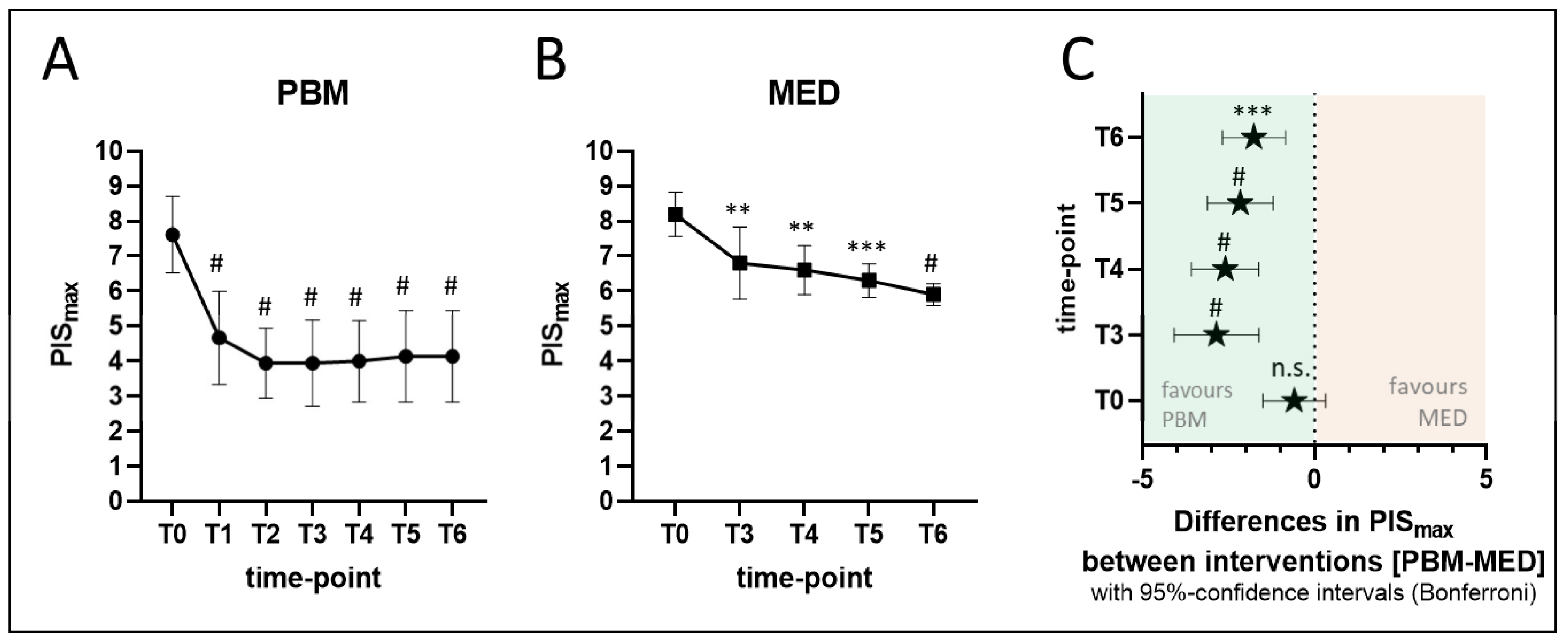
3.3. Self-Reported Maximum Pain Intensity Score (PISmax)
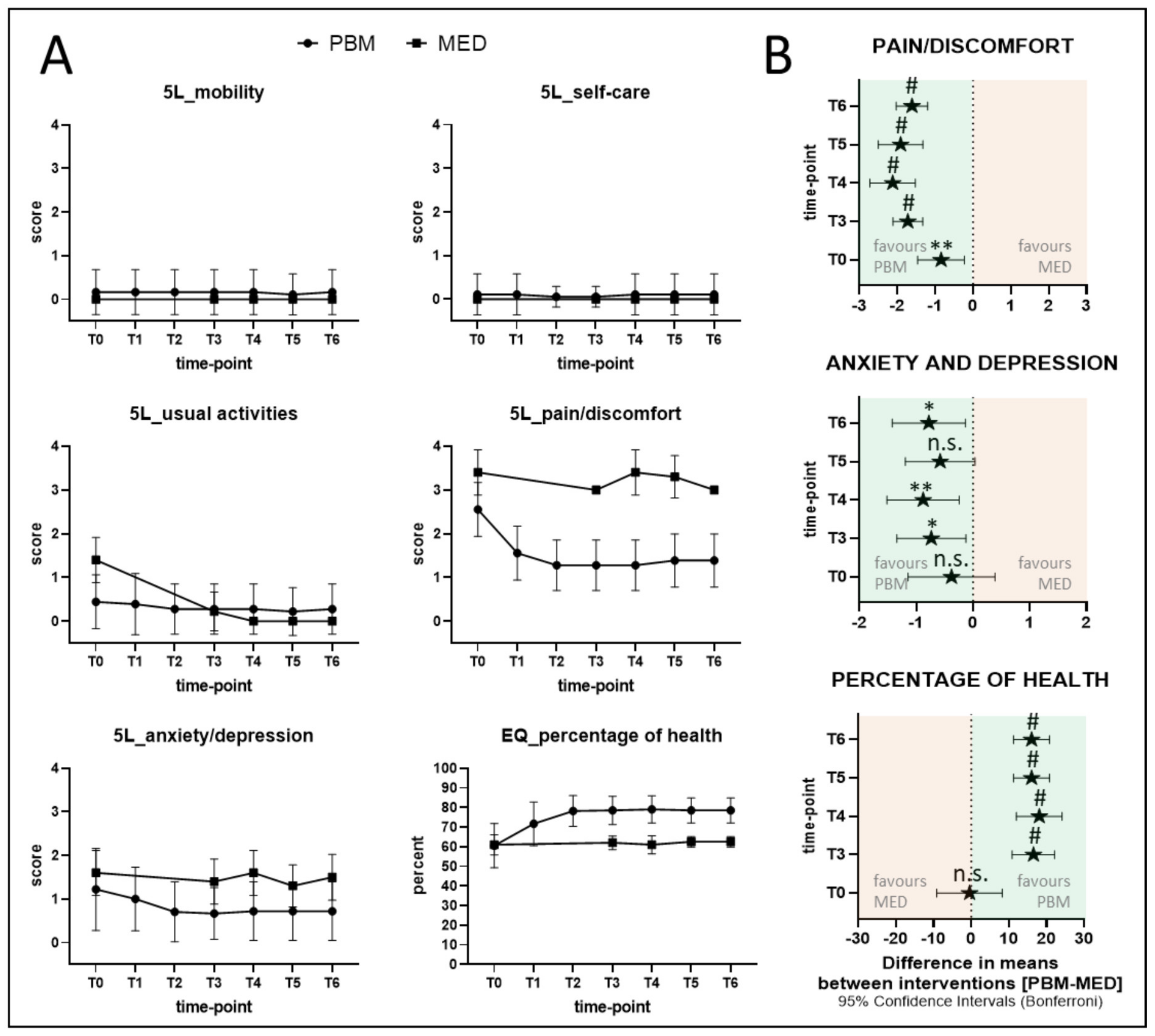
3.4. EQ-5D-5L Indices
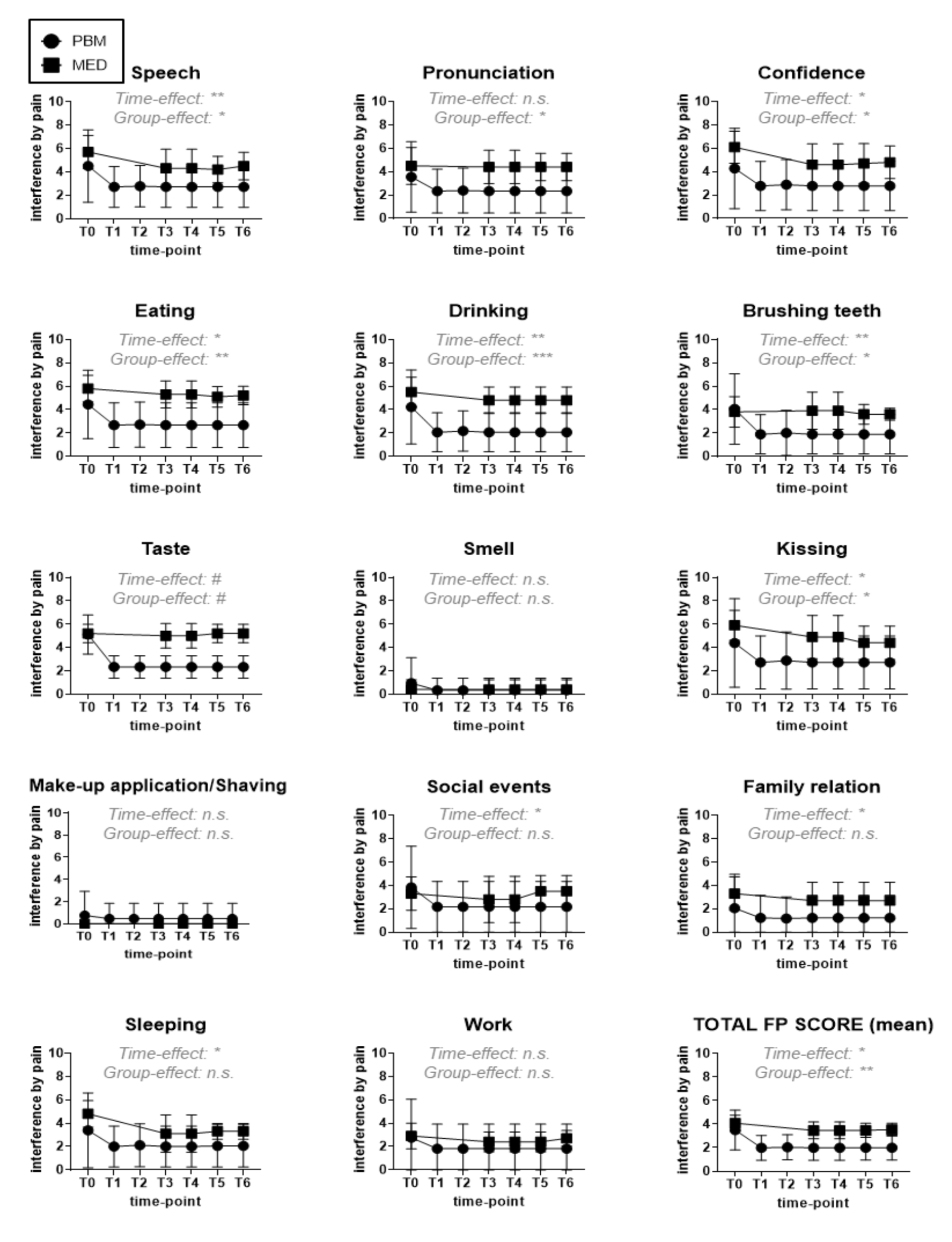
3.5. Extended QoL-Assessment-Functional Indices
4. Discussion
4.1. Demographic Characteristic of Study Cohort
4.2. Evaluation of the Study’s Laser-PBM Protocol and Its Parameters
4.3. Representation of the Study’ Outcome Measures and Their Influences to Determine PBM Efficacy
4.4. Representation of the Treatment Outcomes for Both PBM and MED Groups
4.4.1. Evaluation of the Maximum Pain Intensity Score (PISmax) Reduction
4.4.2. Evaluation of the Functional Problems’ Improvement
4.4.3. Evaluation of the Psychological Status and QoL Improvement of Both PBM and MED Groups
4.4.4. Evaluation of Subjects’ Acceptance to Treatments of Both Groups (PBM and MED) and Reported Adverse Effects
4.5. Strengths and Limitations of the Study
5. Conclusions and Future Perspective
Highlights
- Our prospective parallel study, for the first time, has demonstrated the efficacy of photobiomodulation (PBM) in modulating oral neuropathic pain (NP) intensity, improving functionality and quality of life (QoL) at mid- and end-treatment that sustained throughout all the follow-up time points (one, three, six and nine months).
- Our study, for the first time, proves that PBM; a safe, analgesic, antioxidant and pro-regenerative physical therapy, compares to or even exceeds the clinical benefits of the gold standard analgesic pharmacological approach, thus presenting itself as an up-to-date first validated, medication-free, alternative therapeutic option for the treatment of oral NP.
- Our results furthermore support additional patient’ benefits of PBM by ameliorating the QoL and functional activities which are considerably impaired because of NP, such as eating, drinking and tasting, whereas analgesic medication regimens did not.
- Our effective PBM application protocol and reliable investigational tools are relevant, easily reproducible and therefore suited for well-designed, multi-centre randomised clinical trials (RCTs), utilising large data or any other study with the aim to consolidate or optimise PBM effects on oral NP.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bennett, G.J. Neuropathic pain in the orofacial region: Clinical and research challenges. J. Orofac. Pain 2004, 18, 281–286. [Google Scholar] [PubMed]
- Jensen, T.S.; Baron, R.; Haanpää, M.; Kalso, E.; Loeser, J.D.; Rice, A.S.; Treede, R.-D. A new definition of neuropathic pain. Pain 2011, 152, 2204–2205. [Google Scholar] [CrossRef] [PubMed]
- Bouhassira, D.; Attal, N.; Alchaar, H.; Boureau, F.; Brochet, B.; Bruxelle, J.; Cunin, G.; Fermanian, J.; Ginies, P.; Grun-Overdyking, A.; et al. Comparison of pain syndromes associated with nervous or somatic lesions and development of a new neuropathic pain diagnostic questionnaire (DN4). Pain 2005, 114, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Olesen, J. Preface to the Second Edition. Cephalalgia 2004, 24, 9–10. [Google Scholar] [CrossRef]
- Agbaje, J.O.; Van De Casteele, E.; Hiel, M.; Verbaanderd, C.; Lambrichts, I.; Politis, C. Neuropathy of Trigeminal Nerve Branches After Oral and Maxillofacial Treatment. J. Maxillofac. Oral Surg. 2015, 15, 321–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merskey, H.; Bogduk, N. (Eds.) Classification of Chronic Pain: Descriptions of Chronic Pain Syndromes and Definitions of Pain Terms/Prepared by the Task Force on Taxonomy of the International Association for the Study of Pain, 2nd ed.; IASP: Seattle, WA, USA, 1994; p. 742. [Google Scholar]
- Lauria, G.; Majorana, A.; Borgna, M.; Lombardi, R.; Penza, P.; Padovani, A.; Sapelli, P. Trigeminal small-fiber sensory neuropathy causes burning mouth syndrome. Pain 2005, 115, 332–337. [Google Scholar] [CrossRef] [PubMed]
- Bartoshuk, L.M.; Grushka, M.; Duffy, V.B.; Fast, K.; Lucchina, L.; Prutkin, J. Burning mouth syndrome: Damage to CN VII and pain phantoms in CN V. Chem. Senses 1999, 24, 609. [Google Scholar]
- Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd ed. Cephalalgia 2018, 38, 1–211. [CrossRef] [PubMed]
- Bergdahl, M.; Bergdahl, J. Burning mouth syndrome: Prevalence and associated factors. J. Oral Pathol. Med. 2007, 28, 350–354. [Google Scholar] [CrossRef]
- Grushka, M.; Epstein, J.B.; Gorsky, M. Burning Mouth Syndrome and Other Oral Sensory Disorders: A Unifying Hypothesis. Pain Res. Manag. 2003, 8, 133–135. [Google Scholar] [CrossRef] [Green Version]
- Leone, C.; Biasiotta, A.; La Cesa, S.; Di Stefano, G.; Cruccu, G.; Truini, A. Pathophysiological mechanisms of neuropathic pain. Future Neurol. 2011, 6, 497–509. [Google Scholar] [CrossRef]
- Chung, H.; Dai, T.; Sharma, S.K.; Huang, Y.; Carroll, J.; Hamblin, M.R. The Nuts and Bolts of Low-level Laser (Light) Therapy. Ann. Biomed. Eng. 2011, 40, 516–533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, T.; Shi, X.Q.; Johnson, J.M.; Rone, M.B.; Antel, J.; David, S.; Zhang, J. Peripheral Nerve Injury Induces Persistent Vascular Dysfunction and Endoneurial Hypoxia, Contributing to the Genesis of Neuropathic Pain. J. Neurosci. 2015, 35, 3346–3359. [Google Scholar] [CrossRef] [Green Version]
- Lim, T.K.; Rone, M.B.; Lee, S.; Antel, J.P.; Zhang, J. Mitochondrial and Bioenergetic Dysfunction in Trauma-Induced Painful Peripheral Neuropathy. Mol. Pain 2015, 11, 58. [Google Scholar] [CrossRef] [Green Version]
- Rizzuto, R.; De Stefani, D.; Raffaello, A.; Mammucari, C. Mitochondria as sensors and regulators of calcium signalling. Nat. Rev. Mol. Cell Biol. 2012, 13, 566–578. [Google Scholar] [CrossRef]
- Siau, C.; Bennett, G.J. Dysregulation of Cellular Calcium Homeostasis in Chemotherapy-Evoked Painful Peripheral Neuropathy. Anesth. Analg. 2006, 102, 1485–1490. [Google Scholar] [CrossRef]
- Brand, M.D.; Nicholls, D.G. Assessing mitochondrial dysfunction in cells. Biochem. J. 2011, 435, 297–312. [Google Scholar] [CrossRef] [Green Version]
- Gao, S.; Wang, Y.; Wang, Z. Assessment of trigeminal somatosensory evoked potentials in burning mouth syndrome. Chin. J. Dent. Res. 2000, 3, 40–46. [Google Scholar]
- Noble, M.; Treadwell, J.R.; Tregear, S.J.; Coates, V.H.; Wiffen, P.J.; Akafomo, C.; Schoelles, K.M. Long-term opioid management for chronic noncancer pain. Cochrane Database Syst. Rev. 2010, 2010, CD006605. [Google Scholar] [CrossRef]
- Sommer, C.; Welsch, P.; Klose, P.; Schaefert, R.; Petzke, F.; Häuser, W. Opioide bei chronischem neuropathischem Schmerz. Der Schmerz 2014, 29, 35–46. [Google Scholar] [CrossRef]
- Liu, Y.F.; Kim, Y.; Yoo, T.; Han, P.; Inman, J. Burning mouth syndrome: A systematic review of treatments. Oral Dis. 2017, 24, 325–334. [Google Scholar] [CrossRef]
- De Moraes, M.; Bezerra, B.A.D.A.; Neto, P.C.D.R.; Soares, A.C.A.D.O.; Pinto, L.P.; Costa, A.D.L.L. Randomized trials for the treatment of burning mouth syndrome: An evidence-based review of the literature. J. Oral Pathol. Med. 2011, 41, 281–287. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence (NICE). Neuropathic Pain-Pharmacological Management: The Pharmacological Management of Neuropathic Pain in Adults in Non-Specialist Settings. 2013. Available online: http://www.nice.org.uk/guidance/cg173 (accessed on 29 January 2022).
- Samoilova, K.A.; Zhevago, N.A.; Petrishchev, N.N.; Zimin, A.A. Role of Nitric Oxide in the Visible Light-Induced Rapid Increase of Human Skin Microcirculation at the Local and Systemic Levels: II. Healthy Volunteers. Photomed. Laser Surg. 2008, 26, 443–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karu, T.I.; Ms, L.V.P.; Afanasyeva, N.I. Cellular effects of low power laser therapy can be mediated by nitric oxide. Lasers Surg. Med. 2005, 36, 307–314. [Google Scholar] [CrossRef] [PubMed]
- Gigo-Benato, D.; Geuna, S.; Rodrigues, A.D.C.; Tos, P.; Fornaro, M.; Boux, E.; Battiston, B.; Giacobini-Robecchi, M.G. Low-power laser biostimulation enhances nerve repair after end-to-side neurorrhaphy: A double-blind randomized study in the rat median nerve model. Lasers Med. Sci. 2004, 19, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.-H.; Wang, J.; Gong, D.-X.; Gu, H.-Y.; Hu, S.-S.; Zhang, H. Effects of low-level laser irradiation on mesenchymal stem cell proliferation: A microarray analysis. Lasers Med. Sci. 2011, 27, 509–519. [Google Scholar] [CrossRef] [PubMed]
- Jameie, S.B.; Masoumipoor, M.; Janzadeh, A.; Nasirinezhad, F.; Kerdari, M.; Soleimani, M. Combined therapeutic effects of low power laser (980nm) and CoQ10 on neuropathic pain in adult male rat. Med. J. Islamic Repub. Iran 2014, 28, 5. [Google Scholar]
- Laakso, E.-L.; Cabot, P.J. Nociceptive Scores and Endorphin-Containing Cells Reduced by Low-Level Laser Therapy (LLLT) in Inflamed Paws of Wistar Rat. Photomed. Laser Surg. 2005, 23, 32–35. [Google Scholar] [CrossRef]
- Hagiwara, S.; Iwasaka, H.; Okuda, K.; Noguchi, T. GaAlAs (830 nm) low-level laser enhances peripheral endogenous opioid analgesia in rats. Lasers Surg. Med. 2007, 39, 797–802. [Google Scholar] [CrossRef]
- Cg, S.K.; Maiya, A.G.; Hande, H.M.; Vidyasagar, S.; Rao, K.; Rajagopal, K.V. Efficacy of low level laser therapy on painful diabetic peripheral neuropathy. Laser Ther. 2015, 24, 195–200. [Google Scholar] [CrossRef] [Green Version]
- Sakurai, Y.; Yamaguchi, M.; Abiko, Y. Inhibitory effect of low-level laser irradiation on LPS-stimulated prostaglandin E2 production and cyclooxygenase-2 in human gingival fibroblasts. Eur. J. Oral Sci. 2000, 108, 29–34. [Google Scholar] [CrossRef]
- Cotler, H.B.; Chow, R.T.; Hamblin, M.R.; Carroll, J. The Use of Low Level Laser Therapy (LLLT) For Musculoskeletal Pain. MOJ Orthop. Rheumatol. 2015, 2, 00068. [Google Scholar] [CrossRef]
- Pezelj-Ribarić, S.; Kqiku, L.; Brumini, G.; Urek, M.M.; Antonić, R.; Kuiš, D.; Glažar, I.; Städtler, P. Proinflammatory cytokine levels in saliva in patients with burning mouth syndrome before and after treatment with low-level laser therapy. Lasers Med. Sci. 2012, 28, 297–301. [Google Scholar] [CrossRef] [PubMed]
- Kato, I.T.; Pellegrini, V.D.; Prates, R.A.; Ribeiro, M.S.; Wetter, N.U.; Sugaya, N.N. Low-Level Laser Therapy in Burning Mouth Syndrome Patients: A Pilot Study. Photomed. Laser Surg. 2010, 28, 835–839. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.-W.; Huang, Y.-F. Treatment of Burning Mouth Syndrome with a Low-Level Energy Diode Laser. Photomed. Laser Surg. 2011, 29, 123–125. [Google Scholar] [CrossRef] [PubMed]
- Chow, R.T.; Armati, P.J.; Laakso, E.-L.; Bjordal, J.M.; Baxter, G.D. Inhibitory Effects of Laser Irradiation on Peripheral Mammalian Nerves and Relevance to Analgesic Effects: A Systematic Review. Photomed. Laser Surg. 2011, 29, 365–381. [Google Scholar] [CrossRef] [PubMed]
- Zupin, L.; Ottaviani, G.; Rupel, K.; Biasotto, M.; Zacchigna, S.; Crovella, S.; Celsi, F. Analgesic effect of Photobiomodulation Therapy: An in vitro and in vivo study. J. Biophotonics 2019, 12, e201900043. [Google Scholar] [CrossRef] [PubMed]
- Al-Maweri, S.A.; Javed, F.; Kalakonda, B.; AlAizari, N.A.; Al-Soneidar, W.; Al-Akwa, A. Efficacy of low level laser therapy in the treatment of burning mouth syndrome: A systematic review. Photodiagnosis Photodyn. Ther. 2017, 17, 188–193. [Google Scholar] [CrossRef]
- Bardellini, E.; Amadori, F.; Conti, G.; Majorana, A. Efficacy of the photobiomodulation therapy in the treatment of the burning mouth syndrome. Med. Oral Patol. Oral Cir. Bucal 2019, 24, e787–e791. [Google Scholar] [CrossRef]
- Valenzuela, S.; Lopez-Jornet, P. Effects of low-level laser therapy on burning mouth syndrome. J. Oral Rehabil. 2016, 44, 125–132. [Google Scholar] [CrossRef]
- Arbabi-Kalati, F.; Bakhshani, N.-M.; Rasti, M. Evaluation of the efficacy of low-level laser in improving the symptoms of burning mouth syndrome. J. Clin. Exp. Dent. 2015, 7, e524–e527. [Google Scholar] [CrossRef] [PubMed]
- Arduino, P.G.; Cafaro, A.; Garrone, M.; Gambino, A.; Cabras, M.; Romagnoli, E.; Broccoletti, R. A randomized pilot study to assess the safety and the value of low-level laser therapy versus clonazepam in patients with burning mouth syndrome. Lasers Med. Sci. 2016, 31, 811–816. [Google Scholar] [CrossRef] [PubMed]
- Sugaya, N.N.; Da Silva, F.P.; Kato, I.T.; Prates, R.; Gallo, C.D.B.; Pellegrini, V.D. Low Intensity laser therapy in patients with burning mouth syndrome: A randomized, placebo-controlled study. Braz. Oral Res. 2016, 30, e108. [Google Scholar] [CrossRef] [PubMed]
- Spanemberg, J.C.; López, J.L.; De Figueiredo, M.A.Z.; Cherubini, K.; Salum, F.G. Efficacy of low-level laser therapy for the treatment of burning mouth syndrome: A randomized, controlled trial. J. Biomed. Opt. 2015, 20, 098001. [Google Scholar] [CrossRef] [PubMed]
- Škrinjar, I.; Brzak, B.L.; Vidranski, V.; Boras, V.V.; Rogulj, A.A.; Pavelić, B. Salivary Cortisol Levels and Burning Symptoms in Patients with Burning Mouth Syndrome before and after Low Level Laser Therapy: A Double Blind Controlled Randomized Clinical Trial. Acta Stomatol. Croat. 2020, 54, 44–50. [Google Scholar] [CrossRef]
- Sikora, M.; Včev, A.; Siber, S.; Boras, V.V.; Rotim, Ž.; Matijević, M. The Efficacy of Low-Level Laser Therapy in Burning Mouth Syndrome–A Pilot Study. Acta Clin. Croat. 2018, 57, 312–315. [Google Scholar] [CrossRef]
- Spanemberg, J.-C.; Segura-Egea, J.-J.; Rivera-Campillo, E.R.-D.; Jané-Salas, E.; Salum, F.-G.; López-López, J. Low-level laser therapy in patients with Burning Mouth Syndrome: A double-blind, randomized, controlled clinical trial. J. Clin. Exp. Dent. 2019, 11, e162–e169. [Google Scholar] [CrossRef] [PubMed]
- De Pedro, M.; López-Pintor, R.M.; Casañas, E.; Hernández, G. Effects of photobiomodulation with low-level laser therapy in burning mouth syndrome: A randomized clinical trial. Oral Dis. 2020, 26, 1764–1776. [Google Scholar] [CrossRef]
- Scardina, G.; Casella, S.; Bilello, G.; Messina, P. Photobiomodulation Therapy in the Management of Burning Mouth Syndrome: Morphological Variations in the Capillary Bed. Dent. J. 2020, 8, 99. [Google Scholar] [CrossRef]
- Matos, A.; Silva, P.; Paranhos, L.; Santana, I.; Matos, F. Efficacy of the laser at low intensity on primary burning oral syndrome: A systematic review. Med. Oral Patol. Oral Cir. Bucal 2021, 26, e216–e225. [Google Scholar] [CrossRef]
- Zhang, W.; Hu, L.; Zhao, W.; Yan, Z. Effectiveness of photobiomodulation in the treatment of primary burning mouth syndrome—A systematic review and meta-analysis. Lasers Med. Sci. 2020, 36, 239–248. [Google Scholar] [CrossRef] [PubMed]
- Sun, C.; Jiang, W.-W. Low-level laser treatment of burning mouth syndrome: A systematic review and meta-analysis. Front. Oral Maxillofac. Med. 2019, 1, 10. [Google Scholar] [CrossRef]
- Eldridge, S.M.; Chan, C.L.; Campbell, M.J.; Bond, C.M.; Hopewell, S.; Thabane, L.; Lancaster, G.A. CONSORT 2010 statement: Extension to randomised pilot and feasibility trials. BMJ 2016, 355, i5239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fitzpatrick, R.; Davey, C.; Buxton, M.J.; Jones, D.R. Evaluating patient-based outcome measures for use in clinical trials. Health Technol. Assess. 1998, 2, 1–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dawson, J.; Doll, H.; Fitzpatrick, R.; Jenkinson, C.; Carr, A.J. The routine use of patient reported outcome measures in healthcare settings. BMJ 2010, 340, c186. [Google Scholar] [CrossRef] [PubMed]
- Farag, A.M.; Albuquerque, R.; Ariyawardana, A.; Chmieliauskaite, M.; Forssell, H.; Nasri-Heir, C.; Klasser, G.D.; Sardella, A.; Mignogna, M.D.; Ingram, M.; et al. World Workshop in Oral Medicine VII: Reporting of IMMPACT-recommended outcome domains in randomized controlled trials of burning mouth syndrome: A systematic review. Oral Dis. 2019, 25, 122–140. [Google Scholar] [CrossRef]
- Lopez-Jornet, P.; Molino-Pagan, D.; Parra-Perez, P.; Valenzuela, S. Neuropathic Pain in Patients with Burning Mouth Syndrome Evaluated Using painDETECT. Pain Med. 2017, 18, 1528–1533. [Google Scholar] [CrossRef]
- Gloth, F.M.; Scheve, A.A.; Stober, C.V.; Chow, S.; Prosser, J. Functional Pain Scale: Reliability, Validity, and Responsiveness in an Elderly Population. JAMDA 2001, 2, 110–114. [Google Scholar]
- Feng, Y.-S.; Kohlmann, T.; Janssen, M.F.; Buchholz, I. Psychometric properties of the EQ-5D-5L: A systematic review of the literature. Qual. Life Res. 2020, 30, 647–673. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence (NICE). Neuropathic Pain-Drug Treatment. Available online: https://cks.nice.org.uk/topics/neuropathic-pain-drug-treatment (accessed on 29 January 2022).
- Fornasari, D. Pharmacotherapy for Neuropathic Pain: A Review. Pain Ther. 2017, 6, 25–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Derry, S.; Bell, R.F.; Straube, S.; Wiffen, P.J.; Aldington, D.; Moore, R.A. Pregabalin for neuropathic pain in adults. Cochrane Database Syst. Rev. 2019, 1, CD007076. [Google Scholar] [CrossRef] [PubMed]
- Freynhagen, R.; Serpell, M.; Emir, B.; Whalen, E.; Parsons, B.; Clair, A.; Latymer, M. A Comprehensive Drug Safety Evaluation of Pregabalin in Peripheral Neuropathic Pain. Pain Pract. 2013, 15, 47–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bijur, P.E.; Silver, W.; Gallagher, E.J. Reliability of the Visual Analog Scale for Measurement of Acute Pain. Acad. Emerg. Med. 2001, 8, 1153–1157. [Google Scholar] [CrossRef] [PubMed]
- Joos, E.; Peretz, A.; Beguin, S.; Famaey, J.P. Reliability and reproducibility of visual analogue scale and numeric rating scale for therapeutic evaluation of pain in rheumatic patients. J. Rheumatol. 1991, 18, 1269–1270. [Google Scholar] [PubMed]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCaffrey, N.; Kaambwa, B.; Currow, D.C.; Ratcliffe, J. Health-related quality of life measured using the EQ-5D–5L: South Australian population norms. Health Qual. Life Outcomes 2016, 14, 133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bulamu, N.B.; Kaambwa, B.; Ratcliffe, J. A systematic review of instruments for measuring outcomes in economic evaluation within aged care. Health Qual. Life Outcomes 2015, 13, 179. [Google Scholar] [CrossRef] [Green Version]
- Cavalli, E.; Mammana, S.; Nicoletti, F.; Bramanti, P.; Mazzon, E. The neuropathic pain: An overview of the current treatment and future therapeutic approaches. Int. J. Immunopathol. Pharmacol. 2019, 33, 2058738419838383. [Google Scholar] [CrossRef] [Green Version]
- Doth, A.H.; Hansson, P.; Jensen, M.P.; Taylor, R.S. The burden of neuropathic pain: A systematic review and meta-analysis of health utilities. Pain 2010, 149, 338–344. [Google Scholar] [CrossRef]
- Closs, S.J.; Staples, V.; Reid, I.; Bennett, M.; Briggs, M. The impact of neuropathic pain on relationships. J. Adv. Nurs. 2009, 65, 402–411. [Google Scholar] [CrossRef]
- Smith, B.H.; Torrance, N.; Bennett, M.I.; Lee, A.J. Health and Quality of Life Associated with Chronic Pain of Predominantly Neuropathic Origin in the Community. Clin. J. Pain 2007, 23, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Santoro, V.; Caputo, G.; Peluso, F. Clinical and therapeutic experience in twenty eight patients with burning mouth syndrome. Minerva Stomatol. 2005, 54, 489–496. [Google Scholar] [PubMed]
- Tarkkila, L.; Linna, M.; Tiitinen, A.; Lindqvist, C.; Meurman, J. Oral symptoms at menopause—the role of hormone replacement therapy. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontology 2001, 92, 276–280. [Google Scholar] [CrossRef] [PubMed]
- López-Jornet, P.; Camacho-Alonso, F.; Andujar-Mateos, P.; Sánchez- Siles, M.; Gómez-Garcia, F. Burning mouth syndrome: An update. Med. Oral Patol. Oral Cir. Bucal 2010, 15, e562–e568. [Google Scholar] [CrossRef] [PubMed]
- Klasser, G.D.; Epstein, J.B.; Villines, D. Diagnostic dilemma: The enigma of an oral burning sensation. J. Can. Dent. Assoc. 2011, 77, b146. [Google Scholar] [PubMed]
- Kate, R.J.; Rubatt, S.; Enwemeka, C.S.; Huddleston, W.E. Optimal Laser Phototherapy Parameters for Pain Relief. Photomed. Laser Surg. 2018, 36, 354–362. [Google Scholar] [CrossRef]
- Huang, Y.; Sharma, S.K.; Carroll, J.; Hamblin, M. Biphasic Dose Response in Low Level Light Therapy–an Update. Dose-Response 2011, 9, 602–618. [Google Scholar] [CrossRef] [PubMed]
- Chow, R.; Armati, P.J.; Khan, I.; Arany, P.R. Dosimetry for photobiomodulation therapy: Response to Sommers et al. Ann. Transl. Med. 2016, 4, 208. [Google Scholar] [CrossRef]
- Henderson, T.A.; Morries, L. Near-infrared photonic energy penetration: Can infrared phototherapy effectively reach the human brain? Neuropsychiatr. Dis. Treat. 2015, 11, 2191–2208. [Google Scholar] [CrossRef] [Green Version]
- Ash, C.; Dubec, M.; Donne, K.; Bashford, T. Effect of wavelength and beam width on penetration in light-tissue interaction using computational methods. Lasers Med. Sci. 2017, 32, 1909–1918. [Google Scholar] [CrossRef]
- Hudson, D.E.; Hudson, D.O.; Wininger, J.M.; Richardson, B.D. Penetration of Laser Light at 808 and 980 nm in Bovine Tissue Samples. Photomed. Laser Surg. 2013, 31, 163–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weldring, T.; Smith, S.M. Article Commentary: Patient-Reported Outcomes (PROs) and Patient-Reported Outcome Measures (PROMs). Health Serv. Insights 2013, 6, HSI-S11093. [Google Scholar] [CrossRef] [PubMed]
- Carey, B.; Farag, A.M.; Nasri-Heir, C.; Klasser, G.D.; Ariyawardana, A.; Chmieliauskaite, M.; Sardella, A.; Carlson, C.R.; Miller, C.S.; Mejia, L.; et al. IMMPACT-recommended outcome measures and tools of assessment in burning mouth syndrome RCTs: An international Delphi survey protocol. Trials 2020, 21, 711. [Google Scholar] [CrossRef] [PubMed]
- Serpell, M.; Latymer, M.; Almas, M.; Ortiz, M.; Parsons, B.; Prieto, R. Neuropathic pain responds better to increased doses of pregabalin: An in-depth analysis of flexible-dose clinical trials. J. Pain Res. 2017, 10, 1769–1776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Snedecor, S.J.; Sudharshan, L.; Cappelleri, J.C.; Sadosky, A.; Mehta, S.; Botteman, M. Systematic Review and Meta-Analysis of Pharmacological Therapies for Painful Diabetic Peripheral Neuropathy. Pain Pract. 2013, 14, 167–184. [Google Scholar] [CrossRef] [PubMed]
- Freynhagen, R.; Baron, R.; Kawaguchi, Y.; Malik, R.A.; Martire, D.L.; Parsons, B.; Rey, R.D.; Schug, S.A.; Jensen, T.S.; Tölle, T.R.; et al. Pregabalin for neuropathic pain in primary care settings: Recommendations for dosing and titration. Postgrad. Med. 2021, 133, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Onakpoya, I.J.; Thomas, E.T.; Lee, J.; Goldacre, B.; Heneghan, C.J. Benefits and harms of pregabalin in the management of neuropathic pain: A rapid review and meta-analysis of randomised clinical trials. BMJ Open 2019, 9, e023600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ellis, A.; Bennett, D.L.H. Neuroinflammation and the generation of neuropathic pain. Br. J. Anaesth. 2013, 111, 26–37. [Google Scholar] [CrossRef] [Green Version]
- Popescu, C. Severe Acute Axonal Neuropathy Induced by Ciprofloxacin: A Case Report. Case Rep. Neurol. 2018, 10, 124–129. [Google Scholar] [CrossRef]
- Jerlang, B.B. Burning mouth syndrome (BMS) and the concept of alexithymia—A preliminary study. J. Oral Pathol. Med. 1997, 26, 249–253. [Google Scholar] [CrossRef]
- Morales, D.; Pacurariu, A.; Slattery, J.; Pinheiro, L.; Mcgettigan, P.; Kurz, X. Association Between Peripheral Neuropathy and Exposure to Oral Fluoroquinolone or Amoxicillin-Clavulanate Therapy. JAMA Neurol. 2019, 76, 827–833. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grushka, M.; Ching, V.; Epstein, J. Burning mouth syndrome. In Taste and Smell, An Update; Thomas Hummel, A.W.-L., Ed.; Krager Medical and Scientific Publisher: Basel, Switzerland, 2006; pp. 278–287. [Google Scholar]
- Souza, F.T.; Santos, T.P.; Bernardes, V.F.; Teixeira, A.L.; Kümmer, A.M.; Silva, T.A.; Abreu, M.H. The impact of burning mouth syndrome on health-related quality of life. Health Qual. Life Outcomes 2011, 9, 57. [Google Scholar] [CrossRef] [Green Version]
- Pereira, J.V.; Normando, A.G.C.; Rodrigues-Fernandes, C.I.; Rivera, C.; Santos-Silva, A.R.; Lopes, M.A. The impact on quality of life in patients with burning mouth syndrome: A systematic review and meta-analysis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2020, 131, 186–194. [Google Scholar] [CrossRef]
- El Mobadder, M.; Nammour, S. Photobiomodulation for Taste Alteration. Encyclopedia 2021, 1, 240–248. [Google Scholar] [CrossRef]
- Hanna, R.; Dalvi, S.; Benedicenti, S.; Amaroli, A.; Sălăgean, T.; Pop, I.D.; Todea, D.; Bordea, I.R.; Amaroli, A. Photobiomodulation Therapy in Oral Mucositis and Potentially Malignant Oral Lesions: A Therapy Towards the Future. Cancers 2020, 12, 1949. [Google Scholar] [CrossRef] [PubMed]
- Oron, U.; Ilic, S.; De Taboada, L.; Streeter, J. Ga-As (808 nm) Laser Irradiation Enhances ATP Production in Human Neuronal Cells in Culture. Photomed. Laser Surg. 2007, 25, 180–182. [Google Scholar] [CrossRef] [PubMed]
- Suarez, P.; Clark, G.T. Burning mouth syndrome: An update on diagnosis and treatment methods. J. Calif. Dent. Assoc. 2006, 34, 611–622. [Google Scholar]
- El Mobadder, M.; Farhat, F.; El Mobadder, W.; Nammour, S. Photobiomodulation Therapy in the Treatment of Oral Mucositis, Dysphagia, Oral Dryness, Taste Alteration, and Burning Mouth Sensation Due to Cancer Therapy: A Case Series. Int. J. Environ. Res. Public Health 2019, 16, 4505. [Google Scholar] [CrossRef] [Green Version]
- Braud, A.; Descroix, V.; Ungeheuer, M.-N.; Rougeot, C.; Boucher, Y. Taste function assessed by electrogustometry in burning mouth syndrome: A case-control study. Oral Dis. 2017, 23, 395–402. [Google Scholar] [CrossRef]
- Siviero, M.; Teixeira, M.J.; De Siqueira, J.T.T.; De Siqueira, S.R.D.T. Central mechanisms in burning mouth syndrome involving the olfactory nerve: A preliminary study. Clinics 2011, 66, 509–512. [Google Scholar] [CrossRef] [Green Version]
- Hanna, R.; Dalvi, S.; Bensadoun, R.; Benedicenti, S. Role of Photobiomodulation Therapy in Modulating Oxidative Stress in Temporomandibular Disorders. A Systematic Review and Meta-Analysis of Human Randomised Controlled Trials. Antioxidants 2021, 10, 1028. [Google Scholar] [CrossRef] [PubMed]
- Zecha, J.A.E.M.; Raber-Durlacher, J.E.; Nair, R.G.; Epstein, J.B.; Sonis, S.T.; Elad, S.; Hamblin, M.R.; Barasch, A.; Migliorati, C.A.; Milstein, D.M.J.; et al. Low level laser therapy/photobiomodulation in the management of side effects of chemoradiation therapy in head and neck cancer: Part 1: Mechanisms of action, dosimetric, and safety considerations. Support. Care Cancer 2016, 24, 2781–2792. [Google Scholar] [CrossRef] [Green Version]
- Zecha, J.A.E.M.; Raber-Durlacher, J.E.; Nair, R.G.; Epstein, J.B.; Elad, S.; Hamblin, M.R.; Barasch, A.; Migliorati, C.A.; Milstein, D.M.J.; Genot, M.-T.; et al. Low-level laser therapy/photobiomodulation in the management of side effects of chemoradiation therapy in head and neck cancer: Part 2: Proposed applications and treatment protocols. Support. Care Cancer 2016, 24, 2793–2805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peregrin, T. Improving Taste Sensation in Patients Who Have Undergone Chemotherapy or Radiation Therapy. J. Am. Diet. Assoc. 2006, 106, 1536–1540. [Google Scholar] [CrossRef] [PubMed]
- Bensadoun, R.J.; Epstein, J.B.; Nair, R.G.; Barasch, A.; Raber-Durlacher, J.E.; Migliorati, C.; Genot-Klastersky, M.T.; Treister, N.; Arany, P.; Lodewijckx, J.; et al. Safety and efficacy of photobiomodulation therapy in oncology: A systematic review. Cancer Med. 2020, 9, 8279–8300. [Google Scholar] [CrossRef]
- Forssell, H.; Jääskeläinen, S.; Tenovuo, O.; Hinkka, S. Sensory dysfunction in burning mouth syndrome. Pain 2002, 99, 41–47. [Google Scholar] [CrossRef]
- Hanna, R.; Dalvi, S.; Bensadoun, R.J.; Raber-Durlacher, J.E.; Benedicenti, S. Role of Photobiomodulation Therapy in Neurological Primary Burning Mouth Syndrome. A Systematic Review and Meta-Analysis of Human Randomised Controlled Clinical Trials. Pharmaceutics 2021, 13, 1838. [Google Scholar] [CrossRef] [PubMed]
- Sikora, M.; Verzak, Z.; Matijevic, M.; Vcev, A.; Siber, S.; Music, L.; Carek, A. Anxiety and Depression Scores in Patients With Burning Mouth Syndrome. Psychiatr. Danub. 2018, 30, 466–470. [Google Scholar] [CrossRef]
- Attal, N. Pharmacological treatments of neuropathic pain: The latest recommendations. Rev. Neurol. 2019, 175, 46–50. [Google Scholar] [CrossRef]
- De Pedro, M.; López-Pintor, R.M.; De La Hoz-Aizpurua, J.; Casañas, E.; Hernández, G. Efficacy of Low-Level Laser Therapy for the Therapeutic Management of Neuropathic Orofacial Pain: A Systematic Review. J. Oral Facial Pain Headache 2020, 34, 13–30. [Google Scholar] [CrossRef] [PubMed]
- Sedgwick, P. What is a non-randomised controlled trial? BMJ 2014, 348, g4115. [Google Scholar] [CrossRef] [PubMed]
- Colloca, L.; Ludman, T.; Bouhassira, D.; Baron, R.; Dickenson, A.H.; Yarnitsky, D.; Freeman, R.; Truini, A.; Attal, N.; Finnerup, N.; et al. Neuropathic pain. Nat. Rev. Dis. Primers 2017, 16, 17002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finnerup, N.B.; Attal, N.; Haroutounian, S.; McNicol, E.; Baron, R.; Dworkin, R.H.; Gilron, I.; Haanpää, M.; Hansson, P.; Jensen, T.S.; et al. Pharmacotherapy for neuropathic pain in adults: A systematic review and meta-analysis. Lancet Neurol. 2015, 14, 162–173. [Google Scholar] [CrossRef] [Green Version]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Are Your Daily Functions Affected? | |
|---|---|
| Rated on a Scale from: 0: No Interference 10: Complete Interference | Score |
| Speech | |
| Eating | |
| Drinking | |
| Kissing | |
| Sleeping | |
| Smell | |
| Confidence | |
| Work | |
| Family relationships | |
| Social events | |
| Pronunciation | |
| Taste | |
| Make-up application | |
| Shaving | |
| Brushing teeth | |
| Others (please state) | |
| Device Information | Manufacturer | THOR Photomedicine Ltd. |
| Model identifier | LX2.1 | |
| Semi-conductor materials (emitter type) | GaAIAs | |
| Probe design | Single probe | |
| Beam delivery system | Hand-held probe | |
| Medical/laser class | 3B laser | |
| NOHD | 64 cm | |
| Laser-aiming beam | None | |
| Irradiation Parameters | Wavelength | 810 nm |
| Operating emission mode | Continuous wave | |
| Beam profile | Gaussian distribution | |
| Treatment Parameters | 1/e2 Spot area size area | 0.088 cm2 |
| 1/e2 Spot size and shape | 0.335 cm, circular | |
| Beam divergence full angle | 10° × 54° | |
| Polarisation | Linear | |
| Therapeutic power output | 200 mW | |
| Irradiance | 2 W/cm2 | |
| Irradiance at aperture (mW/cm2) | 1.97 W/cm2 | |
| Fluence (dose) | 59.1 J/cm2 | |
| Energy | 6 J/point | |
| Total energy | 54 J | |
| Power density (irradiance) | 1.97 W/cm2 | |
| Exposure time | 30 s/point | |
| Time interval | Relatively alternate day, excluding weekend | |
| Treatment frequency | Twice a week (Mondays and Wednesdays) | |
| Total number of treatments | 10 | |
| Duration of treatment | 5 consecutive weeks | |
| Number of irradiated points | 9 points | |
| Irradiated target | Trigger points and sites of injury (affected areas) | |
| Scanning technique | Spot technique | |
| Light-tissue distance | <1 mm distance (non-contact) |
| Pt. No. | Condition | Prescribed Medication | Dose of the Medications and Follow-Up Time Points | ||||
|---|---|---|---|---|---|---|---|
| Baseline (T0) | 1-Month Follow-Up (T3) | 3-Month Follow-Up (T4) | 6-Month Follow-Up (T5) | 9-Month Follow-Up (T6) | |||
| 3 | BMS | Nortriptyline | 10 mg | 10 mg | 20 mg | 20 mg | 20 mg |
| 2 | OIN, BMS | Nortriptyline | 20 mg | 20 mg | 40 mg | 40 mg | 40 mg |
| 1 | OIN | Nortriptyline Pregabalin | 10 mg 100 mg | 10 mg 100 mg | 20 mg 200 mg | 20 mg 200 mg | 20 mg 200 mg |
| 1 | BMS | Pregabalin | 100 mg | 100 mg | 200 mg | 200 mg | 200 mg |
| 1 | BMS | Pregabalin | 25 mg | 25 mg | 50 mg | 50 mg | 50 mg |
| 2 | BMS | Gabapentin Nortriptyline | 600 mg | 600 mg | 600 mg 10 mg | 600 mg 10 mg | 600 mg 10 mg |
| Baseline Characteristics | PBM (n = 18) | MED (n = 10) | Different * (Y/N) | p-Value * |
|---|---|---|---|---|
| Age (years; mean ± SD) | 58.00 ± 10.39 | 56.80 ± 10.84 | N | 0.7752 |
| Gender (% female) | 83.33 % | 100.00% | N | 0.5330 |
| Type of NP (% BMS) | 61.11 % | 80.00% | N | 0.4170 |
| Onset (months; mean ± SD) | 57.50 ± 47.93 | 38.90 ± 15.77 | N | 0.7500 |
| Medical history (% fit and well) | 61.11 % | 90.00% | N | 0.1937 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hanna, R.; Bensadoun, R.J.; Beken, S.V.; Burton, P.; Carroll, J.; Benedicenti, S. Outpatient Oral Neuropathic Pain Management with Photobiomodulation Therapy: A Prospective Analgesic Pharmacotherapy-Paralleled Feasibility Trial. Antioxidants 2022, 11, 533. https://doi.org/10.3390/antiox11030533
Hanna R, Bensadoun RJ, Beken SV, Burton P, Carroll J, Benedicenti S. Outpatient Oral Neuropathic Pain Management with Photobiomodulation Therapy: A Prospective Analgesic Pharmacotherapy-Paralleled Feasibility Trial. Antioxidants. 2022; 11(3):533. https://doi.org/10.3390/antiox11030533
Chicago/Turabian StyleHanna, Reem, René Jean Bensadoun, Seppe Vander Beken, Patricia Burton, James Carroll, and Stefano Benedicenti. 2022. "Outpatient Oral Neuropathic Pain Management with Photobiomodulation Therapy: A Prospective Analgesic Pharmacotherapy-Paralleled Feasibility Trial" Antioxidants 11, no. 3: 533. https://doi.org/10.3390/antiox11030533