
Antioxidant-Based Therapy Reduces Early-Stage Intestinal Ischemia-Reperfusion Injury in Rats


 and
and
Abstract
:1. Introduction
2. Materials and Methods
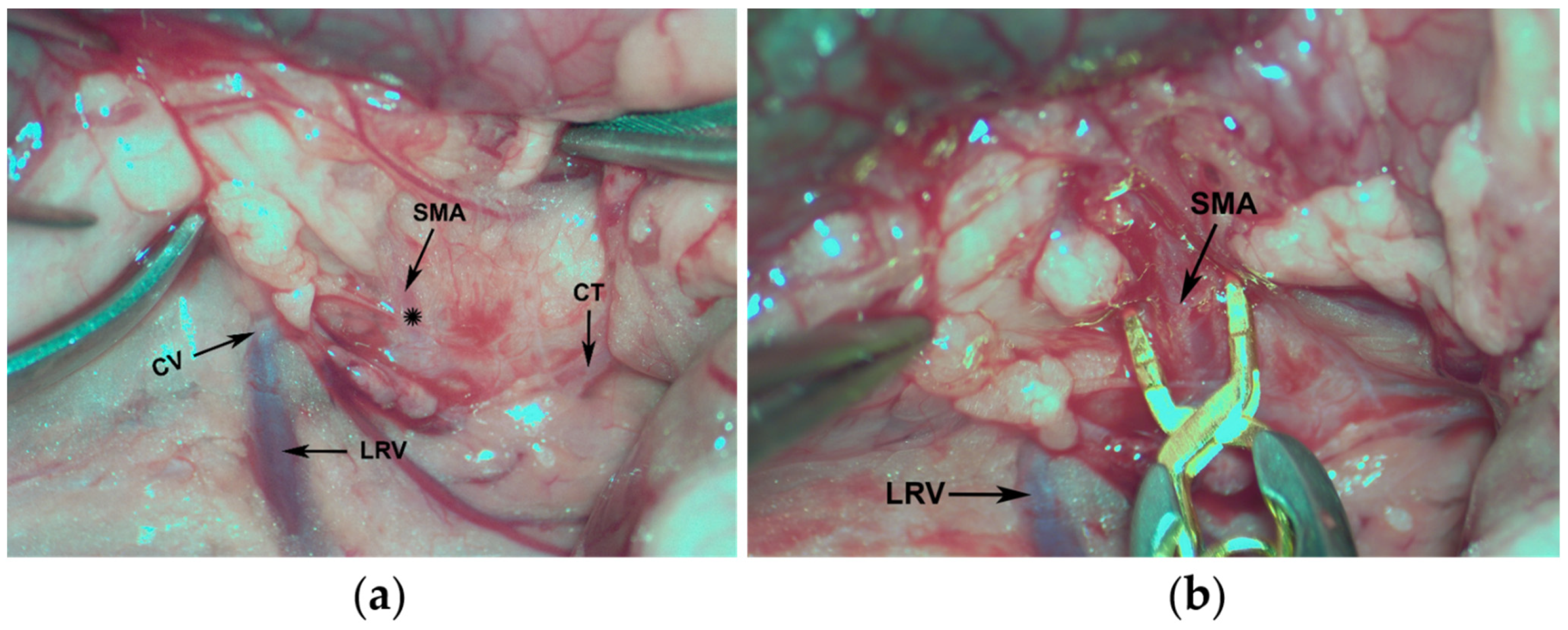
2.1. Surgical Procedure
2.2. Experimental Treatment
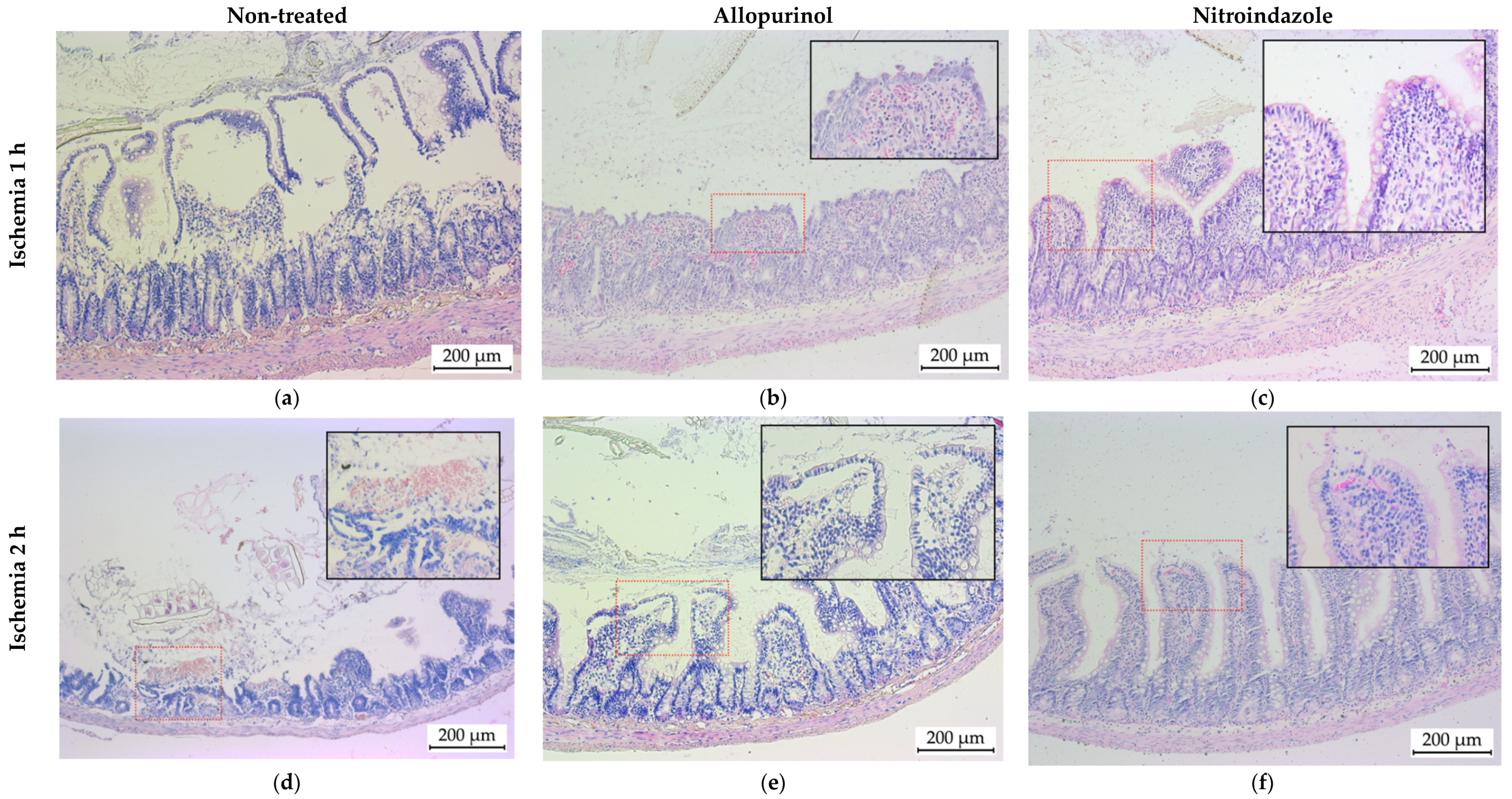
2.3. Tissue Sample Collection and Histological Examination
2.4. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Montoro, M.Á.; García Egea, J.; Fabregat, G. Isquemia intestinal. In Gastroenterología y Hepatología; Montoro, M.A., García Pagán, J.C., Eds.; Jarpyo Editores, S.A: Madrid, Spain, 2012; pp. 383–410. [Google Scholar]
- Wyers, M.C.; Michelle, M.C. Acute Mesenteric Arterial Disease. In Rutherford’s Vascular Surgery and Endovascular Therapy; Sidawy, A.N., Perler, B.A., Eds.; Elsevier Inc.: Amsterdam, The Netherlands, 2019; pp. 1754–1770. [Google Scholar]
- Tendler, D.A.; Lamont, J.T. Nonocclusive Mesenteric Ischemia. Available online: https://www.uptodate.com/contents/nonocclusive-mesenteric-ischemia (accessed on 4 May 2021).
- Bala, M.; Kashuk, J.; Moore, E.E.; Kluger, Y.; Biffl, W.; Gomes, C.A.; Ben-Ishay, O.; Rubinstein, C.; Balogh, Z.J.; Civil, I.; et al. Acute mesenteric ischemia: Guidelines of the World Society of Emergency Surgery. World J. Emerg. Surg. 2017, 12, 38. [Google Scholar] [CrossRef] [Green Version]
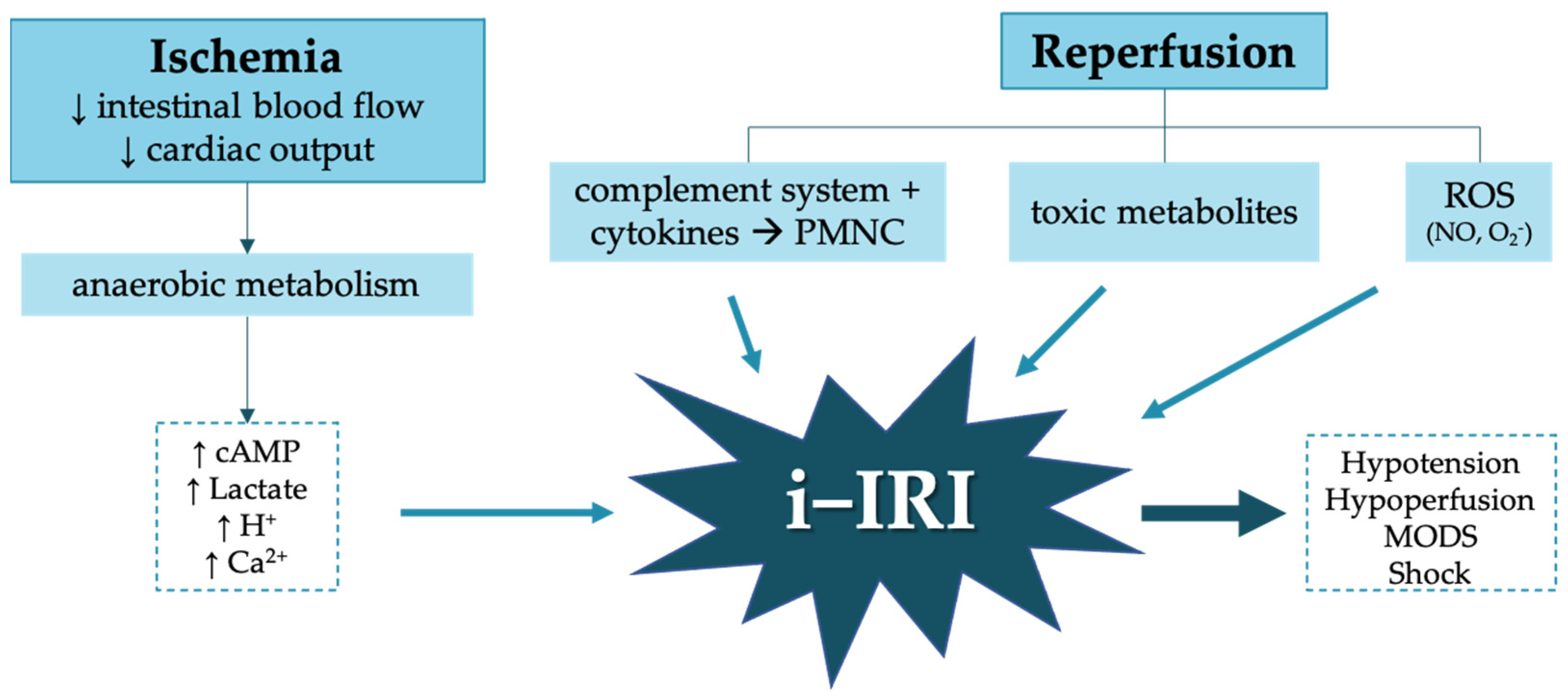
- Cerqueira, N.F.; Hussni, C.A.; Yoshida, W.B. Pathophysiology of mesenteric ischemia/reperfusion: A review. Acta Cir. Bras. 2005, 20, 333–343. [Google Scholar] [CrossRef]
- Eltzschig, H.K.; Collard, C.D. Vascular ischaemia and reperfusion injury. Br. Med. Bull. 2004, 70, 71–86. [Google Scholar] [CrossRef]
- Gonzalez, L.M.; Moeser, A.J.; Blikslager, A.T. Animal models of ischemia-reperfusion-induced intestinal injury: Progress and promise for translational research. Am. J. Physiol. Gastrointest. Liver Physiol. 2015, 308, G63–G75. [Google Scholar] [CrossRef] [Green Version]
- Yasuhara, H. Acute Mesenteric Ischemia: The Challenge of Gastroenterology. Surg. Today 2005, 33, 185–195. [Google Scholar] [CrossRef]
- Pacher, P.; Nivorozhkin, A.; Szabó, C. Therapeutic effects of xanthine oxidase inhibitors: Renaissance half a century after the discovery of allopurinol. Pharmacol. Rev. 2006, 58, 87–114. [Google Scholar] [CrossRef]
- Shadid, M.; Van Bel, F.; Steendijk, P.; Dorrepaal, C.A.; Moison, R.; Van der Velde, E.T.; Baan, J. Pretreatment with allopurinol in cardiac hypoxic-ischemic reperfusion injury in newborn lambs exerts its beneficial effect through afterload reduction. Basic Res. Cardiol. 1999, 94, 23–30. [Google Scholar] [CrossRef]
- Guan, W.; Osanai, T.; Kamada, T.; Hanada, H.; Ishizaka, H.; Onodera, H.; Iwasa, A.; Fujita, N.; Kudo, S.; Ohkubo, T.; et al. Effect of allopurinol pretreatment on free radical generation after primary coronary angioplasty for acute myocardial infarction. J. Cardiovasc. Pharmacol. 2003, 41, 699–705. [Google Scholar] [CrossRef] [PubMed]
- Riaz, A.A.; Schramm, R.; Sato, T.; Menger, M.D.; Jeppsson, B.; Thorlacius, H. Oxygen radical-dependent expression of CXC chemokines regulate ischemia/reperfusion-induced leukocyte adhesion in the mouse colon. Free Radic. Biol. Med. 2003, 35, 782–789. [Google Scholar] [CrossRef]
- Kulah, B.; Besler, H.T.; Akdag, M.; Oruc, T.; Altinok, G.; Kulacoglu, H.; Ozmen, M.M.; Coskun, F. The effects of verapamil vs. allopurinol on intestinal ischemia/reperfusion injury in rats. “An experimental study”. Hepatogastroenterology 2004, 51, 401–407. [Google Scholar]
- Kakita, T.; Suzuki, M.; Takeuchi, H.; Unno, M.; Matsuno, S. Significance of xanthine oxidase in the production of intracellular oxygen radicals in an in-vitro hypoxia-reoxygenation model. J. Hepatobiliary Pancreat. Surg. 2002, 9, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Southan, G.J.; Szabó, C. Selective pharmacological inhibition of distinct nitric oxide synthase isoforms. Biochem. Pharmacol. 1996, 51, 383–394. [Google Scholar] [CrossRef]
- San Cristóbal Epalza, J. Modulación Farmacológica del Síndrome de Isquemia-Reperfusión Retiniana en la Rata. Available online: https://addi.ehu.es/bitstream/handle/10810/23865/TESIS_SANCRISTOBAL_EPALZA_JUAN.pdf?sequence=1&isAllowed=y (accessed on 3 May 2021).
- Rivera, L.R.; Pontell, L.; Cho, H.J.; Castelucci, P.; Thacker, M.; Poole, D.P.; Frugier, T.; Furness, J.B. Knock out of neuronal nitric oxide synthase exacerbates intestinal ischemia/reperfusion injury in mice. Cell Tissue Res. 2012, 349, 565–576. [Google Scholar] [CrossRef]
- Chiu, C.J.; McArdle, A.H.; Brown, R.; Scott, H.J.; Gurd, F.N. Intestinal mucosal lesion in low-flow states I. A morphological, hemodynamic, and metabolic reappraisal. Arch. Surg. 1970, 101, 478–483. [Google Scholar] [CrossRef]
- Catilayan, F. Treatment of Intestinal Reperfusion Using Antioxidative Agents. J. Pediatr. Surg. 1998, 33, 1536–1539. [Google Scholar]
- Castelo Branco Couto de Miranda, C.T.; Fagundes, D.J. The role of ischemic preconditioning in gene expression related to inflammation in a rat model of intestinal. Acta Cir. Bras. 2018, 33, 1095–1102. [Google Scholar] [CrossRef]
- Drucker, N.A.; Jensen, A.R.; Winkel, J.P.; Markel, T.A. ScienceDirect Association for Academic Surgery Hydrogen Sulfide Donor GYY4137 Acts Through Endothelial Nitric Oxide to Protect Intestine in Murine Models of Necrotizing Enterocolitis and Intestinal Ischemia. J. Surg. Res. 2018, 234, 294–302. [Google Scholar] [CrossRef] [PubMed]
- Treskes, N.; Persoon, A.M.; Zanten, A.R.H. Van Diagnostic accuracy of novel serological biomarkers to detect acute mesenteric ischemia: A systematic review and meta-analysis. Intern. Emerg. Med. 2017, 12, 821–836. [Google Scholar] [CrossRef]
- Mohamed, D.A.; Almallah, A.A. Possible protective role of verapamil on ischemia/reperfusion induced changes in the jejunal mucosa of adult male albino rat: Histological and biochemical study. J. Innov. Pharm. Biol. Sci. 2018, 5, 92–102. [Google Scholar]
- Yagmurdur, M.C.; Topaloglu, S.; Kilinc, K. Effects of alpha tocopherol and verapamil on liver and small bowel following mesenteric ischemia-reperfusion. Turk. J. Gastroenterol. 2002, 13, 40–46. [Google Scholar]
- Da Costa Rocha, B. Experimental model of mesenteric ischemia reperfusion by abdominal aorta clamping in Wistar rats. Rev. Col. Bras. Cir. 2012, 39, 207–210. [Google Scholar] [CrossRef]
- Liu, K.-X.; Li, Y.-S.; Huang, W.-Q.; Chen, S.-Q.; Wang, Z.-X.; Liu, J.-X.; Xia, Z. Immediate postconditioning during reperfusion attenuates intestinal injury. Intensive Care Med. 2009, 35, 933. [Google Scholar] [CrossRef]
- Chalimoniuk, M.; Strosznajder, J. NMDA Receptor-Dependent Nitric Oxide and cGMP Synthesis in Brain Hemispheres and Cerebellum During Reperfusion After Transient Forebrain Ischemia in Gerbils: Effect of 7-Nitroindazole. J. Neurosci. Res. 1998, 690, 681–690. [Google Scholar] [CrossRef]
- Rhee, J.; Jung, S.; Shin, S.; Suh, G.; Noh, D.; Youn, Y.; Oh, S.; Choe, K. The Effects of Antioxidants and Nitric Oxide Modulators on Hepatic Ischemic-Reperfusion Injury in Rats. J. Korean Med. Sci. 2002, 107, 502–506. [Google Scholar] [CrossRef] [Green Version]
- Clark, E.T.; Gewertz, B.L. Intermittent ischemia potentiates intestinal reperfusion injury. J. Vasc. Surg. 1991, 13, 601–606. [Google Scholar] [CrossRef]
- Ristow, M.; Schmeisser, S. Extending life span by increasing oxidative stress. Free Radic. Biol. Med. 2011, 51, 327–336. [Google Scholar] [CrossRef] [Green Version]
- Genki, H.; Akahane, K.; Gomes, R.Z.; Paludo, K.S.; Linhares, F. The influence of allopurinol and post-conditioning on lung injuries induced by lower-limb ischemia and reperfusion in. Acta Cir. Bras. 2017, 32, 746–754. [Google Scholar]
- Brandão, R.I.; Gomes, R.Z.; Lopes, L.; Linhares, F.S.; Carlos, J.; Vellosa, R.; Paludo, K.S. Remote post-conditioning and allopurinol reduce ischemia-reperfusion injury in an infra-renal ischemia model. Ther. Adv. Cardiovasc. Dis. 2018, 12, 341–349. [Google Scholar] [CrossRef]
- Sapalidis, K.; Papavramidis, T.S.; Gialamas, E.; Deligiannidis, N.; Tzioufa, V.; Papavramidis, S. The role of allopurinol’s timing in the ischemia reperfusion injury of small intestine. J. Emerg. Trauma Shock 2013, 6, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Tani, T.; Okamoto, K.; Fujiwara, M.; Katayama, A.; Tsuruoka, S. Metabolomics analysis elucidates unique influences on purine/pyrimidine metabolism by xanthine oxidoreductase inhibitors in a rat model of renal ischemia-reperfusion injury. Mol. Med. 2019, 25, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, J.Q.; Qiu, T.; Zhang, L.; Chen, Z.B.; Wang, Z.S.; Ma, X.X.; Li, D. Allopurinol preconditioning attenuates renal ischemia/reperfusion injury by inhibiting HMGB1 expression in a rat model. Acta Cir. Bras. 2016, 31, 176–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keel, C.E.; Wang, Z.; Colli, J.; Grossman, L.; Majid, D.; Lee, B.R. Protective effects of reducing renal ischemia-reperfusion injury during renal hilar clamping: Use of allopurinol as a nephroprotective agent. Urology 2013, 81, 210.e5–210.e10. [Google Scholar] [CrossRef]
- Choi, E.K.; Jung, H.; Kwak, K.H.; Yeo, J.; Yi, S.J.; Park, C.Y.; Ryu, T.H.; Jeon, Y.H.; Park, K.M.; Lim, D.G. Effects of Allopurinol and Apocynin on Renal Ischemia-Reperfusion Injury in Rats. Transplant. Proc. 2015, 47, 1633–1638. [Google Scholar] [CrossRef] [PubMed]
- Gomes, R.Z.; Romanek, G.M.M.; Przybycien, M.; Amaral, D.C.; Akahane, H.G.K. Evaluation of the effect of allopurinol as a protective factor in post ischemia and reperfusion inflammation in Wistar rats. Acta Cir. Bras. 2016, 31, 127–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bánfi, A.; Tiszlavicz, L.; Székely, E.; Peták, F.; Tóth-Szüki, V.; Baráti, L.; Bari, F.; Novak, Z. Development of bronchus-associated lymphoid tissue hyperplasia following lipopolysaccharide-induced lung inflammation in rats. Exp. Lung Res. 2009, 35, 186–197. [Google Scholar] [CrossRef]
- Chi, O.Z.; Rah, K.H.; Barsoum, S.; Liu, X.; Weiss, H.R. Inhibition of neuronal nitric oxide synthase improves microregional O2 balance in cerebral ischemia–reperfusion. Neurol. Res. 2015, 1–8. [Google Scholar] [CrossRef]
- Vitcheva, V.; Simeonova, R.; Kondeva-burdina, M.; Mitcheva, M. Selective Nitric Oxide Synthase Inhibitor 7-Nitroindazole Protects against Cocaine-Induced Oxidative Stress in Rat Brain. Oxid. Med. Cell. Longev. 2015, 2015, 157876. [Google Scholar] [CrossRef] [Green Version]
- Hirabayashi, H.; Takizawa, S.; Fukuyama, N.; Nakazawa, H.; Shinohara, Y. 7-Nitroindazole attenuates nitrotyrosine formation in the early phase of cerebral ischemia-reperfusion in mice. Neurosci. Lett. 1999, 268, 111–113. [Google Scholar] [CrossRef]
- Sorrenti, V.; Di Giacomo, C.; Campisi, A.; Perez-Polo, J.R.; Vanella, A. Nitric Oxide Synthetase Activity in Cerebral Post-Ischemic Reperfusion and Effects of L-NG-Nitroarginine and 7-Nitroindazole on the Survival. Neurochem. Res. 1999, 24, 861–866. [Google Scholar] [CrossRef]
- Liu, P.K. Ischemia-Reperfusion-Related Repair Deficit after Oxidative Stress: Implications of Faulty Transcripts in Neuronal Sensitivity after Brain Injury. J. Biomed. Sci. 2003, 10, 4–13. [Google Scholar] [CrossRef]
- San Cristobal, J.; Garcia-Alonso, I.; Herrero, B. Pharmacological modulation of retinal ischemia—Reperfusion syndrome in rats. Investig. Ophthalmol. Vis. Sci. 2018, 59, 5287. [Google Scholar]
- Huang, L.-M.; Hu, Q.; Huang, X.; Qian, Y.; Lai, X.-H. Preconditioning rats with three lipid emulsions prior to acute lung injury affects cytokine production and cell apoptosis in the lung and liver. Lipids Health Dis. 2020, 19, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Thomas-Gibson, S.; Jawhari, A.; Atlan, P.; Le Brun, A.L.A.; Farthing, M.; Forbes, A. Safe and efficacious prolonged use of an olive oil-based lipid emulsion (ClinOleic) in chronic intestinal failure. Clin. Nutr. 2004, 23, 697–703. [Google Scholar] [CrossRef] [PubMed]
- Center for Drug Evaluation and Research (CDER); United States Food and Drug Administration. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2013/204508Orig1s000MedR.pdf (accessed on 13 May 2021).
- Farías, J.G.; Carrasco-Pozo, C.; Carrasco Loza, R.; Sepúlveda, N.; Álvarez, P.; Quezada, M.; Quiñones, J.; Molina, V.; Castillo, R.L. Polyunsaturated fatty acid induces cardioprotection against ischemia-reperfusion through the inhibition of NF-kappaB and induction of Nrf2. Exp. Biol. Med. 2017, 242, 1104–1114. [Google Scholar] [CrossRef] [Green Version]
- Sukhotnik, I.; Slijper, N.; Pollak, Y.; Chemodanov, E.; Shaoul, R.; Coran, A.G.; Mogilner, J.G. Parenteral omega-3 fatty acids (Omegaven) modulate intestinal recovery after intestinal ischemia-reperfusion in a rat model. J. Pediatr. Surg. 2011, 46, 1353–1360. [Google Scholar] [CrossRef]
- European Union. Commission Implementing Regulation (EU) No 1348/2013, of 16 December 2013 Amending Regulation (EEC) No 2568/91 on the Characteristics of Olive Oil and Olive-Residue Oil and on the Relevant Methods of Analysis; Official Journal of the European Union: Luxembourg, 2013. [Google Scholar]
- Tubert-Brohman, I.; Sherman, W.; Repasky, M.; Beuming, T. Improved docking of polypeptides with Glide. J. Chem. Inf. Model. 2013, 53, 1689–1699. [Google Scholar] [CrossRef]
- Jimenez-Lopez, C.; Carpena, M.; Lourenço-Lopes, C.; Gallardo-Gomez, M.; Lorenzo, J.M.; Barba, F.J.; Prieto, M.A.; Simal-Gandara, J. Bioactive Compounds and Quality of Extra Virgin Olive Oil. Foods 2020, 9, 1014. [Google Scholar] [CrossRef]
- Augustin, A.J.; Lutz, J. Influence of Perflubron on the Creation of Oxygen Free Radical Products in Mesenteric Artery Occlusion Shock. Artif. Cells Blood Substit. Biotechnol. 1994, 22, 1223–1230. [Google Scholar] [CrossRef]
- Demirkan, A.; Savas, B.; Melli, M. Endotoxin level in ischemia–reperfusion injury in rats: Effect of glutamine pretreatment on endotoxin levels and gut morphology. Nutrition 2010, 26, 106–111. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Ischemia | Reperfusion | Treatment | N° of Animals |
|---|---|---|---|---|
| 0 | no | no | no | 6 |
| 1 | 1 h | 30′ | no | 6 |
| 2 | Saline | 6 | ||
| 3 | ClinOleic® 20% 1 | 6 | ||
| 4 | Allopurinol | 6 | ||
| 5 | Nitroindazole | 6 | ||
| 6 | 2 h | 30′ | no | 6 |
| 7 | Saline | 6 | ||
| 8 | ClinOleic® 20% 1 | 6 | ||
| 9 | Allopurinol | 6 | ||
| 10 | Nitroindazole | 6 |
| Grade | Description |
|---|---|
| 0 | Normal mucosal villi; no histological changes |
| 1 | Epithelium of the villi is almost fully preserved; development of Gruenhagen’s subepithelial spaces (normally located in the apex); capillary congestion |
| 2 | Extension of the subepithelial spaces with moderate lifting of the epithelial layer of the lamina propria |
| 3 | Preserved villous structure with almost complete loss of epithelium (preservation > 50%); presence of intraluminal hemorrhage. |
| 4 | Destructuring of the villi, mostly denuded (preservation < 50%) |
| 5 | Loss of villi, disintegration of the lamina propria; hemorrhage and ulceration |
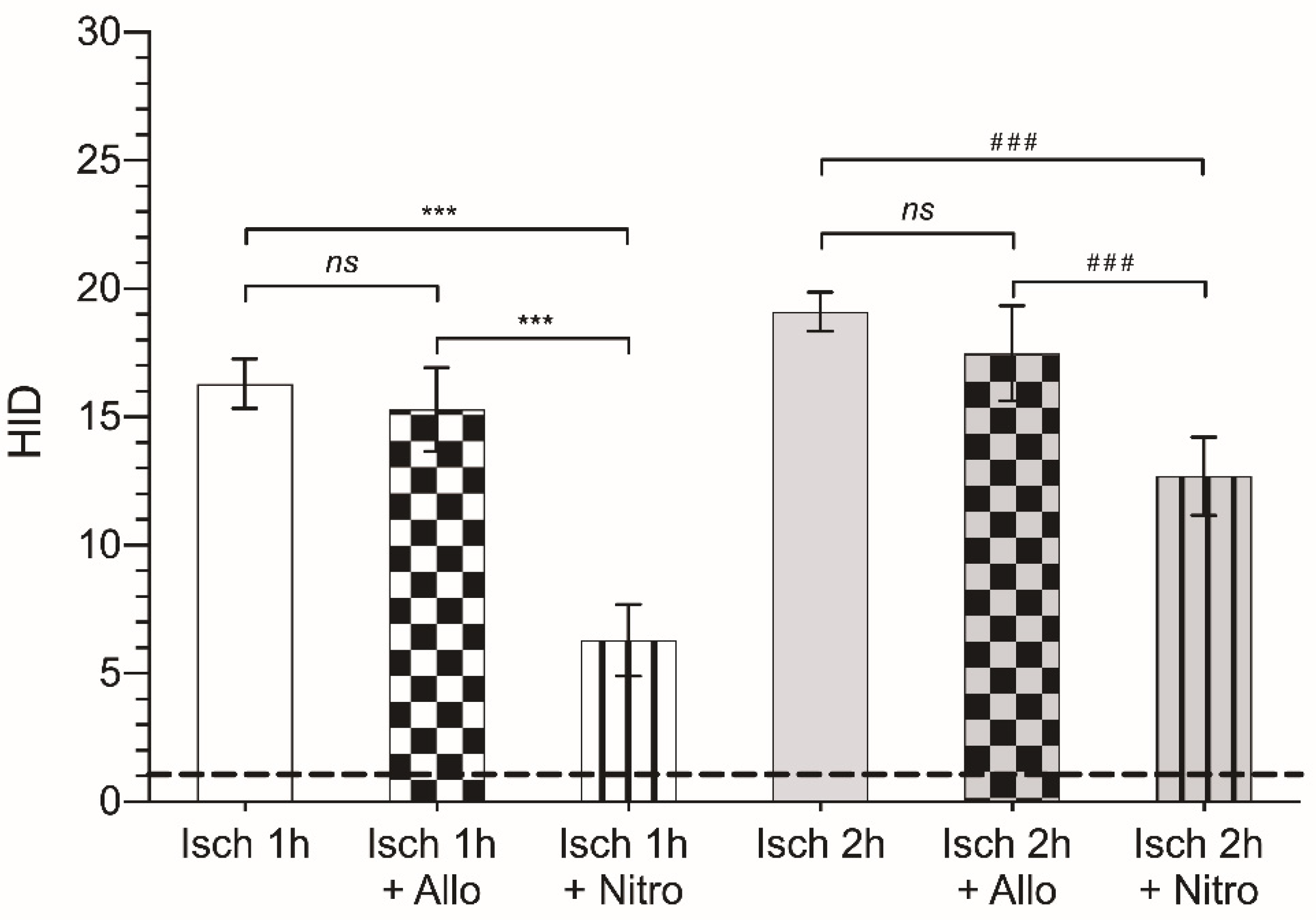
| Group | Control | Saline | Allopurinol | ClinOleic® | Nitroindazole |
|---|---|---|---|---|---|
| Ischemia 1 h | 16.3 ± 0.96 | 15.2 ± 1.91 ns 1 | 15.3 ± 1.64 ns 1 | 14.4 ± 0.98 ns 1 | 6.3 ± 1.4 p < 0.001 |
| Ischemia 2 h | 19.10 ± 0.77 | 18.1 ± 0.9 ns 1 | 17.49 ± 1.86 ns 1 | 17.9 ± 0.67 ns 1 | 12.69 ± 1.52 p < 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gutiérrez-Sánchez, G.; García-Alonso, I.; Gutiérrez Sáenz de Santa María, J.; Alonso-Varona, A.; Herrero de la Parte, B. Antioxidant-Based Therapy Reduces Early-Stage Intestinal Ischemia-Reperfusion Injury in Rats. Antioxidants 2021, 10, 853. https://doi.org/10.3390/antiox10060853
Gutiérrez-Sánchez G, García-Alonso I, Gutiérrez Sáenz de Santa María J, Alonso-Varona A, Herrero de la Parte B. Antioxidant-Based Therapy Reduces Early-Stage Intestinal Ischemia-Reperfusion Injury in Rats. Antioxidants. 2021; 10(6):853. https://doi.org/10.3390/antiox10060853
Chicago/Turabian StyleGutiérrez-Sánchez, Gaizka, Ignacio García-Alonso, Jorge Gutiérrez Sáenz de Santa María, Ana Alonso-Varona, and Borja Herrero de la Parte. 2021. "Antioxidant-Based Therapy Reduces Early-Stage Intestinal Ischemia-Reperfusion Injury in Rats" Antioxidants 10, no. 6: 853. https://doi.org/10.3390/antiox10060853