Environmental Disinfection Strategies to Prevent Indirect Transmission of SARS-CoV2 in Healthcare Settings

 ,
,
Abstract
:1. Introduction
Objectives
2. Materials and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.2.1. Inclusion and Exclusion Criteria
2.2.2. Search, Study Selection, and Data Collection Process
3. Results
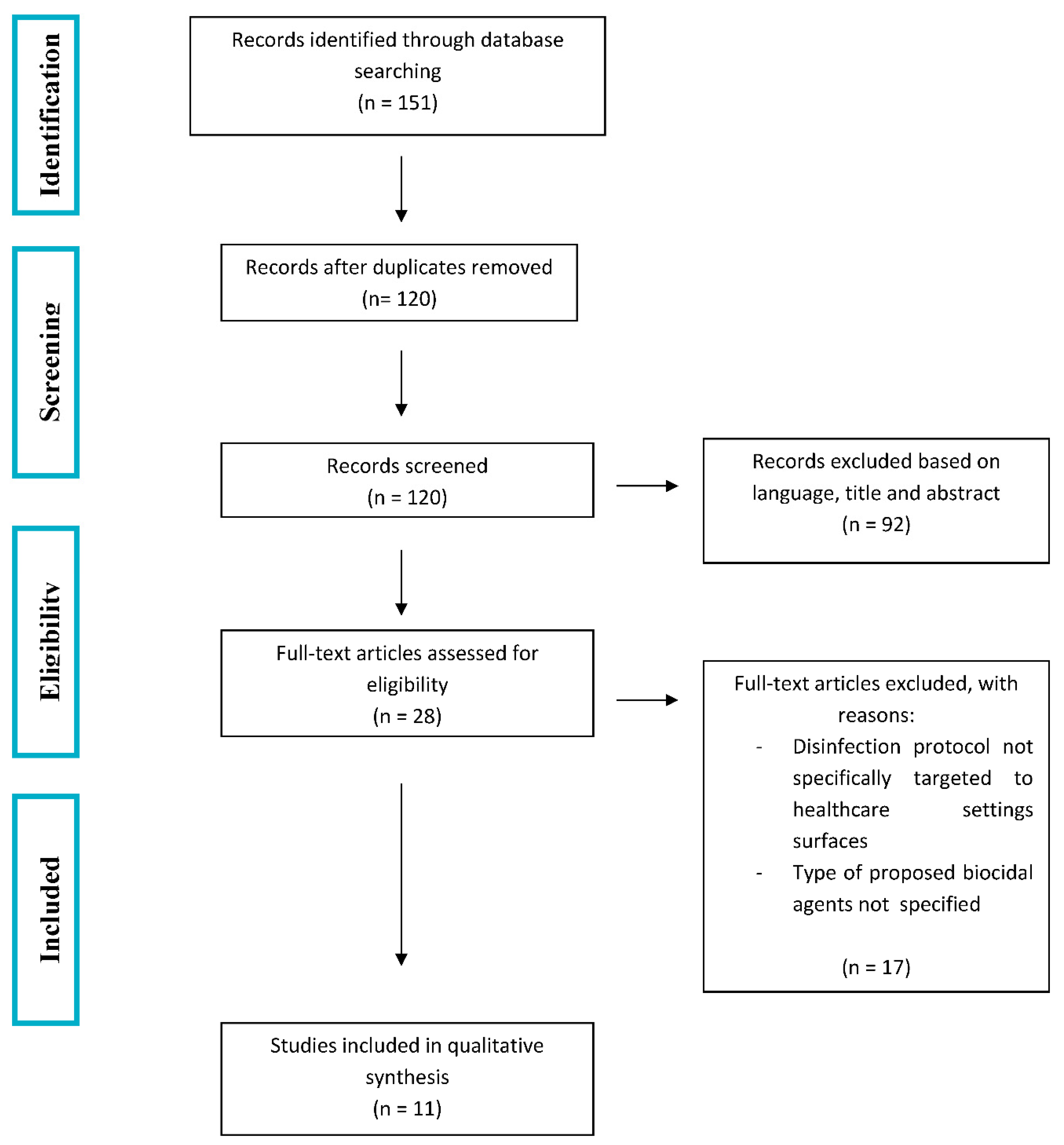
3.1. Study Selection and Characteristics
3.2. Results of Individual Studies
4. Discussion
5. Strengths and Limitations of the Study
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Guo, Y.-R.; Cao, Q.-D.; Hong, Z.; Tan, Y.-Y.; Chen, S.; Jin, H.; Tan, K.S.; Wang, D.; Yan, Y. The origin, transmission and clinical therapies on coronavirus disease 2019 (COVID-19) outbreak—An update on the status. Mil. Med. Res. 2020, 7, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.; Liu, Q.; Guo, D.-Y. Emerging coronaviruses: Genome structure, replication, and pathogenesis. J. Med. Virol. 2020, 92, 418–423. [Google Scholar] [CrossRef] [PubMed]
- Sun, P.; Lu, X.; Xu, C.; Sun, W.; Pan, B. Understanding of COVID-19 based on current evidence. J. Med. Virol. 2020, 92, 548–551. [Google Scholar] [CrossRef]
- Su, S.; Wong, G.; Shi, W.; Liu, J.; Lai, A.C.; Zhou, J.; Liu, W.; Bi, Y.; Gao, G.F. Epidemiology, Genetic Recombination, and Pathogenesis of Coronaviruses. Trends Microbiol. 2016, 24, 490–502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chavez, S.; Long, B.; Koyfman, A.; Liang, S.Y. Coronavirus Disease (COVID-19): A primer for emergency physicians. Am. J. Emerg. Med. 2020. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Adhikari, S.P.; Meng, S.; Wu, Y.-J.; Mao, Y.-P.; Ye, R.-X.; Wang, Q.-Z.; Sun, C.; Sylvia, S.; Rozelle, S.; Raat, H.; et al. Epidemiology, causes, clinical manifestation and diagnosis, prevention and control of coronavirus disease (COVID-19) during the early outbreak period: A scoping review. Infect. Dis. Poverty 2020, 9, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Gabutti, G.; D’Anchera, E.; Sandri, F.; Savio, M.; Stefanati, A. Coronavirus: Update Related to the Current Outbreak of COVID-19. Infect. Dis. Ther. 2020, 9, 241–253. [Google Scholar] [CrossRef]
- Mash, B. Primary care management of the coronavirus (COVID-19). S. Afr. Fam. Pract. (2004) 2020, 62, e1–e4. [Google Scholar] [CrossRef] [Green Version]
- Ling, L.; Wong, W.T.; Wan, W.T.P.; Choi, G.; Joynt, G.M. Infection control in non-clinical areas during the COVID-19 pandemic. Anaesthesia 2020, 75, 962–963. [Google Scholar] [CrossRef] [Green Version]
- Lai, C.-C.; Shih, T.-P.; Ko, W.-C.; Tang, H.-J.; Hsueh, P.-R. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease-2019 (COVID-19): The epidemic and the challenges. Int. J. Antimicrob. Agents 2020, 55, 105924. [Google Scholar] [CrossRef] [PubMed]
- Aitken, C.; Jeffries, D.J. Nosocomial Spread of Viral Disease. Clin. Microbiol. Rev. 2001, 14, 528–546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ros, M.; Neuwirth, L.S. Increasing global awareness of timely COVID-19 healthcare guidelines through FPV training tutorials: Portable public health crises teaching method. Nurse Educ. Today 2020, 91, 104479. [Google Scholar] [CrossRef] [PubMed]
- Powell-Jackson, T.; King, J.J.C.; Makungu, C.; Spieker, N.; Woodd, S.; Risha, P.; Goodman, C. Infection prevention and control compliance in Tanzanian outpatient facilities: A cross-sectional study with implications for the control of COVID-19. Lancet Glob. Health 2020, 8, e780–e789. [Google Scholar] [CrossRef]
- Otter, J.A.; Yezli, S.; French, G. The Role Played by Contaminated Surfaces in the Transmission of Nosocomial Pathogens. Infect. Control Hosp. Epidemiol. 2011, 32, 687–699. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Otter, J.A.; Donskey, C.; Yezli, S.; Douthwaite, S.; Goldenberg, S.D.; Weber, D. Transmission of SARS and MERS coronaviruses and influenza virus in healthcare settings: The possible role of dry surface contamination. J. Hosp. Infect. 2016, 92, 235–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Casanova, L.M.; Jeon, S.; Rutala, W.A.; Weber, D.J.; Sobsey, M.D. Effects of Air Temperature and Relative Humidity on Coronavirus Survival on Surfaces. Appl. Environ. Microbiol. 2010, 76, 2712–2717. [Google Scholar] [CrossRef] [Green Version]
- Booth, T.F.; Kournikakis, B.; Bastien, N.; Ho, J.; Kobasa, D.; Stadnyk, L.; Li, Y.; Spence, M.; Paton, S.; Henry, B.; et al. Detection of Airborne Severe Acute Respiratory Syndrome (SARS) Coronavirus and Environmental Contamination in SARS Outbreak Units. J. Infect. Dis. 2005, 191, 1472–1477. [Google Scholar] [CrossRef]
- Dowell, S.F.; Simmerman, J.M.; Erdman, D.D.; Wu, J.-S.J.; Chaovavanich, A.; Javadi, M.; Yang, J.-Y.; Anderson, L.; Tong, S.; Ho, M.S. Severe Acute Respiratory Syndrome Coronavirus on Hospital Surfaces. Clin. Infect. Dis. 2004, 39, 652–657. [Google Scholar] [CrossRef] [Green Version]
- Ong, S.W.X.; Tan, Y.K.; Chia, P.Y.; Lee, T.H.; Ng, O.-T.; Wong, M.S.Y.; Marimuthu, K. Air, Surface Environmental, and Personal Protective Equipment Contamination by Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) from a Symptomatic Patient. JAMA 2020, 323, 1610. [Google Scholar] [CrossRef] [Green Version]
- Van Doremalen, N.; Bushmaker, T.; Morris, D.H.; Holbrook, M.G.; Gamble, A.; Williamson, B.N.; Tamin, A.; Harcourt, J.L.; Thornburg, N.J.; Gerber, S.I.; et al. Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Pei, S.; Chen, B.; Song, Y.; Zhang, T.; Yang, W.; Shaman, J. Substantial undocumented infection facilitates the rapid dissemination of novel coronavirus (SARS-CoV-2). Science 2020, 368, 489–493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yen, M.Y.; Schwartz, J.; King, C.C.; Lee, C.M.; Hsueh, P.R.; Society of Taiwan Long-Term Care Infection Prevention and Control. Recommendations for protecting against and mitigating the COVID-19 pandemic in long-term care facilities. J. Microbiol. Immunol. Infect. 2020, 53, 447–453. [Google Scholar] [CrossRef] [PubMed]
- Colaneri, M.; Seminari, E.; Novati, S.; Asperges, E.; Biscarini, S.; Piralla, A.; Percivalle, E.; Cassaniti, I.; Baldanti, F.; Bruno, R.; et al. Severe acute respiratory syndrome coronavirus 2 RNA contamination of inanimate surfaces and virus viability in a health care emergency unit. Clin. Microbiol. Infect. 2020, 26, 1094.e1–1094.e5. [Google Scholar] [CrossRef] [PubMed]
- Colaneri, M.; Seminari, E.; Piralla, A.; Zuccaro, V.; Di Filippo, A.; Baldanti, F.; Bruno, R.; Mondelli, M.U.; Brunetti, E.; Di Matteo, A.; et al. Lack of SARS-CoV-2 RNA environmental contamination in a tertiary referral hospital for infectious diseases in Northern Italy. J. Hosp. Infect. 2020, 105, 474–476. [Google Scholar] [CrossRef] [Green Version]
- Liberati, A.; Altman, U.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- Kampf, G.; Todt, D.; Pfaender, S.; Steinmann, E. Persistence of coronaviruses on inanimate surfaces and their inactivation with biocidal agents. J. Hosp. Infect. 2020, 104, 246–251. [Google Scholar] [CrossRef] [Green Version]
- Dexter, F.; Parra, M.C.; Brown, J.R.; Loftus, R.W. Perioperative COVID-19 Defense: An Evidence-Based Approach for Optimization of Infection Control and Operating Room Management. Anesth. Analg. 2020, 131, 37–42. [Google Scholar] [CrossRef]
- Ti, L.K.; Ang, L.S.; Foong, T.W.; Ng, B.S.W. What we do when a COVID-19 patient needs an operation: Operating room preparation and guidance. Can. J. Anesth. 2020, 67, 756–758. [Google Scholar] [CrossRef] [Green Version]
- Li, N.; Liu, T.; Chen, H.; Liao, J.; Li, H.; Luo, Q.; Song, H.; Xiang, F.; Tan, J.; Zhou, J.; et al. Management strategies for the burn ward during COVID-19 pandemic. Burns 2020, 46, 756–761. [Google Scholar] [CrossRef]
- Chandy, P.E.; Nasir, M.U.; Srinivasan, S.; Klass, D.; Nicolaou, S.; Babu, S.B. Interventional radiology and COVID-19: Evidence-based measures to limit transmission. Diagn. Interv. Radiol. 2020, 26, 236–240. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.; Zhao, S.; Li, Z.; Chen, W.; Zhao, L.; Deng, L.; Song, B. The Battle Against Coronavirus Disease 2019 (COVID-19): Emergency Management and Infection Control in a Radiology Department. J. Am. Coll. Radiol. 2020, 17, 710–716. [Google Scholar] [CrossRef] [PubMed]
- Goh, Y.; Chua, W.; Lee, J.K.; Ang, B.W.L.; Liang, C.R.; Tan, C.A.; Choong, D.A.W.; Hoon, H.X.; Ong, M.K.L.; Quek, S.T. Operational Strategies to Prevent Coronavirus Disease 2019 (COVID-19) Spread in Radiology: Experience from a Singapore Radiology Department After Severe Acute Respiratory Syndrome. J. Am. Coll. Radiol. 2020, 17, 717–723. [Google Scholar] [CrossRef] [PubMed]
- List N: Disinfectants for Use Against SARS-CoV-2; Environmental Protection Agency. Available online: https://www.epa.gov/pesticide-registration/list-n-disinfectants-use-against-sars-cov-2 (accessed on 4 September 2020).
- Ather, A.; Patel, B.; Ruparel, N.B.; Diogenes, A.; Hargreaves, K.M. Coronavirus Disease 19 (COVID-19): Implications for Clinical Dental Care. J. Endod. 2020, 46, 584–595. [Google Scholar] [CrossRef]
- Yang, Y.; Soh, H.Y.; Cai, Z.G.; Peng, X.; Zhang, Y.; Bin Guo, C. Experience of Diagnosing and Managing Patients in Oral Maxillofacial Surgery during the Prevention and Control Period of the New Coronavirus Pneumonia. Chin. J. Dent. Res. 2020, 23, 57–62. [Google Scholar] [PubMed]
- National Health and Family Planning Commission of People’s Republic of China. Regulation for Cleaning and Disinfection Management of Environmental Surface in Healthcare (WST-512-2016). Available online: http://www.nhc.gov.cn/ewebeditor/uploadfile/2017/01/20170105092341798.pdf (accessed on 10 April 2020). (In Chinese)
- Wei, W.; Zheng, D.; Lei, Y.; Wu, S.; Verma, V.; Liu, Y.; Wei, X.; Bi, J.; Hu, D.; Han, G. Radiotherapy workflow and protection procedures during the Coronavirus Disease 2019 (COVID-19) outbreak: Experience of the Hubei Cancer Hospital in Wuhan, China. Radiother. Oncol. 2020, 148, 203–210. [Google Scholar] [CrossRef]
- Chen, W.; Su, X.-Y.; Wang, V.J.; Wang, E.C.; Xu, R.; Zhong, S.; Sun, G.; Xia, J. Novel Coronavirus International Public Health Emergency: Guidance on Radiation Oncology Facility Operation. Adv. Radiat. Oncol. 2020, 5, 560–566. [Google Scholar] [CrossRef]
- Phua, J.; Weng, L.; Ling, L.; Egi, M.; Lim, C.-M.; Divatia, J.V.; Shrestha, B.R.; Arabi, Y.M.; Ng, J.; Gomersall, C.D.; et al. Intensive care management of coronavirus disease 2019 (COVID-19): Challenges and recommendations. Lancet Respir. Med. 2020, 8, 506–517. [Google Scholar] [CrossRef]
- Scales, D.C.; Green, K.; Chan, A.K.; Poutanen, S.M.; Foster, D.; Nowak, K.; Raboud, J.M.; Saskin, R.; Lapinsky, S.E.; Stewart, T.E. Illness in intensive care staff after brief exposure to severe acute respiratory syndrome. Emerg. Infect. Dis. 2003, 9, 1205–1210. [Google Scholar] [CrossRef] [Green Version]
- Law, S.; Leung, A.W.; Xu, C. Severe acute respiratory syndrome (SARS) and coronavirus disease-2019 (COVID-19): From causes to preventions in Hong Kong. Int. J. Infect. Dis. 2020, 94, 156–163. [Google Scholar] [CrossRef]
- Abdullah, A.S.; Tomlinson, B.; Cockram, C.S.; Thomas, G.N. Lessons from the Severe Acute Respiratory Syndrome Outbreak in Hong Kong. Emerg. Infect. Dis. 2003, 9, 1042–1045. [Google Scholar] [CrossRef] [Green Version]
- Kramer, A.; Schwebke, I.; Kampf, G. How long do nosocomial pathogens persist on inanimate surfaces? A systematic review. BMC Infect. Dis. 2006, 6, 130. [Google Scholar] [CrossRef] [Green Version]
- Ashokka, B.; Loh, M.-H.; Tan, C.H.; Su, L.L.; Young, B.E.; Lye, D.C.; Biswas, A.; Illanes, S.E.; Choolani, M. Care of the pregnant woman with coronavirus disease 2019 in labor and delivery: Anesthesia, emergency cesarean delivery, differential diagnosis in the acutely ill parturient, care of the newborn, and protection of the healthcare personnel. Am. J. Obstet. Gynecol. 2020, 223, 66–74.e3. [Google Scholar] [CrossRef] [PubMed]
- Hulkower, R.; Casanova, L.M.; Rutala, W.A.; Weber, D.J.; Sobsey, M.D. Inactivation of surrogate coronaviruses on hard surfaces by health care germicides. Am. J. Infect. Control 2011, 39, 401–407. [Google Scholar] [CrossRef] [Green Version]
- Sattar, S. Microbicides and the environmental control of nosocomial viral infections. J. Hosp. Infect. 2004, 56, 64–69. [Google Scholar] [CrossRef] [PubMed]
- Agolini, G.; Raitano, A.; Viotti, P.L.; Vitali, M.; Zorzut, F. SARS: Diagnosis, therapy, and especially prevention (Reveiw). Ann. Ig. Med. Prev. Comunità 2004, 16, 211–224. [Google Scholar]
- Health Quality Ontario. Portable Ultraviolet Light Surface-Disinfecting Devices for Prevention of Hospital-Acquired Infections: A Health Technology Assessment. Ont. Health Technol. Assess. Ser. 2018, 18, 1–73. [Google Scholar]
- Pavia, M.; Simpser, E.; Becker, M.; Mainquist, W.K.; Velez, K.A. The effect of ultraviolet-C technology on viral infection incidence in a pediatric long-term care facility. Am. J. Infect. Control 2018, 46, 720–722. [Google Scholar] [CrossRef] [Green Version]
- Andersen, B.; Bånrud, H.; Bøe, E.; Bjordal, O.; Drangsholt, F. Comparison of UV C Light and Chemicals for Disinfection of Surfaces in Hospital Isolation Units. Infect. Control Hosp. Epidemiol. 2006, 27, 729–734. [Google Scholar] [CrossRef]
- Spagnuolo, G.; De Vito, D.; Rengo, S.; Tatullo, M. COVID-19 Outbreak: An Overview on Dentistry. Int. J. Environ. Res. Public Health 2020, 17, 2094. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Biocidal Agents | Time of Exposure (TE) and Viral Activity Reduction (VAR) | Disinfected Area | Study |
|---|---|---|---|
| Environmental Protection Agency (EPA)-registered disinfectants [34] | Not reported | Dental care unit | Ather et al., 2020 [35] |
| Environmental protection agency (EPA)-registered disinfectants [34] | Not reported | Interventional radiology department | Chandy et al., 2020 [31] |
| Contaminated zone: 2000 mg/L chlorine disinfectant | 30 min VAR not reported | Radiation oncology facility | Chen et al., 2020 [39] |
| 75% ethanol | Use as directed in manufacturer instructions | ||
| Semi-contaminated zone and clean zone: Disinfection according to the regulation of disinfection techniques in the healthcare setting as issued by the country prior to COVID-19 | Not reported | ||
| Quaternary ammonium + alcohol | 1–3 min VAR not reported | Operating room | Dexter et al., 2020 [28] |
| UV-C in high-risk anaesthesia work area | 20–30 min VAR not reported | ||
| Surfaces: Isopropyl alcohol 70% | not reported | Radiology department | Goh et al., 2020 [33] |
| Terminal cleaning of the scan room: Diluted bleach solution (6 mg chlorine releasing disinfectant tablet to 1000 mL water) for machine, walls, and floor. | |||
| For delicate parts of the machine (collimators, control console, exposure buttons) isopropyl alcohol 70% | |||
| Surfaces: 1000 mg/L chlorine-containing disinfectants, wiped twice with 75% ethanol | Not reported | Radiology department | Huang et al., 2020 [32] |
| Equipment: 2000 mg/L chlorine-containing disinfectant | Not reported | ||
| DR and CT gantry wiped with 500 to 1000 mg/L chlorine containing disinfectants or alcohol-containing disposable disinfectant wipes | Twice a day | ||
| Ground: 1000 mg/L chlorine-containing disinfectants | Once every 4 h | ||
| Inactivation of SARS-CoV-1 (Isolate FFM-1 and Hanoi strain) in suspension tests: Ethanol 78%, 80%, 85% and 95% | 30 s with a viral activity reduction of >5.0 log10, >4.3 log10, >5.5 log10, >5.5 log10, respectively | Inanimate surfaces of healthcare settings (department not specified) | Kampf et al., 2020 [27] |
| 2-Propanol 100% | For 30 s with a viral activity reduction of ≥3.3 log10 | ||
| 2-Propanol 45% + 1-Propanol 30% | 30 s with a viral activity reduction of ≥4.3 log10 | ||
| Formaldehyde 0.7 and 1% | 2 min with a viral activity reduction of >3.0 log10 | ||
| Glutardialdehyde 0.5 and 2.5% | 2 and 5 min respectively with a viral activity reduction of >4.0 log10 | ||
| Povidone iodine 0.23–1% | 1 min with a viral activity reduction of ≥3.8 log10 | ||
| Inactivation of SARS-CoV-1 (Strain 229E) in carrier tests: Ethanol 70% | 1 min with a viral activity reduction of >3.0 log10 | ||
| Sodium hypochlorite 0.1 and 0.5% | 1 min with a viral activity reduction of >3.0 log10 | ||
| Glutardialdehyde 2% | 1 min with a viral activity reduction of >3.0 log10 | ||
| 1000 mg/L chlorine-containing disinfectant or 75% alcohol for tables, using wipe or soak disinfection method | Not reported | Burn ward | Li et al., 2020 [30] |
| 1000 mg/L chlorine-containing disinfectant for the ground, using wipe or spray method | For no less than 30 min | ||
| Chlor-Clean for surfaces and floor | Not reported | Operating room | Ti et al., 2020 [29] |
| Mikrozid for computer screens | |||
| Clean zones: Ventilation + disinfecting wipes or ethanol 75% on surfaces | Not reported | Radiation oncology department | Wei et al., 2020 [38] |
| Semi-contaminated zones: Terminal disinfection + good ventilation | |||
| Contaminated zones: Disposable disinfecting wipes or 75% ethanol on surfaces | |||
| Floor: 1000 mg/L chlorine-containing disinfectants with spray method (twice daily) | |||
| Terminal cleaning: 75% ethanol with wipe method for surfaces | |||
| Movable UV lights (1 h) for large equipment | |||
| 1000 mg/L chlorine-containing disinfectants for floors | |||
| WST-512-2016 Guidance of Environmental and Surfaces Cleaning, Disinfection and Infection Control in Hospitals | Not reported | Oral and Maxillofacial Surgery unit | Yang et al., 2020 [36] |
| Active Ingredients | Company | Contact Time | Formulation Type | Surfaces |
|---|---|---|---|---|
| Ethanol |
| 0.5 min (30 s) | RTU | Hard nonporous |
| Hydrogen perioxide |
| 5 min | Dilutable or RTU | Hard nonporous |
| Hydrogen perioxide |
| 5 min | RTU | Hard nonporous |
| Hydrogen peroxide Ammonium carbonate Ammonium bicarbonate |
| 5 min | Pressurized liquid | Hard nonporous |
| Hydrogen peroxide Peroxyacetic acid |
|
| Dilutable | Hard nonporous |
| Hydrogen peroxide Peroxyacetic acid |
| 2 min | Dilutable | Hard nonporous |
| Hydrogen peroxide Peroxyacetic acid |
| 0.5 min (30 s) | Wipe | Hard nonporous |
| Peroxyacetic acid |
| 1 min | Dilutable | Hard nonporous |
| Hypochlorous acid |
| 10 min | RTU | Hard nonporous |
| Octanoic acid |
| 2 min | Dilutable | Hard nonporous |
| Phenolic |
| 10 min | Dilutable | Hard nonporous |
| Phenolic |
| 10 min | Dilutable | Hard nonporous |
| Phenolic |
| 5 min | RTU or wipe | Hard nonporous |
| Quaternary ammonium |
| 10 min | Dilutable | Hard nonporous |
| Quaternary ammonium |
| 10 min | Dilutable | Hard nonporous Porous (laundry pre-soak only) |
| Quaternary ammonium |
| 2 min | RTU | Hard nonporous |
| Quaternary ammonium |
| 5 min | Dilutable | Hard nonporous |
| Quaternary ammonium |
| 5 min or 10 min | Dilutable or wipe | Hard nonporous |
| Quaternary ammonium |
| 1 min | Dilutable | Hard nonporous |
| Quaternary ammonium |
| 2 min or 4 min | Wipe | Hard nonporous |
| Quaternary ammonium |
| 2 min or 3 min or 10 min | Dilutable | Hard nonporous |
| Quaternary ammonium |
| 2 min | RTU | Hard nonporous |
| Quaternary ammonium |
| 2.5 min | Wipe | Hard nonporous |
| Quaternary ammonium |
| 3 min | Wipe | Hard nonporous |
| Quaternary ammonium Ethanol |
| 2 min | RTU | Hard nonporous |
| Quaternary ammonium Ethanol |
| 1 min | Dilutable | Hard nonporous |
| Quaternary ammonium Isopropanol |
| 0.5 min (30 s) | Wipe or RTU | Hard nonporous |
| Quaternary ammonium Isopropanol |
| 2 min | RTU | Hard nonporous |
| Silver ion Citric acid |
| 1 min or 3 min | RTU | Hard nonporous |
| Sodium chlorite |
| 10 min | Dilutable or solid | Hard nonporous |
| Sodium chlorite |
| 10 min | Dilutable | Hard nonporous |
| Sodium hypochlorite |
| 5 min or 10 min | Dilutable | Hard nonporous |
| Sodium hypochlorite |
| 5 min | RTU | Hard nonporous |
| Sodium hypochlorite |
| 2 min | RTU | Hard nonporous |
| Sodium hypochlorite |
| 5 min | Dilutable | Hard nonporous |
| Sodium hypochlorite |
| 1 min or 5 min | RTU | Hard nonporous |
| Sodium hypochlorite |
| 5 min | Dilutable | Hard nonporous |
| Sodium hypochlorite |
| 1 min | RTU | Hard nonporous |
| Sodium hypochlorite |
| 1 min | Wipe | Hard nonporous |
| Risk of Infection | Disinfection Method | Contact Time | Frequency |
|---|---|---|---|
| Low-risk environment: facilities not accessible by patients, including doctors’ and nurses’ lounges |
| 1 or 2 times per day | |
| Medium-risk areas: areas accessible by normal and stable patients, mainly referring to the general ward and doctors’ office |
| Surfaces: 10 to 30 min Floor: 30 min | 1 or 2 times per day |
| High-risk areas: infected or contaminated areas or isolation areas for highly susceptible individuals, such as operating theatres, intensive care units, post-anaesthesia care units, isolation rooms |
| Surfaces: 10 to 30 min Floor: 30 min Terminal cleaning: 30 min (for sodium hypochlorite) | more than 2 times per day |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lauritano, D.; Moreo, G.; Limongelli, L.; Nardone, M.; Carinci, F. Environmental Disinfection Strategies to Prevent Indirect Transmission of SARS-CoV2 in Healthcare Settings. Appl. Sci. 2020, 10, 6291. https://doi.org/10.3390/app10186291
Lauritano D, Moreo G, Limongelli L, Nardone M, Carinci F. Environmental Disinfection Strategies to Prevent Indirect Transmission of SARS-CoV2 in Healthcare Settings. Applied Sciences. 2020; 10(18):6291. https://doi.org/10.3390/app10186291
Chicago/Turabian StyleLauritano, Dorina, Giulia Moreo, Luisa Limongelli, Michele Nardone, and Francesco Carinci. 2020. "Environmental Disinfection Strategies to Prevent Indirect Transmission of SARS-CoV2 in Healthcare Settings" Applied Sciences 10, no. 18: 6291. https://doi.org/10.3390/app10186291