
Extended Infusion of Beta-Lactams and Glycopeptides: A New Era in Pediatric Care? A Systematic Review and Meta-Analysis

Abstract
:1. Introduction
1.1. Antibiotic Resistance
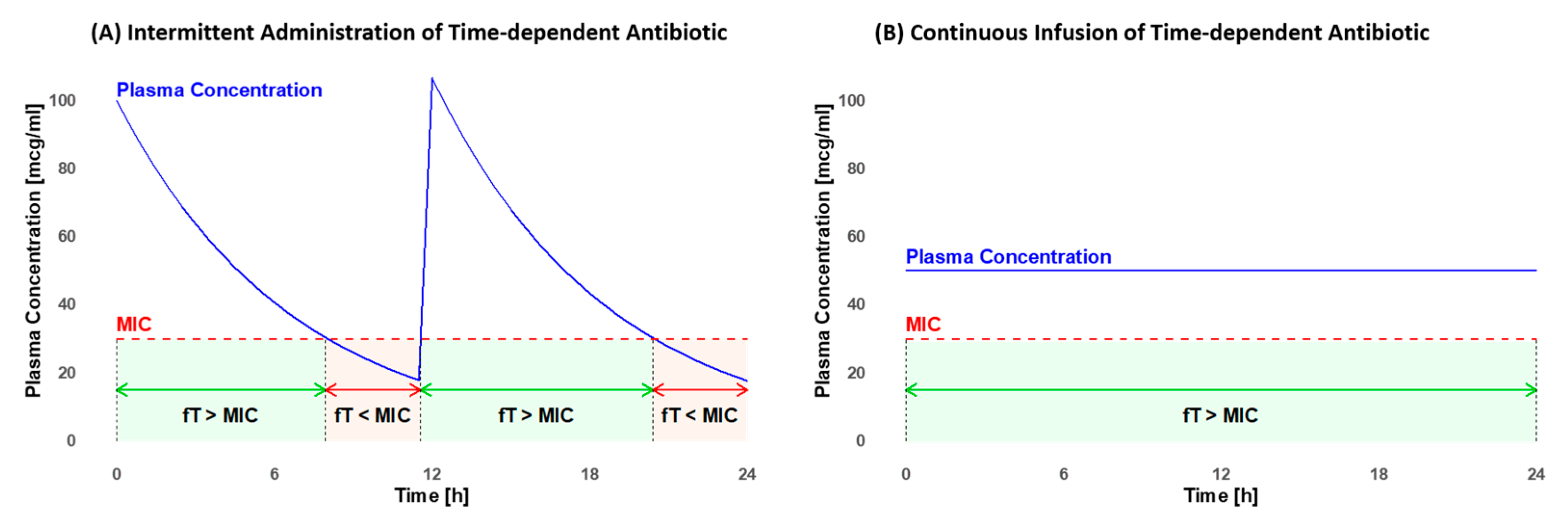
1.2. PK/PD of Beta-Lactams and Glycopeptides
1.3. Considerations for the Pediatric Population
1.4. Objective
2. Results
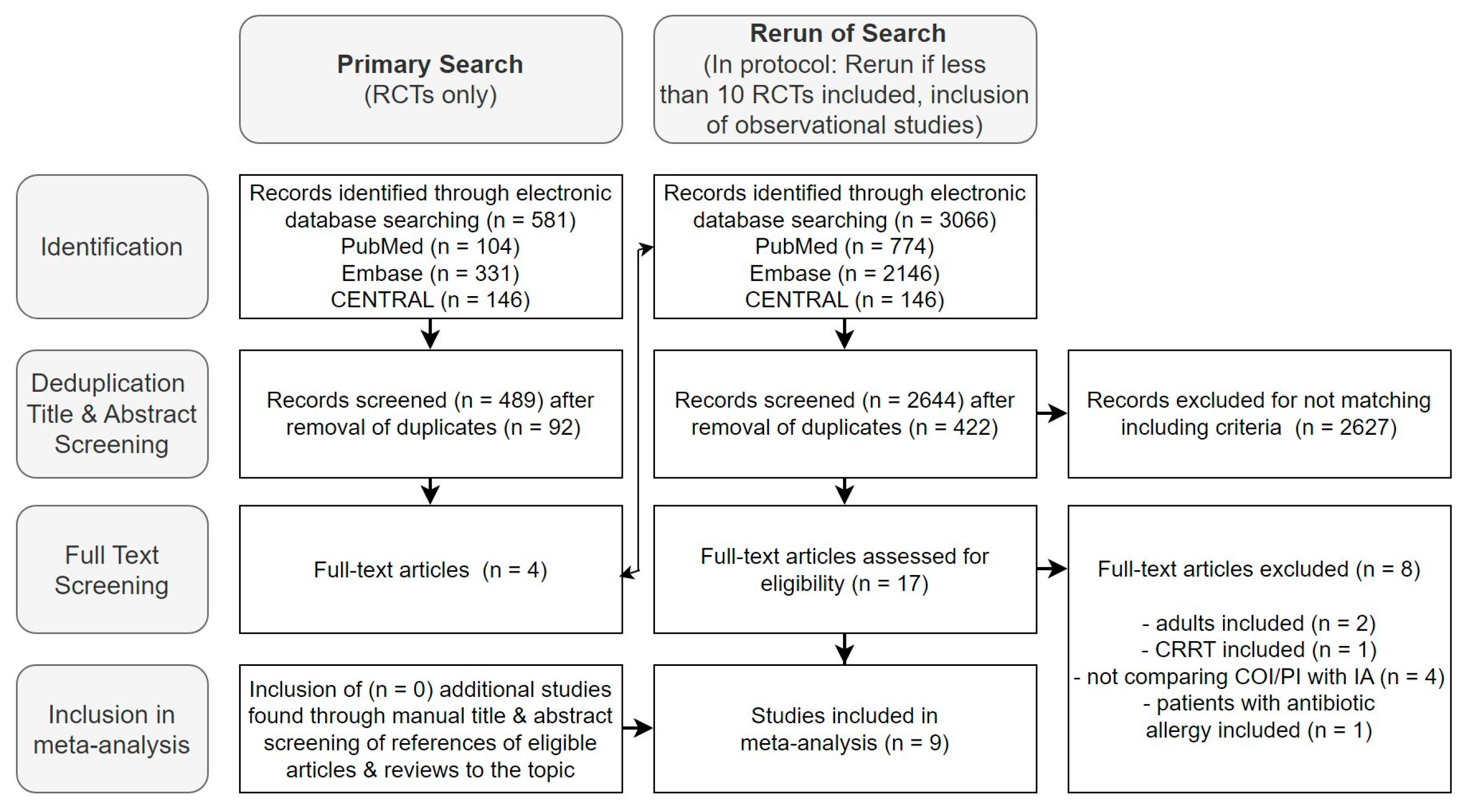
2.1. Study Selection
2.2. Risk of Bias Assessment
2.3. Study Characteristics
2.4. Data Synthesis
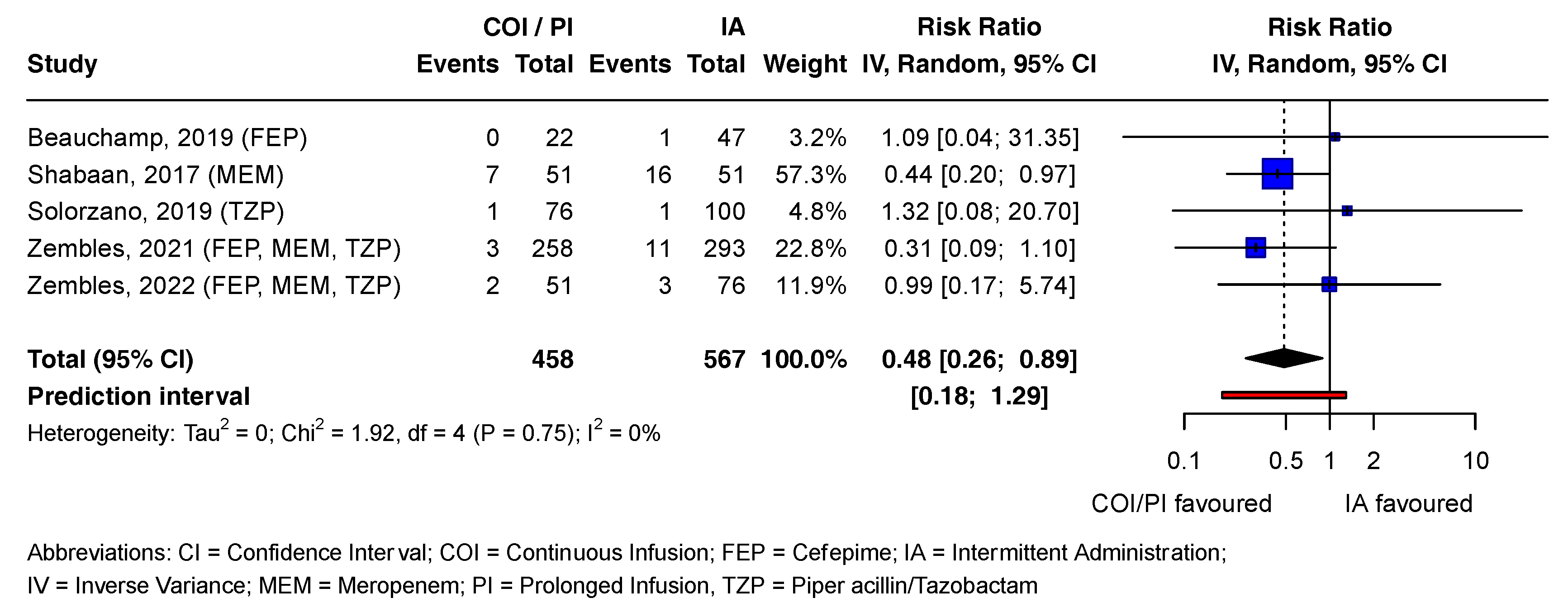
2.4.1. Beta-Lactams: Outcome Mortality
2.4.2. Subgroup Analyses
2.4.3. Publication Bias
2.4.4. Certainty of Evidence
3. Discussion
3.1. Overview of Findings
3.2. Implications for Clinical Practice and Outlook
3.3. Strengths and Limitations
3.4. Conclusions
4. Methods
4.1. Eligibility Criteria
4.2. Search Strategy and Information Sources
4.3. Study Selection
4.4. Data Collection and Analysis
4.5. Risk of Bias Assessment
4.6. Data Synthesis
4.6.1. Subgroup Analyses and Heterogeneity Assessment
4.6.2. Publication Bias
4.6.3. Grade Assessment
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bundesrat. StAR Strategie Antibiotikaresistenzen Schweiz; Vertrieb Bundespublikationen: Bern, Switzerland, 2015; pp. 35–40. [Google Scholar]
- Gerber, J.S.; Newland, J.G.; Coffin, S.E.; Hall, M.; Thurm, C.; Prasad, P.A.; Feudtner, C.; Zaoutis, T.E. Variability in Antibiotic Use at Children’s Hospitals. Pediatrics 2010, 126, 1067–1073. [Google Scholar] [CrossRef] [PubMed]
- Wathne, J.S.; Kleppe, L.K.S.; Harthug, S.; Blix, H.S.; Nilsen, R.M.; Charani, E.; Smith, I. The effect of antibiotic stewardship interventions with stakeholder involvement in hospital settings: A multicentre, cluster randomized controlled intervention study. Antimicrob. Resist. Infect. Control 2018, 7, 109. [Google Scholar] [CrossRef] [PubMed]
- Dhaese, S.; Van Vooren, S.; Boelens, J.; De Waele, J. Therapeutic drug monitoring of β-lactam antibiotics in the ICU. Expert Rev. Anti Infect. Ther. 2020, 18, 1155–1164. [Google Scholar] [CrossRef] [PubMed]
- Dhaese, S.A.M.; Hoste, E.A.; De Waele, J.J. Why We May Need Higher Doses of Beta-Lactam Antibiotics: Introducing the ‘Maximum Tolerable Dose’. Antibiotics 2022, 11, 889. [Google Scholar] [CrossRef]
- Romandini, A.; Pani, A.; Schenardi, P.A.; Pattarino, G.A.C.; De Giacomo, C.; Scaglione, F. Antibiotic Resistance in Pediatric Infections: Global Emerging Threats, Predicting the Near Future. Antibiotics 2021, 10, 393. [Google Scholar] [CrossRef]
- Tamma, P.D.; Putcha, N.; Suh, Y.D.; Van Arendonk, K.J.; Rinke, M.L. Does prolonged β-lactam infusions improve clinical outcomes compared to intermittent infusions? A meta-analysis and systematic review of randomized, controlled trials. BMC Infect. Dis. 2011, 11, 181. [Google Scholar] [CrossRef]
- Costenaro, P.; Minotti, C.; Cuppini, E.; Barbieri, E.; Giaquinto, C.; Donà, D. Optimizing Antibiotic Treatment Strategies for Neonates and Children: Does Implementing Extended or Prolonged Infusion Provide any Advantage? Antibiotics 2020, 9, 329. [Google Scholar] [CrossRef]
- Donà, D.; Barbieri, E.; Daverio, M.; Lundin, R.; Giaquinto, C.; Zaoutis, T.; Sharland, M. Implementation and impact of pediatric antimicrobial stewardship programs: A systematic scoping review. Antimicrob. Resist. Infect. Control 2020, 9, 3. [Google Scholar] [CrossRef]
- Folgori, L.; Ellis, S.J.; Bielicki, J.A.; Heath, P.T.; Sharland, M.; Balasegaram, M. Tackling antimicrobial resistance in neonatal sepsis. Lancet Glob. Health 2017, 5, e1066–e1068. [Google Scholar] [CrossRef] [PubMed]
- Falagas, M.E.; Tansarli, G.S.; Ikawa, K.; Vardakas, K.Z. Clinical outcomes with extended or continuous versus short-term intravenous infusion of carbapenems and piperacillin/tazobactam: A systematic review and meta-analysis. Clin. Infect. Dis. 2013, 56, 272–282. [Google Scholar] [CrossRef] [PubMed]
- Röhr, A.; Köberer, A.; Fuchs, T.; von Freyberg, P.; Frey, O.; Brinkmann, A. SOP Individuelle Dosierung und Applikation von Antiinfektiva auf der Intensivstation. Intensivmedizin Up2date 2018, 14, 238–243. [Google Scholar] [CrossRef]
- Pichichero, M.E.; Casey, J.R. Acute otitis media disease management. Minerva Pediatr. 2003, 55, 415–438. [Google Scholar] [PubMed]
- Gwee, A.; Cranswick, N.; Donath, S.M.; Hunt, R.; Curtis, N. Protocol for a randomised controlled trial of continuous infusions of vancomycin to improve the attainment of target vancomycin levels in young infants: The VANC trial. BMJ Open 2018, 8, e022603. [Google Scholar] [CrossRef]
- De Hoog, M.; Mouton, J.W.; van den Anker, J.N. New dosing strategies for antibacterial agents in the neonate. Semin. Fetal Neonatal Med. 2005, 10, 185–194. [Google Scholar] [CrossRef]
- Walker, M.C.; Lam, W.M.; Manasco, K.B. Continuous and extended infusions of β-lactam antibiotics in the pediatric population. Ann. Pharmacother. 2012, 46, 1537–1546. [Google Scholar] [CrossRef]
- Chongcharoenyanon, T.; Wacharachaisurapol, N.; Anugulruengkitt, S.; Maimongkol, P.; Anunsittichai, O.; Sophonphan, J.; Chatsuwan, T.; Puthanakit, T. Comparison of piperacillin plasma concentrations in a prospective randomised trial of extended infusion versus intermittent bolus of piperacillin/tazobactam in paediatric patients. Int. J. Infect. Dis. 2021, 108, 102–108. [Google Scholar] [CrossRef]
- Fantin, B.; Farinotti, R.; Thabaut, A.; Carbon, C. Conditions for the emergence of resistance to cefpirome and ceftazidime in experimental endocarditis due to Pseudomonas aeruginosa. J. Antimicrob. Chemother. 1994, 33, 563–569. [Google Scholar] [CrossRef] [PubMed]
- Gwee, A.; Cranswick, N.; McMullan, B.; Perkins, E.; Bolisetty, S.; Gardiner, K.; Daley, A.; Ward, M.; Chiletti, R.; Donath, S.; et al. Continuous versus intermittent vancomycin infusions in infants: A randomized controlled trial. Pediatrics 2019, 143, e20182179. [Google Scholar] [CrossRef]
- Downes, K.J.; Hahn, A.; Wiles, J.; Courter, J.D.; Vinks, A.A. Dose optimisation of antibiotics in children: Application of pharmacokinetics/pharmacodynamics in paediatrics. Int. J. Antimicrob. Agents 2014, 43, 223–230. [Google Scholar] [CrossRef]
- Shabaan, A.E.; Nour, I.; Elsayed Eldegla, H.; Nasef, N.; Shouman, B.; Abdel-Hady, H. Conventional Versus Prolonged Infusion of Meropenem in Neonates With Gram-negative Late-onset Sepsis: A Randomized Controlled Trial. Pediatr. Infect. Dis. J. 2017, 36, 358–363. [Google Scholar] [CrossRef]
- Hagel, S.; Fiedler, S.; Hohn, A.; Brinkmann, A.; Frey, O.R.; Hoyer, H.; Schlattmann, P.; Kiehntopf, M.; Roberts, J.A.; Pletz, M.W. Therapeutic drug monitoring-based dose optimisation of piperacillin/tazobactam to improve outcome in patients with sepsis (TARGET): A prospective, multi-centre, randomised controlled trial. Trials 2019, 20, 330. [Google Scholar] [CrossRef] [PubMed]
- Aardema, H.; Bult, W.; van Hateren, K.; Dieperink, W.; Touw, D.J.; Alffenaar, J.C.; Zijlstra, J.G. Continuous versus intermittent infusion of cefotaxime in critically ill patients: A randomized controlled trial comparing plasma concentrations. J. Antimicrob. Chemother. 2020, 75, 441–448. [Google Scholar] [CrossRef] [PubMed]
- Burgess, S.V.; Mabasa, V.H.; Chow, I.; Ensom, M.H. Evaluating outcomes of alternative dosing strategies for cefepime: A qualitative systematic review. Ann. Pharmacother. 2015, 49, 311–322. [Google Scholar] [CrossRef] [PubMed]
- Tu, Q.; Cotta, M.; Raman, S.; Graham, N.; Schlapbach, L.; Roberts, J.A. Individualized precision dosing approaches to optimize antimicrobial therapy in pediatric populations. Expert Rev. Clin. Pharmacol. 2021, 14, 1383–1399. [Google Scholar] [CrossRef] [PubMed]
- Roberts, J.A.; Joynt, G.M.; Lee, A.; Choi, G.; Bellomo, R.; Kanji, S.; Mudaliar, M.Y.; Peake, S.L.; Stephens, D.; Taccone, F.S.; et al. The Effect of Renal Replacement Therapy and Antibiotic Dose on Antibiotic Concentrations in Critically Ill Patients: Data from the Multinational Sampling Antibiotics in Renal Replacement Therapy Study. Clin. Infect. Dis. 2021, 72, 1369–1378. [Google Scholar] [CrossRef] [PubMed]
- Béranger, A.; Oualha, M.; Urien, S.; Genuini, M.; Renolleau, S.; Aboura, R.; Hirt, D.; Heilbronner, C.; Toubiana, J.; Tréluyer, J.-M.; et al. Population Pharmacokinetic Model to Optimize Cefotaxime Dosing Regimen in Critically Ill Children. Clin. Pharmacokinet. 2018, 57, 867–875. [Google Scholar] [CrossRef]
- Krueger, W.A.; Bulitta, J.; Kinzig-Schippers, M.; Landersdorfer, C.; Holzgrabe, U.; Naber, K.G.; Drusano, G.L.; Sörgel, F. Evaluation by monte carlo simulation of the pharmacokinetics of two doses of meropenem administered intermittently or as a continuous infusion in healthy volunteers. Antimicrob. Agents Chemother. 2005, 49, 1881–1889. [Google Scholar] [CrossRef]
- De Cock, P.A.J.G.; van Dijkman, S.C.; de Jaeger, A.; Willems, J.; Carlier, M.; Verstraete, A.G.; Delanghe, J.R.; Robays, H.; Walle, J.V.; Della Pasqua, O.E.; et al. Dose optimization of piperacillin/tazobactam in critically ill children. J. Antimicrob. Chemother. 2017, 72, 2002–2011. [Google Scholar] [CrossRef]
- Zhao, W.; Zhang, D.; Fakhoury, M.; Fahd, M.; Duquesne, F.; Storme, T.; Baruchel, A.; Jacqz-Aigrain, E. Population pharmacokinetics and dosing optimization of vancomycin in children with malignant hematological disease. Antimicrob. Agents Chemother. 2014, 58, 3191–3199. [Google Scholar] [CrossRef]
- Agathe, D.; Delphine, C.; Deborah, H.; Emmanuelle, B.; Sylvain, R.; Laurent, C.; Jean-Marc, T.; Mehdi, O.; Agathe, B. Beta-lactam exposure and safety in intermittent or continuous infusion in critically ill children. Ann. Intensive Care 2022, 182, 965–973. [Google Scholar] [CrossRef]
- Yang, H.; Zhang, C.; Zhou, Q.; Wang, Y.; Chen, L. Clinical Outcomes with Alternative Dosing Strategies for Piperacillin/Tazobactam: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0116769. [Google Scholar] [CrossRef] [PubMed]
- SwissPedDose. Nationale Datenbak zur Dosierung von Arzneimitteln bei Kindern. Available online: https://db.swisspeddose.ch/de/search/?_roa=iv (accessed on 19 May 2023).
- Testa, B.; Krämer, S.D. The biochemistry of drug metabolism—An introduction: Part 1. Principles and overview. Chem. Biodivers. 2006, 3, 1053–1101. [Google Scholar] [CrossRef] [PubMed]
- Ahn, E.; Kang, H. Introduction to systematic review and meta-analysis. Korean J. Anesthesiol. 2018, 71, 103–112. [Google Scholar] [CrossRef] [PubMed]
- von Arx, L.E.; Burch, A.R.; Neumeier, V.; Burden, A. Safety and Efficacy of Continuous and Prolonged Infusion of Beta-Lactams and Glycopeptides Compared to Intermittent Administration in Children: A Systematic Review and Meta-Analysis. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=407772 (accessed on 31 March 2023).
- Beauchamp, L.C.; Nichols, K.R.; Knoderer, C.A. Outcomes of Extended Infusion Cefepime in Pediatric Patients. Infect. Dis. Clin. Pract. 2019, 27, 283–287. [Google Scholar] [CrossRef]
- Solórzano-Santos, F.; Quezada-Herrera, A.; Fuentes-Pacheco, Y.; Rodríguez-Coello, G.; Aguirre-Morales, C.E.; Izelo-Flores, D.; Muñoz-Hernández, O.; Miranda-Novales, M.G.; Labra-Zamora, M.G. Piperacillin/Tazobactam in Continuous Infusion versus Intermittent Infusion in Children with Febrile Neutropenia. Rev. Investig. Clin. 2019, 71, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Zembles, T.N.; Schortemeyer, R.; Kuhn, E.M.; Bushee, G.; Thompson, N.E.; Mitchell, M.L. Extended infusion of beta-lactams is associated with improved outcomes in pediatric patients. J. Pediatr. Pharmacol. Ther. 2021, 26, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Zembles, T.N.; Kuhn, E.M.; Thompson, N.E.; Mitchell, M.L. Extended Infusion b-Lactams for the Treatment of Gram-Negative Bacteremia in Children. J. Pediatr. Pharmacol. Ther. 2022, 27, 677–681. [Google Scholar] [CrossRef]
- Demirel, B.; Imamoglu, E.; Gursoy, T.; Demirel, U.; Topçuoglu, S.; Karatekin, G.; Ovali, F. Comparison of intermittent versus continuous vancomycin infusion for the treatment of late-onset sepsis in preterm infants. J. Neonatal-Perinat. Med. 2015, 8, 149–155. [Google Scholar] [CrossRef]
- Gwee, A.; Cranswick, N. Anti-infective use in children and pregnancy: Current deficiencies and future challenges. Br. J. Clin. Pharmacol. 2015, 79, 216–221. [Google Scholar] [CrossRef]
- Wysocki, E.; Tansmore, J. When There Is No Trough: Use and Outcomes of Continuous-Infusion Vancomycin at a Free-Standing Children’s Hospital. J. Pediatr. Pharmacol. Ther. 2022, 27, 452–456. [Google Scholar] [CrossRef]
- Budai, K.A.; Timar, A.E.; Obeidat, M.; Mate, V.; Nagy, R.; Harnos, A.; Kiss-Dala, S.; Hegyi, P.; Garami, M.; Hanko, B.; et al. Extended infusion of beta-lactams significantly reduces mortality and enhances microbiological eradication in paediatric patients: A systematic review and meta-analysis. EClinicalMedicine 2023, 65, 102293. [Google Scholar] [CrossRef]
- Van Den Anker, J.N.; Pokorna, P.; Kinzig-Schippers, M.; Martinkova, J.; De Groot, R.; Drusano, G.L.; Sorgel, F. Meropenem pharmacokinetics in the newborn. Antimicrob. Agents Chemother. 2009, 53, 3871–3879. [Google Scholar] [CrossRef] [PubMed]
- Grupper, M.; Kuti, J.L.; Nicolau, D.P. Continuous and Prolonged Intravenous β-Lactam Dosing: Implications for the Clinical Laboratory. Clin. Microbiol. Rev. 2016, 29, 759–772. [Google Scholar] [CrossRef]
- Hagel, S.; Bach, F.; Brenner, T.; Bracht, H.; Brinkmann, A.; Annecke, T.; Hohn, A.; Weigand, M.; Michels, G.; Kluge, S.; et al. Effect of therapeutic drug monitoring-based dose optimization of piperacillin/tazobactam on sepsis-related organ dysfunction in patients with sepsis: A randomized controlled trial. Intensive Care Med. 2022, 48, 311–321. [Google Scholar] [CrossRef] [PubMed]
- Dalle, J.H.; Gnansounou, M.; Husson, M.O.; Lambilliotte, A.; Mazingue, F.; Nelken, B. Continuous infusion of ceftazidime in the empiric treatment of febrile neutropenic children with cancer. J. Pediatr. Hematol. Oncol. 2002, 24, 714–716. [Google Scholar] [CrossRef]
- Richter, D.C.; Frey, O.; Röhr, A.; Roberts, J.A.; Köberer, A.; Fuchs, T.; Papadimas, N.; Heinzel-Gutenbrunner, M.; Brenner, T.; Lichtenstern, C.; et al. Therapeutic drug monitoring-guided continuous infusion of piperacillin/tazobactam significantly improves pharmacokinetic target attainment in critically ill patients: A retrospective analysis of four years of clinical experience. Infection 2019, 47, 1001–1011. [Google Scholar] [CrossRef]
- Abdul-Aziz, M.H.; Sulaiman, H.; Mat-Nor, M.-B.; Rai, V.; Wong, K.K.; Hasan, M.S.; Abd Rahman, A.N.; Jamal, J.A.; Wallis, S.C.; Lipman, J.; et al. Beta-Lactam Infusion in Severe Sepsis (BLISS): A prospective, two-centre, open-labelled randomised controlled trial of continuous versus intermittent beta-lactam infusion in critically ill patients with severe sepsis. Intensive Care Med. 2016, 42, 1535–1545. [Google Scholar] [CrossRef] [PubMed]
- Roberts, J.A.; Croom, K.; Adomakoh, N. Continuous infusion of beta-lactam antibiotics: Narrative review of systematic reviews, and implications for outpatient parenteral antibiotic therapy. Expert Rev. Anti-Infect. Ther. 2023, 21, 375–385. [Google Scholar] [CrossRef]
- Jamal, J.A.; Mat-Nor, M.B.; Mohamad-Nor, F.S.; Udy, A.A.; Wallis, S.C.; Lipman, J.; Roberts, J.A. Pharmacokinetics of meropenem in critically ill patients receiving continuous venovenous haemofiltration: A randomised controlled trial of continuous infusion versus intermittent bolus administration. Int. J. Antimicrob. Agents 2015, 45, 41–45. [Google Scholar] [CrossRef]
- Imburgia, T.A.; Kussin, M.L. A Review of Extended and Continuous Infusion Beta-Lactams in Pediatric Patients. J. Pediatr. Pharmacol. Ther. 2022, 27, 214–227. [Google Scholar] [CrossRef]
- Nichols, K.R.; Karmire, L.C.; Cox, E.G.; Kays, M.B.; Knoderer, C.A. Implementing Extended-Infusion Cefepime as Standard of Care in a Children’s Hospital: A Prospective Descriptive Study. Ann. Pharmacother. 2015, 49, 419–426. [Google Scholar] [CrossRef]
- Chen, P.; Chen, F.; Lei, J.; Zhou, B. Clinical outcomes of continuous vs intermittent meropenem infusion for the treatment of sepsis: A systematic review and meta-analysis. Adv. Clin. Exp. Med. 2020, 29, 993–1000. [Google Scholar] [CrossRef]
- Higgins, J.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T. Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; John Wiley & Sons: Chichester, UK, 2019. [Google Scholar]
- Roberts, J.A.; Lipman, J. Antibacterial Dosing in Intensive Care. Clin. Pharmacokinet. 2006, 45, 755–773. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Matusik, E.; Lemtiri, J.; Wabont, G.; Lambiotte, F. Beta-lactam dosing during continuous renal replacement therapy: A survey of practices in french intensive care units. BMC Nephrol. 2022, 23, 48. [Google Scholar] [CrossRef] [PubMed]
- Deldot, M.E.; Lipman, J.; Tett, S.E. Vancomycin pharmacokinetics in critically ill patients receiving continuous venovenous haemodiafiltration. Br. J. Clin. Pharmacol. 2004, 58, 259–268. [Google Scholar] [CrossRef] [PubMed]
- Rethlefsen, M.L.; Kirtley, S.; Waffenschmidt, S.; Ayala, A.P.; Moher, D.; Page, M.J.; Koffel, J.B.; Blunt, H.; Brigham, T.; Chang, S.; et al. PRISMA-S: An extension to the PRISMA Statement for Reporting Literature Searches in Systematic Reviews. Syst. Rev. 2021, 10, 39. [Google Scholar] [CrossRef] [PubMed]
- Lefebvre, C.; Glanville, J.; Briscoe, S.; Featherstone, R.; Littlewood, A.; Marshall, C.; Metzendorf, M.-I.; Noel-Storr, A.; Paynter, R.; Rader, T.; et al. Technical Supplement to Chapter 4: Searching for and Selecting Studies. In Cochrane Handbook for Systematic Reviews of Interventions, version 6.3 (updated February 2022); Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Cochrane; John Wiley & Sons: Chichester, UK, 2022. [Google Scholar]
- The EndNote Team. EndNote, Endnote 20; Clarivate: Philadelphia, PA, USA, 2020. [Google Scholar]
- Page, M.J.; Mckenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Higgins, J.; Savovic, J.; Page, M.J.; Sterne, J.A.C. Revised Cochrane Risk-of-Bias Tool for Randomized Trials (ROB 2); Cochrane; John Wiley & Sons: Chichester, UK, 2022. [Google Scholar]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]
- Balduzzi, S.; Rücker, G.; Schwarzer, G. How to perform a meta-analysis with R: A practical tutorial. Evid.-Based Ment. Health 2019, 22, 153–160. [Google Scholar] [CrossRef]
- RStudio Team. RStudio: Integrated Development Environment for R; Version 2022.12.0+353 (2022.12.0+353); RStudio, PBC: Boston, MA, USA; Available online: http://www.rstudio.com/ (accessed on 1 April 2023).
- Viechtbauer, W. Conducting meta-analyses in R with the metafor package. J. Stat. Softw. 2010, 36, 1–48. [Google Scholar] [CrossRef]
- Schulz, A.; Schürmann, C.; Skipka, G.; Bender, R. Performing Meta-analyses with Very Few Studies. Methods Mol. Biol. 2022, 2345, 91–102. [Google Scholar] [PubMed]
- Sterne, J.A.C.; Sutton, A.J.; Ioannidis, J.P.A.; Terrin, N.; Jones, D.R.; Lau, J.; Carpenter, J.; Rucker, G.; Harbord, R.M.; Schmid, C.H.; et al. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ 2011, 343, d4002. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Coello, P.A.; Guyatt, G.H.; Yepes-Nuñez, J.J.; Akl, E.A.; Hazlewood, G.; Pardo-Hernandez, H.; Etxeandia-Ikobaltzeta, I.; Qaseem, A.; Williams, J.W., Jr.; et al. GRADE guidelines: 20. Assessing the certainty of evidence in the importance of outcomes or values and preferences-inconsistency, imprecision, and other domains. J. Clin. Epidemiol. 2019, 111, 83–93. [Google Scholar] [CrossRef]
- Altman, D.G.; Bland, J.M. How to obtain the P value from a confidence interval. BMJ 2011, 343, d2304. [Google Scholar] [CrossRef]
- Aguinis, H.; Vassar, M.; Wayant, C. On reporting and interpreting statistical significance and p values in medical research. BMJ Evid.-Based Med. 2021, 26, 39–42. [Google Scholar] [CrossRef]
- Wysocki, E.; Tansmore, J. When there is no trough: Continuous infusion vancomycin utilization at a free-standing children’s hospital. J. Pediatr. Pharmacol. Ther. 2021, 26, 525–526. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| PK Process | Observable Differences |
|---|---|
| Absorption |
|
| Distribution |
|
| Metabolism |
|
| Excretion |
|
| Beta-Lactam Study | Outcome | ||
|---|---|---|---|
| Mortality | Clinical Success | Microbiological Eradication | |
| Beauchamp 2019 [37] | High risk | High risk | High risk |
| Chongcharoenyanon 2021 [17] | Some concerns | High risk | n/a |
| Shabaan 2017 [21] | Low risk | Low risk | Low risk |
| Solorzano 2019 [38] | High risk | High risk | n/a |
| Zembles 2021 [39] | Some concerns | Some concerns | n/a |
| Zembles 2022 [40] | Some concerns | Some concerns | n/a |
| Glycopeptide Study | Outcome | ||
|---|---|---|---|
| Mortality | Clinical Success | Microbiological Eradication | |
| Demirel 2015 [41] | High risk | High risk | High risk |
| Gwee 2015 [42] | Some concerns | n/a | n/a |
| Wysocki 2022 [43] | High risk | High risk | High risk |
| Study | Country/ Study Period | Study Design | AB | Sample Size (n) | Sex, f (%) | Main Indication for Treatment | Inclusion Criteria | Outcomes |
|---|---|---|---|---|---|---|---|---|
| Beauchamp, 2019 [37] | USA/January 2007–April 2016 | CS (retrospective) | FEP | 67 | 39 | Gram-negative bacteremia | Age: 31 days to 17 years with documented Gram-negative bacteremia susceptible to FEP. (MIC ≤ 8 µg/mL.) At least 48 h of cefepime and at least 7 days of appropriate culture-directed therapy. | Mortality within 14 days of antibiotic therapy start or bacteremia relapse with the same organism, as evidenced by positive blood culture within 30 days of culture clearance, treatment failure (absence of defervescence, white blood cell normalization, and culture clearance (defervescence = drop of body temperature to less than 38.3)). |
| Chongcharo-enyanon, 2021 [17] | Thailand/ July 2019–April 2020 | RCT (open label) | TZP | 90 | 56 | Pneumonia (32%), febrile neutropenia, and other | Age: 1 month to 18 years, body weight > 3 kg, and suspected or proven multidrug-resistant Gram-negative bacterial infection. | Piperacillin plasma concentrations mid-dosing interval. |
| Shabaan, 2017 [21] | Egypt/ August 2013–June 2015 | RCT (open label) | MEM | 102 | 46 | Gram-negative late-onset sepsis | Age: <28 days, late-onset sepsis (sepsis after 72 h of birth), and Gram-negative bacteria sensitive to MEM. Requirement for confirmation of sepsis: positive blood, cerebrospinal fluid, urine, and/or synovial cultures. | Clinical success (complete resolution of clinical signs and symptoms of sepsis at the end of therapy (hemodynamic stability, normal arterial blood gas values, temperature stability, tolerance for enteral feeding, and discontinuation of inotropes for at least a 48 h duration). Microbiological success: eradication after 7 days of MEM therapy. |
| Solorzano, 2019 [38] | Mexico/April 2012–August 2015 | RCT (open label) | TZP | 176 | 41 | Febrile neutropenia | Age: <18 years, haemato-oncological patients, and febrile neutropenia 8 (T ≥ 38.3 or T ≥ 38.0 over 1 h and absolute neutrophil count < 500 cells/mm3). | Clinical cure (no fever after 96 h of treatment or no clinical sign of infection and discharge). Clinical failure if change in treatment or death. |
| Zembles, 2021 [39] | USA/October 2017–March 2019 | Chart analysis (retrospective) | FEP, MEM, TZP | 551 | 41 | All indications | Age: <18 years; received at least 72 h of FEP/MEM/TZP. | Length of stay, time to blood culture clearance (only patients with Gram-negative bacteremia), hospital readmission within 30 days (only patients discharged within first 14 days after completion of antibiotic therapy), and 30-day mortality after completion. |
| Zembles, 2022 [40] | USA/January 2013–July 2021 | Chart analysis (retrospective) | FEP, MEM, TZP | 124 | 30 | Gram-negative bacteremia | Age: <18 years, confirmed Gram-negative bacteremia, and at least 72 h of FEP/MEM/TZP. | Hospital length of stay, duration of AB treatment, readmission within 30 days, all-cause mortality, time to white blood cell count normalization, time to c-reactive protein normalization, and time to blood culture clearance. |
| Study | Country/Study Period | Study Design | AB | Sample Size (n) | Sex , f (%) | Main Indication for Treatment | Inclusion Criteria | Outcomes |
|---|---|---|---|---|---|---|---|---|
| Demirel, 2015 [41] | Turkey/n/a | Chart analysis (retrospective) | VAN | 77 | 39 | Late-onset sepsis; bacteremia; other | Age: gestational age < 34 weeks, and vancomycin for late-onset sepsis. | Clinical efficacy (clinical failure), safety, and microbiological outcomes of intermittent versus continuous vancomycin infusion in preterm neonates. |
| Gwee, 2019 [19] | Australia/September 2014–December 2017 | RCT (non-blinded) | VAN | 104 | 50 | (Suspected) sepsis; other | Age: 0–90 days old, and vancomycin administration ≥ 48 h. | Difference in the proportion of participants achieving target vancomycin levels at their first steady-state level. |
| Wysocki, 2022 [43] | USA/July 2010–June 2020 | Chart analysis (retrospective) | VAN | 28 | 21 | Bacteremia; other | Age: >4 weeks and <18 years, and at least one serum vancomycin concentration within target range (10–20 mg/L) | Acute kidney injuries (rise in serum creatinine ≥ 1.5 × baseline, infusion reactions recorded in EMR). Treatment failure (defined as persistent positive culture for longer than or equal to 7 days, recurrence of infection within 30 days of the end of COI, or 30-day all-cause mortality). |
| Study Characteristics | Quality Assessment | Number of Patients | Effect | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| AB | Outcome | N, Study Type | ROB | Imprecision | Inconsistency | Indirectness | Publication Bias | COI: Outcome/ Total | IA: Outcome/ Total | RR (95% CI) | GRADE |
| BL | Mortality | 5, nRCT | Serious | Serious | Not serious | Not serious | Undetected | 13/458 | 32/567 | 0.48 (0.26–0.89) | Very low |
| BL | Clinical success | 6, nRCT | Serious | Not serious | Not serious | Serious | Undetected | 389/502 | 462/608 | 1.02 (0.87–1.19) | Very low |
| BL | Microbiological eradication | 2, nRCT | Serious | Serious | Serious | Serious | Undetected | 62/72 | 74/97 | 1.16 (0.97–1.71) | Very low |
| GP | Mortality | 1, nRCT | Serious | Serious | n/a 1 | Not serious | Undetected | 1/35 | 0.5/41 | 2.31 (0.08–66.73) | Very low |
| GP | Clinical success | 1, RCT | Serious | Not serious | n/a 1 | Serious | Undetected | 34/36 | 41/41 | 0.94 (0.87–1.02) | Very low |
| GP | Microbiological eradication | 1, nRCT | Serious | Serious | n/a 1 | Serious | Undetected | 7/11 | 11/19 | 1.10 (0.61–1.98) | Very low |
| Domain | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Study design |
|
|
| Intervention |
| |
| Comparison |
| |
| Outcomes (primary) |
|
|
| Outcomes (secondary) |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burch, A.R.; von Arx, L.; Hasse, B.; Neumeier, V. Extended Infusion of Beta-Lactams and Glycopeptides: A New Era in Pediatric Care? A Systematic Review and Meta-Analysis. Antibiotics 2024, 13, 164. https://doi.org/10.3390/antibiotics13020164
Burch AR, von Arx L, Hasse B, Neumeier V. Extended Infusion of Beta-Lactams and Glycopeptides: A New Era in Pediatric Care? A Systematic Review and Meta-Analysis. Antibiotics. 2024; 13(2):164. https://doi.org/10.3390/antibiotics13020164
Chicago/Turabian StyleBurch, Andrea Rahel, Lukas von Arx, Barbara Hasse, and Vera Neumeier. 2024. "Extended Infusion of Beta-Lactams and Glycopeptides: A New Era in Pediatric Care? A Systematic Review and Meta-Analysis" Antibiotics 13, no. 2: 164. https://doi.org/10.3390/antibiotics13020164