
Updating the Classification of Chronic Inflammatory Enteropathies in Dogs
by
 , , , and
, , , and
Noémie Dupouy-Manescau
1,
Tristan Méric
1,
Odile Sénécat
1,
Amandine Drut
1,2,
Suzy Valentin
3,
Rodolfo Oliveira Leal
4 and
Juan Hernandez
1,2,* 1
Oniris VetAgroBio Nantes, Department of Clinical Sciences, Nantes-Atlantic College of Veterinary Medicine and Food Sciences, 44300 Nantes, France
2
Microbiota Interaction with Human and Animal Team (MIHA), Micalis Institute, AgrosParisTech, Université Paris-Saclay, Institut National de Recherche pour l’Agriculture, l’Alimentation et l’Environnement, 78350 Jouy-en-Josas, France
3
Hopia, Bozon Veterinary Clinic, 78280 Guyancourt, France
4
Associate Laboratory for Animal and Veterinary Sciences, AL4AnimalS, CIISA—Centre for Interdisciplinary Research in Animal Health, Faculty of Veterinary Medicine, University of Lisbon, 1649-004 Lisbon, Portugal
*
Author to whom correspondence should be addressed.
Animals 2024, 14(5), 681; https://doi.org/10.3390/ani14050681
Submission received: 29 December 2023
/
Revised: 8 February 2024
/
Accepted: 20 February 2024
/
Published: 21 February 2024
(This article belongs to the Section Companion Animals)
Abstract
:Simple Summary
Chronic inflammatory enteropathies (CIEs) in dogs are currently classified according to clinical response to sequential treatment trials. The resulting recognized categories are food-responsive (FREs), antibiotic-responsive (AREs), immunosuppressant-responsive (IREs) and non-responsive enteropathies (NREs). Although this classification has benefited clinicians by providing a standardized approach to managing CIEs for almost a decade, the results of recent research challenge our understanding of the underlying pathophysiology and encourage a revision of these categories. The role of diet has been reinforced, and the gut microbiota has been acknowledged as an essential player in intestinal inflammation. Using antibiotics has been shown to result in deleterious, long-lasting effects; thus, approaches aimed at restoring a diverse and functional microbiota (prebiotics, probiotics, fecal microbiota transplantation, etc.) are required. We subsequently propose updating the classification of CIEs by replacing AREs with microbiota-related modulation-responsive enteropathies (MrMREs). The introduction of such a category can serve as a basis for further studies to assess the performance of options targeting the rebalance of the gut microbiota.
Abstract
Chronic inflammatory enteropathies (CIEs) in dogs are currently classified based on response to sequential treatment trials into food-responsive (FREs); antibiotic-responsive (AREs); immunosuppressant-responsive (IREs); and non-responsive enteropathies (NREs). Recent studies have reported that a proportion of NRE dogs ultimately respond to further dietary trials and are subsequently misclassified. The FRE subset among CIEs is therefore probably underestimated. Moreover, alterations in the gut microbiota composition and function (dysbiosis) have been shown to be involved in CIE pathogenesis in recent research on dogs. Metronidazole and other antibiotics that have been used for decades for dogs with AREs have been demonstrated to result in increased antimicrobial resistance and deleterious effects on the gut microbiota. As a consequence, the clinical approach to CIEs has evolved in recent years toward the gradual abandonment of the use of antibiotics and their replacement by other treatments with the aim of restoring a diverse and functional gut microbiota. We propose here to refine the classification of canine CIEs by replacing the AREs category with a microbiota-related modulation-responsive enteropathies (MrMREs) category.
1. Introduction
Canine chronic inflammatory enteropathies (CIEs) are a group of diseases resulting in chronic (i.e., a 3-week duration or longer) or recurrent gastrointestinal clinical signs, including diarrhea, vomiting, nausea, borborygmus, flatulence, eructation, abdominal pain, weight loss or a combination of these signs. The diagnosis is made after the exclusion of extra-digestive disorders causing gastrointestinal clinical signs, intestinal parasitosis, and digestive neoplastic and infectious disorders [1].
The origin of the inflammation remains debated, but the current prevailing hypothesis is that the immune system excessively responds to environmental triggers (including to food and microbiota) in genetically predisposed individuals. Canine chronic inflammatory enteropathies are multifactorial diseases featuring a chronic immune response [2], the disruption of intestinal permeability [3], and the altered composition and function of the gut microbiota, referred to as dysbiosis [4]. Canine chronic inflammatory enteropathies are thought to arise in genetically prone individuals under the influence of epigenetic and environmental factors that alter immunotolerance and trigger the excessive activation of the innate and adaptive response of the host immunity. The microbiota–gut–brain axis is known for its bidirectional interactions between the central nervous system and the digestive tract and is gaining interest in regards to the onset of inflammatory bowel diseases [5].
CIEs are currently classified according to clinical response to treatment as food-responsive enteropathies (FREs), antibiotic-responsive enteropathies (AREs), immunosuppressant-responsive enteropathies (IREs) and non-responsive or refractory enteropathies (NREs). Inflammatory bowel diseases (IBDs) encompass both IREs and NREs with demonstrated mucosal inflammation. An additional group of CIEs named protein-losing enteropathies (PLEs) refers to all chronic enteropathies that result in hypoalbuminemia [6,7].
This classification has benefited clinicians by providing a standardized and consistent approach. However, our knowledge has continued to evolve, and significant limitations now make this system less suitable. Our objective was to propose an updated classification that considers recent advances in canine gastroenterology. With this review, we aim to briefly summarize the rationale of the current classification, discuss its limitations as underlined by recent research and propose a refined classification.
2. Current Classification of CIEs
The true prevalence of CIEs in dogs is unknown. In referral hospitals, CIEs account for 1–2% of cases, and these percentages are likely to be underestimated because about 10 to 20% of consultations undertaken in primary facilities relate to gastrointestinal clinical signs [1,6,8].
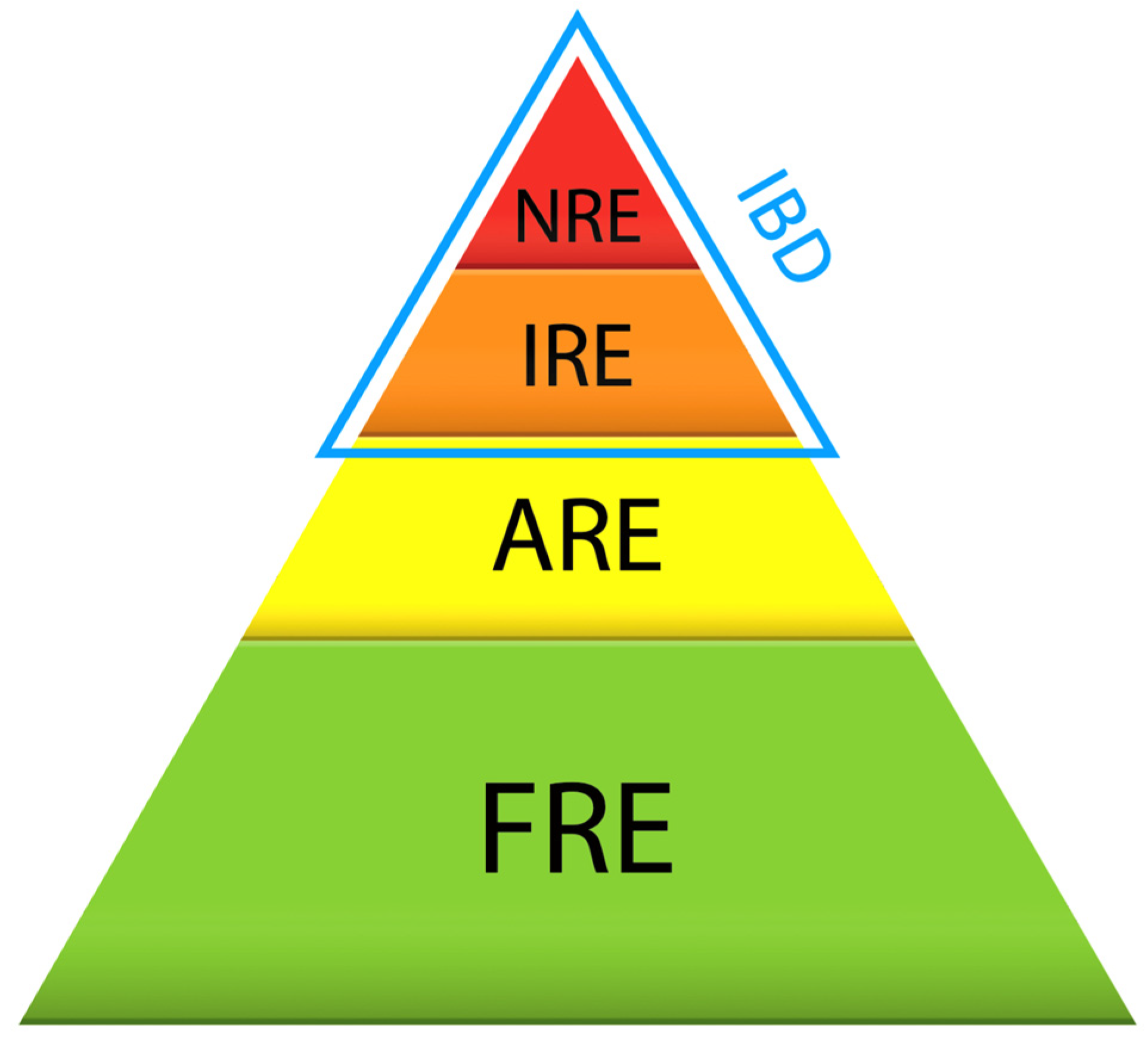
In dogs with chronic gastrointestinal signs, diagnoses of CIEs are considered after the exclusion of intestinal parasitism and extra-digestive disorders. In the current classification, once a CIE is suspected, several dietary trials are performed, usually including a highly digestible diet, a hydrolyzed protein diet, a fiber-rich diet, and/or a home-cooked novel protein diet with limited ingredients [9,10]. If clinical signs resolve with a dietary trial, the diagnosis falls in the FRE category. If clinical signs fail to improve, antibiotics have historically been advocated for (mainly metronidazole or tylosin). If the clinical response to the antibiotic trial is adequate, it is classified as an ARE. In the absence of a response to antibiotics, an ultrasound examination is usually pursued to exclude any focal disease of the gastrointestinal tract. Then, a histological examination of gastrointestinal biopsies is required to confirm mucosal inflammation and rule out diffuse neoplastic disorders and atypical infections. The dogs are then given an immunosuppressant, and the enteropathy is assigned to the IBD group (IRE or NRE, depending on the observed response). A graphical representation of the currently used categories of CIEs is provided in Figure 1 [1].
To date, no pathognomonic clinicals signs or clear scoring values have been determined to discriminate CIE categories.
Food-responsive enteropathies account for the majority of CIEs in dogs, ranging from 50 to 65% of cases [1,6,11,12]. Dogs with FREs seem to be younger than dogs with IREs (FRE median: 3 years, range: 0–12; IRE median: 6 years, range: 1–13 years, with p ≤ 0.001 in a cohort of 203 dogs diagnosed with CIEs [12]) and to exhibit more clinical signs consistent with large bowel disease. They have a lower canine chronic enteropathy clinical activity index (CCECAI) score in comparison with that of dogs suffering from AREs or IBD (median FRE: 6, range: 2–12; median ARE: 8, range: 0–14; median IRE: 9, range: 5–14, p ≤ 0.001 in a cohort of 203 dogs diagnosed with CIEs) [9,12,13,14]. However, no useful cut-off values for age or CCECAI scores and no specific clinical signs have been identified to help predict treatment response on an individual basis. Gluten-sensitive enteropathy in Irish setters and paroxysmal gluten-sensitive dyskesia in Border terriers (50% of affected dogs express gastrointestinal signs) are included in the FRE category [15,16].
Dogs with AREs enter clinical remission following metronidazole, tetracycline or tylosin administration. AREs account for 15 to 35% of CIEs [1,6,12,17]. Hypothesized underlying mechanisms include a decrease in the amount of deleterious bacteria within the gut microbiota and anecdotally direct immunomodulatory properties [18]. In particular, metronidazole and tylosin have recognized anti-inflammatory effects through modulating the synthesis of several mediators and cytokines [19,20]. Affected animals seem to be young large-breed dogs, with an over-representation of German shepherds [12,21]. However, age and dog breeds largely overlap among subtypes of CIEs. Relapses are frequent (diarrhea relapses occurred in 12 of 14 dogs within 30 days after tylosin discontinuation in a prospective study) [6,22].
Immunosuppressant-responsive enteropathies respond to glucocorticoids (prednisolone, budesonide), other immunosuppressants (cyclosporine, azathioprine, chlorambucil) or a combination of these treatments. IREs account for 10 to 25% of CIEs [6].
Five to forty-five percent of dogs with CIEs remain non-responsive (NREs) [6]. These CIEs carry a worse long-term prognosis with a high rate of euthanasia [9,23].
Protein-losing enteropathies (PLEs) encompass all enteropathies that potentiate protein leakage and malabsorption, resulting in hypoalbuminemia. Inflammatory PLEs are considered to be severe versions of CIEs. The usual diagnostic workup and therapeutic approach for CIEs are often modified in the case of hypoalbuminemia. Gut biopsies are usually taken immediately for histological examination and, instead of using a sequential treatment approach, immunosuppressants (mostly glucocorticoids and chlorambucil) are often started early, in combination with a highly digestible, ultra-low-fat diet, with or without antibiotics [1,24,25,26,27]. In addition, PLEs are frequently complicated with a hypercoagulable state and consequently require thromboprophylactic treatment [28]. Although the mechanism has not been clarified yet, the decrease in plasma antithrombin activity, the underlying disease as well as drug treatments (glucocorticoids) are conceivably contributors, with pulmonary thromboembolism being one of the most serious complications in these cases [29,30].
3. Limitations and Reconsideration of the Current Classification
3.1. Targeting the Microbiome toward Eubiosis
The role of the intestinal microbiota in health is now well established in humans and animals. Alterations in the gut microbiota composition and function (dysbiosis) are associated with canine CIEs. Essentially, there are overall decreased levels of richness and diversity. Pseudomonadota and Actinomycetota phyla are overrepresented, and Bacteroidota, Bacillota and Fusobacteria phyla are less abundant in most affected dogs. Among the Pseudomonadota phylum, the abundance of the Enterobacteriaceae family is increased. The abundances of the Bacteroidota phylum, Paraprevotellaceae family and Porphyromonas genus are increased. Finally, among the Bacillota phylum, declines in the Faecalibacterium (a single species of the genus F. prausnitzii), Blautia and Turicibacter genera and Peptacetobacter hiranonis have been reported [18,31,32,33,34,35]. The dysbiosis index (DI) was developed based on a mathematical algorithm using quantitative PCR testing of eight bacterial groups (i.e., Blautia, Peptacetobacter hiranonis, Escherichia coli, Faecalibacterium, Fusobacterium, Streptococcus, Turicibacter and total bacteria) that are commonly altered in dogs with CIEs [36]. A DI with a threshold value of 0 distinguishes dogs with chronic inflammatory enteropathy from healthy dogs with 74% sensitivity and 95% specificity. This tool makes it possible to detect dysbiosis and to monitor the return to eubiosis after appropriate treatment.
Gut dysbiosis entails the disruption of microbial-related metabolic pathways, such as short-chain fatty acids (SCFAs) and indole synthesis, bile acid (BA) biotransformation and proteolytic activities [31,37,38,39,40,41,42,43,44,45,46]. As an example, SCFAs (i.e., acetate, propionate and butyrate) are the main end products of the intestinal bacterial fermentation of non-digestible food components, such as dietary fiber. SCFAs are an essential energy source for colonocytes; they enhance epithelial barrier function by strengthening tight junctions and regulate T-lymphocyte function [47,48,49,50]. In another well-documented example, the deconjugation and dehydroxylation of primary BAs into secondary BAs are executed using enzymes carried by bacteria of the intestinal microbiota (Bacteroides, Clostridium, Bifidobacterium, Lactobacillus…) [51]. A decreased excretion of secondary BAs was detected in dogs with CIEs and presumably attributed to the decreased abundance of Fusobacterium and Peptacetobacter hiranonis [52]. Bile acids have been identified as antibacterial agents regulating gut microbial populations and as signaling ligands for multiple receptors (hormone farnesoid X receptor, Takeda G protein receptor 5…), influencing both host metabolism and immune response [51].
These data provide some evidence that intestinal dysbiosis promotes intestinal inflammation and thus provide the rationale to promote therapeutic strategies aimed at restoring eubiosis [40].
3.2. Towards Restricted Use of Antibiotics
For decades, metronidazole and other antibiotics have been successfully used in dogs with chronic gastrointestinal signs. However, evidence of deleterious effects on the gut microbiota is accumulating. Persistent changes in microbiota richness and composition are reported after metronidazole and tylosin treatments and may explain the frequency of clinical relapse after treatment interruption [4,12,22,53,54,55,56,57,58,59]. The design and conclusions of published papers studying the microbial consequences of using metronidazole or tylosin are summarized in Table 1.
In addition, there is a growing concern about antimicrobial resistance, which is one of the most serious and imminent One Health-related problems worldwide. A report showed that 54% of isolates of Clostridium perfringens from pet dogs with acute diarrhea had decreased susceptibility to metronidazole, including dogs not having had any previous treatment with antibiotics, suggesting that resistant strains might be transmitted from one individual to another [65]. As a consequence, dogs are considered a possible reservoir for antibiotic-resistant bacterial strains [66,67,68,69,70].
As a result, the clinical approach to CIEs has evolved in recent years toward the gradual abandonment of the use of antibiotics and their replacement by approaches aiming at restoring a functional gut microbiota [71].
3.3. Restoring Gut Microbiota
Several strategies aiming at restoring the functionality of the dysbiotic gut microbiota have been explored in recent years and include dietary changes; the use of prebiotics, probiotics, symbiotics, postbiotics; and fecal microbiota transplantation.
- Prebiotics are non-viable substrates that serve as nutrients for beneficial microorganisms. They impact the composition of bacterial communities as well as microbial metabolic activities, including the synthesis of SCFAs [72]. Studies in rodent models and in humans suffering from IBD have demonstrated the benefits of prebiotic use which reduce histological lesions, proinflammatory cytokines and oxidative stress [73,74,75,76,77,78,79]. Although the overall level of evidence of prebiotics’ efficacy in humans with IBD is low, the results of two randomized clinical trials (RCTs) are of interest [80,81]. They evaluated germinated barley foodstuff (GBF), a dietary fiber classified as a prebiotic, which was demonstrated to lower clinical disease activity scores. In dogs with CIEs, two RCTs have been conducted to assess the potential benefits of prebiotics [82,83]. In the first RCT, β-glucans and mannan oligosaccharides (MOSs) did not provide any significant clinical benefits in dogs suffering from a CIE; however, the study was underpowered (with nine dogs in the supplemented group and ten dogs in the placebo group) [82]. In the second RCT, dogs with chronic diarrhea responding to a hydrolyzed diet (FRE) were randomly allocated either to a group supplemented with β-glucans, MOSs, chondroitin sulphate and glycosaminoglycans or to a placebo group. No significant differences in their relapse rates after returning to their initial diet were shown between the groups, but the study was also underpowered (with eight dogs in the test group vs. five in the control group) [83]. In a more recent RCT, a symbiotic-IgY supplement (probiotics: Lactobacillus acidophilus‚ Lactobacillus casei‚ Enterococcus faecium and Bacillus subtilis; prebiotics: beta-glucans, MOSs and D-mannose; immunoglobulin IgY derived from chicken egg yolk) led to decreased levels of fecal calprotectin and serum C-reactive protein; increased numbers of colonic mucosal Clostridia (class of Bacillota phylum) and Bacteroides (genus of Bacteroidota phylum); and decreased numbers of Enterobacteriaceae in CIE dogs. No clinical benefits were demonstrated in that study [84]. Therefore, evidence of any benefit does not exist in dogs and remains low in humans; nevertheless, no adverse effect has been reported in either species. Fructooligosaccharide (FOS) supplementation may be a more promising strategy and worth exploring [85,86].
- Probiotics are defined by the World Health Organization as “live microorganisms which when administered in adequate amounts confer a health benefit on the host” [87]. In dogs suffering from CIEs, RCTs investigating the benefit of probiotics remain scarce [84,88]. The multi-strain probiotic VSL#3 was compared to prednisolone/metronidazole in dogs suffering from IBD [89]. Significant improvement in CCECAI scores was found in both groups on day 90 when compared to those on day 0. In another controlled trial, dogs with IBD were administered conventional treatment (hydrolyzed protein diet, prednisolone and antibiotic) alone or in combination with Saccharomyces boulardii (109/kg BID). The use of the yeast was associated with a lower CCECAI score on days 45 and 60 [90]. Although the evidence remains sparse, these data support the use of probiotics in dogs with CIEs. Based on individual experience and on the VSL#3 study, multi-strain probiotics should be considered.
- Symbiotics result from the combination of pre- and probiotics in the same product and have recently gained popularity for use in dogs and cats. Although studies about their efficacy are scarce, they seem to be promising options in terms of compliance [84].
- Postbiotics refer to dead microorganisms or microbial metabolic products beneficial to gut health [91]. Although postbiotics do not include live microorganisms, they may have beneficial properties based on their pleiotropic effects, including anti-inflammatory, antioxidant, immunomodulatory and anticancer properties [92,93]. After an exhaustive review of the literature, we found no study investigating the use of a product with only postbiotic properties in dogs with CIEs.
- Fecal microbiota transplantation (FMT) is now recognized as the standard of care in people suffering from recurrent Clostridioides difficile infection [94]. Available data suggest beneficial effects of FMT in patients with mild to moderate ulcerative colitis (UC), but there is insufficient evidence to recommend this therapeutic modality in routine clinical practice, and its use is currently limited to a research setting [95]. In dogs, only one RCT, one prospective study and six case reports/series on the use of FMT in dogs with CIEs/IBD have been published to date [96,97,98,99,100,101,102,103]. In the RCT, dogs with IBD were given either a FMT or a sterile saline enema as a placebo in addition to prednisolone and a hydrolyzed diet [102]. CCECAI scores significantly improved in both groups, but there were no significant differences between groups. The study was, however, underpowered (with seven dogs in the FMT group and six dogs in the control group) and might benefit from being repeated with larger cohorts of dogs. No adverse effects were observed in the dogs that received FMTs. The largest study is a retrospective case series on 41 dogs with CIEs not responding to diet, probiotics or immunosuppression [101]. The included dogs received one to five FMTs with fresh frozen feces via rectal enemas. In 31/41 dogs (76%), FMT was associated with clinical improvement. In 20/41 dogs, the dose of corticosteroids could be decreased and the antibiotics treatment was interrupted. The canine inflammatory bowel disease activity index (CIBDAI) significantly decreased. The study, however, did not include a control group to better evaluate the role played by FMT in the observed improvement [101]. As in humans, available data might support the use of FMT in dogs with CIEs, although evidence remains limited and it requires further assessment in a research setting.
- Interestingly, a recent publication reports clinical remission in two dogs suffering from NREs using cholestyramine, a bile acid sequestrant. The beneficial effects are suspected to be due to the correction of excess primary bile acids resulting from bile salt dysmetabolism associated with intestinal dysbiosis (a reduction in bacteria carrying the bile salt dehydrogenase) or due to the reduction in apical sodium-dependent bile acid transporter (ASBT) receptor expression at the brush border of the ileum in dogs with CIEs [104].
Table 2 lists relevant studies on strategies for modulating the gut microbiota in dogs with CIEs.
3.4. Reaffirming the Importance of Diet
Dietary changes remain the simplest way to modulate the intestinal microbiota. In addition to fiber-enriched foods that act as prebiotics, foods with hydrolyzed proteins, initially designed to reduce immunogenicity, have also shown favorable effects on the composition of the gut microbiota and on the biotransformation of bile salts [40]. It is therefore hypothesized that the clinical improvement observed with hydrolyzed diets is not exclusively linked to their immune effect but also to their beneficial effects on the gut microbiota.
Several case series reinforce the role of dietary changes by showing that cases initially classified as NREs could be ultimately reclassified as FREs after an additional dietary modification. A prospective study reported that clinical remission was achieved in eight out of ten dogs with steroid-resistant inflammatory PLEs using an additional dietary trial as a sole treatment change [105]. Another retrospective multicentric study, conducted on 142 dogs suffering from CIEs, initially classified 18% of cases as NREs. However, 88% of these “NREs” were then challenged by a novel commercial or home-cooked diet, and 68% of them responded [106]. It then appears that, although acknowledged as the first step of the current treatment-based approach, dietary benefit is not fully investigated in some dogs before moving toward other therapies. This might have resulted from discouragement from owners due to repeated non-responding trials. The recent evidence about “food-responding NREs” encourages owners to pursue at least one diet of each of the following categories for 2 weeks: a commercial highly digestible diet, commercial novel animal protein or hydrolyzed diet, home-cooked limited-ingredient diet and home-cooked novel protein diet. Also, evidence suggests that clinicians should retry dietary trials in the case of CIEs not responding properly to immunosuppression.
In addition, two recent publications have suggested that at least some inflammatory PLEs respond to diet only. In a case series of eleven Yorkshire terriers suffering from confirmed (n = 4) or presumed (n = 7) inflammatory PLEs that were all treated with a diet change without an immunosuppressant, clinical and biological improvements were observed in eight dogs [25]. In another case series of 27 dogs with confirmed inflammatory PLEs that were treated with an ultra-low-fat diet alone, 23 dogs improved (complete response in 12/27 dogs and partial response in 11/27 dogs) [107]. Interestingly, a CCECAI cut-off of eight showed a sensitivity of 83% and a specificity of 89% to discriminate between food-responders and non-food-responders. An ultra-low-fat diet might therefore be useful as a first-line treatment in many dogs suffering from inflammatory PLEs of low to moderate clinical severity. Based on the response to treatment, PLEs may be subcategorized as either food-responsive PLEs (FR-PLE) or non-food-responsive-PLEs requiring additional immunosuppressant treatment and then subclassified as immunosuppressant-responsive PLEs (IR-PLE) or non-responsive PLEs (NR-PLE).
4. Proposition of a Refined Classification of CIEs in Dogs
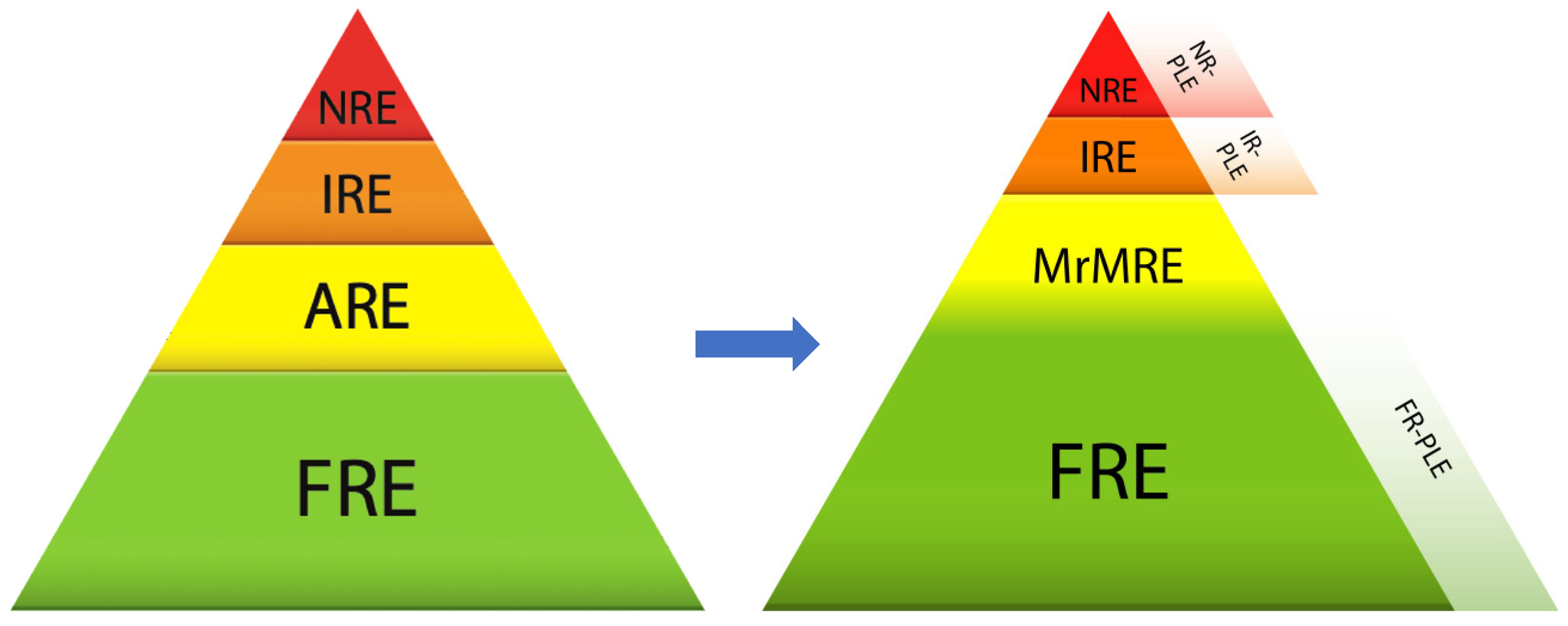
A proposal for an updated classification of canine CIEs is depicted in Figure 2.
4.1. Strengthening the Positioning of FRE
Several arguments lead to the resizing of the category of FRE and the consideration that its proportion is certainly underestimated:
- Intestinal dysbiosis has emerged as an important contributing factor in intestinal inflammation in humans and animals. With diet being the most effective means of modulating the intestinal microbiota, it is likely that part of the beneficial effects observed clinically are due to the rebalancing of the gut microbiota.
- Finally, a proportion of PLEs respond to dietary changes and therefore fall into the FRE category and may be subcategorized as FR-PLE. In practice, it is always difficult to limit treatment to dietary changes in a potentially unstable animal. The CCECAI score could be a valuable tool to distinguish cases that could benefit from dietary changes alone (CCECAI < 8) from those also requiring the administration of an immunosuppressive agent (CCECAI > 8) [107].
4.2. Replacement of AREs by MrMREs
The use of antibiotics in the treatment of CIEs has been gradually replaced by other approaches to intestinal dysbiosis treatment. The term idiopathic intestinal dysbiosis has been suggested by others but does not reflect the extent of the existing treatment options [108]. We propose the replacement of AREs by a category that encompasses all methods of modulation of the intestinal microbiota (microbiota-related modulation-responsive enteropathy—MrMRE). This category would include enteropathies responding to prebiotics, probiotics, postbiotics, symbiotics, fecal microbiota transplantation, bile acid sequestrants and certain dietary changes. In this concept, FRE and MrMRE partially overlap because changing diet might result in clinical improvement attributable to the modulation of the microbiota or another immune or non-immune mechanism. The MrMRE category has the advantage of being adaptable over time because it is reasonable to assume that new modalities will appear in the years to come.
There is no reliable diagnostic criterion for MrMRE category. The clinical relevance of using the dysbiosis index to predict response to microbiota modulation strategies has not yet been demonstrated. This tool remains of interest to monitor animals suffering from intestinal dysbiosis. The association of hypocobalaminemia, hyperfolatemia and normal serum trypsin-like immunoreactivity, although very insensitive, should raise our suspicion of gut dysbiosis (increased consumption of vitamin B12 and increased folate production by the deviated microbiota) [109]. Hypocobalaminemia remains an unspecific observation since it can occur in exocrine pancreatic insufficiency, ileal malabsorption or Imerslund–Gräsbeck syndrome [109].
4.3. Reduction in the Place of IRE and NRE
Due to the growing proportion occupied by FREs and MrMREs, IREs and NREs now appear to constitute a minority of CIEs. New epidemiological studies are needed to determine their real proportions. Also, new treatments (including bile salt sequestrant and specific pre-/pro-/postbiotics aimed at restoring a functional microbiota) that should emerge as beneficial options in subsets of diseased individuals might further lead to a reduction in the proportion of dogs suitable for immunosuppression or dogs that do not respond to any treatment.
The diagnosis of IRE and NRE remains complex because it is the culmination of a complete process of exclusion of all other causes including FRE and MrMRE. A study showed that a serum CRP concentration of 9.1 mg/L or greater distinguished dogs with IRE from dogs with FRE or ARE with a sensitivity of 72% and a specificity of 100% [110]. The use of CRP testing to identify IRE dogs may be clinically relevant, but further studies performed with the current classification on large cohorts are required to confirm this result.
5. Conclusions
In conclusion, we have proposed a refined classification of canine CIEs that takes into account recent advances in our understanding of these diseases. The most relevant new insights are that (i) dietary changes are thought to be more important; (ii) the decreasing use of antibiotics leaves room for several strategies for modulating the intestinal microbiota; and (iii) cases requiring the use of immunosuppressive treatment seem to be less frequent than currently assumed.
Microbiota-related modulation-responsive enteropathies (MrMREs) might encompass an important part of CIEs by focusing on addressing a key pathogenic element. However, the best way to rebalance the gut microbiota remains to be clarified. Future research on such options should aim at testing their ability to restore a functional microbiota.
Author Contributions
Conceptualization, N.D.-M., T.M. and J.H.; methodology, N.D.-M., T.M. and J.H.; writing—original draft preparation, N.D.-M., T.M. and J.H.; writing—review and editing, N.D.-M., T.M., O.S., A.D., S.V., R.O.L. and J.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
T.M. and J.H. have research funding by Royal Canin®. ROL has also benefited from research funding by Royal Canin®, Hill’s® and Purina®. All these manufacturers market hydrolyzed diets for dogs.
References
- Dandrieux, J.R.S. Inflammatory Bowel Disease versus Chronic Enteropathy in Dogs: Are They One and the Same? J. Small Anim. Pract. 2016, 57, 589–599. [Google Scholar] [CrossRef]
- Hernandez, J.; Rouillé, E.; Chocteau, F.; Allard, M.; Haurogné, K.; Lezin, F.; Hervé, J.M.; Bach, J.-M.; Abadie, J.; Lieubeau, B. Nonhypoalbuminemic Inflammatory Bowel Disease in Dogs as Disease Model. Inflamm. Bowel Dis. 2021, 27, 1975–1985. [Google Scholar] [CrossRef]
- Kobayashi, S.; Ohno, K.; Uetsuka, K.; Nakashima, K.; Setoguchi, A.; Fujino, Y.; Tsujimoto, H. Measurement of Intestinal Mucosal Permeability in Dogs with Lymphocytic-Plasmacytic Enteritis. J. Vet. Med. Sci. 2007, 69, 745–749. [Google Scholar] [CrossRef]
- Pilla, R.; Suchodolski, J.S. The Role of the Canine Gut Microbiome and Metabolome in Health and Gastrointestinal Disease. Front. Vet. Sci. 2020, 6, 498. [Google Scholar] [CrossRef] [PubMed]
- Günther, C.; Rothhammer, V.; Karow, M.; Neurath, M.; Winner, B. The Gut-Brain Axis in Inflammatory Bowel Disease—Current and Future Perspectives. Int. J. Mol. Sci. 2021, 22, 8870. [Google Scholar] [CrossRef]
- Dandrieux, J.R.S.; Mansfield, C.S. Chronic Enteropathy In Canines: Prevalence, Impact And Management Strategies. Vet. Med. Res. Rep. 2019, 10, 203–214. [Google Scholar] [CrossRef] [PubMed]
- Heilmann, R.M.; Steiner, J.M. Clinical Utility of Currently Available Biomarkers in Inflammatory Enteropathies of Dogs. J. Vet. Intern. Med. 2018, 32, 1495–1508. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, D.G.; James, H.; Brodbelt, D.C.; Church, D.B.; Pegram, C. Prevalence of Commonly Diagnosed Disorders in UK Dogs under Primary Veterinary Care: Results and Applications. BMC Vet. Res. 2021, 17, 69. [Google Scholar] [CrossRef]
- Allenspach, K.; Wieland, B.; Gröne, A.; Gaschen, F.P. Chronic Enteropathies in Dogs: Evaluation of Risk Factors for Negative Outcome. J. Vet. Intern. Med. 2007, 21, 700–708. [Google Scholar] [CrossRef]
- Mandigers, P.J.J.; Biourge, V.; van Den Ingh, T.S.G.A.M.; Ankringa, N.; German, A.J. A Randomized, Open-Label, Positively-Controlled Field Trial of a Hydrolyzed Protein Diet in Dogs with Chronic Small Bowel Enteropathy. J. Vet. Intern. Med. 2010, 24, 1350–1357. [Google Scholar] [CrossRef]
- Kawano, K.; Shimakura, H.; Nagata, N.; Masashi, Y.; Suto, A.; Suto, Y.; Uto, S.; Ueno, H.; Hasegawa, T.; Ushigusa, T.; et al. Prevalence of Food-Responsive Enteropathy among Dogs with Chronic Enteropathy in Japan. J. Vet. Med. Sci. 2016, 78, 1377–1380. [Google Scholar] [CrossRef]
- Allenspach, K.; Culverwell, C.; Chan, D. Long-term Outcome in Dogs with Chronic Enteropathies: 203 Cases. Vet. Rec. 2016, 178, 368. [Google Scholar] [CrossRef]
- Münster, M.; Hörauf, A.; Bilzer, T. Assessment of disease severity and outcome of dietary, antibiotic, and immunosuppressive interventions by use of the canine IBD activity index in 21 dogs with chronic inflammatory bowel disease. Berl. Munch. Tierarztl. Wochenschr. 2006, 119, 493–505. [Google Scholar] [PubMed]
- Allenspach, K.; Rüfenacht, S.; Sauter, S.; Gröne, A.; Steffan, J.; Strehlau, G.; Gaschen, F.P. Pharmacokinetics and Clinical Efficacy of Cyclosporine Treatment of Dogs with Steroid-Refractory Inflammatory Bowel Disease. J. Vet. Intern. Med. 2006, 20, 239–244. [Google Scholar] [CrossRef]
- Biagi, F.; Maimaris, S.; Vecchiato, C.G.; Costetti, M.; Biagi, G. Gluten-Sensitive Enteropathy of the Irish Setter and Similarities with Human Celiac Disease. Minerva Gastroenterol. Dietol. 2020, 66, 151–156. [Google Scholar] [CrossRef]
- Lowrie, M.; Garden, O.A.; Hadjivassiliou, M.; Sanders, D.S.; Powell, R.; Garosi, L. Characterization of Paroxysmal Gluten-Sensitive Dyskinesia in Border Terriers Using Serological Markers. J. Vet. Intern. Med. 2018, 32, 775–781. [Google Scholar] [CrossRef] [PubMed]
- Dandrieux, J.R.S.; Martinez Lopez, L.M.; Prakash, N.; Mansfield, C.S. Treatment Response and Long Term Follow up in Nineteen Dogs Diagnosed with Chronic Enteropathy in Australia. Aust. Vet. J. 2019, 97, 301–307. [Google Scholar] [CrossRef]
- Honneffer, J.B.; Minamoto, Y.; Suchodolski, J.S. Microbiota Alterations in Acute and Chronic Gastrointestinal Inflammation of Cats and Dogs. World J. Gastroenterol. 2014, 20, 16489–16497. [Google Scholar] [CrossRef] [PubMed]
- Shakir, L.; Javeed, A.; Ashraf, M.; Riaz, A. Metronidazole and the Immune System. Pharmazie 2011, 66, 393–398. [Google Scholar]
- Cao, X.; Dong, M.; Shen, J.; Wu, B.; Wu, C.; Du, X.; Wang, Z.; Qi, Y.; Li, B. Tilmicosin and Tylosin Have Anti-Inflammatory Properties via Modulation of COX-2 and iNOS Gene Expression and Production of Cytokines in LPS-Induced Macrophages and Monocytes. Int. J. Antimicrob. Agents 2006, 27, 431–438. [Google Scholar] [CrossRef]
- German, A.J.; Hall, E.J.; Day, M.J. Immune Cell Populations within the Duodenal Mucosa of Dogs with Enteropathies. J. Vet. Intern. Med. 2001, 15, 14–25. [Google Scholar] [CrossRef]
- Westermarck, E.; Skrzypczak, T.; Harmoinen, J.; Steiner, J.M.; Ruaux, C.G.; Williams, D.A.; Eerola, E.; Sundbäck, P.; Rinkinen, M. Tylosin-Responsive Chronic Diarrhea in Dogs. J. Vet. Intern. Med. 2005, 19, 177–186. [Google Scholar] [CrossRef]
- Craven, M.; Simpson, J.W.; Ridyard, A.E.; Chandler, M.L. Canine Inflammatory Bowel Disease: Retrospective Analysis of Diagnosis and Outcome in 80 Cases (1995–2002). J. Small Anim. Pract. 2004, 45, 336–342. [Google Scholar] [CrossRef]
- Erdmann, C.; Heilmann, R.M. Chronisch-entzündliche Darmerkrankungen beim Hund—Diagnostische und therapeutische Aspekte. Tierärztl. Prax. Ausg. K Kleintiere Heimtiere 2017, 45, 317–327. [Google Scholar] [CrossRef] [PubMed]
- Rudinsky, A.J.; Howard, J.P.; Bishop, M.A.; Sherding, R.G.; Parker, V.J.; Gilor, C. Dietary Management of Presumptive Protein-losing Enteropathy in Yorkshire Terriers. J. Small Anim. Pract. 2017, 58, 103–108. [Google Scholar] [CrossRef]
- Okanishi, H.; Yoshioka, R.; Kagawa, Y.; Watari, T. The Clinical Efficacy of Dietary Fat Restriction in Treatment of Dogs with Intestinal Lymphangiectasia. J. Vet. Intern. Med. 2014, 28, 809–817. [Google Scholar] [CrossRef] [PubMed]
- Dandrieux, J.R.S.; Noble, P.-J.M.; Scase, T.J.; Cripps, P.J.; German, A.J. Comparison of a Chlorambucil-Prednisolone Combination with an Azathioprine-Prednisolone Combination for Treatment of Chronic Enteropathy with Concurrent Protein-Losing Enteropathy in Dogs: 27 Cases (2007–2010). J. Am. Vet. Med. Assoc. 2013, 242, 1705–1714. [Google Scholar] [CrossRef]
- de Laforcade, A.; Bacek, L.; Blais, M.; Boyd, C.; Brainard, B.M.; Chan, D.L.; Cortellini, S.; Goggs, R.; Hoareau, G.L.; Koenigshof, A.; et al. 2022 Update of the Consensus on the Rational Use of Antithrombotics and Thrombolytics in Veterinary Critical Care (CURATIVE) Domain 1- Defining Populations at Risk. J. Vet. Emerg. Crit. Care 2022, 32, 289–314. [Google Scholar] [CrossRef] [PubMed]
- Jacinto, A.M.L.; Ridyard, A.E.; Aroch, I.; Watson, P.J.; Morrison, L.R.; Chandler, M.L.; Kuzi, S. Thromboembolism in Dogs with Protein-Losing Enteropathy with Non-Neoplastic Chronic Small Intestinal Disease. J. Am. Anim. Hosp. Assoc. 2017, 53, 185–192. [Google Scholar] [CrossRef]
- Goodwin, L.V.; Goggs, R.; Chan, D.L.; Allenspach, K. Hypercoagulability in Dogs with Protein-Losing Enteropathy. J. Vet. Intern. Med. 2011, 25, 273–277. [Google Scholar] [CrossRef]
- Suchodolski, J.S.; Markel, M.E.; Garcia-Mazcorro, J.F.; Unterer, S.; Heilmann, R.M.; Dowd, S.E.; Kachroo, P.; Ivanov, I.; Minamoto, Y.; Dillman, E.M.; et al. The Fecal Microbiome in Dogs with Acute Diarrhea and Idiopathic Inflammatory Bowel Disease. PLoS ONE 2012, 7, e51907. [Google Scholar] [CrossRef] [PubMed]
- Packey, C.D.; Sartor, R.B. Commensal Bacteria, Traditional and Opportunistic Pathogens, Dysbiosis and Bacterial Killing in Inflammatory Bowel Diseases. Curr. Opin. Infect. Dis. 2009, 22, 292–301. [Google Scholar] [CrossRef] [PubMed]
- Félix, A.P.; Souza, C.M.M.; De Oliveira, S.G. Biomarkers of Gastrointestinal Functionality in Dogs: A Systematic Review and Meta-Analysis. Anim. Feed Sci. Technol. 2022, 283, 115183. [Google Scholar] [CrossRef]
- Xenoulis, P.G.; Palculict, B.; Allenspach, K.; Steiner, J.M.; van House, A.M.; Suchodolski, J.S. Molecular-Phylogenetic Characterization of Microbial Communities Imbalances in the Small Intestine of Dogs with Inflammatory Bowel Disease: Small Intestinal Microbial Communities in Canine IBD. FEMS Microbiol. Ecol. 2008, 66, 579–589. [Google Scholar] [CrossRef] [PubMed]
- Cassmann, E.; White, R.; Atherly, T.; Wang, C.; Sun, Y.; Khoda, S.; Mosher, C.; Ackermann, M.; Jergens, A. Alterations of the Ileal and Colonic Mucosal Microbiota in Canine Chronic Enteropathies. PLoS ONE 2016, 11, e0147321. [Google Scholar] [CrossRef]
- AlShawaqfeh, M.K.; Wajid, B.; Minamoto, Y.; Markel, M.; Lidbury, J.A.; Steiner, J.M.; Serpedin, E.; Suchodolski, J.S. A Dysbiosis Index to Assess Microbial Changes in Fecal Samples of Dogs with Chronic Inflammatory Enteropathy. FEMS Microbiol. Ecol. 2017, 93, fix136. [Google Scholar] [CrossRef]
- Kathrani, A.; Allenspach, K.; Fascetti, A.J.; Larsen, J.A.; Hall, E.J. Alterations in Serum Amino Acid Concentrations in Dogs with Protein-losing Enteropathy. J. Vet. Intern. Med. 2018, 32, 1026–1032. [Google Scholar] [CrossRef]
- Whitfield-Cargile, C.M.; Cohen, N.D.; Chapkin, R.S.; Weeks, B.R.; Davidson, L.A.; Goldsby, J.S.; Hunt, C.L.; Steinmeyer, S.H.; Menon, R.; Suchodolski, J.S.; et al. The Microbiota-Derived Metabolite Indole Decreases Mucosal Inflammation and Injury in a Murine Model of NSAID Enteropathy. Gut Microbes 2016, 7, 246–261. [Google Scholar] [CrossRef]
- Guard, B.C.; Honneffer, J.B.; Jergens, A.E.; Jonika, M.M.; Toresson, L.; Lawrence, Y.A.; Webb, C.B.; Hill, S.; Lidbury, J.A.; Steiner, J.M.; et al. Longitudinal Assessment of Microbial Dysbiosis, Fecal Unconjugated Bile Acid Concentrations, and Disease Activity in Dogs with Steroid-responsive Chronic Inflammatory Enteropathy. J. Vet. Intern. Med. 2019, 33, 1295–1305. [Google Scholar] [CrossRef]
- Wang, S.; Martins, R.; Sullivan, M.C.; Friedman, E.S.; Misic, A.M.; El-Fahmawi, A.; de Martinis, E.C.P.; O’Brien, K.; Chen, Y.; Bradley, C.; et al. Diet-Induced Remission in Chronic Enteropathy Is Associated with Altered Microbial Community Structure and Synthesis of Secondary Bile Acids. Microbiome 2019, 7, 126. [Google Scholar] [CrossRef] [PubMed]
- Mariaule, V.; Kriaa, A.; Soussou, S.; Rhimi, S.; Boudaya, H.; Hernandez, J.; Maguin, E.; Lesner, A.; Rhimi, M. Digestive Inflammation: Role of Proteolytic Dysregulation. Int. J. Mol. Sci. 2021, 22, 2817. [Google Scholar] [CrossRef]
- Motta, J.; Magne, L.; Descamps, D.; Rolland, C.; Squarzoni–Dale, C.; Rousset, P.; Martin, L.; Cenac, N.; Balloy, V.; Huerre, M.; et al. Modifying the Protease, Antiprotease Pattern by Elafin Overexpression Protects Mice From Colitis. Gastroenterology 2011, 140, 1272–1282. [Google Scholar] [CrossRef]
- Hernandez, J.; Kriaa, A.; Mariaule, V.; Jablaoui, A.; Drut, A.; Sénécat, O.; Maguin, E.; Rhimi, M. Microbiote Intestinal et Équilibre Protéolytique Dans Les Entéropathies Inflammatoires Du Chien. Bull. De L’académie Vétérinaire De Fr. 2022, 175, 1–7. [Google Scholar] [CrossRef]
- Denadai-Souza, A.; Bonnart, C.; Tapias, N.S.; Marcellin, M.; Gilmore, B.; Alric, L.; Bonnet, D.; Burlet-Schiltz, O.; Hollenberg, M.D.; Vergnolle, N.; et al. Functional Proteomic Profiling of Secreted Serine Proteases in Health and Inflammatory Bowel Disease. Sci. Rep. 2018, 8, 7834. [Google Scholar] [CrossRef] [PubMed]
- Maeda, S.; Ohno, K.; Uchida, K.; Igarashi, H.; Goto-Koshino, Y.; Fujino, Y.; Tsujimoto, H. Intestinal Protease-Activated Receptor-2 and Fecal Serine Protease Activity Are Increased in Canine Inflammatory Bowel Disease and May Contribute to Intestinal Cytokine Expression. J. Vet. Med. Sci. 2014, 76, 1119–1127. [Google Scholar] [CrossRef]
- Comito, R.; Porru, E.; Interino, N.; Conti, M.; Terragni, R.; Gotti, R.; Candela, M.; Simoni, P.; Roda, A.; Fiori, J. Metabolic Bile Acid Profile Impairments in Dogs Affected by Chronic Inflammatory Enteropathy. Metabolites 2023, 13, 980. [Google Scholar] [CrossRef] [PubMed]
- Rivière, A.; Selak, M.; Lantin, D.; Leroy, F.; de Vuyst, L. Bifidobacteria and Butyrate-Producing Colon Bacteria: Importance and Strategies for Their Stimulation in the Human Gut. Front. Microbiol. 2016, 7, 00979. [Google Scholar] [CrossRef]
- Arpaia, N.; Campbell, C.; Fan, X.; Dikiy, S.; van Der Veeken, J.; de Roos, P.; Liu, H.; Cross, J.R.; Pfeffer, K.; Coffer, P.J.; et al. Metabolites Produced by Commensal Bacteria Promote Peripheral Regulatory T-Cell Generation. Nature 2013, 504, 451–455. [Google Scholar] [CrossRef] [PubMed]
- Rhimi, S.; Kriaa, A.; Mariaule, V.; Saidi, A.; Drut, A.; Jablaoui, A.; Akermi, N.; Maguin, E.; Hernandez, J.; Rhimi, M. The Nexus of Diet, Gut Microbiota and Inflammatory Bowel Diseases in Dogs. Metabolites 2022, 12, 1176. [Google Scholar] [CrossRef]
- Peng, L.; Li, Z.-R.; Green, R.S.; Holzman, I.R.; Lin, J. Butyrate Enhances the Intestinal Barrier by Facilitating Tight Junction Assembly via Activation of AMP-Activated Protein Kinase in Caco-2 Cell Monolayers. J. Nutr. 2009, 139, 1619–1625. [Google Scholar] [CrossRef] [PubMed]
- Kriaa, A.; Mariaule, V.; Jablaoui, A.; Rhimi, S.; Mkaouar, H.; Hernandez, J.; Korkmaz, B.; Lesner, A.; Maguin, E.; Aghdassi, A.; et al. Bile Acids: Key Players in Inflammatory Bowel Diseases? Cells 2022, 11, 901. [Google Scholar] [CrossRef]
- Blake, A.B.; Guard, B.C.; Honneffer, J.B.; Lidbury, J.A.; Steiner, J.M.; Suchodolski, J.S. Altered Microbiota, Fecal Lactate, and Fecal Bile Acids in Dogs with Gastrointestinal Disease. PLoS ONE 2019, 14, e0224454. [Google Scholar] [CrossRef]
- Suchodolski, J.S.; Dowd, S.E.; Westermarck, E.; Steiner, J.M.; Wolcott, R.D.; Spillmann, T.; Harmoinen, J.A. The Effect of the Macrolide Antibiotic Tylosin on Microbial Diversity in the Canine Small Intestine as Demonstrated by Massive Parallel 16S rRNA Gene Sequencing. BMC Microbiol. 2009, 9, 210. [Google Scholar] [CrossRef]
- Werner, M.; Suchodolski, J.S.; Straubinger, R.K.; Wolf, G.; Steiner, J.M.; Lidbury, J.A.; Neuerer, F.; Hartmann, K.; Unterer, S. Effect of Amoxicillin-clavulanic Acid on Clinical Scores, Intestinal Microbiome, and Amoxicillin-resistant Escherichia Coli in Dogs with Uncomplicated Acute Diarrhea. J. Vet. Intern. Med. 2020, 34, 1166–1176. [Google Scholar] [CrossRef] [PubMed]
- Ziese, A.-L.; Suchodolski, J.S. Impact of Changes in Gastrointestinal Microbiota in Canine and Feline Digestive Diseases. Vet. Clin. North Am. Small Anim. Pract. 2021, 51, 155–169. [Google Scholar] [CrossRef] [PubMed]
- Manchester, A.C.; Webb, C.B.; Blake, A.B.; Sarwar, F.; Lidbury, J.A.; Steiner, J.M.; Suchodolski, J.S. Long-term Impact of Tylosin on Fecal Microbiota and Fecal Bile Acids of Healthy Dogs. J. Vet. Intern. Med. 2019, 33, 2605–2617. [Google Scholar] [CrossRef] [PubMed]
- Suchodolski, J.S. Diagnosis and Interpretation of Intestinal Dysbiosis in Dogs and Cats. Vet. J. 2016, 215, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Kilpinen, S.; Spillmann, T.; Syrjä, P.; Skrzypczak, T.; Louhelainen, M.; Westermarck, E. Effect of Tylosin on Dogs with Suspected Tylosin-Responsive Diarrhea: A Placebo-Controlled, Randomized, Double-Blinded, Prospective Clinical Trial. Acta Vet. Scand. 2011, 53, 26. [Google Scholar] [CrossRef] [PubMed]
- Kilpinen, S.; Spillmann, T.; Westermarck, E. Efficacy of Two Low-Dose Oral Tylosin Regimens in Controlling the Relapse of Diarrhea in Dogs with Tylosin-Responsive Diarrhea: A Prospective, Single-Blinded, Two-Arm Parallel, Clinical Field Trial. Acta Vet. Scand. 2014, 56, 43. [Google Scholar] [CrossRef]
- Igarashi, H.; Maeda, S.; Ohno, K.; Horigome, A.; Odamaki, T.; Tsujimoto, H. Effect of Oral Administration of Metronidazole or Prednisolone on Fecal Microbiota in Dogs. PLoS ONE 2014, 9, e107909. [Google Scholar] [CrossRef]
- Pilla, R.; Gaschen, F.P.; Barr, J.W.; Olson, E.; Honneffer, J.B.; Guard, B.C.; Blake, A.B.; Villanueva, D.; Khattab, M.R.; AlShawaqfeh, M.K.; et al. Effects of Metronidazole on the Fecal Microbiome and Metabolome in Healthy Dogs. J. Vet. Intern. Med. 2020, 34, 1853–1866. [Google Scholar] [CrossRef] [PubMed]
- Belchik, S.E.; Oba, P.M.; Wyss, R.; Asare, P.T.; Vidal, S.; Miao, Y.; Adesokan, Y.; Suchodolski, J.S.; Swanson, K.S. Effects of a Milk Oligosaccharide Biosimilar on Fecal Characteristics, Microbiota, and Bile Acid, Calprotectin, and Immunoglobulin Concentrations of Healthy Adult Dogs Treated with Metronidazole. J. Anim. Sci. 2023, 101, skad011. [Google Scholar] [CrossRef] [PubMed]
- Pinna, C.; Vecchiato, C.G.; Grandi, M.; Mammi, L.M.E.; Stefanelli, C.; Biagi, G. In Vitro Evaluation of the Effects of Tylosin on the Composition and Metabolism of Canine Fecal Microbiota. Animals 2020, 10, 98. [Google Scholar] [CrossRef]
- Marclay, M.; Dwyer, E.; Suchodolski, J.S.; Lidbury, J.A.; Steiner, J.M.; Gaschen, F.P. Recovery of Fecal Microbiome and Bile Acids in Healthy Dogs after Tylosin Administration with and without Fecal Microbiota Transplantation. Vet. Sci. 2022, 9, 324. [Google Scholar] [CrossRef] [PubMed]
- Gobeli, S.; Berset, C.; Burgener, A.I.; Perreten, V. Antimicrobial Susceptibility of Canine Clostridium Perfringens Strains from Switzerland. Schweiz. Arch. Für Tierheilkd. 2012, 154, 247–250. [Google Scholar] [CrossRef]
- Orden, C.; Blanco, J.L.; Álvarez-Pérez, S.; Garcia-Sancho, M.; Rodriguez-Franco, F.; Sainz, A.; Villaescusa, A.; Harmanus, C.; Kuijper, E.; Garcia, M.E. Isolation of Clostridium Difficile from Dogs with Digestive Disorders, Including Stable Metronidazole-Resistant Strains. Anaerobe 2017, 43, 78–81. [Google Scholar] [CrossRef]
- Nagy, E. What Do We Know about the Diagnostics, Treatment and Epidemiology of Clostridioides (Clostridium) Difficile Infection in Europe? J. Infect. Chemother. 2018, 24, 164–170. [Google Scholar] [CrossRef]
- Toombs-Ruane, L.J.; Benschop, J.; French, N.P.; Biggs, P.J.; Midwinter, A.C.; Marshall, J.C.; Chan, M.; Drinković, D.; Fayaz, A.; Baker, M.G.; et al. Carriage of Extended-Spectrum-Beta-Lactamase- and AmpC Beta-Lactamase-Producing Escherichia Coli Strains from Humans and Pets in the Same Households. Appl. Environ. Microbiol. 2020, 86, e01613-20. [Google Scholar] [CrossRef]
- Belas, A.; Menezes, J.; Gama, L.T.; Pomba, C. Sharing of Clinically Important Antimicrobial Resistance Genes by Companion Animals and Their Human Household Members. Microb. Drug Resist. 2020, 26, 1174–1185. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Sanz, E.; Ceballos, S.; Ruiz-Ripa, L.; Zarazaga, M.; Torres, C. Clonally Diverse Methicillin and Multidrug Resistant Coagulase Negative Staphylococci Are Ubiquitous and Pose Transfer Ability Between Pets and Their Owners. Front. Microbiol. 2019, 10, 485. [Google Scholar] [CrossRef] [PubMed]
- Cerquetella, M.; Rossi, G.; Suchodolski, J.S.; Schmitz, S.S.; Allenspach, K.; Rodríguez-Franco, F.; Furlanello, T.; Gavazza, A.; Marchegiani, A.; Unterer, S.; et al. Proposal for Rational Antibacterial Use in the Diagnosis and Treatment of Dogs with Chronic Diarrhoea. J. Small Anim. Pract. 2020, 61, 211–215. [Google Scholar] [CrossRef] [PubMed]
- Aggeletopoulou, I.; Konstantakis, C.; Assimakopoulos, S.F.; Triantos, C. The Role of the Gut Microbiota in the Treatment of Inflammatory Bowel Diseases. Microb. Pathog. 2019, 137, 103774. [Google Scholar] [CrossRef]
- Rufino, M.N.; Aleixo, G.F.P.; Trombine-Batista, I.E.; Giuffrida, R.; Keller, R.; Bremer-Neto, H. Systematic Review and Meta-Analysis of Preclinical Trials Demonstrate Robust Beneficial Effects of Prebiotics in Induced Inflammatory Bowel Disease. J. Nutr. Biochem. 2018, 62, 1–8. [Google Scholar] [CrossRef]
- Koleva, P.T.; Valcheva, R.S.; Sun, X.; Gänzle, M.G.; Dieleman, L.A. Inulin and Fructo-Oligosaccharides Have Divergent Effects on Colitis and Commensal Microbiota in HLA-B27 Transgenic Rats. Br. J. Nutr. 2012, 108, 1633–1643. [Google Scholar] [CrossRef] [PubMed]
- Hedin, C.; Mullard, M.; Sharratt, E.; Jansen, C.; Sanderson, J.; Shirlaw, P.; Howe, L.; Djemal, S.; Stagg, A.; Lindsay, J.; et al. Probiotic and Prebiotic Use in Patients with Inflammatory Bowel Disease: A Case-Control Study. Inflamm. Bowel Dis. 2010, 16, 2099–2108. [Google Scholar] [CrossRef]
- Ferenczi, S.; Szegi, K.; Winkler, Z.; Barna, T.; Kovács, K.J. Oligomannan Prebiotic Attenuates Immunological, Clinical and Behavioral Symptoms in Mouse Model of Inflammatory Bowel Disease. Sci. Rep. 2016, 6, 34132. [Google Scholar] [CrossRef]
- Cai, Y.; Liu, W.; Lin, Y.; Zhang, S.; Zou, B.; Xiao, D.; Lin, L.; Zhong, Y.; Zheng, H.; Liao, Q.; et al. Compound Polysaccharides Ameliorate Experimental Colitis by Modulating Gut Microbiota Composition and Function. J. Gastroenterol. Hepatol. 2019, 34, 1554–1562. [Google Scholar] [CrossRef] [PubMed]
- Valcheva, R.; Koleva, P.; Martínez, I.; Walter, J.; Gänzle, M.G.; Dieleman, L.A. Inulin-Type Fructans Improve Active Ulcerative Colitis Associated with Microbiota Changes and Increased Short-Chain Fatty Acids Levels. Gut Microbes 2019, 10, 334–357. [Google Scholar] [CrossRef]
- Laurell, A.; Sjöberg, K. Prebiotics and Synbiotics in Ulcerative Colitis. Scand. J. Gastroenterol. 2017, 52, 477–485. [Google Scholar] [CrossRef]
- Peters, V.; Dijkstra, G.; Campmans-Kuijpers, M.J.E. Are All Dietary Fibers Equal for Patients with Inflammatory Bowel Disease? A Systematic Review of Randomized Controlled Trials. Nutr. Rev. 2021, 80, 1179–1193. [Google Scholar] [CrossRef]
- Slavin, J. Fiber and Prebiotics: Mechanisms and Health Benefits. Nutrients 2013, 5, 1417–1435. [Google Scholar] [CrossRef]
- Segarra, S.; Martínez-Subiela, S.; Cerdà-Cuéllar, M.; Martínez-Puig, D.; Muñoz-Prieto, A.; Rodríguez-Franco, F.; Rodríguez-Bertos, A.; Allenspach, K.; Velasco, A.; Cerón, J. Oral Chondroitin Sulfate and Prebiotics for the Treatment of Canine Inflammatory Bowel Disease: A Randomized, Controlled Clinical Trial. BMC Vet. Res. 2016, 12, 49. [Google Scholar] [CrossRef]
- Glanemann, B.; Seo, Y.-J.; Priestnall, S.L.; Garden, O.A.; Kilburn, L.; Rossoni-Serao, M.; Segarra, S.; Mochel, J.P.; Allenspach, K. Clinical Efficacy of Prebiotics and Glycosaminoglycans versus Placebo In Dogs with Food Responsive Enteropathy Receiving a Hydrolyzed Diet: A Pilot Study. PLoS ONE 2021, 16, e0250681. [Google Scholar] [CrossRef]
- Sahoo, D.K.; Allenspach, K.; Mochel, J.P.; Parker, V.; Rudinsky, A.J.; Winston, J.A.; Bourgois-Mochel, A.; Ackermann, M.; Heilmann, R.M.; Köller, G.; et al. Synbiotic-IgY Therapy Modulates the Mucosal Microbiome and Inflammatory Indices in Dogs with Chronic Inflammatory Enteropathy: A Randomized, Double-Blind, Placebo-Controlled Study. Vet. Sci. 2022, 10, 25. [Google Scholar] [CrossRef] [PubMed]
- Pinna, C.; Vecchiato, C.G.; Bolduan, C.; Grandi, M.; Stefanelli, C.; Windisch, W.; Zaghini, G.; Biagi, G. Influence of Dietary Protein and Fructooligosaccharides on Fecal Fermentative End-Products, Fecal Bacterial Populations and Apparent Total Tract Digestibility in Dogs. BMC Vet. Res. 2018, 14, 106. [Google Scholar] [CrossRef]
- Rahim, M.A.; Saeed, F.; Khalid, W.; Hussain, M.; Anjum, F.M. Functional and Nutraceutical Properties of Fructo-Oligosaccharides Derivatives: A Review. Int. J. Food Prop. 2021, 24, 1588–1602. [Google Scholar] [CrossRef]
- WHO. Probiotics in Food: Health and Nutritional Properties and Guidelines for Evaluation; Food and Agriculture Organization of the United Nations, World Health Organization, Eds.; FAO Food and Nutrition Paper; Food and Agriculture Organization of the United Nations, World Health Organization: Rome, Italy, 2006; ISBN 978-92-5-105513-7. [Google Scholar]
- Jensen, A.P.; Bjørnvad, C.R. Clinical Effect of Probiotics in Prevention or Treatment of Gastrointestinal Disease in Dogs: A Systematic Review. J. Vet. Intern. Med. 2019, 33, 1849–1864. [Google Scholar] [CrossRef] [PubMed]
- Rossi, G.; Pengo, G.; Caldin, M.; Palumbo Piccionello, A.; Steiner, J.M.; Cohen, N.D.; Jergens, A.E.; Suchodolski, J.S. Comparison of Microbiological, Histological, and Immunomodulatory Parameters in Response to Treatment with Either Combination Therapy with Prednisone and Metronidazole or Probiotic VSL#3 Strains in Dogs with Idiopathic Inflammatory Bowel Disease. PLoS ONE 2014, 9, e94699. [Google Scholar] [CrossRef]
- D’Angelo, S.; Fracassi, F.; Bresciani, F.; Galuppi, R.; Diana, A.; Linta, N.; Bettini, G.; Morini, M.; Pietra, M. Effect of Saccharomyces Boulardii in Dogs with Chronic Enteropathies: Double-Blinded, Placebo-Controlled Study. Vet. Rec. 2018, 182, 258. [Google Scholar] [CrossRef] [PubMed]
- Tsilingiri, K.; Rescigno, M. Postbiotics: What Else? Benef. Microbes 2013, 4, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Dobson, A.; Cotter, P.D.; Ross, R.P.; Hill, C. Bacteriocin Production: A Probiotic Trait? Appl. Environ. Microbiol. 2012, 78, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Takáčová, M.; Bomba, A.; Tóthová, C.; Micháľová, A.; Turňa, H. Any Future for Faecal Microbiota Transplantation as a Novel Strategy for Gut Microbiota Modulation in Human and Veterinary Medicine? Life 2022, 12, 723. [Google Scholar] [CrossRef] [PubMed]
- Chapman, B.C.; Moore, H.B.; Overbey, D.M.; Morton, A.P.; Harnke, B.; Gerich, M.E.; Vogel, J.D. Fecal Microbiota Transplant in Patients with Clostridium Difficile Infection: A Systematic Review. J. Trauma Acute Care Surg. 2016, 81, 756–764. [Google Scholar] [CrossRef] [PubMed]
- Lopetuso, L.R.; Deleu, S.; Godny, L.; Petito, V.; Puca, P.; Facciotti, F.; Sokol, H.; Ianiro, G.; Masucci, L.; Abreu, M.; et al. The First International Rome Consensus Conference on Gut Microbiota and Faecal Microbiota Transplantation in Inflammatory Bowel Disease. Gut 2023, 72, 1642–1650. [Google Scholar] [CrossRef] [PubMed]
- Innocente, G.; Patuzzi, I.; Furlanello, T.; Di Camillo, B.; Bargelloni, L.; Giron, M.C.; Facchin, S.; Savarino, E.; Azzolin, M.; Simionati, B. Machine Learning and Canine Chronic Enteropathies: A New Approach to Investigate FMT Effects. Vet. Sci. 2022, 9, 502. [Google Scholar] [CrossRef]
- Niina, A.; Kibe, R.; Suzuki, R.; Yuchi, Y.; Teshima, T.; Matsumoto, H.; Kataoka, Y.; Koyama, H. Improvement in Clinical Symptoms and Fecal Microbiome After Fecal Microbiota Transplantation in a Dog with Inflammatory Bowel Disease. Vet. Med. Res. Rep. 2019, 10, 197–201. [Google Scholar] [CrossRef] [PubMed]
- Niina, A.; Kibe, R.; Suzuki, R.; Yuchi, Y.; Teshima, T.; Matsumoto, H.; Kataoka, Y.; Koyama, H. Fecal Microbiota Transplantation as a New Treatment for Canine Inflammatory Bowel Disease. Biosci. Microbiota Food Health 2021, 40, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Sugita, K.; Shima, A.; Takahashi, K.; Matsuda, Y.; Miyajima, M.; Hirokawa, M.; Kondo, H.; Kimura, J.; Ishihara, G.; Ohmori, K. Successful Outcome after a Single Endoscopic Fecal Microbiota Transplantation in a Shiba Dog with Non-Responsive Enteropathy during the Treatment with Chlorambucil. J. Vet. Med. Sci. 2021, 83, 984–989. [Google Scholar] [CrossRef]
- Cerquetella, M.; Marchegiani, A.; Rossi, G.; Trabalza-Marinucci, M.; Passamonti, F.; Isidori, M.; Rueca, F. Case Report: Oral Fecal Microbiota Transplantation in a Dog Suffering From Relapsing Chronic Diarrhea—Clinical Outcome and Follow-Up. Front. Vet. Sci. 2022, 9, 893342. [Google Scholar] [CrossRef]
- Toresson, L.; Spillmann, T.; Pilla, R.; Ludvigsson, U.; Hellgren, J.; Olmedal, G.; Suchodolski, J.S. Clinical Effects of Faecal Microbiota Transplantation as Adjunctive Therapy in Dogs with Chronic Enteropathies—A Retrospective Case Series of 41 Dogs. Vet. Sci. 2023, 10, 271. [Google Scholar] [CrossRef]
- Collier, A.J.; Gomez, D.E.; Monteith, G.; Plattner, B.L.; Verbrugghe, A.; Webb, J.; Weese, J.S.; Blois, S.L. Investigating Fecal Microbial Transplant as a Novel Therapy in Dogs with Inflammatory Bowel Disease: A Preliminary Study. PLoS ONE 2022, 17, e0276295. [Google Scholar] [CrossRef]
- Boterro, E.; Benvenuti, E.; Ruggiero, P. Faecal Microbiota Transplantation in 16 Dogs with Idiopathic Inflammatory Bowel Disease. Veterinaria 2017, 31, 1–12. [Google Scholar]
- Toresson, L.; Steiner, J.M.; Suchodolski, J.S. Cholestyramine Treatment in Two Dogs with Presumptive Bile Acid Diarrhoea: A Case Report. Canine Med. Genet. 2021, 8, 1. [Google Scholar] [CrossRef]
- Jablonski Wennogle, S.A.; Stockman, J.; Webb, C.B. Prospective Evaluation of a Change in Dietary Therapy in Dogs with Steroid-resistant Protein-losing Enteropathy. J. Small Anim. Pract. 2021, 62, 756–764. [Google Scholar] [CrossRef] [PubMed]
- Duvergé, S.; Santos, N.; Dias, M.; Hebert, M.; Bettin, E.; Signorelli, F.; Hernandez, J.; Procoli, F.; Leal, R. The Impact of Diet Reassessment in the Medical Management of Refractory Chronic Enteropathy in Dogs-A Retrospective Multicentric Study. In Proceedings of the European Veterinary Internal Medicine—Companion Animals Annual Congress, Gothenburg, Sweden, 3 September 2022. [Google Scholar]
- Nagata, N.; Ohta, H.; Yokoyama, N.; Teoh, Y.B.; Nisa, K.; Sasaki, N.; Osuga, T.; Morishita, K.; Takiguchi, M. Clinical Characteristics of Dogs with Food-responsive Protein-losing Enteropathy. J. Vet. Intern. Med. 2020, 34, 659–668. [Google Scholar] [CrossRef] [PubMed]
- Jergens, A.E.; Heilmann, R.M. Canine Chronic Enteropathy—Current State-of-the-Art and Emerging Concepts. Front. Vet. Sci. 2022, 9, 923013. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, J.; Dandrieux, J.R.S. From Bench Top to Clinics: How New Tests Can Be Helpful in Diagnosis and Management of Dogs with Chronic Enteropathies. Vet. Clin. N. Am. Small Anim. Pract. 2021, 51, 137–153. [Google Scholar] [CrossRef] [PubMed]
- Heilmann, R.M.; Berghoff, N.; Mansell, J.; Grützner, N.; Parnell, N.K.; Gurtner, C.; Suchodolski, J.S.; Steiner, J.M. Association of Fecal Calprotectin Concentrations with Disease Severity, Response to Treatment, and Other Biomarkers in Dogs with Chronic Inflammatory Enteropathies. J. Vet. Intern. Med. 2018, 32, 679–692. [Google Scholar] [CrossRef]
Figure 1.
Representation of the “old” classification of canine chronic inflammatory enteropathies. FRE: food-responsive enteropathy, ARE: antibiotic-responsive enteropathy, IRE: immunosuppressant-responsive enteropathy, NRE: non-responsive enteropathy and IBD: inflammatory bowel disease if mucosal inflammation is demonstrated. Reprinted with permission from Ref. [1]. Copyright 2016 British Small Animal Veterinary Association.
Figure 1.
Representation of the “old” classification of canine chronic inflammatory enteropathies. FRE: food-responsive enteropathy, ARE: antibiotic-responsive enteropathy, IRE: immunosuppressant-responsive enteropathy, NRE: non-responsive enteropathy and IBD: inflammatory bowel disease if mucosal inflammation is demonstrated. Reprinted with permission from Ref. [1]. Copyright 2016 British Small Animal Veterinary Association.

Figure 2.
Proposal for a refined classification for chronic inflammatory enteropathies. FRE: food-responsive enteropathy, FR-PLE: food-responsive protein-losing enteropathy, MrMRE: microbiota-related modulation-responsive enteropathy, IRE: immunosuppressant-responsive enteropathy, IR-PLE: immunosuppressant-responsive protein-losing enteropathy, NRE: non-responsive enteropathy and NR-PLE: non-responsive protein-losing enteropathy.
Figure 2.
Proposal for a refined classification for chronic inflammatory enteropathies. FRE: food-responsive enteropathy, FR-PLE: food-responsive protein-losing enteropathy, MrMRE: microbiota-related modulation-responsive enteropathy, IRE: immunosuppressant-responsive enteropathy, IR-PLE: immunosuppressant-responsive protein-losing enteropathy, NRE: non-responsive enteropathy and NR-PLE: non-responsive protein-losing enteropathy.


{kind=link}
{kind=link}
Table 1.
Summary of studies assessing the impact of metronidazole and tylosin treatments on gut microbiota in dogs.
Table 1.
Summary of studies assessing the impact of metronidazole and tylosin treatments on gut microbiota in dogs.
| Antibiotic | Reference | Design | Conclusions |
|---|---|---|---|
| Metronidazole | [60] | Metronidazole was administered twice daily at 12.5 mg/kg PO to a group of five healthy research dogs and prednisolone at 1.0 mg/kg daily to a second group of five healthy research dogs for 14 days. Fecal samples were collected on days 0, 14, 28 and 42 (14 and 28 days after cessation). | In the group receiving metronidazole, their bacterial diversity indices significantly decreased on day 14 and recovered after cessation. Bacterial composition was also significantly altered by metronidazole on day 14 and returned to its initial proportions by day 42. Conversely, no effect of prednisolone was observed on either the bacterial diversity or composition. |
| [61] | Prospective, non-randomized controlled study. Dogs fed various commercial diets were divided into three groups: the control group; the group receiving a hydrolyzed protein diet, followed by metronidazole administration; and the group receiving metronidazole only. | Metronidazole significantly changed microbiota composition in dogs treated with metronidazole only, and that change did not fully resolve 4 weeks after treatment discontinuation. Increased fecal total lactate and decreased fecal deoxycholic acid and lithocholic acid (secondary bile acids) were concurrently observed. | |
| [62] | Twelve healthy adult female dogs were used in an 8-week crossover design study. All dogs were fed a control diet during a 2-week baseline and then randomly allotted to one of the two treatment arms (diet only or diet + 1% prebiotic GNU100) for another 6 weeks. From weeks 2 to 4, dogs were orally administered metronidazole (20 mg/kg) twice daily. | Metronidazole reduced fecal microbial alpha diversity and Blautia, Fusobacterium (genus belonging to Fusobacteria phylum), Turicibacter, Peptacetobacter hiranonis and Faecalibacterium abundances and increased fecal Streptococcus (genus belonging to Bacillota phylum) and Escherichia coli (species belonging to Pseudomonadota phylum) abundances. Metronidazole also increased fecal primary bile acids and reduced secondary bile acid concentrations. Most changes returned to baseline by week 8. | |
| Tylosin | [56] | Sixteen healthy dogs were randomized to receive 20 mg/kg of tylosin or a placebo capsule PO q12h for 7 days. The microbiota was assessed using 16S rRNA gene sequencing. Unconjugated bile acids were measured. | Samples from tylosin-exposed dogs exhibited decreased bacterial diversity characterized by a decrease in anaerobes Fusobacteriaceae (family of Fusobacteria phylum) and Veillonellaceae (family of Bacillota phylum) by day 7. Primary unconjugated bile acid fecal concentrations were increased on day 21 and day 63 compared to day 0 in dogs receiving tylosin. Changes did not uniformly resolve after discontinuation of tylosin on day 63. |
| [63] | In vitro effects of tylosin, alone or associated with prebiotics, on a canine fecal suspension and the residue of in vitro digested dry dog food. | Tylosin resulted in lower total volatile fatty acids and Lactobacillus abundance; higher Peptacedobacter cluster I abundance after 6 h; and higher pH values, spermidine, and E. coli abundance throughout the study. When associated with tylosin, prebiotics counteracted some undesirable effects of the antibiotic treatment. | |
| [64] | Prospective, randomized, placebo-controlled study. Sixteen healthy dogs received 20 mg/kg PO tylosin once daily (days 1–7) and were randomly assigned to either receive one fecal microbiota transplantation (FMT) via enema (day 8), daily oral FMT capsules (days 8–21) or daily placebo capsules (days 8–21). | Tylosin altered the abundance of most evaluated bacteria and induced a significant decrease in secondary bile acid fecal concentrations by day 7 in all dogs. However, most parameters returned to baseline by day 14 in all dogs. | |
| [53] | Tylosin was administered at 20 to 22 mg/kg q 24 h PO for 14 days to five healthy dogs with a pre-existing jejunal fistula. Jejunal brush samples were collected through the fistula on days 0, 14 and 28. | Microbial diversity was reduced during tylosin treatment. On day 14, the proportions of Enterococcus-like organisms (genus of Bacillota phylum), Pasteurella spp. (genus of Pseudomonadota phylum) and Dietzia spp. (genus of Actinomycetota phylum) significantly increased, and proportions of Spirochaetes (class of Spirochaetota phylum), Streptomycetaceae (family of Actinomycetota phylum) and Prevotellaceae (family of Bacteroidota phylum) significantly decreased. On day 28, the proportion of E. coli-like organisms was increased in comparison to day 0, the phylogenetic composition of the microbiota was similar to that on day 0 in only two out of five dogs, and Spirochaetes, Streptomycetaceae and Prevotellaceae failed to recover. |
Table 2.
Summary of studies assessing the effect of different strategies to modulate gut microbiota.
Table 2.
Summary of studies assessing the effect of different strategies to modulate gut microbiota.
| Strategy | Reference | Design | Conclusion |
|---|---|---|---|
| Prebiotics | [82] | Twenty-seven IBD dogs were randomized to be fed with chondroitin sulphate and prebiotics (resistant starch, β-glucans and mannaoligosaccharides) or placebo in addition to a hydrolyzed diet and were evaluated after 30, 60, 90 and 180 days of treatment. | No significant differences were found between groups at any point for CIBDAI, WSAVA histologic score or fecal microbiota evaluated by PCR-RLFP. |
| [83] | Thirteen dogs with FREs were randomized to be fed a combination of prebiotics (β-glucans and mannan oligosaccharides), chondroitin sulphate and glycosaminoglycans or placebo in addition to a hydrolyzed diet for 10 weeks. Relapse rate was monitored every 2 weeks until week 18. | No significant differences were found over time or between groups for CCECAI, endoscopy scoring or histological scoring, nor in the relapse rate after switching back to the original diet. | |
| Probiotics | [88] | A systematic review of clinical effect of probiotics in prevention or treatment of gastrointestinal disease in dogs, including twelve studies concerning acute gastrointestinal disease and five concerning chronic gastrointestinal disease. | The current data point toward a very limited and possibly clinically unimportant effect for prevention or treatment of acute gastrointestinal disease. For chronic gastrointestinal disease, dietary intervention remains the major key in treatment, whereas probiotic supplement seems not to add significant improvement. |
| [89] | Twenty dogs with IBD were randomized to receive multi-strain probiotic (VSL#3) or prednisolone/metronidazole, monitored for 60 days and re-evaluated 30 days after completing treatment. | The CIBDAI and duodenal histology scores decreased between days 0 and 90 in both groups. | |
| [90] | Twenty dogs with CIEs were randomized to receive Saccharomyces boulardii (109/kg BID) or a placebo, in addition to conventional treatment (hydrolyzed protein diet, prednisolone and antibiotic) for 60 days. | The administration of yeast was associated with a lower CCECAI score on days 45 and 60 | |
| Symbiotics | [84] | Twenty-four dogs with CIE were randomized to be fed a hydrolyzed diet and administered symbiotic-IgY (β-glucans, mannan oligosaccharides, D-mannose, Lactobacillus acidophilusn, Lactobacillus casei, Enterococcus faecium, Bacillus subtilis and immunoglobulin IgY derived from chicken egg yolk) or placebo for 6 weeks. | Dogs administered supplement exhibited decreased levels of fecal calprotectin and high-sensitivity C-reactive protein two weeks post-treatment, decreased levels of hs-CRP two- and six-weeks post-treatment, increased numbers of mucosal Clostridia and Bacteroides and decreased numbers of Enterobacteriaceae in colonic biopsies at the completion of the trial. |
| Fecal microbiota transplantation | [96] | Diversity analysis, differential abundance analysis and machine learning algorithms were applied to investigate the differences in microbiome composition between healthy and pre-FMT CIE-affected dogs, while CCECAI changes and microbial diversity metrics were used to evaluate oral freeze-dried fecal microbiota capsules’ effects. | In the healthy/pre-FMT comparison, differences were noted in alpha and beta diversity and a list of differentially abundant taxa was identified. Improvement of clinical signs was noted in 74% (20/27) of CIE-affected dogs, together with a decrease in CCECAI. Alpha and beta diversity variations between pre- and post-FMT were observed for each receiver, with a high heterogeneity in the response. |
| Fecal microbiota transplantation | [97] | A 10-year-old toy poodle diagnosed with IBD received nine FMTs by rectal enema within 6 months. 16S rRNA sequence analysis was performed before and after the FMTs. | Fecal microbiome diversity after FMT resembled that of the healthy donor dog’s fecal microbiome. The clinical symptoms improved remarkably with regard to the changes in the fecal microbiome. No observable side effects were noted. |
| [98] | FMTs were performed in nine dogs with IBD. Fecal microbiome was examined via 16S rRNA sequencing in three dogs. | The proportion in Fusobacteirum in the post-FMT fecal microbiome was increased, and the CIBDAI decreased in all dogs. | |
| [99] | A 7-year-old Shiba dog diagnosed with protein-losing NRE received one FMT along with chlorambucil. | A single FMT via endoscopic procedure into the cecum and colon drastically recovered clinical signs and clinicopathological abnormalities and corrected dysbiosis in the dog. No recurrences or adverse events were observed. | |
| [100] | A 6-year-old Labrador dog diagnosed with IBD received FMT in the form of frozen oral capsules (five capsules/10 kg body weight for five consecutive days, along with prednisolone). | The CIBDAI switched from mild to clinically insignificant disease in 21 days. In the 18 months following FMT, the dog had some relapses defined as milder than before the FMT. No adverse effects were reported. | |
| [101] | Forty-one dogs with CIEs not responding to diet, probiotics or immunosuppression. Included dogs received one to five FMTs with fresh frozen feces via rectal enemas. | In 31/41 dogs (76%), FMT was associated with clinical improvement. In 20/41 dogs, the dose of corticosteroids was decreased and antibiotics were interrupted. The CIBDAI significantly decreased. | |
| [102] | Thirteen dogs with IBD were randomized to receive either FMT or placebo via rectal enema, along with cortisteroid therapy and a hypoallergenic diet, and were monitored for one month. | No significant differences in CCECAI between groups. | |
| [103] | Sixteen dogs with IBD received FMT, nine via an endoscopic procedure with five of them also given the transplant orally, and seven were administered by frozen capsules. They were monitored for 3 months. At the time of transplantation, all subjects were receiving immunosuppressants, antibiotics or both. | A clinical improvement was shown in most patients after transplantation, whether performed orally or endoscopically. | |
| Bile acid sequestrants | [104] | One dog with NRE and one with IRE but with unacceptable corticosteroids side effects received cholestyramine (2 g q12–24 h). | Treatment with cholestyramine resulted in marked improvement of fecal consistency, frequency of defecation and activity level in both dogs. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Dupouy-Manescau, N.; Méric, T.; Sénécat, O.; Drut, A.; Valentin, S.; Leal, R.O.; Hernandez, J. Updating the Classification of Chronic Inflammatory Enteropathies in Dogs. Animals 2024, 14, 681. https://doi.org/10.3390/ani14050681
AMA Style
Dupouy-Manescau N, Méric T, Sénécat O, Drut A, Valentin S, Leal RO, Hernandez J. Updating the Classification of Chronic Inflammatory Enteropathies in Dogs. Animals. 2024; 14(5):681. https://doi.org/10.3390/ani14050681
Chicago/Turabian StyleDupouy-Manescau, Noémie, Tristan Méric, Odile Sénécat, Amandine Drut, Suzy Valentin, Rodolfo Oliveira Leal, and Juan Hernandez. 2024. "Updating the Classification of Chronic Inflammatory Enteropathies in Dogs" Animals 14, no. 5: 681. https://doi.org/10.3390/ani14050681
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.