

Surveillance of Antimicrobial Resistance and Multidrug Resistance Prevalence of Clinical Isolates in a Regional Hospital in Northern Greece
 ,
, 
Abstract
:1. Introduction
2. Results
2.1. Six-Year Surveillance of Clinical Isolates’ Susceptibility to Certain Antibiotics
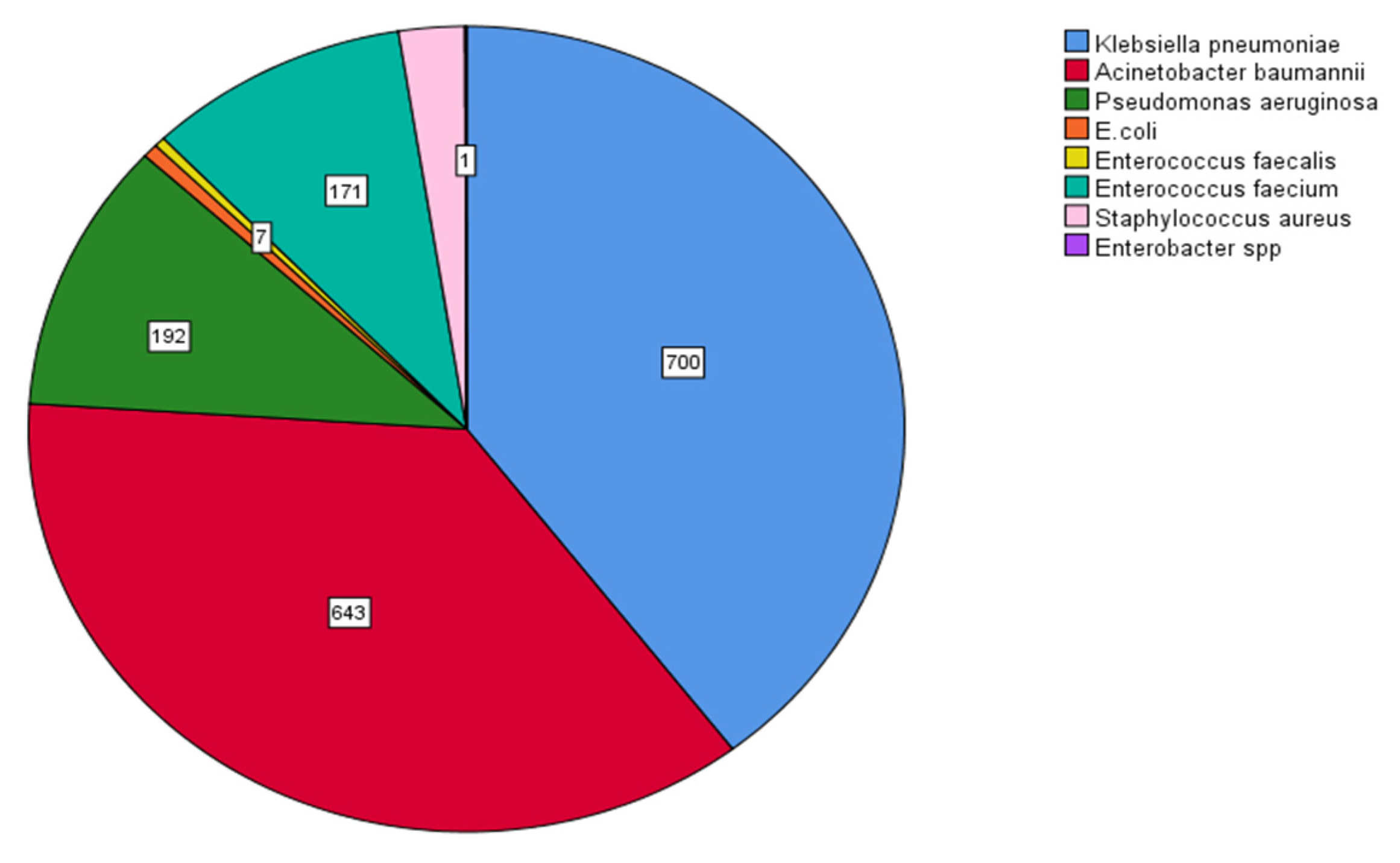
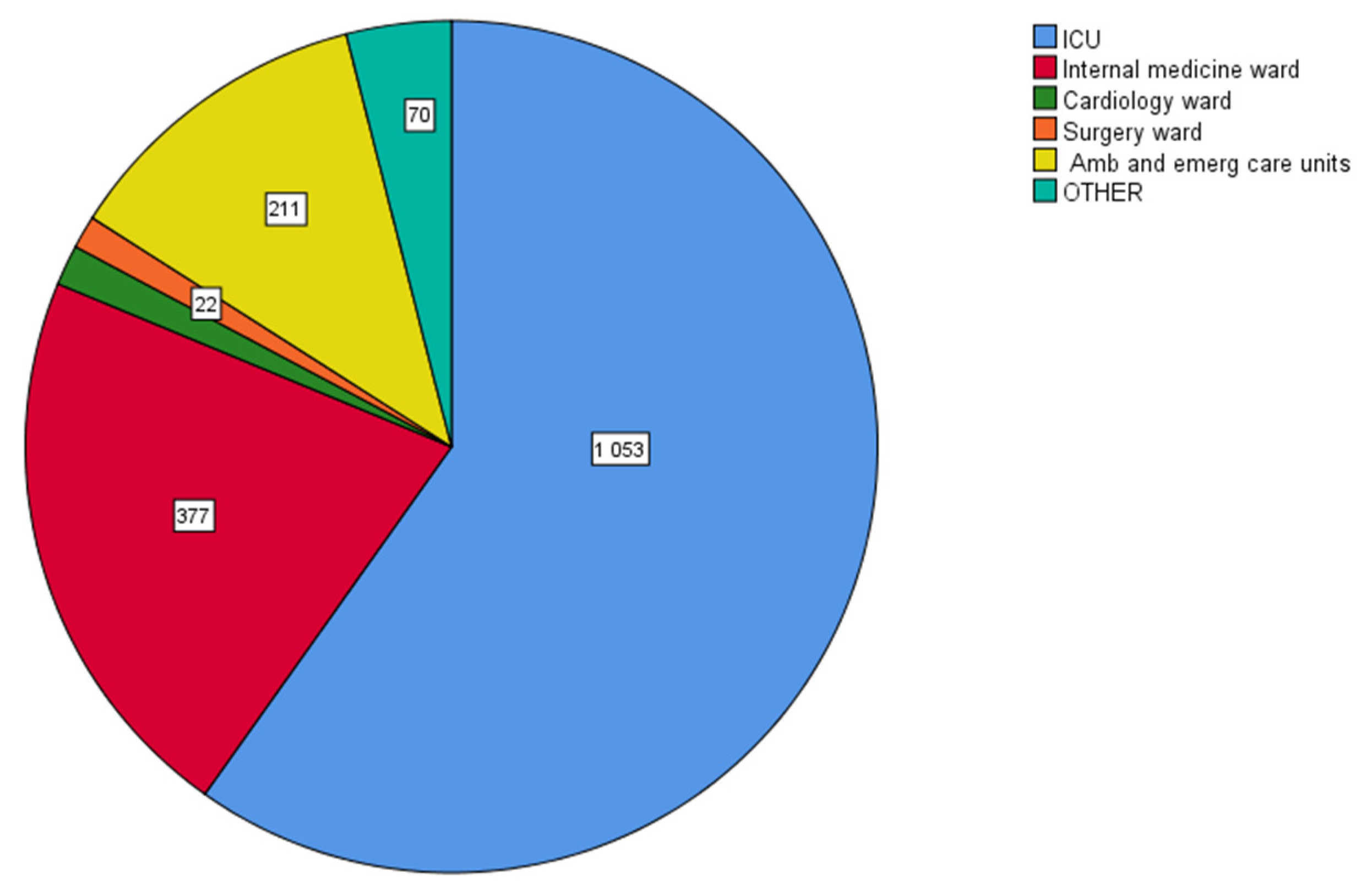
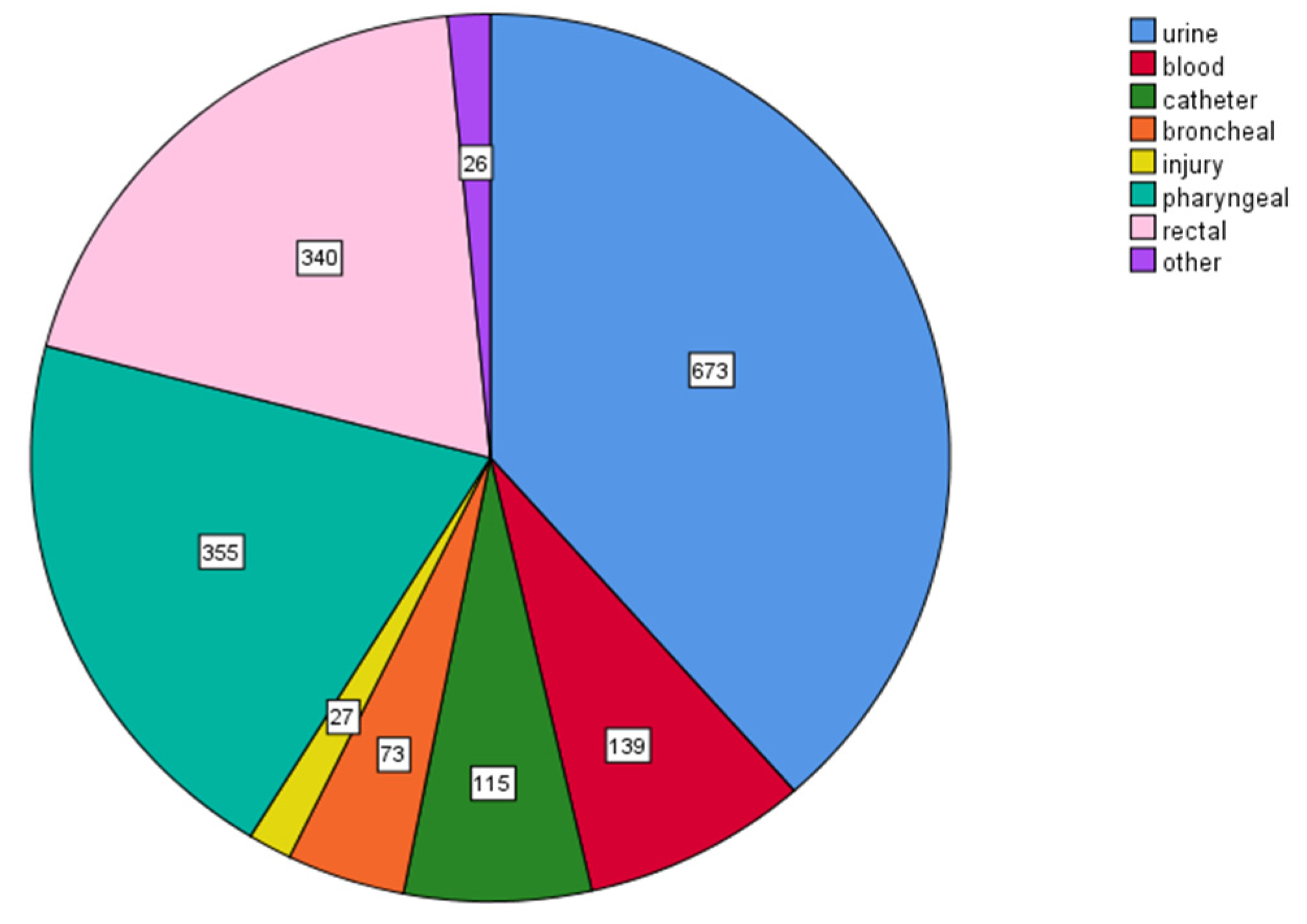
2.1.1. Types of Clinical Isolates
2.1.2. Antimicrobial Resistance of Clinical Isolates
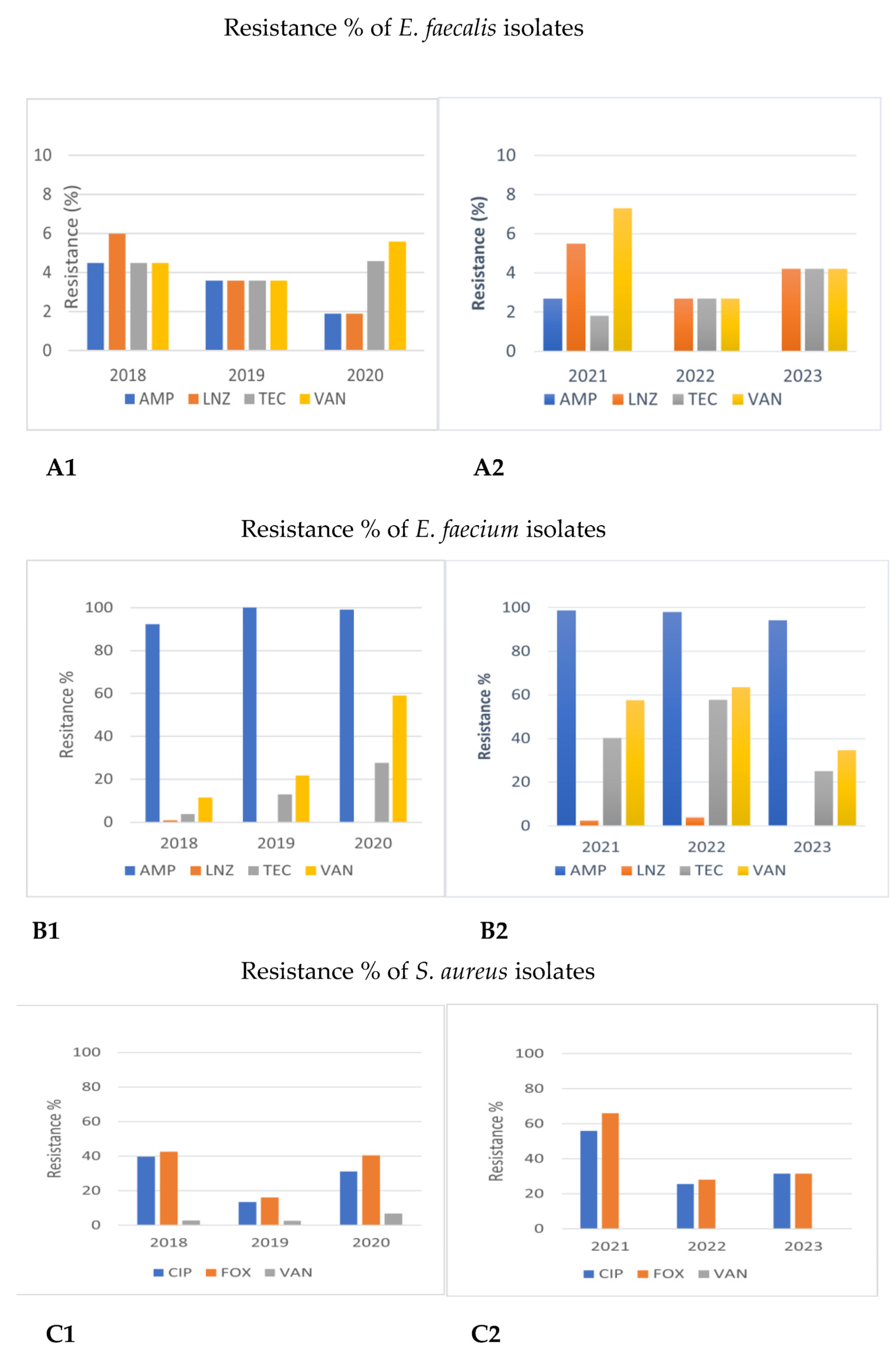
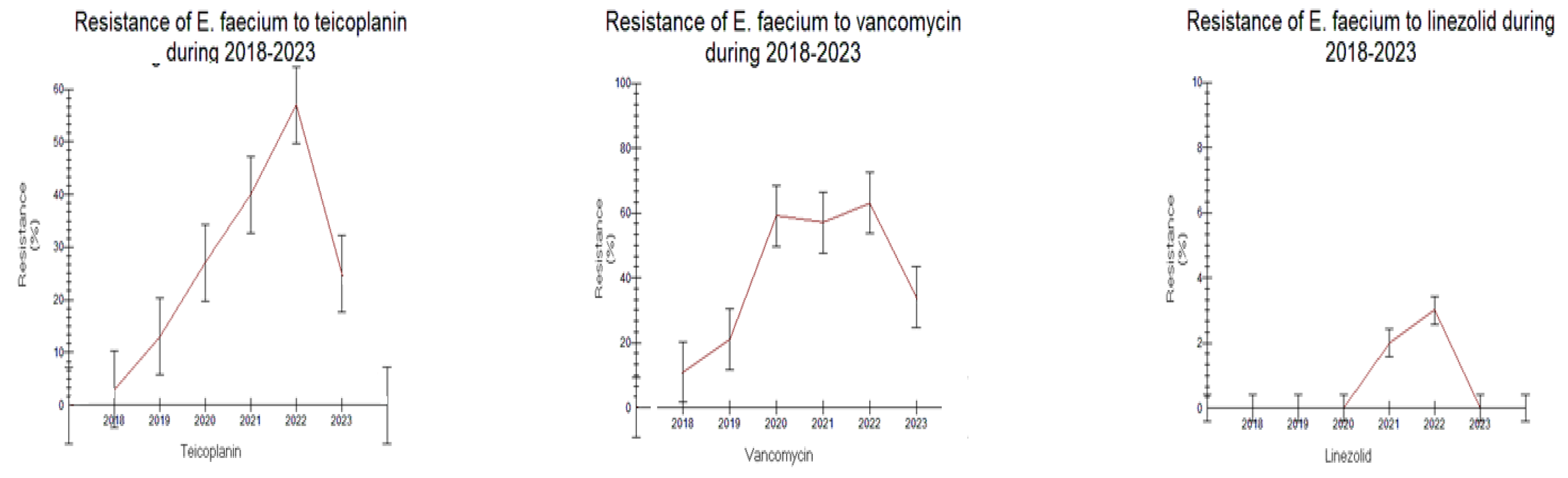
Gram-Positive Cocci
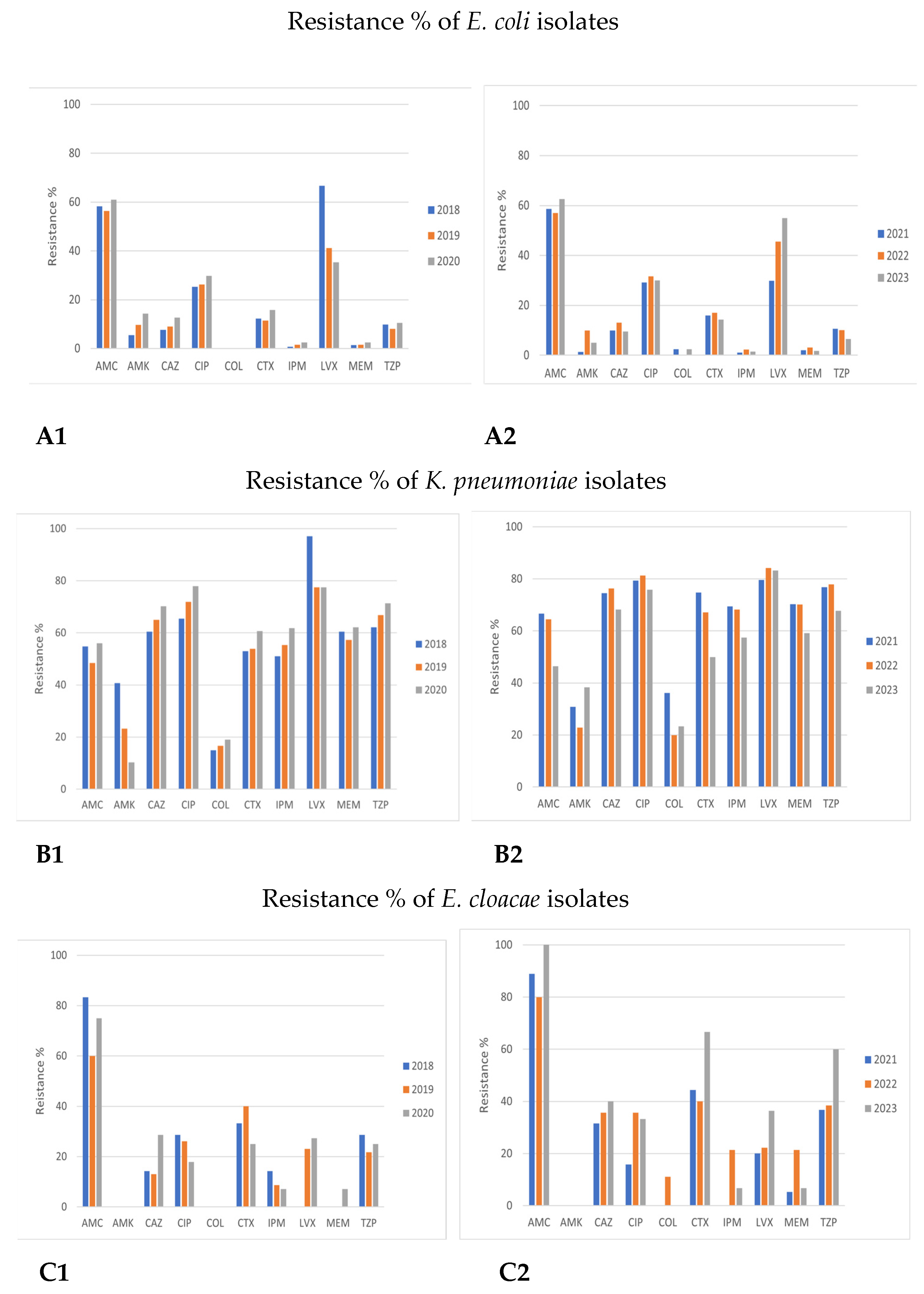
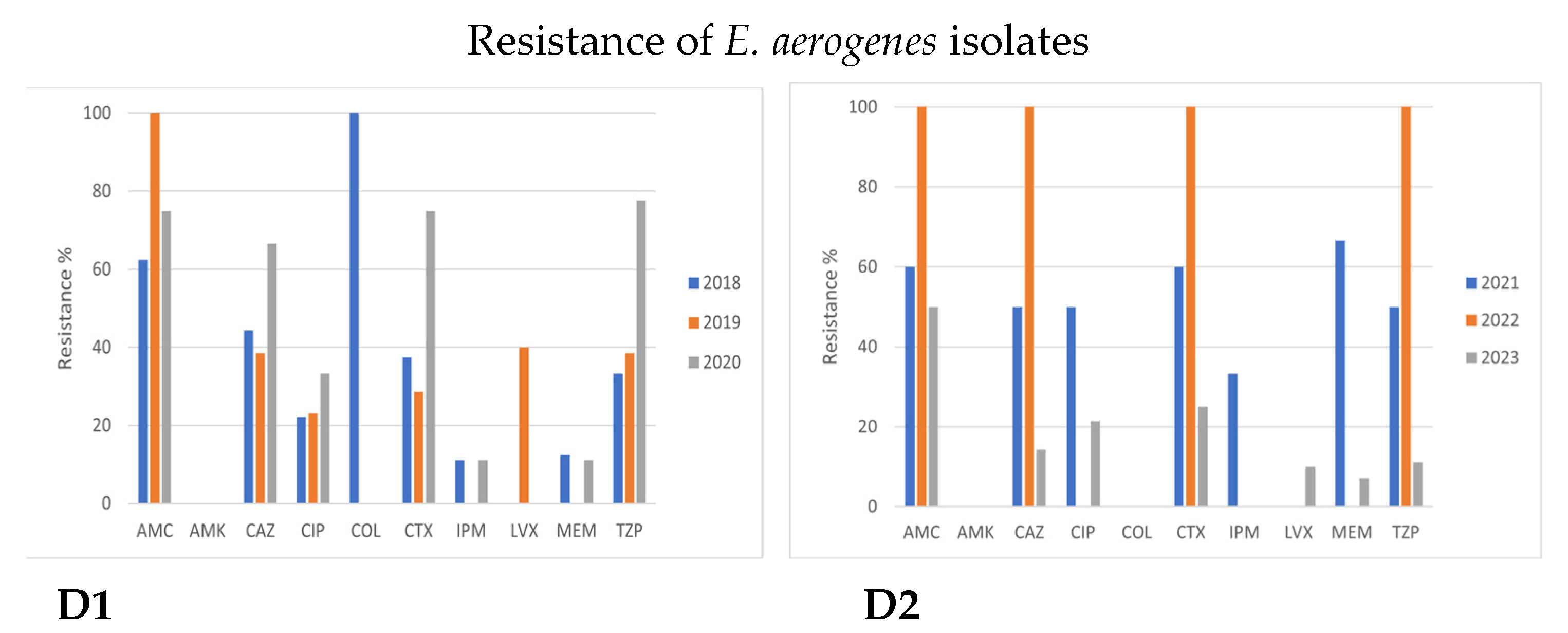
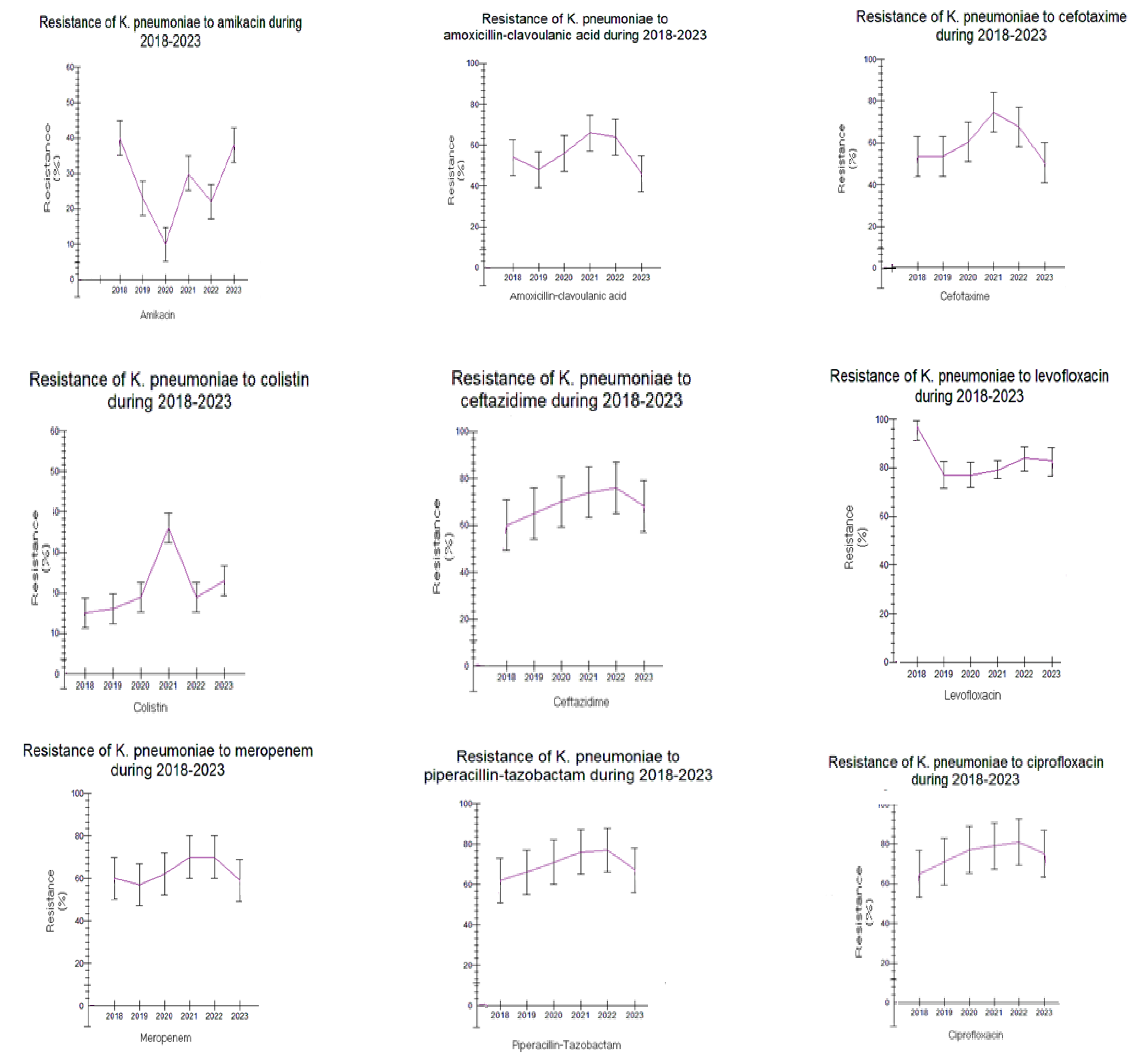
Enterobacterales
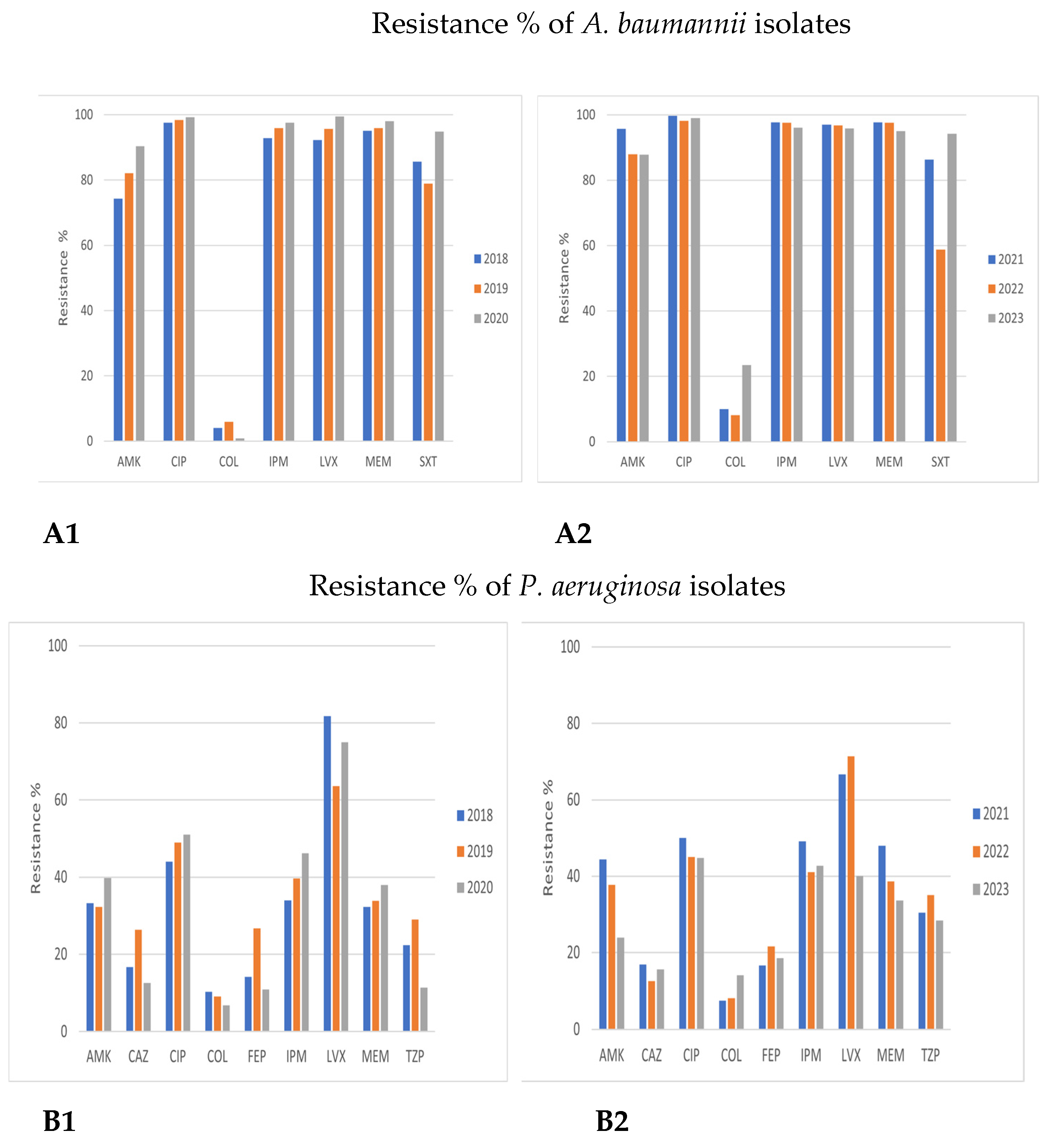
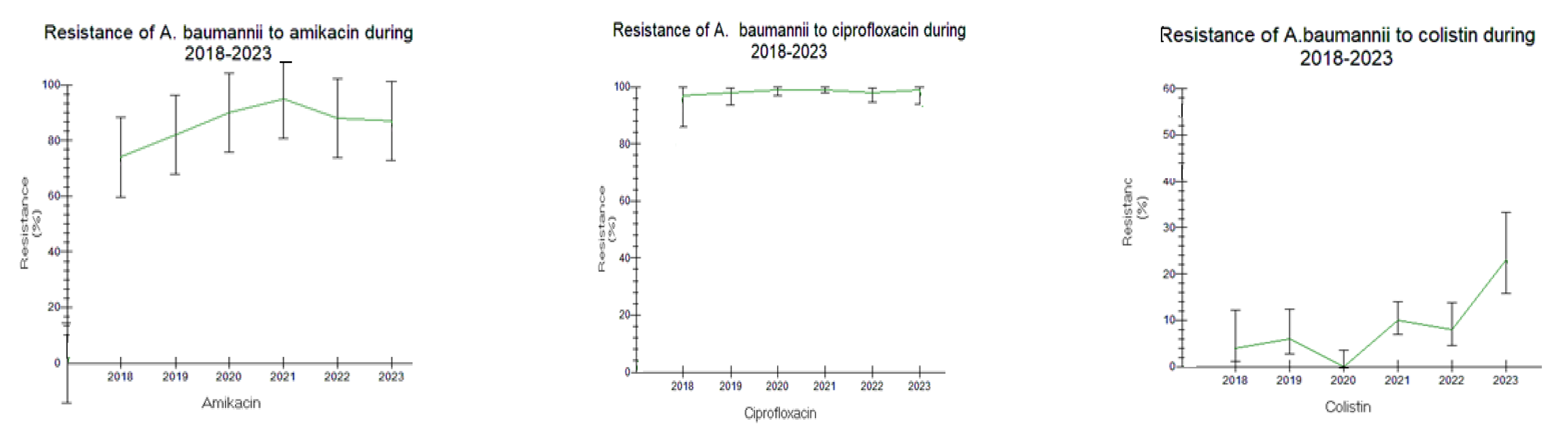
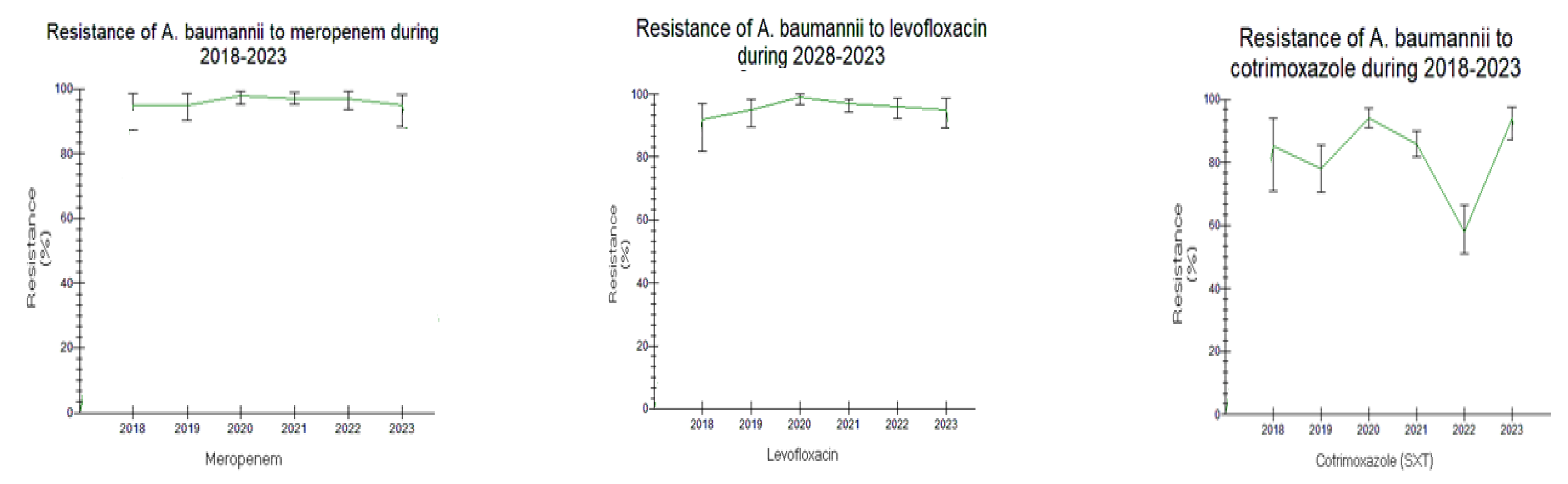
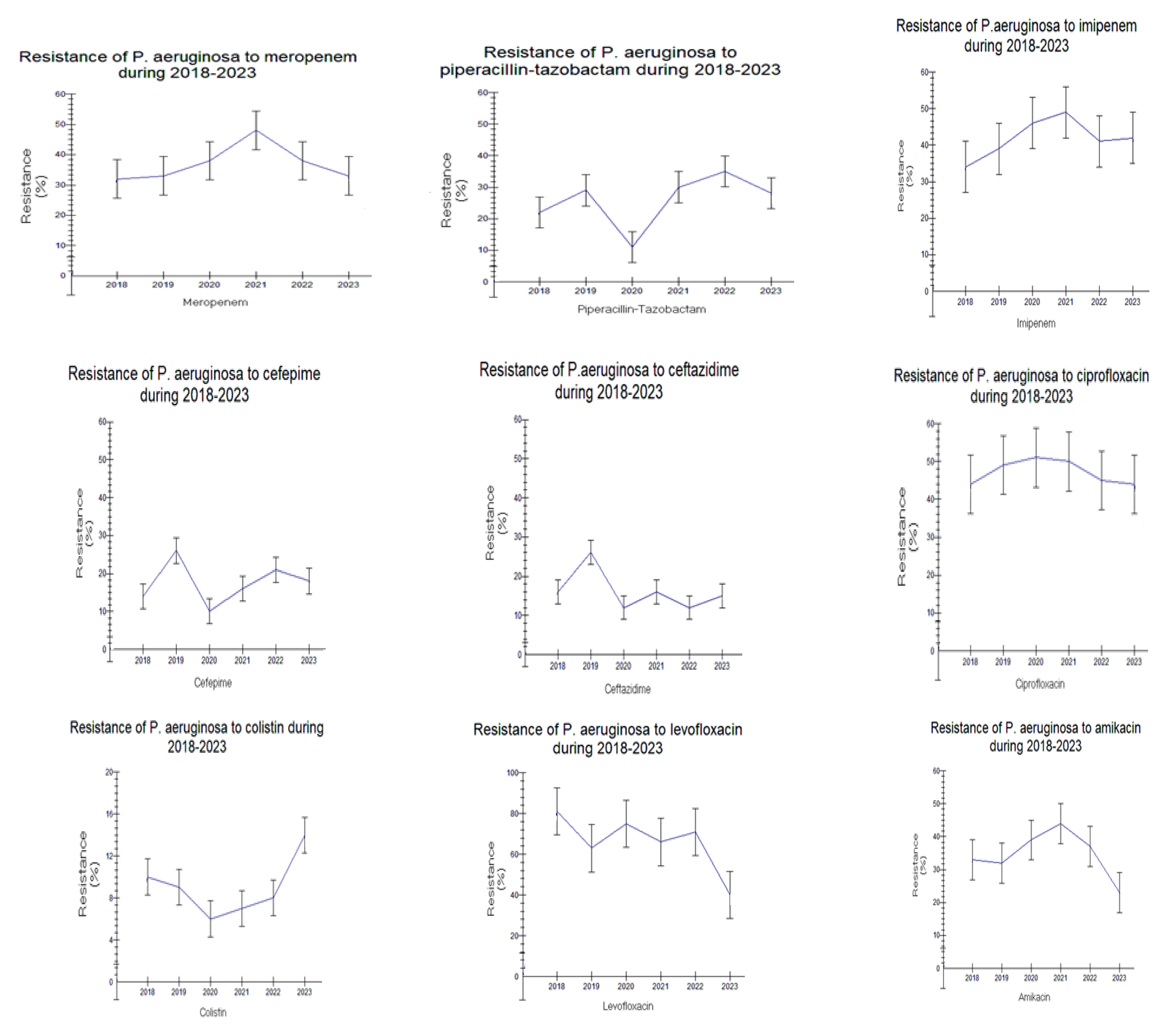
Acinetobacter baumannii and Pseudomonas aeruginosa
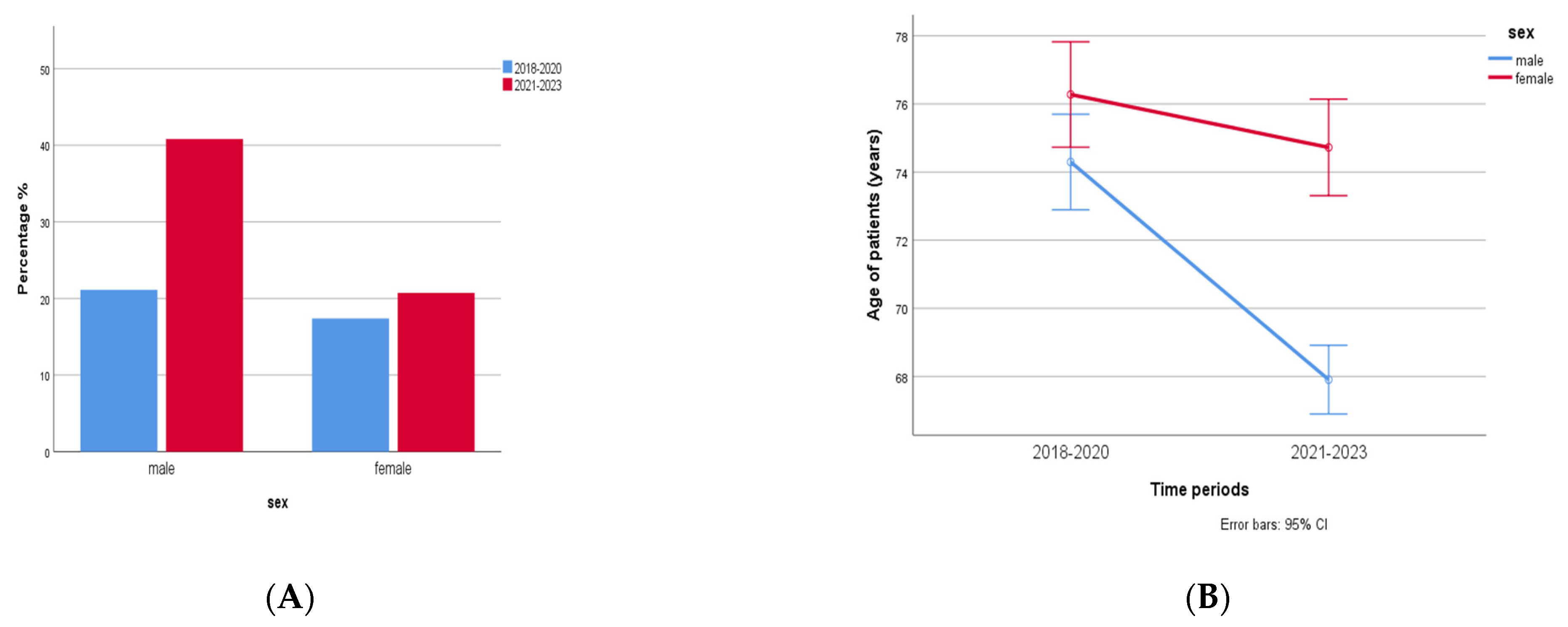
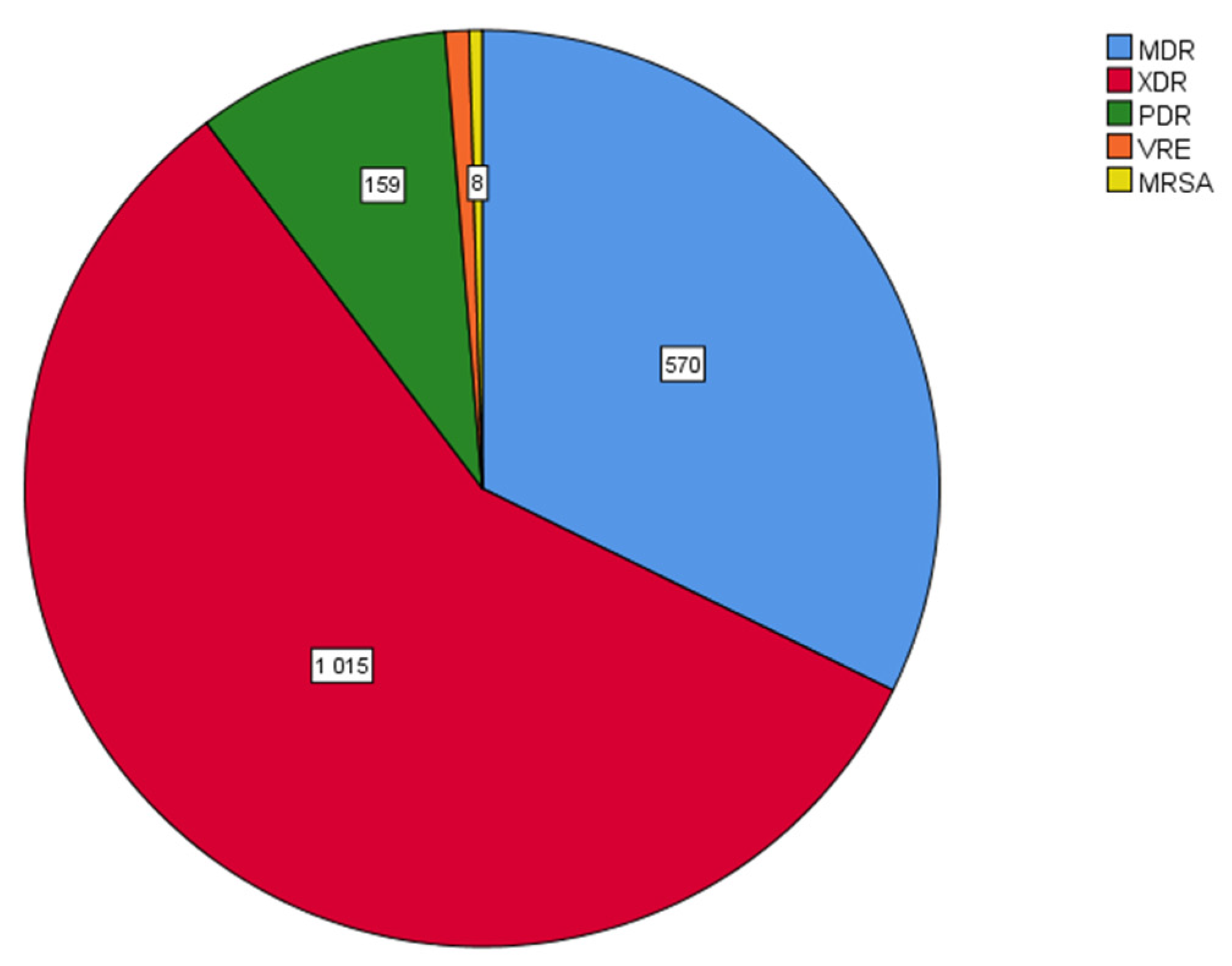
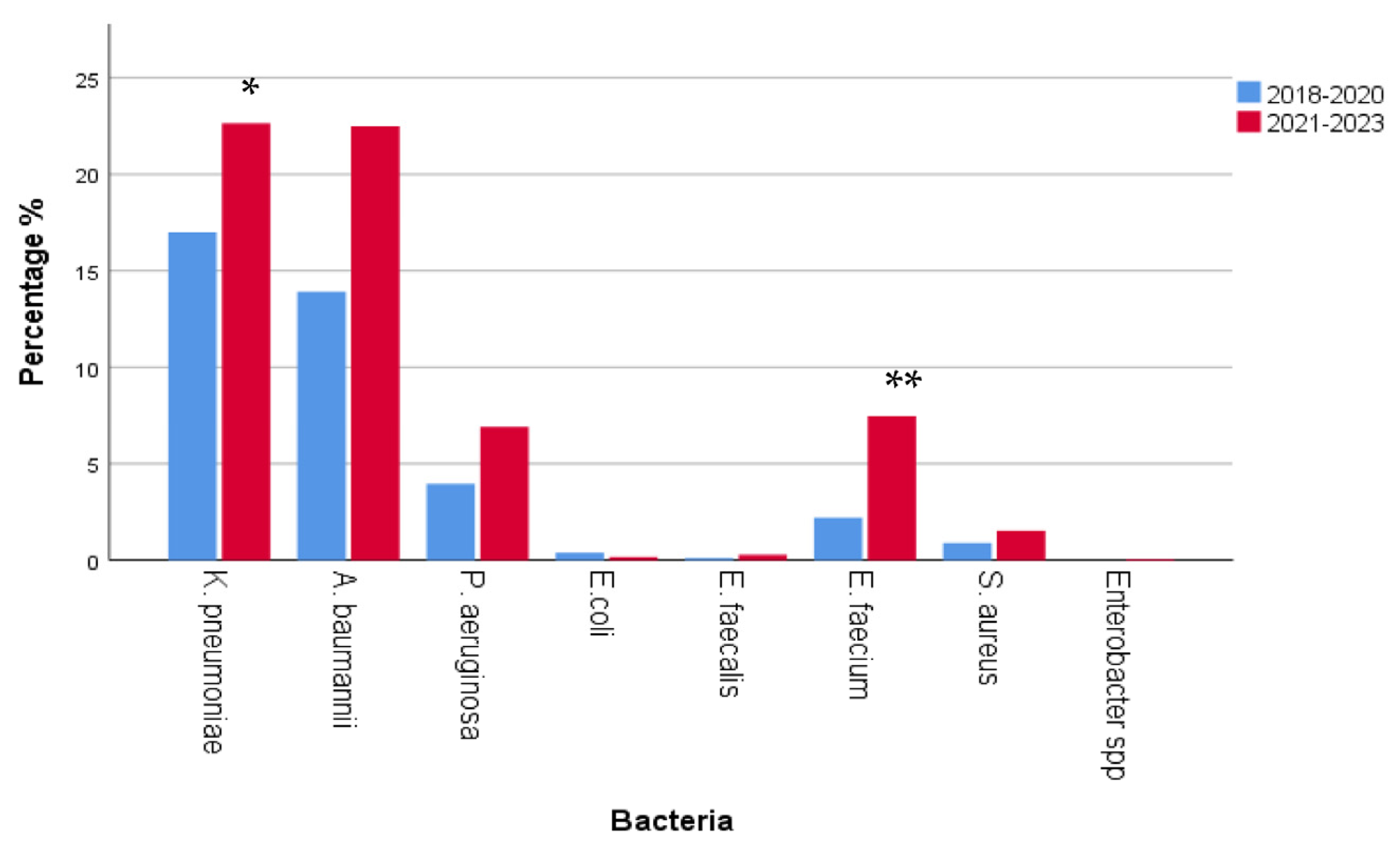
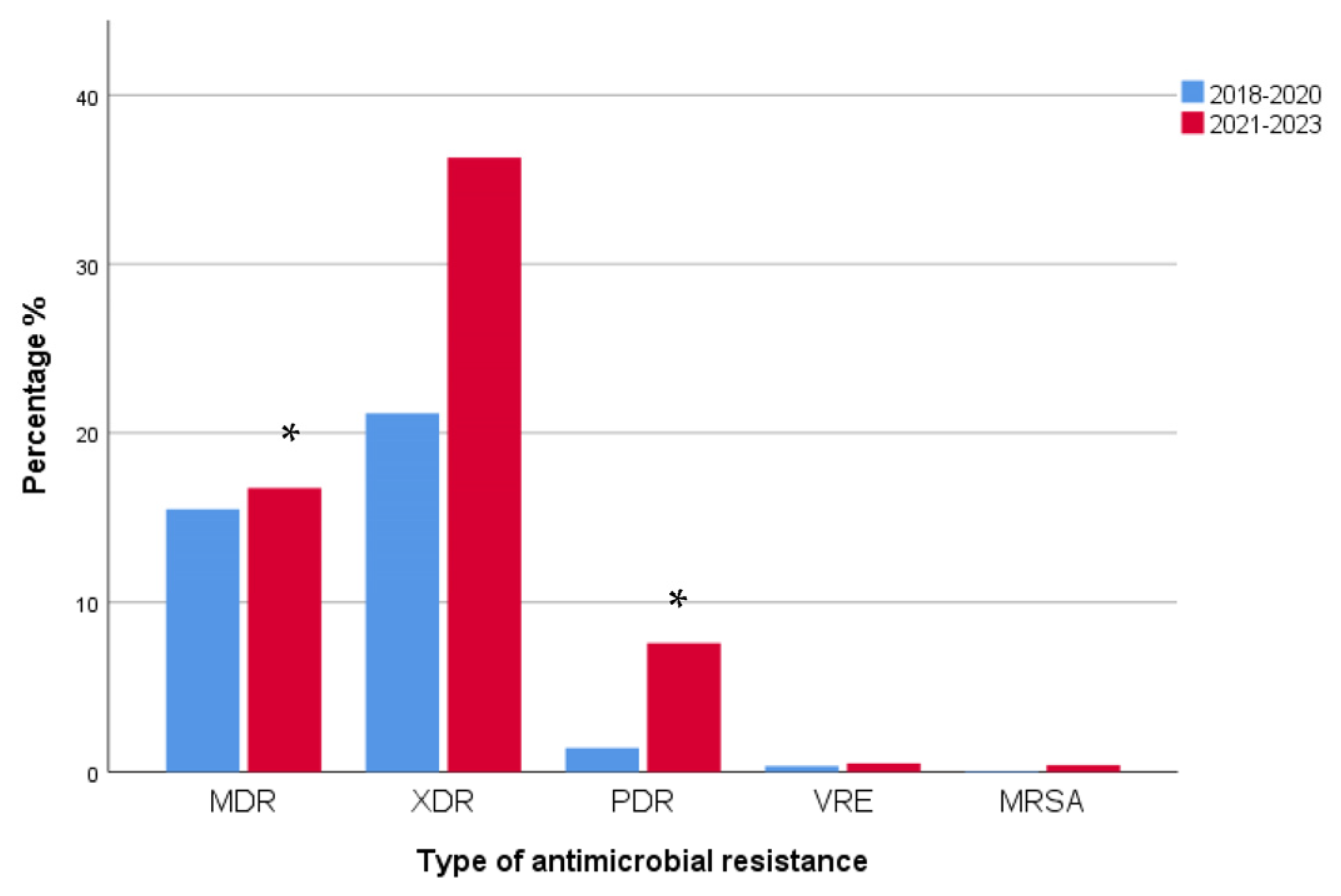
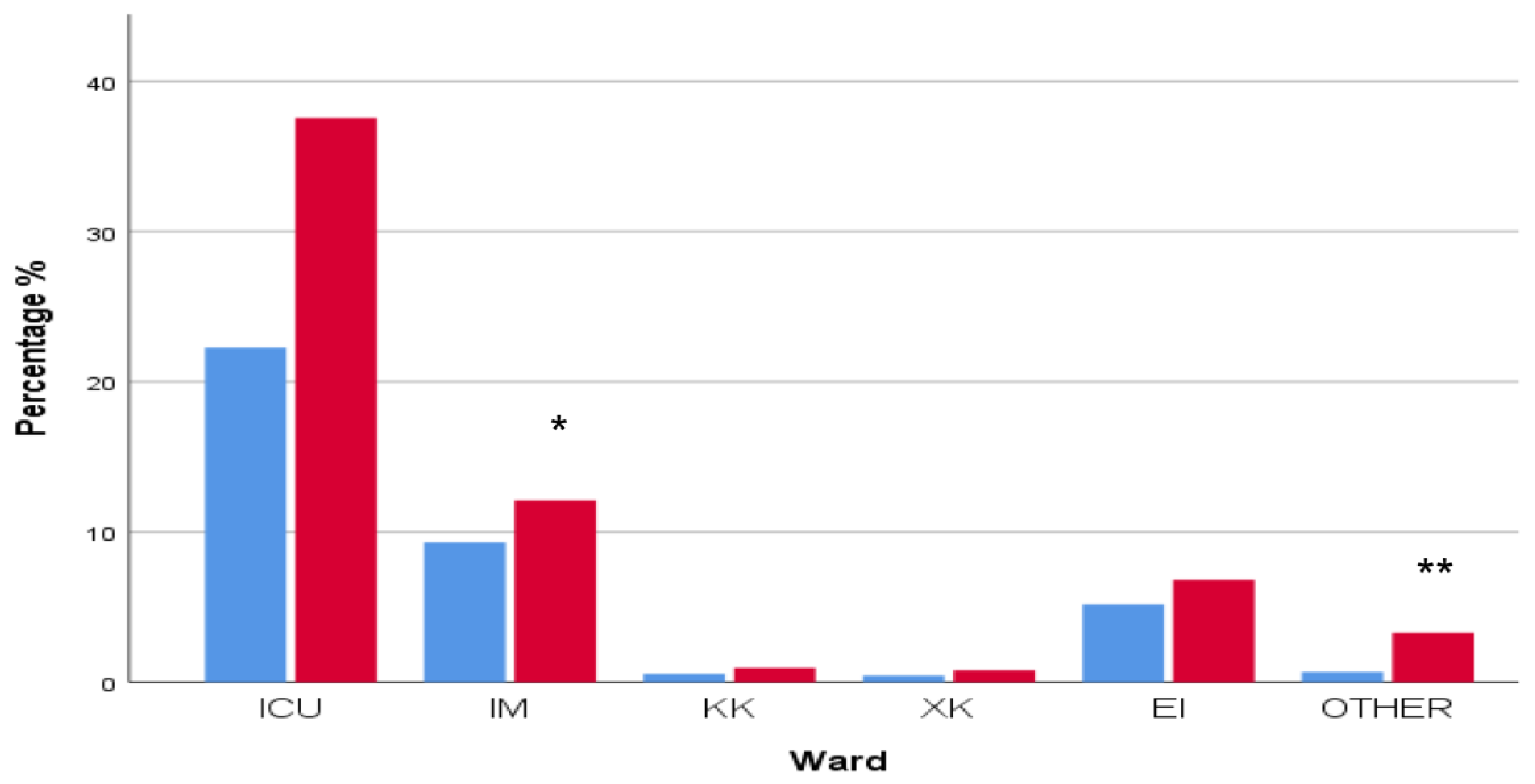
2.2. Epidemiology and Prevalence of Multidrug-Resistant (MDR) Clinical Isolates in 2018–2020 and 2021–2023
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization Ten Threats to Global Health in 2019. Available online: https://www.who.int/emergencies/ten-threats-to-global-health-in-2019 (accessed on 24 August 2023).
- One Health Global Leaders Group on Antimicrobial Resistance. World leaders join forces to fight the accelerating crisis of an antimicrobial resistance. Neurosciences 2021, 26, 112–113. [Google Scholar]
- Mancuso, G.; Midiri, A.; Gerace, E.; Biondo, C. Bacterial antibiotic resistance: The most critical pathogens. Pathogens 2021, 10, 1310. [Google Scholar] [CrossRef] [PubMed]
- Cassini, A.; Högberg, L.D.; Plachouras, D.; Quattrocchi, A.; Hoxha, A.; Simonsen, G.S.; Colomb-Cotinat, M.; Kretzschmar, M.E.; Devleesschauwer, B.; Cecchini, M.; et al. Attributable deaths and disability-adjusted life-years caused by infections with antibiotic-resistant bacteria in the EU and the European Economic Area in 2015: A population-level modelling analysis. Lancet Infect. Dis. 2019, 19, 56–66. [Google Scholar] [CrossRef]
- Kopsidas, I.; Theodosiadis, D.; Triantafyllou, C.; Koupidis, S.; Fanou, A.; Hatzianastasiou, S. Preventing Antimicrobial Resistance and Promoting Appropriate Antimicrobial Use in Inpatient Health Care in Greece 2022 (No. WHO/EURO: 2022-5837-45602-65411); World Health Organization; Regional Office for Europe: København, Denmark, 2022. [Google Scholar]
- Polemis, M.; Tryfinopoulou, K.; Giakkoupi, P.; Vatopoulos, A. WHONET-Greece Study Group. Eight-year trends in the relative isolation frequency and antimicrobial susceptibility among bloodstream isolates from Greek hospitals: Data from the Greek Electronic System for the Surveillance of Antimicrobial Resistance–WHONET-Greece, 2010 to 2017. EuroSurveil 2020, 25, 1900516. [Google Scholar]
- Polemis, M.; Mandilara, G.; Pappa, O.; Argyropoulou, A.; Perivolioti, E.; Koudoumnakis, N.; Pournaras, S.; Vasilakopoulou, A.; Vourli, S.; Katsifa, H.; et al. COVID-19 and Antimicrobial Resistance: Data from the Greek Electronic System for the Surveillance of Antimicrobial Resistance—WHONET-Greece (January 2018–March 2021). Life 2021, 11, 996. [Google Scholar] [CrossRef]
- World Health Organization. Antimicrobial Resistance: Global Report on Surveillance. 2014. Available online: https://www.who.int/antimicrobial-resistance/publications/surveillancereport/en/ (accessed on 23 August 2023).
- Centers for Disease Control and Prevention. Antibiotic Resistant Threats in the United States. 2019. Available online: https://www.cdc.gov/drugresistance/pdf/threats-report/2019-ar-threats-report-508.pdf (accessed on 20 August 2023).
- Weist, K.; Hogberg, L.D. ECDC publishes 2015 surveillance data on antimicrobial resistance and antimicrobial consumption in Europe. Euro Surveill. 2016, 21, 30401. [Google Scholar] [CrossRef]
- Kayange, N.; Kamugisha, E.; Mwizamholya, D.L.; Jeremiah, S.; Mshana, S.E. Predictors of positive blood culture and deaths among neonates with suspected neonatal sepsis in a tertiary hospital, Mwanza-Tanzania. BMC Pediatr. 2010, 10, 39. [Google Scholar] [CrossRef] [PubMed]
- Seijas-Pereda, L.; Rescalvo-Casas, C.; Hernando-Gozalo, M.; Angmorkie-Eshun, V.; Agyei, E.; Adu-Gyamfi, V.; Sarsah, I.; Alfonso-Romero, M.; Cuadros-González, J.; Soliveri-de Carranza, J.; et al. The Antimicrobial Resistance (AMR) Rates of Enterobacterales in a Rural Hospital from the Eastern Region, Ghana: A Retrospective Study, 2022. Antibiotics 2023, 12, 1321. [Google Scholar] [CrossRef] [PubMed]
- Akova, M. Epidemiology of antimicrobial resistance in bloodstream infections. Virulence 2016, 7, 252–266. [Google Scholar] [CrossRef]
- Rice, L.B. Federal funding for the study of antimicrobial resistance in nosocomial pathogens: No ESKAPE. J. Infect. Dis. 2008, 197, 1079–1081. [Google Scholar] [CrossRef]
- Mulani, M.S.; Kamble, E.; Kumkar, S.N.; Tawre, M.S.; Pardesi, K.R. Emerging Strategies to Combat ESKAPE Pathogens in the Era of Antimicrobial Resistance: A Review. Front. Microbiol. 2019, 10, 539. [Google Scholar] [CrossRef]
- De Oliveira, D.M.P.; Forde, B.M.; Kidd, T.J.; Harris, P.N.A.; Schembri, M.A.; Beatson, S.A.; Paterson, D.L.; Walker, M.J. Antimicrobial Resistance in ESKAPE Pathogens. Clin. Microbiol. Rev. 2020, 33, e00181-19. [Google Scholar] [CrossRef]
- Beatson, S.A.; Walker, M.J. Microbiology. Tracking antibiotic resistance. Science 2014, 345, 1454–1455. [Google Scholar] [CrossRef]
- Bin Zaman, S.; Hussain, M.A.; Nye, R.; Mehta, V.; Mamun, K.T.; Hossain, N. A review on antibiotic resistance: Alarm bells are ringing. Cureus 2017, 9, e1403. [Google Scholar] [CrossRef]
- Naylor, N.R.; Atun, R.; Zhu, N.; Kulasabanathan, K.; Silva, S.; Chatterjee, A.; Knight, G.M.; Robotham, J.V. Estimating the burden of antimicrobial resistance: A systematic literature review. Antimicrob. Resist. Infect. Control 2018, 7, 58. [Google Scholar] [CrossRef] [PubMed]
- Iguchi, S.; Mizutani, T.; Hiramatsu, K.; Kikuchi, K. Rapid acquisition of linezolid resistance in methicillin-resistant Staphylococcus aureus: Role of hypermutation and homologous recombination. PLoS ONE 2016, 11, e0155512. [Google Scholar] [CrossRef] [PubMed]
- Giddins, M.J.; Macesic, N.; Annavajhala, M.K.; Stump, S.; Khan, S.; McConville, T.H.; Mehta, M.; Gomez-Simmonds, A.; Uhleman, A.-C. Successive emergence of ceftazidime-avibactam resistance through distinct genomic adaptations in bla (KPC-2)-harboring Klebsiella pneumoniae sequence type 307 isolates. Antimicrob. Agents Chemother. 2017, 62, e02101-17. [Google Scholar] [CrossRef]
- Herc, E.S.; Kauffman, C.A.; Marini, B.L.; Perissinotti, A.J.; Miceli, M.H. Daptomycin nonsusceptible vancomycin resistant Enterococcus bloodstream infections in patients with hematological malignancies: Risk factors and outcomes. Leuk. Lymphoma 2017, 58, 2852–2858. [Google Scholar] [CrossRef] [PubMed]
- Paterson, D.L.; Bonomo, R.A. Extended-spectrum beta-lactamases: A clinical update. Clin. Microbiol. Rev. 2005, 18, 657–686. [Google Scholar] [CrossRef]
- Kussmann, M.; Karer, M.; Obermueller, M.; Schmidt, K.; Barousch, W.; Moser, D.; Nehr, M.; Ramharter, M.; Poeppl, W.; Makristathis, A.; et al. Emergence of a dalbavancin induced glycopeptide/lipoglycopeptide non-susceptible Staphylococcus aureus during treatment of a cardiac device-related endocarditis. Emerg. Microbes Infect. 2018, 7, 202. [Google Scholar] [CrossRef]
- Census Results of the Population-Residents for the Year 2021 Concerning the Legal Population (Citizens) of Greece. Government Gazette 6951/Β/30 December 2022. Archived from the Original on 21 April 2023—Via Hellenic Statistical Authority (ELSTAT). Available online: https://olympiobima.gr/apografi-2021-se-123-245-atoma-o-plithysmos-tis-pierias-pinakas/ (accessed on 18 August 2023).
- European Centre for Disease Prevention and Control. Surveillance of Antimicrobial Resistance in Europe—Annual Report of the European Antimicrobial Resistance Surveillance Network (EARS-Net) 2017; ECDC: Stockholm, Sweden, 2018.
- Vatopoulos, A. High rates of metallo-beta-lactamase-producing Klebsiella pneumoniae in Greece—A review of the current evidence. Euro Surveill. 2008, 13, 8023. [Google Scholar] [CrossRef] [PubMed]
- Maltezou, H.C.; Giakkoupi, P.; Maragos, A.; Bolikas, M.; Raftopoulos, V.; Papahatzaki, H.; Vrouhos, G.; Liakou, V.; Vatopoulos, A.C. Outbreak of infections due to KPC-2-producing Klebsiella pneumoniae in a hospital in Crete (Greece). J. Infect. 2009, 58, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Giakkoupi, P.; Maltezou, H.; Polemis, M.; Pappa, O.; Saroglou, G.; Vatopoulos, A. Greek System for the Surveillance of Antimicrobial Resistance KPC-2-producing Klebsiella pneumoniae infections in Greek hospitals are mainly due to a hyperepidemic clone. Euro Surveill. 2009, 14, 19218. [Google Scholar] [CrossRef]
- Voulgari, E.; Gartzonika, C.; Vrioni, G.; Politi, L.; Priavali, E.; Levidiotou-Stefanou, S.; Tsakris, A. The Balkan region: NDM-1-producing Klebsiella pneumoniae ST11 clonal strain causing outbreaks in Greece. J. Antimicrob. Chemother. 2014, 69, 2091–2097. [Google Scholar] [CrossRef] [PubMed]
- Giakkoupi, P.; Tryfinopoulou, K.; Kontopidou, F.; Tsonou, P.; Golegou, T.; Souki, H.; Tzouvelekis, L.; Miriagou, V.; Vatopoulos, A. Emergence of NDM-producing Klebsiella pneumoniae in Greece. Diagn. Microbiol. Infect. Dis. 2013, 77, 382–384. [Google Scholar] [CrossRef]
- Grundmann, H.; Glasner, C.; Albiger, B.; Aanensen, D.M.; Tomlinson, C.T.; Andrasević, A.T.; Tzouvelekis, L.; Miriagou, V.; Vatopoulos, A. European Survey of Carbapenemase-Producing Enterobacterales (EuSCAPE) Working Group Occurrence of carbapenemase-producing Klebsiella pneumoniae and Escherichia coli in the European survey of carbapenemase-producing Enterobacterales (EuSCAPE): A prospective, multinational study. Lancet Infect. Dis. 2017, 17, 153–163. [Google Scholar]
- Galani, I.; Karaiskos, I.; Karantani, I.; Papoutsaki, V.; Maraki, S.; Papaioannou, V.; Tsorlini, H.; Charalampaki, N.; Toutouza, M.; Vagiakou, H.; et al. On Behalf of The Study Collaborators Epidemiology and resistance phenotypes of carbapenemase-producing Klebsiella pneumoniae in Greece, 2014 to 2016. Euro Surveill. 2018, 23, 1700775. [Google Scholar] [CrossRef]
- Voulgari, E.; Zarkotou, O.; Ranellou, K.; Karageorgopoulos, D.E.; Vrioni, G.; Mamali, V.; Themeli-Digalaki, K.; Tsakris, A. Outbreak of OXA-48 carbapenemase-producing Klebsiella pneumoniae in Greece involving an ST11 clone. J. Antimicrob. Chemother. 2013, 68, 84–88. [Google Scholar] [CrossRef]
- Dey, D.K.; Park, J.; Kang, S.C. Genotypic, phenotypic, and pathogenic characterization of the soil isolated Acinetobacter courvalinii. Microb. Pathog. 2020, 149, 104287. [Google Scholar] [CrossRef]
- Oikonomou, O.; Sarrou, S.; Papagiannitsis, C.C.; Georgiadou, S.; Mantzarlis, K.; Zakynthinos, E.; Dalekos, G.N.; Petinaki, E. Rapid dissemination of colistin and carbapenem resistant Acinetobacter baumannii in Central Greece: Mechanisms of resistance, molecular identification and epidemiological data. BMC Infect. Dis. 2015, 15, 559. [Google Scholar] [CrossRef]
- Pournaras, S.; Dafopoulou, K.; Del Franco, M.; Zarkotou, O.; Dimitroulia, E.; Protonotariou, E.; Poulou, A.; Zarrilli, R.; Tsakris, A. Greek Study Group on Acinetobacter Antimicrobial Resistance Predominance of international clone 2 OXA-23-producing-Acinetobacter baumannii clinical isolates in Greece, 2015: Results of a nationwide study. Int. J. Antimicrob. Agents 2017, 49, 749–753. [Google Scholar] [CrossRef] [PubMed]
- European Committee on Antimicrobial Susceptibility Testing (EUCAST). Recommendations for MIC Determination of Colistin (Polymyxin E) as Recommended by the Joint CLSI-EUCAST Polymyxin Breakpoints Working Group. EUCAST. 2016. Available online: http://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/General_documents/Recommendations_for_MIC_determination_of_colistin_March_2016.pdf (accessed on 5 March 2021).
- Samaras, K.; Tsalidou, M.; Goutsiou, R.; Bostanitis, I.; Varsou, E.; Bostanitis, C.; Gara, S. Colistin susceptibility testing methods of Acinetobacter baumannii isolates: Verifying accuracy and reliability among two methods. In Proceedings of the 31st ECCMID, Vienna, Austria, 9–12 July 2021. [Google Scholar]
- Tsakris, A.; Pournaras, S.; Woodford, N.; Palepou MF, I.; Babini, G.S.; Douboyas, J.; Livermore, D.M. Outbreak of infections caused by Pseudomonas aeruginosa producing VIM-1 carbapenemase in Greece. J. Clin. Microbiol. 2000, 38, 1290–1292. [Google Scholar] [CrossRef]
- Giakkoupi, P.; Petrikkos, G.; Tzouvelekis, L.S.; Tsonas, S.; Legakis, N.J.; Vatopoulos, A.C. WHONET Greece Study Group Spread of integron-associated VIM-type metallo-beta-lactamase genes among imipenem-nonsusceptible Pseudomonas aeruginosa strains in Greek hospitals. J. Clin. Microbiol. 2003, 41, 822–825. [Google Scholar] [CrossRef]
- Meletis, G.; Vavatsi, N.; Exindari, M.; Protonotariou, E.; Sianou, E.; Haitoglou, C.; Sofianou, D.; Pournaras, S.; Diza, E. Accumulation of carbapenem resistance mechanisms in VIM-2-producing Pseudomonas aeruginosa under selective pressure. Eur. J. Clin. Microbiol. Infect. Dis. 2014, 33, 253–258. [Google Scholar] [CrossRef]
- Liakopoulos, A.; Mavroidi, A.; Katsifas, E.A.; Theodosiou, A.; Karagouni, A.D.; Miriagou, V.; Petinaki, E. Carbapenemase-producing Pseudomonas aeruginosa from central Greece: Molecular epidemiology and genetic analysis of class I integrons. BMC Infect. Dis. 2013, 13, 505. [Google Scholar] [CrossRef]
- Zhang, J.J.; Dong, X.; Liu, G.H.; Gao, Y.D. Risk and Protective Factors for COVID-19 Morbidity, Severity, and Mortality. Clin. Rev. Allergy Immunol. 2023, 64, 90–107. [Google Scholar] [CrossRef]
- Papaioannidou, P.; Skoumpa, K.; Bostanitis, C.; Michailidou, M.; Stergiopoulou, T.; Bostanitis, I.; Tsalidou, M. Age, Sex and BMI Relations with Anti-SARS-CoV-2-Spike IgG Antibodies after BNT162b2 COVID-19 Vaccine in Health Care Workers in Northern Greece. Microorganisms 2023, 13, 1279. [Google Scholar] [CrossRef]
- Vassilaki, N.; Gargalionis, A.N.; Bletsa, A.; Papamichalopoulos, N.; Kontou, E.; Gkika, M.; Patas, K.; Theodoridis, D.; Manolis, I.; Ioannidis, A.; et al. Impact of Age and Sex on Antibody Response Following the Second Dose of COVID-19 BNT162b2 mRNA Vaccine in Greek Healthcare Workers. Microorganisms 2021, 13, 1725. [Google Scholar] [CrossRef] [PubMed]
- La, Y.; Hong, J.Y.; Lee, H.S.; Lee, E.H.; Lee, K.H.; Song, Y.G.; Kim, S.B.; Han, S.H. Increase of multidrug-resistant bacteria after the COVID-19 pandemic in South Korea: Time-series analyses of a long-term multicenter cohort. J. Infect. 2022, 85, 702–769. [Google Scholar] [CrossRef]
- Hu, S.; You, Y.; Zhang, S.; Tang, J.; Chen, C.; Wen, W.; Wang, C.; Cheng, Y.; Zhou, M.; Feng, Z. Multidrug-resistant infection in COVID-19 patients: A meta-analysis. J. Infect. 2023, 86, 66–117. [Google Scholar] [CrossRef] [PubMed]
- Magiorakos, A.P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria. Clin. Microbiol. Infect. 2012, 1, 268–281. [Google Scholar] [CrossRef] [PubMed]


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Bacterial Strains | 2018 No. | 2019 No. | 2020 No. | 2021 No. | 2022 No. | 2023 No. | Total No. | Mean % * |
|---|---|---|---|---|---|---|---|---|
| Enterococcus faecalis | 69 | 60 | 111 | 113 | 77 | 25 | 455 | 3.7 |
| Enterococcus faecium | 33 | 48 | 106 | 176 | 106 | 54 | 523 | 4.3 |
| Staphylococcus aureus | 70 | 38 | 76 | 60 | 39 | 19 | 302 | 2.5 |
| Escherichia coli | 1033 | 954 | 779 | 759 | 651 | 409 | 4585 | 37.4 |
| Klebsiella pneumoniae | 366 | 377 | 391 | 563 | 302 | 236 | 2235 | 18.2 |
| Enterobacter cloacae | 15 | 15 | 8 | 25 | 33 | 20 | 116 | 0.95 |
| Enterobacter aerogenes | 9 | 14 | 9 | 6 | 2 | 14 | 54 | 0.44 |
| Acinetobacter baumannii | 86 | 127 | 253 | 314 | 172 | 106 | 1058 | 8.6 |
| Pseudomonas aeruginosa | 228 | 145 | 208 | 274 | 174 | 97 | 1126 | 9.2 |
| Total | 2205 | 2140 | 2321 | 2658 | 1800 | 1150 | 12,274 | 100 |
| Cultures | 2018 No. | 2019 No. | 2020 No. | 2021 No. | 2022 No. | 2023 No. |
|---|---|---|---|---|---|---|
| Urine | 1714 (78%) | 1582 (75%) | 1498 (65%) | 1658 (63%) | 1293 (72%) | 807 (71%) |
| Blood | 124 (6%) | 144 (7%) | 229 (10%) | 260 (10%) | 156 (9%) | 111 (10%) |
| Pharyngeal | 53 (2%) | 78 (4%) | 128 (6%) | 175 (7%) | 89 (5%) | 52 (5%) |
| Rectal | 53 (2%) | 70 (3%) | 138 (6%) | 193 (7%) | 68 (4%) | 51 (4%) |
| Catheter | 27 (1%) | 46 (2%) | 100 (4%) | 121 (5%) | 38 (2%) | 28 (2%) |
| Bronchial | 46 (2%) | 64 (3%) | 56 (2%) | 63 (2%) | 13 (1%) | 28 (2%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsalidou, M.; Stergiopoulou, T.; Bostanitis, I.; Nikaki, C.; Skoumpa, K.; Koutsoukou, T.; Papaioannidou, P. Surveillance of Antimicrobial Resistance and Multidrug Resistance Prevalence of Clinical Isolates in a Regional Hospital in Northern Greece. Antibiotics 2023, 12, 1595. https://doi.org/10.3390/antibiotics12111595
Tsalidou M, Stergiopoulou T, Bostanitis I, Nikaki C, Skoumpa K, Koutsoukou T, Papaioannidou P. Surveillance of Antimicrobial Resistance and Multidrug Resistance Prevalence of Clinical Isolates in a Regional Hospital in Northern Greece. Antibiotics. 2023; 12(11):1595. https://doi.org/10.3390/antibiotics12111595
Chicago/Turabian StyleTsalidou, Maria, Theodouli Stergiopoulou, Ioannis Bostanitis, Christina Nikaki, Kalypso Skoumpa, Theofani Koutsoukou, and Paraskevi Papaioannidou. 2023. "Surveillance of Antimicrobial Resistance and Multidrug Resistance Prevalence of Clinical Isolates in a Regional Hospital in Northern Greece" Antibiotics 12, no. 11: 1595. https://doi.org/10.3390/antibiotics12111595