
Role of Coenzyme Q10 in Health and Disease: An Update on the Last 10 Years (2010–2020)

 , , and
, , and
Abstract
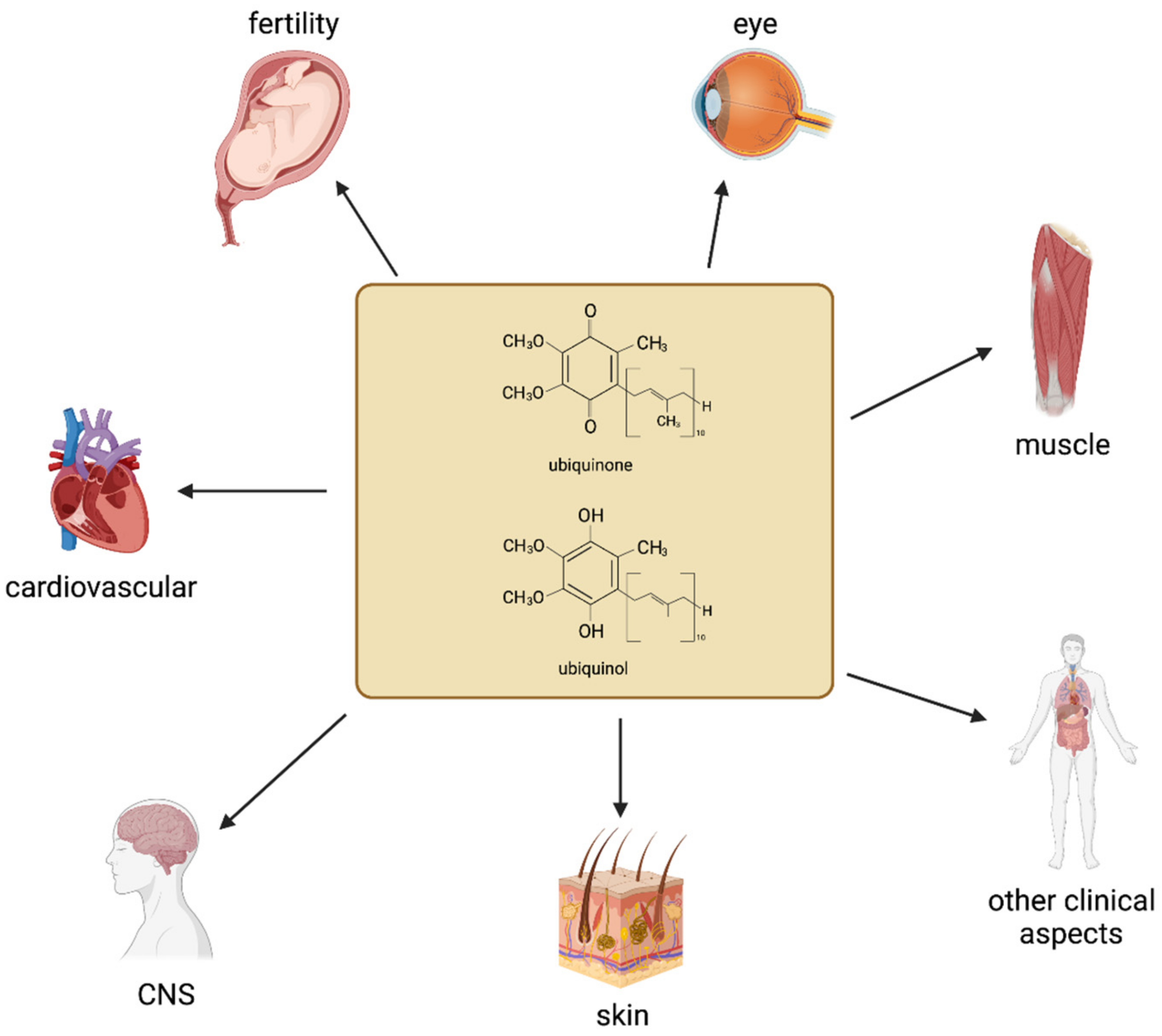
:1. Introduction
2. Cardiovascular Health
3. Fertility
4. Muscle Health and Physical Exercise
5. Other Clinical Aspects
6. Emerging Applications of Coenzyme Q10
7. Concluding Remarks

{kind=link}
| Author, Year | Country | Participants | CoQ10 Dosage and Duration | Main Findings |
|---|---|---|---|---|
| [158] Kurban et al., 2010 | Turkey | Healthy volunteers | Received 100 or 150 mg/day acetylsalicylic acid for 2 months before quantification of total CoQ10 | Reduced total oxidant status and oxidized low-density lipoprotein (Ox-LDL) concentration without significantly affecting CoQ10 levels |
| [54] Dai et al., 2011 | China | Patients with ischemic left ventricular systolic dysfunction (LVSD) | Received 300 mg/day CoQ10 (ubiquinone) for 8 weeks | Improved mitochondrial function and flow-mediated dilation (FMD) to enhance endothelial function |
| [159] Fumagalli et al., 2011 | Italy | Patients with chronic heart failure subjected to physical performance | Received 320 mg/day of Q-terclatrate (equivalent to 16 mg of native CoQ10) and 340 mg/day of creatine for 8 weeks | Improved exercise tolerance, by enhancing peak oxygen consumption and quality of life |
| [160] Mikhin et al., 2011 | Russia | Patients with hypertension | Received CoQ10 in combination with an angiotensin converting enzyme inhibitor enalapril, during a 24 h blood pressure profile | Combination therapy promoted normalization of vascular endothelial function |
| [161] Toyama et al., 2011 | Japan | Hyperlipidemic patients with coronary artery disease on statins | Quantification of total plasma CoQ10 (ubiquinol) levels | Atorvastatin and rosuvastatin, when combined with exercise could significantly preserve ubiquinol levels associated with an increase in HDL-c |
| [162] Young et al., 2011 | New Zealand | Patients with phenotypic or genotypic familial hypercholesterolemia on long-term statin | Quantification of total plasma CoQ10 levels | Low CoQ10 levels are associated with increased arterial stiffness |
| [163] Brugè et al., 2012 | Italy | Healthy subjects | Received 20 mL extra virgin olive oil per day for 2 weeks, followed by 2 weeks of olive oil enriched with 20 mg and 2 more weeks with 40 mg of CoQ10 (ubiquinol) | Increased plasma levels of CoQ10 were associated with reduced susceptibility of LDL to peroxidation and improved redox status |
| [164] Larijani et al., 2013 | United States | Firefighters | Received 300 mg/tablet aged garlic extract plus 30 mg/tablet CoQ10 (ubiquinone) for 1 year | Combination therapy induced beneficial effects on vascular elasticity and endothelial function |
| [47] Lee et al., 2012 | Taiwan | Patients with coronary artery disease (CAD) | Quantification of total plasma CoQ10 levels | Higher CoQ10 concentration was correlated with a lower risk of CAD, even after adjusting for the risk factors for CAD |
| [48] Lee et al., 2012 | Taiwan | Patients with CAD | Received 60 or 150 mg/day of CoQ10 (ubiquinone) for 12 weeks | Higher CoQ10 dose (150 mg) reduced oxidative stress parameters like lipid peroxidation (MDA levels) and increased antioxidant enzyme (superoxide dismutase; SOD) activity |
| [56] Perez-Sanchez et al., 2012 | Spain | Patients with antiphospholipid syndrome | Preincubating of purified monocytes with CoQ10 for 24 h | Reduced oxidative stress, improved mitochondrial structure, reverted altered mitochondrial membrane potential, including decreasing the expression of tissue factor, VEGF, and Flt1 |
| [49] Lee et al., 2013 | Taiwan | Patients with cardiovascular disease on statins | Received 150 mg twice a day or a single dose 300 mg/day CoQ10 (ubiquinone) for 12 weeks | High CoQ10 plasma levels were consistent with significantly enhanced antioxidant enzymes activities and lower inflammation |
| [43] Mortensen et al., 2014 | Europe | Patients with moderate to severe heart failure | Received 100 mg/3 times a day to total 300 mg/day of CoQ10 (ubiquinol) for 2 years | Improved symptoms and reduced major adverse cardiovascular events. Biomarker status included Brain-Natriuretic Peptide (BNP), and long-term Outcome (hospitalizations/mortality) |
| [165] Sharp et al., 2014 | United States | Patients with pulmonary arterial hypertension | Received 100 mg/3 times a day to total 300 mg/day of CoQ10 (ubiquinol) for 12 weeks | High plasma CoQ10 levels were associated with improved cardiac parameters and mitochondrial synthetic function. Hemoglobin increased and red cell distribution. However, metabolic and redox parameters, including glutathione levels were not affected |
| [46] Alehagen et al., 2015 | Sweden | Healthy elderly individuals | Received 200 mg/day CoQ10 (ubiquinone) plus 200 μg/day organic selenium for 48 months to a 10-year follow-up | Significantly reduced cardiovascular mortality, confirmed not at intervention but during 10-year follow-up |
| [52] Mohseni et al., 2015 | Iran | Hyperlipidemic patients with myocardial infarction | Received 200 mg/day CoQ10 (ubiquinone) for 12 weeks | Although did not affect total cholesterol, beneficial effects of CoQ10 supplementation were related to increased high-density lipoprotein (HDL) levels, and decreased concentrations of (intercellular adhesion molecule-1 (ICAM-1) and IL-6 |
| [51] Bagheri et al., 2015 | Iran | Patients with mild hypertension | Received 100 mg/day CoQ10 (ubiquinone) for 12 weeks | Beneficial effects of CoQ10 were related to decreasing some pro-inflammatory factors, such as IL-6 and high-sensitivity C-reactive protein (hs-CRP), and in increasing adiponectin |
| [166] Pérez-Sánchez et al., 2017 | Spain | Patients with antiphospholipid syndrome | Received 200 mg/day CoQ10 (ubiquinol) for 1 month | Improved endothelial function and decreased monocyte expression of prothrombotic and proinflammatory mediators, inhibited phosphorylation of thrombosis-related protein kinases, and decreased peroxides and percentage of monocytes with depolarized mitochondria |
| [44] Mortensen et al., 2019 | Europe | Patients with moderate to severe heart failure | Received 300 mg/day CoQ10 (ubiquinone) for 3 months and 2 years | Reduced major adverse cardiovascular events, all-cause mortality, cardiovascular mortality, hospitalization and improvement of symptoms |
| [55] Kawashima et al., 2020 | Japan | Patients with heart failure with reduced ejection fraction | Received 400 mg/day CoQ10 (ubiquinol) for 3 months | Significantly improved peripheral endothelial function |
| [58] Sabbatinelli et al., 2020 | Italy | Healthy subjects with moderate dyslipidemia | Received 100 or 200 mg/day CoQ10 (ubiquinol) for 8 weeks | Significantly ameliorated dyslipidemia-related endothelial dysfunction. This was in part by improving blood flow through enhancing nitric oxide bioavailability and lowering oxidized low-density lipoprotein cholesterol |
| [167] Shikh et al., 2020 | Russia | Patients with cardiovascular diseases (CVDs) | Effects of atorvastatin, amlodipine and ethoxidol on the endogenous CoQ10 plasma concentration | Patients with CVDs treated with various drugs had CoQ10 plasma level statistically significantly lower than in practically healthy individuals |
| [45] Zhao et al., 2015 | China | Patients with moderate to severe heart failure (HF | Received 30 mg/day of CoQ10 (ubiquinone) for 6 and 12 months | CoQ10 induced significant reduction in the level of malondialdehyde and may attenuate the incidence of atrial fibrillation in patients with HF |
| [50] Orlando et al., 2020 | Italy | Patients with aortic stenosis (AS) | Received 400 mg/day of CoQ10 (ubiquinol) from 7 days before to 5 days after surgery | Post-operative increase in troponin I was curbed, plasma CoQ10 declined and oxidation were counteracted |
| [59] Langsjoen at al., 2014 | United States | Healthy volunteers | Received 200 mg/day of ubiquinone for 4 weeks before and 200 mg/day of ubiquinol for other 4 weeks, after 4 weeks of washout | Plasma total CoQ10 and total CoQ10/cholesterol ratio were significantly higher after ubiquinol than ubiquinone |
Funding
Conflicts of Interest
References
- Littarru, G.P.; Tiano, L. Bioenergetic and antioxidant properties of coenzyme Q10: Recent developments. Mol. Biotechnol. 2007, 37, 31–37. [Google Scholar] [CrossRef]
- Littarru, G.P.; Tiano, L. Clinical aspects of coenzyme Q10: An update. Nutrition 2010, 26, 250–254. [Google Scholar] [CrossRef]
- WHO. The Top 10 Causes of Death. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 17 August 2021).
- North, B.J.; Sinclair, D.A. The intersection between aging and cardiovascular disease. Circ. Res. 2012, 110, 1097–1108. [Google Scholar] [CrossRef]
- Gosse, P. Left ventricular hypertrophy as a predictor of cardiovascular risk. J. Hypertens. Suppl. 2005, 23, S27–S33. [Google Scholar] [CrossRef]
- Krim, S.R.; Campbell, P.; Lavie, C.J.; Ventura, H. Micronutrients in chronic heart failure. Curr. Heart Fail. Rep. 2013, 10, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Gao, L.; Mao, Q.; Cao, J.; Wang, Y.; Zhou, X.; Fan, L. Effects of coenzyme Q10 on vascular endothelial function in humans: A meta-analysis of randomized controlled trials. Atherosclerosis 2012, 221, 311–316. [Google Scholar] [CrossRef] [PubMed]
- Fotino, A.D.; Thompson-Paul, A.M.; Bazzano, L.A. Effect of coenzyme Q(1)(0) supplementation on heart failure: A meta-analysis. Am. J. Clin. Nutr. 2013, 97, 268–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kosmas, C.E.; Alkhawam, H.; El-Hunjul, M.; Wagman, G.; Kahn, M.R.; Grady, K.M.; Vittorio, T.J. Statin-mediated low-density lipoprotein lowering in chronic congestive heart failure. Am. J. Med. Sci. 2014, 347, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Ayer, A.; Macdonald, P.; Stocker, R. CoQ(1)(0) Function and Role in Heart Failure and Ischemic Heart Disease. Annu. Rev. Nutr. 2015, 35, 175–213. [Google Scholar] [CrossRef] [PubMed]
- Jankowski, J.; Korzeniowska, K.; Cieslewicz, A.; Jablecka, A. Coenzyme Q10—A new player in the treatment of heart failure? Pharmacol. Rep. 2016, 68, 1015–1019. [Google Scholar] [CrossRef]
- Oleck, S.; Ventura, H.O. Coenzyme Q10 and Utility in Heart Failure: Just Another Supplement? Curr. Heart Fail. Rep. 2016, 13, 190–195. [Google Scholar] [CrossRef] [PubMed]
- Ba, Y.J.; Miao, Y.; Sun, Y.; Li, Z.; Cheng, G. Efficacy of coenzyme Q10 as adjuvant therapy in heart failure: A meta-analysis. Chin. J. Evid. Based Med. 2016, 16, 311–318. [Google Scholar]
- Yang, Y.K.; Wang, L.P.; Chen, L.; Yao, X.P.; Yang, K.Q.; Gao, L.G.; Zhou, X.L. Coenzyme Q10 treatment of cardiovascular disorders of ageing including heart failure, hypertension and endothelial dysfunction. Clin. Chim. Acta 2015, 450, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Dludla, P.V.; Nyambuya, T.M.; Orlando, P.; Silvestri, S.; Mxinwa, V.; Mokgalaboni, K.; Nkambule, B.B.; Louw, J.; Muller, C.J.F.; Tiano, L. The impact of coenzyme Q10 on metabolic and cardiovascular disease profiles in diabetic patients: A systematic review and meta-analysis of randomized controlled trials. Endocrinol. Diabetes Metab. 2020, 3, e00118. [Google Scholar] [CrossRef] [Green Version]
- Dludla, P.V.; Orlando, P.; Silvestri, S.; Marcheggiani, F.; Cirilli, I.; Nyambuya, T.M.; Mxinwa, V.; Mokgalaboni, K.; Nkambule, B.B.; Johnson, R.; et al. Coenzyme Q10 Supplementation Improves Adipokine Levels and Alleviates Inflammation and Lipid Peroxidation in Conditions of Metabolic Syndrome: A Meta-Analysis of Randomized Controlled Trials. Int. J. Mol. Sci. 2020, 21, 3247. [Google Scholar] [CrossRef]
- Suarez-Rivero, J.M.; Pastor-Maldonado, C.J.; de la Mata, M.; Villanueva-Paz, M.; Povea-Cabello, S.; Alvarez-Cordoba, M.; Villalon-Garcia, I.; Suarez-Carrillo, A.; Talaveron-Rey, M.; Munuera, M.; et al. Atherosclerosis and Coenzyme Q10. Int. J. Mol. Sci. 2019, 20, 5195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dragan, S.; Buleu, F.; Christodorescu, R.; Cobzariu, F.; Iurciuc, S.; Velimirovici, D.; Xiao, J.; Luca, C.T. Benefits of multiple micronutrient supplementation in heart failure: A comprehensive review. Crit. Rev. Food Sci. Nutr. 2019, 59, 965–981. [Google Scholar] [CrossRef]
- Dludla, P.V.; Orlando, P.; Silvestri, S.; Mazibuko-Mbeje, S.E.; Johnson, R.; Marcheggiani, F.; Cirilli, I.; Muller, C.J.F.; Louw, J.; Obonye, N.; et al. N-Acetyl cysteine ameliorates hyperglycemia-induced cardiomyocyte toxicity by improving mitochondrial energetics and enhancing endogenous Coenzyme Q9/10 levels. Toxicol. Rep. 2019, 6, 1240–1245. [Google Scholar] [CrossRef]
- Dludla, P.V.; Silvestri, S.; Orlando, P.; Mazibuko-Mbeje, S.E.; Johnson, R.; Marcheggiani, F.; Cirilli, I.; Muller, C.J.F.; Louw, J.; Chellan, N.; et al. Palmitate-induced toxicity is associated with impaired mitochondrial respiration and accelerated oxidative stress in cultured cardiomyocytes: The critical role of coenzyme Q9/10. Toxicol. In Vitro 2020, 68, 104948. [Google Scholar] [CrossRef]
- Koziel, A.; Woyda-Ploszczyca, A.; Kicinska, A.; Jarmuszkiewicz, W. The influence of high glucose on the aerobic metabolism of endothelial EA.hy926 cells. Pflugers Arch. 2012, 464, 657–669. [Google Scholar] [CrossRef] [Green Version]
- Cirilli, I.; Orlando, P.; Marcheggiani, F.; Dludla, P.V.; Silvestri, S.; Damiani, E.; Tiano, L. The Protective Role of Bioactive Quinones in Stress-induced Senescence Phenotype of Endothelial Cells Exposed to Cigarette Smoke Extract. Antioxidants 2020, 9, 1008. [Google Scholar] [CrossRef] [PubMed]
- Olivieri, F.; Lazzarini, R.; Babini, L.; Prattichizzo, F.; Rippo, M.R.; Tiano, L.; Di Nuzzo, S.; Graciotti, L.; Festa, R.; Bruge, F.; et al. Anti-inflammatory effect of ubiquinol-10 on young and senescent endothelial cells via miR-146a modulation. Free Radic. Biol. Med. 2013, 63, 410–420. [Google Scholar] [CrossRef] [PubMed]
- Tsai, K.L.; Chen, L.H.; Chiou, S.H.; Chiou, G.Y.; Chen, Y.C.; Chou, H.Y.; Chen, L.K.; Chen, H.Y.; Chiu, T.H.; Tsai, C.S.; et al. Coenzyme Q10 suppresses oxLDL-induced endothelial oxidative injuries by the modulation of LOX-1-mediated ROS generation via the AMPK/PKC/NADPH oxidase signaling pathway. Mol. Nutr. Food Res. 2011, 55 (Suppl. 2), S227–S240. [Google Scholar] [CrossRef] [PubMed]
- Tsuneki, H.; Tokai, E.; Suzuki, T.; Seki, T.; Okubo, K.; Wada, T.; Okamoto, T.; Koya, S.; Kimura, I.; Sasaoka, T. Protective effects of coenzyme Q10 against angiotensin II-induced oxidative stress in human umbilical vein endothelial cells. Eur. J. Pharmacol. 2013, 701, 218–227. [Google Scholar] [CrossRef] [PubMed]
- Alehagen, U.; Johansson, P.; Aaseth, J.; Alexander, J.; Wagsater, D. Significant changes in circulating microRNA by dietary supplementation of selenium and coenzyme Q10 in healthy elderly males. A subgroup analysis of a prospective randomized double-blind placebo-controlled trial among elderly Swedish citizens. PLoS ONE 2017, 12, e0174880. [Google Scholar] [CrossRef] [PubMed]
- Nemec Svete, A.; Verk, B.; Jazbec Križman, P.; Druzhaeva, N.; Bohanec, A.; Petrič, D. Blood variables associated with survival in canine congestive heart failure patients. Bulg. J. Vet. Med. 2020, 23, 257–261. [Google Scholar] [CrossRef]
- Svete, A.N.; Verk, B.; Seliskar, A.; Tomsic, K.; Krizman, P.J.; Petric, A.D. Plasma coenzyme Q10 concentration, antioxidant status, and serum N-terminal pro-brain natriuretic peptide concentration in dogs with various cardiovascular diseases and the effect of cardiac treatment on measured variables. Am. J. Vet. Res. 2017, 78, 447–457. [Google Scholar] [CrossRef]
- Gvozdjakova, A.; Kucharska, J.; Kura, B.; Vancova, O.; Rausova, Z.; Sumbalova, Z.; Ulicna, O.; Slezak, J. A new insight into the molecular hydrogen effect on coenzyme Q and mitochondrial function of rats. Can. J. Physiol. Pharmacol. 2020, 98, 29–34. [Google Scholar] [CrossRef]
- Erol, B.; Bozlu, M.; Hanci, V.; Tokgoz, H.; Bektas, S.; Mungan, G. Coenzyme Q10 treatment reduces lipid peroxidation, inducible and endothelial nitric oxide synthases, and germ cell-specific apoptosis in a rat model of testicular ischemia/reperfusion injury. Fertil. Steril. 2010, 93, 280–282. [Google Scholar] [CrossRef]
- Nasoohi, S.; Simani, L.; Khodagholi, F.; Nikseresht, S.; Faizi, M.; Naderi, N. Coenzyme Q10 supplementation improves acute outcomes of stroke in rats pretreated with atorvastatin. Nutr. Neurosci. 2019, 22, 264–272. [Google Scholar] [CrossRef]
- Tillman, P.; Mann, K.; Agu, R.U.; Yeung, P.K. Effect of coenzyme Q10 on ATP metabolism in red blood cells and cardiovascular hemodynamics in an awaken rat model. Curr. Top. Pharmacol. 2019, 23, 23–30. [Google Scholar]
- Shamardl, H.A.; El-Ashmony, S.M.; Kamel, H.F.; Fatani, S.H. Potential Cardiovascular and Renal Protective Effects of Vitamin D and Coenzyme Q10 in l-NAME-Induced Hypertensive Rats. Am. J. Med. Sci. 2017, 354, 190–198. [Google Scholar] [CrossRef] [PubMed]
- Kozaeva, L.P.; Gorodetskaya, E.A.; Ruuge, E.K.; Kalenikova, E.I.; Medvedev, O.S. Beneficial effect of coenzyme Q10 injection on nitric oxide -related dilation of the rat aorta. Eur. J. Pharmacol. 2017, 794, 15–19. [Google Scholar] [CrossRef]
- Kulyak, O.Y.; Gorodetskaya, E.; Kalenikova, E.I.; Makarova, M.N.; Pozharitskaya, O.N.; Medvedev, O.S. Evaluation of cardioprotective efficacy of innovative dosage form of ubiqinol for intravenous administration. Eksperimental’naya Klin. Farmakol. 2018, 81, 8–11. [Google Scholar]
- Botelho, A.F.M.; Lempek, M.R.; Branco, S.; Nogueira, M.M.; de Almeida, M.E.; Costa, A.G.; Freitas, T.G.; Rocha, M.; Moreira, M.V.L.; Barreto, T.O.; et al. Coenzyme Q10 Cardioprotective Effects Against Doxorubicin-Induced Cardiotoxicity in Wistar Rat. Cardiovasc. Toxicol. 2020, 20, 222–234. [Google Scholar] [CrossRef]
- Ulla, A.; Mohamed, M.K.; Sikder, B.; Rahman, A.T.; Sumi, F.A.; Hossain, M.; Reza, H.M.; Rahman, G.M.S.; Alam, M.A. Coenzyme Q10 prevents oxidative stress and fibrosis in isoprenaline induced cardiac remodeling in aged rats. BMC Pharmacol. Toxicol. 2017, 18, 29. [Google Scholar] [CrossRef] [Green Version]
- Gairola, C.G.; Howatt, D.A.; Daugherty, A. Dietary coenzyme Q10 does not protect against cigarette smoke-augmented atherosclerosis in apoE-deficient mice. Free Radic. Biol. Med. 2010, 48, 1535–1539. [Google Scholar] [CrossRef]
- Xie, T.; Wang, C.; Jin, Y.; Meng, Q.; Liu, Q.; Wu, J.; Sun, H. CoenzymeQ10-Induced Activation of AMPK-YAP-OPA1 Pathway Alleviates Atherosclerosis by Improving Mitochondrial Function, Inhibiting Oxidative Stress and Promoting Energy Metabolism. Front. Pharmacol. 2020, 11, 1034. [Google Scholar] [CrossRef]
- Dudylina, A.L.; Ivanova, M.V.; Kalatanova, A.V.; Kalenikova, E.I.; Makarov, V.G.; Makarova, M.N.; Shumaev, K.B.; Ruuge, E.K. The generation of superoxide radicals by cardiac mitochondria and the antioxidant effect of the water-soluble form of ubiquinol-10. Cell Biophys. 2019, 64, 203–208. [Google Scholar] [CrossRef]
- Gharib, A.; De Paulis, D.; Li, B.; Augeul, L.; Couture-Lepetit, E.; Gomez, L.; Angoulvant, D.; Ovize, M. Opposite and tissue-specific effects of coenzyme Q2 on mPTP opening and ROS production between heart and liver mitochondria: Role of complex I. J. Mol. Cell Cardiol. 2012, 52, 1091–1095. [Google Scholar] [CrossRef]
- Giorgi, C.; Agnoletto, C.; Bononi, A.; Bonora, M.; De Marchi, E.; Marchi, S.; Missiroli, S.; Patergnani, S.; Poletti, F.; Rimessi, A.; et al. Mitochondrial calcium homeostasis as potential target for mitochondrial medicine. Mitochondrion 2012, 12, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Mortensen, S.A.; Rosenfeldt, F.; Kumar, A.; Dolliner, P.; Filipiak, K.J.; Pella, D.; Alehagen, U.; Steurer, G.; Littarru, G.P.; Q-SYMBIO Study Investigators. The effect of coenzyme Q10 on morbidity and mortality in chronic heart failure: Results from Q-SYMBIO: A randomized double-blind trial. JACC Heart Fail. 2014, 2, 641–649. [Google Scholar] [CrossRef]
- Mortensen, A.L.; Rosenfeldt, F.; Filipiak, K.J. Effect of coenzyme Q10 in Europeans with chronic heart failure: A sub-group analysis of the Q-SYMBIO randomized double-blind trial. Cardiol. J. 2019, 26, 147–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, Q.; Kebbati, A.H.; Zhang, Y.; Tang, Y.; Okello, E.; Huang, C. Effect of coenzyme Q10 on the incidence of atrial fibrillation in patients with heart failure. J. Investig. Med. 2015, 63, 735–739. [Google Scholar] [CrossRef]
- Alehagen, U.; Aaseth, J.; Johansson, P. Reduced Cardiovascular Mortality 10 Years after Supplementation with Selenium and Coenzyme Q10 for Four Years: Follow-Up Results of a Prospective Randomized Double-Blind Placebo-Controlled Trial in Elderly Citizens. PLoS ONE 2015, 10, e0141641. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.J.; Yen, C.H.; Hsu, H.C.; Lin, J.Y.; Hsia, S.; Lin, P.T. A significant correlation between the plasma levels of coenzyme Q10 and vitamin B-6 and a reduced risk of coronary artery disease. Nutr. Res. 2012, 32, 751–756. [Google Scholar] [CrossRef]
- Lee, B.J.; Huang, Y.C.; Chen, S.J.; Lin, P.T. Coenzyme Q10 supplementation reduces oxidative stress and increases antioxidant enzyme activity in patients with coronary artery disease. Nutrition 2012, 28, 250–255. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.J.; Tseng, Y.F.; Yen, C.H.; Lin, P.T. Effects of coenzyme Q10 supplementation (300 mg/day) on antioxidation and anti-inflammation in coronary artery disease patients during statins therapy: A randomized, placebo-controlled trial. Nutr. J. 2013, 12, 142. [Google Scholar] [CrossRef] [Green Version]
- Orlando, P.; Sabbatinelli, J.; Silvestri, S.; Marcheggiani, F.; Cirilli, I.; Dludla, P.V.; Molardi, A.; Nicolini, F.; Tiano, L. Ubiquinol supplementation in elderly patients undergoing aortic valve replacement: Biochemical and clinical aspects. Aging 2020, 12, 15514–15531. [Google Scholar] [CrossRef]
- Bagheri Nesami, N.; Mozaffari-Khosravi, H.; Najarzadeh, A.; Salehifar, E. The Effect of Coenzyme Q10 Supplementation on Pro-Inflammatory Factors and Adiponectin in Mildly Hypertensive Patients: A Randomized, Double-Blind, Placebo-Controlled Trial. Int. J. Vitam. Nutr. Res. 2015, 85, 156–164. [Google Scholar] [CrossRef]
- Mohseni, M.; Vafa, M.; Zarrati, M.; Shidfar, F.; Hajimiresmail, S.J.; Rahimi Forushani, A. Beneficial Effects of Coenzyme Q10 Supplementation on Lipid Profile and Intereukin-6 and Intercellular Adhesion Molecule-1 Reduction, Preliminary Results of a Double-blind Trial in Acute Myocardial Infarction. Int. J. Prev. Med. 2015, 6, 73. [Google Scholar] [CrossRef] [PubMed]
- Endemann, D.H.; Schiffrin, E.L. Endothelial dysfunction. J. Am. Soc. Nephrol. 2004, 15, 1983–1992. [Google Scholar] [CrossRef] [PubMed]
- Dai, Y.L.; Luk, T.H.; Yiu, K.H.; Wang, M.; Yip, P.M.; Lee, S.W.; Li, S.W.; Tam, S.; Fong, B.; Lau, C.P.; et al. Reversal of mitochondrial dysfunction by coenzyme Q10 supplement improves endothelial function in patients with ischaemic left ventricular systolic dysfunction: A randomized controlled trial. Atherosclerosis 2011, 216, 395–401. [Google Scholar] [CrossRef] [PubMed]
- Kawashima, C.; Matsuzawa, Y.; Konishi, M.; Akiyama, E.; Suzuki, H.; Sato, R.; Nakahashi, H.; Kikuchi, S.; Kimura, Y.; Maejima, N.; et al. Ubiquinol Improves Endothelial Function in Patients with Heart Failure with Reduced Ejection Fraction: A Single-Center, Randomized Double-Blind Placebo-Controlled Crossover Pilot Study. Am. J. Cardiovasc/Drugs 2020, 20, 363–372. [Google Scholar] [CrossRef] [PubMed]
- Perez-Sanchez, C.; Ruiz-Limon, P.; Aguirre, M.A.; Bertolaccini, M.L.; Khamashta, M.A.; Rodriguez-Ariza, A.; Segui, P.; Collantes-Estevez, E.; Barbarroja, N.; Khraiwesh, H.; et al. Mitochondrial dysfunction in antiphospholipid syndrome: Implications in the pathogenesis of the disease and effects of coenzyme Q(10) treatment. Blood 2012, 119, 5859–5870. [Google Scholar] [CrossRef] [Green Version]
- Raitakari, O.T.; McCredie, R.J.; Witting, P.; Griffiths, K.A.; Letters, J.; Sullivan, D.; Stocker, R.; Celermajer, D.S. Coenzyme Q improves LDL resistance to ex vivo oxidation but does not enhance endothelial function in hypercholesterolemic young adults. Free Radic. Biol. Med. 2000, 28, 1100–1105. [Google Scholar] [CrossRef]
- Sabbatinelli, J.; Orlando, P.; Galeazzi, R.; Silvestri, S.; Cirilli, I.; Marcheggiani, F.; Dludla, P.V.; Giuliani, A.; Bonfigli, A.R.; Mazzanti, L.; et al. Ubiquinol Ameliorates Endothelial Dysfunction in Subjects with Mild-to-Moderate Dyslipidemia: A Randomized Clinical Trial. Nutrients 2020, 12, 1098. [Google Scholar] [CrossRef] [Green Version]
- Langsjoen, P.H.; Langsjoen, A.M. Comparison study of plasma coenzyme Q10 levels in healthy subjects supplemented with ubiquinol versus ubiquinone. Clin. Pharmacol. Drug Dev. 2014, 3, 13–17. [Google Scholar] [CrossRef]
- Tournaye, H. Evidence-based management of male subfertility. Curr. Opin. Obstet. Gynecol. 2006, 18, 253–259. [Google Scholar] [CrossRef]
- Wang, Q.; Sun, Q.Y. Evaluation of oocyte quality: Morphological, cellular and molecular predictors. Reprod. Fertil. Dev. 2007, 19, 1–12. [Google Scholar] [CrossRef]
- Bykova, M.; Athayde, K.; Sharma, R.; Jha, R.; Sabanegh, E.; Agarwal, A. Defining the reference value of seminal reactive oxygen species in a population of infertile men and normal healthy volunteers. Fertil. Steril. 2007, 88. [Google Scholar] [CrossRef]
- Miao, Y.L.; Kikuchi, K.; Sun, Q.Y.; Schatten, H. Oocyte aging: Cellular and molecular changes, developmental potential and reversal possibility. Hum. Reprod. Update 2009, 15, 573–585. [Google Scholar] [CrossRef] [Green Version]
- Tremellen, K. Oxidative stress and male infertility—A clinical perspective. Hum. Reprod. Update 2008, 14, 243–258. [Google Scholar] [CrossRef] [PubMed]
- Alahmar, A.T.; Calogero, A.E.; Sengupta, P.; Dutta, S. Coenzyme Q10 Improves Sperm Parameters, Oxidative Stress Markers and Sperm DNA Fragmentation in Infertile Patients with Idiopathic Oligoasthenozoospermia. World J. Men’s Health 2021, 39, 346–351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nadjarzadeh, A.; Shidfar, F.; Amirjannati, N.; Vafa, M.R.; Motevalian, S.A.; Gohari, M.R.; Nazeri Kakhki, S.A.; Akhondi, M.M.; Sadeghi, M.R. Effect of Coenzyme Q10 supplementation on antioxidant enzymes activity and oxidative stress of seminal plasma: A double-blind randomised clinical trial. Andrologia 2014, 46, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Cakiroglu, B.; Eyyupoglu, S.E.; Gozukucuk, R.; Uyanik, B.S. Ubiquinol effect on sperm parameters in subfertile men who have astheno-teratozoospermia with normal sperm concentration. Nephrourol. Mon. 2014, 6, e16870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Safarinejad, M.R.; Safarinejad, S.; Shafiei, N.; Safarinejad, S. Effects of the reduced form of coenzyme Q10 (ubiquinol) on semen parameters in men with idiopathic infertility: A double-blind, placebo controlled, randomized study. J. Urol. 2012, 188, 526–531. [Google Scholar] [CrossRef] [Green Version]
- Tirabassi, G.; Vignini, A.; Tiano, L.; Buldreghini, E.; Bruge, F.; Silvestri, S.; Orlando, P.; D’Aniello, A.; Mazzanti, L.; Lenzi, A.; et al. Protective effects of coenzyme Q10 and aspartic acid on oxidative stress and DNA damage in subjects affected by idiopathic asthenozoospermia. Endocrine 2015, 49, 549–552. [Google Scholar] [CrossRef]
- Safarinejad, M.R. The effect of coenzyme Q(1)(0) supplementation on partner pregnancy rate in infertile men with idiopathic oligoasthenoteratozoospermia: An open-label prospective study. Int. Urol. Nephrol. 2012, 44, 689–700. [Google Scholar] [CrossRef]
- Gvozdjakova, A.; Kucharska, J.; Dubravicky, J.; Mojto, V.; Singh, R.B. Coenzyme Q(1)(0), alpha-tocopherol, and oxidative stress could be important metabolic biomarkers of male infertility. Dis. Mark. 2015, 2015, 827941. [Google Scholar] [CrossRef] [Green Version]
- Kobori, Y.; Ota, S.; Sato, R.; Yagi, H.; Soh, S.; Arai, G.; Okada, H. Antioxidant cosupplementation therapy with vitamin C, vitamin E, and coenzyme Q10 in patients with oligoasthenozoospermia. Arch. Ital. Urol. Androl. 2014, 86, 1–4. [Google Scholar] [CrossRef]
- Giannubilo, S.R.; Orlando, P.; Silvestri, S.; Cirilli, I.; Marcheggiani, F.; Ciavattini, A.; Tiano, L. CoQ10 Supplementation in Patients Undergoing IVF-ET: The Relationship with Follicular Fluid Content and Oocyte Maturity. Antioxidants 2018, 7, 141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gat, I.; Blanco Mejia, S.; Balakier, H.; Librach, C.L.; Claessens, A.; Ryan, E.A. The use of coenzyme Q10 and DHEA during IUI and IVF cycles in patients with decreased ovarian reserve. Gynecol. Endocrinol. 2016, 32, 534–537. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Nisenblat, V.; Lu, C.; Li, R.; Qiao, J.; Zhen, X.; Wang, S. Pretreatment with coenzyme Q10 improves ovarian response and embryo quality in low-prognosis young women with decreased ovarian reserve: A randomized controlled trial. Reprod. Biol. Endocrinol. 2018, 16, 29. [Google Scholar] [CrossRef] [PubMed]
- Bentov, Y.; Hannam, T.; Jurisicova, A.; Esfandiari, N.; Casper, R.F. Coenzyme Q10 Supplementation and Oocyte Aneuploidy in Women Undergoing IVF-ICSI Treatment. Clin. Med. Insights Reprod. Health 2014, 8, 31–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Said, R.S.; Mohamed, H.A.; Kamal, M.M. Coenzyme Q10 mitigates ionizing radiation-induced testicular damage in rats through inhibition of oxidative stress and mitochondria-mediated apoptotic cell death. Toxicol. Appl. Pharmacol. 2019, 383, 114780. [Google Scholar] [CrossRef]
- Delkhosh, A.; Delashoub, M.; Tehrani, A.A.; Bahrami, A.M.; Niazi, V.; Shoorei, H.; Banimohammad, M.; Kalarestaghi, H.; Shokoohi, M.; Agabalazadeh, A.; et al. Upregulation of FSHR and PCNA by administration of coenzyme Q10 on cyclophosphamide-induced premature ovarian failure in a mouse model. J. Biochem. Mol. Toxicol. 2019, 33, e22398. [Google Scholar] [CrossRef]
- Zhang, M.; ShiYang, X.; Zhang, Y.; Miao, Y.; Chen, Y.; Cui, Z.; Xiong, B. Coenzyme Q10 ameliorates the quality of postovulatory aged oocytes by suppressing DNA damage and apoptosis. Free Radic. Biol. Med. 2019, 143, 84–94. [Google Scholar] [CrossRef]
- Niu, Y.J.; Zhou, W.; Nie, Z.W.; Zhou, D.; Xu, Y.N.; Ock, S.A.; Yan, C.G.; Cui, X.S. Ubiquinol-10 delays postovulatory oocyte aging by improving mitochondrial renewal in pigs. Aging 2020, 12, 1256–1271. [Google Scholar] [CrossRef]
- Ben-Meir, A.; Burstein, E.; Borrego-Alvarez, A.; Chong, J.; Wong, E.; Yavorska, T.; Naranian, T.; Chi, M.; Wang, Y.; Bentov, Y.; et al. Coenzyme Q10 restores oocyte mitochondrial function and fertility during reproductive aging. Aging Cell 2015, 14, 887–895. [Google Scholar] [CrossRef]
- Radak, Z.; Zhao, Z.; Koltai, E.; Ohno, H.; Atalay, M. Oxygen consumption and usage during physical exercise: The balance between oxidative stress and ROS-dependent adaptive signaling. Antioxid. Redox Signal. 2013, 18, 1208–1246. [Google Scholar] [CrossRef] [Green Version]
- Guescini, M.; Tiano, L.; Genova, M.L.; Polidori, E.; Silvestri, S.; Orlando, P.; Fimognari, C.; Calcabrini, C.; Stocchi, V.; Sestili, P. The Combination of Physical Exercise with Muscle-Directed Antioxidants to Counteract Sarcopenia: A Biomedical Rationale for Pleiotropic Treatment with Creatine and Coenzyme Q10. Oxid. Med. Cell Longev. 2017, 2017, 7083049. [Google Scholar] [CrossRef] [Green Version]
- Orlando, P.; Silvestri, S.; Galeazzi, R.; Antonicelli, R.; Marcheggiani, F.; Cirilli, I.; Bacchetti, T.; Tiano, L. Effect of ubiquinol supplementation on biochemical and oxidative stress indexes after intense exercise in young athletes. Redox Rep. 2018, 23, 136–145. [Google Scholar] [CrossRef] [PubMed]
- Fischer, A.; Onur, S.; Niklowitz, P.; Menke, T.; Laudes, M.; Rimbach, G.; Doring, F. Coenzyme Q10 Status as a Determinant of Muscular Strength in Two Independent Cohorts. PLoS ONE 2016, 11, e0167124. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyere, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [Green Version]
- Andreani, C.; Bartolacci, C.; Guescini, M.; Battistelli, M.; Stocchi, V.; Orlando, F.; Provinciali, M.; Amici, A.; Marchini, C.; Tiano, L.; et al. Combination of Coenzyme Q10 Intake and Moderate Physical Activity Counteracts Mitochondrial Dysfunctions in a SAMP8 Mouse Model. Oxid. Med. Cell Longev. 2018, 2018, 8936251. [Google Scholar] [CrossRef] [Green Version]
- Christiansen, L.B.; Dohlmann, T.L.; Ludvigsen, T.P.; Parfieniuk, E.; Ciborowski, M.; Szczerbinski, L.; Kretowski, A.; Desler, C.; Tiano, L.; Orlando, P.; et al. Atorvastatin impairs liver mitochondrial function in obese Gottingen Minipigs but heart and skeletal muscle are not affected. Sci. Rep. 2021, 11, 2167. [Google Scholar] [CrossRef]
- La Guardia, P.G.; Alberici, L.C.; Ravagnani, F.G.; Catharino, R.R.; Vercesi, A.E. Protection of rat skeletal muscle fibers by either L-carnitine or coenzyme Q10 against statins toxicity mediated by mitochondrial reactive oxygen generation. Front. Physiol. 2013, 4, 103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, L.W.; Jabbour, A.; Hayward, C.S.; Furlong, T.J.; Girgis, L.; Macdonald, P.S.; Keogh, A.M. Potential role of coenzyme Q10 in facilitating recovery from statin-induced rhabdomyolysis. Intern. Med. J. 2015, 45, 451–453. [Google Scholar] [CrossRef] [PubMed]
- Derosa, G.; D’Angelo, A.; Maffioli, P. Coenzyme q10 liquid supplementation in dyslipidemic subjects with statin-related clinical symptoms: A double-blind, randomized, placebo-controlled study. Drug Des. Devel. Ther. 2019, 13, 3647–3655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muraki, A.; Miyashita, K.; Mitsuishi, M.; Tamaki, M.; Tanaka, K.; Itoh, H. Coenzyme Q10 reverses mitochondrial dysfunction in atorvastatin-treated mice and increases exercise endurance. J. Appl. Physiol. (1985) 2012, 113, 479–486. [Google Scholar] [CrossRef] [Green Version]
- Piercy, K.L.; Troiano, R.P.; Ballard, R.M.; Carlson, S.A.; Fulton, J.E.; Galuska, D.A.; George, S.M.; Olson, R.D. The Physical Activity Guidelines for Americans. JAMA 2018, 320, 2020–2028. [Google Scholar] [CrossRef] [PubMed]
- Simon, H.B. Exercise and Health: Dose and Response, Considering Both Ends of the Curve. Am. J. Med. 2015, 128, 1171–1177. [Google Scholar] [CrossRef] [PubMed]
- Diaz-Castro, J.; Moreno-Fernandez, J.; Chirosa, I.; Chirosa, L.J.; Guisado, R.; Ochoa, J.J. Beneficial Effect of Ubiquinol on Hematological and Inflammatory Signaling during Exercise. Nutrients 2020, 12, 424. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, K.; Yamada, M.; Kurakake, S.; Okamura, N.; Yamaya, K.; Liu, Q.; Kudoh, S.; Kowatari, K.; Nakaji, S.; Sugawara, K. Circulating cytokines and hormones with immunosuppressive but neutrophil-priming potentials rise after endurance exercise in humans. Eur. J. Appl. Physiol. 2000, 81, 281–287. [Google Scholar] [CrossRef]
- Chen, H.C.; Huang, C.C.; Lin, T.J.; Hsu, M.C.; Hsu, Y.J. Ubiquinol Supplementation Alters Exercise Induced Fatigue by Increasing Lipid Utilization in Mice. Nutrients 2019, 11, 2550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarmiento, A.; Diaz-Castro, J.; Pulido-Moran, M.; Moreno-Fernandez, J.; Kajarabille, N.; Chirosa, I.; Guisado, I.M.; Javier Chirosa, L.; Guisado, R.; Ochoa, J.J. Short-term ubiquinol supplementation reduces oxidative stress associated with strenuous exercise in healthy adults: A randomized trial. Biofactors 2016, 42, 612–622. [Google Scholar] [CrossRef]
- Bloomer, R.J.; Canale, R.E.; McCarthy, C.G.; Farney, T.M. Impact of oral ubiquinol on blood oxidative stress and exercise performance. Oxid. Med. Cell Longev. 2012, 2012, 465020. [Google Scholar] [CrossRef] [Green Version]
- Gul, I.; Gokbel, H.; Belviranli, M.; Okudan, N.; Buyukbas, S.; Basarali, K. Oxidative stress and antioxidant defense in plasma after repeated bouts of supramaximal exercise: The effect of coenzyme Q10. J. Sports Med. Phys. Fitness 2011, 51, 305–312. [Google Scholar]
- Emmanuele, V.; Lopez, L.C.; Berardo, A.; Naini, A.; Tadesse, S.; Wen, B.; D’Agostino, E.; Solomon, M.; DiMauro, S.; Quinzii, C.; et al. Heterogeneity of coenzyme Q10 deficiency: Patient study and literature review. Arch. Neurol. 2012, 69, 978–983. [Google Scholar] [CrossRef] [Green Version]
- Yubero, D.; Montero, R.; Martin, M.A.; Montoya, J.; Ribes, A.; Grazina, M.; Trevisson, E.; Rodriguez-Aguilera, J.C.; Hargreaves, I.P.; Salviati, L.; et al. Secondary coenzyme Q10 deficiencies in oxidative phosphorylation (OXPHOS) and non-OXPHOS disorders. Mitochondrion 2016, 30, 51–58. [Google Scholar] [CrossRef]
- Berardo, A.; Quinzii, C.M. Redefining infantile-onset multisystem phenotypes of coenzyme Q10-deficiency in the next-generation sequencing era. J. Transl. Genet. Genom. 2020, 4, 22–35. [Google Scholar] [CrossRef] [PubMed]
- Salviati, L.; Trevisson, E.; Doimo, M.; Navas, P. Primary Coenzyme Q10 Deficiency. In GeneReviews((R)); Adam, M.P., Ardinger, H.H., Pagon, R.A., Wallace, S.E., Bean, L.J.H., Mirzaa, G., Amemiya, A., Eds.; University of Washington: Seattle, WA, USA, 2017. [Google Scholar]
- Montero, R.; Yubero, D.; Salgado, M.C.; Gonzalez, M.J.; Campistol, J.; O’Callaghan, M.D.M.; Pineda, M.; Delgadillo, V.; Maynou, J.; Fernandez, G.; et al. Plasma coenzyme Q10 status is impaired in selected genetic conditions. Sci. Rep. 2019, 9, 793. [Google Scholar] [CrossRef] [PubMed]
- Neergheen, V.; Hargreaves, I.P. Secondary Coenzyme Q10 Deficiency: Causes and Consequence; Grigoryeva, S., Ed.; NOVA Biomedical: New York, NY, USA, 2018. [Google Scholar]
- Yubero, D.; Montero, R.; Artuch, R.; Land, J.M.; Heales, S.J.; Hargreaves, I.P. Biochemical diagnosis of coenzyme q10 deficiency. Mol. Syndromol. 2014, 5, 147–155. [Google Scholar] [CrossRef] [Green Version]
- Wainwright, L.; Hargreaves, I.P.; Georgian, A.R.; Turner, C.; Dalton, R.N.; Abbott, N.J.; Heales, S.J.R.; Preston, J.E. CoQ10 Deficient Endothelial Cell Culture Model for the Investigation of CoQ10 Blood-Brain Barrier Transport. J. Clin. Med. 2020, 9, 3236. [Google Scholar] [CrossRef]
- Mancuso, M.; Orsucci, D.; Volpi, L.; Calsolaro, V.; Siciliano, G. Coenzyme Q10 in neuromuscular and neurodegenerative disorders. Curr. Drug Targets 2010, 11, 111–121. [Google Scholar] [CrossRef] [Green Version]
- Salama, M.; Yuan, T.F.; Machado, S.; Murillo-Rodriguez, E.; Vega, J.A.; Menendez-Gonzalez, M.; Nardi, A.E.; Arias-Carrion, O. Co-enzyme Q10 to treat neurological disorders: Basic mechanisms, clinical outcomes, and future research direction. CNS Neurol. Disord. Drug Targets 2013, 12, 641–664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duran-Prado, M.; Frontinan, J.; Santiago-Mora, R.; Peinado, J.R.; Parrado-Fernandez, C.; Gomez-Almagro, M.V.; Moreno, M.; Lopez-Dominguez, J.A.; Villalba, J.M.; Alcain, F.J. Coenzyme Q10 protects human endothelial cells from beta-amyloid uptake and oxidative stress-induced injury. PLoS ONE 2014, 9, e109223. [Google Scholar] [CrossRef]
- Komaki, H.; Faraji, N.; Komaki, A.; Shahidi, S.; Etaee, F.; Raoufi, S.; Mirzaei, F. Investigation of protective effects of coenzyme Q10 on impaired synaptic plasticity in a male rat model of Alzheimer’s disease. Brain Res. Bull. 2019, 147, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Zaki, M.E.; El-Bassyouni, H.T.; Tosson, A.M.; Youness, E.; Hussein, J. Coenzyme Q10 and pro-inflammatory markers in children with Down syndrome: Clinical and biochemical aspects. J. Pediatr. Rio J. 2017, 93, 100–104. [Google Scholar] [CrossRef] [Green Version]
- Tiano, L.; Carnevali, P.; Padella, L.; Santoro, L.; Principi, F.; Bruge, F.; Carle, F.; Gesuita, R.; Gabrielli, O.; Littarru, G.P. Effect of Coenzyme Q10 in mitigating oxidative DNA damage in Down syndrome patients, a double blind randomized controlled trial. Neurobiol. Aging 2011, 32, 2103–2105. [Google Scholar] [CrossRef]
- Larsen, E.L.; Padella, L.; Bergholdt, H.K.M.; Henriksen, T.; Santoro, L.; Gabrielli, O.; Poulsen, H.E.; Littarru, G.P.; Orlando, P.; Tiano, L. The effect of long-term treatment with coenzyme Q10 on nucleic acid modifications by oxidation in children with Down syndrome. Neurobiol. Aging 2018, 67, 159–161. [Google Scholar] [CrossRef]
- Miles, M.V.; Patterson, B.J.; Chalfonte-Evans, M.L.; Horn, P.S.; Hickey, F.J.; Schapiro, M.B.; Steele, P.E.; Tang, P.H.; Hotze, S.L. Coenzyme Q10 (ubiquinol-10) supplementation improves oxidative imbalance in children with trisomy 21. Pediatr. Neurol. 2007, 37, 398–403. [Google Scholar] [CrossRef]
- Chang, K.H.; Chen, C.M. The Role of Oxidative Stress in Parkinson’s Disease. Antioxidants 2020, 9, 597. [Google Scholar] [CrossRef] [PubMed]
- Park, H.W.; Park, C.G.; Park, M.; Lee, S.H.; Park, H.R.; Lim, J.; Paek, S.H.; Choy, Y.B. Intrastriatal administration of coenzyme Q10 enhances neuroprotection in a Parkinson’s disease rat model. Sci. Rep. 2020, 10, 9572. [Google Scholar] [CrossRef] [PubMed]
- Sanoobar, M.; Eghtesadi, S.; Azimi, A.; Khalili, M.; Jazayeri, S.; Reza Gohari, M. Coenzyme Q10 supplementation reduces oxidative stress and increases antioxidant enzyme activity in patients with relapsing-remitting multiple sclerosis. Int. J. Neurosci. 2013, 123, 776–782. [Google Scholar] [CrossRef]
- Garcia-Corzo, L.; Luna-Sanchez, M.; Doerrier, C.; Ortiz, F.; Escames, G.; Acuna-Castroviejo, D.; Lopez, L.C. Ubiquinol-10 ameliorates mitochondrial encephalopathy associated with CoQ deficiency. Biochim. Biophys. Acta 2014, 1842, 893–901. [Google Scholar] [CrossRef] [Green Version]
- Gupta, B.K.; Kumar, S.; Kaur, H.; Ali, J.; Baboota, S. Attenuation of Oxidative Damage by Coenzyme Q 10 Loaded Nanoemulsion Through Oral Route for the Management of Parkinson’s Disease. Rejuvenation Res. 2018, 21, 232–248. [Google Scholar] [CrossRef] [PubMed]
- Sadeghiyan Galeshkalami, N.; Abdollahi, M.; Najafi, R.; Baeeri, M.; Jamshidzade, A.; Falak, R.; Davoodzadeh Gholami, M.; Hassanzadeh, G.; Mokhtari, T.; Hassani, S.; et al. Alpha-lipoic acid and coenzyme Q10 combination ameliorates experimental diabetic neuropathy by modulating oxidative stress and apoptosis. Life Sci. 2019, 216, 101–110. [Google Scholar] [CrossRef]
- Shi, T.J.; Zhang, M.D.; Zeberg, H.; Nilsson, J.; Grunler, J.; Liu, S.X.; Xiang, Q.; Persson, J.; Fried, K.J.; Catrina, S.B.; et al. Coenzyme Q10 prevents peripheral neuropathy and attenuates neuron loss in the db-/db- mouse, a type 2 diabetes model. Proc. Natl. Acad. Sci. USA 2013, 110, 690–695. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.P.; Eber, A.; Yuan, Y.; Yang, Z.; Rodriguez, Y.; Levitt, R.C.; Takacs, P.; Candiotti, K.A. Prophylactic and antinociceptive effects of coenzyme Q10 on diabetic neuropathic pain in a mouse model of type 1 diabetes. Anesthesiology 2013, 118, 945–954. [Google Scholar] [CrossRef] [Green Version]
- Ahmadvand, H.; Tavafi, M.; Khosrowbeygi, A. Amelioration of altered antioxidant enzymes activity and glomerulosclerosis by coenzyme Q10 in alloxan-induced diabetic rats. J. Diabetes Complicat. 2012, 26, 476–482. [Google Scholar] [CrossRef] [PubMed]
- Tsai, H.Y.; Lin, C.P.; Huang, P.H.; Li, S.Y.; Chen, J.S.; Lin, F.Y.; Chen, J.W.; Lin, S.J. Coenzyme Q10 Attenuates High Glucose-Induced Endothelial Progenitor Cell Dysfunction through AMP-Activated Protein Kinase Pathways. J. Diabetes Res. 2016, 2016, 6384759. [Google Scholar] [CrossRef] [Green Version]
- Sun, J.; Zhu, H.; Wang, X.; Gao, Q.; Li, Z.; Huang, H. CoQ10 ameliorates mitochondrial dysfunction in diabetic nephropathy through mitophagy. Endocrinology 2019, 240, 445–465. [Google Scholar] [CrossRef] [PubMed]
- Tarry-Adkins, J.L.; Fernandez-Twinn, D.S.; Madsen, R.; Chen, J.H.; Carpenter, A.; Hargreaves, I.P.; McConnell, J.M.; Ozanne, S.E. Coenzyme Q10 Prevents Insulin Signaling Dysregulation and Inflammation Prior to Development of Insulin Resistance in Male Offspring of a Rat Model of Poor Maternal Nutrition and Accelerated Postnatal Growth. Endocrinology 2015, 156, 3528–3537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ustuner, M.A.; Kaman, D.; Colakoglu, N. Effects of benfotiamine and coenzyme Q10 on kidney damage induced gentamicin. Tissue Cell 2017, 49, 691–696. [Google Scholar] [CrossRef] [PubMed]
- Carrasco, J.; Anglada, F.J.; Campos, J.P.; Muntane, J.; Requena, M.J.; Padillo, J. The protective role of coenzyme Q10 in renal injury associated with extracorporeal shockwave lithotripsy: A randomised, placebo-controlled clinical trial. BJU Int. 2014, 113, 942–950. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.J.; Xu, Y.X.; Jia, H.P.; Zhang, L.; Cao, X.Y.; Zuo, X.W.; Cai, G.Y.; Chen, X.M. Associations of coenzyme Q10 with endothelial function in hemodialysis patients. Nephrology 2021, 26, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Farsi, F.; Mohammadshahi, M.; Alavinejad, P.; Rezazadeh, A.; Zarei, M.; Engali, K.A. Functions of coenzyme Q10 supplementation on liver enzymes, markers of systemic inflammation, and adipokines in patients affected by nonalcoholic fatty liver disease: A double-blind, placebo-controlled, randomized clinical trial. J. Am. Coll. Nutr. 2016, 35, 346–353. [Google Scholar] [CrossRef]
- Mohamed HA, S.R. Coenzyme Q10 attenuates inflammation and fibrosis implicated in radiation enteropathy through suppression of NF-kB/TGF-β/MMP-9 pathways. Int. Immunopharmacol. 2021, 92, 107347. [Google Scholar] [CrossRef]
- El-Sheikh, A.A.; Morsy, M.A.; Mahmoud, M.M.; Rifaai, R.A. Protective mechanisms of coenzyme-Q10 may involve up-regulation of testicular P-glycoprotein in doxorubicin-induced toxicity. Environ. Toxicol. Pharmacol. 2014, 37, 772–781. [Google Scholar] [CrossRef]
- Noh, Y.H.; Kim, K.Y.; Shim, M.S.; Choi, S.H.; Choi, S.; Ellisman, M.H.; Weinreb, R.N.; Perkins, G.A.; Ju, W.K. Inhibition of oxidative stress by coenzyme Q10 increases mitochondrial mass and improves bioenergetic function in optic nerve head astrocytes. Cell Death Dis. 2013, 4, e820. [Google Scholar] [CrossRef]
- Lee, D.; Shim, M.S.; Kim, K.Y.; Noh, Y.H.; Kim, H.; Kim, S.Y.; Weinreb, R.N.; Ju, W.K. Coenzyme Q10 inhibits glutamate excitotoxicity and oxidative stress-mediated mitochondrial alteration in a mouse model of glaucoma. Investig. Ophthalmol. Vis. Sci. 2014, 55, 993–1005. [Google Scholar] [CrossRef] [Green Version]
- Parisi, V.; Centofanti, M.; Gandolfi, S.; Marangoni, D.; Rossetti, L.; Tanga, L.; Tardini, M.; Traina, S.; Ungaro, N.; Vetrugno, M.; et al. Effects of coenzyme Q10 in conjunction with vitamin E on retinal-evoked and cortical-evoked responses in patients with open-angle glaucoma. J. Glaucoma 2014, 23, 391–404. [Google Scholar] [CrossRef] [PubMed]
- Arranz-Romera, A.; Davis, B.; Bravo-Osuna, I.; Esteban-Pérez, S.; Molina-Martínez, I.T.; Shamsher, E.; Ravindran, N.; Guo, L.; Cordeiro, M.F.; Herrero-Vanrell, R. Simultaneous co-delivery of neuroprotective drugs from multi-loaded PLGA microspheres for the treatment of glaucoma. J. Control. Release 2019, 297, 26–38. [Google Scholar] [CrossRef] [PubMed]
- Mencucci, R.; Favuzza, E.; Boccalini, C.; Lapucci, A.; Felici, R.; Resta, F.; Chiarugi, A.; Cavone, L. CoQ10-containing eye drops prevent UVB-induced cornea cell damage and increase cornea wound healing by preserving mitochondrial function. Investig. Ophthalmol. Vis. Sci. 2014, 55, 7266–7271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, D.; Kim, K.Y.; Shim, M.S.; Kim, S.Y.; Ellisman, M.H.; Weinreb, R.N.; Ju, W.K. Coenzyme Q10 ameliorates oxidative stress and prevents mitochondrial alteration in ischemic retinal injury. Apoptosis 2014, 19, 603–614. [Google Scholar] [CrossRef] [Green Version]
- Fernández-Vega, B.; Nicieza, J.; Álvarez-Barrios, A.; Álvarez, L.; García, M.; Fernández-Vega, C.; Vega, J.A.; González-Iglesias, H. The Use of Vitamins and Coenzyme Q10 for the Treatment of Vascular Occlusion Diseases Affecting the Retina. Nutrients 2020, 12, 723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cevenini, E.; Invidia, L.; Lescai, F.; Salvioli, S.; Tieri, P.; Castellani, G.; Franceschi, C. Human models of aging and longevity. Expert Opin. Biol. Ther. 2008, 8, 1393–1405. [Google Scholar] [CrossRef]
- Pardeike, J.; Schwabe, K.; Muller, R.H. Influence of nanostructured lipid carriers (NLC) on the physical properties of the Cutanova Nanorepair Q10 cream and the in vivo skin hydration effect. Int. J. Pharm. 2010, 396, 166–173. [Google Scholar] [CrossRef]
- Shindo, Y.; Witt, E.; Han, D.; Epstein, W.; Packer, L. Enzymic and non-enzymic antioxidants in epidermis and dermis of human skin. J. Investg. Dermatol. 1994, 102, 122–124. [Google Scholar] [CrossRef] [Green Version]
- Kalen, A.; Appelkvist, E.L.; Dallner, G. Age-related changes in the lipid compositions of rat and human tissues. Lipids 1989, 24, 579–584. [Google Scholar] [CrossRef]
- Passi, S.; De Pita, O.; Puddu, P.; Littarru, G.P. Lipophilic antioxidants in human sebum and aging. Free Radic. Res. 2002, 36, 471–477. [Google Scholar] [CrossRef]
- Ely, J.T.; Krone, C.A. A Brief Update on Ubiquinone Coenzyme Q10. J. Orthomol. Med. 2000, 15, 63–68. [Google Scholar]
- Marcheggiani, F.; Cirilli, I.; Orlando, P.; Silvestri, S.; Vogelsang, A.; Knott, A.; Blatt, T.; Weise, J.M.; Tiano, L. Modulation of Coenzyme Q10 content and oxidative status in human dermal fibroblasts using HMG-CoA reductase inhibitor over a broad range of concentrations. From mitohormesis to mitochondrial dysfunction and accelerated aging. Aging 2019, 11, 2565–2582. [Google Scholar] [CrossRef]
- Marcheggiani, F.; Kordes, S.; Cirilli, I.; Orlando, P.; Silvestri, S.; Vogelsang, A.; Moller, N.; Blatt, T.; Weise, J.M.; Damiani, E.; et al. Anti-ageing effects of ubiquinone and ubiquinol in a senescence model of human dermal fibroblasts. Free Radic. Biol. Med. 2021, 165, 282–288. [Google Scholar] [CrossRef]
- Zmitek, K.; Zmitek, J.; Rogl Butina, M.; Pogacnik, T. Effects of a Combination of Water-Soluble CoenzymeQ10 and Collagen on Skin Parameters and Condition:Results of a Randomised, Placebo-Controlled, Double-Blind Study. Nutrients 2020, 12, 618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zmitek, K.; Pogacnik, T.; Mervic, L.; Zmitek, J.; Pravst, I. The effect of dietary intake of coenzyme Q10 on skin parameters and condition: Results of a randomised, placebo-controlled, double-blind study. Biofactors 2017, 43, 132–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schniertshauer, D.; Gebhard, D.; Bergemann, J. Age-Dependent Loss of Mitochondrial Function in Epithelial Tissue Can Be Reversed by Coenzyme Q10. J. Aging Res. 2018, 2018, 6354680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knott, A.; Achterberg, V.; Smuda, C.; Mielke, H.; Sperling, G.; Dunckelmann, K.; Vogelsang, A.; Kruger, A.; Schwengler, H.; Behtash, M.; et al. Topical treatment with coenzyme Q10-containing formulas improves skin’s Q10 level and provides antioxidative effects. Biofactors 2015, 41, 383–390. [Google Scholar] [CrossRef] [PubMed]
- Yue, Y.; Zhou, H.; Liu, G.; Li, Y.; Yan, Z.; Duan, M. The advantages of a novel CoQ10 delivery system in skin photo-protection. Int. J. Pharm. 2010, 392, 57–63. [Google Scholar] [CrossRef]
- Bruge, F.; Damiani, E.; Puglia, C.; Offerta, A.; Armeni, T.; Littarru, G.P.; Tiano, L. Nanostructured lipid carriers loaded with CoQ10: Effect on human dermal fibroblasts under normal and UVA-mediated oxidative conditions. Int. J. Pharm. 2013, 455, 348–356. [Google Scholar] [CrossRef] [PubMed]
- El-Leithy, E.S.; Makky, A.M.; Khattab, A.M.; Hussein, D.G. Optimization of nutraceutical coenzyme Q10 nanoemulsion with improved skin permeability and anti-wrinkle efficiency. Drug Dev. Ind. Pharm. 2018, 44, 316–328. [Google Scholar] [CrossRef]
- Zhang, M.; Dang, L.; Guo, F.; Wang, X.; Zhao, W.; Zhao, R. Coenzyme Q10 enhances dermal elastin expression, inhibits IL-1α production and melanin synthesis in vitro. Int. J. Cosmet. Sci. 2012, 34, 273–279. [Google Scholar] [CrossRef]
- Kurban, S.; Mehmetoglu, I. Effects of acetylsalicylic acid on serum paraoxonase activity, Ox-LDL, coenzyme Q10 and other oxidative stress markers in healthy volunteers. Clin. Biochem. 2010, 43, 287–290. [Google Scholar] [CrossRef] [PubMed]
- Fumagalli, S.; Fattirolli, F.; Guarducci, L.; Cellai, T.; Baldasseroni, S.; Tarantini, F.; Di Bari, M.; Masotti, G.; Marchionni, N. Coenzyme Q10 terclatrate and creatine in chronic heart failure: A randomized, placebo-controlled, double-blind study. Clin. Cardiol. 2011, 34, 211–217. [Google Scholar] [CrossRef]
- Mikhin, V.P.; Kharchenko, A.V.; Rosliakova, E.A.; Cherniatina, M.A. Application of coenzyme Q(10) in combination therapy of arterial hypertension. Kardiologiia 2011, 51, 26–31. [Google Scholar] [PubMed]
- Toyama, K.; Sugiyama, S.; Oka, H.; Iwasaki, Y.; Tomoko, H.; Shinji Tayama, H.; Jinnouchi, H.; Matsui, K.; Ogawa, H. Rosuvastatin combined with regular exercise preserves coenzyme Q10 levels associated with a significant increase in high-density lipoprotein cholesterol in patients with coronary artery disease. Atherosclerosis 2011, 217, 158–164. [Google Scholar] [CrossRef]
- Young, J.M.; Molyneux, S.L.; Reinheimer, A.M.; Florkowski, C.M.; Frampton, C.M.; Scott, R.S.; George, P.M. Relationship between plasma coenzyme Q10, asymmetric dimethylarginine and arterial stiffness in patients with phenotypic or genotypic familial hypercholesterolemia on long-term statin therapy. Atherosclerosis 2011, 218, 188–193. [Google Scholar] [CrossRef]
- Brugè, F.; Bacchetti, T.; Principi, F.; Scarpa, E.S.; Littarru, G.P.; Tiano, L. Olive oil supplemented with Coenzyme Q(10): Effect on plasma and lipoprotein oxidative status. Biofactors 2012, 38, 249–256. [Google Scholar] [CrossRef]
- Larijani, N.V.; Ahmadi, N.; Zeb, I.; Khan, F.; Flores, F.; Budoff, M. Beneficial effects of aged garlic extract and coenzyme Q10 on vascular elasticity and endothelial function: The FAITH randomized clinical trial. Nutrition 2013, 29, 71–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharp, J.; Farha, S.; Park, M.M.; Comhair, S.A.; Lundgrin, E.L.; Tang, W.H.W.; Bongard, R.D.; Merker, M.P.; Erzurum, S.C. Coenzyme Q supplementation in pulmonary arterial hypertension. Redox Biol. 2014, 2, 884–891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pérez-Sánchez, C.; Aguirre, M.A.; Ruiz-Limón, P.; Ábalos-Aguilera, M.C.; Jiménez-Gómez, Y.; Arias-de la Rosa, I.; Rodriguez-Ariza, A.; Fernández-Del Río, L.; González-Reyes, J.A.; Segui, P.; et al. Ubiquinol Effects on Antiphospholipid Syndrome Prothrombotic Profile: A Randomized, Placebo-Controlled Trial. Arterioscler. Thromb. Vasc. Biol. 2017, 37, 1923–1932. [Google Scholar] [CrossRef] [Green Version]
- Shikh, E.; Zozina, V.; Kondratenko, S.; Melnikov, E.; Kukes, V. The particulars of certain drugs’ effect on the endogenous coenzyme Q10 plasma level in patients with cardiovascular diseases. Drug Metab. Pers. Ther. 2020, 35. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cirilli, I.; Damiani, E.; Dludla, P.V.; Hargreaves, I.; Marcheggiani, F.; Millichap, L.E.; Orlando, P.; Silvestri, S.; Tiano, L. Role of Coenzyme Q10 in Health and Disease: An Update on the Last 10 Years (2010–2020). Antioxidants 2021, 10, 1325. https://doi.org/10.3390/antiox10081325
Cirilli I, Damiani E, Dludla PV, Hargreaves I, Marcheggiani F, Millichap LE, Orlando P, Silvestri S, Tiano L. Role of Coenzyme Q10 in Health and Disease: An Update on the Last 10 Years (2010–2020). Antioxidants. 2021; 10(8):1325. https://doi.org/10.3390/antiox10081325
Chicago/Turabian StyleCirilli, Ilenia, Elisabetta Damiani, Phiwayinkosi Vusi Dludla, Iain Hargreaves, Fabio Marcheggiani, Lauren Elizabeth Millichap, Patrick Orlando, Sonia Silvestri, and Luca Tiano. 2021. "Role of Coenzyme Q10 in Health and Disease: An Update on the Last 10 Years (2010–2020)" Antioxidants 10, no. 8: 1325. https://doi.org/10.3390/antiox10081325