
The Accuracy of Molecular Detection Targeting the Mutation C2611T for Detecting Moderate-Level Azithromycin Resistance in Neisseria gonorrhoeae: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Methods
2.1. Literature Search and Study Selection
2.2. Data Extraction
2.3. Quality Assessment
2.4. Statistical Analyses
3. Results
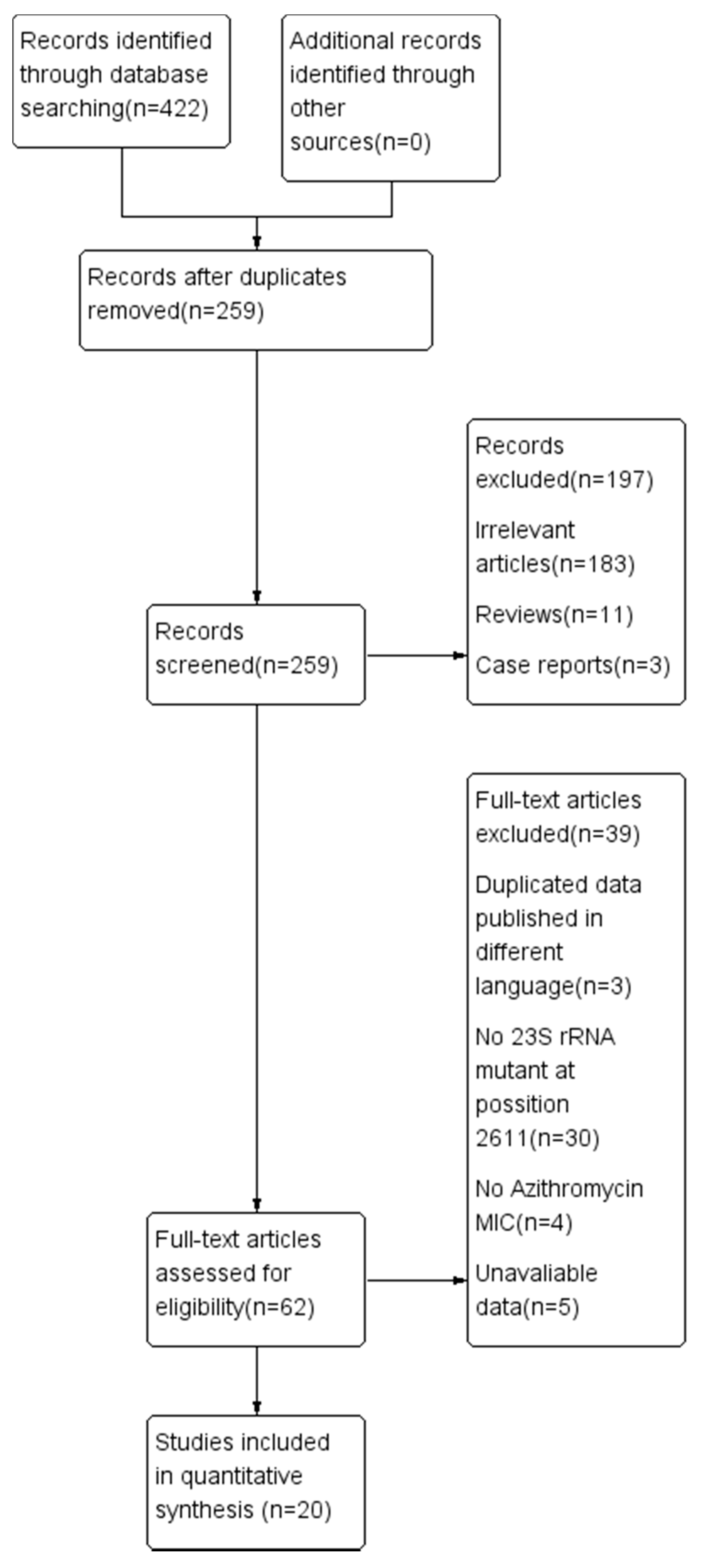
3.1. Study Selection
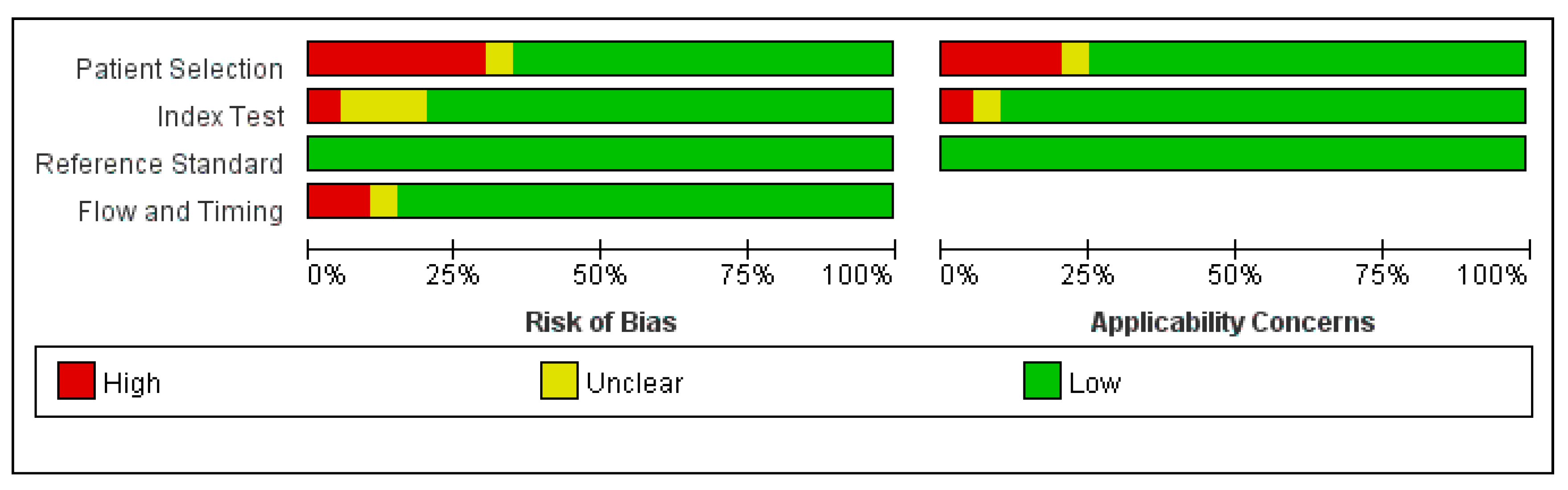
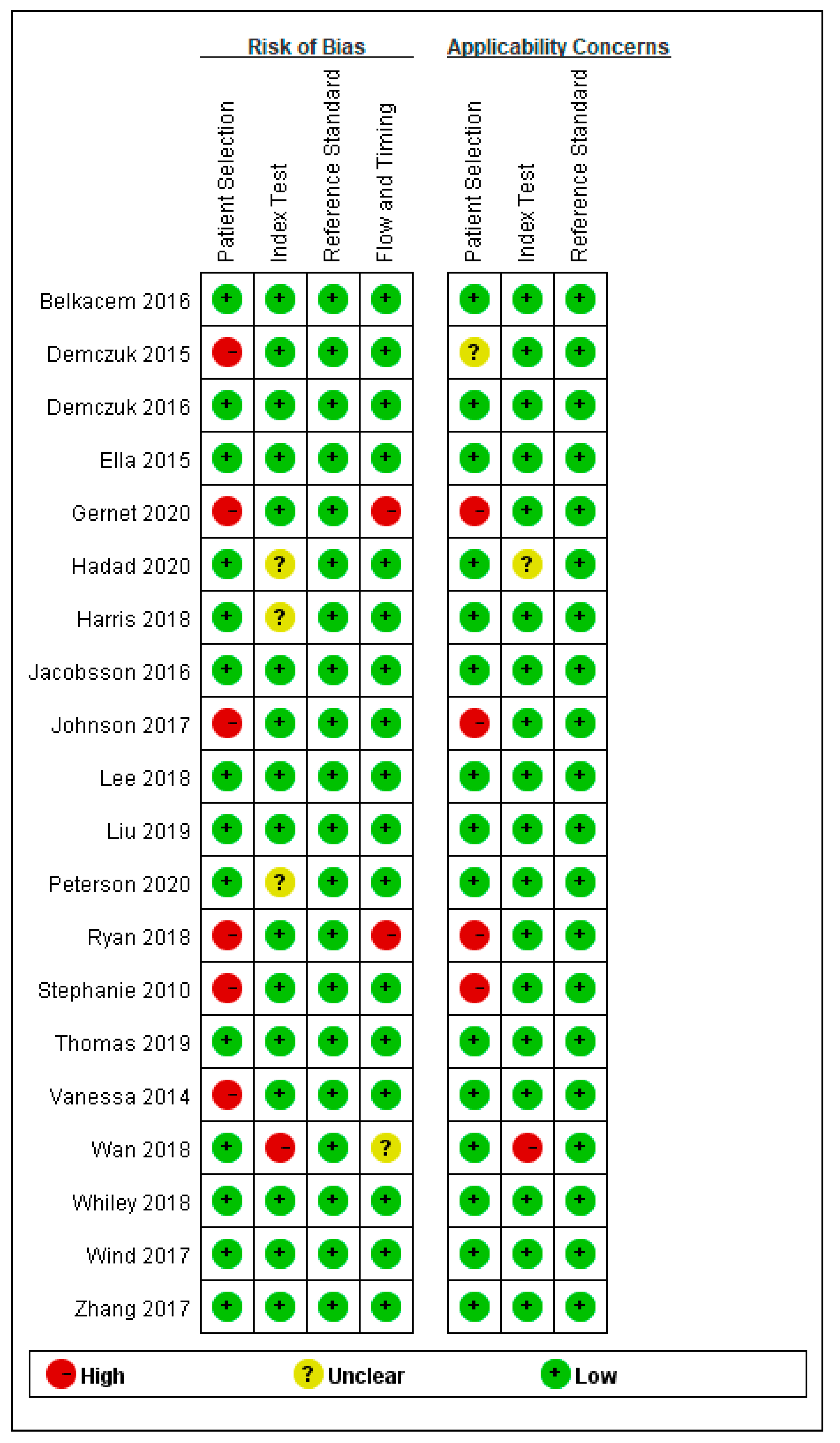
3.2. Quality Assessment
3.3. Meta-Analysis
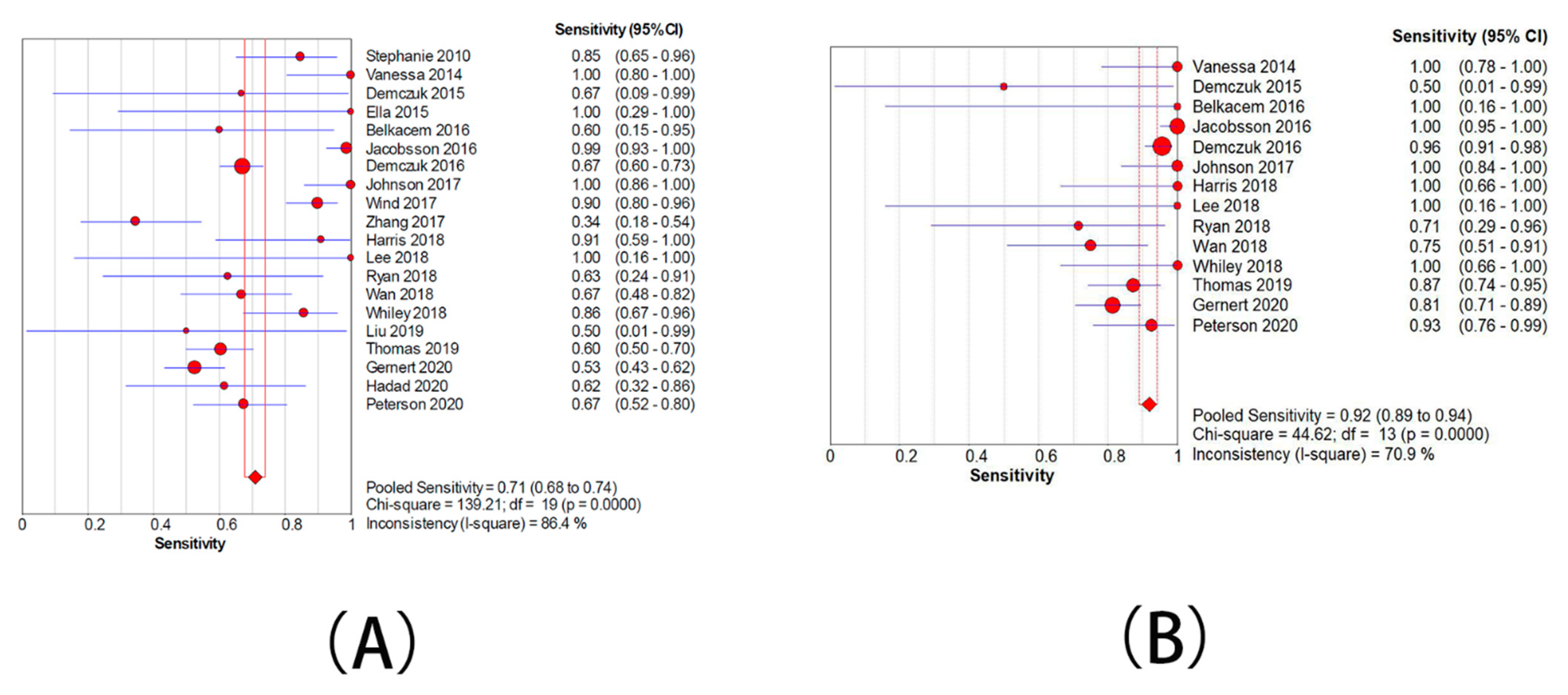
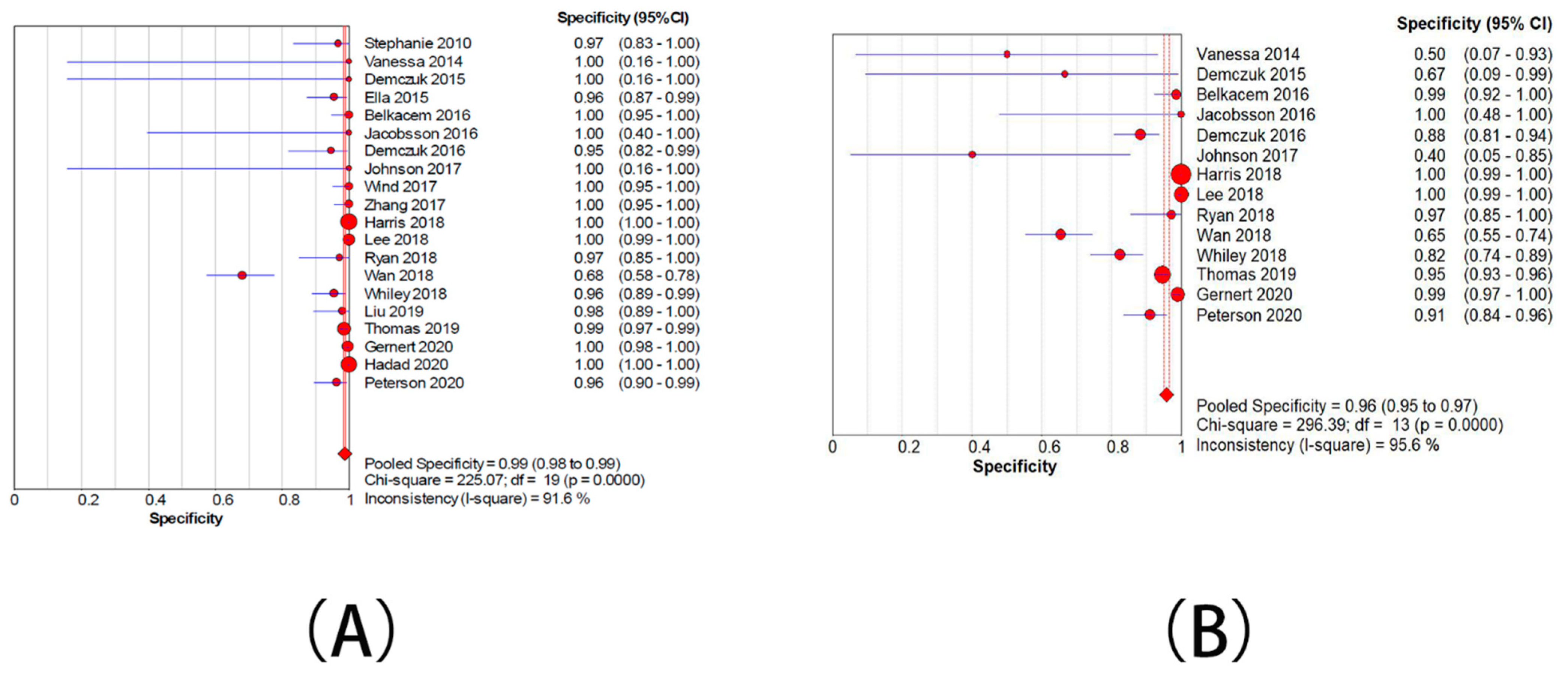
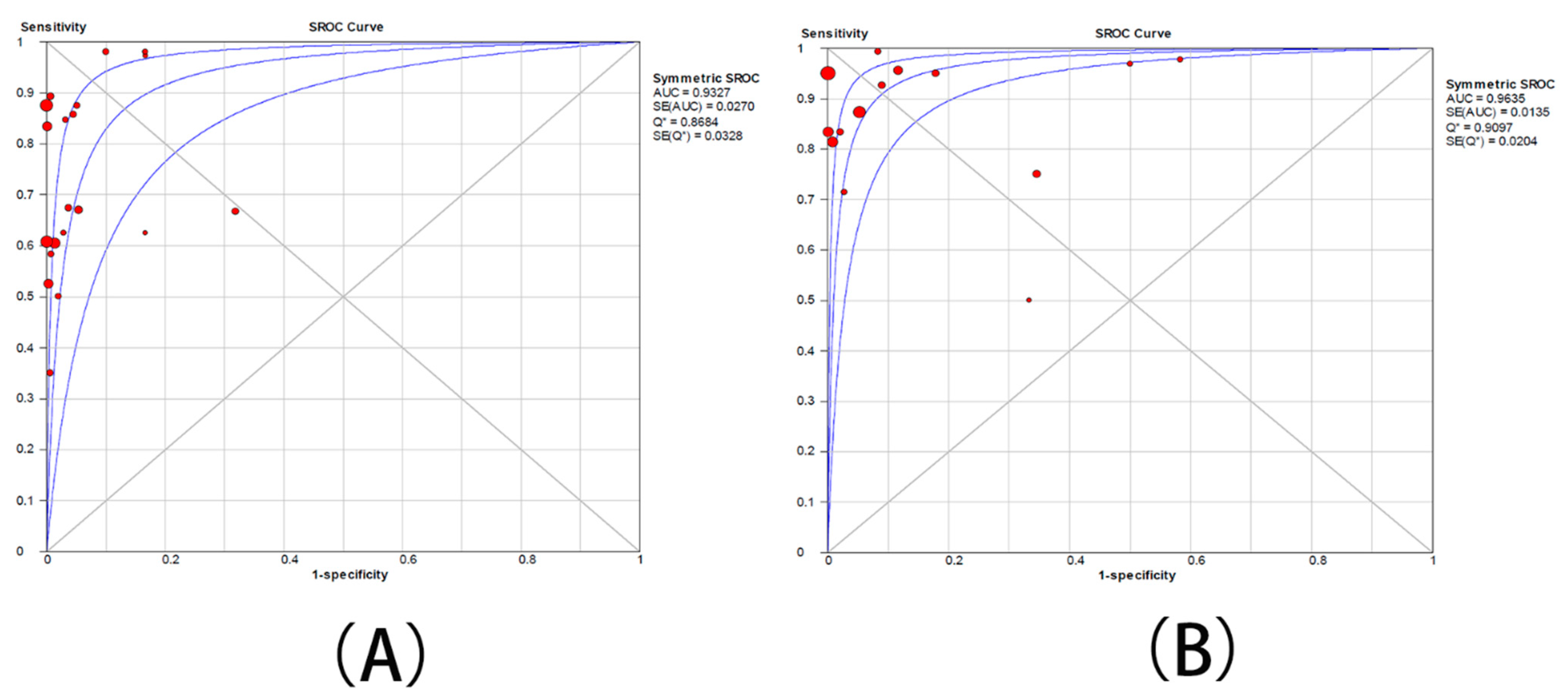
3.3.1. Meta-Analysis of the Group with Moderate Resistance Limited to 2–128 mg/L
3.3.2. Meta-Analysis of the Group with Moderate Resistance Limited to 4–128 mg/L
3.3.3. Analysis of the Causes of Heterogeneity in the Included Studies
Meta-Regression Analysis of the Group with Moderate Resistance Limited to 2–128 mg/L
Meta-Regression Analysis of the Group with Moderate Resistance Limited to 4–128 mg/L
3.4. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Funding
Data Availability Statement
Conflicts of Interest
References
- Quillin, S.J.; Seifert, H.S. Neisseria gonorrhoeae host adaptation and pathogenesis. Nat. Rev. Microbiol. 2018, 16, 226–240. [Google Scholar] [CrossRef]
- Wang, Q. Guidelines for diagnosis and treatment of syphilis, gonorrhea and genital Chlamydia trachomatis infection (2020). Chin. J. Dermatol. 2020, 53, 168–179. [Google Scholar]
- Unemo, M.; Seifert, H.S.; Hook, E.W., 3rd; Hawkes, S.; Ndowa, F.; Dillon, J.R. Gonorrhoea. Nat. Rev. Dis. Primers 2019, 5, 79. [Google Scholar] [CrossRef]
- Unemo, M.; Shafer, W.M. Antimicrobial resistance in Neisseria gonorrhoeae in the 21st century: Past, evolution, and future. Clin. Microbiol. Rev. 2014, 27, 587–613. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global Surveillance Network for Gonococcal Antimicrobial Susceptibility; World Health Organization: Geneva, Switzerland, 1990. [Google Scholar]
- Centers for Disease Control and Prevention. Update to CDC’s Sexually transmitted diseases treatment guidelines, 2010: Oral cephalosporins no longer a recommended treatment for gonococcal infections. MMWR. Morb. Mortal. Wkly. Rep. 2012, 61, 590–594. [Google Scholar]
- Bignell, C.; Fitzgerald, M. UK National guideline for the management of gonorrhoea in adults, 2011. Int. J. STD AIDS 2011, 22, 541–547. [Google Scholar] [CrossRef] [PubMed]
- Yin, Y.P.; Han, Y.; Dai, X.Q.; Zheng, H.P.; Chen, S.C.; Zhu, B.Y.; Yong, G.; Zhong, N.; Hu, L.H.; Cao, W.L.; et al. Susceptibility of Neisseria gonorrhoeae to azithromycin and ceftriaxone in China: A retrospective study of national surveillance data from 2013 to 2016. PLoS Med. 2018, 15, e1002499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liang, J.Y.; Cao, W.L.; Li, X.D.; Bi, C.; Yang, R.D.; Liang, Y.H.; Li, P.; Ye, X.D.; Chen, X.X.; Zhang, X.B. Azithromycin-resistant Neisseria gonorrhoeae isolates in Guangzhou, China (2009–2013): Coevolution with decreased susceptibilities to ceftriaxone and genetic characteristics. BMC Infect. Dis. 2016, 16, 152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qin, X.; Zhao, Y.; Chen, W.; Wu, X.; Tang, S.; Li, G.; Yuqi, Y.; Cao, W.; Liu, X.; Huang, J.; et al. Changing antimicrobial susceptibility and molecular characterisation of Neisseria gonorrhoeae isolates in Guangdong, China: In a background of rapidly rising epidemic. Int. J. Antimicrob. Agents 2019, 54, 757–765. [Google Scholar] [CrossRef]
- Vester, B.; Douthwaite, S. Macrolide resistance conferred by base substitutions in 23S rRNA. Antimicrob. Agents Chemother. 2001, 45, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [Green Version]
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Goodacre, S.; Sutton, A.J.; Sampson, F.C. Meta-analysis: The value of clinical assessment in the diagnosis of deep venous thrombosis. Ann. Intern. Med. 2005, 143, 129–139. [Google Scholar] [CrossRef] [Green Version]
- Chisholm, A.C.; Jayshree, D.; Ison, C.A. High-level azithromycin resistance occurs in Neisseria gonorrhoeae as a result of a single point mutation in the 23S rRNA genes. Antimicrob. Agents Chemother. 2010, 54, 3812–3816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allen, V.G.; Seah, C.; Martin, I.; Melanoa, R.G. Azithromycin resistance is coevolving with reduced susceptibility to cephalosporins in neisseria gonorrhoeae in ontario, Canada. Antimicrob. Agents Chemother. 2014, 58, 2528–2534. [Google Scholar] [CrossRef] [Green Version]
- Belkacem, A.; Jacquier, H.; Goubard, A.; Mougari, F.; La Ruche, G.; Patey, O.; Micaëlo, M.; Semaille, C.; Cambau, E.; Bercot, B. Molecular epidemiology and mechanisms of resistance of azithromycin-resistant Neisseria gonorrhoeae isolated in France during 2013–14. J. Antimicrob. Chemother. 2016, 71, 2471–2478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demczuk, W.; Lynch, T.; Martin, I.; Van Domselaar, G.; Graham, M.; Bharat, A.; Allen, V.; Hoang, L.; Lefebvre, B.; Tyrrell, G.; et al. Whole-genome phylogenomic heterogeneity of Neisseria gonorrhoeae isolates with decreased cephalosporin susceptibility collected in Canada between 1989 and 2013. J. Clin. Microbiol. 2015, 53, 191–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gernert, K.M.; Seby, S.; Schmerer, M.W.; Thomas, J.C., IV; Pham, C.D.; Cyr, S.S.; Schlanger, K.; Weinstock, H.; Shafer, W.M.; Raphael, B.H.; et al. Azithromycin susceptibility of Neisseria gonorrhoeae in the USA in 2017: A genomic analysis of surveillance data. Lancet Microbe 2020, 1, e154–e164. [Google Scholar] [CrossRef]
- Harris, S.R.; Cole, M.J.; Spiteri, G.; Sánchez-Busó, L.; Golparian, D.; Jacobsson, S.; Goater, R.; Abudahab, K.; Yeats, C.A.; Bercot, B.; et al. Public health surveillance of multidrug-resistant clones of Neisseria gonorrhoeae in Europe: A genomic survey. Lancet Infect. Dis. 2018, 18, 758–768. [Google Scholar] [CrossRef]
- Jacobsson, S.; Golparian, D.; Cole, M.; Spiteri, G.; Martin, I.; Bergheim, T.; Borrego, M.J.; Crowley, B.; Crucitti, T.; Van Dam, A.P.; et al. WGS analysis and molecular resistance mechanisms of azithromycin-resistant (MIC > 2 mg/L) Neisseria gonorrhoeae isolates in Europe from 2009 to 2014. J. Antimicrob. Chemother. 2016, 71, 3109–3116. [Google Scholar] [CrossRef] [Green Version]
- Johnson, S.R.; Grad, Y.; Abrams, A.J.; Pettus, K.; Trees, D.L. Use of whole-genome sequencing data to analyze 23S rRNA-mediated azithromycin resistance. Int. J. Antimicrob. Agents 2017, 49, 252–254. [Google Scholar] [CrossRef]
- Lee, R.S.; Seemann, T.; Heffernan, H.; Kwong, J.C.; da Silva, A.G.; Carter, G.P.; Woodhouse, R.; Dyet, K.H.; Bulach, D.M.; Stinear, T.P.; et al. Genomic epidemiology and antimicrobial resistance of Neisseria gonorrhoeae in New Zealand. J. Antimicrob. Chemother. 2018, 73, 353–364. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.H.; Wang, Y.H.; Liao, C.H.; Hsuehg, P.R. Emergence and spread of Neisseria gonorrhoeae strains with high-level resistance to azithromycin in Taiwan from 2001 to 2018. Antimicrob. Agents Chemother. 2019, 63, e00773-19. [Google Scholar] [CrossRef] [Green Version]
- Peterson, S.W.; Martin, I.; Demczuk, W.; Barairo, N.; Naidu, P.; Lefebvre, B.; Allen, V.; Hoang, L.; Hatchette, T.F.; Alexander, D.; et al. Multiplex real-time PCR assays for the prediction of cephalosporin, ciprofloxacin and azithromycin antimicrobial susceptibility of positive Neisseria gonorrhoeae nucleic acid amplification test samples. J. Antimicrob. Chemother. 2020, 75, 3485–3490. [Google Scholar] [CrossRef] [PubMed]
- Ronza, H.; Jayne, C.M.; Samantha, E.; Susanne, J.; Yeen, T.L.; Daniel, G.; Simon, E.; Michaela, D.; David, W.; Magnus, U. Evaluation of the SpeeDx ResistancePlus® GC and SpeeDx GC 23S 2611 (beta) molecular assays for prediction of antimicrobial resistance/susceptibility to ciprofloxacin and azithromycin in Neisseria gonorrhoeae. J. Antimicrob. Chemother. 2020, 76, 84–90. [Google Scholar]
- Ryan, L.; Golparian, D.; Fennelly, N.; Rose, L.; Walsh, P.; Lawlor, B.; Mac Aogain, M.; Unemo, M.; Crowley, B. Antimicrobial resistance and molecular epidemiology using whole-genome sequencing of Neisseria gonorrhoeae in Ireland, 2014–2016: Focus on extended-spectrum cephalosporins and azithromycin. Eur. J. Clin. Microbiol. Infect. Dis. 2018, 37, 1661–1672. [Google Scholar] [CrossRef] [PubMed]
- Thomas, J.C.; Seby, S.; Abrams, A.J.; Cartee, J.; Lucking, S.; Vidyaprakash, E.; Schmerer, M.; Pham, C.D.; Hong, J.; Torrone, E.; et al. Evidence of recent genomic evolution in gonococcal strains with decreased susceptibility to cephalosporins or azithromycin in the United States, 2014–2016. J. Infect. Dis. 2019, 220, 294–305. [Google Scholar] [CrossRef] [PubMed]
- Trembizki, E.; Buckley, C.; Donovan, B.; Chen, M.; Guy, R.; Kaldor, J.; Lahra, M.M.; Regan, D.G.; Smith, H.; Ward, J.; et al. Direct real-time PCR-based detection of Neisseria gonorrhoeae 23S rRNA mutations associated with azithromycin resistance. J. Antimicrob. Chemother. 2015, 70, 3244–3249. [Google Scholar] [PubMed] [Green Version]
- Walter, D.; Irene, M.; Shelley, P.; Amrita, B.; Gary, V.D.; Morag, G.; Brigitte, L.; Vanessa, A.; Linda, H.; Greg, T.; et al. Genomic epidemiology and molecular resistance mechanisms of azithromycin-resistant Neisseria gonorrhoeae in Canada from 1997 to 2014. J. Clin. Microbiol. 2016, 54, 1304–1313. [Google Scholar]
- Wan, C.; Li, Y.; Le, W.-J.; Liu, Y.-R.; Li, S.; Wang, B.-X.; Rice, P.A.; Su, X.-H. Increasing resistance to azithromycin in Neisseria gonorrhoeae in eastern Chinese cities: Resistance mechanisms and genetic diversity among isolates from Nanjing. Antimicrob. Agents Chemother. 2018, 62, e02499-17. [Google Scholar] [CrossRef] [Green Version]
- Whiley, D.M.; Kundu, R.L.; Jennison, A.V.; Buckle, C.; Limnios, A.; Hogan, T.; Enriquez, R.; El Nasser, J.; George, C.R.; Lahra, M.M. Azithromycin-resistant Neisseria gonorrhoeae spreading amongst men who have sex with men (MSM) and heterosexuals in New South Wales, Australia, 2017. J. Antimicrob. Chemother. 2018, 73, 1242–1246. [Google Scholar] [CrossRef]
- Wind, C.M.; Bruisten, S.M.; van der Loeff, M.F.S.; Dierdorp, M.; de Vries, H.J.C.; van Dam, A.P. A case-control study of molecular epidemiology in relation to azithromycin resistance in Neisseria gonorrhoeae isolates collected in Amsterdam, the Netherlands, between 2008 and 2015. Antimicrob. Agents Chemother. 2017, 61, e02374-16. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.; Wang, F.; Peng, Y.; Mo, J. Antibiotic resistant mechanism and epidemiological characteristics of azithromycin-resistant Neisseria gonorrhoeae strains in Shenzhen. Chin. J. Microbiol. Immunol. 2017, 37, 219–224. [Google Scholar] [CrossRef]
- Wang, F.; Liu, J.; Liu, H.; Huang, J.; Chen, S.; Chen, X.; Yin, Y. Evaluation of the accuracy of molecular assays targeting the mutation A2059G for detecting high-level azithromycin resistance in Neisseria gonorrhoeae: A systematic review and meta-analysis. Infect. Drug Resist. 2019, 12, 95–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yasuda, M.; Ito, S.; Hatazaki, K.; Deguchi, T. Remarkable increase of Neisseria gonorrhoeae with decreased susceptibility of azithromycin and increase in the failure of azithromycin therapy in male gonococcal urethritis in Sendai in 2015. J. Infect. Chemother. 2016, 22, 841–843. [Google Scholar] [CrossRef] [PubMed]
- Cole, M.J.; Tan, W.; Fifer, H.; Brittain, C.; Duley, L.; Hepburn, T.; Lawrence, T.; Montgomery, A.A.; Sprange, K.; Thandi, S.; et al. Gentamicin, azithromycin and ceftriaxone in the treatment of gonorrhoea: The relationship between antibiotic MIC and clinical outcome. J. Antimicrob. Chemother. 2020, 75, 449–457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Unemo, M.; Ross, J.; Serwin, A.B.; Gomberg, M.; Cusini, M.; Jensen, J.S. 2020 European guideline for the diagnosis and treatment of gonorrhoea in adults. Int. J. STD AIDS 2020. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Azithromycin Susceptibility | With Mutants at Position 2611 | Without Mutants at Position 2611 |
|---|---|---|
| ML-AzmR isolates | true positive | false negative |
| Non ML-AzmR isolates | false positive | true negative |
| Study Number | Year, First Author | Location | Isolate Collection Period | Technique | Diagnostic Test Results of Molecular Assays | |||
|---|---|---|---|---|---|---|---|---|
| TP | FP | FN | TN | |||||
| 1 | Stephanie 2010 | U.K. | 2001–2007 | PCR | 22 | 1 | 4 | 30 |
| 2 | Vanessa 2014 | Canada | 2010–2013 | PCR | 17 | 0 | 0 | 2 |
| 3 | Demczuk 2015 | Canada | 1989–2013 | WGS | 2 | 0 | 1 | 2 |
| 4 | Ella 2015 | Australia | 2012 | PCR | 3 | 3 | 0 | 64 |
| 5 | Belkacem 2016 | France | 2013–2014 | PCR | 3 | 0 | 2 | 67 |
| 6 | Jacobsson 2016 | Europe | 2009–2014 | WGS | 72 | 0 | 1 | 4 |
| 7 | Demczuk 2016 | Canada | 1997–2014 | WGS | 140 | 2 | 69 | 35 |
| 8 | Johnson 2017 | USA | 2009–2010 | WGS | 24 | 0 | 0 | 2 |
| 9 | Wind 2017 | The Netherlands | 2008–2015 | PCR | 62 | 0 | 7 | 73 |
| 10 | Zhang 2017 | Shenzhen, China | 2011–2015 | PCR | 10 | 0 | 19 | 79 |
| 11 | Harris 2018 | Europe | 2013 | WGS | 10 | 0 | 1 | 1043 |
| 12 | Lee 2018 | New Zealand | 2014–2015 | WGS | 2 | 0 | 0 | 396 |
| 13 | Ryan 2018 | Ireland | 2014–2016 | WGS | 5 | 1 | 3 | 34 |
| 14 | Wan 2018 | Nanjing, China | 2013–2014 | PCR | 22 | 29 | 11 | 62 |
| 15 | Whiley 2018 | Australia | 2017 | PCR | 24 | 4 | 4 | 85 |
| 16 | Liu 2019 | Taiwan | 2001–2018 | PCR | 1 | 1 | 1 | 49 |
| 17 | Thomas 2019 | USA | 2014–2016 | WGS | 58 | 8 | 38 | 545 |
| 18 | Gernert 2020 | USA | 2017 | WGS | 63 | 1 | 57 | 289 |
| 19 | Hadad 2020 | Europe | 2013 | WGS | 8 | 0 | 5 | 950 |
| 20 | Peterson 2020 | Canada | 2009–2019 | PCR | 31 | 3 | 15 | 78 |
| Study Number | Year, First Author | Location | Isolate Collection Period | Technique | Diagnostic Test Results of Molecular Assays | |||
|---|---|---|---|---|---|---|---|---|
| TP | FP | FN | TN | |||||
| 1 | Vanessa 2014 | Canada | 2010–2013 | PCR | 15 | 2 | 0 | 2 |
| 2 | Demczuk 2015 | Canada | 1989–2013 | WGS | 1 | 1 | 1 | 2 |
| 3 | Belkacem 2016 | France | 2013–2014 | PCR | 2 | 1 | 0 | 69 |
| 4 | Jacobsson 2016 | Europe | 2009–2014 | WGS | 72 | 0 | 0 | 5 |
| 5 | Demczuk 2016 | Canada | 1997–2014 | WGS | 129 | 13 | 6 | 98 |
| 6 | Johnson 2017 | USA | 2009–2010 | WGS | 21 | 3 | 0 | 2 |
| 7 | Harris 2018 | Europe | 2013 | WGS | 9 | 1 | 0 | 1044 |
| 8 | Lee 2018 | New Zealand | 2014–2015 | WGS | 2 | 0 | 0 | 396 |
| 9 | Ryan 2018 | Ireland | 2014–2016 | WGS | 5 | 1 | 2 | 35 |
| 10 | Wan 2018 | Nanjing, China | 2013–2014 | PCR | 15 | 36 | 5 | 68 |
| 11 | Whiley 2018 | Australia | 2017 | PCR | 9 | 19 | 0 | 89 |
| 12 | Thomas 2019 | USA | 2014–2016 | WGS | 41 | 32 | 6 | 570 |
| 13 | Gernert 2020 | USA | 2017 | WGS | 61 | 3 | 14 | 332 |
| 14 | Peterson 2020 | Canada | 2009–2019 | PCR | 25 | 9 | 2 | 91 |
| Variables | Coefficient | p-Value | RDOR | 95% CI |
|---|---|---|---|---|
| detection method | 0.967 | 0.3102 | 2.63 | (0.37; 18.83) |
| isolates sampling | 0.003 | 0.9984 | 1.00 | (0.06; 16.86) |
| location | 0.802 | 0.4384 | 2.23 | (0.26; 19.23) |
| sample size | −0.416 | 0.7281 | 0.66 | (0.05; 8.17) |
| Variables | Coefficient | p-Value | RDOR | 95% CI |
|---|---|---|---|---|
| detection method | 1.705 | 0.2457 | 5.50 | (0.24; 127.00) |
| isolates sampling | 1.565 | 0.2457 | 4.78 | (0.07; 266.26) |
| location | 0.375 | 0.8096 | 1.46 | (0.05; 46.95) |
| sample size | −0.089 | 0.9611 | 0.91 | (0.02; 53.97) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, Q.; Liu, J.; Chen, S.; Xu, W.; Han, Y.; Yin, Y. The Accuracy of Molecular Detection Targeting the Mutation C2611T for Detecting Moderate-Level Azithromycin Resistance in Neisseria gonorrhoeae: A Systematic Review and Meta-Analysis. Antibiotics 2021, 10, 1027. https://doi.org/10.3390/antibiotics10091027
Zhou Q, Liu J, Chen S, Xu W, Han Y, Yin Y. The Accuracy of Molecular Detection Targeting the Mutation C2611T for Detecting Moderate-Level Azithromycin Resistance in Neisseria gonorrhoeae: A Systematic Review and Meta-Analysis. Antibiotics. 2021; 10(9):1027. https://doi.org/10.3390/antibiotics10091027
Chicago/Turabian StyleZhou, Qian, Jingwei Liu, Shaochun Chen, Wenqi Xu, Yan Han, and Yueping Yin. 2021. "The Accuracy of Molecular Detection Targeting the Mutation C2611T for Detecting Moderate-Level Azithromycin Resistance in Neisseria gonorrhoeae: A Systematic Review and Meta-Analysis" Antibiotics 10, no. 9: 1027. https://doi.org/10.3390/antibiotics10091027